
Abstract
Introduction
Asian Indians (AIs) have the highest prevalence rates (18.3%-29%) of diabetes in any minority group in the United States, yet little is known about their beliefs about what causes type 2 diabetes. The purpose of this study was to examine first generation AIs causal beliefs about type 2 diabetes.
Method
Interpretative phenomenology was used to interview 12 first-generation AI participants with type 2 diabetes to elicit causal beliefs of their disease. Interpretative and thematic analysis were completed.
Results
Beliefs about the causes of diabetes in AIs were influenced by a general familiarity with the disease, limited knowledge about causal and preventative factors of the disease, and gender specific roles and norms.
Discussion
Health programs that aim to incorporate AI’s cultural and health beliefs about the causes of diabetes are warranted.
The International Diabetes Federation (2019) has estimated that 463 million people, 9.3% of the world’s adult population have diabetes, and numbers are expected to reach 578 million by 2030. India will have roughly 101 million people with diabetes and will be the second largest population of people with the disease by 2030 (Saeedi et al., 2019).
South Asians come from India, Bangladesh, Pakistan, Africa, and Fiji. Their religious affiliations (e.g., Hindus, Sikhs, Muslims, and Christians) are as diverse as their geographic distribution. Roughly 5.4 million South Asians live in the United States, 80% of whom are Asian Indians (AIs; U.S. Census Bureau, 2019). Studies have found that AIs are 4 to 6 times more likely to have diabetes and develop it at a younger age than non-Hispanic Whites (Cowie et al., 2009). In the San Francisco Bay Area, AIs were found to have a higher risk of developing diabetes than any other ethnic group in the United States. The prevalence of diabetes between the ages 45 and 79 years of age was 29% (Kanaya et al., 2010). Similarly, Venkataraman et al. (2004) found that the overall prevalence of diabetes mellitus in AIs in Atlanta, Georgia, was 18.3%, much higher than among Blacks (12.8%), Hispanics (8.4%), and Whites (6.6%) living in the United States (Cowie et al., 2009).
Most of the studies on AIs with diabetes have been conducted in the United Kingdom and report that patients believe external factors beyond their control caused the disease. Hereditary factors, fatalism or a belief in a divine power that influences health, and the stress of immigration were identified by patients as causes of their diabetes (Farooqi et al., 2000; Lawton et al., 2007; Macaden & Clarke, 2006).
In the United States, AIs are one of the largest immigrant groups and will become the largest foreign-born group by 2055 (Budiman, 2020). Currently, there are no published studies that have examined AIs’ beliefs about the causes and understandings regarding diabetes in the United States. Because AIs experience high prevalence of diabetes, and a genetic predisposition to develop diabetes and complications that occur earlier than in other ethnic groups, understanding AI’s beliefs about causes of diabetes is essential. Personal, family, and cultural illness beliefs form the basis of many health behaviors. Since Hindus and Sikhs share similar personal, family, cultural, and dietary practices, the purpose of this study was to examine and understand their beliefs about the causes of diabetes and to identify commonalities and differences by gender among Hindus and Sikhs with type 2 diabetes.
Method
This was an interpretive phenomenological study aimed at understanding AIs beliefs about the causes of diabetes. As a methodology, interpretive phenomenology is underpinned by Heideggerian philosophy (Dreyfus, 1991) and illuminate’s aspects of experiences that may be taken for granted. A key tenet of this approach is that narratives of concrete, specific events provide insight to participants’ activities (Chesla et al., 2018). The method aims to uncover everyday beliefs and understandings that guide action. Given its focus on background understandings in a given situation, this method is particularly appropriate to explore participants’ concerns, resources, capabilities, actions taken to cope, and the subsequent outcomes (Benner, 1994; Benner et al., 2009; Smith et al., 2010).
Participants for this study were recruited from Sikh Temples in Northern California and through snowball sampling. Inclusion criteria included being of AI origin, first generation, diagnosed with type 2 diabetes for at least 6 months, over the age 18 years, and a legal permanent resident of the United States. To better understand illness beliefs, participants who were stable with their diabetes and who had no hospital admissions in the past 6 months were recruited. This study was approved by the Committee on Human Research, Institutional Review Board. Written consent to participate was obtained from each participant. An interview guide that had been tested in an earlier pilot study was used to conduct private open-ended interviews focused on health beliefs and practices with each participant; second interviews were conducted with each participant to clarify understanding and complete all study questions. All interviews were audio recorded, translated from Punjabi or Hindi to English by the first author, transcribed verbatim, and checked for accuracy for interpretive phenomenology analysis by the author.
Data Analysis
The interviews were read several times to understand the range of beliefs participants held about the causes of diabetes. All the interviews were systematically coded in Atlas ti. For this analysis, text coded as “belief of causes” and the associated narratives were retrieved for further analysis. Interpretive notes were entered into Atlas ti for each narrative and were summarized to identify qualitative distinctions and exemplars in beliefs about the causes of diabetes in AIs.
Results
Sample Characteristics
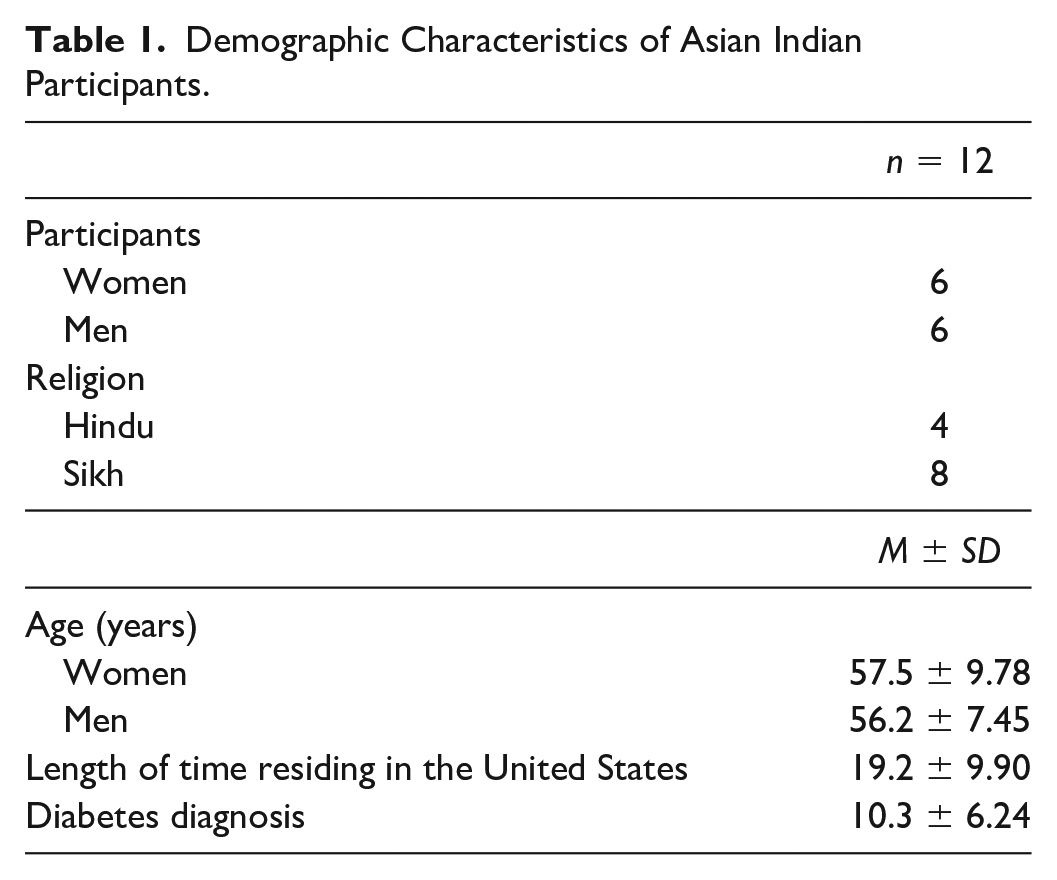
A sample of 12 adult participants (six men and six women) aged 40 to 75 years, four Hindus and eight Sikhs were recruited from local temples. The average U.S. residency was 19 years (range 1-43 years) and the average time since diagnosis of diabetes was 10 years (range 1-25 years). All the female participants worked as part-time nannies. Male participants had varied occupations, including small business owners or managerial positions. Three of the male participants were unemployed (see Table 1).
Demographic Characteristics of Asian Indian Participants.
Beliefs about the causes of diabetes were influenced by (1) general familiarity with the disease within the family or community, (2) limited knowledge about the factors that cause and prevent diabetes, and (3) gender specific roles and norms that influence causal beliefs.
General Familiarity With Diabetes Within the Family and Community
Many participants were born into a world where diabetes was an expected health event. They characterized the disease as a simple and accepted part of their everyday lives. Looking after family members with diabetes led to an early awareness and familiarity with aspects of the disease and influenced how participants anticipated and accepted their own diagnosis. A female participant became aware of diabetes as an adolescent assisting her grandmother.
P104F: It is since I was born, I have been aware of diabetes—I know it very well. My paternal grandmother had diabetes when I was 15-16 years old. I used to test her sugar and give her shots, her medications and everything she needed.
Similarly, a participant whose father-in-law had diabetes, recounted that she had no fear of being diagnosed. Having seen her father-in-law manage made it easier for her to accept her diagnosis.
P101F: I was not scared: there is no reason to be scared. My father-in-law had diabetes, and I told the physician that it is in the family. The physician told me it can happen even without a family history. So, I said okay, then it can happen.
The pervasiveness of diabetes and its symptoms in the AI community led participants to anticipate its onset in their own lives. Several participants monitored their symptoms, acknowledged that their lifestyle could cause diabetes, and sought medical care once they suspected the disease had arrived. Participants compared their symptoms with those of family members with diabetes. One man sought medical advice when he experienced “burning feet” like his wife who had diabetes.
P106M: I had burning in my feet. I knew there was something wrong and she said, “Check your blood sugar.” It was high. I went to see the doctor and he put me on medicine.
Diabetes was so prevalent in the AI community that for many it was their fate and a common part of everyday life. Participants believed that it was only a matter of time before they were diagnosed. Early awareness, familiarity, and anticipation led to a casual acceptance of the diagnosis, especially if participants had family members with diabetes. A fatalism about developing the disease, prevented participants from taking measures to prevent it. A female participant who had seen her father and brother develop diabetes acknowledged that it was inevitable that she too would acquire the disease. She believed that her family history had sealed her fate. There was nothing she could have done or could do now to avoid the disease.
P105F: No, I don’t think I could have changed anything. I knew all along about diabetes and could not have stopped it from happening to me. I knew that I would get it because my dad and my younger brother have it.
Limited Knowledge About the Factors That Cause and Prevent Diabetes
Although some participants pointed to familial history as a cause of their diabetes, others were uncertain. This uncertainty stemmed from limited knowledge about the disease, which further facilitated passive acceptance by many participants. One participant said that she was uncertain about what caused her diabetes but on reflection, she felt that her family history, childhood diet, and her physiology were all possible causes. She acknowledged that she lacked accurate information and could not identify the actual cause of her illness.
P111F: I had no idea how I got diabetes. Sometimes I think when I was small, I should not have eaten ice cream, or popsicles. Then I should not have had diabetes. If my parents had given us brown rice, brown flour when we were small. But I don’t know . . . they say never mind so even if you eat sweets, if your insulin does not build then you are going to get diabetes. So, when I take all that in consideration, I think it is not my parents. It is because of our genes.
Some participants believed that they could have prevented diabetes as younger adults, had they known about the disease and its complications.
P102F: I think if I could have controlled my habit a little bit in the past, I could have maybe avoided it. If I knew early, then I would have changed a little bit about my lifestyle, learn how diabetes affects your body. And why it is so dangerous, and I could have controlled my diet, exercised at an early age. They are somethings I wish I had known and done.
Gender Specific Social Roles and Norms That Influence Causal Beliefs About Diabetes
There were gender differences regarding what caused the disease, that were likely influenced by the distinct cultural roles of AI men and women. Female participants described personal stress, family stressors, and a lack of medical advice as causes of their disease. In contrast, male participants identified nonfamily factors as causal in diabetes, such as the sedentary lifestyle and dietary practices of everyday life in the United States.
Female Participants: Personal and Family Stressors
Although several female participants had a family history of diabetes, they described stress and worry as major contributors to their disease.
P104F: I was so surprised and concerned when I found out I was diabetic. I feel that I think that I got it because of tension. Worries caused me diabetes.
Stress as a cause of diabetes was a pervasive and strongly held belief among female participants. One woman was convinced that she and her son developed diabetes because of stress from worries.
P110F: I think, it is because of all the worries and concerns that I had. Usually, when that is the case, one develops diabetes. . . . My oldest son has developed it too. When I was sick, he cried so much and he did not take care of his health, and he got so stressed out that he developed diabetes.
Family stressors during immigration were also described as a major cause of diabetes. Several female participants reported that worrying about the adult children they left behind was a key causal stressor in their diabetes. One woman provided a vivid example. Although she had immigrated to the United States about 3 years earlier, she returned to India several times a year to look after her ailing son. This compounded the stress of acculturation in her new country. Yet she felt responsible to provide her son with financial and emotional support. Her son’s suffering, the frequent travel, and the financial and emotional stress of providing care were considered insurmountable stressors that led her to develop diabetes.
P105F: He would adjust his dislocated knee and continued to work on the farm. . . . He then went and had surgery. And with the surgery, he got an infection and was bed ridden for a whole year in Amritsar. So, I had to go every 2-3 months for 2-3 months. It was hard here in the US too; we did not have permanent work here. And you know how it is there, you can have a lot of money there, but still people need help from what you earn in the U.S. So, we helped them financially. I would come here earn some money, and then go back . . . we have gone through a lot of hardships which caused diabetes.
Separation from family during immigration to America was described by female participants as a major cause of their diabetes. Several women believed that the tension, lack of sleep, and worrying about their adult children’s immigration status caused their diabetes.
P104F: My son was all alone here, and nothing would work for him. He could not get his paperwork done; he could not come and visit us because if he left the US, he would not be able to come back—he was illegal. We were left there, in India all alone. Then slowly, we got our immigration to the US. And then we had a younger daughter, and we could not leave her alone in India either. There was a lot of tension in those days, and I was surprised and concerned why I got diagnosed with diabetes. I think that I got it from tension and worries.
A female participant, who was left alone in India with her young children while her husband immigrated to the United States, similarly believed that worrying about her family caused her diabetes.
P110F: Yes, my husband was here, and I was in India. That was stress and then I had my children to worry about—all this stress and worry led to me developing diabetes.
Traditional social norms were described, especially the expectation that that women were responsible for maintaining social harmony within the family. Household responsibilities were often overwhelming for AI women who were expected to cook, work outside the home, and maintain the family unit. One woman believed her overwhelming responsibilities, including a busy daily routine and lack of personal time caused her diabetes. Consumed by her responsibilities, she said that she had no time to take action to prevent the disease.
P108F: You know so much stress, the Asian woman working so hard—they don’t care about their health. They just watch out for their family and responsibilities, all the time busy. They don’t know the disease, or they don’t understand. But it is going to be like that until it is too late. Then they can’t go back.
Most female participants held physicians and health care providers in high regard and respected their advice. They expected their providers to monitor their disease progression and management. However, there were occasional breakdowns. One woman blamed her physician for not giving her enough information about her thyroid condition and ignoring her symptoms of prediabetes. She felt that the physician ignored her weight and fatigue. She believed that if she had received medical guidance and knowledge about thyroid disease, she could have avoided diabetes.
P108F: After my second son was born, I got problem like thyroid, and I don’t know what thyroid is. My physician did not explain to me what is thyroid and never told me to take thyroid pills every day. Sometimes I took my pills in the morning and sometimes not. I did not care about the thyroid. I gained weight- 70 pounds almost. I became tired—I told my physician, so many times. She did not do any blood tests or anything. . . Yeah, I think it is because of my physician I have this problem.
Male Participants: Work, Activity, and Food Environments
Although all male participants reported a family history of diabetes, several attributed their diabetes to external factors associated with immigrating to the United States, including lack of exercise, sedentary employment, and an overabundance of food as causal factors.
Male participants described adapting to a new work environment, sedentary employment, long hours, and a lack of exercise as causes of their diabetes. One man attributed his disease to long working hours, although he continued to worry about the heritability of the disease for his children. It is intriguing that his efforts to prevent diabetes in his children focused on dietary changes, rather than reducing stress or overwork.
P109M: Actually, when my sons came here, they got handed over more responsibility. My older son realized that I was working extremely hard, and he started working with me at the liquor store. We would get up every day at 6 am, and the go work till midnight. I have told them not to eat sweet stuff because they can get diabetes, because I have it. But it is due to my circumstances that I got diabetes. It is not hereditary, and that is why I think they will not get diabetes.
Another participant explained that long hours at his sedentary job and a lack of control over his work environment were precursors to his diabetes.
P106M: If I had a different kind of job, maybe one that you walk around a little bit, that would probably help. My job sitting is sitting down. I ride in the train. I’m a locomotive engineer—we work 24 hours on the train.
Immigrating to the United States required several male participants to change their profession. Once a teacher in Fiji, a participant now worked in a bank. In Fiji, he was physically active during the day, routinely walking 6 to 10 miles. Since he immigrated to the United States, his daily physical activity decreased considerably as his bank job which required siting for long hours at a desk, which he believed caused his diabetes.
P112M: No one is diabetic in my family except my mother. It’s because of my lifestyle changes. I am positive about it and the major reason is when I say that this type of work I do here. When I came over here, my clothes were loose, and I had to change my set of clothes here since I gained weight from the type of work I do here. It is not physically active. Over there my job was physically active, I probably walked 6-10 miles a day. Here I sit, work and eat donuts.
Male participants described food as readily available and affordable in the United States. Novel and abundant foods were blamed for participants’ overindulgence and weight gain, which in turn caused their diabetes.
P112M: There is an abundance of food here like cakes, donuts and those things. And honestly, I loved eating those. We did not have them over there, you know. We did not have those things there. It was so tasty and cheap too and you know I just made good use of what was available, without taking into consideration of what impact it would or could have on me.
Some male participants believed that AI food was the cause of their diabetes. A common breakfast food “paratha” was singled out by one participant as the cause of his diabetes. Paratha is a flat bread stuffed with potatoes or cauliflower and that is fried with oil or butter. This participant, a resident in the United States for 50 years, conceded that overeating Indian food was the cause of his diabetes. He still ate the delicious and hard to resist “parathas” several times a week.
P106M: Roti (whole wheat chapatis) have a lot of carbs, paratha, my wife is good at making them. That’s what did it—the two big parathas a day did it.
Changes of their work environment, an overabundance of food, and weight gain were described by males as precursors to the disease.
Discussion
Causal beliefs about diabetes in the current study suggest AIs immigrants to the United States identified similar beliefs about diabetes as reported in studies conducted in the United Kingdom (Farooqi et al., 2000; Macaden & Clarke, 2006; Stone et al., 2005). Hereditary factors and stress of immigration were believed to inevitably lead to diabetes.
As reported in previous studies (Bean et al., 2007; Macaden & Clarke, 2006) participants in this study reported that they had little knowledge about the process of their disease development. Most of their knowledge was derived from personal and social experiences with diabetes, rather than from medical sources. Limited knowledge and uncertainty about the causes of diabetes hindered participants from taking preventive measures and led to a passive and casual acceptance of the disease. Several participants believed their disease could have been prevented if they had had more access to medical knowledge. Despite familiarity, awareness, and anticipation of diabetes, there was a lack of attention given to disease prevention.
In AI culture, women are traditionally considered to be more passive than men and are often in charge of caring for children and maintaining the home (Kaikaya, 2000). Men traditionally provide financial support for the family and are the primary contacts outside the home. In this study, there were gender differences in the type of immigration stressors that were believed to cause diabetes. Female participants reported immigrating to theUnited States led to family stressors that contributed to their disease. Ailing adult children and separation from adult children and husbands during immigration to the United States were stressors that disrupted family harmony. Female participants felt strongly that adapting to life in the United States and maintaining family harmony were combined stressors that led to their diabetes. Overwhelming household responsibilities, lack of personal time, care giving, and family obligations were also contributors. In addition, lack of quality communication with physicians, inattentiveness and lack of guidance were also believed to be causal. These external factors fomented the worry, stress, and lack of control that led to diabetes.
Many immigrants experience downward mobility and hold positions in the United States that are lower in skills, expertise, or prestige compared to their previous occupation in their country of origin (Batalova & Fix, 2008). Male participants in the current study identified lifestyle factors they believed contributed to disease development: changes in work, increased sedentariness, and decreased daily physical exercise were additionally noted as causes. Finally, the context of disease development, particularly an overabundance of food and inexpensive sweet foods, was noted as a novel risk factor for developing diabetes after immigration in male participants.
Implications
This first known U.S. study of diabetes beliefs in AI immigrants offers insights relevant to transcultural practice, education and research. Similar to previous studies (Grace et al., 2008; Mukherjea et al., 2013; Stone et al., 2005) AIs are well aware of their increased risk for diabetes. However, they lack biomedical knowledge about what causes the disease and how it might be prevented. These findings suggest that health programs that aim to incorporate AI’s cultural beliefs and knowledge about the causes of diabetes are warranted. Clinical programs should address AIs beliefs about risks, but limited understanding of the causes and prevention of the disease. Straightforward and accessible information about multiple mutable risk factors that can cause and reduce the disease are needed. For example, AI men should be encouraged to maintain preimmigration habits such as walking, and to avoid the development of dietary practices, such as overindulging in high-carbohydrate or high-fat food. Programs that acknowledge family immigration stressors and enable post immigration stress management skills are warranted. As well, programs that increase community support for women who are expected to take on multiple family and works roles, and for men who are experiencing downward mobility in their work roles would benefit AI immigrants. Early screening and education about preventive behaviors should be offered during routine health care visits with this population, especially if there is a family history of diabetes.
Further research is warranted with this large and growing population of AI immigrants who are at a substantial risk of developing type 2 diabetes. Exploration of causal beliefs in a larger representative sample of diverse AI groups and second-generation AIs is warranted. As well, research on cultural adaptations to existing diabetes education and support programs for AIs are urgently needed.
Limitations
This study described beliefs about the cause of diabetes in nonprofessional first generation AIs (Hindus and Sikhs) in Northern California and are not generalizable to Christian or Muslim AIs, professional AIs, second-generation AIs or AIs with type 1 diabetes.
Footnotes
Acknowledgements
The author would like to thank all the participants who gave their time to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.