
Abstract
Introduction:
The World Health Organization states that suicide is the second leading cause of death among youngs, and racism has been proven to have detrimental effects on both physical and mental health. These two plagues represent a public health priority, especially for susceptible minorities.
Method:
This systematic review analyzed 23 studies from multiple database searches, to understand the relationship between racism and suicidality in young minority groups.
Results:
The review demonstrated the correlation between racism and suicidality with the consequent development of mental disorders. There is strong evidence that the main suicide risk factor is acculturation, interpreted as the assimilation of the dominant culture with the loss of values from one’s cultural background.
Discussion:
Health care professionals should not underestimate the risk of suicidality associated with racism. Prevention is crucial and it should be implemented from a young age, in schools, through a joint intervention with children and their families, aiming toward integration without acculturation.
Background
Racism has profound effects on a broad variety of social interactions, including access and nature of medical treatment (Duggan et al., 2020) and it is a worldwide problem which causes inequalities in power, resources, and opportunities (McKenzie, 2003; Priest et al., 2013). It stems from the belief that humans are subdivided into distinct groups that are different in their social behavior and innate capacities (Newman, 2012) and is rooted in the historical oppression by a group defined/perceived as dominant to a group defined/perceived as inferior or undesirable (Harrell, 2000). It created a system of dominance, power, and privilege based on racial group designations, especially where members of the dominant group accept their societal privilege by maintaining structures, ideology, values, and behavior that have the intent or effect of leaving nondominant-group members relatively excluded from power, esteem, status, and/or equal access to societal resources (Harrell, 2000). These definitions are still widely accepted, because perpetuation of racism, whether subtle or overt, has often or almost always been the subject of maltreatment, unjust burden, discrimination, and hindrance toward the lives of racial/ethnic minority groups (Keum & Miller, 2018). We can distinguish two main forms of racism: individual racism and systemic racism. The first form is the most common and easier to detect, while systemic racism is not as noticeable since its effects are supported across multiple institutions such as education, economy, and law, so it becomes cumulative, pervasive, and durable (Ikuenobe, 2011; Neblett, 2019).
While the link between suicide and mental disorders (in particular, depression and anxiety disorders) is well established in high-income countries, many suicides happen abruptly in moments of crisis such as financial problems, relationship break-up, or chronic pain and illness (Janssen et al., 2003; McKenzie, 2003). In addition, experiencing conflict, disaster, violence, abuse, loss, or a sense of isolation are strongly associated with suicidal behavior (McKenzie, 2003). As the Equality and Human Rights Commission has highlighted, an individual from a Black, Asian, or minority ethnic background is more prone to experience poverty, to have impoverished educational outcomes, to be jobless and to come in contact with the criminal justice system: these represent risk factors for the development of a mental illness. Minority groups are also less likely to receive medical care or support when needed (Mullins et al., 2005). Systemic racism can lead to substantial disparity in access to psychiatric care and racism indeed has a negative impact on the mental health of minority groups, apart from the country of origin (Wallace et al., 2016). Moreover, racial discrimination perpetrated in work environment can cause depressive symptomatology which is demonstrated to be linked to suicidal behavior and poor mental health conditions (Di Napoli et al., 2017).
The World Health Organization (WHO) states that every 40 second a person takes its own life, this means that approximately 800,000 people commit suicide every year. As the suicide attempts rise uncontrollably these actions negatively affect families, communities, and entire countries. Suicide may happen throughout the life span of a person and it was declared to be the second leading cause of death among 15- to 29-year-olds globally in 2016. Suicide involves more men than women and mostly occurs in high-income countries (Iemmi et al., 2016; WHO, 2019), but it is a global phenomenon in all regions of the world. The WHO statistics show the alarming figures of this phenomenon that is constantly increasing on a global scale especially among young people (WHO, 2019). Thus, the WHO considers suicide a public health priority especially for vulnerable groups such as refugees and immigrants, indigenous people, lesbian, gay, bisexual, transgender, intersex persons, and prisoners, who are exposed to racism episodes and discrimination. According to the data provided by the WHO, suicidality in minority or ethnic groups is alarming (WHO, 2019). The term suicidality defines one’s suicidal ideation, suicide plans, and suicide attempts (Slade et al., 2009).
Over the past decade, suicide rates in the United States have increased dramatically among racial and ethnic minorities, and Black Americans in particular. For Black young adults aged 15 to 24 years, suicide is the third leading cause of death with approximately 3,000 Black Americans dying by suicide each year (Brooks et al., 2020). Not only black Americans but also the Native Americans and Alaskan minorities face a great emergency in terms of suicide ideation and suicide attempts (Suicide Prevention Resource Center, 2018). For Native populations, the age-adjusted suicide death rate increased from 15.4 per 100,000 in 2009 to 22.1 per 100,000 in 2018. American Indian/Alaska Native adults are at highest risk for past-year suicide-related thoughts, followed by White and Black adults. For past-year suicide attempts, American Indian/Alaska Native adults are again at highest risk, followed by Black and Hispanic adults (Suicide Prevention Resource Center, 2020).
The present study supports the hypothesis that racism is a risk factor for suicidality in young people belonging to minority groups in developed countries. Our main research question was as follows: Is belonging to a minority group a risk factor for suicidality for young people in developed countries?
The secondary questions were as follows: What are the minority groups considered by researchers on racism and suicidality? Is there a difference in belonging to a specific minority group in terms of risk of suicidality? What are the types of racism considered? What are the risk factors, related to racism, for suicidality for young people belonging to a minority group? Are there other relevant aspects we have not considered to support the relationship between racism and suicidality emerging from the studies?
Method
This systematic review was conducted with Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines (Moher et al., 2009).
Eligibility Criteria
We included studies with an abstract and full text in order to allow researchers to sort the papers; about the age frame from 13 to 25 years, because suicide among young people (adolescents and young adults) has been an alarming factor all over the world (WHO, 2019); involving one or multiple minority or ethnic groups, considered by WHO as a fragile group and therefore more exposed to racism episodes and suicidality (WHO, 2019); conducted in the United States, in order to avoid bias related to different laws and social politics; including subjects having at least one episode of racism during life course; including at least one suicide ideation or suicide attempt and conducted in developed countries, where suicide attempts are higher (Khazaei et al., 2017).
We decided to exclude studies in other languages than English or Italian due to the language availability of the researchers; written before 2010 to make sure to use only recent studies; considering lesbian, gay, bisexual, trans, queer, and other sexual and/or gender minority community, because, however important, this parameter could represent a discrimination bias (belonging to a minority group of a minority group could be a major risk factor for suicidality, but it will not be discussed here); only regarding the U.S. setting, avoiding bias of different cultural context, meaning, societal definitions of racism.
Search Strategy
The PICO strategy was used to specify study characteristics, using the PIO version (Population, Phenomena of Interest, and Outcome) proposed for qualitative reviews (Lockwood et al., 2015). The population considered for this study are young minority groups or young ethnic groups; the phenomena of interest contemplated were racism episodes and racial discrimination and the outcomes acknowledged were suicide or suicide attempts or suicidality (the tendency of a person to commit suicide).
The electronic search was conducted according to the research questions using PubMed, CINAHL, and PsycINFO databases by combining a list of terms using Boolean operators (Table 1). We used “past 10 years” as a limit to our research. The latest search was performed on July 31, 2020.
Search Strategy.

Study Selection Strategy
Two authors performed a three-stage process of scrutinizing the documents. In the first stage, the two authors independently screened the selected titles and abstracts. After a comparison, the papers were either selected for the next phase or discarded based on a consensus using the eligibility or exclusion criteria. In cases of disagreement, a face-to-face discussion took place to achieve a consensus. In the second stage, the full text of documents meeting the eligibility criteria were independently assessed by the two authors, and the documents judged to be pertinent subsequently underwent a cross-comparison with achieve a consensus. A manual search was also conducted using the reference lists of the chosen documents.
Quality Screening of Selected Studies
In the third stage, the selected studies were assessed for their eligibility based on methodological quality and risk of bias by checking whether a set of items had been satisfied according to the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology; see online supplementary quality assessment material) statement (von Elm et al., 2007) for observational studies, the COREQ (COnsolidated criteria for REporting Qualitative research; see online supplementary quality assessment material) checklist (Tong et al., 2007) for qualitative studies, the SANRA (Scale for the Assessment of Narrative Reviews Article, see online supplementary quality assessment material; Baethge et al., 2019) for narrative reviews, the Preferred Reporting Items for Systematic reviews and Meta-Analyses checklist (Moher et al., 2009) for systematic reviews and the TRIPOD (Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis; see online supplementary quality assessment material) checklist (Collins et al., 2015). Based on these criteria, the methodological quality and risk of bias of the studies was assessed with a scoring process (0 = not reported/not considered, 1 = partially/weakly reported, and 2 = correctly and exhaustively reported; the items not applicable for a particular study were not considered). The final score was defined by the ration between the number of items scored as 2 and the total number of applicable items (range: 0-100), and the overall rating was defined as follows: <60 = poor quality (very high risk of bias), 60 to 79 = low quality (high risk of bias), 80 to 89 = good quality (moderate risk of bias), and ≥90 = high quality (low risk of bias) (Sanson et al., 2017). For each study, the scoring process was performed independently by the two authors. There was no disagreement between the two authors in reaching the final score by consensus.
Synthesis of Results
Data on year of publication, study design, minority group and ages considered, emerging risk factors for suicidality, type of racism considered, support on relationship between racism episode and suicidality were extracted from the included studies. On the basis of what emerged during studies’ analysis, we also considered signs and symptoms associated to suicidality, preventative measures, and support to the relationship between suicidality and acculturation.
Results
Study Selection
A total of 224 articles were identified through database searching and after removing the 80 duplicates, 144 articles were screened for relevance according to inclusion and exclusion criteria. The full texts were considered for 65 studies, and no additional articles were identified from reference lists. The full-text articles excluded were 42 because they did not follow the inclusion criteria (Figure 1). A total of 23 articles were included for qualitative summary as reported on Table 2.
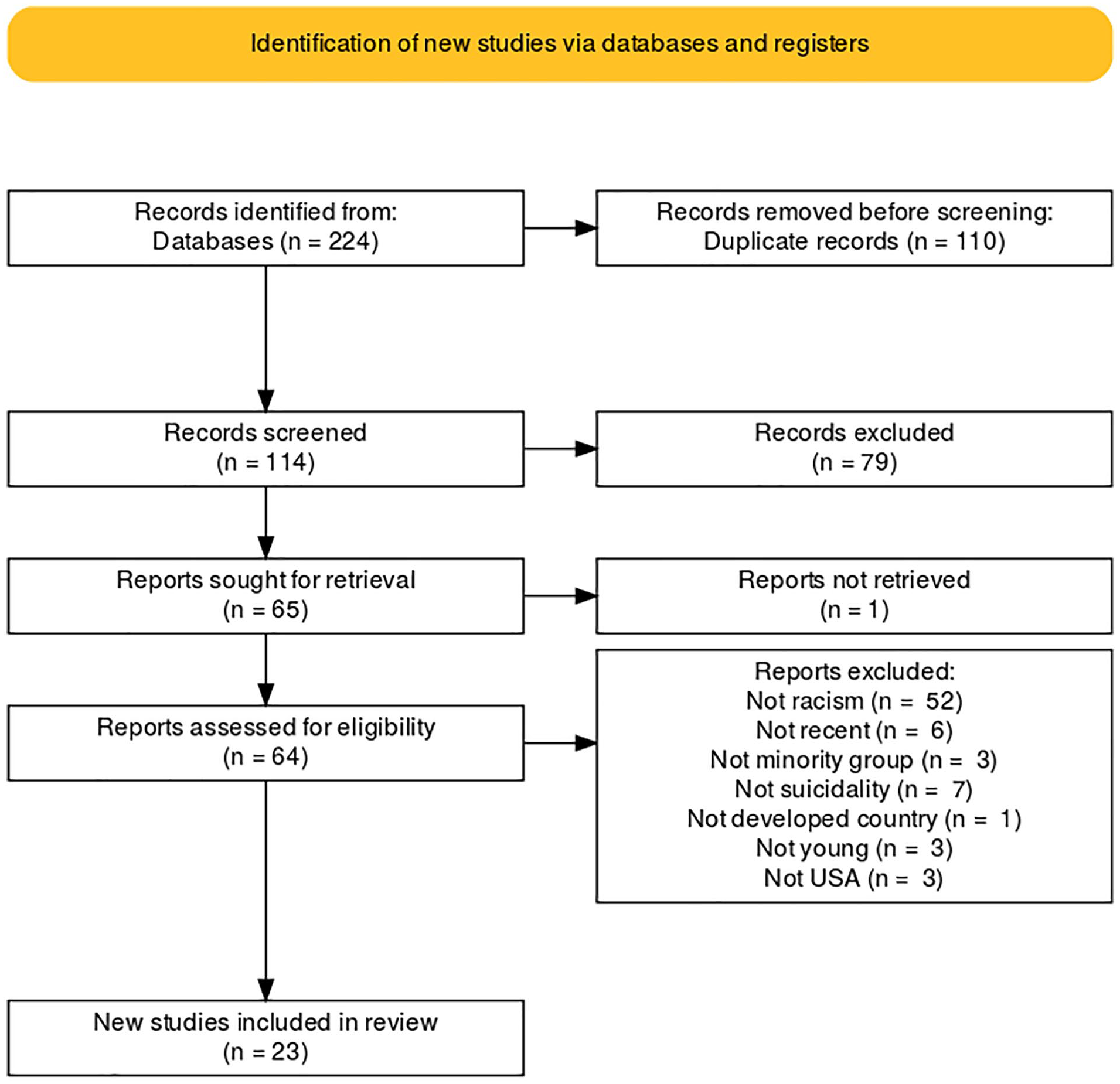
PRISMA Flowchart.
Synthesis of Findings.
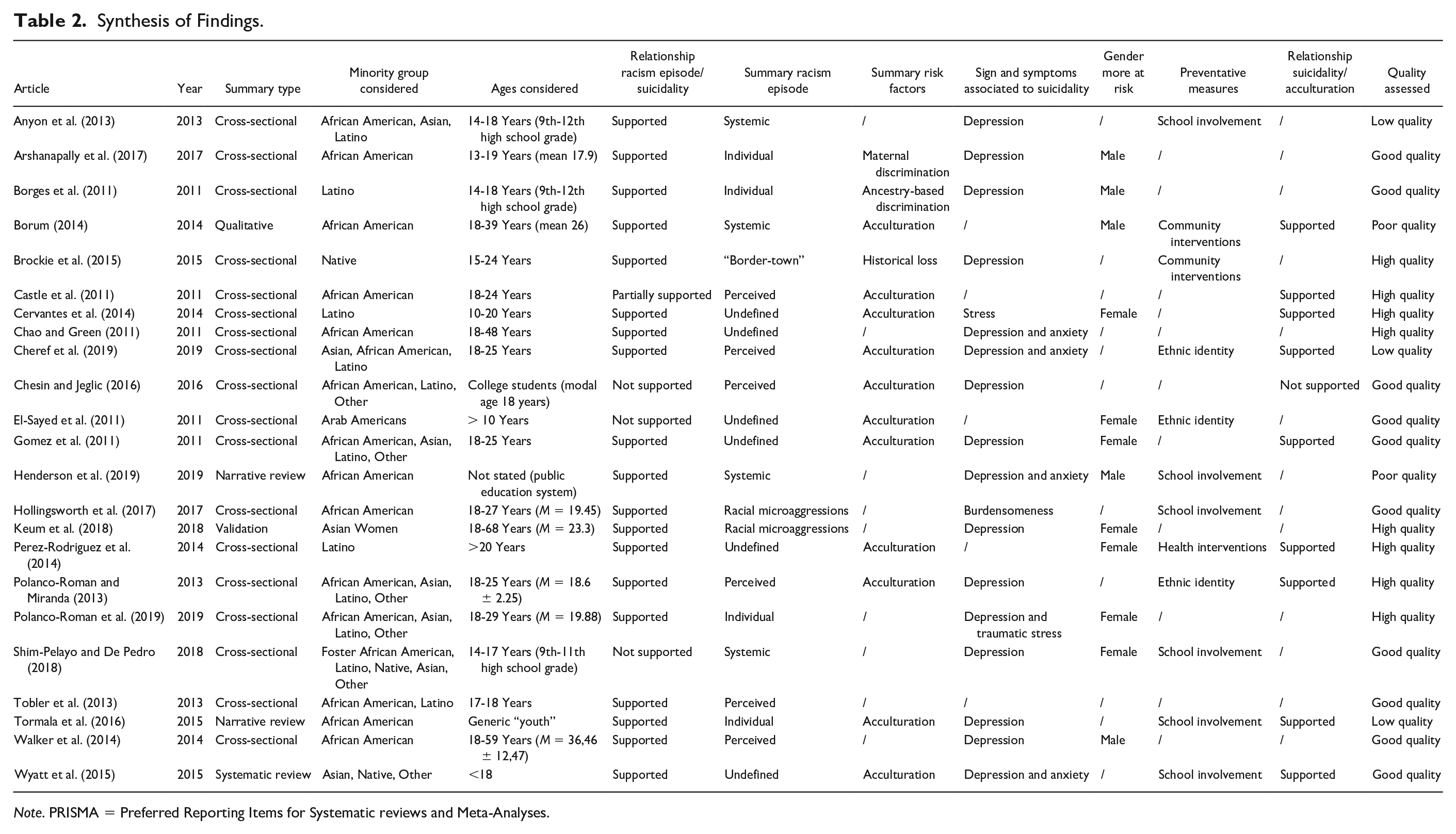
Note. PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Papers were quite equally distributed from 2011 to 2019 (max 5 in 2011, min 1 in 2016, M = 2.8, SD = 1.24), with 15 out of 23 published before 2016. In total, we analyzed 18 cross-sectional studies, 2 narrative reviews, 1 qualitative research, 1 systematic review, and 1 diagnostic tool validation.
Synthesis of Findings
The overall findings support our hypothesis: 20 studies out of 23 suggested a positive relationship between suicidality and young people belonging to a minority group in developed countries.
Minority Groups and Risk of Suicidality
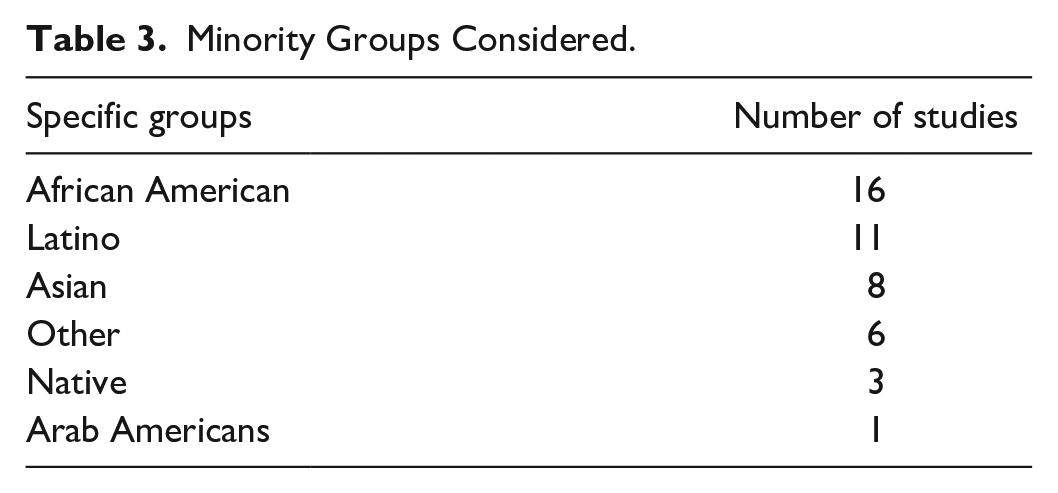
The studies considered four main minority groups: African American (16), Asian (8), Latino (11), and Native (3 studies) only one study included Arab American youths, while in 6 studies the category “Other” appeared, including all other minorities not directly mentioned (Table 3). Two studies addressed a subcategory of minority groups: Asian women (Keum et al., 2018) and foster children (Shim-Pelayo & De Pedro, 2018).
Minority Groups Considered.
There are no studies that directly compare the risk of suicidality versus belonging to a particular minority group. Being a Hispanic emerging adult and episodes of perceived discrimination would predict suicidal ideation, but not for Asian or African American individuals (Cheref et al., 2019). Moreover, racial discrimination against the family of origin increases the risk of deliberate self-harm and suicidal ideation for Latino youth (Borges et al., 2011). In addition to that, the perceptions of discrimination and racism showed an increased risk for suicidal ideation or suicidal attempts for African Americans, because these events generate stress, anger, and depression (Castle et al., 2011).
Assessment tools were developed to better understand the relationship between racial discrimination and mental health outcomes. The MSMHS (Multiculturally Sensitive Mental Health Scale) shows that perceived racism for African Americans has been found to be a more powerful predictor of psychological symptoms that were linked to depression, anxiety, and suicidal thoughts (Chao & Green, 2011). The GRMSAAW (Gendered Racial Microaggressions Scale for Asian American Women) scores predicted unique variance in depressive symptoms that were unaccounted by racism or sexism measures alone (Keum et al., 2018).
Type of Racism
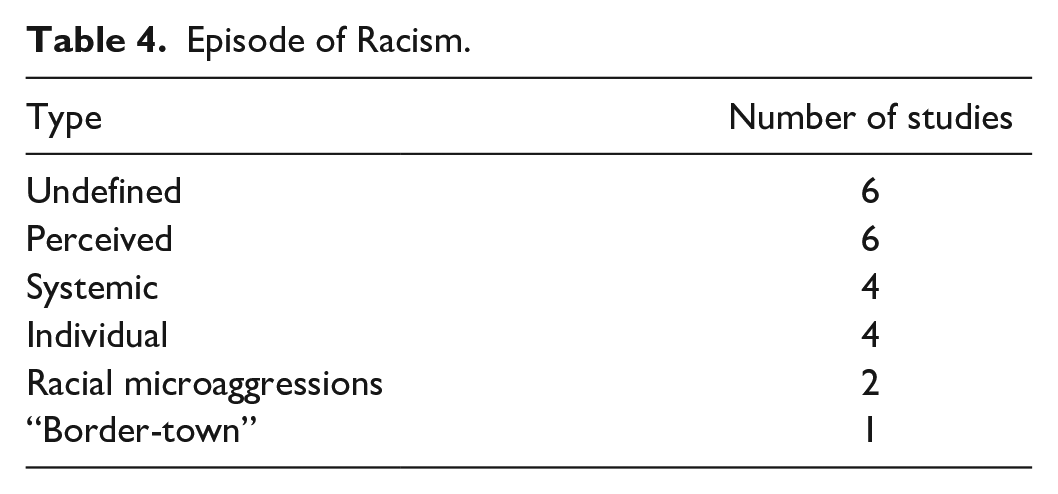
We divided the type of racism highlighted in the studies into 6 main categories: perceived, systemic, individual, racial microaggressions, “border-town racism,” and undefined (Table 4). Perceived racism consists in perceptions of prejudiced attitudes and discriminatory behaviors and it may also include perceptions of discrete forms of racism as symbolic beliefs and behaviors (Castle et al., 2011; Cheref et al., 2019; Chesin & Jeglic, 2016; Polanco-Roman & Miranda, 2013; Tobler et al., 2013; Walker et al., 2014). Systemic racism is perpetrated by institutions such as law, education, and economy and it is embedded as normal practice within society or organizations (Anyon et al., 2013; Borum, 2014; Henderson et al., 2019; Shim-Pelayo & De Pedro, 2018). Individual racism involves discriminating against a single person on the color of their skin, their cultural background, or their beliefs (Arshanapally et al., 2017; Borges et al., 2011; Polanco-Roman et al., 2019; Tormala et al., 2015). Racial microaggressions are a more contemporary form of racism and consist in verbal, behavioral, and environmental discriminations directed to a person who belongs in an ethnic or minority group. Research shows that racial microaggressions are especially popular in African Americans and have been linked to deleterious effects on their mental health (Hollingsworth et al., 2017; Keum et al., 2018). Border-town racism represents the discrimination experienced by reservations and communities. It is hypothesized to have direct effects on identity development and it mostly interests native or aboriginal communities and exacerbates the effects of historical trauma and the young person’s development (Brockie et al., 2015). We grouped under the term undefined racism the studies that did not directly express the type of racism episode investigated.
Episode of Racism.
Risk Factors for Suicidality Related to Racism
We found 14 articles regarding suicidality risk factors and, among them, 11 stated that acculturation represents the biggest risk factor for suicidality after racism. Acculturation is the assimilation of the cultural elements of the dominant society. This has been highlighted as a factor that may affect the risk for suicidality among different ethnic groups in particular Natives, African Americans, and Latinos. Acculturation compromises the individuality and values of the person making it a risk factor for suicidal ideation. Acculturative stress is associated with feelings of alienation and isolation and has been found to be associated with other suicidal risk factors such as depression (Gomez et al., 2011). Further risks were identified such as: historical loss, ancestry discrimination, and maternal discrimination. Historical loss is defined as historical trauma experiences (loss of language, culture, and land and broken treaties) along with the boarding school experience throughout the life span. It is usually associated to Native Americans (Brockie et al., 2015). Ancestry discrimination is a form of discrimination based on ancestry or nativity status, such as being an immigrant or son of immigrants (Borges et al., 2011). Maternal discrimination includes the mother’s history of racially discriminatory experiences, which could influence her children’s perceptions; notably, it is associated with suicidality only in African American male offspring, suggestive of gender-specific suicidality risk; (Arshanapally et al., 2017).
Other Relevant Aspects Emerging Form Studies
Acculturation
Since acculturation has widely emerged in the studies as an important risk factor, we broadly investigated the association between acculturation and suicidality. A total of 9 out of 11 studies supported the relationship between acculturation and suicidality. There are three main potential causes for the association between acculturation and suicidality: acculturation may signal a movement toward White culture where there is a greater propensity for suicidal thought, it may bring conflict or stress that exacerbates the risk of suicidality and it may lead to the loss of long-held values and traditions (Castle et al., 2011). African Americans, as they adapt to the mainstream culture, could lose resources from their cultural background that were previously available to them such as family cohesion, support which increases risk for suicide-related behaviors (Cheref et al., 2019). Native Americans, on the other hand, have undergone significant traumatic experiences including forced removal from sacred territories, confinement to reservations, mandatory boarding school, and mass depopulation due to starvation, disease, and military action. The historical trauma which includes loss of land, language, culture, and the mandatory boarding school, forced natives to adapt to the predominant culture resulting in suicidal thoughts or suicidal attempts (Brockie et al., 2015).
Acculturation seems to be especially problematic for Latinos: when Hispanics assimilate the culture of the country they live in much faster than their parents who attempt to maintain traditions and values, can create discrepancies in the family relationships that can develop in suicidal ideation (Cervantes et al., 2014). Moreover, acculturation has been shown to modulate the risk for suicidal ideation and attempts among Hispanics, with higher levels of acculturation associated with increased suicide risk due to factors like family disintegration, isolation, lack of language proficiency, and tension in cultural values (Perez-Rodriguez et al., 2014).
Gender as a Risk Factor
Overall findings also suggest that racism and culturally related stressors play a role in suicidality that varies by racial and ethnic group but also by gender. In this review, 16 papers studied this relationship: seven regarded only female youngs, five only male youngs. There is evidence that co-occurrence of depression and racial discrimination may evolve in suicidal ideation particularly among young women (Polanco-Roman et al., 2019). In addition to that, a research focused on Asian women, proved that racism and racial microaggressions tend to find significant relationships with psychological symptoms such as stress and depression (Keum et al., 2018).
Development of Mental Illness
Many studies (19) prove the strong relationship amid racial discrimination and the development of mental illnesses which defines the importance of recognizing the signs and symptoms that are associated to suicidality. There is compelling evidence demonstrating links between racial/ethnic discrimination and depressive symptoms (16 out of 23 studies). Research demonstrates that depression may explain the relationship between racism and suicidal ideation (Polanco-Roman et al., 2019). Specifically, one study found that increased perceptions of racial discrimination were associated with increased depression symptomatology, which was, in turn, associated with increased suicidal thoughts (Walker et al., 2014). Moreover, the combination between depression and anxiety plays an important role (Chao & Green, 2011; Cheref et al., 2019; Henderson et al., 2019; Wyatt et al., 2015). Late adolescence and early adulthood has been recognized as a time of elevated vulnerability to psychological distress from racism episodes. The experience of racism was associated with depression, anxiety, and suicidal ideation; the available literature suggests that anxiety and perceived discrimination share qualities that may exacerbate suicidality across different minority groups (Cheref et al., 2019). Other additional symptoms were found such as: stress (Cervantes et al., 2014), the association between depression and traumatic stress (Polanco-Roman et al., 2019), and burdensomeness (Hollingsworth et al., 2017).
Preventative Measures
In the overall findings, 13 studies reported methods to prevent suicidality such as school involvement (6 studies), ethnic identity (3), community interventions (2), and health interventions (1). School is one of the primary places where the development of adolescents takes part. For youth of color, social support from relevant networks such as school, neighborhood, and family, play an important role to prevent suicidality. High school social integration is an important protective factor against suicide risk. Research shows that supportive teachers and students are associated with a lower risk of suicide (Tormala et al., 2015). Improving a school’s cultural climate involves preparing school professionals to meet the various needs of youth, strengthening family and community collaboration, and tackling those actions and behaviors that exclude minorities (Shim-Pelayo & De Pedro, 2018). Findings suggest that there is a need to expand the use of culturally responsive practices and representativeness in schools (Henderson et al., 2019). A caring and affirming school climate, specifically a sense of connectedness to a school and teacher and school adult support, could play a protective role in mental health and well-being of youth (Shim-Pelayo & De Pedro, 2018). Other studies, on the other hand, focus on the development of ethnic identity as a preventative measure for suicide. Ethnic identity is the meaning an individual ascribes to identifying with his or her ethnic group, this phenomenon is accompanied by feelings of belongingness. Previous research has linked higher ethnic identity concurrently with lower symptoms of depression and suicidality. Accordingly, there may be protective properties in identifying with a racial or ethnic group (Polanco-Roman et al., 2019). Integrating ethnic culture in public health, thus in the community, is crucial in order to create a pathway for researchers to understand the role of ethnic culture and suicidal behavior in minority groups, by identifying the deep structure of cultural views (Borum, 2014).
Discussion
The results emerging from this review allow us to conclude that belonging to a minority group is a risk factor for suicidality for young people in developed countries. We already stated that 19 out of 23 studies supported this hypothesis. One study is classified as “partially supporting” the hypothesis because it strongly supports the relationship between acculturation and suicidality: it states that the acts of racism and discrimination usually are perpetrated by members of the dominant culture than by one’s family and personal network, so these victimization experiences could be less risk promoting compared with other victimization experiences that are clearly linked with suicidal thoughts and behavior (Castle et al., 2011). Three studies do not support the relationship between racism and suicidality. In one of them this finding was contrary to expectation, but researchers explained that in the population of study, students of minority race and ethnicity were in the majority, thus they may not have perceived or experienced the same minority stressors as minority students attending college where White students are the majority (Chesin & Jeglic, 2016). Another study of this group stated that the experience of being a foster child is far more stressful than belonging to a race minority: in this case, White foster youth showed a significantly higher rate of suicidal ideation and depression tendencies when compared with racial minority peers. According to authors, this could happen because the nondominant cultural capital was instrumental in the status positioning within socially marginalized groups; therefore, this may imply that foster youth of color who are placed in custody with those of another race, possess cultural capital that may contribute as a form of support (Shim-Pelayo & De Pedro, 2018). The last study opposed to our hypothesis is the only one involving Arab Americans: it found that suicide rates among them were lower than among nonethnic Whites and they concluded that stronger religious belief systems and spiritually based coping, communalism and collective social orientation, strong family bonds, affective expressiveness, and positive ethnic group identity among ethnic minority group could be protective factors for suicidality (El-Sayed et al., 2011). We can therefore conclude that these three examples may represent more the exception than the rule, given that they refer to small realities that are not representative of the general population.
Limitations
The data collection process has limitations. The study was conducted in English and Italian, excluding other languages not accessible to the researchers, therefore excluding articles potentially inherent to the study. During the search of the articles, some were not found, thus excluded.
Also the analysis has its limitations: only studies published after December 31, 2009 were taken into consideration, meaning that potentially relevant articles were not included. We must also consider that most included studies were based on cross-sectional, providing limited insight into the nature of the relationship, and based on self-reported measures which may be capturing perceived, rather than actual, experiences, and these may be subject to recall bias. Moreover, the current research comprehends articles that belong only to the United States of America and the results may not be eligible for generalization in other countries.
Conclusion
In conclusion, we can affirm that racism can lead to suicidal ideation and suicidal attempts among minority groups with a strong association between acculturation and suicidality. The studies that we focused on were set in the United States of America, therefore additional research is needed to better understand the risk factors and suicidal behaviors related to racism in other countries, especially where the migration phenomenon is growing and many racism episodes have been reported but never studied by the scientific community.
The present findings also highlight the development of preventative measures on suicidality, primarily in schools and in community settings, where the problem of racism is relevant and negatively affects the mental health of young people. It is crucial to offer a supportive environment for all students, building a network to assess the risk of suicidality in minority youngs, as well as its sign and symptoms or the needs for additional and more specific care, because the ongoing global campaign on suicide prevention and recovery states that a vital aspect of prevention lies in the early recognition and early intervention (Chan et al., 2008). Around a third of the population is expected to experience a mental health condition during their lifetime. Mental health problems affect 1 every 10 young people and an alarming 70% of young people presenting a psychological problem have not had appropriate interventions (Mental Health Foundation, 2015; WHO, 2018). Fewer than half of children with an identified mental health disorder have access to mental health services, resulting in lost education opportunities incarceration or early death due to suicide. School nurses are specialized professionals who protect and promote student health, facilitate optimal development, advance academic success, bridge health care and education, provide care coordination, advocate for quality student-centered care, and collaborate to design systems that allow individuals and communities to develop their full potential (Council on School Health, 2008; Mazyck et al., 2015). They are important for the safeguard of students’ mental disorders since they often represent the first point of contact with students and possess skills in identifying psychological issues and facilitate linkage to further resources (Bohnenkamp et al., 2015). In the larger community setting, made up of the network of schools, health and social health services, associations and other gathering places, community nurses seek to maintain and improve over time the balance and state of health of individuals in the community, and helping people avoid or manage health threats (Allard, 2020; Pisano González et al., 2019). Community nurses can also be specialized in mental health, knowing how to build trusting relationships with people who have thoughts of suicide and/or engage in suicidal behavior users and helping them to adhere to treatment programs and advising on therapies and lifestyle choices that support good mental health (Cusack et al., 2017; Cutcliffe & Stevenson, 2008). Both these professional figures could play a critical role in assessing and recognizing the effects of racism on psychological well-being but also prevent suicidal behaviors by providing nursing interventions and redirecting the students or young people of the community to a specialized health professional.
Working together, community nurses and school nurses could promote initiatives to raise awareness among both students and parents about suicidality, especially among ethnic groups, and the problem it represents for the entire population. Creating a care network around the children/adolescents at risk, interacting with family, friends, general practitioners/pediatrician, social workers, and any other subject involved in the person’s life could be crucial. It is essential to cement relations with welfare services for a multisectoral approach, whereas young people belonging to minority groups are more fragile in the social sphere and at high risk of acculturation. Interventions have to be person centered and included in a whole system of care and support, so it is necessary to enhance not just a multidimensional strategy from risk assessment to treatments, but a holistic approach to the young person, seen in the absolute uniqueness of his identity and history, and his and her social context and culture.
Supplemental Material
sj-pdf-1-tcn-10.1177_10436596211046983 – Supplemental material for The Association Between Racism and Suicidality Among Young Minority Groups: A Systematic Review
Supplemental material, sj-pdf-1-tcn-10.1177_10436596211046983 for The Association Between Racism and Suicidality Among Young Minority Groups: A Systematic Review by Giorgia Rudes and Claudia Fantuzzi in Journal of Transcultural Nursing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.