
Abstract
Introduction:
Asian Americans (AsAms) have a high prevalence of metabolic syndrome (MetS) and are one of the least physically active racial groups in America. The purpose of this study was to examine the relationship between MetS and moderate-to-vigorous physical activity (MVPA) among AsAm adults and whether acculturation modifies this relationship.
Method:
Data were from 2,259 AsAms participating in the 2011–2016 National Health and Nutrition Examination Survey. Physical activity (PA) was self-reported as minutes of weekly MVPA. Acculturation included nativity, length of residency in America, and language preference. The International Diabetes Federation criteria was used to determine the presence of MetS.
Results:
About 64.4% of AsAms did not meet the PA recommendation (MVPA ≥150 min/week). The prevalence of MetS was 39.2%. The odds of having MetS were greater among AsAms who did not meet MVPA recommendations compared with those who did meet MVPA recommendations (odds ratio [OR] = 1.5, 95% confidence interval [CI] = [1.11, 2.07]). When stratified by acculturation, this association remained statistically significant in the groups who immigrated to America more than 15 years ago and who spoke English only.
Conclusion:
MVPA reduces MetS risk in AsAm adults, especially among more acculturated AsAms. Culturally adapted programs are warranted to promote PA and adequate knowledge of disease prevention in this population.
Metabolic syndrome (MetS) is a public health concern in the United States (U.S.), which increases risk for type II diabetes, cardiovascular disease (CVD), cirrhosis, and other circulatory disorders (Moore et al., 2017; Tune et al., 2017). MetS is a clustering of CVD risk factors, including dyslipidemia, elevated blood glucose, hypertension, and central adiposity (McCracken et al., 2018). MetS in Asian Americans (AsAms) is poorly understood because this group is often omitted from public health research and national reports (Moore et al., 2017). The MetS prevalence increased significantly among AsAms from 19.9% to 26.2% from 2011 to 2016 (Hirode & Wong, 2020). Meanwhile, AsAms are overlooked or understudied because of their lower rate of obesity, leading researchers to assume they are a healthy population (Kanaya et al., 2022; Ogden et al., 2013). Consequently, little is known about MetS in AsAms, which is a barrier for addressing MetS in this population.
Physical activity (PA) has shown a favorable effect on reducing MetS risk (Lee et al., 2016; Suliga et al., 2018) and is recommended as an effective treatment for MetS (Myers et al., 2019; Wewege et al., 2018). A recent meta-analysis of exercise to reduce cardiovascular risk in people with MetS found that aerobic exercise appears to be the most beneficial form of PA for reducing MetS, particularly at longer durations (Wewege et al., 2018). Furthermore, previous studies and a meta-analysis demonstrated that leisure-time PA can reduce risk of MetS and risk of individual MetS components (He et al., 2014; Lee et al., 2018). Regular PA can reduce weight, improve blood pressure (BP), raise high-density lipoprotein (HDL), and decrease triglycerides (Abdelbasset et al., 2019; Muscella et al., 2020; Pucci et al., 2017).
The population of AsAms has increased 82% in the past two decades, making them the fastest growing minority group in the U.S. (U.S. Census Bureau, 2021). In 2019, there were 22.9 million AsAms in the U.S., with about six in 10 being non-U.S.-born (U.S. Census Bureau, 2021). Migration to the U.S. can represent a significant change in a person’s lifestyle (Baas & Yeoh, 2018; Joseph et al., 2019). Acculturation reflects social, psychological, and cultural changes, resulting in the adoption of host culture while retaining heritage culture. Acculturation has become a well-recognized area of study that may have an important influence on PA and health outcomes (Khan et al., 2016; Mao et al., 2020). Acculturation seems to play a positive effect on PA in AsAms (Zhu et al., 2021). However, other evidence suggested some immigrants’ health patterns (i.e., increasing body weight) seem to decline with more extended residence in the U.S. (Afable et al., 2016). Changes in environments and behaviors can result in challenges, such as acculturative stress and language barriers (Khullar & Chokshi, 2019) that can affect AsAms’ health. However, there are limited data on the acculturation influences in AsAms and no consistent evidence of declining or improving health behavior or health outcomes with acculturation in AsAms.
Despite the numerous benefits of PA, AsAms are the least physically active ethnic group in the U.S. (Kao et al., 2016; Yi, Roberts, et al., 2015). Meanwhile, obesity rates are dramatically increasing among this population, with an increase of 102% between 2002 and 2012, compared with a 35% increase in Whites (Yi, Kwon, et al., 2015). The increasing obesity rate among AsAms is particularly concerning, given that some adverse weight-related health outcomes, including MetS, tend to occur at lower body mass index (BMI) in this group (Fang et al., 2019; Hood et al., 2019; Hsu et al., 2015). Furthermore, as a racial group dominated by immigrants, the influences of acculturation are important aspects of AsAm health but remain understudied.
The purpose of this study was to examine the relationship between MetS and moderate-to-vigorous physical activity (MVPA) among AsAm adults and whether acculturation modifies this relationship. This study is aimed to answer the following questions:
Method
Study Design
This was a cross-sectional secondary data analysis from the 2011–2016 National Health and Nutrition Examination Survey (NHANES). The NHANES is an ongoing health-related study conducted in 2-year cycles targeting noninstitutionalized U.S. adults and uses a complex, multistage, stratified geographic area design for data collection. Since 2011, NHANES oversampled AsAms to better estimate health outcomes for this group.
Setting and Participants
The assessments consist of survey questionnaires and a standardized health examination. Participants first completed survey questionnaires administered by trained personnel at participants’ homes. Participants were then invited to a mobile examination center (MEC) for the standardized health examination, including biological samples. The unweighted sample of this study included 2,259 (weighted sample = 12,722,231) AsAm adults (age ≥18 years). Of those included, 1,034 (weighted sample = 5,781,856) underwent a health examination in which a fasting plasma sample was used for MetS determination.
Measurements
PA
The Global Physical Activity Questionnaire (GPAQ) was used to measure minutes of MVPA in a typical week. Specifically, the following questions were asked: (a) “In a typical week, did you do any moderate-intensity activities for at least 10 min that caused a small increase in breathing or heart rate? Some examples are brisk walking, bicycling, golf, and dancing.” (b) “In a typical week, did you do any vigorous-intensity activities for at least 10 min that cause large increases in breathing or heart rate? Some examples are running, lap swimming, aerobics classes, or fast bicycling.” Participants with a “yes” answer to either question were then asked about specific MVPA, how many times per week they participated in these activities, and the average duration each time they engaged in the activity. Based on the 2018 PA guidelines for Americans (Piercy et al., 2018), two levels of PA were created: (a) meeting PA recommendations (≥150 min/week of MVPA), or (b) not meeting PA recommendations (<150 min/week of MVPA).
MetS
The International Diabetes Federation (IDF) has proposed a definition of MetS, emphasizing ethnic specific values for central adiposity that are more pertinent for screening and estimating cardiovascular risk in Asians (Zhu et al., 2020). MetS was defined according to the IDF criteria as meeting three or more of the following criteria: (a) waist circumference (WC) ≥90 cm for Asian men and ≥80 cm for Asian women, (b) serum triglycerides level of ≥150 mg/dL, (c) HDL cholesterol level <40 mg/dL for men and <50 mg/dL for women, (d) fasting glucose level ≥100 mg/dL or use of antidiabetic medication (insulin or oral agents), or (e) systolic/diastolic BP ≥130/85 mmHg or use of antihypertensive medications (IDF, 2006). WC (n = 1,997) was determined by placing an anthropometric tape measure around the uppermost lateral border of the ilium while in a standing position. Fasting blood samples obtained at MECs were used to assess blood glucose (n = 993) and serum triglycerides (n = 959). Non-fasting or fasting samples were used for HDL cholesterol (n = 1,986). BP (n = 2,023) was measured after participants rested in a seated position for 5 min. Three consecutive BP readings were obtained by a certified BP examiner and the average of the three was used. Only those with fasting blood samples were eligible for analyses involving MetS determination, given two of the five components of MetS required a fasted blood sample. However, all available data were used when analyzing each MetS component separately.
Acculturation
Consistent with previous research, we used three proxies to assess acculturation: nativity, length of time in the U.S., and language use at home (Ma et al., 2012). We combined nativity and length of residency in the U.S. as one variable. Nativity was defined by U.S.-born versus non-U.S.-born. Only non-U.S.-born AsAms reported their length of residency in the U.S. Thus, temporality and nativity include three categories: living in the U.S. <15 years, living in the U.S. ≥15 years, and U.S.-born (Ma et al., 2012). The language used at home has three categories: non-English only, some English and some non-English, and English only.
Covariates
Covariates included age, sex, education, marital status, income, insurance, house food security, perceived health status, perceived weight status, sleep duration, smoking status, asthma, and arthritis. To protect participants’ privacy, NHANES grouped people aged 80 years or above as 80 years old. Sex was categorized as male or female. Education was categorized as less than high school, high school, some college, or college graduate or above. Marital status was categorized as single never married, widow/divorced/separated, and married/living with a partner. Income was categorized less than US$20,000, US$20,000–US$34,999, US$35,000–US$65,000, and more than US$65,000. Insurance was categorized as yes or no. Household food security was measured by the 18-item food security module developed by the U.S. Department of Agriculture (Coleman-Jensen et al., 2017). Household food security was categorized into three levels: full, marginal, and low or very low. NHANES originally had more food security categories. However, low and very low were combined due to the small sample size in the very low food security category. Perceived health status included excellent, very good, good, and fair or poor. Perceived weight status was categorized as normal or underweight and overweight. Sleep duration was measured as the self-reported hours of sleep duration per night. Smoking status was categorized as never smoker, current smoker, or former smoker. Asthma and arthritis were categorized as yes or no. These covariates were selected as they have an established theoretical association with MetS or PA levels and have been regularly used in similar studies (Myers et al., 2019; Park et al., 2014; Serrano-Sanchez et al., 2019). BMI was included in descriptive analysis and was calculated by objective measurement of height and weight during the health examination.
Statistical Analysis
SAS 9.4 Software (SAS Institute, Cary, North Carolina) was used to perform data analyses. To accurately represent the general AsAm population, sample weights were employed to account the complex survey design and procedures. Given that 6 years of NHANES data were used, 6-year weights were created by multiplying the 2-year weights by one third. Chi-square tests and Survey procedures were used to examine frequency or means by PA and MetS status. Logistic regression analyses were used to examine the associations between PA and MetS, using continuous and categorical forms of MVPA in separate models. Each MetS component and overall MetS presence were evaluated separately, in the following models: Model 1 adjusted for age and sex (minimally adjusted model), Model 2 additionally adjusted for perceived weight status and perceived health status (statistical model), and Model 3 additionally added education, marital status, income, insurance, house food security, smoking status, asthma, and arthritis (theoretical model). For Model 2, a variable selection procedure was used. Starting from the full model, each variable was removed, starting with the variable with the highest p value. Age and sex were a priori covariates for Model 2 as well. If there was no clinically significant change in the MVPA beta coefficient after removal of a covariate and that covariate had a p value more than .05, that variable remained out of the model. Exploratory analyses were utilized to assess how acculturation affected the relationship between PA and MetS. Interactions between PA and acculturation were tested and were nonsignificant. Due to limited research on acculturation influences on PA and MetS in AsAms, stratified analyses based on acculturation proxies were conducted despite interactions not reaching statistical significance.
Results
Table 1 shows the sample characteristic of 2,259 adults. All 2,259 participants were used for descriptive analyses related to PA. MetS was determined using 1,034 of those included; however, it should be noted that for some of the individual MetS components, the full sample size was available for analysis. Overall, the population was slightly more female (53.5%), had at least some college education (72.6%), was married or living with a partner (70%), had income more than US$35,000 (74.2%), had health insurance (84.8%), was middle aged (44.2 ± .7), and was overweight (24.8 ± .1 kg/m2) using the Asian-specific BMI definition (≥23.0 kg/m2). Approximately, 85.8% was non-U.S.-born, with 47.1% being non-English speaking at home.
Weighted Demographics Regarding PA and Metabolic Syndrome: NHANES 2011–2016 (N = 2,259).
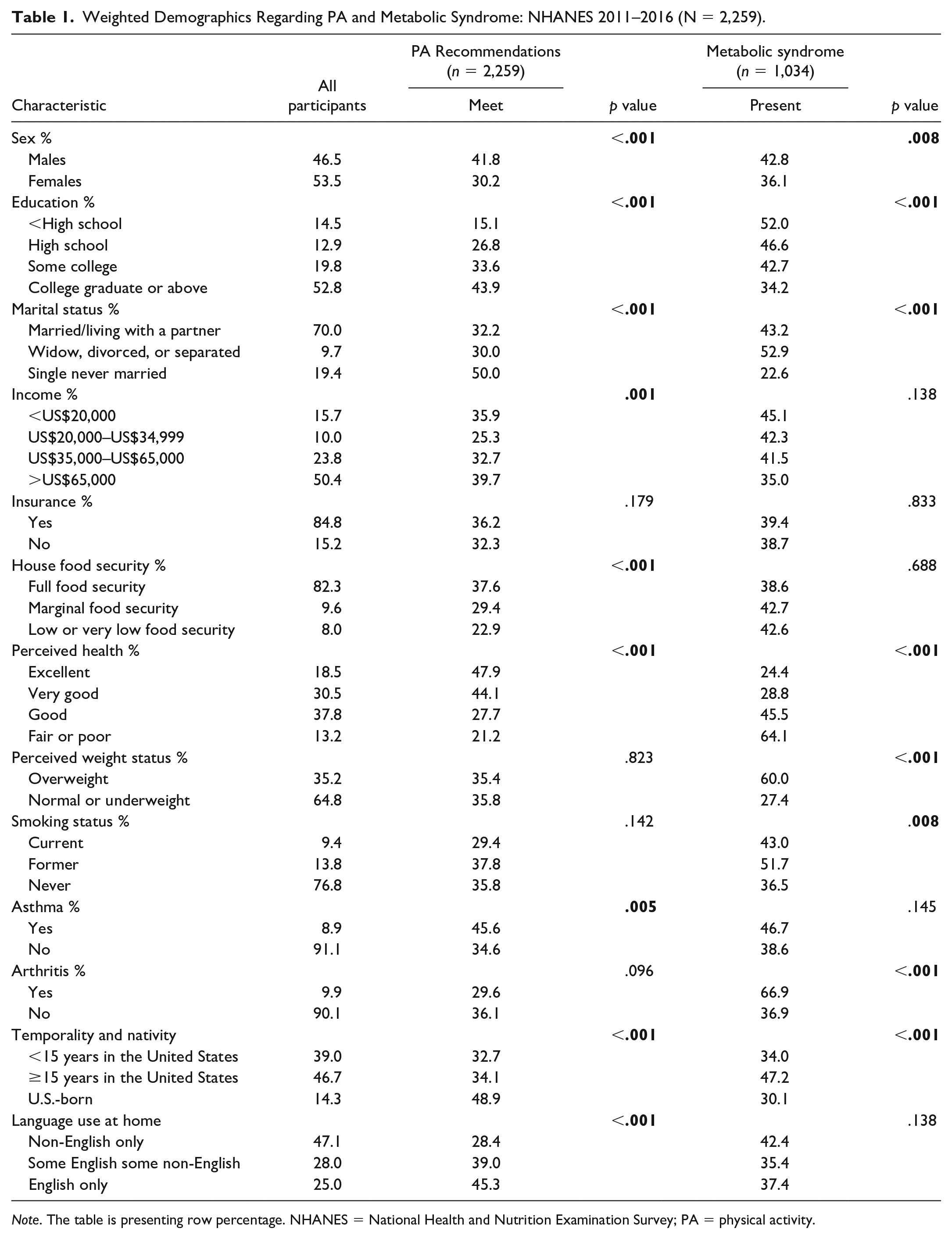
Note. The table is presenting row percentage. NHANES = National Health and Nutrition Examination Survey; PA = physical activity.
Research Question 1(a): What Is the Prevalence of MetS Among AsAms?
Among included AsAms (n = 1,034), 39.2% met the criteria for having MetS. As shown in Table 1, men (p = .008), those with a lower education level (p < .001); were widowed, divorced, or separated (p < .001); reported lower perceived health status (fair or poor, p < .001); perceived themselves as overweight (p < .001); were former smokers (p = .008); had arthritis (p > .001); and were non-U.S.-born living in the U.S. for more than 15 years (p < .001) were more likely to have MetS.
Research Question 1(b): What Is the Prevalence of Meeting National Recommendations for MVPA Among AsAms?
Approximately, two thirds (64.4%) of AsAms did not meet the recommendation of engaging in 150 weekly minutes of MVPA. AsAms spent an average of 146.5 (SE = 6.2) weekly minutes engaging in MVPA. The weekly minutes of MVPA were zero at the 25th percentile, 60 at the 50th percentile, 225 at the 75th percentile, and 1,800 min at the maximum. Men (p < .001), those with a higher education (p < .001), those who were single never married (p < .001), had a higher annual income (p = .001), had a full household food security (p < .001), reported excellent health (p < .001), had asthma (p = .005), were U.S.-born (p < .001), and only speak English (p < .001, Table 1) were more likely to meet the MVPA recommendation.
Table 2 shows the means of continuous variables according to PA and MetS status. Those who met PA recommendation had a younger mean age (p < .001), a lower mean diastolic and systolic BP (p = .035 and .009; respectively), and a lower mean triglyceride (p = .019).
Characteristics of Continuous Measures According to PA and Metabolic Syndrome (N = 2,259).
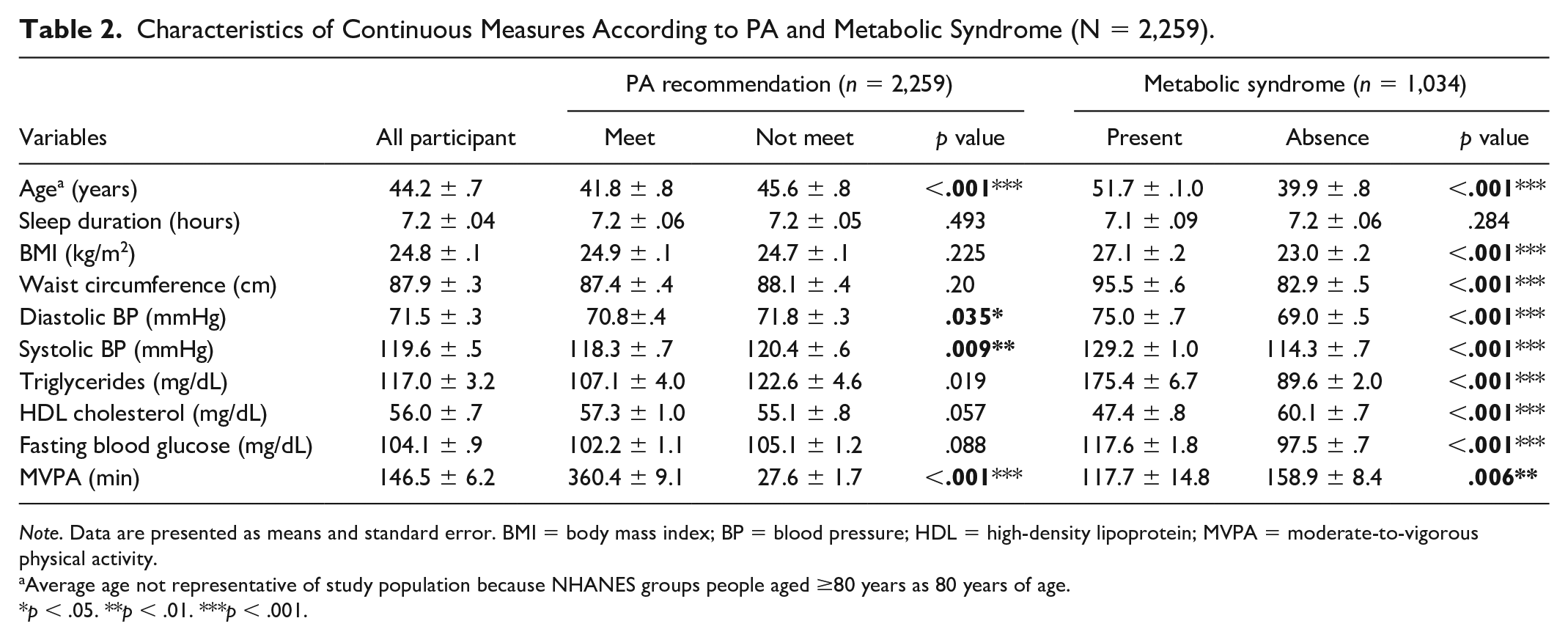
Note. Data are presented as means and standard error. BMI = body mass index; BP = blood pressure; HDL = high-density lipoprotein; MVPA = moderate-to-vigorous physical activity.
Average age not representative of study population because NHANES groups people aged ≥80 years as 80 years of age.
p < .05. **p < .01. ***p < .001.
Research Question 2: What Is the Relationship Between MetS and PA in AsAms?
All three regression models showed that AsAms who do not meet the weekly MVPA recommendation (≥ 150 min/week) had higher odds of having MetS (Model 3: odds ratio [OR] = 1.52, 95% confidence interval [CI] = [1.03, 2.22]; Table 3) compared with those meeting the MVPA recommendation. Continuously, each 30-min increase in weekly MVPA decreased the odds of MetS by about 3% in all three models (Model 3: OR = .97, 95% CI = [.95, .99]). Compared with physically active AsAms, those who were insufficiently active trended toward having a larger WC (Model 3: OR = 1.22, 95% CI = [.93, 1.01]) and reduced HDL (Model 3: OR = 1.93, 95% [1.32, 2.82]). For the same outcomes (i.e., WC and HDL), there were significant decreases in odds for a 30-min increase in MVPA of about 2.4% and 6.4%, respectively (Table 3). No other relationships with individual MetS components were observed.
Weighted ORs and 95% CIs of Metabolic Syndrome According to MVPA (N = 1,034).
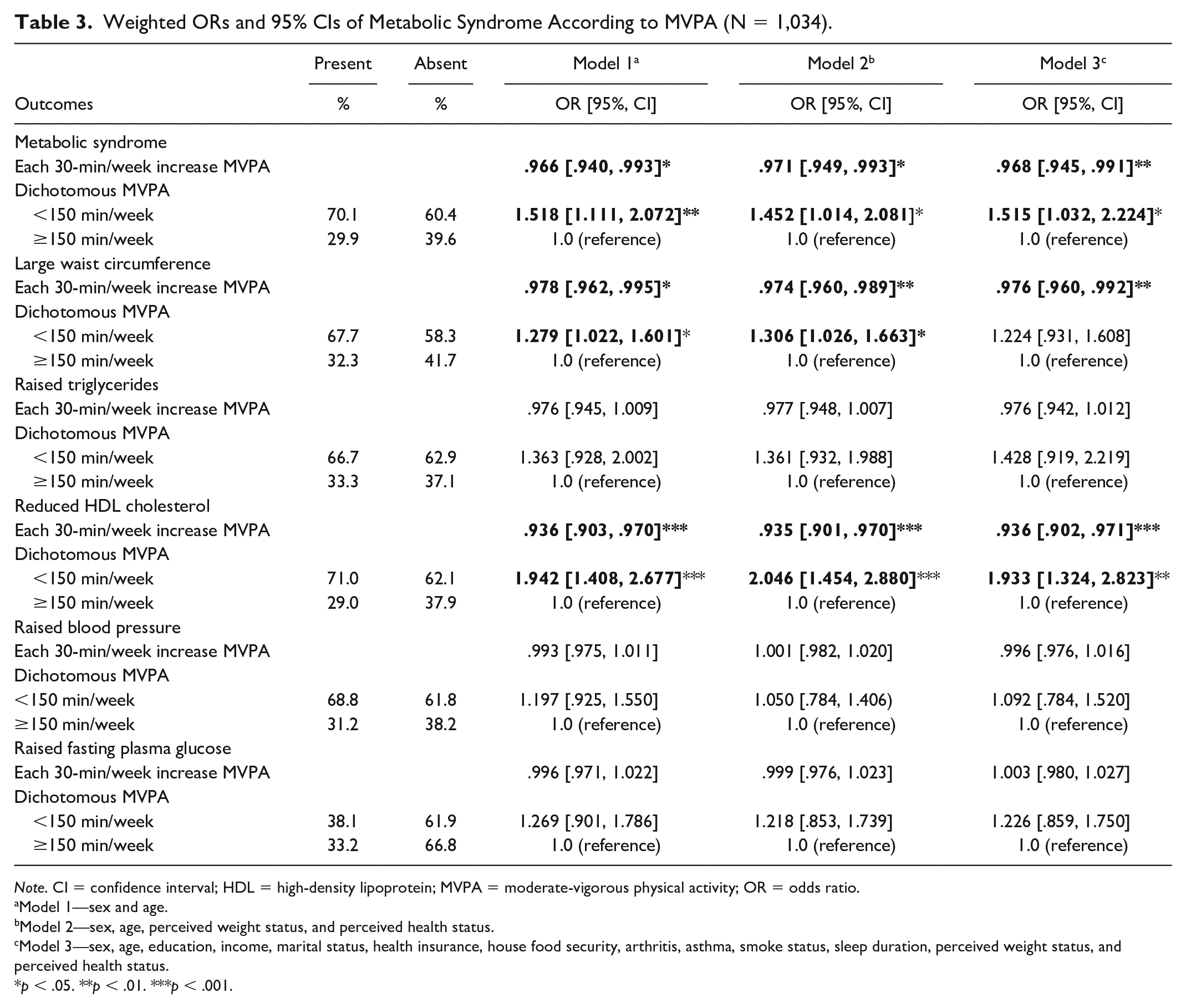
Note. CI = confidence interval; HDL = high-density lipoprotein; MVPA = moderate-vigorous physical activity; OR = odds ratio.
Model 1—sex and age.
Model 2—sex, age, perceived weight status, and perceived health status.
Model 3—sex, age, education, income, marital status, health insurance, house food security, arthritis, asthma, smoke status, sleep duration, perceived weight status, and perceived health status.
p < .05. **p < .01. ***p < .001.
Research Question 3: Does Acculturation Affect the Relationship Between MetS and PA in AsAms?
The proportion of AsAm who met the PA guidelines differed significantly by acculturation proxies (Table 1). U.S.-born AsAms had a higher percentage of meeting the PA guidelines (48.9%) than those who lived in the U.S. equal to or more than 15 years (34.1%), and AsAms who lived in the United States less than 15 years (32.7%). AsAms who only spoke English at home had the highest percentage of meeting PA guidelines (45.3%), followed by AsAms who spoke both non-English and English (39%) and the AsAms who spoke only non-English (28.4%). Regarding MetS status by acculturation, AsAms who lived in the United States for at least 15 years had the highest percentage of MetS (47.2%), followed by those who lived in the United States less than 15 years (34%) and the U.S.-born AsAms. The proportion of AsAms who had MetS did not differ by language use at home. Exploratory analyses of MetS and continuous MVPA based on acculturation are shown in Table 4. When stratifying by nativity and length of residence, we observed the association between MetS and MVPA to be stronger in those who immigrated to the U.S. more than 15 years ago. When stratifying by language spoken at home, for each 30-min increase in MVPA, the ORs for English only were between .94 and .96, and were significant in Models 1 and 3, whereas significance was not observed for non-English only or some English and some non-English.
Weighted ORs and 95% CIs of MetS Based on MVPA After Stratifying by Acculturation Proxies (N = 1,034).
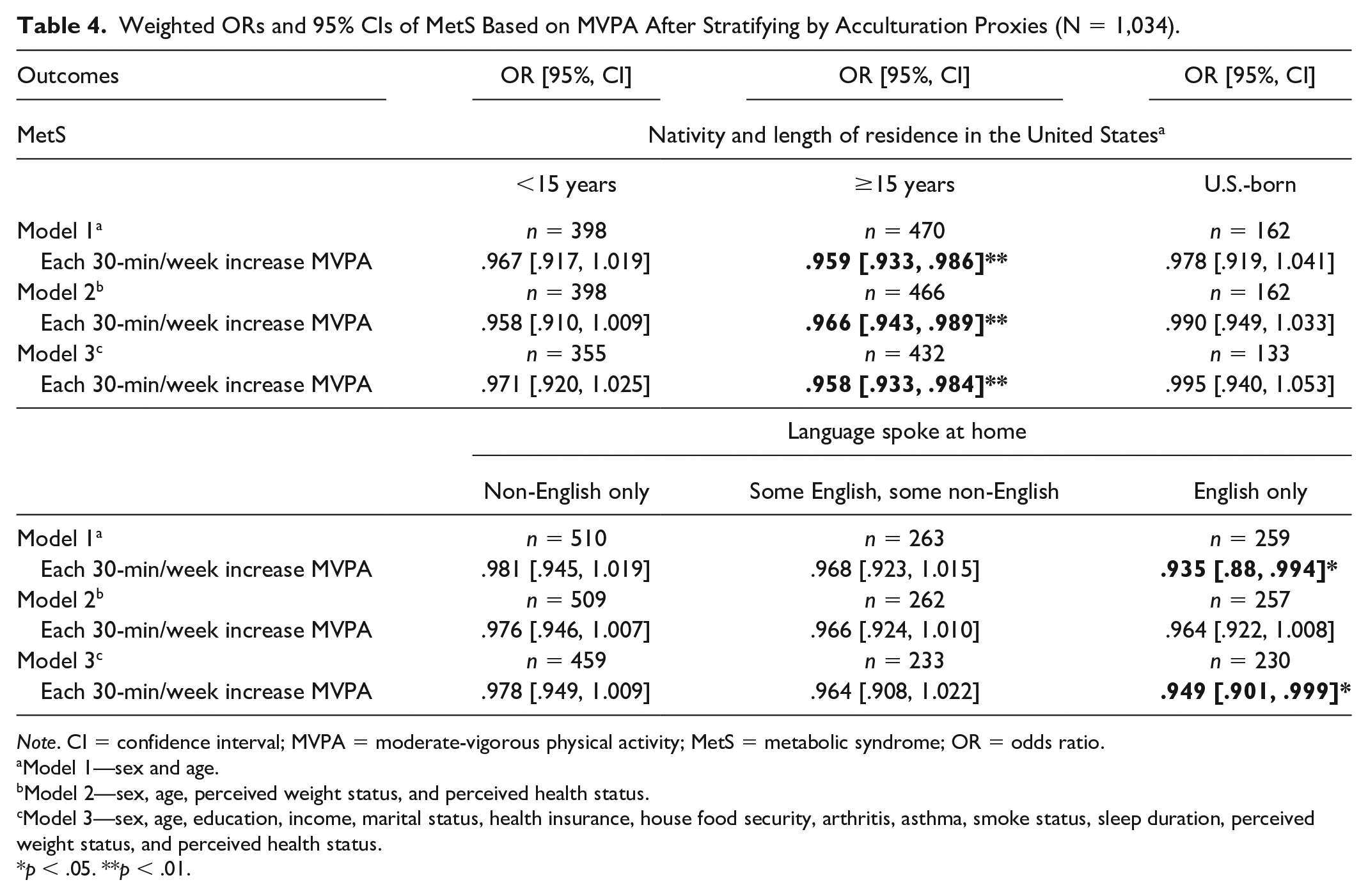
Note. CI = confidence interval; MVPA = moderate-vigorous physical activity; MetS = metabolic syndrome; OR = odds ratio.
Model 1—sex and age.
Model 2—sex, age, perceived weight status, and perceived health status.
Model 3—sex, age, education, income, marital status, health insurance, house food security, arthritis, asthma, smoke status, sleep duration, perceived weight status, and perceived health status.
p < .05. **p < .01.
Discussion
The primary finding of our study indicated that a physically active lifestyle is associated with lower MetS risk. This inverse relationship has been found in previous studies involving samples of other racial groups (Gallardo-Alfaro et al., 2021; Perez-Martinez et al., 2017; Zajac-Gawlak et al., 2021). Prior research suggests that the odds of having MetS in children decreased by 12% with every 10-min increase in MVPA (Cho et al., 2009; Ilanne-Parikka et al., 2010; Renninger et al., 2020). A 7-year longitudinal study of physical active older women showed that risk of MetS decreased from 41% to 12% with an increase in daily step from 10,944 to 11,652 (Zajac-Gawlak et al., 2021). Increasing MVPA among AsAms is likely to confer similar risk reductions in MetS.
Our study found that MetS was prevalent in 39% of AsAm adults, as defined by the IDF criteria, which is slightly higher than in general U.S. adults (33% from 2007 to 2012, and 35% from 2011 to 2016) based on previous research using NHANES data (Aguilar et al., 2015; Hirode & Wong, 2020). Both of those previous studies used the National Cholesterol Education Program’s Adult Treatment Panel III (ATP III) criteria to measure MetS, which could underestimate MetS prevalence among AsAms. The difference between ATP III and IDF criteria is on the central obesity component. The IDF definition provides an ethnicity-specified WC for Asians (IDF, 2006), whereas ATP III used a single threshold across all ethnicities (Zhu et al., 2020). Furthermore, current findings showed the average BMI was 24.8 kg/m2 in AsAm adults, which is much lower than U.S. adults (28.7 kg/m2; Flegal et al., 2012). A previous study reported that MetS prevalence was significantly higher in AsAms than Whites in every BMI category (Palaniappan et al., 2011). This study used a medical record to estimate MetS in which WC was not available; Therefore, MetS was defined as those who met two MetS criteria. Because the purpose of Palaniappan’s study was to compare AsAm subgroups with Whites who were similarly defined, their findings provide a better picture of MetS prevalence in different racial groups. A 20-year prospective longitudinal study found that, at the same BMI, AsAms had double the risk of developing diabetes than Whites, and their risk of diabetes increased by 85% with each 5 kg weight gain compared with 37% for Whites, 38% for Blacks, and 44% for Hispanics (Shai et al., 2006). Along with the previous research, current findings suggested that overweight or obesity defined by the general BMI definition may not accurately reflect MetS risk among Asians. Despite the lower BMI, Asians have a markedly higher risk of these adverse health outcomes, including MetS and mortality at any given BMI (Fang et al., 2019; Iyer et al., 2019; Palaniappan et al., 2011; Thornton et al., 2020).
Acculturation is a multidimensional process that reflects the interaction between cultures, which can positively or negatively influence individuals’ health behaviors (Bornstein, 2017). The traditional perspective is that Asian immigrants who have lived in the U.S. for a longer period of time have more exposure to the Western environment and tend to adopt more unhealthy behaviors (Ro, 2014). However, acculturation seems to have more favorable effects on the PA and MetS relationship. Our results found MVPA and MetS were significantly associated among those who immigrated more than 15 years ago and those who only speak English. Results for the other categories of nativity and language spoken were of similar magnitude but were not significant. This likely explains the non-statistically significant MVPA and acculturation interaction p values. One speculation for our significant findings is that MetS prevalence was proportionally higher among AsAms living in the U.S. for more than 15 years, but this group was less likely to meet PA recommendations. Therefore, this group could benefit most from increasing MVPA. Interestingly, the protective effect of MVPA in MetS was seen in the spoken English-only AsAms. English-only AsAms were more likely to meet PA recommendation and were less likely to have MetS. A recent study on acculturation and MVPA showed similar findings that English-only AsAms performed more MVPA than those who spoke non-English and both English and non-English (Zhu et al., 2021). One possible reason is better English proficiency reflects greater exposure to information and social norms. Better English proficiency may demonstrate a better health literacy that allows them to obtain and understand basic health information.
For future research and practice, considering 85% of AsAms were non-U.S.-born and about half of them spoke a language other than English at home, it is crucial to reach this population, using their native language to disseminate health information and address health care needs. Furthermore, AsAms constitute very diverse ethnic groups and face substantial health challenges, including limited English proficiency, differing cultural beliefs and behaviors, and unfamiliarity with the American health system. Non-U.S.-born AsAms had experienced a higher percentage of having MetS and a lower percentage of meeting the PA guidelines than those born in the U.S. Therefore, depending on the ethnic characteristics of AsAms, culturally adapted intervention can be designed for the first-generation AsAms to educate them about PA benefits for health and chronic illness prevention. Finally, given that data on AsAms are limited, aggregated, or nonexistent (Kanaya et al., 2022), additional research is needed to understand why MVPA has a more potent protective effect in higher acculturated AsAms.
Strengths and Limitations
Using a larger nationally representative sample of AsAm adults, our study examined the relationship between PA and MetS. The NHANES has a rigorous data collection protocol with a wide range of information that allowed for many factors to be assessed as possible confounders. Another important strength of our study is that MetS prevalence was measured by race-specific MetS criteria for Asians, which provides a more appropriate risk estimation in this population. Several limitations of the study should be noted. The cross-sectional study design limits inference about the direction of causality between PA and risk of MetS. We assessed acculturation by proxies, which are commonly used in research (Alegria et al., 2022; Le et al., 2019). However, proxy alone omits individual differences that cannot account for every domain of acculturation. In addition, this study aggregated AsAm subgroups that may mask the difference in AsAm subgroups. Due to heterogeneous cultural background in AsAms, further research may investigate a single subgroup to eliminate misleading results. In future, valid questionnaires are needed to measure acculturation in research examining the impact of culture on AsAms’ health behaviors and health outcomes.
Conclusion
Increasing MVPA is associated with lower MetS risk among AsAms. More acculturated AsAms may receive more potent benefits by increasing time spent in MVPA. Acculturation seems to play an important role in PA and MetS, but whether or how it affects PA, MetS, and the relationship between them remains uncertain due to the lack of consistency of acculturation measurement in the literature and paucity of research among AsAms. Further research may be needed to determine a better measurement of acculturation and to consider disaggregating AsAm subgroups in acculturation studies. Meanwhile, it will be necessary for health care professionals to increase awareness and knowledge of health outcomes that may differ among AsAms across acculturation levels. Given that only a quarter of AsAms spoke English at home, it is of utmost importance to expand ongoing culturally and linguistically appropriate programs focused on PA promotion and health education.
Footnotes
Authors’ Note
The study was a secondary data analyses. The National Health and Nutrition Examination Survey was approved by the National Center for Health Statistics Research Ethics Review Board and documented consent was obtained from participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Demetrius Abshire was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under award number K23MD013899. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. J. Sheng, M. D. Wirth, and S. P. Heiney declare that no funds, grants, or other support were received during the preparation of this article.