
Abstract
Introduction:
We aimed to describe the health and well-being of family caregivers of Native Hawaiian and Pacific Islander (NHPI) adults living with Alzheimer’s disease and related dementias (ADRD), explore cultural values related to caregiving, and characterize barriers and facilitators to their health and well-being.
Methodology:
Caregivers of NHPIs living with ADRD were recruited from across the United States to complete a multimethod study including a survey followed by an interview about their health and well-being.
Results:
Eleven participants completed surveys, six of whom completed an interview. Themes included caring as a community, lōkahi (balance), and the importance of sleep, food, and physical activity. Cultural values included connection to cultural practices, kūpuna (elders) as cultural knowledge holders, and the kuleana (responsibility) of caregiving.
Discussion:
Caregiving for an NHPI adult living with ADRD occurs beyond the dyad, and is a matter of family and community. Culturally-based interventions offered through community and healthcare organizations may be critical to promoting caregiver health.
Introduction
Family caregivers provide most of the necessary care for people living with Alzheimer’s disease and related dementias (ADRD)(Alzheimer’s Association, 2021). Despite this common occurrence, providing care for a family member increases the caregiver’s own risk for stress, depression, poorer-self rated health, chronic disease, and ultimately, mortality (Etters et al., 2008; Schoenmakers et al., 2010; Schulz & Beach, 1999). With an increasingly older population, it is imperative to public health to promote the health and well-being of family caregivers of adults living with ADRD (Alzheimer’s Association, 2021).
The number of people diagnosed with ADRD is projected to increase by 128% to nearly 14 million people by 2060 (Alzheimer’s Association, 2021; Rajan et al., 2021), suggesting that both the number and, by extension, the diversity of people providing care for family members with ADRD will increase. Caregiving is shaped by cultural values, expectations, and beliefs, and thus it is important to expand on this diversity in caregiving research by embracing the importance of history, context, cultural beliefs and values, and social roles within the needs and health of caregivers (Dilworth-Anderson et al., 2020).
The Indigenous Connectedness Framework offers a theoretical orientation to cultural values in the relationships between caregiving with health and well-being (Ullrich, 2019). The Indigenous Connectedness Framework was developed to identify core concepts and mechanisms to promote child well-being and frames health and well-being as interconnectedness of the community, environment, family, and intergenerational connectedness (Ullrich, 2019). Intergenerational connectedness involves awareness of language, genealogy, history, and a grounded identity; family connectedness honors the relationships beyond the nuclear family and importance of strong relationships beyond the parent-child dyad; community connectedness includes cultural values, practices, and norms, being part of an interconnected whole, and the importance of gathering; lastly environmental connectedness illustrates how the land is inseparable from being. According to this framework, connectedness and the relationships between individuals and everything are an important key to Indigenous survival and well-being (Ullrich, 2019), thus offering an important theoretical orientation to understanding relationships between caregiving with health and well-being in Indigenous communities.
Despite their elevated risk of ADRD, Native Hawaiian and Pacific Islander (NHPI) adults have received scant research attention. Compared with people of other racial and ethnic identities, NHPI adults experience disparities in chronic disease risk factors for ADRD, such as hypertension and type 2 diabetes (McElfish, Purvis, Esquivel et al., 2019; Waitzfelder et al., 2023); they have higher prevalence of subjective cognitive decline (Ganbat & Wu, 2021) and are at higher risk for early onset dementia (Sentell et al., 2015). Further, NHPI adults living with ADRD have higher rates of hospital readmission than their counterparts in the general population (Hermosura et al., 2020). These findings suggest the potential for a higher prevalence of and worse health outcomes from ADRD in NHPI communities. An improved understanding of how NHPI families care for their loved ones with ADRD has the potential to mitigate such risks.
Research on general NHPI family caregiving (i.e., not specific to ADRD) indicates that NHPI caregivers provide care for a longer period of time, compared to White and Asian American caregivers (Lum et al., 2010) and report distinct challenges including the combination of financial limitations, potential conflict with majority-cultural values, and social stressors when providing care (Browne et al., 2014). Family caregivers in Hawaiʻi have reported difficulties in financially suporting kūpuna (grandparent, older adult) 1 , particularly managing the high costs of food, competing demands of family and work, and access to healthcare and culturally-relevant services (Browne et al., 2014). Cultural incongruity represents another challenge. While there is heterogeneity across NHPI cultural groups, many NHPI cultures share a strong kuleana (responsibility) to care for kūpuna (Braun et al., 2015). The cultural values held among NHPI communities are evidenced by the following quote: “As Hawaiians, we brought up to care for one another. Living in [the] states, you old, we put you in a home. Not in Hawai’i” (Browne et al., 2014). These caregiving values extend to NHPI communities living on the continent, with Hawaiian elders reporting that they maintain the kuleana to provide care when living on the continent, even though family care is less valued in mainstream culture (Browne & Braun, 2017). Additionally, kūpuna on the continent shared that as they continue to care for family members on the continent they would appreciate programs and services that center Hawaiian culture (Browne & Braun, 2017). Kūpuna are highly regarded as teachers and keepers of knowledge (Browne et al., 2014). Thus, the kuleana of caregiving is important to the community and preservation of Hawaiian culture. Finally, social stressors include the costs of caregiving, competing demands between work and family, and reports of discrimination and disrespectful services (Browne et al., 2014).
To better understand how to mitigate these changes to promote family caregiver health and well-being, we aimed: 1) to describe the health and well-being of family caregivers of NHPI adults living with ADRD (family caregivers); 2) to explore cultural values related to caregiving; 3) to characterize barriers and facilitators to health and well-being experienced by family caregivers. This study addresses the public health importance in mitigating risk factors associated with caregiving, contributes to improving our understanding of health disparities faced by NHPI communities, and elucidates cultural values important to NHPI communities.
Methodology
Positionality
Herein, we provide a brief summary of the authors’ respective positionalities, as the way we view the world depends on our position within society which influences the way research is conducted and interpreted (Jacobson & Mustafa, 2019). Specifically, we provide information about the identity of the authors in relation to the current areas of research. None of the authors identify as NHPI, yet six of authors have experience growing up in, working, and living with NHPI communities (AMJ, SKO, ZC, AO, KI, KS). Four authors have expertise and training in caregiving, aging, and gerontology (AMJ, RHW, SK, MH, NS), and five authors have experience in research on cultural aspects of NHPI health and well-being (CJM, SKO, RHW, SK, MH, KS). Recognizing that no authors identify as NHPI, to ensure authenticity in representation we asked members of the NHPI community and participants to review and approve of the findings prior to publication. We also refrain from assigning value to the practices identified or comparing our findings to other populations.
Participants and Procedures
Adults 18 and older who spoke English and provided unpaid care for a NHPI adult family member with ADRD within the past five years were recruited to complete a multimethod study including an online survey and interview about caregiving responsibilities and experiences. Surveys and interviews assessed financial changes and economic costs related to caregiving; cultural values related to caregiving; access to caregiving services and supports; and self-rated health, well-being, and health behaviors. As our first attempts at recruitment using social media were thwarted by bots and mischievous responders (Jackson et al., 2023), we changed our recruitment strategy and recruited caregivers through a national online registry (Ta Park et al., 2022) and partnerships with community organizations across the United States (US) who serve NHPI adults, caregivers, or individuals living with ADRD from July 2022 through April 2023. Recruitment concluded in April 2023 after reaching out to all identified community organizations at least three times.
Participants were paid $50 to participate in the online survey via Qualtrics, which took about 30 minutes to complete. If participants had provided care for multiple family members who were NHPI and living with ADRD, they were asked to provide information about the person they currently or most recently provided care for. Participants who were no longer providing care were asked to think back to the last month they provided care for a NHPI adult living with ADRD when completing the survey.
After completion of the survey, all participants were invited to participate in an interview either via Zoom or phone. The interview took about 30 minutes and participants were paid an additional $50. All interviews were conducted by the first author, who used a semi-structured interview protocol. Interviews were audio recorded, transcribed verbatim using a transcript service, and then reviewed for accuracy by at least one co-author. After data analysis was complete, all of the participants who completed an interview were invited to serve in the member checking process to review the findings to ensure credibility and to promote rigor (Patton, 2014).
The study was certified as Exempt by the first author’s university institutional review board. Written informed consent was obtained from all participants prior to participation in the study.
Quantitative Measures
The survey included questions such as reported age, sex at birth, primary ethnicity (from a list of 17 ethnicities, with the option for an open-ended response), marital status, number of adults and children staying in the household, geographic location (e.g., rural, suburban, urban), US region (e.g., west coast, Hawaiʻi), education status, and household income (Table 1). Participants reported if they were currently providing care and their relationship to the care recipient. To describe caregiver health and well-being, we included the following prompt “In general, would you say your health is:” with a 5-point response scale ranging from 1 = Poor to 5 = Excellent (Knäuper & Turner, 2003). To assess well-being, participants were asked, “Taking all things together, how satisfied are you with your life as a whole these days?” with a 4-point response scale ranging from 1 = not at all satisfied to 4 = very satisfied (Krueger & Schkade, 2008).
Sociodemographic Characteristics of the Sample.
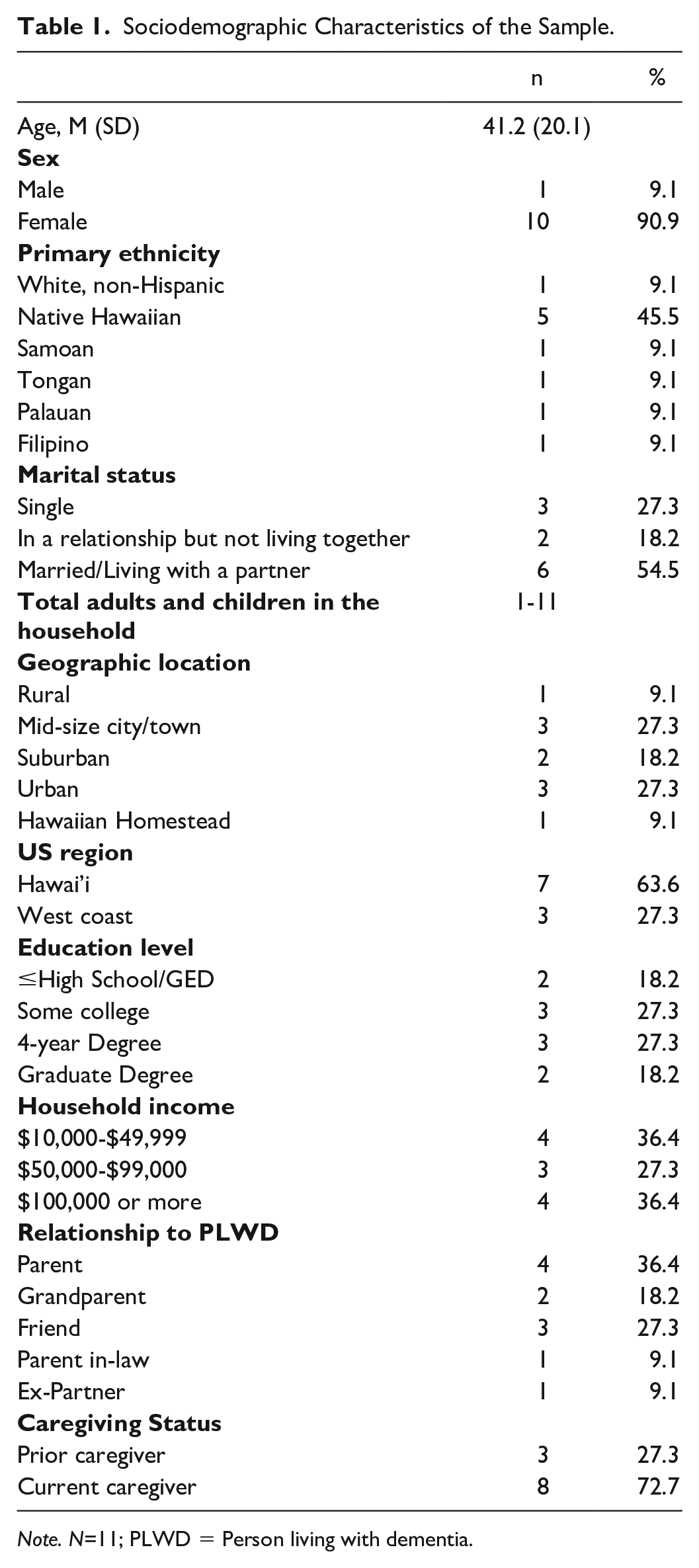
Note. N=11; PLWD = Person living with dementia.
Interview Protocol
The semi-structured interview protocol (Supplemental Material) was developed and pilot tested for semantic and logistical appropriateness. The interview protocol included open-ended questions exploring the facilitators and challenges to self-care, culturally relevant values in caregiving, benefits of caregiving, and services and supports needed by caregivers of NHPI adults living with ADRD. Potential probes were included for clarification and additional insight.
Analysis
Quantitative and qualitative data were collected in parallel. We used SPSS (version 28) for quantitative data management and analyses. We present descriptive statistics including means, standard deviations, and frequencies for categorical variables (Table 2) to describe the health and well-being of family caregivers.
Caregiver Health and Well-being.
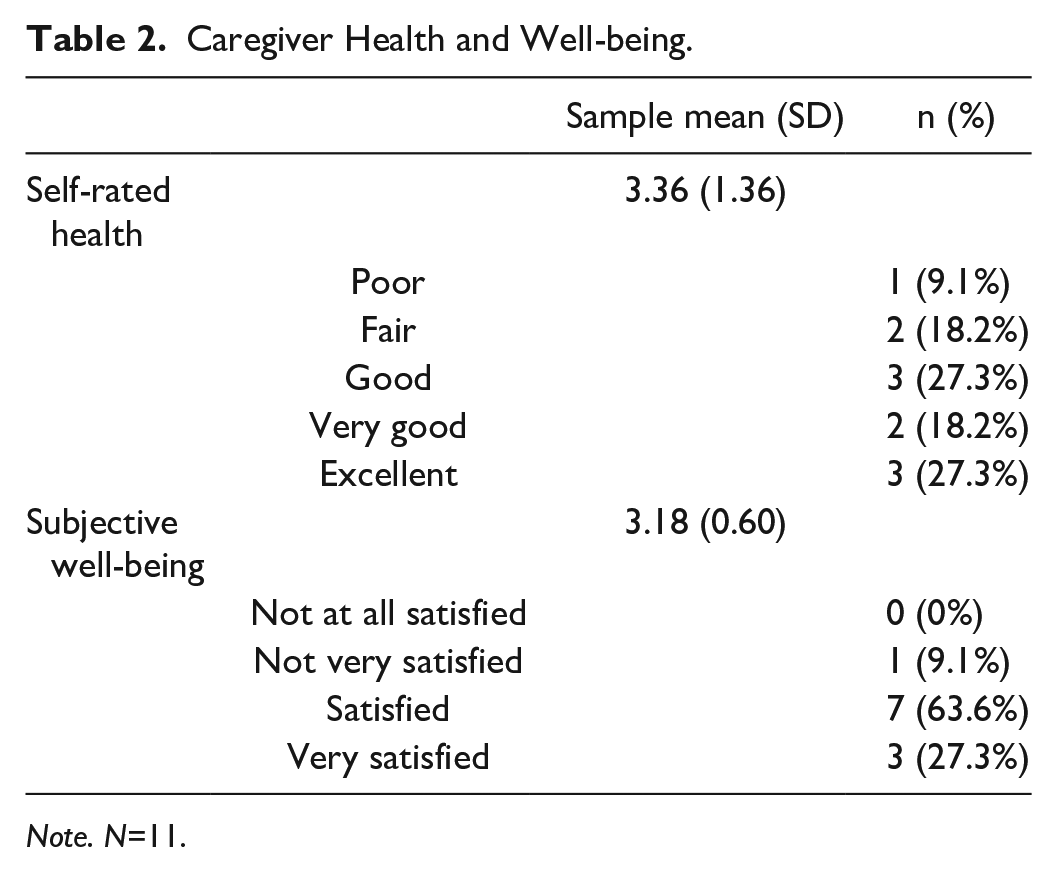
Note. N=11.
Qualitative data were analyzed using reflexive thematic analysis (Braun & Clarke, 2006, 2022). The first author engaged with the data by reviewing the transcripts multiple times and taking notes. The first author then created an initial codebook and coded the transcripts line by line using MAXQDA (2022). During this process, the transcripts and codes were reviewed and revised by four members of the research team who provided additional perspectives on the codes, coding schema, and when the codes were applied. Codes were then reviewed, revised, and grouped into themes and subthemes. The codes and themes were discussed among the research team who helped refine and define the structure and content of themes, subthemes, and codes. Throughout this process, the first author revisited the existing literature andcultural references, and connected with cultural practitioners to continue to interpret the data, both describing and interpreting caregiver experiences. The Indigenous Connectedness Framework (Ullrich, 2019) offered an important theoretical orientation in the analysis and interpretation of the findings regarding health and well-being. While this framework was developed to promote child well-being, with the child as the center of the model, it has been applied to a variety of outcomes across the lifespan and the authors welcome modification and adaptation to improve understanding of Indigenous connectedness and well-being (Ullrich, 2019). In the current study, we include the overarching importance of interconnectedness and an interdependent world while focusing on the application of the four aspects of the model: environmental, community, intergenerational, and family connectedness as they apply to caregiving.
In alignment with our three research questions, we first present quantitative data describing the health and well-being of family caregivers. We then used the themes generated from the qualitative data to expand on the quantitative description of health and well-being of family caregivers. Next, we explored cultural values related to caregiving identified in the qualitative interviews. Lastly, we analyzed the qualitative data to explore barriers and facilitators to health and well-being among family caregivers. We use the term “person living with dementia” (PLWD) in alignment with the literature throughout the results and discussion sections to describe the person being cared for and want to acknowledge that this may not be the term used by caregivers themselves.
To ensure the findings accurately represent their experiences, all interview participants were invited to review a report generated from this data and given a copy of this manuscript for review prior to publication. One participant met with the first author, reviewed the findings, and provided feedback. Based on their feedback, we made revisions to the description of importance of sleep, food, and physical activity as relational in caring for self and the PLWD. The caregiver also provided examples offering additional nuance within the changing responsibilities or kuleana of caregiving, specifically with the progression of dementia.
Results
Sociodemographic data are presented in Table 1. Caregivers (n= 11) were primarily female, ranged from 20 to 76 years old, with an average of 41 years old. Most caregivers identified Native Hawaiian as their primary ethnicity. All caregivers lived in Hawai’i or the West Coast, and most were living with a partner. Eight participants were currently providing care and none of the caregivers was providing care for a spouse. Rather, caregivers provided care for a parent, grandparent, friend, or parent of a partner; one participant was providing care for a former partner. While three caregivers indicated they were the sole caregiver, eight others reported additional caregivers also providing care, ranging from one to more than five additional caregivers. Of the 11 participants who completed the survey, 6 (54.5%) also completed the interview. Interviews ranged from 20-49 minutes, with an average length of 30 minutes.
We first present quantitative data describing the health and well-being of family caregivers followed by qualitative data expanding on this description. Then, we present qualitative data depicting cultural values related to caregiving and describing barriers and facilitators to health and well-being of caregivers.
Health and Well-being of Family Caregivers
Descriptive data of the health and well-being of caregivers is in Table 2. None of the prior caregivers rated their health as very good or excellent, suggesting lower levels of health compared to current caregivers. Only one participant reported being not very satisfied, while the other ten indicated they were satisfied or very satisfied. Caregivers rated their self-rated health from poor to excellent. We identified the following themes describing the health and well-being as a family caregiver in the qualitative data: caring as community and a subtheme of maintaining social connections; lōkahi (harmony, unity, balance); and importance of sleep, food, and physical activity with a subtheme of relational self-care.
Caring as Community
Caregivers shared the importance of community to both their own health and that of the PLWD. All of the participants who completed the interviews reported sharing caregiving responsibilities with at least one other person; and most reported having a large support system that they provide care within. For example, one participant stated,
I come from a large family, both Pacific Islander and roots with Hawaiian ancestry. So having that large family and that large support system, at least in my experience, has been unique for me. Whereas there are others that I know that don’t have that luxury, I guess, of having multiple people there to support this person that’s living with dementia.
Thus, caregivers described coming together as a community to provide care. Another caregiver described creating a group text message thread so everyone knew what was going on with the PLWD, while others described having family members move back “home” to the islands, or moving to the islands themselves to provide care for the PLWD. As caregiving occurred across multiple family and community members, caregivers also described the importance of spending time together while providing care. For example, in talking about the benefits of providing care, one caregiver stated,
I think just that connection, building that bond with them. Definitely in the beginning it’s hard to see an elder that go[es] through something. And then, with other relatives just coming together to be there for that person. So, I think having that special bond with my elder over time has been really special for me. As heartbreaking as it is, I think it was definitely, for me, something that was worth it in the end to be there for them.
Maintaining social connections
We identified that maintaining social connections was a subtheme of caring as community, which is evident in caregivers sharing the importance of social connection and interaction to the health of the caregiver and the PLWD. One participant shared the following:
She [PLWD] benefits from regular exercise and socialization . . . I’ve started going to a senior aerobics class, a water aerobics class and knowing that she’s a social exerciser, she won’t do it if it’s just her. I’ve really, really encouraged her to come with me and then because she’s made friendships within the class, and when she’s not there, they’ll ask for her, that it actually motivates her to be more physically active. Because of the social aspect and then also because we try to do things as a family, with friends, on a regular basis. So, every Friday, we’ll go to the park with friends and play volleyball and my mom used to play volleyball in college, and so she’ll come and be score keeper and critique. You know? She’s motivated to stand up and maybe play a round, play one round or one game, she’ll sit down but then she’ll have the socialization and being around others versus being home and anxious and just watching television. Because, as a family, we’re incorporating her care into our socialization. Then she is by default more social and happier, because she’s a highly social person and her diagnosis has isolated her to some extent where she doesn’t want to go. Because the grandchildren will go and, “We’re all going to go. Mom, you want to go?” Someone will always be willing to be like, “Oh, you ready to go home? We’ll take you home.” We share the load of making sure that she has access to friends and those who want to see her and places she wants to go and activities she’d like to do. That way we all are able to spend time together and spend time with friends, and make sure she gets her activities in.
Within this example, the caregiver recognizes the importance of social connections to encourage physical activity, engage with the family, promote mental health, and include the PLWD in activities. In this description, the caregiver also indicates they communicate to the PLWD that their presence is wanted and valued by the community and the family. It is evident that family members are ready to step in and to help ensure she is comfortably engaged and her needs are met (e.g., needing to leave early).
Another caregiver shared a similar, yet different, example of the importance of social connection, stating,
The great part about our community is most of us have the same childhood friends from elementary, and I still have the same friends. So, for me, if I need to decompress or I need to get away, a lot of times, I’m either at the beach . . . or twice a month, I meet out with my girlfriends just to get out. But we also do that [decompress] with my mother-in-law, right? Because she has a group of friends herself that I think it’s positive for her to kind of see them and do the same things. I mean, if we weren’t there and she was healthy, she’d be with them all the time because they’re all retired. So as much as possible, we all tried to balance ourselves to just decompress on our own without the stresses that comes with our family, yeah.
This caregiver identifies the importance of social connection and interaction for the caregiver and PLWD, but also describes effective communication strategies between caregivers and the importance of finding a calm space or place to decompress for their own health.
Lōkahi (Unity, Harmony, Balance)
As caring occurs within the community, the relevance of maintaining balance in relationships to health and well-being emerged. While participants did not explicitly use the term lōkahi to describe the importance of balancing relationships, we label this theme “lōkahi” as what was shared aligns with our understanding of this Hawaiian value. We reviewed this term with a Native Hawaiian participant to ensure this term appropriately reflected their experiences, who agreed this is an accurate descriptor.
Lōkahi is a core Hawaiian value that is believed to stem from living on an isolated island chain (Paglinawan et al., 2019). With this isolation, Hawaiians learned the importance of taking care of the land and relationships with each other, as all they had were relationships between the people and spaces around them (Paglinawan et al., 2019). Lōkahi, or living in harmony, fosters relationships that are pono (balance), whereas if someone is not doing their part for others, they are said to be out of balance or pono ʻole (Paglinawan et al., 2019). Lōkahi can be seen in the following participant quote, which captures the importance of maintaining family relationships, and the importance of that relationship above all else.
It’s not so much caring, the actual caregiving, it’s coordinating the care between different ones in the family and everybody knows that sometimes your immediate family has drama that you cannot help, because everyone is busy. Maintaining that family relationship, which is very important, ʻohana (family) is very important to Hawaiians, that that is actually the biggest contributor I think to effective care for someone with dementia. Not per se, money or education or any of those things. It’s actually that relationship within the family that helps to provide stable care. That’s important to Hawaiians. I think that’s important to everybody.
Another caregiver described the importance of a cultural practice called hoʻoponopono (to make something right). Also sharing the additional challenge or responsibility in providing care on top of existing family dynamics, with health and maintenance of relationships being at the forefront.
I think the biggest thing is hoʻoponopono, it’s to make something right. When there is a family member with dementia, and it involves multiple people caring for them, the communication between them has to be very good and problems need to be resolved quickly, so that you don’t get rifts in the family, because different ones think differently on how care should go. I think having a primary caregiver and someone that the rest of the family respects in that role and that person being able to delegate to others in the family, that really helps in effective care for the person with dementia. I think with Hawaiian families, there is a lot of residual issues probably from growing up and just life, that different ones are not able to do things as needed just because their lives are busy.
In this quote, the participant illustrating the importance of decision making as a family and the importance of communication with changes both among family members and in the progression of the disease. Across each of these factors within the family, the caregiver points out the relevance of historical challenges that many families face that can come to the forefront when trying to maintain balance and provide effective care for the PLWD.
Importance of Sleep, Food, and Physical Activity
Caregivers described the importance of sleep, food, and physical activity to promote both their health and their ability to provide care. Caregivers reported participating in these health behaviors to improve their own health, better care for the PLWD, and to support lōkahi between the caregiver and PLWD. For example, one caregiver shared,
If I don’t sleep then I have kind of a more negative attitude towards the chores of caring for someone else. Then I feel like the quality of care that I’m giving isn’t as good. So that’s just my sleep. If I’m not eating good, I don’t have as much energy to go through with all the things, so it definitely affects it a 100%.
Similarly, another caregiver mentioned the importance of taking care of themselves physically, emotionally, and mentally to be the best care provider they are able to be.
And so that definitely just took a toll on me, not just physically, but emotionally and mentally as well. And so, I found myself just lashing out when I’m providing care, getting easily frustrated, not being able to control my emotions when providing care to my elder. And I knew that a lot of that was just because of the sleep that I wasn’t getting, which doesn’t help with the stress of providing care to someone living with dementia.
Both of these caregivers describe the realization of the importance of health promoting behaviors or self-care to provide optimal care for the PLWD. Thus, illustrating the need to care for themselves to have the energy, patience, and self-control to engage effectively as caregivers.
Relational self-care
Lastly, one caregiver shared that they have a difficult time with “self-care” as it often is conceptualized. Instead, they described what self-care looks like to them: preparing food and spending time with family in meaningful ways.
But also trying to remind myself that self-care is not like “I’m going to buy this bath bomb and sprinkle it in my shower.” I felt like my self-care, what made me feel good, was doing things like cooking next to my mom and remembering, “Oh yeah, you used to make that for me when I was a kid.” It was more activities with others to help me remember what my life used to be, and just those childhood memories. So, smelling things and like, “oh my mom and I are chopping things, the aromas,” and I think that to me was more relaxing than things that are sold to us as self-care. I’m someone who really recognizes that the “self-care industry,” they love for us to spend money on all these things, but really what I needed was to spend time with my family in meaningful ways. So yeah, I’m terrible at self-care. I eat with my family and I cook with my family and that’s what makes me feel good, typically. It’s like medicine, that’s our medicine, our food is our medicine, so that’s how I want to take care of myself.
In this quote, the caregiver describes the importance of self-care as a relational, meaning-focused activity, including engaging in an activity with the PLWD, which also promotes their own health. Thus, circling back to the importance of relationships and lōkahi to caregiver health.
Cultural Values Related to Caregiving
We identified three cultural values related to caregiving: connection to cultural practices, kūpuna as cultural knowledge holders, and the kuleana of caregiving with the subtheme of responsive kuleana when caregiving.
Connection to Cultural Practices
Caregivers described the benefits of connecting with the PLWD, including benefits in participating in cultural practices together and continuing to learn from the PLWD. One caregiver living in the continental US shared,
I actually was contracted at the time to do these virtual workshops for Palauan culture, so I actually had my mom help me with some of it. So, I had her on camera to help teach some of the Palauan lessons, so I was really trying to find ways to do it during the pandemic. But yeah, she was able to sing songs with us, and we even videotaped her making coconut oil from scratch, and it was amazing what we were able to do during the pandemic, but it was really hard because we couldn’t take her to go visit other aunts and uncles, and sharing Palauan food, and all that, but I did my best to make sure to always [take her to] Asian grocery stores out here. Thankfully, [they] have taro, tapioca, the things that she wants to eat. Parrotfish, they have parrotfish here, which made my mom so happy.
This caregiver was able to connect through Palauan lessons and food, which engaged her mom in cultural practices; they found ways to participate in these practices on the continent—away from their islands.
Kūpuna as Cultural Knowledge Holders
The PLWD (often referred to as kupuna) was frequently described as holding immense knowledge and wealth by their caregivers. Caregivers described the PLWD as the history of the family, sources to perpetuate culture, holders of knowledge, and sources of wisdom. One caregiver shared,
For Native Hawaiians, that’s your history. Growing up, kūpuna are super important. I mean, they’re so valuable in life skills and information and your history. And so for me, it was a no-brainer for us. Like you said, as it expected, it’s kind of expected because of the wealth that they bring to you as you’re growing up.
Similarly, another caregiver described the wealth of cultural knowledge and importance of kūpuna in sharing that knowledge with the next generations.
But without our kūpuna, we lose . . . I don’t even know, we would lose a lot. For me, the wealth of information, the wealth of things that they know most of it is through word of mouth, so them talking and discussing. I have a passion for kūpuna, really do have a passion to learning and knowing these things because we’re all going to die. And how do we perpetuate our culture and carry it on without sharing it with our children and experiencing it with our children.
Lastly, a caregiver shared “her [PLWD] wealth of knowledge and cultivating the land, I would say, is so valuable, and it’s completely been transformed and instilled into my children, so that you can’t take away those kinds of things.” These were benefits of caregiving for the PLWD in their home. Contrary to the common use of “wealth,” which frequently is used in the context of economic value, all three of these caregivers describe wealth in the context of knowledge. When conducting member checks, the caregiver affirmed the use of “wealth” in relation to the knowledge of kūpuna, sharing “that experience, that they can look at a situation, and even with dementia they can tell when something’s wrong, or they can tell when something is like, you’re going to have a problem there, that kind of experience and knowledge is invaluable. Yeah, culturally, they are the knowledge holders.”
Kuleana of Caring
Caregiving was described as an expectation, responsibility, or kuleana, and a cyclical process. For example, a caregiver said, “It just makes me realize my parents are getting older and then pretty soon I’m going to have to take care of them. It’s just a constant cycle of just being caring to everyone.” Another caregiver stated, “I’ve always been the caretaker. . . It’s just natural for me to just help my mother-in-law.” Lastly, another caregiver stated
“This is what we do,” telling my kids, “We don’t really have an ‘old folks’ home’ right on Guam or Palau, we retire and we die in our homes, and we’re taken care of at home,’ so trying to pass on that information about who takes care of who and those responsibilities as kids. So that’s what I’ve recognized of this journey that I went through with my mom.
Caregivers described caring for elders while growing up and that expectation and the cyclical nature of this responsibility; expecting the younger generations to care for them as well.
Within the description of this responsibility, it is important to acknowledge the nuanced meaning of kuleana. While the simple translation of kuleana is responsibility, kuleana has additional meanings, including right, privilege, reason, cause, function. According to participants, caregiving is both a responsibility and a privilege; having a kuleana includes the privilege to have that responsibility.
Responsive kuleana when caregiving
With this kuleana, one of the caregivers emphasized the importance of the changing caregiving role, particularly with the progression of dementia, and the need for flexibility and responsiveness in the kuleana of caregiving. The caregiver offered the example that in Hawaiian culture, the oldest daughter takes on the caregiving role. However, as dementia progresses, the PLWD might prefer to have another family member take over the caregiving role. With this change in kuleana at the request of the PLWD, the family needs to allow for fluidity, flexibility, negotiation, and renegotiation of responsibilities to respect the wishes of the PLWD.
Barriers and Facilitators to Health and Well-being for Caregivers
We were interested in characterizing the barriers and facilitators to health and well-being that caregivers described during the interviews. Barriers included costs associated with caregiving, not being aware of resources that are available, difficulties in scheduling to ensure someone is available to provide care, the cost of living in Hawaiʻi, lack of resources available to Compacts of Free Association (COFA) Islanders, access to interpreters (who are not related to the PLWD), distrust of the medical system, and the cultural stigma of using caregiving resources. As the cost of living in Hawaiʻi, resources available to COFA Islanders, distrust of the medical system, and cultural stigma of using caregiving resources might be unique to caregivers of NHPI adults living with ADRD, we expand on these themes. Caregivers described the high costs of living in Hawaiʻi, with one caregiver explaining that “most of us work two jobs just to not live on a paycheck-to-paycheck basis.” In return for military control over the islands, COFA Islanders are allowed to work, live, and study within the US without visas, however, they are not US citizens, limiting access to many US programs (McElfish, Purvis, Riklon et al., 2019). COFA Islanders are not eligible for Medicaid, even though large numbers of COFA Islanders serve in the US military and live within the US (McElfish, Purvis, Riklon et al., 2019). One caregiver, whose PLWD was a COFA Islander, shared their experience of moving the PLWD to the continent “Before I moved her here, I had tried to call around places, different resources, and they’re like, ‘Oh yeah, go ahead, bring your mom,’ and when I did, they’re like, ‘Oh, she’s not a US citizen so she can’t get these different benefits.’” Similarly, while they shared the following challenges in using interpreters when accessing medical care, “we would have to ask for a Palauan translator, who ended up being also a relative, which makes it also hard for [PLWD] . . . to be able to share what she needs to share and not have to go through her own relatives, which makes her just say, ‘Oh no, I’m fine, I’m okay, nothing’s wrong.’” This was further complicated by distrust in the medical system, which was described by a caregiver who said, “But as someone who grew up not trusting doctors, and for good reason, our people have not been treated well by science and scientists and researchers, and people who are trying to help us, but not really, but are harmful.” Lastly, caregivers described stigma or the lack of acceptance of external help. One caregiver said, “We did try it, to go outside of the family and get some help. It didn’t work. My elder was very . . . they were against it pretty much, and they didn’t. And I think a lot of that too comes back to the cultural background that we have. But we considered it, and in the end it came down to providing care within the family.” Taken together, these unique barriers faced by caregivers of NHPI adults living with ADRD may negatively impact their health and well-being.
Facilitators included engaging in cultural practices, caring as a family or ʻohana, having financial resources, having knowledge of the medical system and available supports, and using technology to support communication. Culturally-unique facilitators to health and well-being including caring as a family and engaging in cultural practices and are described in the themes previously presented including caring as community, connection to cultural practices, and kūpuna as knowledge holders. These themes illustrate an important cultural strength with many caregivers describing the importance of caring as a family and larger community as well as the appreciation for the cultural wealth held by the PLWD that can be shared while providing care.
Discussion
The prevalence of family caregiving for NHPI adults living with ADRD is likely to rise with the increasing life expectancy, aging population, and high rates of ADRD among an already high-risk population. As NHPI adults likely have a higher prevalence of ADRD and thus, are a priority population, we aimed to describe the health and well-being of family caregivers of NHPI living with ADRD; explore cultural values related to caregiving; and characterize barriers and facilitators to their health and well-being. We identified that caring as a community, lōkahi, and the importance of sleep, food, and physical activity were important to caregiver health and well-being. Cultural values included connection to cultural practices, kūpuna as cultural knowledge holders, and the kuleana of caregiving. Lastly, unique cultural barriers included the cost of living in Hawaiʻi, resources available to COFA Islanders, distrust of the medical system, and cultural stigma of using caregiving resources while facilitators included caring as a family and engaging in cultural practices.
Our findings illustrate multiple sources of support throughout the caring process, expanding beyond the common conceptualization of caregiving as a dyadic relationship. Interviews with caregivers reveal a relational, community, and family approach to care instead of a dyadic pair. Furthermore, caregivers prioritize balance (lōkahi) in relationships when providing care, aligning with the four aspects of the Indigenous Connectedness Framework: community, environment, family, and intergenerational connectedness (Ullrich, 2019). In applying this framework, caregivers described each of the four aspects of this model: the wealth of knowledge kūpuna, particularly about culture and the land (environment and family connectedness); community connections through cultural practices and social activities (cultural connectedness); and intergenerational connections in family histories and the strengths of the community (intergenerational connectedness). Maintaining social connections was an important subtheme, with caregivers intentionally including the PLWD in activities, acknowledging the PLWD needs social interaction just like they do. As caregivers realized the need for their own inclusion and social interaction, they identified ways to offer structure and support in activities to encourage participation from the PLWD.
Caregivers also described how providing care heightened the importance of also caring for themselves. Prior research suggests that caregivers may be at high risk for negative health outcomes due to insufficient time to engage in promotive health behaviors, experiencing elevated levels of stress, and engaging in negative health behaviors (e.g., substance use) as a coping mechanism (Acton, 2002; Rabinowitz et al., 2007), with many caregivers reporting that they feel their needs are secondary to the needs of the care recipient (Tatangelo et al., 2018). While the health of caregivers in the current study varied, caregivers realized they were less effective caregivers when they did not take care of themselves. Thus, encouraging self-care to provide effective care for the PLWD may be an important additional rationale to include in caregiving interventions. For example, when discussing the negative impacts of caregiving in a caregiver intervention, encouraging self-care behaviors not only to promote their own health but to provide improved care may help the caregiver adopt those behaviors. Similarly, considering the strong cultural ties, including sharing cultural practices and promoting culture may be helpful for caregivers.
While NHPI adults comprise more than 50 groups, they are often aggregated and referenced collectively. We identified relevant cultural differences in caregiving across NHPI groups. For example, a caregiver of a COFA Islander described unique barriers including the cost of medical care, distrust of the medical system, and access to interpreters. Alternatively, among Native Hawaiian caregivers, access to interpreters may be less relevant as Hawaiian language was historically discouraged and banned with colonization (McCubbin & Marsella, 2009). While we also identified shared cultural values across groups, important structural and historical barriers persist according to each group’s specific identity and legacy and thus, recognition and inclusion of these differences and values in interventions to support caregivers is imperative.
Limitations of this research include the small sample size and the use of cross-sectional data, which limited our ability to identify how perceptions of caregiving change over time and may be associated with health. Additionally, dementia diagnosis was self-reported, we did not assess the stage of dementia of each caregiver’s respective PLWD, and all data from prior caregivers were retrospectively reported. We faced significant challenges in recruiting participants as our study was hacked by bots and mischievous responders (Jackson et al., 2023). However, we were able to develop a process using referrals from community organizations to recruit participants and verify the identity of participants, allowing us to recruit NHPI participants both in Hawaiʻi and the continental US. While our sample is relatively small, caregivers of NHPI adults living with ADRD are a relatively specific population and our findings from both quantitative and qualitative data point to the importance of family-centered and community-based caregiving.
While caregiving is viewed as an expected kuleana in NHPI culture, there is great privilege to care for kūpuna who hold substantial wealth within the community. Within this privilege, caring often extends beyond a dyadic relationship, and the importance of maintaining family relationships while the disease progresses. However, family-centered caregiving is rarely the focus of caregiving interventions. A recent scoping review identified 13 family-centered interventions, or interventions that focus on family rather than dyadic care (Ramachandran et al., 2023), which has also been identified as an important gap in the literature with prior research focusing on a primary caregiver, which may not consider the larger family unit or family dynamics (Pillemer & Gilligan, 2018). As illustrated in our findings, shifting to a family-centered perspective may also require including family dynamics and family history (Crandall et al., 2023), and the measurement of aspects of caregiving (e.g., caregiving burden or mastery) at the family-level rather than the individual. Building on these findings and the indigenous connectedness framework (Ullrich, 2019), viewing the family or ʻohana as a unit of well-being (rather than individual) and developing family-centered culturally tailored interventions may be an important step to promote caregiver health in NHPI communities. To effectively support caregivers in NHPI communities, we suggest that researchers, practitioners, and community members work together to develop or tailor caregiving interventions that center family (rather than dyads), focus on family relationships, recognize the heterogeneity in NHPI communities, and prioritize cultural practices as methods to promote self-care. In alignment with existing caregiving interventions (Gallagher-Thompson et al., 2012; Ramachandran et al., 2023), these newly developed or tailored interventions can be delivered by trained community members, community health workers or healthcare professionals either in community or healthcare organizations to promote caregiver health.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596241286232 – Supplemental material for Health and Well-being of Family (‘Ohana) Caregivers of Native Hawaiian and Pacific Islander Adults Living with Alzheimer’s Disease and Related Dementias
Supplemental material, sj-docx-1-tcn-10.1177_10436596241286232 for Health and Well-being of Family (‘Ohana) Caregivers of Native Hawaiian and Pacific Islander Adults Living with Alzheimer’s Disease and Related Dementias by Alexandra Malia Jackson, Clemma Jacobsen Muller, Scott K. Okamoto, Raven H. Weaver, Steffi M. Kim, Magdalena Haakenstad, Cortney Pfeaster, Zowey Cachola, Ashley Oshiro, Kacyn Ideue, Nancy Schoenberg and Ka’imi Sinclair in Journal of Transcultural Nursing
Footnotes
Acknowledgements
Author contributions include: AMJ, CJM, SKO, and KS: designed research; AMJ, CJM, SKO, MH, SK, CP, ZC, AO, KI supported data analysis; AMJ and RHW wrote the manuscript; all authors read and approved the final manuscript. We would like to share our appreciation for other members of the NAD-RCMAR cohort and leadership team for their thoughtful insight and for the participants and their family members they provided care for.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Native Alzheimer’s Disease Resource Center for Minority Aging Research (NAD-RCMAR) which is funded by the National Institute on Aging (Grant P30AG059295-05).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.