
Abstract
Introduction:
This study examines acculturation’s impact on sleep quality, efficiency, and obstructive sleep apnea (OSA) risk among Thai women in the United States transitioning through menopause.
Methodology:
This cross-sectional descriptive study recruited 120 Thai women aged 40 to 65. Questionnaires assessed sleep quality (Pittsburgh Sleep Quality Index [PSQI]), OSA risk (Berlin), menopausal symptoms (Menopause Rating), acculturation (Suinn-Lew Asian Self-Identity Scale), and anxiety (Patient-Reported Outcome Measurement Information System). Data were analyzed using bivariate correlations, multivariable regression, and mediation/moderation analyses.
Results:
Mean age was 51.53 (SD = 7.73) years. Most were good sleepers (PSQI <5: 80.83%) and 14.17% at high risk of OSA. Acculturation was associated with better sleep quality (B = −1.086, p = .027) and higher sleep efficiency (B = 2.425, p = .021). Mediation analysis indicated that length of stay in the United States indirectly affected sleep quality (B = −0.022, p = .026) and efficiency (B = 0.051, p = .018) via acculturation.
Discussion:
Acculturation significantly affects sleep among Thai women; higher acculturation correlates with better sleep quality and efficiency. Acculturation did not affect OSA risk, suggesting context-specific influences that may benefit sleep through increased social integration. Future research should explore underlying mechanisms in immigrant populations.
Introduction
The menopausal transition encompassing perimenopause, menopause, and postmenopause is a significant life stage characterized by hormonal, physiological, and lifestyle changes. These changes often lead to sleep disturbances, affecting approximately 50% of women during this period (Baker et al., 2018; Fetveit et al., 2019; Jones et al., 2018). Poor sleep quality, frequent nighttime awakenings, and short sleep duration (less than 7 hr) are common sleep disturbances in this period (Kalleinen et al., 2021; Pien et al., 2008; Tandon et al., 2022; Zak et al., 2023). Obstructive sleep apnea (OSA) is also prevalent in women during and after the menopausal transition, ranging from 6% to 47%, with higher rates observed in postmenopausal women (Ishikura et al., 2022; Kalleinen et al., 2021). Its prevalence is 6.3% among Thai women, but it is not known among Thai women living in the United States (American Sleep Apnea Association, 2023; Julia, 2022; Neruntarat & Chantapant, 2011). Sleep disturbances were linked to increased risks of cardiovascular disease (CVD), depression, mortality, and premature mortality (Cappuccio & Miller, 2017; Choi & Choi, 2020; Hafner et al., 2017; Ormiston et al., 2022; Ravichandran et al., 2023; Yin et al., 2017). These health implications underscore the importance of understanding and addressing sleep issues in menopausal women.
While the general link between menopause and sleep disturbances is well established (Baker et al., 2018; Tandon et al., 2022; Zak et al., 2023), there is a significant gap in the literature regarding the specific experiences of Thai immigrant women. This population presents a unique case for studying sleep during menopause due to the multifaceted influence of Thai culture on their experiences (Richters, 1997). Buddhism, a central aspect of Thai culture, promotes acceptance of menopause as a natural stage, emphasizing reflection and community support (“sanuk”; Richters, 1997; Winzer & Gray, 2019). Traditional beliefs may favor natural remedies, while cultural attitudes toward aging and femininity can vary.
Acculturation, as the process of adopting the cultural traits and norms of a new society (Rothe et al., 2010), adds another layer of complexity to the sleep experiences of Thai immigrant women (Chapagai & Martyn-Nemeth, 2022). Recent studies have identified acculturation as a critical factor influencing sleep in Asian Americans, including those of Thai origin (Aqua et al., 2023). Asian Americans have been found to have shorter sleep duration and poorer sleep quality compared with White Americans (Carnethon et al., 2016; Nandagiri et al., 2023; Ryu et al., 2021). Moreover, the length of residence in the United States was significantly associated with worse sleep among immigrants, including Asians (Liu et al., 2024). Importantly, acculturation in the United States can further affect their experience by potentially changing their views on menopause and influencing help-seeking behaviors.
A combination of factors can influence sleep and circadian health disparities in immigrant populations, particularly women. These include psychosocial (e.g., acculturation stress), cultural (e.g., sleep beliefs and attitudes), and societal factors (e.g., non-leisure physical inactivity, language acculturation; Chapagai & Martyn-Nemeth, 2022; Ghani et al., 2020; Hale et al., 2014; Hale & Rivero-Fuentes, 2011; Kandula & Lauderdale, 2005; Sephton & Kay, 2024; Whinnery et al., 2014; Zou et al., 2021). Thai immigrant women often face challenges balancing work and family life in a new cultural context, potentially lacking the support networks available in their home country (Cadge & Sangdhanoo, 2005). These factors, combined with acculturation stress, may significantly affect their sleep health compared with other Asian immigrant groups during the menopausal transition.
To address the research gap, our study aims to investigate how acculturation mediates and moderates the association between participant characteristics, health factors, and sleep parameters in Thai immigrant women (40–65 years old) transitioning through menopause residing in the United States. Our specific hypotheses are as follows: (a) acculturation mediates the relationship between length of stay in the United States and sleep parameters; (b) acculturation moderates the relationship between participant characteristics (e.g., age, education, income) and sleep parameters; and (c) higher levels of acculturation will be associated with worse sleep quality and efficiency, and increased OSA risk in Thai immigrant women transitioning through menopause. This research is necessary to fill the existing gap in the literature to how menopause and acculturation interact to affect sleep in this specific population. The findings of this study also inform culturally sensitive interventions that can improve the well-being of Thai immigrant women during the menopausal transition.
Method
Study Design and Sample
This study employed a non-experimental, cross-sectional, descriptive design. It was performed in Illinois, USA, from May to November 2021, using convenient sampling methods. Power analysis performed by G Power software version 3.1.9.4 is used to calculate the sample size at the effect size of 0.26 based on a previous study (Chair et al., 2017). Assuming a statistical power of 0.80 and an alpha level of .05, a sample size of 113 is needed in this study. This study included 120 Thai women between the ages of 40 and 65. Most Thai women (90%) were recruited at Thai churches, temples, and community centers because these locations serve as important cultural hubs for the Thai community in this area. These venues provided a familiar and trusted environment for potential participants, facilitating outreach and recruitment. In addition, holding recruitment events at these central locations allowed for efficient access to a larger pool of Thai women. The remaining were recruited online via social media groups. Inclusion criteria included ages between 40 and 65 as this age range typically encompasses the period of menopausal transition in a woman’s life (National Institute on Aging, 2021; Noonil et al., 2012; Thomas et al., 2018); self-identified as Thai women; and knowledge of English. Exclusion criteria were serious mental conditions (e.g., severe major depression) or serious health problems (e.g., cancer); history of CVD (e.g., stroke or transient ischemic attack, heart failure, myocardial infarction, angina, intermittent claudication, significant limb ischemia, aortic atherosclerosis, thoracic aortic aneurysm, or abdominal aortic aneurysm); taking sleeping pills/sleep aids (e.g., melatonin), excessive alcohol intake (greater than 3 glasses per day) or drug abuse; and pregnancy or breastfeeding.
This study was approved by the Institutional Review Board of the University of Illinois Chicago (protocol #2020-0738). E-consent was obtained before enrolling participants in the study.
Measurements
All participants were asked to complete questionnaires related to demographic features (e.g., age, education, marital status, and employment status), acculturation, sleep, and health-related factors, including the Pittsburgh Sleep Quality Index and the Berlin questionnaire. Weight and height were measured in the same manner for all participants.
Statistical Analyses
Stata 15.1 was used to perform the data analyses (StataCorp, 2017). Descriptive statistics, bivariate Spearman’s correlation analysis, multivariable linear regression, and structural equation models (SEMs) were performed. In selecting variables for our models, we considered both theoretical and statistical associations (Heinze et al., 2018; Hilbe, 2009). We included variables that were relevant to our research question and had a relationship with the dependent variable at p < .2. To avoid multicollinearity, we assessed the correlation between variables and avoided including highly correlated variables in the same model. We also aimed for a model that was as simple as possible while still adequately explaining the data. By following this process, we were able to select a set of variables that provided a good balance between model fit and parsimony. Estimation was applied in robust standard errors (SEs) due to the heteroskedasticity of data (Freedman, 2006; James et al., 2013) Tobit regression was applied to estimate the coefficient for sleep efficiency (Long & Long, 1997; Tobin, 1958) because its data skewed toward maximum (ceiling effect); Logistic regression was used to examine the risk of OSA. The p-value of .05 was set to determine the statistical significance of the association among the studied variables.
Mediation analysis was performed to explore the existing relationship between dependent (Y) and independent (X) variable through a mediating (M) variable (X indirectly affects Y through M). The model was drawn based on the bivariate analysis or actual data. The mediating effect was considered to be present if the multiplicative equation (indirect effect) was statistically significant (Jenatabadi, 2015).
Finally, moderation analysis was tested to examine whether the direction or strength of the relation between an independent variable on the dependent variable depends on another independent variable (moderator). It can be tested by entering the interaction terms into the multiple, Tobit, and logistic regression models. The moderating effects were considered if the interaction terms were deemed statistically significant (Hayes, 2022).
Results
Characteristics of the Participants
The participants’ characteristics are presented in Table 1. The mean age was 51.53 years (SD = 7.73). Their average length of stay in the United States was 21.77 years (SD = 12.96). The majority of the participants were foreign-born (96.67%). Most participants were employed (70.83%) and 12.50% worked night shifts. The participants had a mean acculturation score of 1.90 points (SD = 0.58).
Participant Characteristics: Demographic, Acculturation, Health, and Sleep.
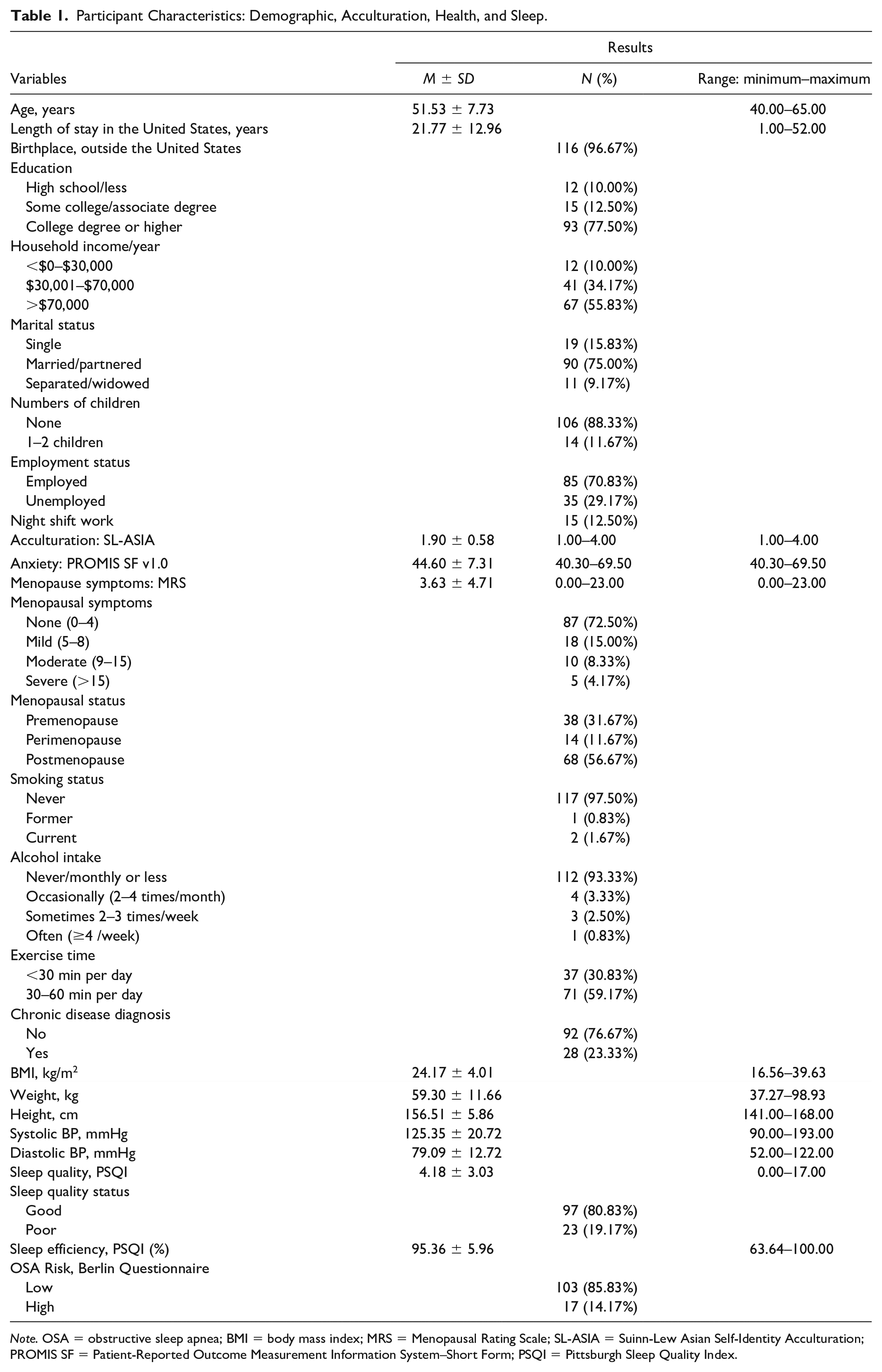
Note. OSA = obstructive sleep apnea; BMI = body mass index; MRS = Menopausal Rating Scale; SL-ASIA = Suinn-Lew Asian Self-Identity Acculturation; PROMIS SF = Patient-Reported Outcome Measurement Information System–Short Form; PSQI = Pittsburgh Sleep Quality Index.
The average anxiety t-score was 44.60 (SD = 7.31), and the menopausal symptoms score was 3.63 (SD = 4.71; Table 1). More than half of the participants had no menopausal symptoms (72.50%). According to the menopausal status, 31.67% of the women were premenopausal, 11.67% were perimenopausal, and 56.67% were postmenopausal. Twenty-eight participants were diagnosed with chronic disease. Their average BMI was 24.17 (SD = 4.01).
Sleep Characteristics of Participants
Sleep quality based on the PSQI score among participants was 4.18 (SD = 3.03), of which 97 participants were good sleepers (80.83%). Sleep efficiency on average was 95.36% (SD = 5.96), and 14.17% (n = 17) of them had a high risk of OSA (Table 1).
Associations Among Sleep Characteristics, Acculturation, and Participant Characteristics
Anxiety, menopausal symptoms, and chronic disease diagnosis positively correlated with PSQI score (r = .281, p = .002; r = .454, p < .001; r = .233, p = .011, respectively). On the other hand, menopausal symptoms and chronic disease diagnosis were found to have negative correlations with sleep efficiency (r = −.318, p < .001; r = −.224, p = .014). The risk of OSA was positively correlated with BMI, menopausal symptoms, and chronic disease diagnosis (r = .226, p = .013; r = .303, p = .001; r = .454, p < .001, respectively). However, the risk of OSA is negatively correlated with longer exercise time (r = −.226, p = .013; Table 2).
Bivariate Associations Among Participant Characteristics, Sleep Characteristics, and Acculturation.
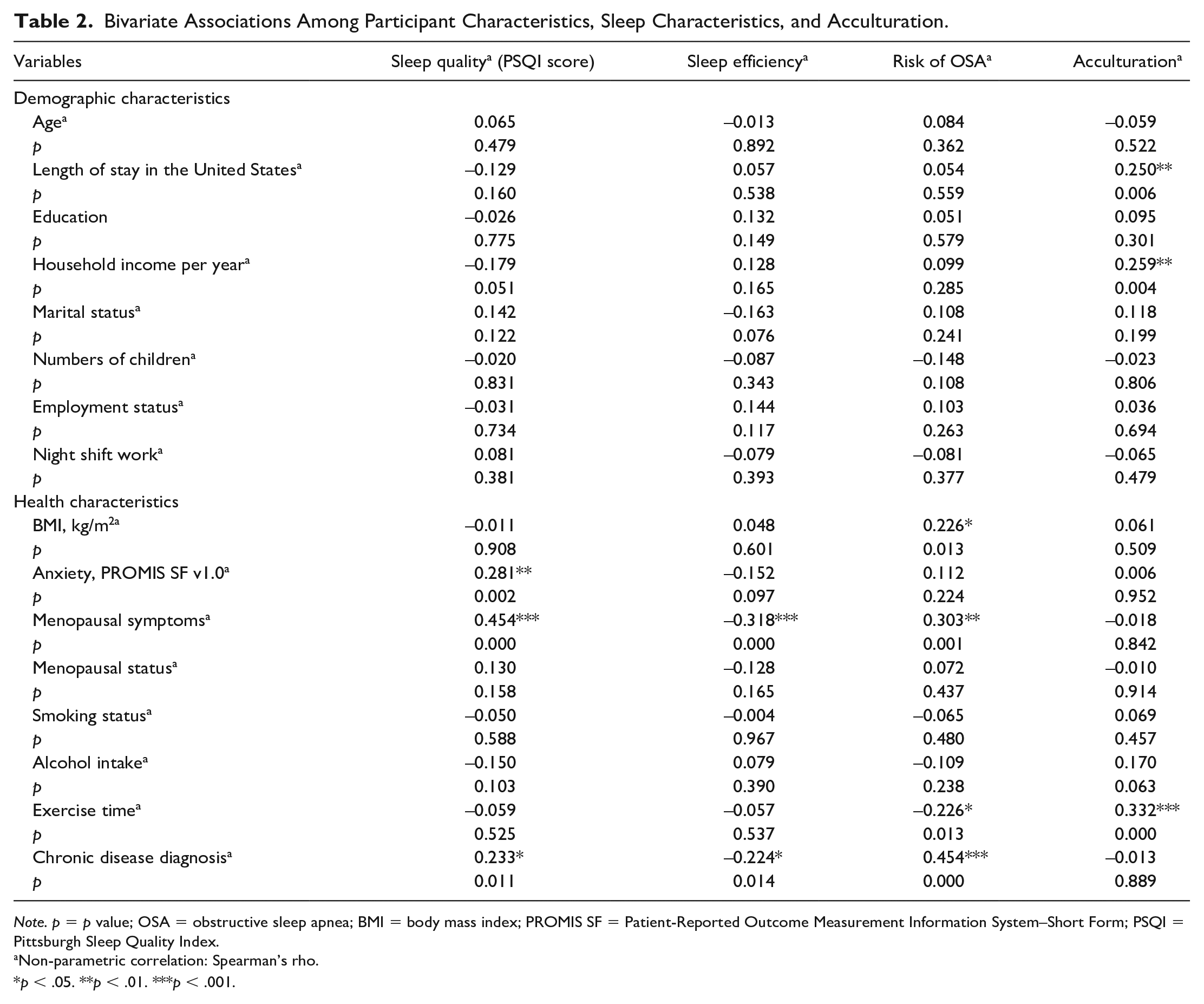
Note. p = p value; OSA = obstructive sleep apnea; BMI = body mass index; PROMIS SF = Patient-Reported Outcome Measurement Information System–Short Form; PSQI = Pittsburgh Sleep Quality Index.
Non-parametric correlation: Spearman’s rho.
p < .05. **p < .01. ***p < .001.
The household income and length of stay in the United States were significantly associated with acculturation (r = .259, p = .004 and r = .250, p = .006, respectively). Exercise time was found to have positive correlations with acculturation (r = .332, p < .001; Table 2).
Associations of Acculturation and Sleep
In unadjusted models (Supplemental Material 1), PSQI score and sleep efficiency were significantly associated with acculturation (B = −1.105, p = .019 and B = 1.962, p = .035, respectively). After adjusting for the age, length of stay in the United States, education, household income, marital status, number of children, employment status, BMI, anxiety, menopausal symptoms, exercise time, and chronic disease diagnosis, the associations of PSQI score and sleep efficiency with acculturation remained significant (PSQI score B = −1.086, p = .027; sleep efficiency B = 2.425, p = .021, respectively). Thus, acculturation is independently associated with sleep, in which the higher the acculturation, the lower the PSQI score and the higher the sleep efficiency. In the regression model for the risk of OSA, chronic disease diagnoses and BMI were excluded due to their relation to the Berlin questionnaire (r = .454, p < .001; −.226, p < .05, respectively). Other categorical variables (household income, marital status, number of children) were excluded afterward due to showing no effects on the risk of OSA in the logistic regression. None of the unadjusted or adjusted models for the risk of OSA showed significant effects of acculturation.
Mediation Analysis
We used models to estimate mediation and moderation paths toward sleep outcomes (see Figures 1, 2, and 3, Supplemental Materials 2 and 3, which demonstrate proposed models). The SEM analysis results are reported in Table 3. While the length of stay itself did not directly affect the PSQI score (Table 3), our analysis revealed a significant indirect effect mediated by acculturation (coefficient = −.022, p = .026; Table 4). A similar pattern emerged for sleep efficiency, where length of stay indirectly influenced sleep efficiency through acculturation in a positive direction (coefficient = .051, p = .018; Table 4).
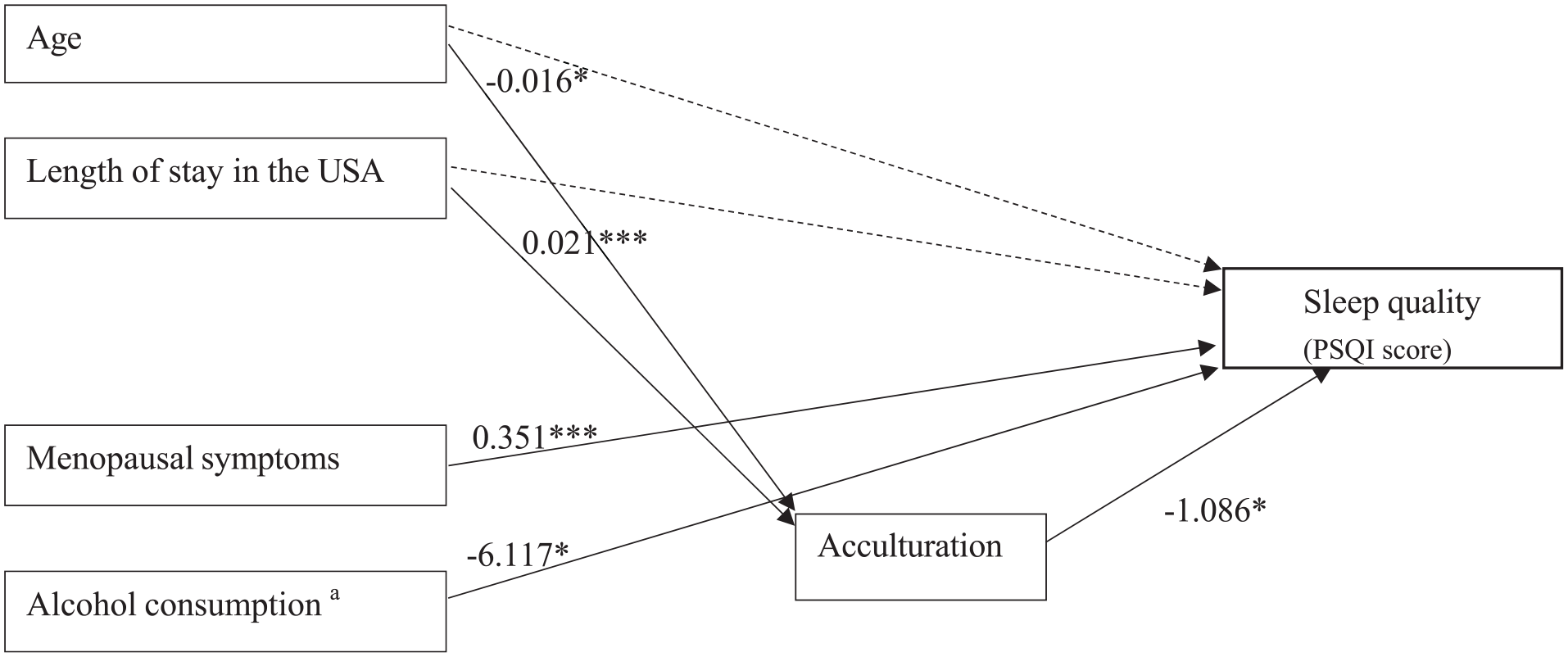
Path Diagram for the Final Model of Sleep Quality. Figure 1 shows the final model of sleep quality (PSQI score) with non-standardized estimates for statistically significant effects. The indirect effect of length of stay in the United States was significant (Coefficient = −0.022, p = .026), while the indirect effect of age was not (Coefficient = 0.018, p = .093).
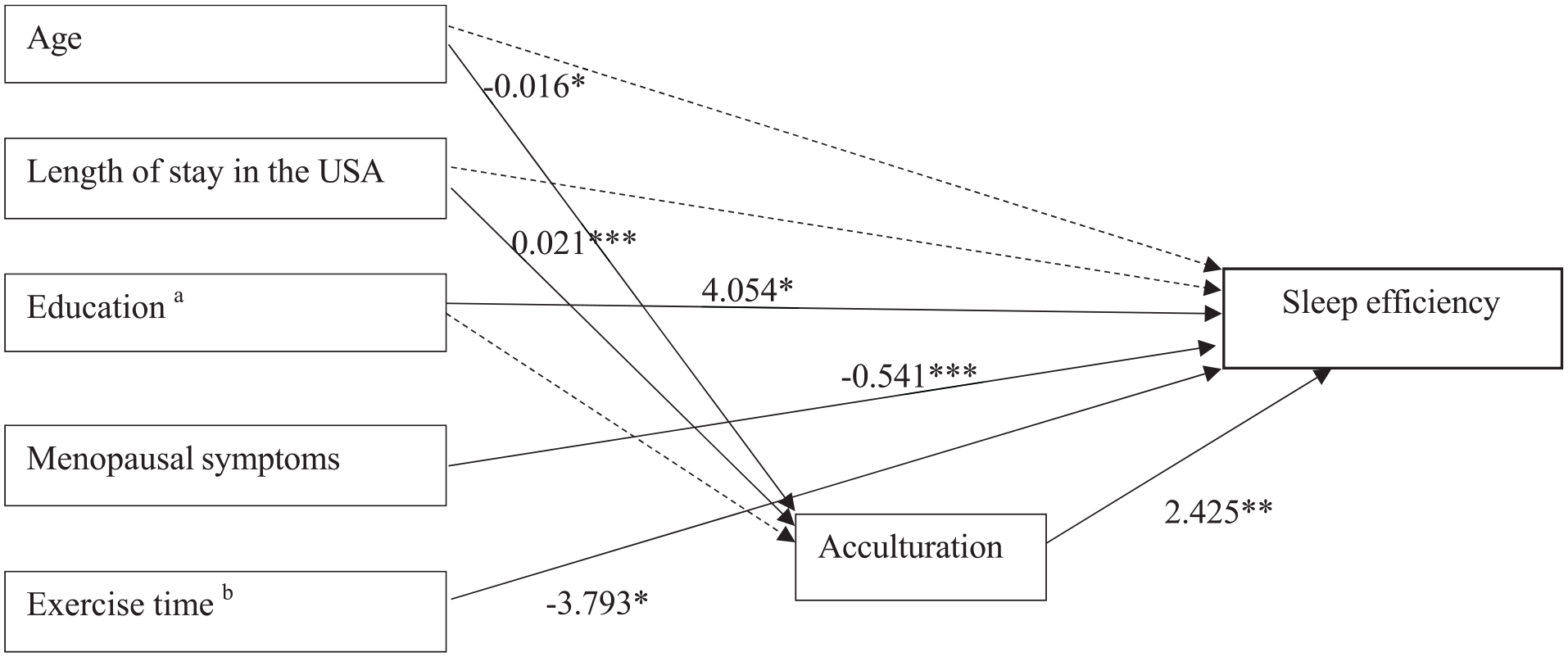
Path Diagram for the Final Model of Sleep Efficiency. Non-significant paths and covariates are omitted for clarity. The indirect effect of length of stay in the United States was significant (Coefficient = 0.051, p = .018), but the indirect effect of age was not significant (Coefficient = −0.040, p = .083).
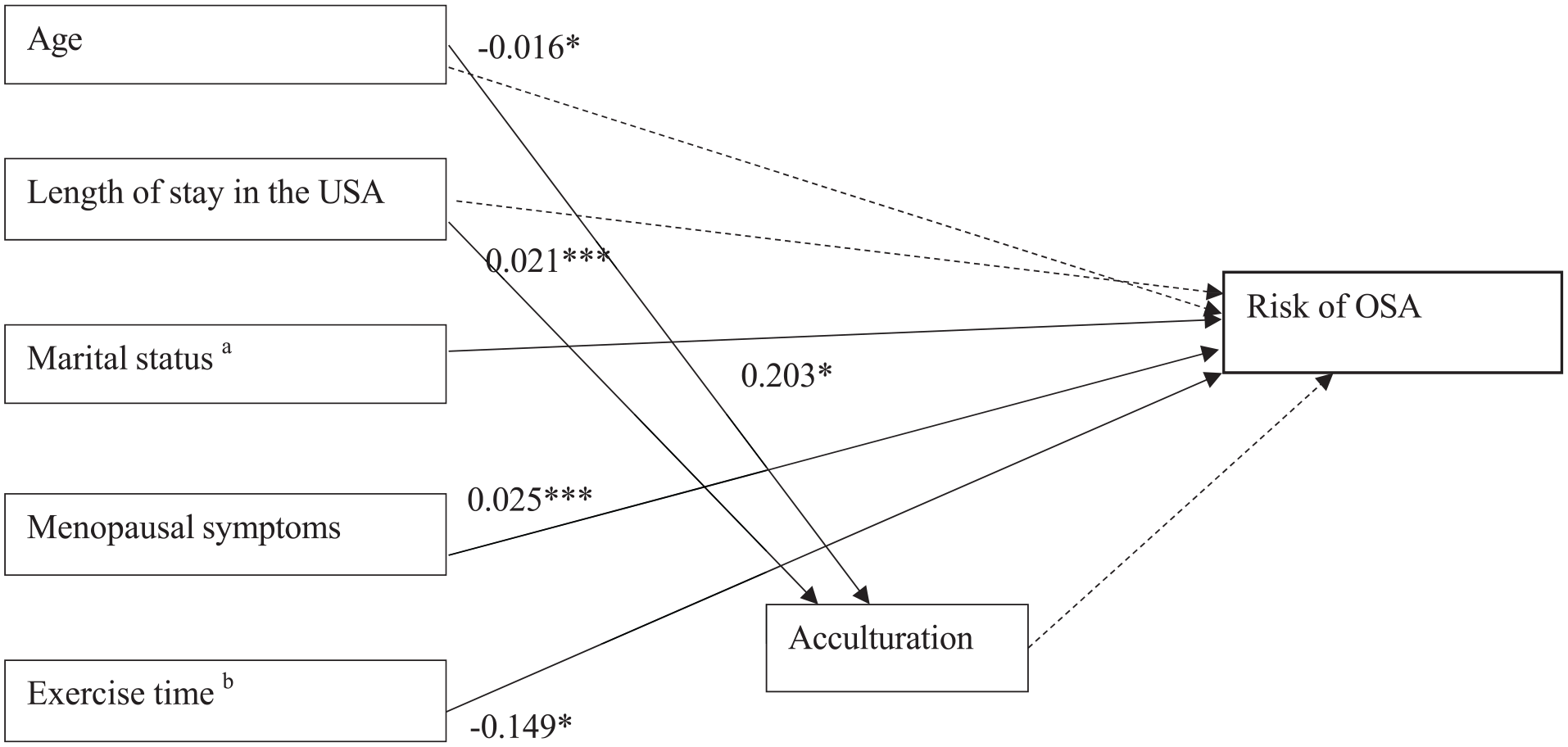
Path Diagram for the Final Model of Risk of Obstructive Sleep Apnea. The indirect effect of age and length of stay in the United States was not significant (Coefficient = 0.001, p = .754 and Coefficient = −0.001, p = .752, Respectively).
Summary of Structural Equation Model of Participants’ Socioeconomic and Health Characteristics on Sleep Quality, Sleep Efficiency, and Risk of Obstructive Sleep Apnea.
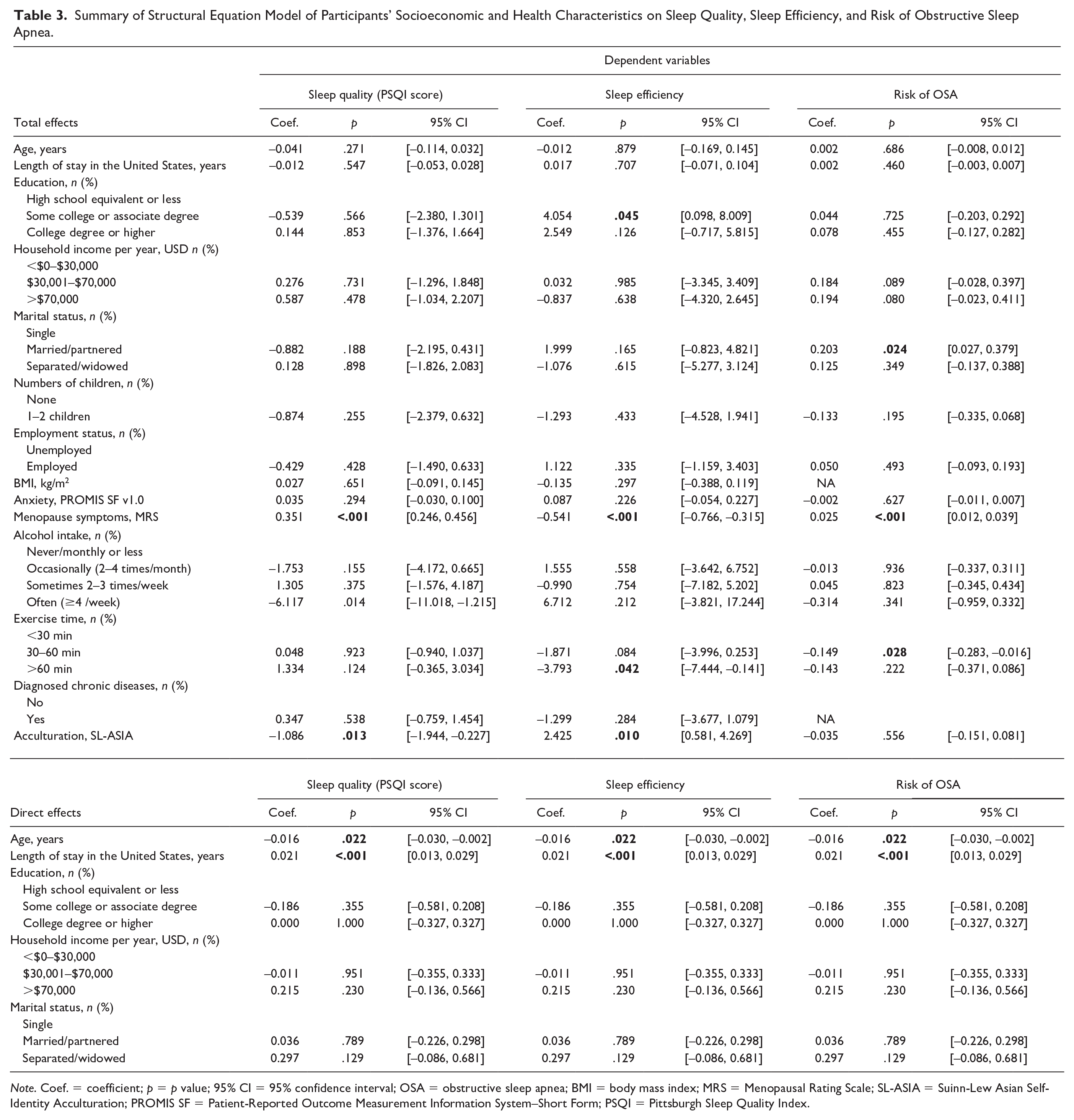
Note. Coef. = coefficient; p = p value; 95% CI = 95% confidence interval; OSA = obstructive sleep apnea; BMI = body mass index; MRS = Menopausal Rating Scale; SL-ASIA = Suinn-Lew Asian Self-Identity Acculturation; PROMIS SF = Patient-Reported Outcome Measurement Information System–Short Form; PSQI = Pittsburgh Sleep Quality Index.
Summary of Multiplicative Approach Estimation of Structural Equation Model of Participants’ Characteristics and Sleep Outcomes.
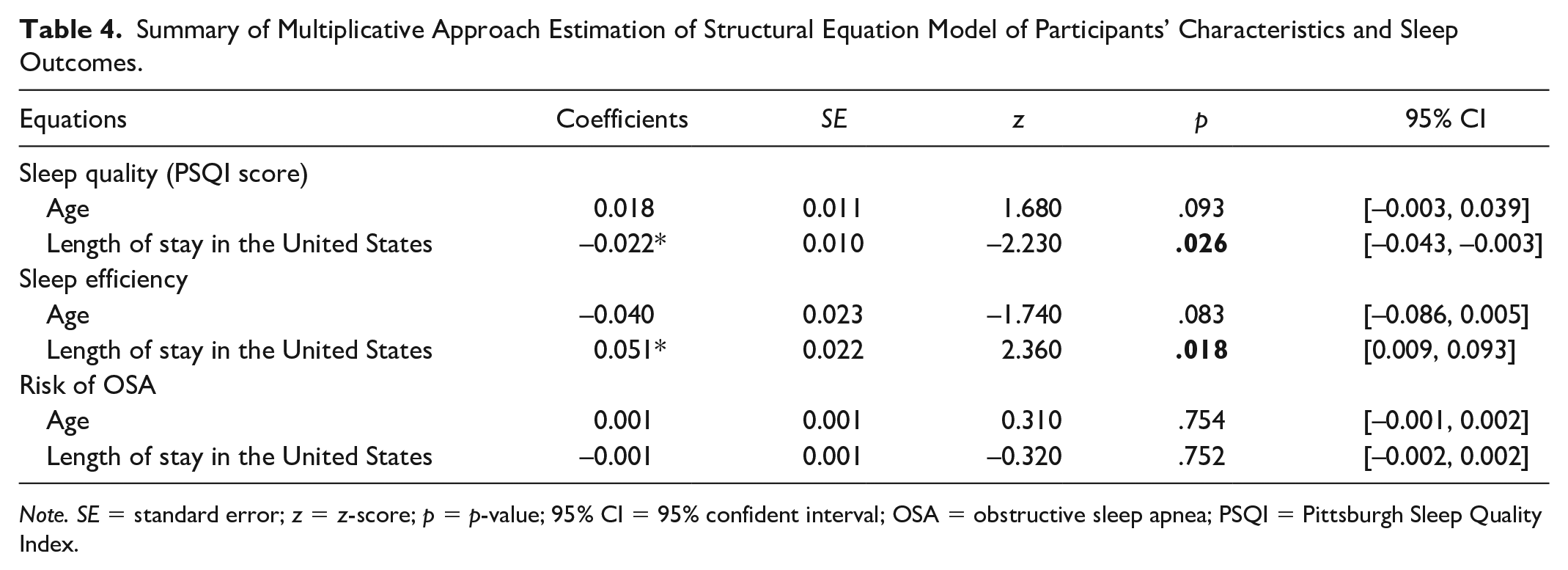
Note. SE = standard error; z = z-score; p = p-value; 95% CI = 95% confident interval; OSA = obstructive sleep apnea; PSQI = Pittsburgh Sleep Quality Index.
Importantly, the multiplicative approach revealed no indirect effects of acculturation on the relationships between either age or length of stay in the United States with the risk of OSA (Table 4). Finally, path diagrams for final models concerning the mediating effects of acculturation on PSQI score, sleep efficiency, and risk of OSA are shown in Figures 1, 2, and 3, respectively, and the indirect effects among the participants’ characteristics, socioeconomic factors, health-related factors, and acculturation on sleep outcomes are summarized in Supplemental Material 4, which demonstrates summary of direct, indirect, and mediating effects.
Moderation Analysis
In this study, to investigate whether acculturation modifies the relationships between demographic characteristics, health-related factors, and sleep outcomes, we examined specific interaction terms in each model. In the PSQI score (sleep quality) model, menopausal symptoms (≥3 moderate-severe symptoms) and alcohol consumption (often, ≥4 times/week) were chosen as moderators due to their known associations with sleep disturbances and potential interaction with acculturation processes. In the sleep efficiency model, education (some college or associate degree) was included alongside menopausal symptoms and alcohol consumption. Finally, the risk of OSA model included menopausal symptoms and exercise time (30–60 min per day) as interaction terms, as exercise time is known to benefit sleep and respiratory function, potentially interacting with acculturation-related lifestyle changes. Our analysis revealed no significant interaction effects of acculturation on any sleep predictor variables (Table 5).
Moderating Effects of Acculturation on the Relationship Between Participants’ Socioeconomic and Health Characteristics With Sleep Quality, Sleep Efficiency, and Risk of Obstructive Sleep Apnea.

Note. Coef. = coefficient; p = p value; 95% CI = 95% confidence interval; OSA = obstructive sleep apnea; BMI = body mass index; MRS = Menopausal Rating Scale; SL-ASIA = Suinn-Lew Asian Self-Identity Acculturation; PSQI = Pittsburgh Sleep Quality Index.
Multiple linear regression with Robust Standard Errors estimation.
Discussion
Our study is the first of its kind that aimed to explore the complex interplay between acculturation, demographic characteristics, health factors, and sleep health in Thai women transitioning through menopause in the United States. It contributes to the understanding of sleep health parameters, including sleep quality and efficiency in this specific population. Our study revealed a novel positive association between higher acculturation and improved sleep quality and sleep efficiency in this population after adjusting for a range of potential confounders. We found that these women (~97% foreign-born) had high sleep quality and efficiency, with most of them being good sleepers at low risk of OSA. Although acculturation did not moderate the effects of women’s demographic characteristics, health-related factors, and sleep (i.e., sleep quality, sleep efficiency, and risk of OSA), indirect effects suggest that acculturation, particularly the length of stay in the United States had an impact on their sleep quality and efficiency. This unexpected finding suggests that acculturation may play a more nuanced role in sleep health than previously understood and highlights the importance of considering relevant demographic and health factors in future research on this topic.
In this study, Thai women with higher acculturation levels experienced fewer sleep problems. The findings are consistent with previous studies on the Latino populations in the United States, highlighting a connection between higher acculturation levels and improved sleep outcomes (Martinez-Miller et al., 2019). This association may be explained by acculturative stress (Lee et al., 2022). Factors such as perceived discrimination, limited English language proficiency, and low levels of family cohesion have been identified as significant predictors of acculturative stress (Lueck & Wilson, 2010), leading to sleep disturbances (Lee et al., 2022). Individuals with lower U.S. acculturation may experience increased acculturative stress due to limited social support, perceived discrimination, and language barriers. Moreover, our study found that participants experienced lower anxiety scores compared to the general population’s average or higher anxiety t-scores (≥50; Rothrock et al., 2020) which are usually associated with worse sleep quality. These psychological factors influence their mental health and contribute to poorer sleep quality (Lee et al., 2022; Lueck & Wilson, 2010).
Previous studies found that greater social support from family and community members has been associated with increased life satisfaction and fewer sleep-related symptoms (Hombrados-Mendieta et al., 2019; Im et al., 2020). In this study, most Thai women were recruited from locations like Thai temples, churches, and community centers, offering strong community support. This supportive environment may help them adjust to the U.S. culture, improving their coping skills potentially resulting in lower acculturative stress and better sleep-promoting strategies. Furthermore, our study identified an intriguing indirect effect of acculturation. Longer lengths of stay in the United States were associated with higher acculturation, which, in turn, was linked to improved sleep quality and efficiency. Similarly, an earlier study observed that the length of stay in the United States, along with acculturation, accounted for the numbers and severity of sleep-related symptoms; however, the length of stay in the United States alone did not predict sleep-related symptoms (Im et al., 2020). This suggests that acclimatization to the U.S. culture over time, potentially through increased social integration and access to resources likely due to high income, might contribute to better sleep health.
In this study, the majority of participants in the study (97%) were foreign-born, suggesting fewer sleep problems and better sleep health among first-generation immigrants compared with US-born immigrants (Hale et al., 2014; Im et al., 2020; Newsome et al., 2017; Seicean et al., 2011). Similar to the Hispanic paradox, cultural factors may play a role (Seicean et al., 2011). This suggests that foreign-born immigrants may carry cultural practices that promote better sleep or adopt healthier lifestyles, which positively affect their sleep health (Chapagai & Martyn-Nemeth, 2022; Hale & Rivero-Fuentes, 2011). However, conflicting findings exist, with some studies stating that foreign-born Asians who have lived longer in the United States have more sleep difficulties and shorter sleep duration compared with those with shorter durations of residence (Liu et al., 2024; Ryu et al., 2021; Zou et al., 2021). These discrepancies highlight the need for further research to clarify the complex interplay of acculturation, length of stay, and sleep health among immigrants.
Our finding of higher sleep efficiency with increasing acculturation adds a layer of complexity to the understanding of acculturation and sleep. While a previous study performed at the US-Mexico Border observed lower weekend sleep efficiency in individuals with higher Anglo acculturation (Ghani et al., 2020), our results suggest a different potential impact of social factors. We speculate that individuals with higher acculturation may engage in different social activities on weekdays versus weekends, leading to variations in sleep patterns. For instance, busy weekdays and short sleep duration might lead them to prioritize sleep efficiency, while weekend leisure activities could result in longer sleep duration. However, we did not collect data to directly compare weekday/weekend sleep duration and efficiency and their associations with social behaviors. Future research should explore these nuances to clarify the interplay between acculturation, social activities, and sleep across different time frames.
Our research highlights a substantial connection between menopausal symptoms and sleep health among Thai women. Increased menopausal symptoms were correlated with poorer sleep quality, reduced sleep efficiency, and a heightened risk of OSA. More importantly, the significant role of acculturation as a mediator was observed in the relationship between participant characteristics and health-related factors with sleep disturbances, including sleep quality and sleep efficiency. Our findings are compatible with previous research showing that menopausal transition and symptoms are associated with sleep disturbances (Woods & Mitchell, 2016; Zak et al., 2023) and that middle-aged women with menopausal symptoms experience a higher prevalence of sleep disorders and risk of OSA (Mirer et al., 2017). Menopausal symptoms such as fatigue, excessive daytime sleepiness, morning headaches, and mood changes or irritability are also linked to sleep disturbances (Odai et al., 2022). In addition, certain physical and hormonal changes associated with menopause may contribute to sleep apnea development, further impacting sleep quality and efficiency (Barot, 2021). Distinguishing between sleep disturbances stemming from menopausal symptoms and an underlying sleep disorder like OSA can be challenging due to overlapping symptoms. It is recommended to conduct comprehensive sleep assessments for middle-aged women facing sleep issues, which should include thorough evaluations of menopausal symptoms and potential risk factors for OSA.
Limitations and Strengths
The current study offers valuable information, but it is important to acknowledge its limitations to interpret the findings accurately. Most Thai women in this study were foreign-born and recruited from Thai temples, churches, and community centers around Chicago areas using convenience sampling strategies. This may limit the generalizability of our findings to all Thai women in the United States. Future research should utilize more rigorous sampling methods, such as stratified or probability sampling, to include Thai women from different backgrounds and social connections. In addition, the cross-sectional design cannot capture the full dynamic nature of sleep changes. Finally, we collected data using only subjective sleep measures which introduces potential bias and did not assess acculturative stress. Future studies should use longitudinal designs that incorporate subjective and objective measures to provide a more accurate and comprehensive understanding of sleep.
Despite these limitations, the combined strengths of this study delineated below enhance the accuracy of our findings and also lay the groundwork for future investigations to further advance our understanding of sleep health in diverse populations. This study comprehensively examines the relationships among demographic characteristics, health-related factors, acculturation, and sleep among Thai women living in the United States, filling a significant gap in existing research. We also employed a validated acculturation scale which ensures more accurate and nuanced assessment of this complex concept compared to relying on language or English proficiency as a proxy measure for acculturation. Furthermore, utilizing structural equation modeling (SEM) analysis elevates this study beyond simple correlations. This sophisticated approach investigates the causal pathways and intricate interactions between the identified variables, revealing the underlying mechanisms influencing sleep health within this context.
Conclusion
This study found a nuanced and context-dependent relationship between acculturation and sleep health in Thai immigrant women. Higher acculturation was associated with improved sleep quality and efficiency but not with OSA risk. Acculturation indirectly influenced sleep through length of stay in the United States, suggesting that social integration and resource access may contribute to better sleep. However, acculturation did not moderate the associations between other factors and sleep, indicating a complex interplay. These findings have significant implications for community health initiatives and clinical practice. The positive association between acculturation and sleep health in Thai menopausal women underscores the importance of culturally tailored interventions to promote sleep health in a manner that is accessible, acceptable, and empowering to this specific population. Community outreach programs, particularly those based in Thai temples, churches, and community centers, can focus on reducing acculturative stress through language support, social integration, and mental health resources. Health care providers should be educated about the nuanced role of acculturation in sleep health to provide informed and culturally sensitive care. Moreover, policy efforts aimed at facilitating immigrant integration can indirectly enhance sleep health outcomes. Furthermore, studying diverse populations, including US-born and foreign-born groups and various racial and ethnicities, using both objective and subjective sleep measures, is necessary to gain a more comprehensive understanding of acculturation’s role in promoting sleep health in immigrants.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596241297982 – Supplemental material for How Acculturation Shapes Sleep in Thai Women in the United States During Menopausal Transition: A Mediation and Moderation Analysis
Supplemental material, sj-docx-1-tcn-10.1177_10436596241297982 for How Acculturation Shapes Sleep in Thai Women in the United States During Menopausal Transition: A Mediation and Moderation Analysis by Manassawee Srimoragot, Sirimon Reutrakul, Patricia E. Hershberger, Chang Park, Lauretta Quinn, Kylea Laina Liese and Bilgay Izci Balserak in Journal of Transcultural Nursing
Footnotes
Acknowledgements
The authors would like to acknowledge Bahar Banaisad at the Academic Center for Excellent at UIC for assisting with academic writing.
Author Contributions
Manassawee Srimoragot: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft, review & editing. Sirimon Reutrakul: Conceptualization, Methodology, Review & editing. Patricia E. Hershberger: Conceptualization, Methodology, Review & editing. Chang Park: Conceptualization, Methodology, Formal analysis, Review & editing. Lauretta Quinn: Conceptualization, Methodology, Review & editing. Kylea Laina Liese: Conceptualization, Methodology, Review & editing. Bilgay Izci Balserak: Supervision, Conceptualization, Methodology, Writing, Review & editing.
Data Availability
Data will be made available on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript. SR received a speaker fee from Eli Lilly, outside the submitted work. The authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bilgay Izci Balserak was supported by a grant from the National Institute of Health, The National Institute on Minority Health and Health Disparities (NIH, NIMHD): R01MD015724 (USA).
Ethics Approval
The study protocol was approved by the Institutional Review Board of the University of Illinois Chicago (protocol #2020-0738).
Consent to Participate
Written informed consent was obtained from all participants.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.