
Abstract
Introduction:
Purnell’s Model for Cultural Competence outlines that cultural competence is essential for bridging the gap between health care providers and patients from diverse cultural backgrounds.’
Methodology:
This study followed PRISMA-ScR guidelines, focusing on studies involving nurses, nursing students, and educators using Purnell’s Model. Literature was searched across six databases up to July 2024.
Results:
From 834 records, 20 studies met the inclusion criteria. The primary themes identified were “Cultural competence in health care” and “Nursing interventions and patient relationships.” Subtopics included Cultural health care practices, Patient-centric nursing, holistic and culturally sensitive care, and integrated care and education. These subtopics provide a nuanced understanding of cultural competence application across various settings.
Discussion:
Findings highlight the importance of integrating cultural competence training to reduce health care disparities, improve patient–provider communication, and enhance the efficacy of nursing interventions in diverse populations. Incorporating these aspects into education and practice is crucial for achieving cultural competence in nursing.
Keywords
Introduction
In the fast-evolving health care landscape, addressing diverse populations’ unique challenges is paramount (Betancourt et al., 2005; James & Al-Kofahy, 2021; Truong et al., 2014). Cultural competence emerges as a critical component in bridging the gap between health care providers and the multifaceted cultural backgrounds of their patients (James, Al-Kofahy, 2021). Understanding, communicating, and effectively interacting with people across cultures is not merely a desirable skill but a necessary one. It significantly enhances the quality of care, fosters trust, and ultimately leads to improved health care outcomes (Germain, 2024). As health care systems strive to be more inclusive and responsive to the needs of diverse populations, the need for culturally competent practices becomes increasingly evident (James, Al-Kofahy, 2021). This emphasis on cultural competence is key to patient satisfaction, the efficacy of treatment, and patient adherence to medical advice (Maxwell, 2023).
Nurses stand at the forefront of health care delivery, playing an indispensable role in administering culturally competent care that profoundly influences patient experiences and outcomes (Brottman et al., 2020; Magon et al., 2023). Nursing care and nursing competencies demand an acute awareness and sensitivity to the cultural contexts of patients, making cultural competence not just an asset but a necessity in nursing practice (Lalithabai et al., 2021; Stievano et al., 2019). L. Purnell’s (2019) Model for Cultural Competence is particularly noteworthy among the frameworks designed to guide nurses in this endeavor. This model offers a comprehensive, systematic approach to understanding cultural dynamics in health care settings (L. Purnell, 2000, 2002, 2019). Purnell’s Model for Cultural Competence gives health care practitioners an organized approach to understanding and addressing cultural dynamics within health care settings. This model emphasizes the importance of recognizing and respecting cultural diversity to enhance patient care (L. D. Purnell & Fenkl, 2021).
L. Purnell’s (2019) Model for Cultural Competence consists of 12 domains, each addressing a significant aspect of cultural beliefs and practices. These 12 domains are: (1) Heritage—the country of origin, reasons for migration, and associated cultural traditions; (2) Communication—language, voice volume, tone, nonverbal communication, and cultural nuances in conversation; (3) Family Roles and Organization—gender roles, family dynamics, decision-making hierarchies, and social status; (4) Workforce Issues—acculturation, autonomy, and individual versus collective decision-making within a professional context; (5) Biocultural Ecology—variations in skin color, genetics, physical traits, and susceptibility to specific diseases; (6) High-Risk Behaviors—behaviors such as tobacco use, alcohol consumption, and dietary patterns that impact health; (7) Nutrition—dietary preferences, restrictions, and nutritional habits specific to cultural and religious backgrounds; (8) Pregnancy and Childbearing Practices—fertility beliefs, birthing practices, and postpartum rituals; (9) Death Rituals—cultural practices surrounding death, including mourning traditions, burial customs, and bereavement; (10) Spirituality—religious practices, use of prayer, spiritual beliefs regarding health and illness; (11) Health care Practices—cultural views on health care providers, alternative medicine, and traditional healing practices; and (12) Health care Providers—perceptions and expectations of health care professionals, including preferences for same-gender providers and trust in medical systems. These domains offer health care providers a structured framework to assess and integrate patients’ cultural backgrounds into care plans, promoting culturally competent and congruent care.
Compared to other models, such as Campinha-Bacote’s (2002) model, which emphasizes the process of becoming culturally competent through ongoing self-assessment and encounters, and Leininger’s Theory of Culture Care, which emphasizes the interdependence of care and cultural phenomena, aiming to provide culturally congruent care to enhance health and well-being or to support individuals facing disabilities, dying, or death (McFarland & Wehbe-Alamah, 2019), Purnell’s Model stands out for its comprehensive and systematic approach. While each model has its own strengths and areas of focus, the applicability of Purnell’s Model is particularly high due to its holistic and adaptable framework, which makes it suitable for both individual and organizational levels of cultural competence (L. D. Purnell & Fenkl, 2021).
Purnell’s Model provides a domain-based approach that integrates multiple aspects of culture into patient care plans. Despite the differences, all the available models for culturally competent care share a common goal: to enhance the delivery of culturally sensitive care. The practical utility of Purnell’s Model extends beyond education, encompassing clinical practice, administration, and research (Fadaeinia et al., 2022). The model encourages health care providers to consider the broader social and cultural context surrounding patients, helping them recognize how factors such as immigration, socioeconomic status, and acculturation influence health behaviors and care preferences (L. Purnell, 2019). Health care providers could enhance their cultural awareness and sensitivity and systematically evaluate their own cultural biases by engaging in self-reflection, as highlighted by Purnell’s Model. This approach fosters improved communication, builds trust, and ultimately aligns care with patients’ cultural values and expectations, leading to better patient outcomes.
Integrating this model into everyday clinical practice presents complexities requiring attention and ongoing assessment. As the demographic landscape of patient populations continues to evolve, so must the approaches nurses employ to meet their diverse cultural needs (Caruso et al., 2017; Stievano et al., 2019). The model’s theoretical framework offers a foundation for fostering cultural competence among health care providers. Although L. D. Purnell’s (2021) Model has been widely translated and is available in numerous languages, comprehensive mapping of its practical implementation and efficacy is still lacking. In particular, it is challenging to understand how Purnell’s Model impacts patient outcomes, as no synthesis of its practical applications across diverse health care settings is currently available. In addition, the barriers to its adoption and the model’s adaptability to rapidly changing cultural dynamics remain unclear. Similarly, in nursing education, it is difficult to discern what exists in terms of trends, patterns, and topics covered by the literature regarding how Purnell’s Model is being utilized to prepare future health care professionals for culturally diverse environments. Without a clear understanding of these aspects, the overall efficacy of the model and its broader implications for practice and education cannot be fully assessed. This gap highlights the necessity of a comprehensive review that systematically maps the available literature to provide insights into these critical areas, offering a foundation for future research and practical advancements. For this reason, this scoping review aimed to systematically map the available literature utilized in nursing practice and/or education in Purnell’s Model for Cultural Competence and identify key themes and trends to provide a foundation for future advancements in culturally competent health care.
Method
Design
This scoping review was conducted following the last updated methodological guidance for conducting scoping studies (Peters et al., 2021). The “Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews” (PRISMA-ScR) checklist was employed to guide the scientific reporting (Tricco et al., 2018), which is available in Supplementary File 1.
Population, Concept, and Context
The definition of the Population, Concept, and Context (PCC) framework was instrumental in developing the research question and shaping the search strategy for this scoping review (Pollock et al., 2023). This review focuses on studies involving nurses, nursing students, or nursing educators who have engaged with Purnell’s Model for Cultural Competence (population). Therefore, the target population encompasses individuals in various nursing roles and educational stages, providing a comprehensive overview of how the model is utilized across different nursing practice and education levels. The central concept explored in this review is the application of Purnell’s Model for Cultural Competence. This includes examining how the model is implemented in nursing practice, its effects on enhancing cultural competence, and the outcomes associated with its use. The context for this review includes both clinical and educational settings within the nursing discipline. Clinical settings encompass hospitals, community health centers, and other health care environments where nurses provide direct patient care. Educational settings include nursing schools, training programs, and continuing education initiatives aimed at enhancing cultural competence among nursing professionals.
Based on the PCC framework, the main research question guiding this scoping review is: How has Purnell’s Model for Cultural Competence been applied within nursing clinical and educational practices, and what are the key themes, trends, and gaps identified in the existing literature?
Eligibility Criteria
The eligibility criteria for this scoping review were defined to ensure a comprehensive and relevant literature synthesis. Studies were included to determine whether they utilized Purnell’s Model for Cultural Competence in clinical or educational nursing settings. All types of study designs were considered, including qualitative, quantitative, mixed methods, case studies, descriptive studies, peer-reviewed articles, theses, and conference proceedings to ensure a broad scope. The target population comprised nurses, nursing students, or nursing educators. No language restrictions were applied if the records were available in an HTML version and deemed translatable using web-based automatic translation tools (Peters et al., 2021). In the case of the unavailability of an HTML version of an eligible record, the English language was set as an inclusion criterion. There were no time limits set for the included studies. Studies were excluded if they applied Purnell’s Model in disciplines other than nursing or were conducted in noneducational or nonclinical settings.
Search Strategy
A comprehensive search strategy was employed to identify studies utilizing Purnell’s Model for Cultural Competence in nursing clinical and educational practices. Multiple databases were searched, including PubMed, Embase, Scopus, Web of Science (WoS), CINAHL, and Google Scholar. The search terms used in these databases targeted variations of “Purnell model” and related keywords to capture relevant studies. A full list of query terms and detailed searches for each database is provided in Supplementary File 2 for transparency and replicability.
The search strategy was developed using a stepwise process, building queries in strata that aligned with the PCC framework. Within each stratum, sensitivity was prioritized by using the operator OR to include all relevant terms and variations, while specificity was achieved by unifying the strata with the operator AND (see Supplementary File 2). This approach ensured the breadth and depth necessary for a comprehensive review of the literature.
Study Selection Process
As depicted in Figure 1, the PRISMA 2020 flow diagram guided the study selection process. Initially, records were identified from PubMed (n = 45), Embase (n = 17), Scopus (n = 668), WoS (n = 49), CINAHL (n = 55), and Google Scholar (n = 573), totaling 834 records. Duplicate records (n = 138) were removed before screening, resulting in 696 records for screening. Two independent authors conducted the screening process, first assessing titles and abstracts for relevance. Any disagreements between the two reviewers were resolved through discussion and, if necessary, consultation with a third reviewer to ensure consistency and minimize bias.
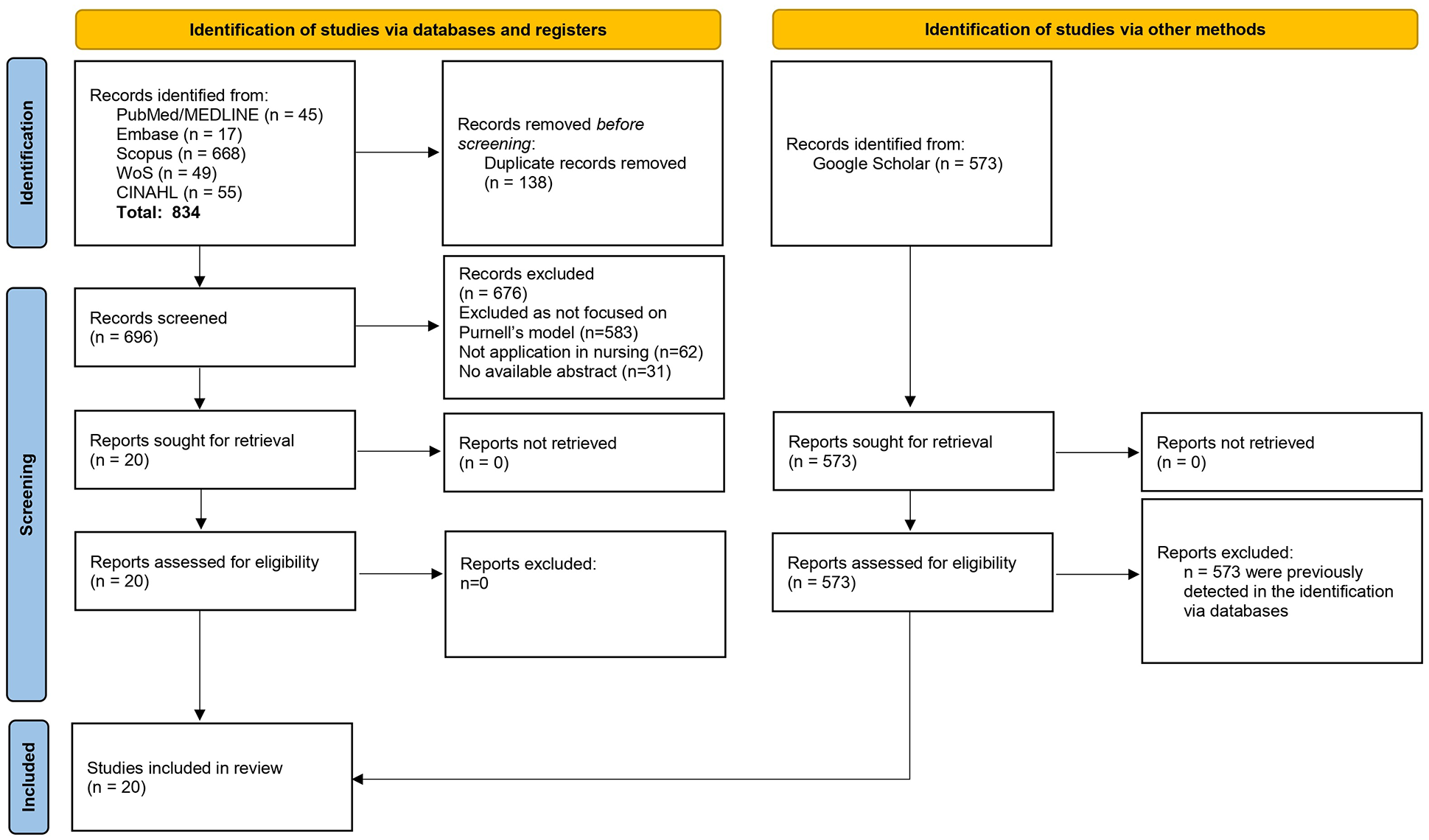
PRISMA 2020 Flow Diagram.
During the title and abstract screening, 676 records were excluded based on predefined criteria: 583 were not focused on Purnell’s Model, 62 were not applicable to nursing, and 31 lacked available abstracts. Records identified via Google Scholar (n = 573) were also screened, but these were duplicates of those already identified through the other databases, and no additional reports were retrieved from this source.
The remaining 20 reports were retrieved and assessed for eligibility, and none were excluded at this stage. Thus, 20 studies were included in the review. Although the process was rigorous, challenges in conducting the selection process included the large volume of initial records and ensuring consistency in screening decisions, which was managed through regular team discussions and consensus-building.
Data Extraction and Rationale for Data Mining Analytics
Data for each included study were initially extracted considering the following categories: author and year of publication, country, study design, research focus, objective, sample, and main results. In the first extraction, the main results were extracted narratively and in an extended version, reflecting a summary for each included study (see Supplementary File 3).
The decision to integrate data mining, specifically latent Dirichlet allocation (LDA), into this scoping review emerged from the goal to go beyond traditional coding-based methods and employ a more innovative, data-driven approach to mapping the literature (Caruso et al., 2024; Chauhan & Shah, 2022). Given the broad and unstructured nature of the data, LDA was ideal for identifying hidden topics in a way that manual coding or framework-guided reviews, often associated with subjectivity, could not achieve. LDA uses statistical models to systematically analyze large, unstructured textual datasets, revealing patterns and relationships that may otherwise remain unnoticed. This approach ensures a more comprehensive and objective exploration of the literature, especially when dealing with diverse studies.
Moreover, using LDA for topic identification, followed by k-means clustering for subtopics, allowed us to break down the data into distinct thematic layers, providing a richer and more nuanced understanding of the research landscape. This innovative combination of techniques streamlined the review process and revealed deeper insights into the field, ultimately pushing the boundaries of traditional scoping reviews.
While valuable in synthesizing quantitative data, a traditional meta-analysis was not applicable in this context due to the heterogeneity of study designs, objectives, and outcomes within the included literature. Furthermore, pooling effect sizes do not align with the broad, exploratory questions typical of a scoping review (Pollock et al., 2023). Instead, the focus here was on identifying broad themes and knowledge gaps, aligning with the goals of a scoping review. Data mining, supported by LDA, allowed us to analyze this diversity and extract meaningful themes without the limitations of a traditional meta-analytic approach.
Data Analysis
The main results of the data extraction form were then used to perform an LDA in R version 4.4.2, following the description of the lexicometric characteristics of the textual corpus. To determine the optimal number of topics (see Supplementary File 4), the “ldatuning” package was utilized (Moor, 2023), which assesses the optimal number of topics using four metrics (Arun et al., 2010; Cao et al., 2009; Deveaud et al., 2014; Griffiths & Steyvers, 2004). Based on the assessment of the top-used words and word clouds produced for each topic (Supplementary File 4), two key topics emerged as the most plausible to summarize the main results of the included studies: “Cultural competence in health care” and “Nursing interventions and patient relationships.”
To ensure the robustness of the LDA results, we employed Multiple Correspondence Analysis (MCA) and k-means cluster analysis as complementary techniques for model validation (Hjellbrekke, 2019). This validation was necessary because LDA, while effective at identifying topics, relies on probabilistic models that may not fully capture relationships between variables in the data. Therefore, MCA was used to visually and statistically validate how well the topics generated by LDA aligned with key variables such as year of publication, country, and study design. This analysis allowed us to assess the coherence and separation of topics in a multidimensional space, further strengthening the validity of the LDA results (Hjellbrekke, 2019).
The k-means clustering suggested the optimal number of subtopic clusters, indicating distinct groupings of studies based on the identified subtopics and their relationships with the analyzed variables. A detailed description of this approach is available in Supplementary File 4.
In line with standard methodologies for scoping reviews (Peters et al., 2021), this study did not include a risk of bias assessment for the studies it examined. This choice aligns with the primary aim of scoping reviews: to broadly and inclusively map the existing evidence on a specific topic. Unlike systematic reviews or meta-analyses that critically evaluate the quality of evidence and synthesize detailed results, scoping reviews focus on summarizing available research to identify knowledge gaps and suggest areas for future inquiry.
Knowledge Synthesis Process
Following the data analysis using LDA, along with validation techniques such as MCA and k-means clustering, the process of knowledge synthesis was conducted in a structured manner. First, the two overarching topics identified through LDA—“ Cultural competence in health care” and “Nursing interventions and patient relationships”—formed the foundation for synthesizing the findings. These topics were interpreted by reviewing the top-used words and word clouds generated during the analysis, which clarified the thematic focus of each topic (Supplementary File 4). The synthesis process involved a two-tiered approach: thematic consolidation and interpretation of findings.
In thematic consolidation, the LDA results were reviewed to group thematic clusters emerging from the topics and subtopics, capturing both overarching themes and more nuanced insights from the k-means clustering. We evaluated the relationship of these themes with variables such as country, year, and study design. For the interpretation of findings, the criteria for synthesis included the relevance to the research question, recurrence across studies, and alignment with existing cultural competence and nursing frameworks. We also considered the contextual implications of each topic by triangulating the findings with study characteristics, allowing us to identify both patterns and knowledge gaps. The synthesis process highlighted consistent themes, uncovered novel insights, and pointed to areas where evidence was limited, suggesting the need for further research. The ultimate goal was to identify practical implications for improving clinical practice, nursing education, and health care policy, ensuring that the synthesized findings provided actionable insights while addressing key gaps in the literature.
Results
Characteristics of the Included Studies
The results of this scoping review include 20 studies (N = 20) (Aksoy Derya et al., 2022; Al-Hamidi, 2016; Badanta-Romero et al., 2021; Carpenter & Theeke, 2018; Debiasi & Selleck, 2017; Eche & Kline, 2012; Elliott, 2018; Elliott & Patterson, 2017; Estevan & del Carmen Solano Ruíz, 2017; Long, 2011; Louis, 2016; Nieto-Vázquez et al., 2009; Phelps & Johnson, 2004; L. Purnell, 1999, 2001; Rodríguez et al., 2014; Romanello & Holtgrefe, 2009; Sasnett et al., 2010; Škorničková & Moravcová, 2018; Yalcin Gursoy & Tanriverdi, 2020), covering a range of publication years from 1999 to 2022.
As shown in Supplementary File 5, most studies (70%) were published between 2011 and 2021, indicating a growing interest and application of Purnell’s Model for Cultural Competence in recent years. Geographically, half of the included studies originated from North America (50%), while the remaining studies were distributed across Central America (10%), South America (10%), Europe (15%), and Asia (15%).
Regarding the economic context of the countries where the studies were conducted, a significant majority were from high-income countries (80%). Studies from upper-middle-income countries accounted for 15%, and only one study (5%) was conducted in a middle-income country.
The type of publications predominantly consisted of journal articles (85%), followed by conference proceedings or abstracts (10%), and one thesis (5%). This distribution underscores the academic and professional engagement with Purnell’s Model within peer-reviewed literature and scholarly discourse.
Regarding study designs, descriptive observational studies were the most common (45%). Mixed methods studies accounted for 15%, qualitative studies for 10%, literature reviews for 10%, and case reports for 10%, with one thesis (5%) and one randomized controlled trial (5%).
Summary of the Included Literature
The literature reviewed provides a comprehensive overview of Purnell’s Model for Cultural Competence’s application and efficacy across various nursing practices and educational contexts. Studies included in the review span diverse geographic regions, methodologies, and research focuses, reflecting the model’s versatility and widespread relevance ( see Supplementary File 6).
The findings consistently highlight the critical role of cultural competence in enhancing patient care and outcomes. For instance, Aksoy Derya et al. (2022) utilized the model to identify cultural care needs among infertile couples in Turkey, revealing significant emotional and spiritual dimensions. Similarly, Badanta-Romero et al. (2021) applied the model in Peru to address health disparities in indigenous populations, emphasizing the need for culturally tailored health plans.
Several studies underscored the importance of culturally competent training for health care professionals. Debiasi and Selleck (2017) demonstrated the positive impact of cultural competence training on nurse practitioners’ abilities to provide better care. Elliott (2018) used the model to assess and improve home care nurses’ knowledge and confidence in caring for military veterans.
The review also included educational settings, such as the work by Sasnett et al. (2010), which described implementing cultural sensitivity training for health science students, illustrating the model’s applicability in academic curricula.
Emerging Topics: LDA Results
The process leading to identifying the topics that emerged from the main results of the included studies is based on a detailed analysis of the lexicometric properties of the dataset (Supplementary File 4). The lexicometric analysis involved 20 texts, with a total of 1,081 occurrences (N) and 599 distinct forms (V). The high number of unique forms, reflected in the type/token ratio of 55%, indicates substantial diversity in the language used across the included studies. In addition, 407 hapax legomena (H)—words that appeared only once—were identified, representing a significant portion of the vocabulary. This suggests that the dataset contains a considerable number of rare terms, which may contribute to the nuanced understanding of the topics. The mean occurrences per text were 54.05, demonstrating that each study contributed a relatively consistent volume of content to the analysis. These lexicometric properties laid the foundation for the subsequent topic modeling using LDA.
The LDA model was tuned by using four validated metrics—log-likelihood, topic density, symmetric Kullback-Leibler divergence, and topic coherence—to determine the optimal number of topics, with two topics emerging as the most plausible fit. The model produced clear distinctions between the two topics: “Cultural competence in health care,” (40% of the corpus) characterized by terms such as culture, health care, competence, and elderly, indicating a focus on cultural sensitivity in health care settings, and “Nursing interventions and patient relationships,” (60% of the corpus) which centered around terms such as nursing, intervention, group, and family, highlighting the importance of nursing care practices and the dynamics of patient relationships. The word clouds for each topic are available in Supplementary File 4.
Analysis of Topics in Relation to Year, Country, and Study Design
Figure 2 illustrates the distribution of topics derived from the main results of the included studies using MCA, where the biplot explained 20.1% of the overall variance. The differentiation between the topics highlights the varied focus areas within the field of cultural competence in nursing, with one cluster emphasizing the broad cultural competence framework’s applications and the other delving into specific nursing practices and patient care dynamics.
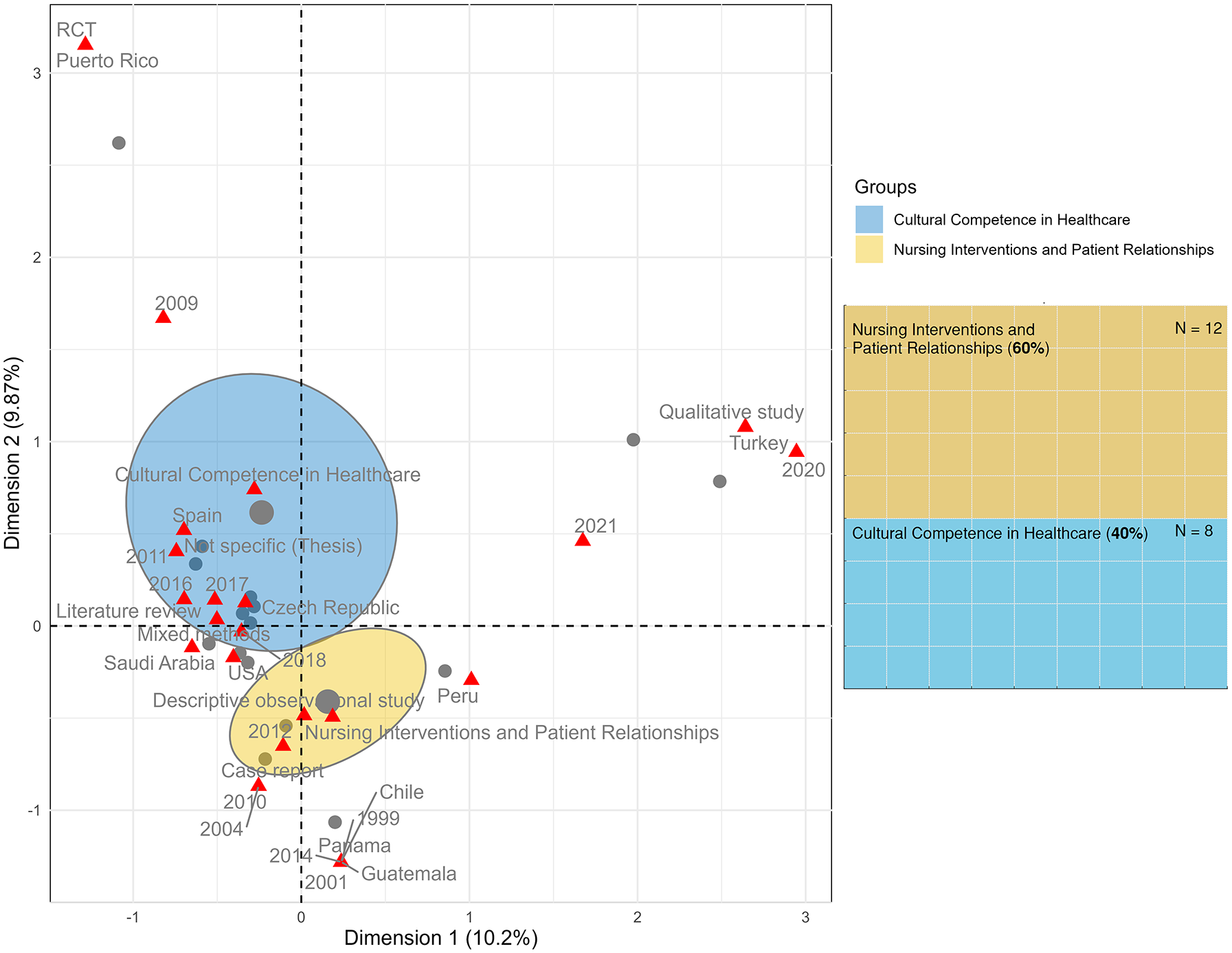
MCA of Topics With Ellipses.
Cultural competence in health care, represented by the blue ellipses (N = 8), predominantly includes studies focused on implementing and assessing cultural competence frameworks in health care settings (Aksoy Derya et al., 2022; Carpenter & Theeke, 2018; Elliott & Patterson, 2017; Estevan & del Carmen Solano Ruíz, 2017; Long, 2011; Louis, 2016; Nieto-Vázquez et al., 2009; Škorničková & Moravcová, 2018). Studies grouped on this topic are mainly from recent years (2016–2021), indicating a growing interest and recognition of cultural competence in contemporary health care research. Most of these studies are from diverse countries such as Spain, Saudi Arabia, and the Czech Republic, highlighting the global relevance of cultural competence. The study designs within this cluster are varied, including literature reviews, mixed methods, and descriptive observational studies, underscoring the multifaceted approach to understanding and implementing cultural competence.
Nursing interventions and patient relationships were represented in the yellow ellipses (N = 12), representing studies focused on specific nursing interventions and the dynamics of patient relationships (Al-Hamidi, 2016; Badanta-Romero et al., 2021; Debiasi & Selleck, 2017; Eche & Kline, 2012; Elliott, 2018; Phelps & Johnson, 2004; L. Purnell, 1999, 2001; Rodríguez et al., 2014; Romanello & Holtgrefe, 2009; Sasnett et al., 2010; Yalcin Gursoy & Tanriverdi, 2020). This topic includes older studies (1999–2014) as well as more recent ones, suggesting a sustained interest in these aspects over time. Countries represented in this cluster include Peru, Panama, Chile, and Guatemala, reflecting a strong focus on patient care and nursing practices in diverse cultural contexts. The study designs here are primarily qualitative and descriptive observational, indicating a detailed exploration of nursing practices and patient interactions.
Identifying Subtopics: Clustering Analysis
The clustering analysis presented in Figures 3 and 4 provides a deeper understanding of the distribution and relationships between the studies included in this scoping review. The studies are grouped into four distinct clusters:
Cluster 1 (subtopic labeled as cultural health care practices = 5% of the total) includes the study by Nieto-Vázquez et al. (2009), emphasizing the topic of cultural competence in health care. This cluster highlights a unique focus within the research landscape on cultural competence.
Cluster 2 (subtopic labeled as patient-centric nursing = 10% of the total) comprises studies such as Al-Hamidi (2016), Long (2011), and Louis (2016), all of which concentrate on Nursing interventions and patient relationships. This cluster signifies the thematic coherence in nursing practices and patient care interventions.
Cluster 3 (subtopic labeled as integrated care and education = 70% of the total) encompasses a broad range of works, including those by Badanta-Romero et al. (2021), Carpenter and Theeke (2018), Debiasi and Selleck (2017), Eche and Kline (2012), Elliott (2018), Elliott & Patterson (2017), Estevan and del Carmen Solano Ruíz (2017), Phelps and Johnson (2004), L. Purnell (1999, 2001) Rodriguez et al. (2014), Romanello & Holtgrefe (2009), Sasnett et al. (2010), and Škorničková and Moravcová (2018). This cluster integrates studies focusing on Integrated Care Practices and Patient Education, showcasing a diverse thematic emphasis.
Cluster 4 (subtopic labeled as holistic and culturally sensitive care = 10% of the total) includes studies by Aksoy Derya et al. (2022) and Yalcin Gursoy and Tanriverdi (2020), both centered on Comprehensive Care and Cultural Sensitivity. This cluster aligns closely with certain methodological and topical aspects, emphasizing comprehensive care approaches with a focus on cultural sensitivity.
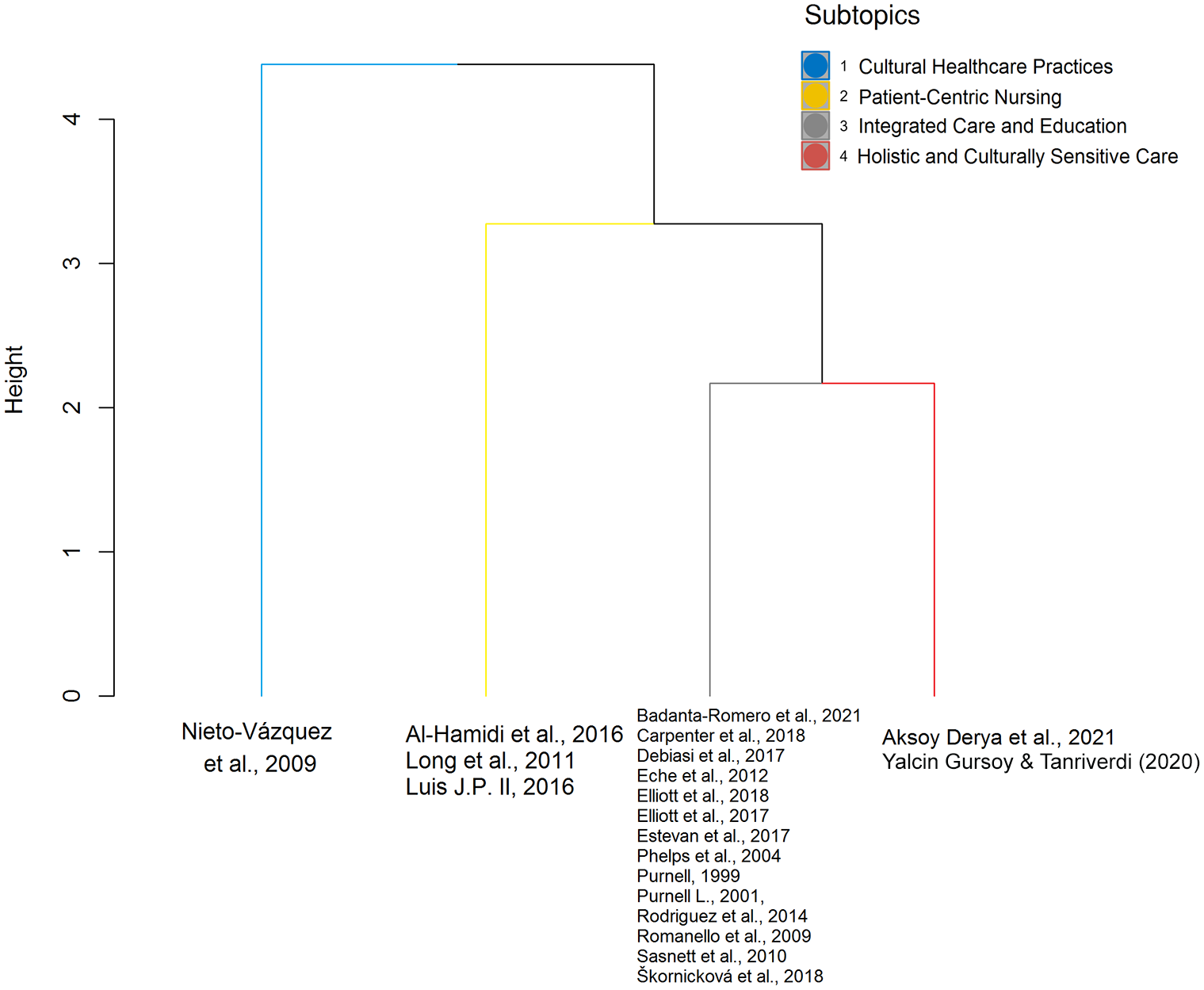
Dendrogram of K-Means Clustering.
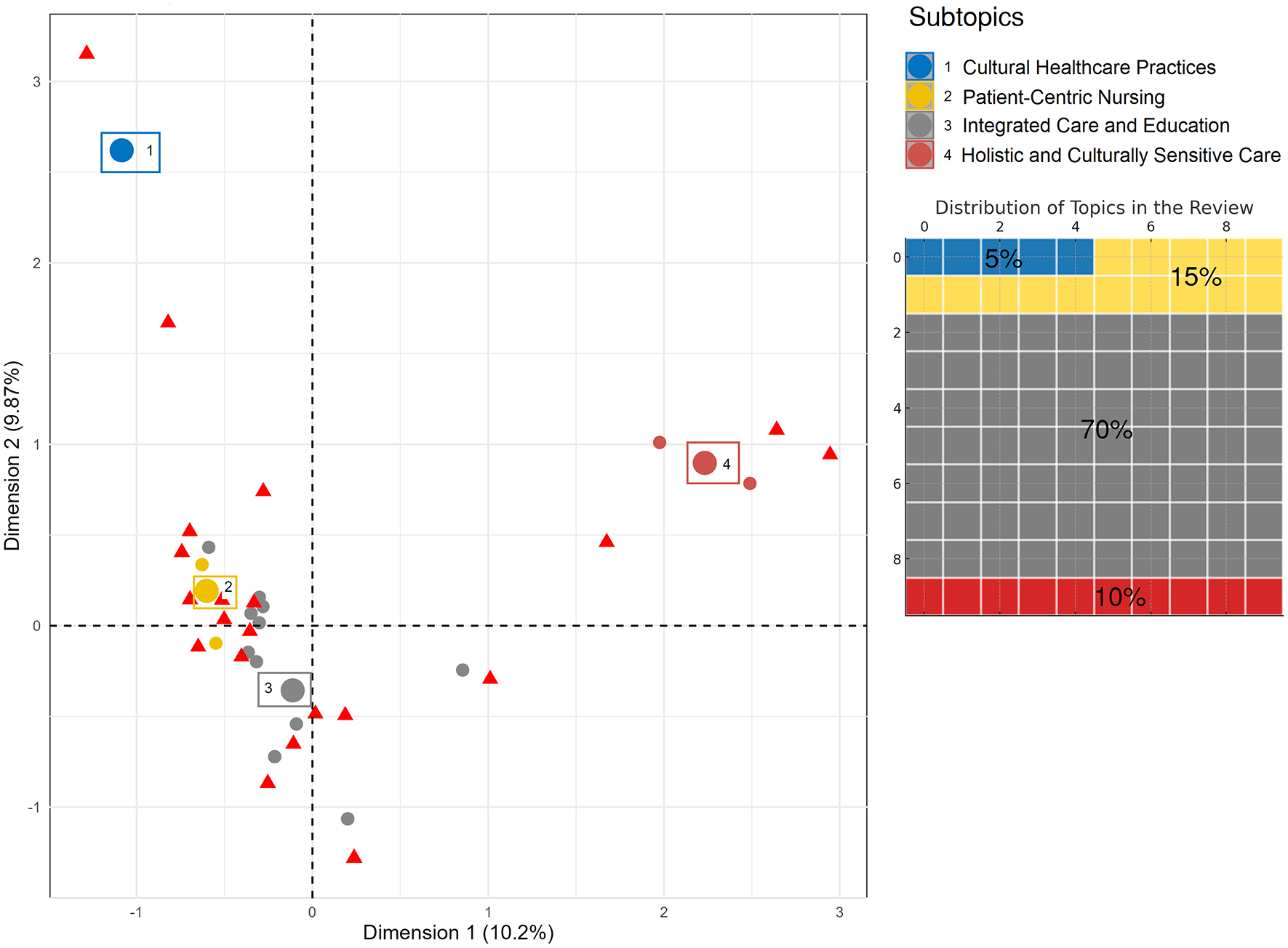
MCA of Subtopics Identified With K-Means Clusters.
Figure 4 further visualizes these clusters within the context of the MCA biplot. The biplot reveals how the studies, represented by different colors, are distributed across two dimensions of the MCA. This plot confirms the separation identified in the dendrogram and provides insights into the relative positions of the studies within the MCA space. The alignment of clusters (subtopics) with specific topics and variables, such as the year of publication, country, and study design, helps in understanding the thematic and methodological coherence within each cluster. Cluster 1 (Cultural health care practices) is closely associated with studies focusing on “cultural competence in health care.” In contrast, Cluster 2 (Patient-centric nursing) and Cluster 4 (Holistic and culturally sensitive care) are more aligned with “nursing interventions and patient relationships,” and Cluster 3 (Integrated care and education) presents overlaps between the two topics.
Consistent Patterns and Knowledge Gaps
The findings from this scoping review reveal several consistent patterns across the literature. Most studies emphasize cultural competence’s critical role in improving patient care and outcomes, particularly in diverse health care settings. This is evident in the high prevalence of studies focusing on the practical application of cultural competence in health care (40%) and nursing interventions (60%). Studies utilizing Purnell’s Model in health care settings, such as those conducted by Aksoy Derya et al. (2022) and Carpenter and Theeke (2018), consistently underscore the importance of cultural awareness and tailored care plans in enhancing patient outcomes. Similarly, studies focusing on nursing interventions and patient relationships, such as those by Debiasi and Selleck (2017) and Rodriguez et al. (2014), highlight the necessity of culturally competent training for nurses to address specific patient care needs.
However, significant knowledge gaps persist. While many studies address the implementation of Purnell’s Model, few provide longitudinal data to assess the long-term impact of cultural competence on patient outcomes (Aksoy Derya et al., 2022; Carpenter & Theeke, 2018; Debiasi & Selleck, 2017). In addition, the application of the model in nursing education remains poorly explored, with limited studies examining how well it prepares future health care professionals for diverse cultural environments. Furthermore, studies predominantly come from high-income countries (80%), highlighting a gap in research from middle- and low-income regions, where culturally competent care may face different challenges.
Discussion
This scoping review has mapped the literature on the application of Purnell’s Model for Cultural Competence within nursing practice and education, revealing critical themes and prevailing trends. The emerging themes from the literature encompass two differentiated topics confirmed by the MCA: (a) cultural competence in health care and (b) nursing interventions and patient relationships.
The first theme, “cultural competence in health care,” focuses on systematically implementing and assessing cultural competence frameworks within health care settings. Studies demonstrate that these frameworks improve patient care, foster trust, and enhance the provision of culturally congruent health care services (Aksoy Derya et al., 2022; Carpenter & Theeke, 2018; Elliott & Patterson, 2017; Estevan & del Carmen Solano Ruíz, 2017; Long, 2011; Louis, 2016; Nieto-Vázquez et al., 2009; Škorničková & Moravcová, 2018). For example, two studies (Carpenter & Theeke, 2018; Estevan & del Carmen Solano Ruíz, 2017) show how culturally competent care strengthens patient–provider rapport, improving adherence to treatment and patient satisfaction.
Despite their importance, there is considerable variability in how these frameworks are applied across health care contexts, with most studies (80%) emerging from high-income countries. This regional focus raises questions about the adaptability of these models in low- and middle-income settings, and there remains a gap in longitudinal studies that assess the long-term impact of sustained cultural competence interventions on patient outcomes (Aksoy Derya et al., 2022).
The gaps in longitudinal research and the overrepresentation of high-income countries in the literature likely stem from several systemic factors. First, focusing on short-term studies may reflect resource constraints or funding models prioritizing immediate, measurable outcomes over long-term evaluation (Gopalkrishnan, 2021). In low- and middle-income settings, cultural competence frameworks may be underdeveloped due to limited institutional resources, training infrastructure, or differing health policy priorities. In addition, health care systems in these regions may face broader structural challenges, such as limited access to continuous professional development, which hinders the consistent application and evaluation of cultural competence over time (Moeti et al., 2022). Addressing these gaps will require targeted efforts, including investment in longitudinal studies and adaptations of cultural competence frameworks to suit the unique needs and constraints of low- and middle-income countries. Future research should explore how culturally adaptable models could be implemented globally, ensuring that cultural competence frameworks are both scalable and sustainable across diverse health care contexts.
The second theme, “nursing interventions and patient relationships,” highlights the practical application of cultural competence in day-to-day nursing care. Culturally tailored nursing interventions are shown to enhance the quality of care by addressing patients’ diverse needs and preferences (Al-Hamidi, 2016; Badanta-Romero et al., 2021; Debiasi & Selleck, 2017; Eche & Kline, 2012; Elliott, 2018; Phelps & Johnson, 2004; L. Purnell, 1999, 2001; Rodríguez et al., 2014; Romanello & Holtgrefe, 2009; Sasnett et al., 2010; Yalcin Gursoy & Tanriverdi, 2020). For instance, studies by Al-Hamidi (2016) and Badanta-Romero et al. (2021) underscore the value of cultural sensitivity in improving patient satisfaction and outcomes. However, many studies also point to barriers that nurses face in implementing these interventions, such as institutional constraints, lack of training, and insufficient resources (Ličen & Prosen, 2023). While the literature acknowledges the significance of culturally tailored care, there is limited research tracking how nurses’ cultural competence evolves over time through ongoing education and professional development, highlighting an area for future research (Walkowska et al., 2023).
In addition, this review identified four distinct subtopics through k-means clustering, providing a more nuanced understanding of the literature. These subtopics—Cultural health care practices (n = 1, 5%), Patient-centric nursing (n = 3, 15%), Holistic and culturally sensitive care (n = 2, 10%), and Integrated care and education (n = 14, 70%)—allow for a more granular analysis of the literature and show how Purnell’s Model is applied in various settings.
“Cultural health care practices” reflect the growing global recognition of structured approaches to enhance patient care in culturally diverse settings (Nieto-Vázquez et al., 2009). This subtopic closely aligns with the broader theme of cultural competence, highlighting the systematic application of these frameworks across various clinical contexts. Such practices ensure that health care providers are equipped to meet the unique needs of culturally diverse populations, promoting equitable care and reducing health disparities across different patient groups.
“Patient-centric nursing” emphasizes the importance of patient-centered care that prioritizes individual cultural needs and preferences (Al-Hamidi, 2016; Long, 2011; Louis, 2016). This subtopic underscores that cultural competence is not just about broad frameworks but also about tailoring care to each patient’s unique background. However, literature reveals that institutional support, training, and resources are often insufficient to fully support the consistent application of patient-centric interventions (Magon et al., 2023).
“Holistic and culturally sensitive care” expands patient-centered approaches to include emotional and spiritual well-being within a cultural context (Aksoy Derya et al., 2022; Yalcin Gursoy & Tanriverdi, 2020). This approach integrates cultural sensitivity into broader, more comprehensive health care practices, as seen in Aksoy Derya et al. (2021). However, challenges remain in standardizing these practices due to the diverse cultural contexts in which they are applied (Yalcin Gursoy & Tanriverdi, 2020).
“Integrated care and education” explores the intersection of clinical practice and nursing education, showing how cultural competence frameworks could be embedded into nursing curricula to prepare future health care professionals for diverse environments (Badanta-Romero et al., 2021; Carpenter & Theeke, 2018; Debiasi & Selleck, 2017; Eche & Kline, 2012; Elliott, 2018; Elliott & Patterson, 2017; Estevan & del Carmen Solano Ruíz, 2017; Phelps & Johnson, 2004; L. Purnell, 1999, 2001; Rodríguez et al., 2014; Romanello & Holtgrefe, 2009; Sasnett et al., 2010; Škorničková & Moravcová, 2018). While educational interventions are increasingly incorporated into academic curricula, there is a need for more research on how well these programs translate into effective clinical practice after graduation (Tehee et al., 2020; Vangone et al., 2024).
An important intersection exists between “patient-centric nursing” and “holistic and culturally sensitive care.” Both emphasize tailoring care to meet individual patient needs but differ in scope. Patient-centric care focuses on addressing patients’ unique preferences and expectations, while holistic care expands this approach by encompassing physical, emotional, and spiritual well-being within a cultural context (Dossey & Keegan, 2013). These two approaches complement each other and, when integrated, offer a comprehensive care model that is both culturally sensitive and patient-centered. For instance, a culturally tailored intervention, such as respecting a patient’s dietary preferences, can also address spiritual and emotional well-being as part of a holistic care plan (L. D. Purnell, 2021).
To fully integrate cultural competence frameworks into nursing practice, future research must move beyond theoretical discussions and focus on practical, evidence-based strategies that can be consistently applied in everyday care (Campinha-Bacote, 2002; L. Purnell, 2002). The reviewed studies suggest that the successful implementation of Purnell’s Model requires developing culturally tailored protocols co-designed with input from patients and health care professionals to ensure relevance and practicality (Cuellar, 2024; Harazneh et al., 2024). For example, operationalizing the 12 domains of Purnell’s Model into specific nursing workflows—such as using culturally adapted assessment tools or guidelines for communication and family involvement—could enhance patient care (Phelps & Johnson, 2004; L. Purnell, 2000; Qin & Chaimongkol, 2021; Rodríguez et al., 2014; Romanello & Holtgrefe, 2009). These strategies improve nurse–patient interactions and help institutionalize cultural competence as a core component of nursing practice. Future research should evaluate the long-term outcomes of these practical approaches and explore how they could be scaled across diverse health care settings (Albanesi et al., 2022; Vangone et al., 2024).
Limitations
This review has some limitations. One limitation of this review is the potential for publication bias, where studies with positive outcomes regarding cultural competence interventions may be more likely to be published than those with null or negative results. This phenomenon could skew our understanding of the feasibility and effects of these interventions. Another limitation is the heterogeneity of the included studies in terms of design, population, and intervention type, which makes direct comparisons and synthesis of results challenging. In addition, this scoping review did not focus on assessing the quality of the included articles to keep the focus on the exploratory nature of the research question aimed to map literature and describe trends as a whole instead of rating the quality of evidence. The absence of a critical appraisal of individual sources of evidence is acceptable in scoping reviews and represents an intrinsic limitation of this approach (Peters et al., 2021).
Strengths
One of the key strengths is the innovative use of LDA, MCA, and k-means clustering to analyze and categorize the data, playing the role of data mining techniques. This approach allowed us to identify distinct subtopics within the literature, providing a more nuanced understanding of the themes and trends in cultural competence. Data mining analytics goes beyond traditional qualitative synthesis by offering a data-driven way to uncover patterns and relationships among the studies, enhancing our analysis’s robustness and depth. Another strength of this review is its comprehensive scope, which includes studies from diverse geographic regions and methodologies. This broad inclusion allowed for a global perspective on the application of Purnell’s Model for Cultural Competence, highlighting both universal themes and region-specific challenges.
Conclusion
This scoping review highlights the critical importance of cultural competence in enhancing health care delivery and educational outcomes. Using data mining analytical techniques, we identified distinct subtopics within the literature that provide nuanced insights into the application and impact of Purnell’s Model for Cultural Competence. The findings emphasize the need for comprehensive and tailored cultural competence training programs in clinical settings, which are crucial for improving patient outcomes and reducing health disparities. In educational settings, integrating cultural competence frameworks into nursing curricula is essential for preparing future health care professionals to serve diverse patient populations effectively.
The findings of this review offer valuable directions for future work for researchers, educators, and clinicians. Researchers are encouraged to explore further the practical implementations of cultural competence frameworks and their long-term impacts on health care outcomes. Educators should continue to refine and integrate cultural competence into their curricula, utilizing diverse and interactive teaching methods. Clinicians are urged to adopt and advocate for comprehensive cultural competence training within their organizations, continuously assessing and improving these programs to meet the evolving needs of diverse patient populations.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-docx-1-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Supplemental Material
sj-docx-2-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-docx-2-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Supplemental Material
sj-docx-3-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-docx-3-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Supplemental Material
sj-docx-4-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-docx-4-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Supplemental Material
sj-docx-5-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-docx-5-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Supplemental Material
sj-xlsx-6-tcn-10.1177_10436596251323273 – Supplemental material for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics
Supplemental material, sj-xlsx-6-tcn-10.1177_10436596251323273 for Integrating Cultural Competence in Nursing: A Scoping Review of Purnell’s Model in Clinical Practice and Education With Data Mining Analytics by Rosario Caruso, Stefano Terzoni, Maura Lusignani, Ester Varano, Francesco Pittella, Viktorija Xharra, Sara Carrodano, Greta Ghizzardi, Gianluca Conte, Arianna Magon, Maddalena De Maria, Gennaro Rocco and Alessandro Stievano in Journal of Transcultural Nursing
Footnotes
Authors Contributions
Study design: R.C., A.S.; Data collection: E.V., V.B., S.C., A.M.; Data analysis: R.C., G.G., G.C.; Study supervision: A.S., M.L., G.R.; Manuscript writing (draft): all authors; Manuscript writing (editing and revision): all authors; Critical revisions for important intellectual content: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by “Ricerca Corrente” funding from the Italian Ministry of Health to IRCCS Policlinico San Donato.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.