
Abstract
Introduction:
Bereavement disclosure in dementia care presents ethical and cultural challenges in Japan.
Methods:
A cross-sectional survey was conducted with 25 family caregivers who had experience caring for a person with dementia and who had also experienced the death of a significant person, assessing attitudes toward disclosure and preferences for support.
Results:
About 80% supported disclosure, citing dignity and relational closeness. Non-disclosure was most often attributed to physical condition, confusion, unpredictable reactions, or professional advice. Younger caregivers favored internet-based support, whereas older caregivers preferred booklets, lectures, and family association services.
Conclusion:
Findings highlight ethical tension between dignity and avoidance of confusion, with relational and situational factors shaping decisions. Hybrid support models that combine asynchronous online resources with family association services may enhance accessibility and provide caregivers with sustained support in dementia care.
Introduction
Dementia is a progressive condition characterized by declining cognitive functions including memory and judgment, with prevalence increasing with age. The global number of people living with dementia is projected to reach approximately 139 million by 2050 (Pace et al., 2011). In Japan, where the proportion of older adults is among the highest worldwide, the number of persons with dementia continues to rise, with recent nationwide projections indicating that the prevalence among adults aged 65 and older may exceed 25% by 2035 (Nakahori et al., 2021), making this issue especially salient in the Japanese context. Communicating with persons with dementia can be challenging, particularly when conveying emotionally significant information such as the death of a family or close friend. Due to memory impairment, caregivers are often repeatedly asked about the deceased, facing the dilemma of whether to disclose the truth each time, which may result in psychological distress (Grief & Myran, 2006; Rentz et al., 2005).
Caregiver support has been shown to be beneficial not only at the time of bereavement disclosure but also from the early stages of caregiving (Kimura et al., 2024). Reducing information gaps and anxiety in the initial phase may help caregivers maintain psychological stability when later facing difficult situations, potentially alleviating dilemmas associated with bereavement disclosure. It has been reported that differences in values and perceptions between family members and care facility staff may complicate decisions regarding disclosure, and such cases are not uncommon (Berenbaum et al., 2017; Grief & Myran, 2006). These disagreements—for example, situations in which staff consider disclosure appropriate while family members do not—can create ethical tensions and practical challenges in determining what should be communicated and by whom. While situational judgment and family preferences are frequently cited as reasons for non-disclosure, other factors such as anticipated reactions of the person, institutional policies, and cultural background have not been systematically examined. Some studies suggest that persons with dementia exhibit diverse responses depending on their living environment, indicating that bereavement disclosure requires sensitive ethical and psychological consideration (Watanabe & Suwa, 2017).
Grief is shaped by social relationships and cultural contexts (Rosenblatt, 2008; Worden, 2011). Given that Japan has distinct cultural norms surrounding family roles, emotional expression, and end-of-life communication, research grounded in the Japanese cultural and ethical context is essential. Most existing research has focused on relatively homogeneous Western populations, highlighting the need for studies in diverse cultural contexts (Werner et al., 2013). Against this background, the present study aimed to explore factors influencing the disclosure of bereavement information to persons with dementia in Japan, examine the challenges caregivers may face, and identify potential support strategies.
Method
This study employed a cross-sectional survey design using a self-administered questionnaire (Sharma et al., 2021). This study was approved by the ethics committee of the affiliated university (Approval No. Kyo 33-41B) and was conducted in accordance with the tenets of the Declaration of Helsinki. Participants were informed of the study’s purpose, methods, anonymity, and voluntary nature. Consent was implied through the returning of mailed questionnaires or the submission of web responses.
Participants
Participants were family caregivers residing in Japan who had experience supporting persons with dementia through the bereavement of important individuals such as family members, relatives, or close friends. Eligibility criteria for persons with dementia were as follows:
Having experienced the death of a significant person,
Having been diagnosed with dementia prior to the bereavement experience, and
Being aged 65 years or older.
The severity of dementia was classified according to the Ministry of Health, Labour and Welfare’s scale for activities of daily living (Levels I–IV), with corresponding Mini-Mental State Examination (MMSE) scores as follows: Level I (MMSE > 24), Level II (MMSE 23–19), Level III (MMSE 18–10), and Level IV (MMSE 9–0) (Sugishita et al., 2018).
Recruitment
Five dementia family associations in the Kanto region were approached. However, only Branch A indicated that they had eligible participants, and all participants were therefore recruited through this branch, with which the researchers had an existing connection. Questionnaires were mailed to all 328 members, with an anticipated response rate of approximately 10% based on prior studies. Responses were accepted either online or by mail; mailed responses were requested to omit personally identifiable information.
Data Collection
Data were collected from September to December 2021 using a self-administered questionnaire developed from previous studies (Johansson & Grimby, 2013; Low et al., 2019; Pace et al., 2011; Watanabe & Suwa, 2017) and existing knowledge. A pilot test with 15 health care professionals and family caregivers confirmed clarity. Reliability was assessed using Cronbach’s alpha: bereavement disclosure items = .89; support information items = .80, indicating high internal consistency. Three co-authors (AW, YH, MT) independently reviewed procedures to ensure consistency and reached consensus.
The questionnaire comprised three domains: (a) Demographics: caregiving duration, support experience, dementia type and severity, relationship to the person (Table 1). (b) Perceptions of Bereavement Disclosure: eight items rated on a 4-point Likert-type scale, reverse-coded so that higher scores indicated more positive attitudes toward disclosure. Items included reasons for non-disclosure, such as “not telling because the person would be saddened” and “not telling due to unpredictable reactions.” An even-numbered scale was used to avoid neutral bias and clarify the respondent’s stance (Table 2). (c) Support Information Preferences: experience and preferences regarding sources of caregiving support. Online responses were automatically digitized. Paper-based responses were manually entered into an electronic database. All data were anonymized and securely stored.
Demographic and Clinical Characteristics of Family Caregivers and Bereaved Older Adults With Dementia.
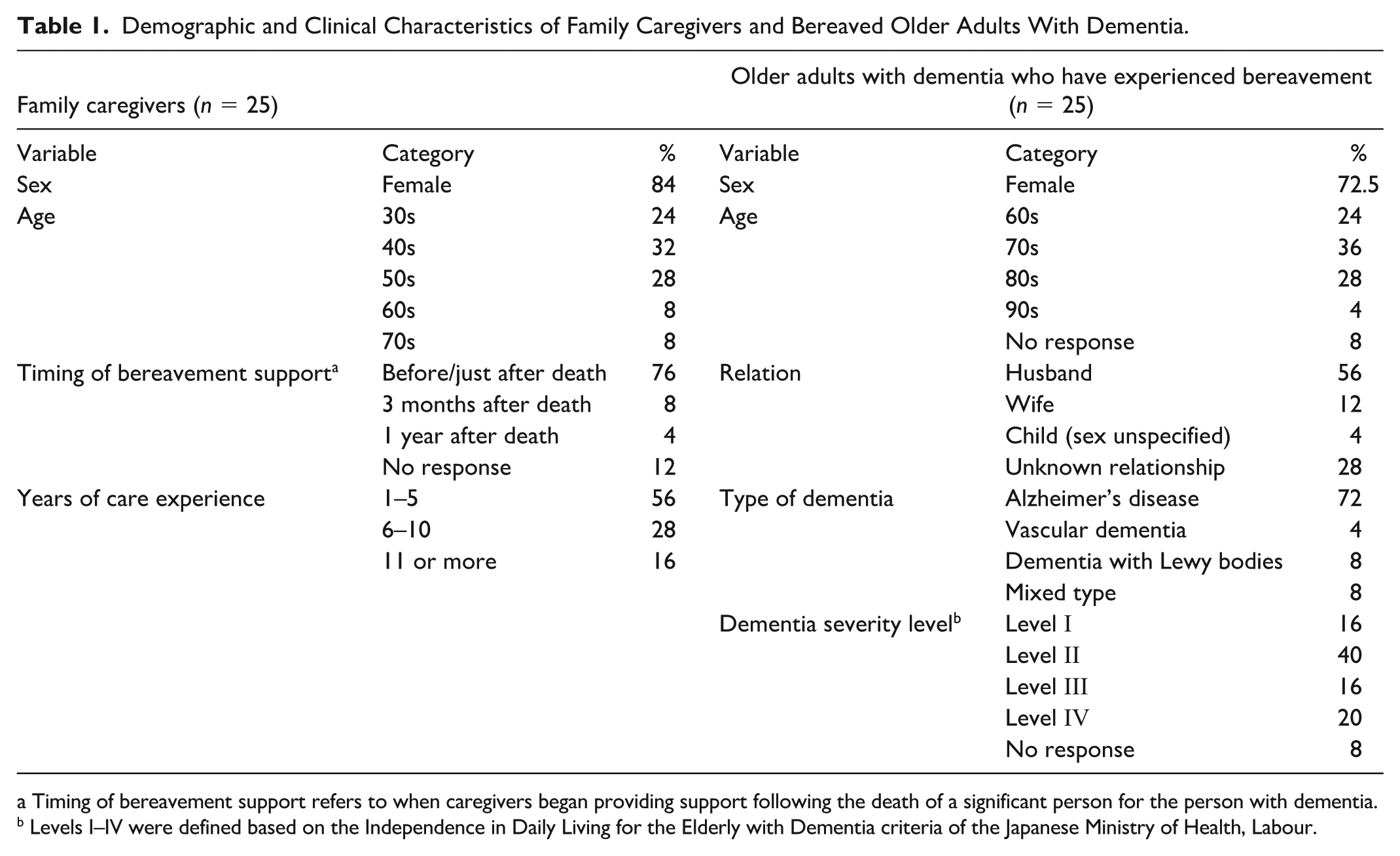
Timing of bereavement support refers to when caregivers began providing support following the death of a significant person for the person with dementia. b Levels I–IV were defined based on the Independence in Daily Living for the Elderly with Dementia criteria of the Japanese Ministry of Health, Labour.
Reasons for Non-Disclosure of Bereavement to Older Adults With Dementia (Questionnaire Items).
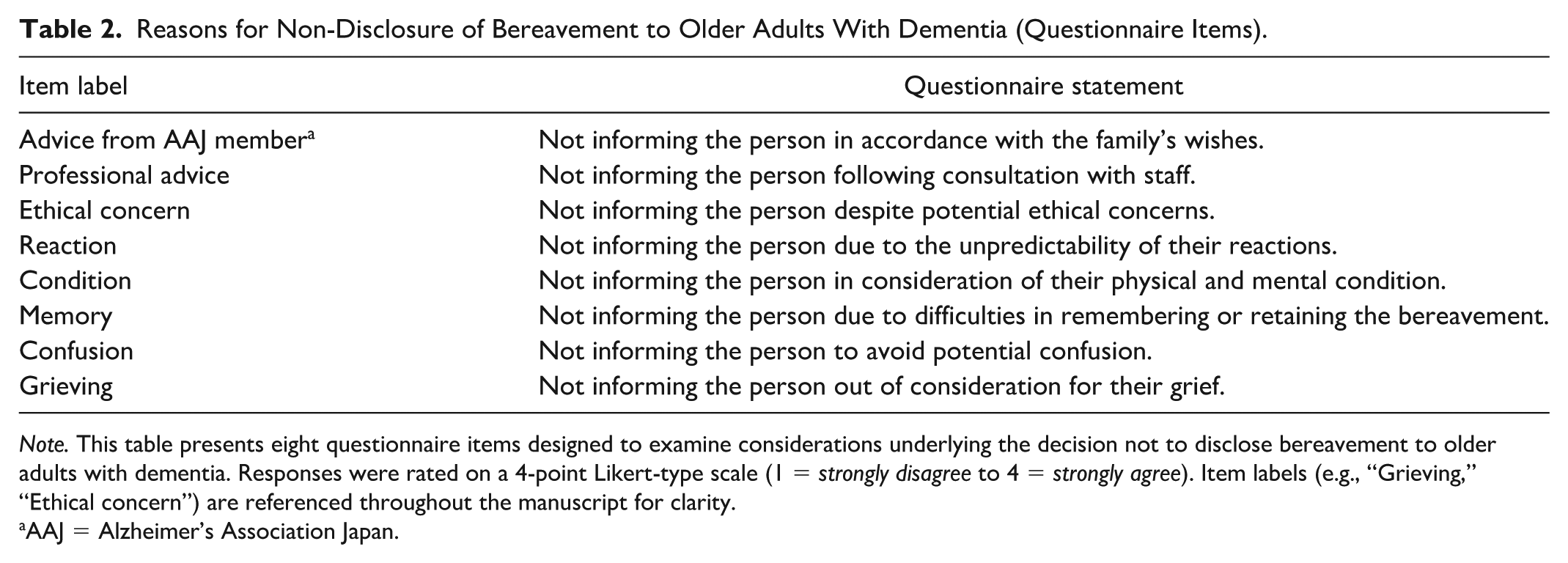
Note. This table presents eight questionnaire items designed to examine considerations underlying the decision not to disclose bereavement to older adults with dementia. Responses were rated on a 4-point Likert-type scale (1 = strongly disagree to 4 = strongly agree). Item labels (e.g., “Grieving,” “Ethical concern”) are referenced throughout the manuscript for clarity.
AAJ = Alzheimer’s Association Japan.
Data Analysis
Of the 328 distributed questionnaires, 36 were returned. Six with substantial amounts of missing data and five from individuals without grief support experience were excluded, resulting in 25 valid responses (effective response rate: 7.6%, validity rate: 69.4%).
Reasons for non-participation could not be determined due to anonymity, but time constraints and lack of interest were considered plausible factors. Group comparisons were conducted using chi-square tests, focusing on bereavement support experience. A post hoc power analysis was conducted using G*Power 3.1. Assuming a medium-to-large effect size (w =0.5), α = .05, df = 5, and a total sample size of 25, the achieved power was 0.45. Given the rarity of the target population and the ethical considerations involved, the sample size was limited despite efforts to recruit more participants (Faul et al., 2009).
Groups were classified as follows: (a) Age (younger adults: 30–50s; older adults: 60+), (b) Support initiation timing (short-term: before/immediately after bereavement; long-term: 6 months–2+ years), (c) Relationship (spouse vs. non-spouse), (d) Dementia severity (mild: Levels I–II; moderate/severe: Levels III–IV), and (e) Dementia type (Alzheimer’s disease [AD] vs. non-AD). Bereavement disclosure was categorized as “disclose” versus “withhold” and support preferences as “prefer to use” versus “prefer not to use.” Chi-square tests and effect sizes (r) were calculated using IBM SPSS Statistics ver.28.0, with significance set at p < .05.
Results
Participant Characteristics
Table 1 presents the characteristics of the family caregivers and the individuals with dementia in their care. The caregiver’s relationship to the person with dementia was recorded from the latter’s perspective. Female caregivers comprised 84% of respondents, with a particularly high proportion among the younger age group (30s–50s). In contrast, the older age group (60s–70s) showed a slightly higher proportion of male caregivers.
Caregiving duration was distributed as follows: 57% had provided care for 1 to 5 years and 44% for 6 to 11 years, indicating inclusion of both short- and long-term caregivers. Regarding dementia type, approximately 70% of individuals had AD and 10% had vascular dementia, consistent with the distribution of dementia subtypes in Japan (Japanese Society of Neurology, 2017). Approximately 60% of the deceased were spouses, a pattern consistent with bereavement trends among older adults in Japan (Statistics Bureau & Ministry of Internal Affairs and Communications, 2021). Taken together, while the rarity of eligible participants must be acknowledged, the sample was representative of the population.
Analytical Findings
Bereavement Disclosure
Figure 1 illustrates the distribution of responses to eight items concerning disclosure of bereavement to persons with dementia. Approximately 80% of respondents indicated that they “disclosed,” suggesting that disclosure tendencies were common. Significant differences were observed only in relation to the timing of support in ethical matters (p < .001). Caregivers involved “before or immediately after bereavement” were more likely to disclose. They tended to reject the option indicating that disclosure was ethically problematic and therefore withheld from the person with dementia. In contrast, caregivers who became involved 6 months or more after bereavement tended to choose non-disclosure. Those who became involved after 6 months but nevertheless opted for disclosure were limited to long-distance caregivers. No significant differences were found for other variables, including dementia subtype, severity, gender, caregiving duration, and relationship.
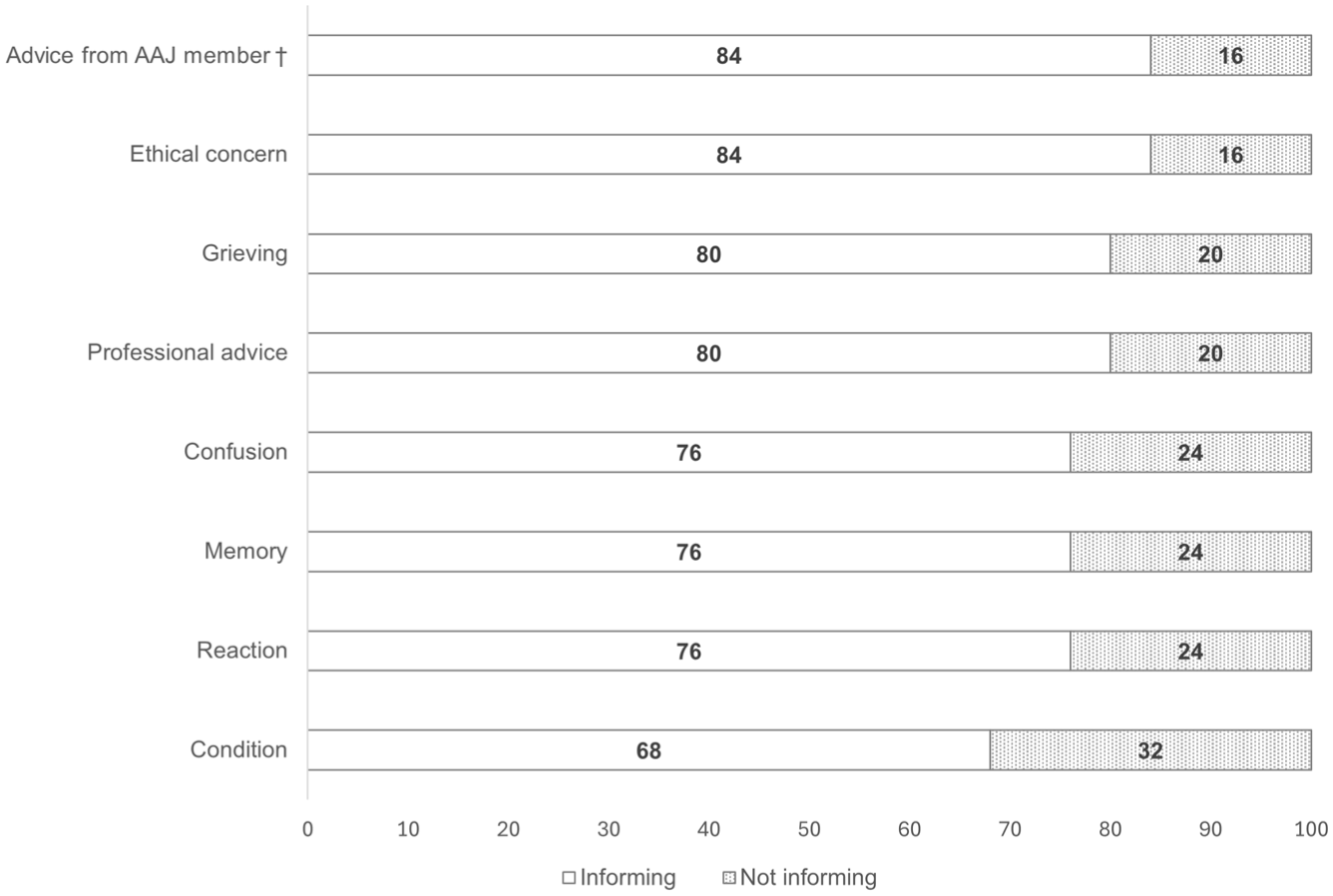
Reasons for Not Disclosing Bereavement to Older Adults With Dementia.
Free-text responses included statements such as: “If we consider the person as a dignified individual, the truth should not be hidden, and a way to convey it should be found” and “Disclosure was necessary because the person repeatedly asked.” Reasons for non-disclosure most frequently cited “physical condition,” followed by “concerns about confusion,” “unpredictable reactions,” and “professional advice,” each occurring at similar frequencies. Examples included: “I chose not to disclose because the person became confused and quickly forgot,” “I refrained from disclosure due to concerns about unpredictable reactions,” and “Although aware of ethical issues, I withheld disclosure.” Fourteen percent of respondents acknowledged that they refrained from disclosure despite recognizing ethical concerns. One caregiver wrote: “I had to make the decision not to disclose alone, and it weighed heavily on me.”
Preferences for Information Sources
Figure 2 shows preferences regarding sources of caregiving support information. Attitudes toward internet-based support differed significantly among caregivers of persons with mild dementia, χ2(1) = 8.77, p = .003. This tendency was particularly pronounced among caregivers in their 30s to 50s. Among caregivers in their 60s to 70s, similar tendencies were observed but were not statistically significant, χ2(1) = 3.18, p = .075.
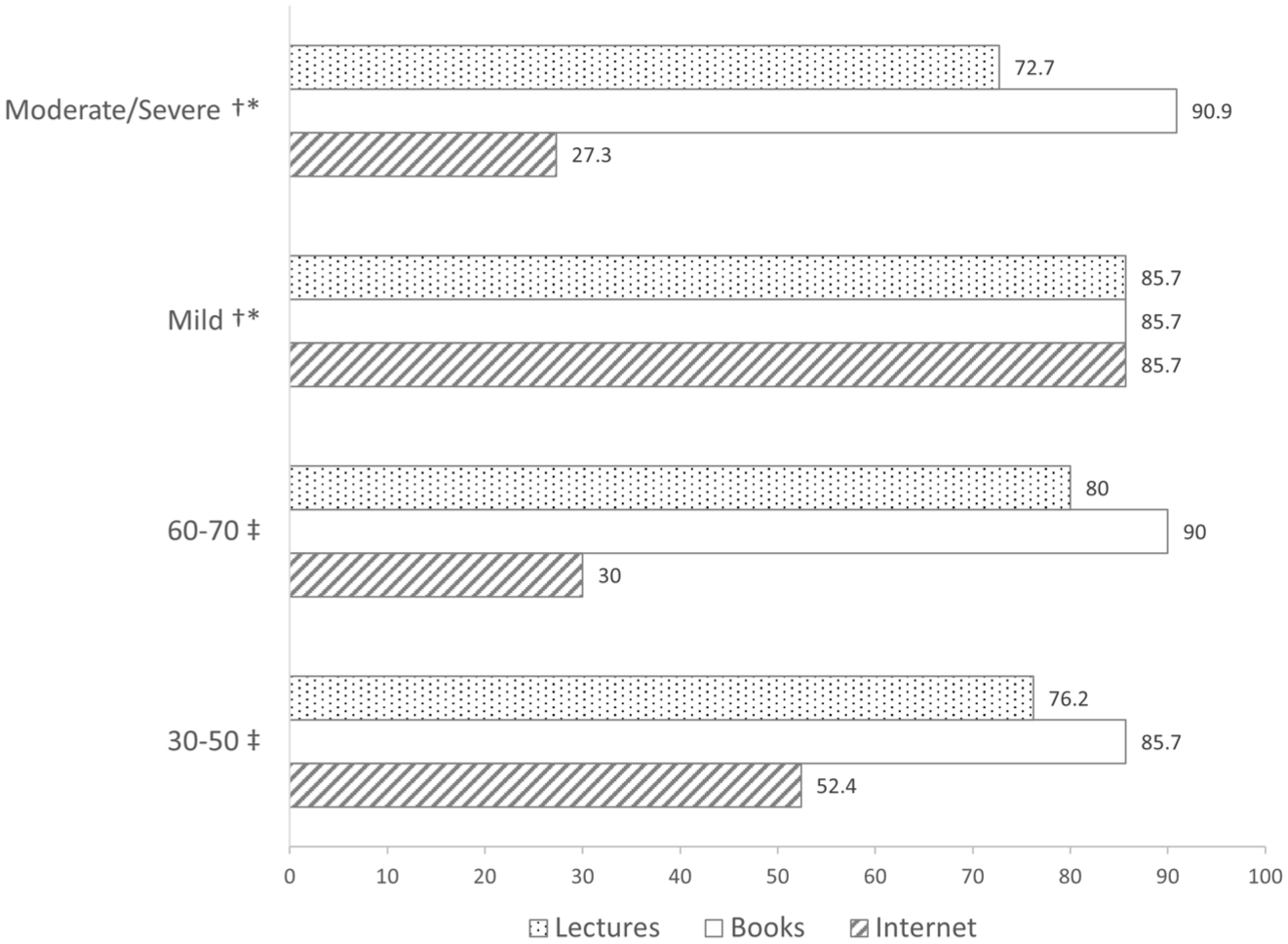
Preferences for Support Information Sources by Age Group and Dementia Severity.
By contrast, printed materials and lecture-style support consistently received high levels of endorsement regardless of dementia severity or caregiver age, with no significant differences observed. Notably, older caregivers continued to express interest in face-to-face support. Free-text responses highlighted practical constraints, such as: “I would like to attend lectures, but caregiving responsibilities make it difficult to go out.”
Discussion
Disclosure Trends and Influencing Factors
Approximately 80% of family caregivers supported bereavement disclosure to people with dementia, contradicting the initial hypothesis that caregivers tend to conceal such information. This finding is consistent with previous studies (Berenbaum et al., 2017; Dubois et al., 2016), suggesting a cross-cultural inclination toward disclosure. While earlier research identified memory impairment as a primary reason for non-disclosure (Grief & Myran, 2006; Rentz et al., 2005), only 24% of respondents in this study cited memory problems. The most frequent reasons for non-disclosure were physical condition, concerns about confusion, unpredictable reactions, and professional advice. These results indicate that disclosure decisions are shaped by a complex interplay of physical, psychological, and social factors.
Free-text responses revealed that decisions were influenced not only by ethical principles but also by caregivers’ living arrangements and relational closeness. This aligns with Nolan’s relationship-centered care model (Nolan et al., 2002) and Kitwood’s concept of personhood (Michel & Agnelli, 2015). In Western contexts, bereavement disclosure is typically guided by principles of individual autonomy and truth-telling, which emphasize the person’s right to know (Beauchamp, 2010; Worden, 2011). By contrast, Japanese caregiving practices are shaped by communal values and a cultural tendency to restrain open discussion of death (Yoshikawa, 2022). Caregivers often prioritize relational harmony and the prevention of confusion, viewing protection from distress as an expression of care. These contrasts suggest that while Nolan’s and Kitwood’s models are applicable across cultures, their implementation in Japan must account for relational decision making and the coexistence of communal and individually oriented values.
Compared with diagnostic disclosure, which is mainly based on cognitive status (Low et al., 2019), bereavement disclosure was strongly influenced by situational factors such as co-residence and timing of caregiving involvement. In cases of severe dementia, non-disclosure was often chosen based on the judgment that understanding was difficult. Caregivers who were involved early tended to emphasize dignity and responsibility, while those who became involved later prioritized avoiding confusion. Co-resident caregivers often judged non-disclosure as a rational choice based on their intimate knowledge of the patient’s condition, whereas non-co-resident caregivers were more likely to adopt values external to the caregiving relationship and lean toward disclosure. Ethical tension between respecting dignity and avoiding confusion was evident, reflecting the coexistence of values in the Japanese context.
Preferences for Support
Caregivers of younger age groups and those caring for persons with mild dementia showed a marked preference for internet-based support, reflecting flexible time management and information-seeking skills (Statistics Bureau & Ministry of Internal Affairs and Communications, 2021). Older caregivers did not express rejection, indicating potential receptivity. Free-text responses highlighted barriers such as difficulty leaving home due to caregiving responsibilities. On-demand and asynchronous online support can help caregivers learn flexibly and reduce stress (Blanka et al., 2019; Lim, 2021). Combining online resources with family association services suggests the effectiveness of multimodal support in addressing diverse needs and access disparities .(Lau et al., 2020; Stratton et al., 2017; Tsuyuki et al., 2021, 2024).
Cultural Background and Ethics
In Japanese culture, public dialogue about death and grief tends to be restrained, although diversity exists across generations, regions, and religious backgrounds (Yoshikawa, 2022). Nevertheless, about 80% of caregivers in this study supported bereavement disclosure, suggesting practical judgments that transcend traditional norms. The annual Obon festival provides a cultural framework for continuing bonds with the deceased, reflecting how mourning traditions sustain ongoing relationships and narrative reconstruction after loss (Neimeyer et al., 2011). Within this context, caregivers’ belief that “truth should be conveyed to respect dignity” resonates with Kitwood’s concept of personhood. Bereavement disclosure in Japan thus emerges not merely as information-sharing but as a relational process embedded in cultural traditions and evolving values.
Limitations and Strengths of the Study
This study has some limitations. First, the sample size was small (n = 25), which increases the risk of type II error and limits statistical power, thereby restricting the generalizability of findings. Second, participants were recruited from a single dementia family association, which may have introduced selection bias and reduced the cultural and experiential diversity of caregiving perspectives. Future studies should recruit from multiple regions and associations to enhance representativeness. Third, reliance on self-reported data raises the possibility of recall bias and social desirability effects.
Moreover, the relationship between caregivers and the deceased was not explicitly recorded, which may have led to classification ambiguity. Although significant differences were found in preferences for digital support, detailed data on digital technology usage were not collected, warranting further investigation in future studies.
Despite these limitations, the study offers valuable insights for clinical practice. It highlights the importance of communication decisions that are sensitive to relational contexts and the lived realities of caregivers.
Conclusion
This study found that most family caregivers supported bereavement disclosure, emphasizing dignity and relational involvement. Decisions were shaped by situational factors such as physical condition and professional advice. Younger caregivers preferred online resources, while older caregivers favored traditional formats. Hybrid support models may enhance accessibility and reduce caregiver burden.
Footnotes
Acknowledgements
We sincerely thank all participants for their valuable contributions to this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI, Grant Number JP20K19244.
Ethical Approval and Informed Consent
This study was approved by the Ethics Committee of the affiliated university (Approval No. Kyo 33-41B). Informed consent was obtained through the return of mailed questionnaires or submission of web responses.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Due to the sensitive nature of the data, they are not publicly available.