
Abstract
Introduction:
Tobacco use is disproportionately high among Arab Americans (AAs), with hookah normalized within social networks (SNs). Gaps remain in understanding how SNs, cultural norms, and migration-related identity shape tobacco use. This study examined how cultural norms, religion, and SNs are associated with tobacco use among AA adults.
Methods:
A cross-sectional survey of 178 Massachusetts-based AA adults assessed tobacco use, cultural attitudes, religiosity, and SN structural and compositional characteristics.
Results:
Current tobacco use was 51.69%, with hookah at 45.51%. Smoking, particularly hookah, was widely accepted within family and peer networks, with females reporting higher peer acceptability. Cultural norms, religious stance, and SN characteristics were significantly associated with tobacco use (p < .05).
Discussion:
Tobacco use reflected identity, belonging, and adaptation within migration contexts, serving as a sociocultural connector. Culturally congruent, gender-sensitive, and network-informed cessation strategies engaging families, peers, and faith communities are recommended to enhance intervention effectiveness among AAs.
Keywords
Introduction
Tobacco use remains a leading cause of preventable morbidity and mortality worldwide, accounting for over 7 million deaths annually (World Health Organization [WHO], 2025). Although smoking rates have declined in the United States, these gains are uneven, with persistent disparities among racial, ethnic, and immigrant populations (Centers for Disease Control and Prevention [CDC], 2024a). Arab Americans (AAs) are largely invisible in national health data due to racial and ethnic misclassification (Abuelezam et al., 2018, 2022), obscuring tobacco-related inequities, including disproportionate use, harms, and limited access to culturally congruent cessation resources (Al Suwaidi, 2016; El-Sayed et al., 2011; Merizian et al., 2021).
The AAs have elevated rates of cigarette and hookah use. Hookah is embedded in culturally normative practices emphasizing hospitality, social connection, and collective identity (Atrooz et al., 2024; Haddad et al., 2012; Rice, 2012) and is tied to socially sanctioned rituals symbolizing belonging and cultural continuity (Alzyoud et al., 2014; El-Shahawy & Haddad, 2015), reinforcing beliefs that it is less harmful despite comparable or greater toxicant exposure (American Lung Association [ALA], 2025; Grekin & Ayna, 2012). These misperceptions contribute to high social acceptability, particularly among AA youth who link hookah use to cultural pride and belonging (El-Hajj et al., 2017; Maziak et al., 2004). Tobacco use varies by gender, generation, and acculturation, with men reporting higher use (El-Hajj et al., 2017; Hamadeh et al., 2020; Nakkash et al., 2022), and women concealing use due to gendered expectations (Giuliani et al., 2012; Kassem et al., 2015). These patterns are reinforced within family and peer networks that transmit norms and model behavior (Athamneh et al., 2015).
Despite growing literature, gaps remain. Most studies emphasize individual behaviors and prevalence, with limited attention to the relational and cultural contexts in which tobacco use is initiated and maintained. Post-migration contexts by which norms, identity, and belonging shape tobacco use are rarely examined. Although SNs, particularly family, peer, and religious networks, are central to Arab life, their role in shaping tobacco norms and behaviors remains understudied, and individual behavior models inadequately capture AAs’ collectivist values and relational dynamics. Religiosity rooted in Islam and Christianity is an inconsistently examined influence. Teachings about health preservation and avoidance of harm may discourage smoking (Haddad & Corcoran, 2013); however, religiosity is often treated as an individual attribute rather than a socially embedded influence, limiting attention to gender and sociocultural variations.
Guided by Berkman et al.’s (2000) Social Network model, this study situates AAs’ tobacco use within macro-, meso-, and micro-level contexts. Cultural norms, religious beliefs, and migration experiences shape tobacco-related boundaries at the macro-level; family, peer, and religious networks transmit norms at the meso-level; and social support, influence, and modeling operate at the micro-level. Social Identity (Tajfel, 1974) and Acculturation theories (Berry, 1997, 2005) further frame tobacco use as identity negotiation and belonging in diasporic contexts. Together, these perspectives conceptualize tobacco use as a practice shaped by identity, migration, and relational ties. Fawcett and DeSanto-Madeya’s (2013) Conceptual–Theoretical–Empirical structure (see Figure 1) links theory to measurement through SN characteristics (e.g., size, kin composition, and members’ tobacco use) and individual attributes (e.g., gender), shifting focus from individual risk to social influences in understudied AA communities. This study examines how SN characteristics, cultural identity, norms, and religiosity shape tobacco use among AA adults, aligning with transcultural nursing’s emphasis on culturally grounded prevention and cessation strategies.
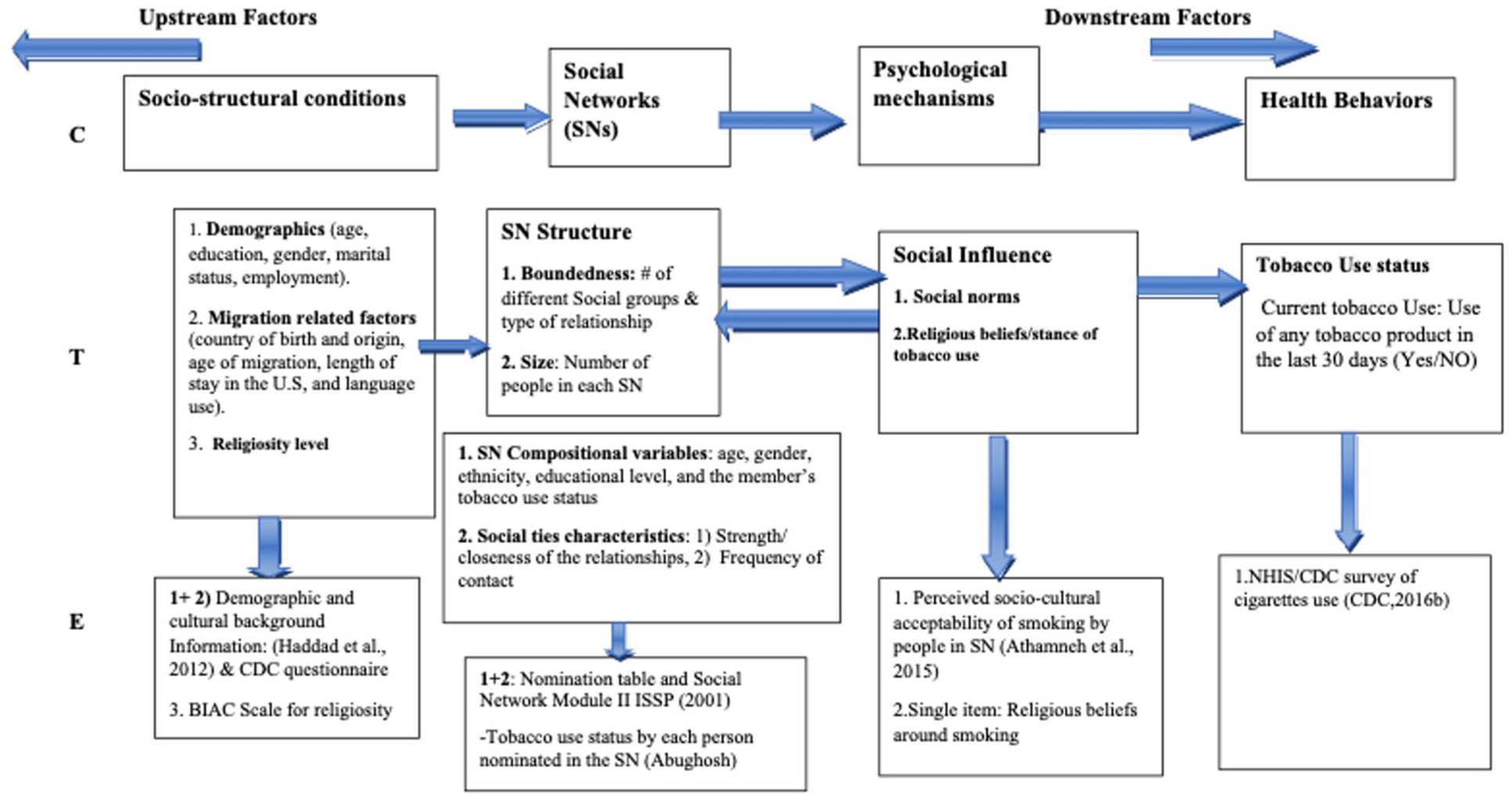
CTE Model Explaining Pathways Associations Between Social Network and Adult U.S. Arabs’ Tobacco Use.
Method
Ethical Considerations
The study was approved by the Institutional Review Board (IRB #2017176) after expedited review. Participants gave informed consent in person or by phone.
Study Design
Using cross-sectional, community-based data from AA adults in Massachusetts, this study applies Berkman et al.’s (2000) SN framework to examine how cultural beliefs, social ties, and structural and compositional features of SNs shape tobacco use, with particular attention to hookah use, gender differences, and religiosity.
Setting and Participants
A convenience sample of 178 AAs was recruited from mosques, churches, faith-based schools, outreach centers, and Middle Eastern businesses in Massachusetts. Bilingual flyers (Arabic/English) were distributed at recruitment sites. Eligible participants were ≥18 years old, of Arab descent, Massachusetts residents, and proficient in English or Arabic. Screening included birthdate, self-identified ethnicity, and nativity (self and parents). Surveys, administered via phone, face-to-face, or mail, assessed demographics, migration background, SNs, religiosity, social beliefs around tobacco, and tobacco use.
Survey Development and Translation
Adapted from validated tools in AA health studies, the survey was translated and back-translated by bilingual researchers. Cognitive testing with eight diverse community members helped refine wording related to religiosity and hookah use for cultural clarity and appropriateness.
Variables and Measures
Tobacco Use Status
Current tobacco use was defined as use of any tobacco product (e.g., cigarettes and hookah; CDC, 2017), within the past 30 days, consistent with the National Center for Health Statistics (NHIS, 1994). The survey included images of ten tobacco products to aid recall. Research indicates that among AA, hookah use may serve as an introduction to cigarette use and can be used either as a substitute for cigarettes or alongside them.
Social Network Composition
Based on Berkman’s framework, SN characteristics included structure (size and relationship type), composition (member age, gender, education, ethnicity, and tobacco use), and relationship quality (closeness, contact frequency; Berkman et al., 2000; Christakis & Fowler, 2008; Kennedy et al., 2015; Valente, 2010). Respondents nominated up to 25 individuals they could contact. Figure 2 illustrates the instrument that the first author designed to gather data on members’ traits, relational dynamics, and attributes. Each personal network was treated as a unit of analysis to examine the network’s structure and composition of each of the personal SN (ego). Networks were analyzed using averages and percentages, and these values were treated as attribute variables of the ego.
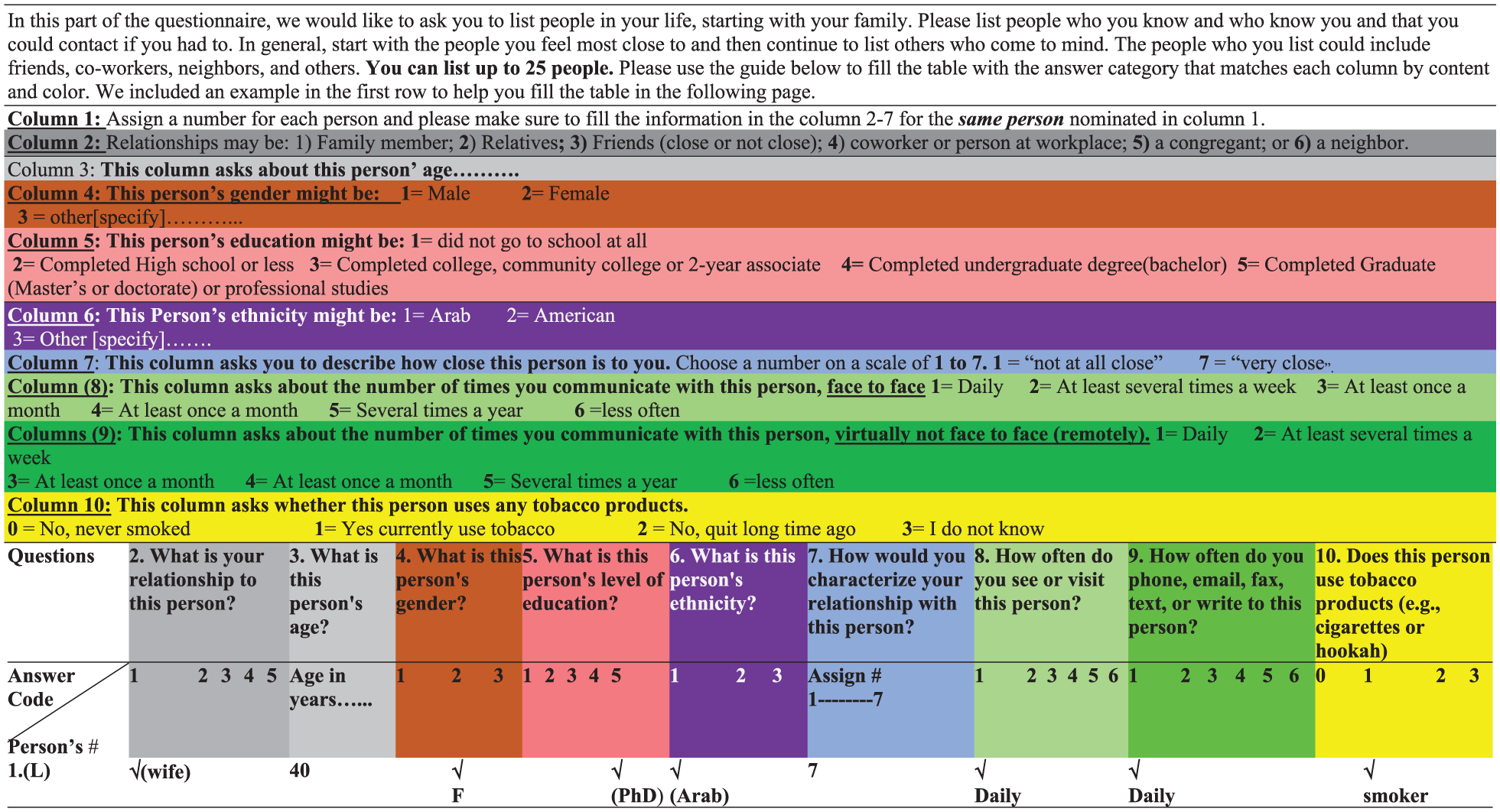
Social Network (SN) Nomination Table.
Cultural Attitudes
This variable was measured using a 7-item scale assessing the acceptability of seven types of tobacco across three social groups (family, Arab peers, and non-Arab peers) on a 0 to 3 scale (Athamneh et al., 2015). Total scores (0–21) were categorized as low, medium, or high acceptability. This approach captured product-specific cultural norms, particularly regarding hookah, and evaluated how tobacco use was perceived within different social environments, indicating the level of normalization or restriction. The sociocultural acceptability items have been used and validated among AAs (Athamneh et al., 2015, 2017); however, the psychometric properties were not reported.
Religious Beliefs
This variable was assessed using two approaches. First, religious stance on tobacco measured by a single item (5 = prohibits, 1 = actively encourages), adapted from studies with Muslim populations (Arfken et al., 2015; Islam & Johnson, 2003), without reported psychometric performance. Second, religiosity was assessed using the Belief to Action Scale (BIAC), a validated 10 to 100 scale measuring involvement in monotheistic traditions across diverse religious populations (Koenig, Nelson, et al., 2015; Koenig, Wang, et al., 2015; Wang et al., 2015). The BIAC scale demonstrates strong reliability, with high internal consistency (Cronbach’s alpha =.89), and excellent test–retest reliability (.92), and acceptable reliability in Arabic (Cronbach’s alpha = .80; Alakhdhair et al., 2016). Together, these measures explored how personal and institutional religiosity intersect with tobacco-related attitudes and practices.
Data Analysis
Descriptive statistics included mean, SD, frequency, and percentage. Differences between tobacco users and nonusers were tested using Student’s t-test or the Wilcoxon rank-sum test. Logistic regression examined associations with tobacco use (independent variable), including demographics, SN features, cultural attitudes, and religiosity. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported, significance at p < .05. Analyses were done in Stata 15.1 (StataCorp LLC, College Station, TX).
Results
Sample Characteristics
The final analytic sample included 178 AA adults residing in Massachusetts (Table 1), with a mean age of 41.39 years, and almost 45% female, married or cohabiting (69.1%), working (65.91%). The majority (87.08%) were foreign born, while the remainder were U.S.-born children of Arab immigrants, with the mean age of migration to the United States being 25.68 years. Over 69% completed at least a college education, most identified as Muslim (68.36%), mostly either from the Middle East (41.57%) or Gulf countries (17.98).
Sample Demographics, Migration-Related Variables, and Differences Between Tobacco Users and Nonusers.
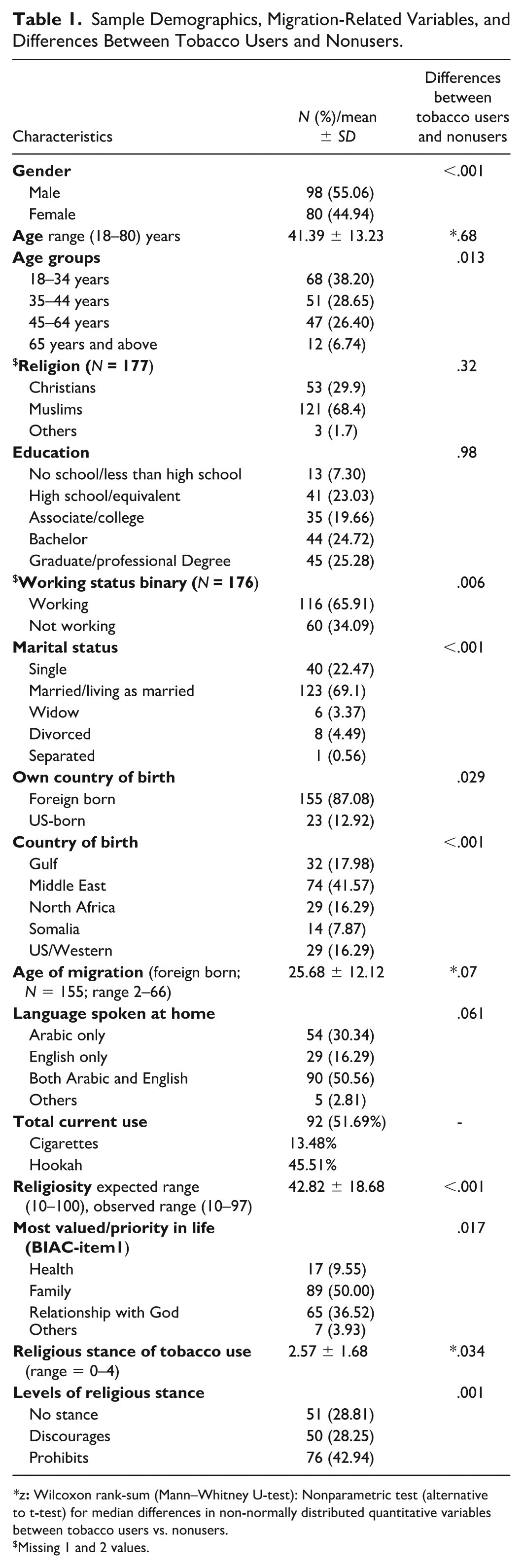
Missing 1 and 2 values.
Social and Cultural Factors
Cultural Perceptions and Norms Around Tobacco and Hookah Use
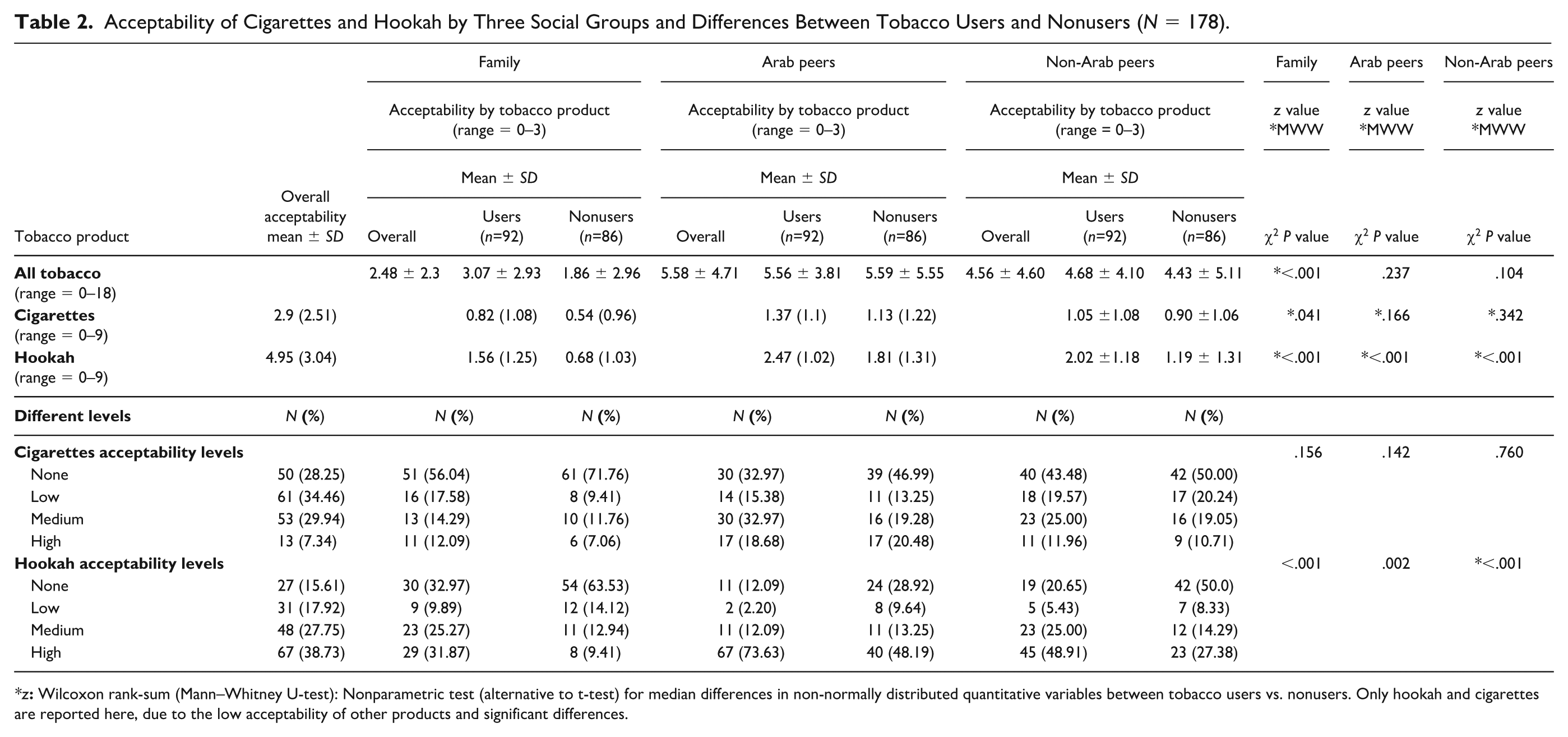
The highest overall acceptability of tobacco was reported among Arab peers, while only 14.94% of participants indicated no acceptability of tobacco. In contrast, 38.64% reported that their families did not accept tobacco use (Table 2). Hookah had the highest mean acceptability (mean = 4.95), followed by regular cigarettes (mean = 2.95), with 86% of the sample reporting medium to high peer acceptability of hookah, primarily from Arab peers. As shown in Table 3, increasing family sociocultural acceptability was associated with a higher likelihood of tobacco use, with those reporting any family acceptability significantly more likely to use tobacco compared to those whose families had no acceptability (OR = 3.51, 95% CI = 1.16–10.67, p = .027), indicating the central value of family attitudes on individuals’ behaviors. Acceptability from Arab and non-Arab peers also remained significantly associated with use; however, individuals reporting low peer acceptability were even more likely to use tobacco than those reporting medium or high acceptability. High acceptability of hookah was associated with over six times greater odds of use, while cigarette acceptability showed a marginally significant association. Females generally reported lower tobacco acceptability than males, with a significant gender difference in perceived Arab peer acceptability, highlighting gendered patterns of social influence.
Acceptability of Cigarettes and Hookah by Three Social Groups and Differences Between Tobacco Users and Nonusers (N = 178).
Associations Between Acceptability of Tobacco by Social Groups and Specific Tobacco Products, Religious Stance, and Current Tobacco Use.
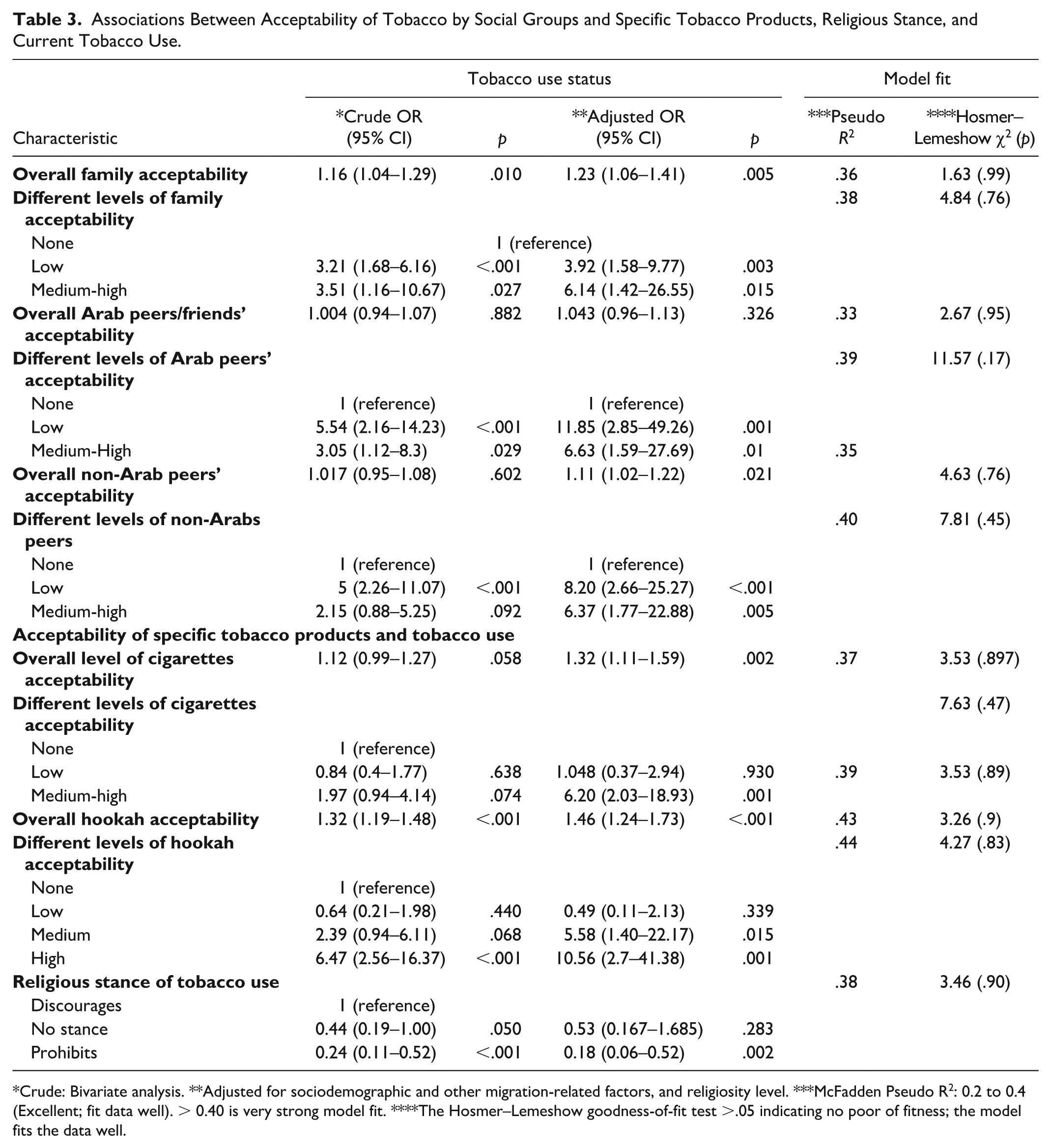
Crude: Bivariate analysis. **Adjusted for sociodemographic and other migration-related factors, and religiosity level. ***McFadden Pseudo R2: 0.2 to 0.4 (Excellent; fit data well). > 0.40 is very strong model fit. ****The Hosmer–Lemeshow goodness-of-fit test >.05 indicating no poor of fitness; the model fits the data well.
Religiosity, Religious Stance, and Tobacco Use
The study found that explicit religious prohibitions against smoking significantly reduced tobacco use (OR = 0.24, 95% CI= 0.11–0.5, p ≤ .001), as shown in Table 3. While 42.92% of respondents said their religion prohibits tobacco, a similar share reported no stance (28.81%) or discouragement (28.25%), as shown in Table 1. Muslim participants were much more likely than Christians to report religious prohibition (98.67% vs. 1.33%). The average religiosity score (BIAC) was 42.8. Tobacco users had lower scores; however, after adjusting for demographics, the association with tobacco use was inconsistently insignificant.
Social Network Structural and Compositional Attributes, and Tobacco Use
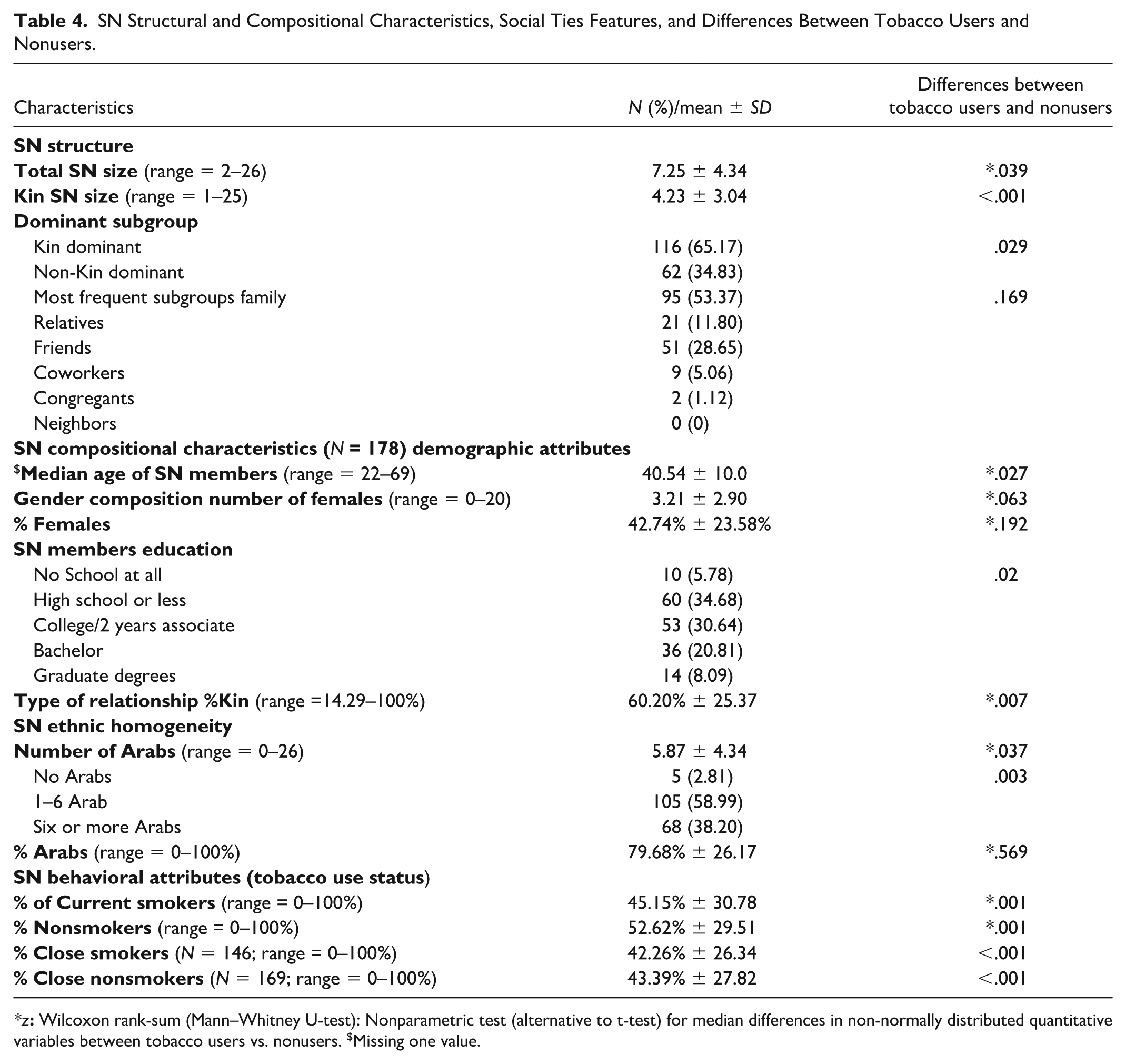
The SN played a central and contextual role in shaping tobacco behavior among participants. As shown in Table 4, the average SN size was seven individuals (M = 7.25; SD = 4.34), with kin comprising 60.2% of the SNs. Every SN included kin members; family was the most common subgroup nominated (53.37%), followed by friends (28.65%) and relatives (11.8%). Demographically, the median age of network members was 40.54 years. Females comprised an average of 42.74% of SNs. Educational attainment varied, with more than half of the sample (59.54%) possessed at least a college/associate degree. Ethnically, networks were predominantly Arab (79.68%). Tobacco users were present in 82% of SNs, averaging three users per network. The average proportion of SN who were tobacco users was 45.15%. Most networks (94.5%) included at least one nontobacco user, and nontobacco users represented 52.62% of all SNs members. Each SN typically had about five close members, with 75.8% classified as intimate. On average, 42.26% of SNs consisted of intimate tobacco users.
SN Structural and Compositional Characteristics, Social Ties Features, and Differences Between Tobacco Users and Nonusers.
As shown in Table 5, the association of the SN size and compositional characteristics with tobacco use was examined in logistic regressions. A larger SN size was linked to reduced tobacco use (OR = 0.38, 95% CI = 0.20–0.73, p = .004). Specifically, more kin in the SN was associated with lower tobacco use odds (OR = 0.81, 95% CI = 0.71–0.93, p = .002), while non-kin-dominated SNs had double the likelihood of tobacco use compared to kin-dominated ones (OR = 2.02, 95% CI = 1.07–3.79, p = .03). These associations became non-significant after adjusting for sociodemographic and migration-related factors, but the trends persisted. In terms of the network ethnic density, participants’ networks were predominantly composed of same-ethnic, family-based ties. Initially, more Arab members or females in an SN were linked to a lower likelihood of tobacco use. However, after adjusting for SN size and sociocultural factors, both variables were associated with higher odds of tobacco use (Arab members: OR = 1.53, 95% CI = 1.03–2.28, p = .03; females: OR = 1.45, 95% CI = 1.009–2.07, p = .045). In addition, SN members’ demographics showed that having older and more educated network members was associated with a lower likelihood of tobacco use (see Table 4). However, after adjusting for socio-structural factors, these associations were no longer significant, suggesting that age and education within networks may influence tobacco use but do not independently predict it.
Associations Between Social Network Structure and Compositional Characteristics and Tobacco Use (N = 178).
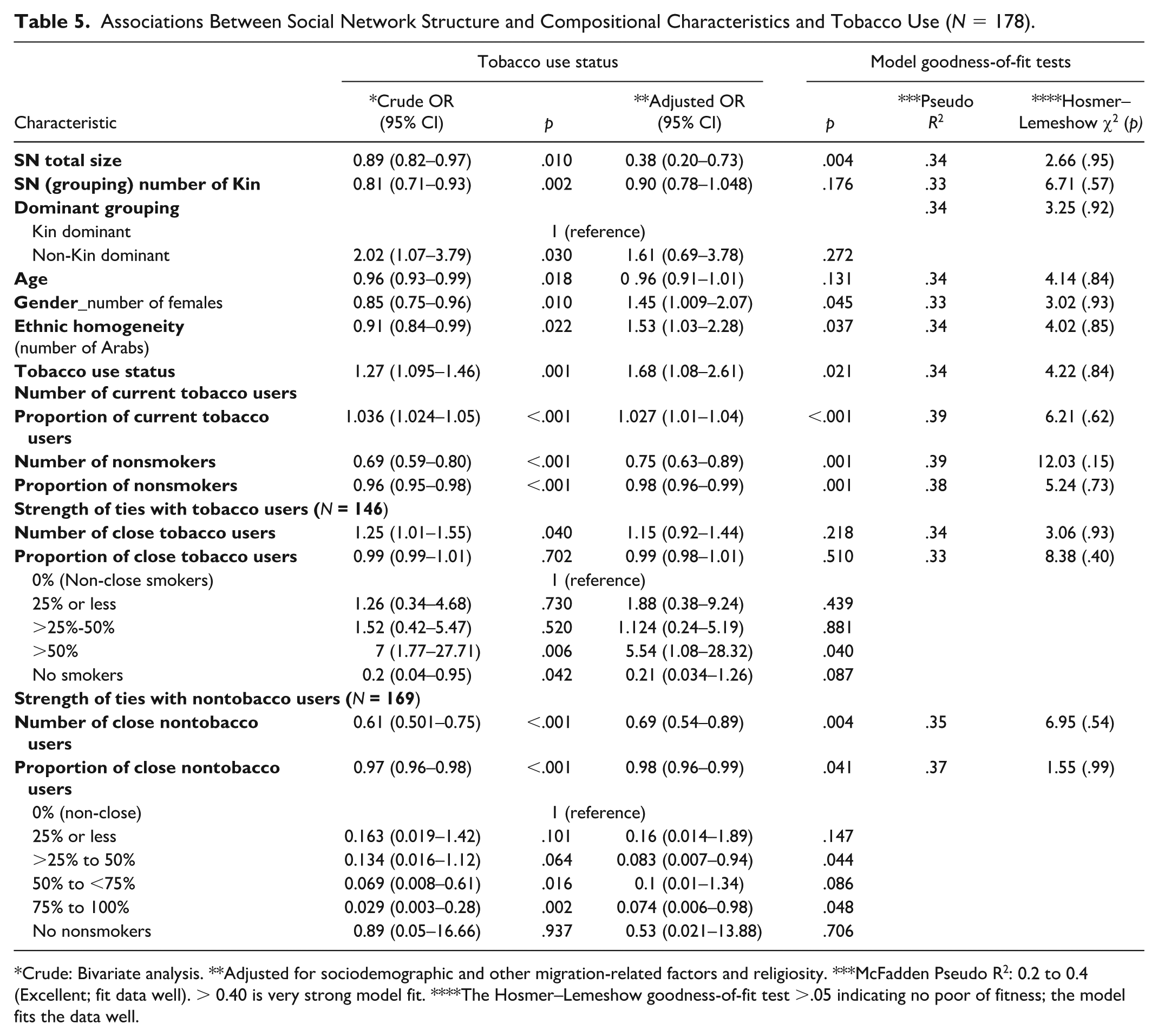
Crude: Bivariate analysis. **Adjusted for sociodemographic and other migration-related factors and religiosity. ***McFadden Pseudo R2: 0.2 to 0.4 (Excellent; fit data well). > 0.40 is very strong model fit. ****The Hosmer–Lemeshow goodness-of-fit test >.05 indicating no poor of fitness; the model fits the data well.
It is noteworthy that of the 178 Arabs studied, 82% reported being tobacco users in their SNs, while 32 (N = 18%) did not. The number of tobacco users in an SN was strongly associated with increased tobacco use (OR = 1.27, 95% CI = 1.095–1.46, p = .001). In contrast, having more nontobacco users in the network was associated with reduced tobacco use (OR = 0.69, 95% CI = 0.59–0.80, p < .001). These associations remained significant and indicated the same pattern after adjusting for socio-structural factors. Over half of those with tobacco users in their SNs (52.74%) reported at least three close smoking contacts, and a small percentage (8.22%) had only non-close ties with smokers in their networks. Those with mostly non-smoking ties showed lower odds of smoking, while a high proportion of close tobacco users in one’s SN greatly significantly increased the odds of current tobacco use (OR = 5.54, 95% CI = 1.08–28.32, p = .040), especially those who reported at least 50% of their SN were close tobacco users.
Discussion
Beyond statistical associations, these findings show how tobacco use among AAs is deeply embedded in the social fabric of migration and identity formation, where smoking behaviors symbolize belonging, cultural continuity, and negotiation of modernity. The inverse relationship between SN and tobacco use reflects more than mere numeric association: larger and cohesive networks provide emotional support, accountability, and modeling of health-promoting norms that reinforce behaviors consistent with collective wellbeing. Conversely, smaller or fragmented networks may increase isolation or exposure to smoking peers, illustrating how social structures embody sociocultural mechanisms influencing behavior. These findings demonstrate the interaction among macro-level cultural norms, meso-level family and peer relationships, and micro-level identity processes described by Berkman et al. (2000), underscoring that SNs are lived, fluid systems rather than static categories. Unlike earlier descriptive research that cataloged cultural predictors of tobacco use, this interpretation aligns with recent transcultural health debates emphasizing intersectionality, power, and relationality (Hamamra, Daraghmeh, & Al-Asi, 2025a), addressing prior gaps in understanding how migration and identity shape smoking behaviors.
This study shows how SNs, cultural norms, and religion shape tobacco use, especially hookah, which is normalized through family and peer gatherings among AA adults. Its broad acceptability, especially within families, reflects communal bonding rather than health risk awareness. This normalization represents a negotiation of identity and belonging in the diaspora, where shared smoking rituals sustain cultural connectedness. For younger generations, such practices may also signify agency and adaptation. Religiosity, meanwhile, functions as both a behavioral moderator and a symbolic boundary defining moral propriety and group membership. Smoking behaviors thus operate not only as health outcomes but also as embodied expressions of cultural alignment, belonging and autonomous decisions. These findings mirror research showing waterpipe smoking is often viewed as benign socialization in Middle Eastern and diaspora communities (Alzyoud et al., 2014; Athamneh et al., 2015, 2017; El-Hajj et al., 2017; El-Shahawy & Haddad, 2015; Jamil et al., 2009; Rice, 2012). Few studies explored how tobacco’s social meanings intersect with migration and identity; this study addresses that gap.
Family influence strongly predicts tobacco use, with family acceptability linked to higher smoking odds, consistent with Arab community studies (Arfken et al., 2015; Athamneh et al., 2015, 2017; Haddad et al., 2012; Jamil et al., 2009, 2014). This reflects collectivist values where family norms shape individual behavior (Kulwicki, 1996; Meleis, 1991). These mechanisms operate differently across generations and genders due to shifting interpretations of culture, authority, and belonging. Among first-generation immigrants, familial norms may anchor moral behavior, while U.S.-born or younger AAs balance family expectations with peer and societal norms framing smoking as social or identity-driven. Similarly, religiosity may reinforce abstinence for some or symbolize heritage adherence or autonomy for others. These variations show that family and religion influence not only behavior but the negotiation of cultural continuity and adaptation, addressing gaps in prior research that often overlooked such intersectional complexities. In contrast, peer acceptability showed less consistent influence. Familial expectations outweigh peer norms, reflecting enduring collectivist authority and intergenerational obligation. Migration may amplify this pattern as families preserve cultural and traditional hierarchies. Peer networks, though influential, operate within family moral frameworks. Interestingly, individuals reporting low peer acceptability had higher tobacco use odds than those with moderate/high acceptability, indicating family norms may outweigh peer influence, particularly among men.
Gendered patterns emerged; women reported lower tobacco acceptability from different social influences, greater peer accessibility reflecting relative freedom in peer settings, and limited behaviors under family surveillance. Women’s smoking represents moral negotiation and agency within patriarchal systems, sometimes as subtle resistance or self-expression, highlighting that gendered health behaviors must be understood within broader politics of visibility, identity, and autonomy.
In diasporic Arab communities, women’s smoking, particularly hookah use, can serve as acts of visibility and resistance, reflecting cultural hybridity. Individuals navigate overlapping expectations from heritage and host societies through acculturation dynamics (Berry, 2005), shifting transcultural nursing from cultural sensitivity to critical analysis of power and identity. Ethnographic research from Palestine supports this; Hamamra, Daraghmeh, & Al-Asi, (2025a) describe evolving attitudes toward female smoking amid tradition-modernity tensions, and Hamamra, Shehab, et al. (2025b) show young women using smoking to negotiate moral hierarchies. These studies deepen understanding and contextualize our findings, farming women’s smoking as culturally coded acts of identity and resistance. Migration and acculturation may reframe smoking as social freedom for women (Hooper et al., 2012), contributing to a narrowing gender gap in hookah use (Jawad et al., 2013; Yeretzian & Afifi, 2009). These insights underscore the need for gender-sensitive, culturally tailored cessation efforts.
Religious beliefs were significant. Participants perceiving their religion as discouraging smoking were less likely to smoke, consistent with religiosity’s protective role (Arfken et al., 2015; Berkman & Breslow, 1983; Ellison & Levin, 1998). However, this protection was not consistent, particularly for hookah, where cultural normalization attenuated religiosity’s effect. Religiosity should be seen as dynamic and context-dependent rather than universally protective. Quantitative religiosity scores were slightly lower than those of other Arab Muslim samples (Alakhdhair et al., 2016; Koenig, Wang, et al., 2015), and no significant associations emerged between religious affiliation and tobacco use. Underreporting may reflect private religiosity, discrimination concerns (Abuelezam et al., 2018), or demographic shifts among U.S. Arabs driven by Middle Eastern events (Arab American Institute [AAI], 2024). Nonetheless, religious practices such as prayer and fasting previously supported cessation (Haddad & Corcoran, 2013). Further research should explore integrating faith-based practices into culturally tailored cessation strategies for AAs.
SN structure and composition influenced tobacco use. Larger SNs were associated with lower smoking odds, suggesting protective effects through support for non-smoking norms or social accountability. However, composition moderated these benefits: networks with more women and Arab members initially appeared protective, but after adjusting for norms, effects reversed. Networks with many smokers can override protective features, especially in dense, homophilic groups (Valente, 2010). This underscores the need to consider structural, compositional, and normative aspects when designing gender-responsive, culturally sensitive cessation strategies for AAs, a gap in prior SN-based tobacco research.
These findings call for culturally responsive, network-informed cessation strategies. Nurses and public health practitioners should assess SN contexts to identify relational dynamics sustaining tobacco use. Network mapping and structured interviews can guide tailored interventions. Programs should engage family members and community leaders using Arabic-language materials, faith-based initiatives, and family-centered counseling. Collaboration with imams, priests, and respected elders may enhance credibility, particularly among recent immigrants or older adults. Nursing education should integrate transcultural models emphasizing social, spiritual, and cultural contexts, moving beyond individual-level interventions to relational, community-oriented care. Curricula should include case-based learning, role-playing, and SN analysis to prepare students to assess and respond to culturally patterned health behaviors. Curricula should use case-based learning, role-play, and SN analysis to help students assess and respond to culturally patterned health behaviors. Embedding transcultural nursing within frameworks of acculturation-related social dynamics and post-migration identity exposes how migration, gender, and power affect health, filling gaps in previous research and guiding interventions tailored to diasporic communities’ real experiences, such as AAs.
Berkman et al.’s (2000) SN framework proves useful in transcultural health research, showing how macro-level norms, meso-level relationships, and micro-level behaviors intersect to shape tobacco use. Situating SN influences within cultural and migratory frameworks enhances understanding of how identity, autonomy, and belonging shape AA health behaviors, strengthening transcultural nursing, engaging relational and symbolic dimensions of health, and providing a stronger foundation for culturally congruent interventions.
Limitations include the Massachusetts regional sample, which may limit generalizability to AAs in other regions with different levels of cultural assimilation, religious affiliation, or health service access. Recruitment from faith-based sites may overrepresent religious participants, though religiosity did not differ by site. Cross-sectional data preclude causal inference, and language nuances may have affected responses. Future research should examine longitudinal changes in SN composition, tobacco use, and religiosity across acculturation stages, and use community-based participatory research and gender- or generation-specific network-based interventions (peer- or family-led programs) to advance cessation among AAs.
Conclusion
This study demonstrates that tobacco use among AAs is shaped by interconnected social, cultural, and religious factors rather than individual choice alone. Smoking, particularly hookah, functions as a culturally embedded practice linked to identity, belonging, and adaptation within migration contexts. Larger, cohesive SNs appear protective by reinforcing collective health norms, while smaller or fragmented networks may increase exposure to pro-smoking influences. Applying Berkman et al.’s (2000) SN framework revealed how macro-level cultural norms, meso-level family and peer ties, and micro-level identity processes interact to shape smoking behaviors. Family acceptability and religiosity were key determinants, reflecting collectivist values that both discourage and, in some cases, normalize tobacco use. Gendered patterns highlighted how women navigate moral surveillance and social expectations, using smoking as both conformity and subtle resistance within patriarchal and diasporic contexts.
These findings address critical gaps by framing tobacco use as a socially and symbolically embedded behavior. They underscore the need for culturally congruent, gender-responsive, and network-informed cessation strategies engaging families, peers, and faith-based institutions. Nurses and public health practitioners can incorporate cultural, relational, and spiritual dimensions into assessments, education, and interventions, advancing transcultural nursing theory and promoting health equity among AA communities.
Footnotes
Acknowledgements
The authors express thanks to the generous, welcoming Arab community for participation in the study.
Author Contributions
Sabreen Darwish was responsible for study conceptualization, design, method development, translation, cognitive testing, data collection and analysis, and manuscript writing. Suha Ballout contributed valuable cultural insights to the study. Ling Shi assisted with verification of the statistical analysis. Rosalyn Negrón provided expertise in social network conceptualization and methodology. Mary E. Cooley contributed her experience as a tobacco researcher and supported the conceptualization of tobacco use behaviors. All authors contributed to the overall writing and critical revision of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from the Institutional Review Board (IRB) of UMASS Boston, and all participants provided informed consent. We sincerely appreciate your consideration of our submission for publication in your esteemed journal. We believe that our findings will significantly advance knowledge about SN impact on tobacco use especially underserved communities as Arab Americans and will help inform a culturally relevant cessation intervention.