
Abstract
Introduction:
Participation in free nationwide population-based breast and cervical cancer screening in the Netherlands has declined, especially among underserved women in low socioeconomic neighborhoods in The Hague.
Aim:
This study aims to identify the social networks, needs, and barriers of these women regarding informed screening decisions.
Method:
A qualitative study with interviews, focus groups, and field observations.
Results:
Social networks—including family, community centers, religious institutions, and key community figures—were central to reach underserved women. Women expressed a need for clear, accessible information in their native language and from trusted sources. Barriers included language difficulties, lack of knowledge, limited digital skills, cultural and religious beliefs, fear, and distrust in health care.
Discussion:
Findings suggest that providing culturally sensitive information and engaging social networks are essential for supporting informed decisions and reducing health disparities. Effective strategies should focus on trust-building, communication, and community involvement. Future research should evaluate these strategies.
Keywords
Introduction
Breast cancer (BC) and cervical cancer (CC) are among the most frequently diagnosed cancers in women worldwide (Bray et al., 2024; World Health Organization, 2026). Screening plays a key role in the early detection of cancer, reducing mortality, and improving survival outcomes (Aarts et al., 2011; Broeders et al., 2012; Hartman et al., 2009; Rijksinstituut voor Volksgezondheid en Milieu [RIVM], 2022). In the Netherlands, nationwide cost-free population-based cancer screening programs have therefore been implemented as part of the National Screening Program. These programs are coordinated by the National Institute for Public Health and the Environment (“Rijksinstituut voor Volksgezondheid en Milieu”; RIVM) in collaboration with the National Health Screening Organization (“Bevolkingsonderzoek Nederland”).
Population-based BC screening covers ages 50 to 75, a 25-year period with biennial invitations (RIVM, 2022). Population-based CC screening targets women between the ages 30 to 60, a 30-year period during which they receive five screening invitations at regular intervals.
High participation rates are crucial, with a minimum threshold of 70% deemed necessary to ensure adequate coverage and early cancer detection (RIVM, 2022). In The Hague, a super-diverse city in the Netherlands, participation in population-based BC and CC screening remains substantially below national averages, with rates of 33% and 58%, respectively, in 2022 (RIVM, 2022; Vertovec et al., 2023), both substantially below national averages, indicating significant local underparticipation (RIVM, 2022).
Population-based screening programs have been shown to reduce both cancer incidence (through the detection of precancerous lesions) and mortality. Where people do not participate, they are more likely to be diagnosed at a later, more advanced stage, when treatment is less effective and more burdensome (Van Stigt et al., 2025). This is especially evident among underserved women—those facing substantial barriers to health care access and equity. This group includes first-generation migrant women who speak languages other than English or Dutch, born outside the country, women with limited literacy or low health literacy, and women from lower socioeconomic status (SES) (Bongaerts et al., 2020, 2023).
These women are currently not adequately reached through existing communication channels and may therefore struggle to make an informed decision about participation in population-based screening programs. This is due to various cultural, practical, emotional, and religious barriers, including limited knowledge about screening, stigma and taboo, fear, religious fatalism, lack of resources, limited social support, language barriers, low (health) literacy, having a male general practitioner (GP), and limited awareness of or trust in the health care system (Bongaerts et al., 2020; Hamdiui et al., 2022; Kasmi, 2018).
Participation rates—particularly in cities such as The Hague—represent a significant public health concern, exacerbating health disparities by limiting equitable access to health information and care. This underscores the need to better understand the barriers experienced by underserved women and to develop effective communication and intervention strategies to enhance informed decision-making regarding population-based BC and CC screening.
To promote informed decision-making, researchers connected with Mammarosa, a Dutch organization that support women with BC who experience language barriers due to low literacy or cultural differences. Mammarosa assists these women in accessing health information, making informed decisions, and connecting with peers through self-help groups. Together, we conducted a pilot study: the Screening the Neighborhoods (StN) project. This paper focuses on the StN project and assesses the needs of underserved women. Specifically, we address three research questions: (1) How can non-participating women be effectively reached and engaged at the start of the research to assess their needs?; (2) What social networks (e.g., key figures, contact persons), locations, and activities characterize these women?; and (3) What barriers do underserved women face, and what potential solutions can inform the development of effective communication and intervention strategies to enhance informed decision-making?
Method
Ethical Consideration
This study received Institutional Review Board (IRB) approval (registration number: 2023-019) and was conducted in accordance with the Declaration of Helsinki. All recordings and transcripts were anonymized and stored following the ethical guidelines for human research of TNO and principles of good research practice, as approved by the TNO ethical board. The study is reported in line with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Buus et al., 2025).
Samples and Setting
On-the-Spot Interviews With Women
Neighborhoods in The Hague were selected through desk research identifying areas with below-threshold participation in population-based cancer screening. Between June and July 2023, on-the-spot interviews (n = 30) were conducted with women aged 30 to 75 years across 18 neighborhoods. Interviews took place in public locations (e.g., stations, markets, parks), lasted approximately 10 min, and explored screening participation, social networks, frequently visited locations, and activities. These brief interviews generated rapid, real-life insights (Gaia et al., 2025).
Interviews With Underserved Women and Key Figures
In May 2023, individual and focus group interviews were conducted with underserved women (n = 28) and key figures (n = 11), many with Turkish, Moroccan-Berber, Surinamese, Iranian, Eritrean, or Ethiopian migration backgrounds, residing in low-participation neighborhoods. Participant volunteers from Mammarosa organized an informational session on population-based cancer screening programs. Focus groups lasted approximately 60 min and were conducted in Dutch, with multilingual students providing translation when needed to ensure a comfortable setting and foster trust (Hammersley & Atkinson, 2019). Interviews addressed social networks, access to information, barriers, support for informed decision-making, and community activities. Student researchers received prior training in qualitative interview techniques.
Interviews With Health Care Workers
Semi-structured interviews were conducted with health care workers (n = 11) employed in low-socioeconomic status neighborhoods. Participants were recruited through purposive and snowball sampling. Interviews lasted approximately 60 min and explored their role in supporting women’s decision-making regarding cancer screening, including perceived barriers, challenges, opportunities, and forms of support.
Recruitment and Consent to Participate
Women, key figures, and health care workers were recruited through community outreach, purposive sampling, and snowball sampling. At inclusion, participants received verbal information about the study from multilingual students, researchers (AH and ZH), and the project leader (SK) from Mammarosa. Written informed consent was obtained for participation and audio recording prior to data collection.
Data Collection
Data were collected between May and July 2023 through on-the-spot interviews, individual interviews, focus groups, and participatory fieldwork. All interviews were audio-recorded and transcribed verbatim. In addition, participatory observation was conducted during a community center event focused on engagement strategies for non-participating women. Detailed field notes and logbooks were maintained to produce thick descriptions of interactions and women’s engagement (Silverman & Patterson, 2021).
Data Analysis
Qualitative data were analyzed using the framework for inductive thematic analysis described by Virginia Braun and Victoria Clarke (2006). All audio-recorded interviews were transcribed verbatim. Segments conducted in Moroccan-Berber, Arabic, or Turkish were directly transcribed into Dutch by multilingual health science students. Transcripts were read repeatedly to achieve familiarization with the data. Subsequently, open and axial coding were performed to identify patterns and develop themes and subthemes, which were organized into a coding tree and approved by the first author (AH). Selective coding was then conducted to generate overarching concepts related to barriers and potential solutions for informed decision-making. Codes concerning social networks, locations, and activities were systematically compared, validated with key figures, and grouped using ATLAS.ti.
To enhance analytic rigor, multiple researchers independently coded transcripts. Discrepancies were discussed until consensus was reached, strengthening credibility and ensuring that findings accurately reflected the data.
Rigor
Methodological rigor was ensured through triangulation of data sources (interviews, focus groups, and field observations), inclusion of diverse participant groups (women, key figures, health care workers), and collaborative coding among researchers. The use of thick descriptions supported transferability (Silverman & Patterson, 2021), and adherence to the COREQ checklist enhanced transparency and reporting quality (Buus et al., 2025).
Results
The results are presented according to the three research questions. First, we describe how non-participating women were reached and engaged (research question 1). Second, we present findings on women’s social networks, key figures, locations, and activities (research question 2). Third, we outline the barriers underserved women face and the potential solutions to support informed decision-making (research question 3). In addition, similarities and differences in women’s experiences with population-based BC and CC screening are presented, highlighting overlapping and distinct barriers and facilitators for informed decision-making.
Participant Characteristics
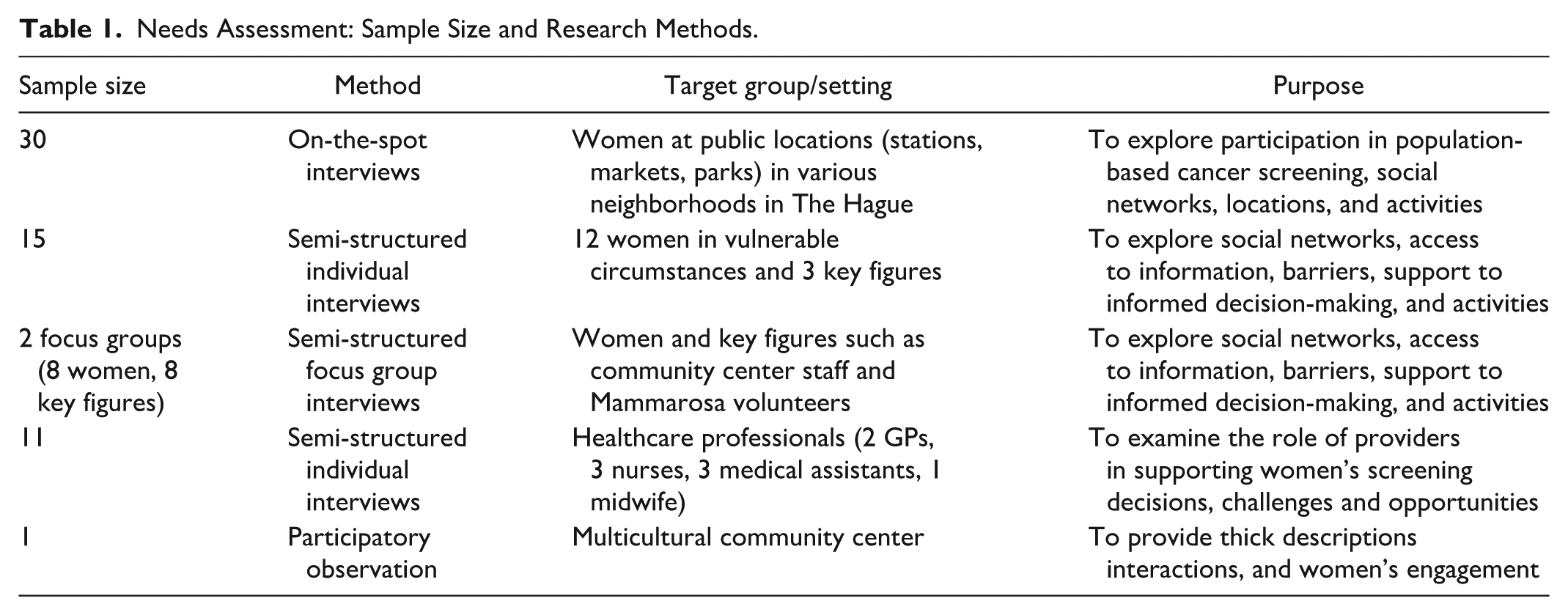
Participant characteristics (n = 80) are presented in Table 1 and include women aged 30 to 75 from low-participation neighborhoods in The Hague, key community figures, and health care workers such as GPs, GP assistants, and nurses. Many of the women and community figures had diverse migration backgrounds. Below, the findings are presented according to the three research questions, followed by similarities and differences between population-based BC and CC screening.
Needs Assessment: Sample Size and Research Methods.
Reach and Engage Non-Participating Women
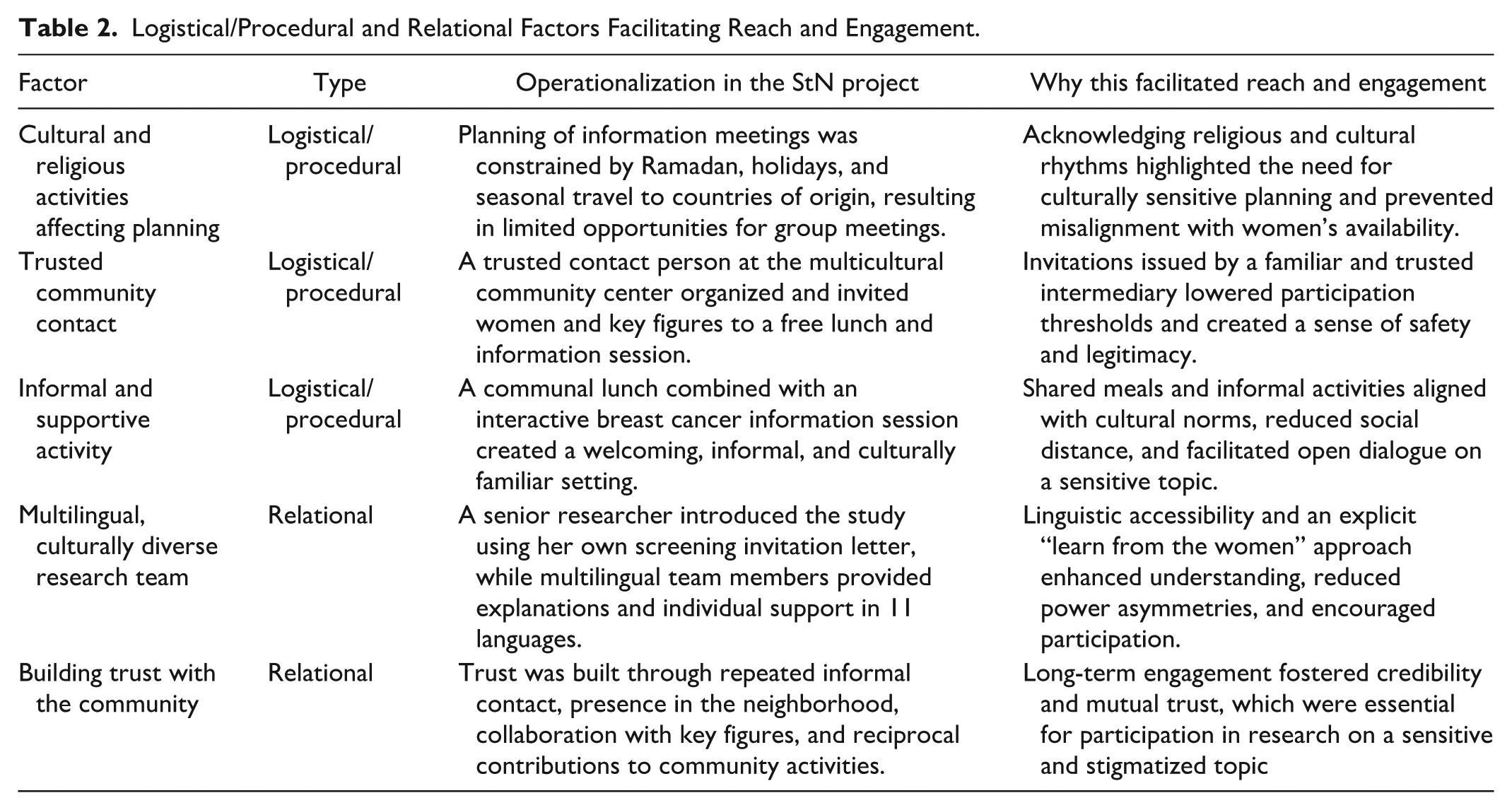
Five factors facilitated reaching and engaging non-participating women and key community figures at the start of the research (Table 2). Three factors were logistical/procedural and concerned culturally and religiously sensitive planning, the involvement of a trusted community contact, and the use of an informal and supportive activity. Two factors were relational, emphasizing the importance of a multilingual, culturally diverse research team and sustained trust-building with the community. Together, these factors created a safe and accessible environment in which women felt comfortable engaging in conversations about population-based cancer screening and participating in the research.
Logistical/Procedural and Relational Factors Facilitating Reach and Engagement.
Women’s Social Networks, Locations, and Activities
On-the-spot interviews with women and key figures showeds that women connect in neighborhood streets, parks, markets, stations, and schools, with younger women also using social media (e.g., WhatsApp). First-generation older woman often gather through family, churches or mosques, and community centers. As a woman with a Turkish background (60 years) explained: “We meet with family, in the mosque, and in the community center.” Another Dutch woman (68 years) stated: “I am active in the church council.” A Moroccan-Berber woman (45 years) shared: “We meet once a week for sewing lessons in the community center in the Schilderswijk.” Women also have contact with health care providers. Suggested channels for population-based cancer screening information included group activities, videos in their language in waiting rooms at GPs’ offices, television or billboards campaigns, tram advertising, or social media.
Barriers and Solutions to Increase Informed Decision-Making
Thematic analysis of individual and focus group interviews with women, key figures, and health care workers revealed six themes: (a) language barrier and lack of information about population-based BC and CC screening; (b) lack of social support and access; (c) cultural and religious factors; (d) fear of pain, cancer, and death; (e) lack of trust and limited time; and (f) similarities and differences regarding population-based BC and CC screening. These themes include determinants that need to be addressed to develop effective communication and intervention strategies to improve informed decision-making.
Language Barrier and Lack of Information
Interviews with women and key figures revealed that a lack of knowledge about population-based BC and CC screening, and procedures is a key barrier to participation. A major issue is the absence of information in the women’s mother tongues. Some women did not recognize or read the Dutch invitation letter. As one woman with a Surinamese background stated: “I do not receive this letter,” and woman with a Turkish background added: “I’ve never seen this letter.” The women emphasized the need for accessible information cancer causes, prevention, and appointment scheduling.
Health care workers similarly reported linguistic and literacy barriers, which hindered communication, with even interpreters or translation apps being used. One Dutch GP explained: “These are sensitive topics . . . Especially women with an Eritrean or Ethiopian background—they simply do not speak easily when a man [interpreter] is translating, even in an anonymous telephone conversation.” These barriers contribute to a lack of knowledge about population-based cancer screening. Therefore, making the invitation letter recognizable, understandable, and available in the women’s native languages is essential.
Lack of Social Support and Access to Screening
Women and key figures reported that making an online appointment is difficult, especially due to limited computer skills and challenges using DigiD, leading to rely on their children or loved ones for help. As one key figure explained: “The location for screening is not easy to reach. A mobile bus in the neighborhood would really help . . . that would make it easier and lower the barrier” (35-year-old woman, Surinamese background).
Health workers emphasized the need for easily accessible population-based cancer screening centers and support networks, such as information in mosques or peer mentoring (“train the trainer”) to encourage women to support each other and facilitate population-based BC and CC screening participation. They highlighted the role of health care providers in encouraging participation during routine check-ups and working together with women, key figures, and female doctors. According to women and professionals personal, narrative explanation assistance with (online) appointment scheduling—combined with accessible locations and community support—can improve informed decision-making regarding population-based BC and CC screening.
Cultural and Religious Factors
Women and key figures frequently noted that cancer is not openly discussed in Turkish and Moroccan communities: “First-generation Moroccans and Turkish . . . have difficulty talking about cancer. Because it is something that only concerns you and your partner” (62-year-old woman, Turkish background). Feelings of shame and taboo were common: “In our culture . . . we do not even say the word [cancer].” Some believed that discussing cancer could cause it: “Don’t talk about it, or you’ll get it yourself” (57-year-old woman, Iranian background).
Perspectives on faith varied. Some Muslim Moroccan women felt that cancer is determined by God and therefore chose not to participate: “We have to accept what God gives.” Others saw screening as a religious responsibility: “Our lives are determined to a certain extent, but how we follow a path depends on ourselves” (67-year-old-woman, Turkish background). Another participant emphasized bodily care: “God wants us to treat our bodies pure and clean” (54-year-old-woman, Moroccan background).
Women and key figures valued community meetings, such as those organized by Mammarosa, and suggested offering similar meetings in mosques. Health care workers recommended targeted awareness campaigns and training female cultural or religious key figures to address health concerns, (religious) values, and provide information in women’s native languages.
Fear of Pain, Cancer, and Death
Women frequently mentioned fear of pain during mammography as a significant barrier to BC screening. As one participant noted: “I think many women are afraid of the pain of that thing [mammography machine]” (Woman, age unknown, Surinamese background). Others confirmed this fear. Fear also related to receiving a diagnosis. Some women with Turkish backgrounds said: “I do not want to know if I have cancer,” avoiding screening due to fear of the disease, or stigma tied to unhealthy lifestyle behaviors such as smoking and alcohol consumption. Several women expressed fear of dying and leaving their children behind. Health care workers reported similar concerns among patients, including fear of discovering a serious condition and the stigma specifically associated with cervical cancer. As one GP assistant explained: “ . . . there is also the group of women who are simply afraid that something will be discovered . . . cervical cancer is very stigmatizing . . . They say: ‘I can’t have it, because I have one partner.ʼ” Some women feared that screening might lead others to assume that they were sexually active outside of marriage, causing shame or gossip.
According to women and key figures, role models who share their cultural background and speak openly about screening or cancer experiences could support informed decision-making. Health care workers emphasized the need for culturally sensitive communication, tailored to women’s language skills, education, health literacy, and cultural background.
Lack of Trust and Time
A lack of trust significantly hinders women’s willingness to participate in population-based BC and CC screening programs. Many migrant women, for example, expressed more confidence in their doctors abroad than in those in the Netherlands: “The doctor in the Netherlands doesn’t take me seriously; I get paracetamol and have to wait. That’s why I prefer to go to Morocco, where I get a diagnosis and medication” (Woman with a Moroccan background, 68 years old).
This aligns with the statements of key figures, who emphasized that explanations and information must come from someone the women trust, who speak their language, and who can provide culturally sensitive information.
Health care workers indicated that information about population-based BC and CC screening can be shared during consultation hours. However, some admitted that they do not always think about discussing screening, especially when the primary complaint is unrelated to cancer. Addressing screening information to illiterate women who do not speak Dutch requires time:
. . . once I’ve explained what a cervical smear test is and whether she’s ever had one, well, by the time I find out whether she has or not, then I’m happy that she understood that at all. And then I don’t actually have time to explain it in more detail. (GP with a Dutch background)
Yet time cannot be an excuse: “A personal invitation might improve the screening participation, and a lack of time cannot actually be an excuse for this” (Health care worker with a Turkish background). Some emphasized the need for repeated efforts: “This is a target group for which just one talk is not enough. You just have to do this a hundred times again” (Nurse with a Dutch background). All expressed motivation to contribute to higher BC and CC screening attendance, highlighting the importance of personal relationships with women.
Similarities and Differences Between Population-Based BC and CC Screening
For population-based BC screening, women mainly reported fear of pain during the mammogram and lack of time. For population-based CC screening, barriers more often involved embarrassment, cultural sensitivities, and misconceptions—such as believing screening is unnecessary when not sexually active or after menopause. The findings show diversification within diversity, indicating that a cultural background alone cannot fully explain barriers; instead, women’s experiences are shaped by linguistic, cultural, and structural factors, aligning with the notion of avoiding culturalization (Hoffman & Verdooren, 2019).
Health care professionals emphasized limited time during consultations to address preventive issues, like population-based BC and CC screening, and they were not always aware which patients received invitations from Bevolkingsonderzoek Nederland. Feelings of embarrassment, especially with male practitioners, remained a recurrent barrier to population-based CC screening.
Discussion
Our study contributes new insights into barriers and facilitators of breast and cervical cancer screening among underserved women. Although many of the identified barriers—such as limited knowledge, language difficulties, culturally rooted beliefs, fear, and distrust of health care providers—have been well documented in previous systematic reviews and qualitative research (Ferrari et al., 2024, 2025), our findings add context-specific evidence by illustrating how these factors manifest and interact within underserved communities in The Hague. This contextualization is particularly relevant for informing the design and implementation of culturally and linguistically adapted screening interventions.
Reaching and Engaging Non-Participating Women
Involving underserved women early in research projects is crucial. Our findings highlight the need to connect with women’s social networks, regular activities, and relevant community organizations. Engaging women not typically involved in research has been emphasized previously (Bongaerts et al., 2023, 2021; Hamdiui et al., 2022; Kasmi, 2018), as a key step to identifying barriers and facilitators of BC and CC screening participation.
Contemporary evidence further suggests that structural barriers—including health care system bureaucracy, mistrust in services, and socioeconomic obstacles—compound individual-level challenges, underscoring the need for diverse, culturally tailored strategies to reach and support underserved populations (Wearn & Shepherd, 2024).
In addition to relational factors, logistical and procedural considerations—such as scheduling around cultural and religious events, creating welcoming environments, and offering activities like free meals—proved crucial. Combining information sessions with a free lunch and interviews provided effectively engaging the women. The research team’s cultural and language diversity helped break down barriers by allowing communication in participants’ native languages. Accessibility was key: holding the event in a familiar multicultural community center encouraged participation and dialogue. Providing information in women’s native languages and creating welcoming community settings supported participation, aligning with evidence that culturally adapted outreach enhances engagement (Agénor et al., 2024).
Women’s Social Network, Locations, and Activities
This research highlights the value of outreach strategies embedded in women’s social networks, daily environments, and community structures. Contemporary literature on community-based and social network approaches shows that interventions integrated into existing social relations and activities can improve access and uptake of preventive services among harder-to-reach groups. Social network strategies have been shown to effectively disseminate health information and influence preventive behaviors through peer support and trusted interpersonal ties (Greenley et al., 2023). Building on this, a bottom-up approach not only promotes screening participation but also strengthens women’s empowerment, social cohesion, and community ownership—an approach recommended by recent public health research focused on reducing inequities in preventive care engagement (Greenley et al., 2023).
Relational and Logistical Factors in Reaching the Target Group
The success of the engagement strategy in this study aligns with previous models on reaching and retaining target groups (e.g., Agénor et al., 2024) Overall, our findings highlight the importance of combining relational, logistical, and cultural strategies to engage underserved women and in population-based BC and CC screening programs. Considering social networks, familiar community locations, and culturally sensitive approaches enables researchers and health care workers to reduce barriers, foster trust, and improve participation rates, ensuring that vulnerable groups have the opportunity to make informed health decisions.
Barriers and Solutions to Increase Informed Decision-Making
The needs assessment identified barriers limiting women’s informed decisions about population-based BC and CC screening, including lack of knowledge, difficulty recognizing Dutch invitation letters, need for support with understanding screening information, cultural beliefs, fear of pain, and a distrust of health care providers. These findings align with prior systematic reviews (Escribà-Agüir et al., 2016; Wearn & Shepherd, 2024) qualitative studies (Hamdiui et al., 2022; Kasmi, 2018) highlighting low SES, limited knowledge about BC and CC screening, and language barriers as key determinants of low participation.
Interventions that address these multifaceted barriers—including self-sampling options, tailored communication, peer support, and community health worker models—show promise in expanding access and supporting informed decision-making among underserved groups (Gillibrand et al., 2025; Hamdiui et al., 2022).
Limitations and Strengths
Our research had several limitations. As a pilot study with a small number of participants, the findings have limited generalizability to the broader population in the Netherlands. In addition, the information provided at the community center focused more on BC than on CC screening, which may have limited participants’ ability to fully express their views on CC screening. However, the aim was not broad generalization but in-depth insights to inform intervention strategies for improving informed decision-making in population-based cancer screening participation.
This study had notable strengths. We successfully engaged women and key figures in low-SES neighborhoods in The Hague, facilitated by multilingual health student researchers, which likely increased comfort and participation. Organizing meetings following existing activities at the community center, enabled us to reach a diverse group of women and key figures, and providing a free lunch may have further supported engagement and willingness to engage in the study.
Conclusion
Women in marginalized positions connect through public places, social media, family gatherings, community events, and religious institutions. Dissemination of population-based screening information should leverage these social networks and locations through using group activities, videos, TV promotions, billboards, tram ads, and social media.
Primary barriers to population-based BC and CC screening include lack of knowledge, difficulty understanding Dutch invitation letters, cultural beliefs, fear, and distrust of health care practitioners. Overcoming these barriers requires a culturally sensitive approach that builds trust, improves communication, and addresses practical and emotional challenges. Integrating community-involvement, accessible information, and peer support can enhance participation and informed decision-making.
Although organizations like the National Institute for Public Health and the Environment (RIVM) and Mammarosa provide multilingual materials, awareness and digital literacy remain limited among first-generation migrants. Solutions include sharing materials via trusted key community figures in native languages, improving accessibility, and offering neighborhood-based support such as peer mentoring.
Engaging marginalized women in research is essential and should involve trusted community figures and multilingual researchers to foster trust. Future research should implement and evaluate these strategies to better support underserved populations and reduce health disparities.
Supplemental Material
sj-pdf-1-tcn-10.1177_10436596261435968 – Supplemental material for Enhancing Participation in Population Based Cancer Screening: Culturally Sensitive Approaches for Underserved Women
Supplemental material, sj-pdf-1-tcn-10.1177_10436596261435968 for Enhancing Participation in Population Based Cancer Screening: Culturally Sensitive Approaches for Underserved Women by Anita Ham, Zeena Harakeh, Samia Kasmi, Daniella Gidaly and Nicole van Kesteren in Journal of Transcultural Nursing
Footnotes
Acknowledgements
We would like to express our sincere gratitude to the members of the target group and the key figures of the multilingual community meeting center for their participation in this study, including the interviews, and for granting permission to conduct the information session and interviews at the center. We also extend our appreciation to the volunteers from Mammarosa and to the health sciences student researchers from The Hague University of Applied Sciences for their invaluable support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Dutch ZonMW Foundation [Zorg Onderzoek Nederland Medische Wetenschappen] [NWO] (Health Research and Innovation in Care) under the call: Vroege Opsporing (Early Detection) 2020-2021, SA 2021, file no. 05550402110023.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.