
Abstract
Introduction:
Mental health among Black and Latino adults is shaped by social and cultural dynamics. We examined associations of social support-seeking, interpersonal violence, and loneliness with depressive and anxious symptoms in a low-income urban context.
Methods:
A cross-sectional survey of 453 low-income Black and Latino adults in a Northeastern U.S. minority urban community. Data analyses included descriptive statistics, correlations, and regressions that controlled for all interpersonal experiences and sociodemographic characteristics.
Results:
Latino adults reported greater depressive symptoms than Black adults. Loneliness was the strongest predictor of depressive and anxious symptoms. Social support-seeking predicted greater anxious symptoms only for Black adults in unadjusted models. Interpersonal violence predicted greater depressive symptoms in unadjusted models, and greater anxious symptoms only for Black adults in both models.
Discussion:
Loneliness may be a key risk factor for mental health symptoms. Some interpersonal factors appeared more salient to Black adults’ mental health, informing culturally congruent care.
Keywords
Introduction
Black and Latino adults face elevated risk for depressive and anxious symptoms due to chronic stressors such as racism, discrimination, and socioeconomic disadvantage (Office of Disease Prevention and Health Promotion [ODPHP], 2021; Williams & Etkins, 2021). Interpersonal experiences play a central role in shaping mental health in these contexts. Supportive relationships can buffer distress, whereas negative interactions, including interpersonal violence and feelings of loneliness, increase vulnerability to poor mental health outcomes (Acoba, 2024; Horne et al., 2020; Richardson et al., 2017)
Prior research shows that greater social support is associated with fewer depressive and anxious symptoms, although its protective effects may vary across racial and ethnic groups (Almquist et al., 2016; Jacob et al., 2022; Johnson-Esparza et al., 2021). In contrast, exposure to interpersonal violence is a strong risk factor for mental health challenges among Black and Latino adults, including heightened depressive and anxious symptoms (Fedina et al., 2017; Mugoya et al., 2017). Loneliness has also emerged as a robust predictor of poor mental health across racial and ethnic groups, often showing stronger associations with depressive and anxious symptoms than either social support or interpersonal violence (Gabarrell-Pascuet et al., 2023; H. O. Taylor & Nguyen, 2020).
Social support, loneliness, and interpersonal violence are very often examined separately, but they represent interrelated yet distinct interpersonal processes. Social support reflects access to helpful relational resources, whereas interpersonal violence involves harmful or threatening interactions within close relationships (Fedina et al., 2017). Further, loneliness captures a subjective sense of social disconnection even in the presence of social ties (Erzen & Çikrikci, 2018; National Institute on Aging [NIA], 2024). These experiences can occur at the same time as individuals simultaneously experience support, conflict, and feelings of isolation (Lincoln et al., 2005; R. J. Taylor et al., 2015). Understanding these co-occurring experiences together offers a more comprehensive understanding of how protective (e.g., support) and harmful (e.g., loneliness) relational processes uniquely and jointly shape depressive and anxious symptoms among Black and Latino adults.
These interpersonal processes operate within distinct cultural and structural contexts. Among Black adults, extended kin, religious, and community networks may provide support while also creating interpersonal strain under conditions of chronic stress (Adu et al., 2025; R. J. Taylor et al., 2015). Among Latino adults, values such as familismo can foster resilience and belonging, yet conflict or disruption within family networks may intensify distress (Ayón et al., 2010; Valdivieso-Mora et al., 2016).
Despite extensive research on these groups separately, less is known about how interpersonal experiences relate to mental health when Black and Latino adults are examined together in a shared low-income urban context. In this study, we examined how three key interpersonal experiences – social support-seeking, interpersonal violence, and loneliness – are associated with depressive and anxious symptoms among low-income Black and Latino adults. We hypothesized that greater social support-seeking would be associated with fewer depressive and anxious symptoms, whereas greater interpersonal violence and greater loneliness would be associated with greater depressive and anxious symptoms (Hypothesis 1a). We further hypothesized that loneliness would emerge as the strongest interpersonal predictor of both depressive and anxious symptoms when all three interpersonal experiences were considered simultaneously and after adjusting for sociodemographic covariates (Hypothesis 1b). In addition, we explored whether these associations differed between Black and Latino adults (Aim 2).
Method
Ethical Considerations
The study (IRB ID: Pro2022001068) was approved by the university’s Institutional Review Board under exempt status. Written informed consent was obtained from all participants.
Study Design
This study employed an observational, cross-sectional, and correlational design and adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines (von Elm et al., 2007).
Study Setting
This study was conducted in Camden, New Jersey, a low-income, predominantly Black and Latino urban community in the Northeastern United States. Camden is characterized by long-standing socioeconomic disadvantages and health inequities, providing an important context for examining how interpersonal experiences are associated with mental health among residents facing chronic structural stressors.
Sampling
Purposive sampling was used to recruit adult residents in the city of Camden, New Jersey. Inclusion criteria included the following: Adults aged
Recruitment and Informed Consent
The study flyer was distributed and posted in residential communities and the local housing authority, as well as at community events, food banks, and by word of mouth in the city of Camden. If eligible and willing, potential participants came to community centers, local schools, or churches near their residences at the specified time indicated on the flyer. The researchers confirmed residents’ interest and determined their eligibility for the study. The researchers explained the study’s purpose and procedures to potential participants and provided them with the informed consent document. Potential participants were given enough time to read the consent form, or it was read to them; the researchers were available to answer any questions regarding the study and informed consent. The researchers emphasized to potential participants that participation in the study was voluntary, that they could withdraw at any time, and that all information obtained would be kept confidential. Names or any other identifiers were not associated with the data, and only unique, anonymous subject ID numbers were used to identify the data. All the participants signed the consent form.
Data Collection
Participants were recruited between October and December 2022. Data collection occurred in community centers, local schools, or churches. Participants selected whether they wanted the researchers to interview them or complete the survey themselves, either in person or online via Qualtrics in English or Spanish. The study took 30 to 40 minutes to complete. Participants received $20 in cash or an electronic gift card.
Measures
Predictors: Interpersonal Experiences
Social Support-Seeking
Social support-seeking was measured using 4 items from two Brief COPE Inventory subscales, a validated and widely used assessment tool (Carver, 1997). Participants rated how often they sought social support during stressful situations on a 4-point scale (1 = You usually don’t do this at all, 4 = You usually do this a lot). Emotional and instrumental support were assessed by asking participants how often they sought emotional support, comfort, help, and advice from others. A composite measure of overall social support was created by summing the four items (α = .73). This measure has been shown to capture variability in mental health outcomes in similar contexts (García et al., 2018).
Interpersonal Violence
Interpersonal violence was assessed using a 4-item Safety Concern subscale (Centers for Medicare and Medicaid Services, 2017). Participants were asked how often they were physically hurt, insulted or talked down to, threatened with harm, or screamed or cursed at. Participants rated their responses on a 5-point scale (0 = never, 4 = frequently). A composite measure was created by summing the four items (α =.81). This measure has been shown to effectively capture experiences of interpersonal aggression, providing valuable insights into personal safety concerns (Billioux et al., 2017).
Loneliness
Loneliness was assessed using a single item (Family and Community Support subscale; Centers for Medicare and Medicaid Services, 2017). Participants were asked, “How often do you feel lonely or isolated from those around you?” Participants rated their responses on a 5-point scale (0 = never, 4 = always). This broad measure of perceived loneliness is practical for community-based research and has been used to examine associations with mental health outcomes (Gordon & Stiefel, 2024).
Outcomes: Mental Health Symptoms
Depressive Symptoms
Depressive symptoms were assessed using the 2-item Patient Health Questionnaire (PHQ-2; Kroenke et al., 2003). Participants reported how often during the past 2 weeks they experienced two core symptoms of depression: “Little interest or pleasure in doing things” and “Feeling down, depressed, or hopeless.” Participants rated their responses on a 4-point scale (0 = not at all, 3 = nearly every day). A composite measure was created by summing the two items (rSB = .78). This brief screening tool is widely used and has demonstrated good sensitivity and specificity for identifying depressive symptoms (Kroenke et al., 2003).
Anxious Symptoms
Anxious symptoms were assessed using the 2-item Generalized Anxiety Disorder scale (GAD-2; Sapra et al., 2020). Participants indicated how often during the past 2 weeks they had experienced two common anxious symptoms: “Feeling nervous, anxious, or on edge” and “Not being able to stop or control worrying.” Participants rated their responses on a 4-point scale (0 = not at all, 3 = nearly every day). A composite measure was created by summing the two items (rSB = .77). This brief measure has shown strong sensitivity and specificity for detecting generalized anxiety symptoms (Hughes et al., 2018).
Moderator: Race/Ethnicity
Participants self-reported as either Black/African American (coded as 1) or Hispanic/Latino (coded as 0).
Covariates
The following covariates were considered in analyses, based on previous literature on their associations with mental health outcomes and interpersonal experiences: age, gender (male, female, other [reference group]), income (dichotomized at the approximate median split into <$10K versus ≥$10K) and education level (high school, high school graduate, > high school [reference group]), and physical functioning (assessed via the 10-item SF-36 Physical Functioning subscale; Ware & Sherbourne, 1992). The covariates with significant bivariate associations with either of the outcomes were gender, income, education level, and physical functioning, and thus were included in the final models.
Data Analysis
All analyses were conducted using SPSS version 29. Data were checked for completeness, with missing data on ≤1.10% of key variables and ≤1.99% of covariates. Pairwise deletion was used for missing data. For descriptive purposes, we tested racial/ethnic differences using independent samples t-tests.
To examine how interpersonal experiences were associated with depressive and anxious symptoms and which interpersonal experiences had the strongest association with depressive and anxious symptoms (Hypothesis 1), we used intercorrelations to examine unadjusted associations (bivariate analyses) among key variables, stratified by race/ethnicity. We also conducted two simultaneous regressions (multivariate analyses), with all predictors included in the model, controlling for gender, income, education, and physical functioning.
Finally, to examine whether the association between interpersonal experiences with depressive and anxious symptoms was stronger for Latino or Black adults (Aim 2), we repeated the regression analyses for each outcome and added an interaction term between each centered predictor and race/ethnicity. Significant interactions were probed using simple slopes at ±1 SD for interpersonal experiences and for each racial/ethnic group.
Results
Participant Characteristics
Participant characteristics by race/ethnicity are reported in Table 1. Participants’ ages ranged from 18 to 85 years (M = 52.43 years, SD = 15.17); 61.1% were women and 37.4% were men. Of the sample, 75.9% identified as Black/African American and 24.1% identified as Hispanic/Latino (individuals who were biracial were removed from the analyses). The most common living arrangement was living alone (36.7%); household size averaged 2.45 people (SD = 1.66). The greatest percentage of participants had a high school diploma (48.9%). More than half (52.3%) of participants reported an annual income below $10,000. None of these characteristics significantly differed by race/ethnicity.
Participant Characteristics by Race/Ethnicity.
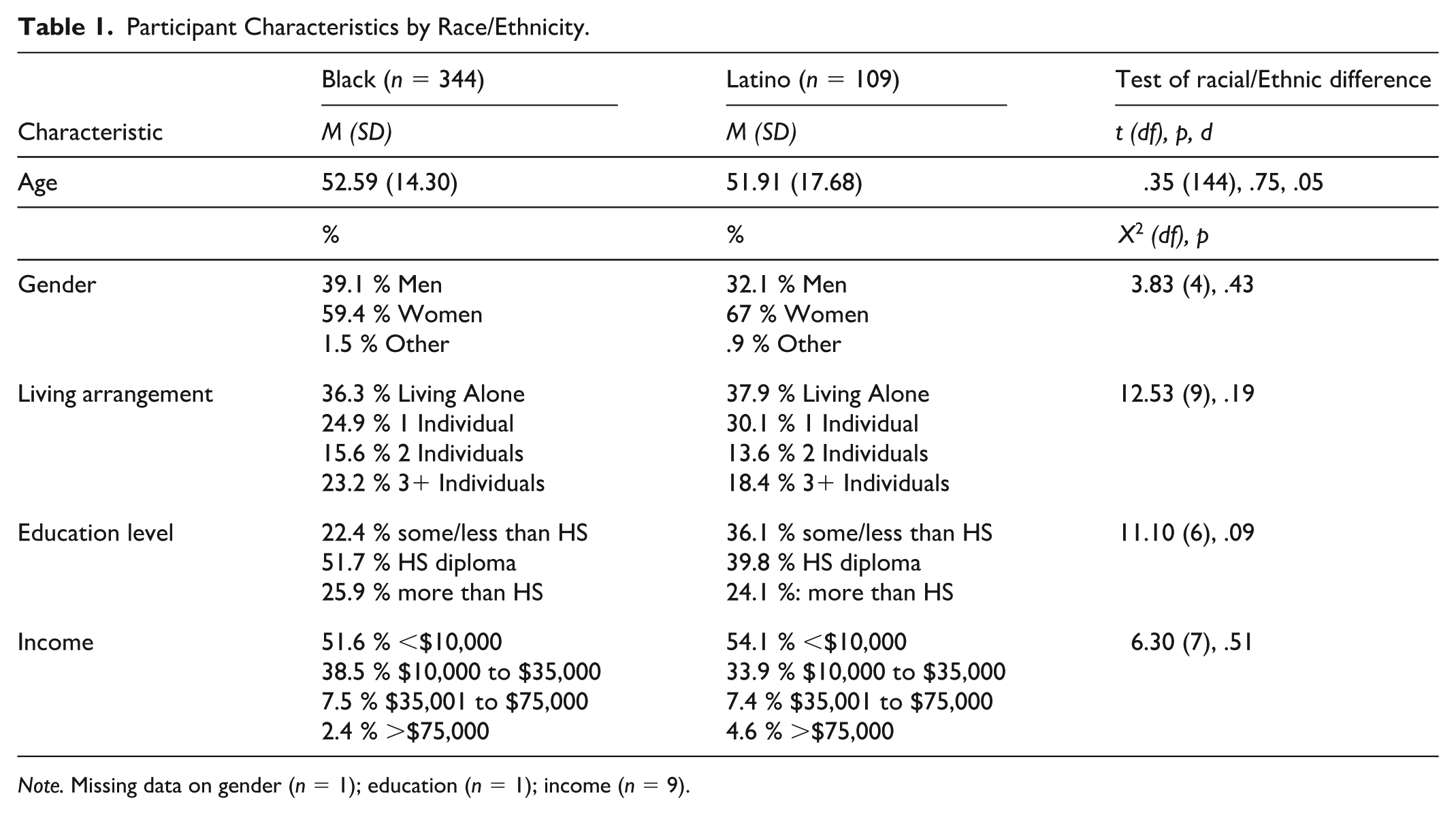
Note. Missing data on gender (n = 1); education (n = 1); income (n = 9).
Descriptive statistics for key variables stratified by race/ethnicity are presented in Table 2. Approximately one-third of individuals in both groups had mental health symptoms above the established clinical cutoff. The only significant racial/ethnic difference in key variables was for depressive symptoms, with Latino participants reporting higher levels of depressive symptoms than Black participants (t(446) = 2.13, p = .03, d = .25).
Means, Standard Deviations, Intercorrelations, and Racial/Ethnic Differences in Key Variables.
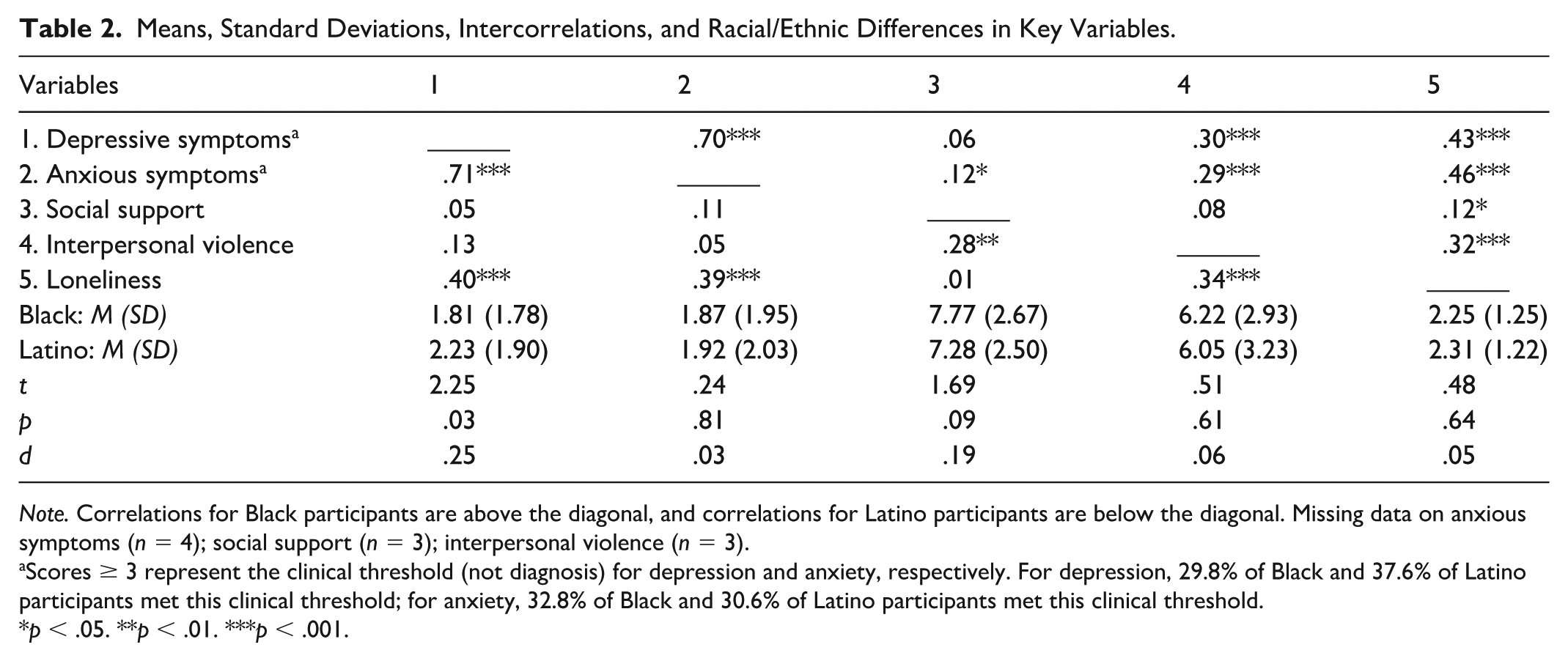
Note. Correlations for Black participants are above the diagonal, and correlations for Latino participants are below the diagonal. Missing data on anxious symptoms (n = 4); social support (n = 3); interpersonal violence (n = 3).
Scores ≥ 3 represent the clinical threshold (not diagnosis) for depression and anxiety, respectively. For depression, 29.8% of Black and 37.6% of Latino participants met this clinical threshold; for anxiety, 32.8% of Black and 30.6% of Latino participants met this clinical threshold.
p < .05. **p < .01. ***p < .001.
Depressive symptoms and anxious symptoms were positively and strongly associated for both Black and Latino participants. Social support-seeking exhibited a small, positive association with interpersonal violence for Latino, but not Black, participants. In contrast, social support-seeking exhibited a small, positive association with loneliness for Black, but not Latino, participants. Interpersonal violence exhibited a medium, positive association with loneliness for both racial/ethnic groups.
Interpersonal Experiences and Mental Health Symptoms
Findings for Hypothesis 1 are presented in Table 2 (the unadjusted models), stratified by race/ethnicity) and Table 3 (the adjusted models). In unadjusted models, social support-seeking was not significantly associated with depressive symptoms for either racial/ethnic group, but exhibited a small, significant positive association with anxious symptoms for Black participants only. In adjusted models, social support-seeking was not significantly associated with depressive or anxious symptoms.
Regression Analyses Examining Interpersonal Experiences in Predicting Mental Health Symptoms, with Race/Ethnicity as a Moderator.
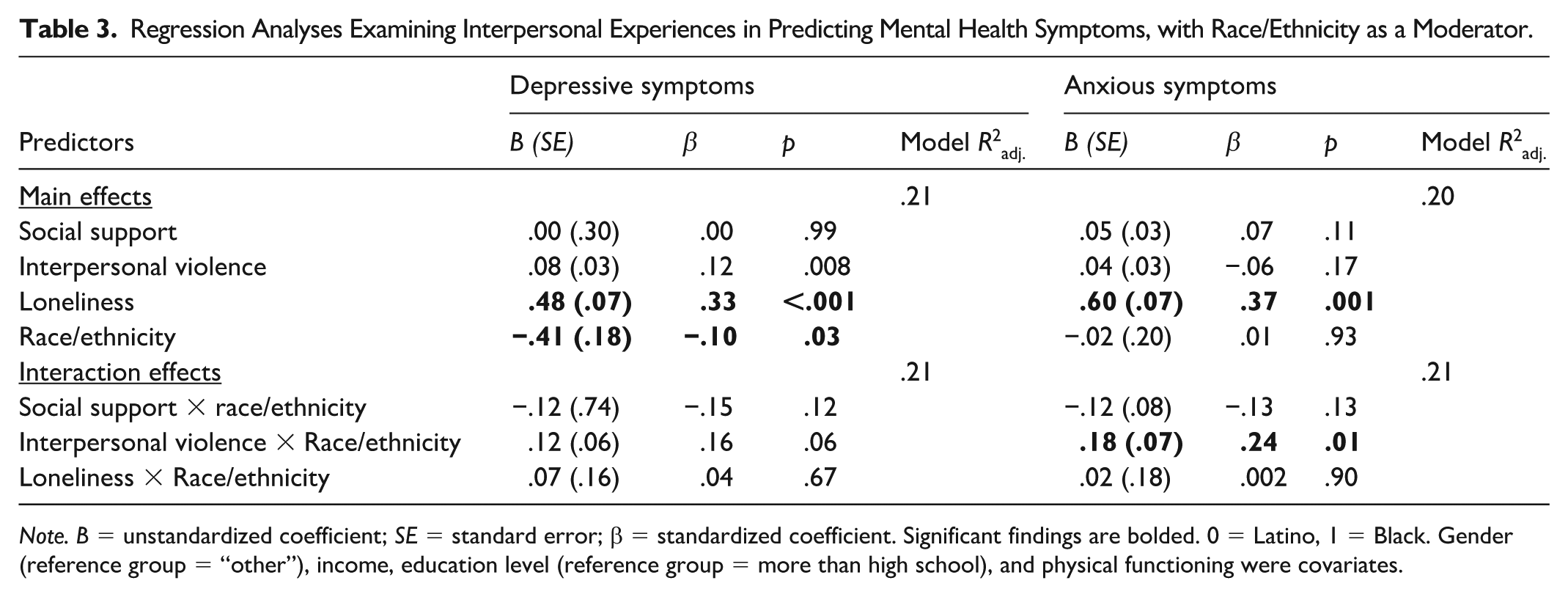
Note. B = unstandardized coefficient; SE = standard error; β = standardized coefficient. Significant findings are bolded. 0 = Latino, 1 = Black. Gender (reference group = “other”), income, education level (reference group = more than high school), and physical functioning were covariates.
In unadjusted models, interpersonal violence exhibited a small, positive association with both depressive and anxious symptoms for Black, but not Latino, participants. In adjusted models, interpersonal violence was significantly associated with depressive symptoms (β = .12, p < .008) but not anxious symptoms.
In unadjusted models, loneliness exhibited a medium, positive association with depressive and anxious symptoms for both racial/ethnic groups. In adjusted models, loneliness was a significant predictor of both depressive and anxious symptoms, with higher levels of loneliness associated with greater depressive symptoms (β = .33, p < .001) and greater anxious symptoms (β = .37, p < .001).
Differences by Race/Ethnicity
Findings for Aim 2 are presented in Table 3. Only one significant interaction emerged: the interaction between interpersonal violence and race/ethnicity in predicting anxious symptoms (β = .23, p = .009). Probing this interaction revealed that greater interpersonal violence was related to greater anxious symptoms among Black participants (simple slope = 0.10 (SE = .02), t = 4.25, p < .001), but there was no significant association among Latino participants (simple slope = −0.09 (SE = .06), t = −1.57, p = .14); see Figure 1. No significant interactions were found in predicting depressive symptoms, nor between race/ethnicity and social support-seeking or loneliness in predicting anxious symptoms.
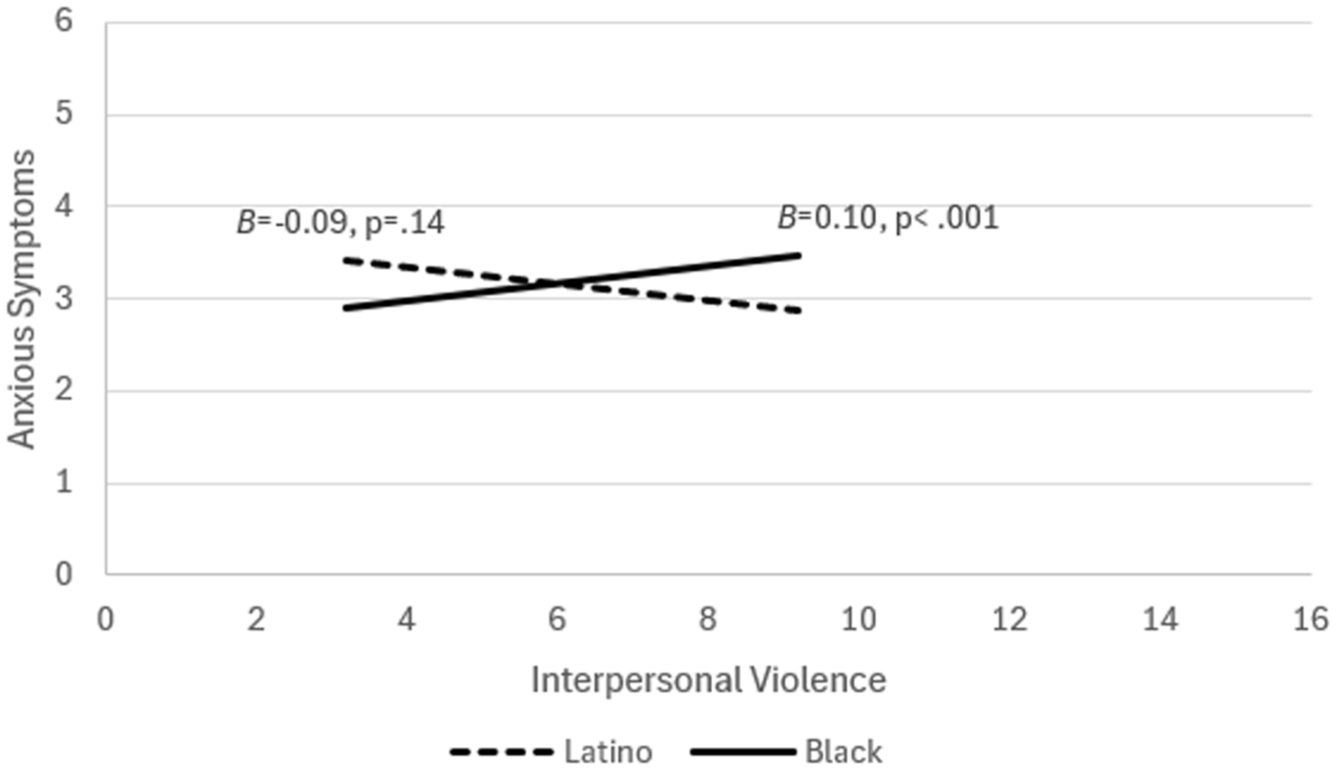
Interaction between interpersonal violence and race/ethnicity in predicting anxious symptoms.
Discussion
Consistent with Hypothesis 1a, loneliness was associated with greater depressive and anxious symptoms; interpersonal violence was associated with greater depressive and anxious symptoms for Black participants in unadjusted models, and with depressive symptoms only in adjusted models. In partial support for Hypothesis 1a, social support-seeking was associated with anxious symptoms only among Black participants in unadjusted models. Consistent with Hypothesis 1b, loneliness remained the strongest interpersonal predictor when all interpersonal variables were modeled together. Finally, in relation to our exploratory Aim 2, interpersonal violence was associated with anxious symptoms only among Black participants. These findings suggest that while loneliness appears to be a robust interpersonal risk factor across groups, other interpersonal processes may operate differently depending on sociocultural context.
Compared with national PHQ-8 and GAD-7 estimates – 8.1% and 6.9% among Black adults and 7.0% and 6.2% among Hispanic adults – our sample showed markedly higher rates of depression and anxiety (Terlizzi & Zablotsky, 2024). Our study focused on the assessment of symptoms during a short time period rather than clinical diagnoses. Findings of our study may reflect true elevations in symptoms tied to the socioeconomic challenges faced by our low-income sample. The only significant racial/ethnic difference in key variables that emerged was for depressive symptoms, with Latino participants reporting higher levels than Black participants, consistent with prior findings (Hargrove et al., 2020). However, a meta-analysis of 421 studies found higher pooled prevalence among Black adults (Cénat et al., 2025). This discrepancy may reflect differences in measurement (self-reported symptoms vs. diagnosed prevalence), cultural expression of distress, or contextual factors unique to the samples, suggesting that additional factors such as socioeconomic stressors, acculturation-related stress, or community support differences may contribute to these disparities.
No racial/ethnic differences were found in anxious symptoms, social support-seeking, interpersonal violence, or loneliness, suggesting that these risk and protective factors may be similarly distributed across groups due to shared socioeconomic disadvantage (Belle & Doucet, 2003; ODPHP, 2021). Structural barriers such as discrimination, limited health care access, and stigma around mental illness affect both communities (Grieb et al., 2023; Williams & Etkins, 2021). Both Black and Latino participants in our study were from a low-income community, a factor consistently linked to greater psychological distress due to financial instability/strain and limited access to mental health resources (Belle & Doucet, 2003; ODPHP, 2021). This idea is reflected in the relative lack of significant racial/ethnic differences observed in multivariate (versus bivariate) analyses after controlling for sociodemographic factors. These findings suggest that mental health screening should consider socioeconomic context and cultural expression of distress rather than assume uniform risk by race/ethnicity.
Social support-seeking was only significantly associated with anxious symptoms in unadjusted models – but in the opposite direction than expected and only for Black adults. This finding diverges from prior work highlighting the protective effects of social support (Almquist et al., 2016; Dour et al., 2013; Johnson-Esparza et al., 2021). One explanation may be related to measurement; in our study, social support-seeking was assessed by how often it was sought, rather than whether it was received or perceived as adequate and accessible. Most research demonstrating the protective effects of social support has assessed perceived or received support, whereas our study measured support-seeking behavior; these constructs are related but not interchangeable. Seeking social support was relatively infrequent in our sample; approximately 2/3 of participants reported seeking social support “not at all” or “a little bit,” on average. For Black and Latino adults, the benefits of social support often depend less on frequency of seeking and more on whether it is experienced as helpful within the context of supportive and high-quality relationships (Jacob et al., 2022; Lincoln et al., 2005).
The positive association we found may suggest reverse causation – i.e., Black adults with greater anxious symptoms may seek support more often. This unexpected finding could also reflect co-rumination or negative exchanges, whereby seeking support amplifies worry rather than alleviating it. Among Black adults, reliance on kin networks and obligations within stressed families may mean that seeking support can result in greater exposure to stress or yield mixed-quality interactions (Adu et al., 2025; Dalencour et al., 2016; de Crane & Spielberger, 1981).
Finally, the lack of associations in adjusted models suggests these dynamics are intertwined with sociodemographic and other interpersonal factors. Further, the lack of associations among Latino participants could be a function of the protective effects of familismo (Ayón et al., 2010). To help provide a greater understanding of the link between social support-seeking and mental health symptoms among these populations, future research would benefit from examining support quality, type of support, source, and racial/ethnic-specific mechanisms.
The findings for interpersonal violence reinforce past research that has also found interpersonal violence to be a significant predictor of poor mental health (Horne et al., 2020), Our findings align with earlier work showing heightened anxiety among Black adults exposed to interpersonal violence and extend this work by highlighting racial/ethnic variation in outcomes (Mitchell et al., 2006).
The stronger association among Black participants may reflect interpersonal violence co-occurring with unique stressors such as racialized violence, aggressive policing, and incarceration (Williams & Etkins, 2021), as well as stigma and reliance on kin networks that can both help and harm coping (Adu et al., 2025; Dalencour et al., 2016). Among Latino participants, familismo may buffer anxious symptoms through immediate reassurance of family members but not depressive symptoms (Ayón et al., 2010; Fedina et al., 2017). Anxiety’s future-oriented focus may make it more responsive to present family support, whereas depression, which is tied to past experiences and rumination, may be less easily mitigated (Alderman et al., 2015; Grupe & Nitschke, 2013). These findings highlight the need for clinicians to assess not only the presence of interpersonal violence but also its severity, context, and perceived impact. Clinicians should attend to both the nature of the violence and the cultural norms that influence how individuals cope with and interpret these experiences.
Consistent with prior research (Gabarrell-Pascuet et al., 2023), loneliness emerged as the strongest predictor of both depressive and anxious symptoms, suggesting it may be one of the most robust interpersonal indicators of mental health vulnerability in this population. Rather than the mere absence of social contact, loneliness reflects maladaptive perceptions, such as sensitivity to rejection and negative self-views, that perpetuate feelings of isolation even in the presence of social opportunities (Erzen & Çikrikci, 2018; NIA, 2024).
For low-income Black and Latino populations, chronic stressors such as financial insecurity, discrimination and neighborhood violence may reinforce these perceptions and deepen vulnerability to loneliness (Belle & Doucet, 2003; Williams & Etkins, 2021). Lower educational attainment, linked to fewer coping resources, may further exacerbate risk (Beller, 2024). In this study, no racial/ethnic differences emerged in the relationship between loneliness and mental health, suggesting that shared socioeconomic challenges outweighed cultural distinctions (ODPHP, 2021). Mental health stigma, common to both groups, may also reinforce perceived isolation despite available social networks (Dalencour et al., 2016).
Interventions targeting maladaptive cognitions, such as cognitive-behavioral approaches, may be more effective than strategies simply encouraging greater social contact (Beller, 2024). Among low-income Black and Latino communities, such interventions should address both cognitive and structural contributors to loneliness. Clinicians can help by screening for loneliness and referring patients to culturally responsive mental health services.
Limitations and Future Directions
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design prevents conclusions about causality or direction of effects; longitudinal designs are needed to clarify how interpersonal experiences and mental health influence one another over time.
Second, reliance on self-report measures raises the possibility of social desirability and recall biases. Incorporating multiple data sources, such as clinician assessments or reports from close others, could enhance reliability. This may be especially important for Black and Latino populations, as many mental health assessments were validated primarily among White adults, and cultural differences in symptom expression have been documented (General, 2001). In addition, health- or support-seeking behaviors may be shaped by culturally specific norms within Black and Latino communities. However, the present study was not designed to assess these cultural processes. Future research that explicitly measures culturally specific mental health experiences and support-seeking- norms within Black and Latino communities may help clarify cultural differences that were not detectable in the present analyses.
A further limitation is the lack of marital status and quality measures, which may clarify links between interpersonal experiences and mental health. For example, prior research has shown that married individuals report substantially lower loneliness than unmarried adults (e.g., Vedder et al., 2024). Future work should examine both marital status and relationship quality as potential moderators of the associations examined in the current study. Future research should consider other potential moderating factors (e.g., coping strategies) to also inform tailored interventions as well as perceived prejudice or “inability to get ahead.”
Inconsistencies in measurement timeframes also complicate interpretation. While mental health symptoms were assessed over the past 2 weeks, other variables (e.g., social support- seeking, loneliness) did not specify timeframes, making it unclear whether findings reflect stable traits or more transient states. Future research should align or distinguish these timeframes to clarify the nature of associations. In addition, loneliness was assessed using a single item, which did not allow differentiation between emotional loneliness (lack of close attachment) and social isolation (limited social network integration).
Finally, the use of broad racial/ethnic categories (i.e., “Black” and “Latino”) does not capture within-group heterogeneity. Future research should examine more nuanced ethnic subgroups and intersectional identities to better understand variability within these populations.
Implications for Transcultural Health Care
The findings inform transcultural health care practice with low-income Black and Latino adults. Because loneliness emerged as the strongest and most consistent predictor of both depressive and anxious symptoms, culturally responsive screening should move beyond symptom checklists to include assessment of social connectedness and perceived isolation. For Black adults, the heightened association between interpersonal violence and anxious symptoms underscores the need for trauma-informed approaches that recognize how chronic exposure to threat within close relationships and communities may manifest in hypervigilance and distress. For Latino adults, interventions that build on familismo and existing family networks while addressing relational conflict may help mitigate loneliness and its mental health consequences. Across both groups, clinicians should integrate culturally sensitive questions about relationship quality, safety, and belonging into routine care, and connect patients with community-based and culturally congruent supports that strengthen meaningful social ties.
Conclusion
In conclusion, this study highlights the importance of negative interpersonal experiences in shaping mental health outcomes among Black and Latino adults, even after accounting for sociodemographic and health covariates. The findings suggest that assessing these experiences may enhance the identification of mental health risk among low-income Black and Latino adults and support more culturally-targeted intervention efforts. By expanding research in this area, we can better inform interventions aimed at promoting well-being in underserved communities.
Supplemental Material
sj-docx-1-tcn-10.1177_10436596261452219 – Supplemental material for Interpersonal Experiences and Mental Health Among Low-Income Black and Latino Adults
Supplemental material, sj-docx-1-tcn-10.1177_10436596261452219 for Interpersonal Experiences and Mental Health Among Low-Income Black and Latino Adults by Mumin A. Rabgie, Kristin J. August, Mei R. Fu and Zeyuan Qiu in Journal of Transcultural Nursing
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board at Rutgers University.
Consent to Participate
Informed consent was obtained from all participants prior to data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Rutgers University Research Council Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Permission to Reproduce Material
This study did not reproduce any copyrighted material. The survey instruments (PHQ-2, GAD-2, Brief COPE items) are widely used, validated tools. No figures or tables were reproduced from other sources.
Clinical Trial Registration
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.