
Abstract
Introduction:
Children immigrating to the United States from Latin America experience cumulative stressors and trauma across the premigration, migration, and postmigration phases, placing them at increased risk for adverse mental health outcomes. This integrative review examined mental health outcomes associated with immigration-related trauma in Latin American immigrant children.
Methods:
Using Whittemore and Knafl’s framework, a systematic search of PubMed, CINAHL, and APA PsycINFO identified peer-reviewed English-language studies published between 2014 and 2026 involving children aged 0 to 18 years.
Results:
Ten studies met the inclusion criteria (five quantitative, two qualitative, and three mixed methods). Posttraumatic stress disorder occurred across all migration phases, while anxiety and depression were most common postmigration. Behavioral disorders and substance use, or risk-taking behaviors were also reported.
Discussion:
Cumulative migration-related trauma contributes to poor mental health outcomes. Trauma-informed, culturally congruent nursing assessment and interventions are critical to reduce long-term psychological morbidity.
Introduction
Thousands of children cross the United States border each year. Families with children and unaccompanied youth migrate for many overlapping reasons. These include extreme poverty, community violence, political instability, and family reunification. U.S. Customs and Border Protection reported 152,880 encounters with immigrant children nationwide in 2022 (Nationwide Encounters, 2023). Children from Latin America, also called Latinx, come from over 20 countries across Central America, South America, Mexico, and the Caribbean. This group is the fastest growing, rising from 9% in 1980 to 26% in 2022 (Childstats.gov, 2023). The term Latinx includes gender-neutral and non-binary individuals of Latin American descent (Chung et al., 2022). In this integrative review, we use Latinx as an umbrella term while recognizing diversity among Latin American immigrant children. Differences exist in nationality, country of origin, and legal status. Where possible, we detail these sample differences and acknowledge remaining heterogeneity as a limitation.
Children in this review are defined as individuals aged 0 to 18 years. Developmental stage is a key moderating factor in trauma response; younger children may demonstrate behavioral dysregulation and attachment disruption, whereas adolescents may exhibit internalizing symptoms, identity-related stress, and risk-taking behaviors (Stevens et al., 2016). Although many studies (Andrade et al., 2023; Cardoso, 2018; Chung et al., 2022; Cleary et al., 2017) aggregate age groups, developmental variability remains an important limitation in the current literature.
The phases of migration include premigration (home country), migration (journey), and postmigration (receiving country). Each phase poses different trauma risks. Trauma is defined as
an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life-threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being. (Miller et al., 2019, pp. 1–2)
During the premigration phase, children often face extreme poverty, physical and sexual abuse, neglect, abandonment, kidnapping, and interpersonal violence (Cardoso, 2018). During migration, children may encounter a dangerous journey into the United States. They can be exposed to starvation, physical abuse, rape, molestation, gang violence, extortion, kidnapping, and incarceration (Cardoso, 2018). After arrival, postmigration stressors include acculturative stress, prolonged detention, unstable housing, family reunification challenges, and difficulties in unfamiliar educational and legal systems (Cardoso, 2018; Cleary et al., 2017).
Trauma from each migration phase can accumulate over time. This pattern matches findings from studies of migrant and refugee children, which we reference as context rather than exact numbers for Latinx youth. A recent scoping review found patterns of emotional distress, internalizing symptoms, and behavioral problems among migrant children exposed to stressors before, during, and after migration (Andrade et al., 2023). A 2020 systematic review and meta-analysis among child and adolescent refugees and asylum seekers reported pooled estimates of about 23% for posttraumatic stress disorder (PTSD), 14% for depression, and 16% for anxiety. This highlights the large mental health burden in this population (Blackmore et al., 2020). The pooled estimates show the scale of mental health needs among children facing migration trauma, displacement, persecution, and forced migration.
Trauma exposure during migration is consistently linked to poor mental health outcomes (Cleary et al., 2017). Multiple traumas may cause new or worsening symptoms that last into adulthood. The most common outcomes are PTSD, anxiety, depression, behavioral disorders, substance use, and risk-taking behaviors. Research by De Arellano et al. (2018) showed that childhood trauma has a stronger and long-lasting link to adult mental health problems. This finding underscores the lasting effects of early immigration-related trauma. At any migration phase, children may face forced separation, violence without caregiver protection, detention, unstable living conditions, and acculturative stress. All these factors are associated with poorer mental health outcomes (Cleary et al., 2017; de Arellano et al., 2018). In one study, Cleary et al. (2017) found that two-thirds of 104 Latinx children had experienced at least one traumatic event: 59% in the home country, 20% during migration, and 18% after arriving in the United States.
Despite this growing body of literature, important gaps remain. What is insufficiently understood is how mental health outcomes vary across each phase of migration and how premigration and migration-related trauma contribute to psychological distress following resettlement. Although some studies address premigration and migration-phase trauma, much of the existing empirical work on Latinx immigrant children has focused on postmigration stressors, such as discrimination, acculturative stress, and reunification challenges, limiting a comprehensive understanding of early trauma exposure and its cumulative effects across the migration trajectory. Addressing this gap is critical to improving early identification, trauma-informed assessment, and timely intervention.
Importantly, not all children exposed to migration-related adversity experience negative outcomes. A growing body of literature highlights protective and resilience factors, including family cohesion, caregiver support, ethnic identity, and community belonging, which can buffer the effects of trauma (Masten, 2013; Ungar, 2013). Disruptions to these protective systems, such as family separation or social isolation, may increase vulnerability to adverse mental health outcomes.
This review is informed by a cumulative risk and developmental trauma framework, which posits that repeated exposures to adversity across time have additive and interacting effects on child development and mental health (Evans et al., 2013; Shonkoff & Garner, 2013). Within this framework, migration-related stressors are conceptualized as cumulative rather than discrete events, shaping psychological outcomes across the life course. Examining the current state of the science with an integrative review is both timely and relevant. Latinx immigrant children represent a large, understudied population whose premigration, migration, and postmigration trauma exposures are not fully captured in existing research. An integrative review is well suited for a study of mental Health Outcomes Associated with Immigration-Related Trauma of Latinx children because it enables the rigorous synthesis of varied methodologies and sources, providing a holistic perspective on the topic while strengthening the scholarly foundation and relevance of the work. Research identifying these outcomes is essential to inform and improve the quality, accessibility, and effectiveness of mental health services for this growing population. These gaps limit the development of targeted, culturally responsive mental health nursing interventions. Therefore, the purpose of this integrative review is to synthesize the existing literature on mental health outcomes associated with immigration-related trauma across the premigration, migration, and postmigration phases among Latinx children.
Method
Data Sources and Search Strategy
This integrative review followed the organizational framework described by Whittemore and Knafl (2005), which includes five stages: problem identification, literature search, data evaluation, data analysis, and presentation. A comprehensive search was conducted across PubMed, CINAHL, and APA PsycINFO databases using the following key terms: emigrant* OR migrant* OR immigrant* OR refugee* OR “asylum seeker” AND Hispanic* OR Latin* OR Mexican* OR “Central American” OR “South American” OR Cuban* OR “Puerto Rican” OR Spanish* OR Espanol* AND youth* OR adolescent* OR “young people” OR teen* OR child* OR kid OR kids AND trauma* OR anxiet* OR “emotional exhaustion” OR “psychological stress” OR depression* OR worry OR tiredness OR fear* OR panic* OR distress* OR “mental health” OR “well-being” OR “well being” OR “emotional health” OR “psychological health” OR suicid* OR PTSD OR “post-traumatic stress” OR “post traumatic stress” OR “physical health”. The search was limited to PubMed, CINAHL, and APA PsycINFO because they are the primary databases indexing peer-reviewed literature on child health, nursing, psychology, and mental health, and together provide broad coverage of medical, nursing, and behavioral science research relevant to Latin American immigrant children.
Articles were eligible for inclusion if they met the following criteria: (a) participants were first-generation immigrants born in Latin America; (b) participants were between birth and 18 years of age; (c) the study was published in English; (d) the article was peer-reviewed and available in full-text electronic format; and (e) the study focused on mental health outcomes related to immigration experiences (premigration, migration, or postmigration). Because immigration policies, patterns of child migration, and service systems have changed substantially over the past decade, we restricted the review to 2014–2026. This decision prioritized contemporary evidence most applicable to present-day clinical decision-making and policy debates, while also keeping the search and synthesis methodologically manageable. Exclusion criteria comprised studies focused on adults, research unrelated to immigration or mental health outcomes, literature reviews, editorials, poster presentations, and book reviews.
The initial database search yielded 983 articles. After removing duplicates and screening titles and abstracts, 71 articles were assessed for eligibility based on the inclusion and exclusion criteria. Sixty-two articles were subsequently excluded, leaving 10 studies that met all criteria. The PRISMA flow diagram illustrating the selection process is presented in Figure 1.
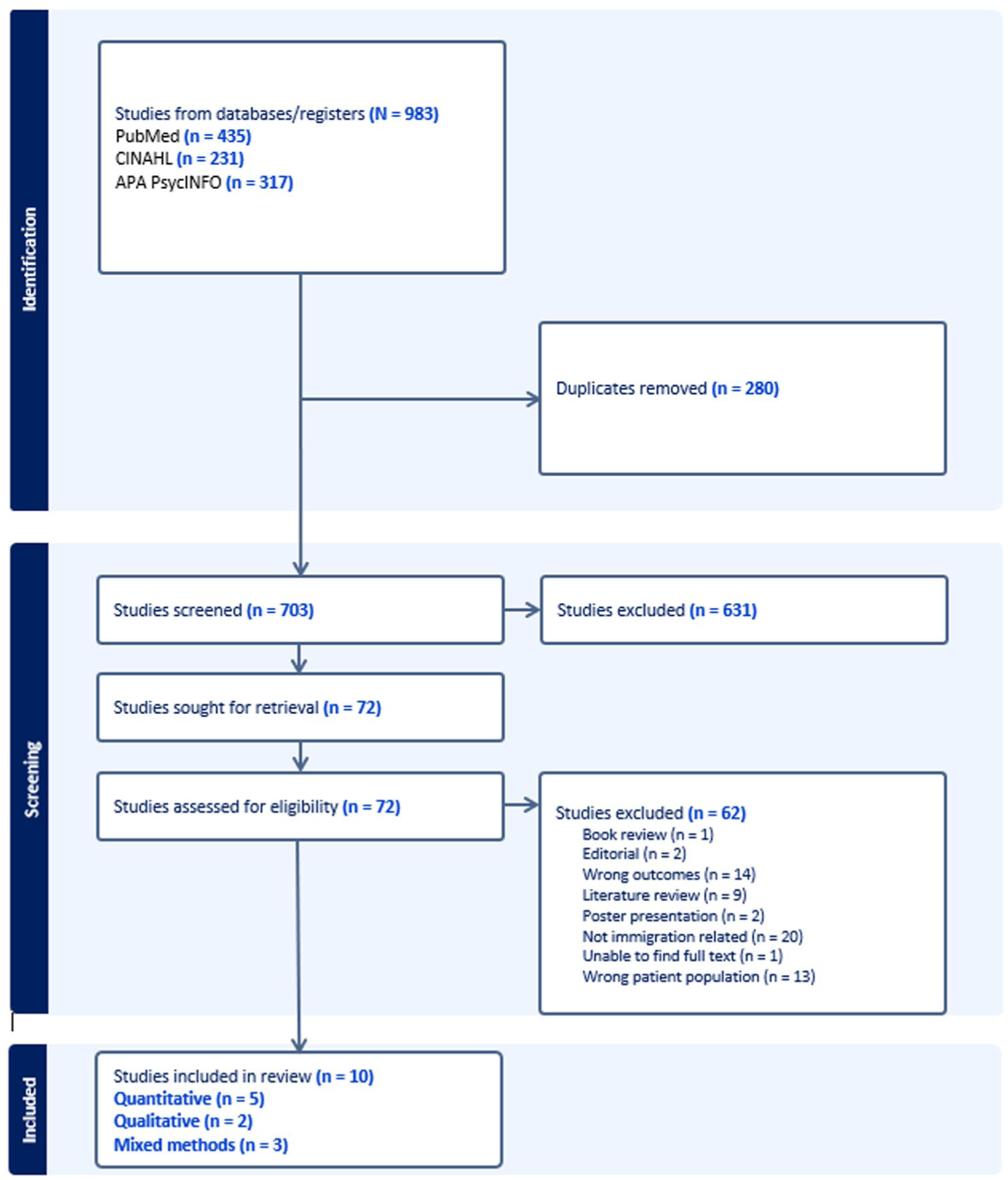
PRISMA flow diagram.
Data Extraction
Data extraction was conducted systematically to ensure consistency and methodological rigor across included studies. For each article, key information was extracted using a standardized data extraction matrix, including author(s), year of publication, study design, sample characteristics (age, country of origin, immigration status when available), migration phase(s) examined (premigration, migration, postmigration), measures or instruments used, mental health outcomes assessed, and key findings relevant to immigration-related trauma. Extraction also captured contextual factors such as family separation, detention, acculturation stressors, and discrimination when reported. This structured approach facilitated comparison across studies and supported the identification of recurring patterns and phase-specific mental health outcomes.
Analysis
Articles were analyzed using a constant comparison method: data reduction, data display, data comparison, conclusion drawing, and verification (Glaser & Strauss, 1967). An annotated bibliography was created during the data reduction phase of the review. Objectives, measures, methods, and key findings are presented in Table 1 to facilitate the review of the extracted data.
Immigration-Related Mental Health Outcomes in Children From Latin America.
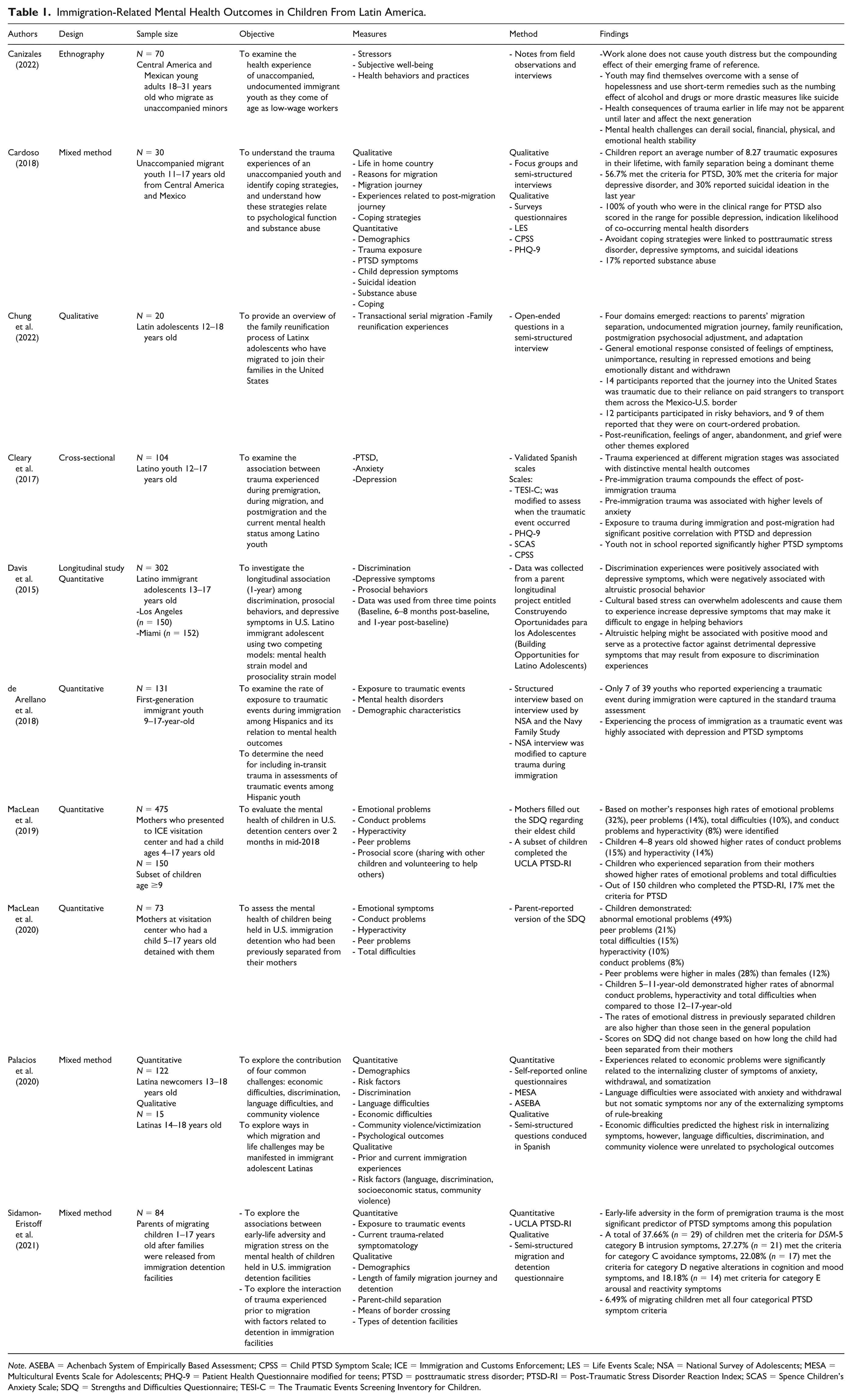
Note. ASEBA = Achenbach System of Empirically Based Assessment; CPSS = Child PTSD Symptom Scale; ICE = Immigration and Customs Enforcement; LES = Life Events Scale; NSA = National Survey of Adolescents; MESA = Multicultural Events Scale for Adolescents; PHQ-9 = Patient Health Questionnaire modified for teens; PTSD = posttraumatic stress disorder; PTSD-RI = Post-Traumatic Stress Disorder Reaction Index; SCAS = Spence Children’s Anxiety Scale; SDQ = Strengths and Difficulties Questionnaire; TESI-C = The Traumatic Events Screening Inventory for Children.
Results
A total of 10 studies were included in this review (Table 1): five quantitative (Cleary et al., 2017; Davis et al., 2015; de Arellano et al., 2018; MacLean et al., 2019, 2020), two qualitative (Canizales, 2022; Chung et al., 2022), and three mixed-methods studies (Cardoso, 2018; Palacios et al., 2020; Sidamon-Eristoff et al., 2021). Three studies incorporated parent perspectives (MacLean et al., 2019, 2020; Sidamon-Eristoff et al., 2021). In addition, one study utilized adult participants who reflected on their own childhood migration experiences (Canizales, 2022).
Premigration Phase
Across studies, premigration trauma was both widespread and strongly associated with later PTSD symptoms among Latinx immigrant children (Cardoso, 2018; Cleary et al., 2017; Sidamon-Eristoff et al., 2021). Latinx children seeking to migrate to the United States had high rates of premigration exposure to abuse, neglect, sexual assault, kidnapping, and community-based violence, frequently perpetrated by police or transnational gangs (Cardoso, 2018).
Cumulative trauma in childhood, rather than adult trauma exposure, was associated with higher PTSD symptom severity, indicating that early adversity is a critical predictor of mental health risk (Cleary et al., 2017; de Arellano et al., 2018; Sidamon-Eristoff et al., 2021). For example, Sidamon-Eristoff et al. (2021) reported that nearly all children in detention had experienced at least one premigration traumatic event and that substantial proportions met criteria for Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) intrusion, avoidance, negative alterations in cognition and mood, and arousal and reactivity symptom clusters (Sidamon-Eristoff et al., 2021). Premigration trauma was also linked with elevated anxiety, although these symptoms were less consistently emphasized than PTSD in the premigration context (Cleary et al., 2017).
Migration Phase
Across studies that assessed trauma occurring during migration, the journey itself emerged as a significant source of acute, life-threatening stressors, including starvation, physical abuse, sexual violence, gang and cartel violence, extortion, kidnapping, and incarceration (Cardoso, 2018). Exposure to traumatic events during immigration showed significant positive correlations with PTSD symptoms and was also associated with depressive symptoms, even when accounting for other trauma types (Cleary et al., 2017; de Arellano et al., 2018).
Immigration-related trauma was also frequently under-identified using standard assessment tools, with one study reporting that only seven of 39 migration-related traumatic events were captured (de Arellano et al., 2018). Findings suggest that failure to assess migration-specific trauma may contribute to underestimation of psychological distress in immigrant youth.
Studies of recently migrated youth consistently reported high self-reported PTSD symptom levels, indicating that migration-phase adversity compounds premigration trauma and contributes to substantial psychological distress soon after arrival (Cardoso, 2018; MacLean et al., 2019).
Postmigration
Anxiety and Depression
In the postmigration phase, anxiety and depressive symptoms were most closely associated with ongoing stressors such as economic hardship, language barriers, discrimination, and challenges with acculturation and reunification (Canizales, 2022; Chung et al., 2022; Davis et al., 2015; Palacios et al., 2020). Among newcomer Latina adolescents, economic strain during settlement in the United States was significantly associated with internalizing clusters of anxiety, withdrawal, and somatization (Chung et al., 2022; Palacios et al., 2020). Persistent financial difficulties and limited future prospects were described as contributing to ongoing anxiety and emotional distress (Canizales, 2022; Palacios et al., 2020).
Language difficulties were associated with anxiety and withdrawal, but not externalizing symptoms, and were linked with social isolation and difficulties engaging in mainstream activities (Palacios et al., 2020). These patterns of isolation and withdrawal were described as contributing to poor acculturation and increased postmigration stress (Palacios et al., 2020).
Immigration-related stressors and limited coping resources were consistently associated with depressive symptoms among Latinx immigrant youth (Cardoso, 2018; Davis et al., 2015). Discrimination emerged as a prominent postmigration stressor, with longitudinal data indicating that discrimination experiences were positively associated with depressive symptoms (Davis et al., 2015). Higher levels of depressive symptoms were linked to patterns of chronic sadness, withdrawal, and isolation in unaccompanied youth (Cardoso, 2018; Davis et al., 2015). In one sample of unaccompanied immigrant youth, approximately one-third met the criteria for major depressive disorder, and one-third reported suicidal ideation in the previous year, underscoring the severity of postmigration depressive symptoms in some subgroups (Cardoso, 2018). Depression scores were also elevated among children in the clinical range for PTSD, suggesting a high burden of co-occurring mental disorders (Canizales, 2022; Cardoso, 2018; Cleary et al., 2017).
Behavioral Disorders, Substance Use, and Risk-Taking
According to studies, behavioral disorders in children were most often described in the context of family disruption, especially forced separation and later reunification in the receiving country (MacLean et al., 2019, 2020). Children who had been held in an immigration detention center and subsequently reunited with their mothers demonstrated high rates of emotional problems, peer problems, hyperactivity, and conduct problems, with younger children showing particularly elevated conduct and hyperactivity scores (MacLean et al., 2019, 2020). Emotional distress among previously separated children exceeded that observed in the general population, and these difficulties were noted regardless of the duration of separation (MacLean et al., 2020).
Substance use and risk-taking behaviors were also primarily reported during the postmigration phase and were frequently linked to feelings of emptiness, longing for caregivers, and a sense of being unimportant following reunification (Canizales, 2022; Chung et al., 2022). In one study of Latinx adolescents, these emotional responses were followed by engagement in risky behaviors for a majority of participants, with nearly half reporting court-ordered probation (Chung et al., 2022). Some youth described using alcohol and illicit drugs as short-term strategies to manage hopelessness and emotional numbness after migration, particularly when family relationships and identity development were strained (Canizales, 2022).
Discussion
Findings from this integrative review show that mental health outcomes among Latin American immigrant children follow a clear phase pattern: PTSD is present across premigration, migration, and postmigration, whereas anxiety, depression, and behavioral problems cluster more heavily after resettlement (Canizales, 2022; Cardoso, 2018; Cleary et al., 2017; Davis et al., 2015; MacLean et al., 2019, 2020; Palacios et al., 2020; Sidamon-Eristoff et al., 2021). These phase-specific differences may be explained by the nature and timing of stress exposure: acute and life-threatening trauma early in the migration trajectory is more likely to elicit PTSD symptomatology, whereas chronic, ongoing stressors encountered after resettlement may erode coping capacity over time, manifesting as anxiety and depressive symptoms. This pattern is consistent with cumulative risk and developmental trauma frameworks, which posit that repeated exposures to adversity over time have additive and interactive effects on neurobiological development and stress regulation (Evans et al., 2013; Shonkoff & Garner, 2013).
In addition, these findings align with work in other forcibly displaced children, where pooled prevalence estimates for PTSD, depression, and anxiety highlight the substantial symptom burden associated with displacement and persecution (Blackmore et al., 2020). At the same time, children in this review face distinct threats, including cartel and gang violence, extortion, and U.S. immigration detention that differ from trauma profiles described in children displaced by war or large-scale political conflict (Cardoso, 2018; MacLean et al., 2019, 2020; Sidamon-Eristoff et al., 2021). These findings suggest that although overall symptom patterns are similar to those observed in refugee youth globally, the specific trauma experiences and policy contexts shaping Latinx children’s lives require responses that are tailored to their unique context.
A second notable finding is the strong association between family disruption and the development of behavioral disorders and risk-taking behaviors among immigrant children and adolescents. Behavioral disorders were particularly prevalent among children who experienced forced separation from parents or caregivers, underscoring the profound psychological consequences of disrupted attachment and caregiving relationships (MacLean et al., 2019, 2020). Substance use and risk-taking behaviors also emerged primarily in the postmigration phase, often in the context of family reunification challenges and identity-related stressors during adolescence (Canizales, 2022; Chung et al., 2022). A plausible explanation is that separation and reunification disrupt attachment security and family role expectations during critical developmental periods, producing anger, mistrust, and impaired emotion regulation that may be expressed through acting-out behaviors, substance use, or affiliation with high-risk peer groups, particularly when adolescents are simultaneously navigating acculturative stress and discrimination in the receiving country.
Taken together, embedding these phase-specific findings within cumulative risk and developmental trauma frameworks points to the need for multilevel, developmentally informed interventions that address trauma before, during, and after migration. It also underscores that Latinx immigrant children’s experiences overlap with those of other migrant and refugee populations, yet remain shaped by distinct regional, political, and policy contexts, with important implications for how systems design assessment, prevention, and treatment efforts (Blackmore et al., 2020; MacLean et al., 2020; Miller et al., 2019).
Implications for Practice
Cumulative trauma during any phase of migration will compound its effect and put children at risk for co-occurring mental health disorders. Nurses and other health care providers need to recognize and be aware of the high prevalence of mental health disorders in Latinx immigrant children and remain attentive to how risk may differ across premigration, migration, and postmigration. Assessment of trauma experienced across the immigration process is necessary to understand the context and determinants of mental health outcomes, and immigration-specific items are needed to capture trauma exposure among immigrant children, regardless of the time spent living in the United States. In practice, this may include routine use of brief, culturally adapted trauma screens, asking explicit questions about premigration, journey, and postmigration stressors, and incorporating questions about detention, separation, and reunification into standard history taking. Nurses and mental health providers need to remain knowledgeable about current immigration policies and political trends related to family reunification, residency, visa statuses, and immigration in their states (Chung et al., 2022).
Developing interventions for immigrant youth that balance past trauma with current acculturation stressors within the context of a new language and culture is a challenge (Cleary et al., 2017). Trauma-informed approaches can include providing education about common trauma responses, teaching basic emotion-regulation techniques and grounding skills, and coordinating with community agencies that offer bilingual services for immigrant youth. Health policies should include multisector and context-specific mental health programs to address the needs of immigrant children, particularly at the time of arrival, and to ensure timely referral to the appropriate services. Furthermore, developmentally appropriate and culturally sensitive interventions should be implemented in schools and health care facilities to provide early intervention and improve the well-being of young immigrants (Cardoso, 2018).
The findings of this review support the importance of a comprehensive assessment, treatment, and the need for multilevel interventions for young immigrants who have experienced a range of immigration-related trauma. This review can serve as a starting point for validating the need for expanded mental health resources and for evaluating and coordinating services for this vulnerable population.
Implications for Future Research
This review’s findings also have implications for future research. Research should focus on exploring the relationships between each stage of immigration trauma (premigration, during migration, and postmigration) and mental health outcomes. Subsequent studies should use national samples of immigrant youth, thereby allowing greater representation of the diverse Latinx immigrant populations in the United States. Considering that one in three immigrant youth reported immigration trauma, and few of those traumatic events were captured in standard trauma assessment (de Arellano et al., 2018), future studies should examine trauma assessment tools and their cultural adaptations. In addition, because cross-sectional data do not allow for inference of directionality, longitudinal studies should explore the causal relationship between immigration trauma and proposed mental health outcomes. Finally, subsequent studies should explore the relationship between immigration trauma as a possible explanatory factor in mental health differences between immigrant children and U.S.-born children.
Limitations
Despite these implications, this study has limitations. This literature review was restricted to three databases, PubMed, CINAHL, and APA PsycINFO, so relevant studies indexed elsewhere or in the gray literature may have been missed. Much of the literature focuses on post-immigration and resettling challenges, such as acculturation and reunification. This leaves gaps in the research of premigration and during migration trauma-related mental health outcomes that can lead to delays in the identification and proper referral.
The lack of research within the last 12 years was also identified; several studies cited research over 12 years old and were therefore not current with the present political climate. Also, most studies used convenience and snowball sampling; these techniques can inflate the sample’s homogeneity, limiting the generalizability of the mental health outcome. Although this review included children from Latin America, most of the samples were from Central America and Mexico, suggesting the results may not represent other regions of Latin America. Furthermore, the majority of the studies reviewed were cross-sectional; therefore, they were unable to answer the causality relationship between traumatic events, PTSD, anxiety, depression, behavioral disorder, substance abuse, and risk-taking behavior. Finally, this review was conducted by a single reviewer, which may have introduced selection or extraction bias despite the use of a structured, transparent review process.
Conclusion
This integrative review underscores the critical importance of assessing trauma across all phases of the immigration process to better understand the contextual and cumulative factors influencing mental health outcomes among immigrant children from Latin America. Exposure to immigration-related trauma is strongly associated with adverse outcomes, including PTSD, anxiety, depression, and behavioral disorders. Notably, limited research has focused on the premigration and migration phases, despite their potential to provide essential insight into early trauma exposure and opportunities for timely intervention before the onset of postmigration stressors. Early identification and intervention during these phases may reduce the compounding effects of trauma across the immigration trajectory.
PTSD emerged as the most prevalent mental health outcome affecting this population, highlighting the need for prompt, trauma-informed assessment and diagnosis to support healthy developmental transitions into adulthood. Given the ongoing political shifts and sustained influx of immigrant children entering the United States, updated research is urgently needed to reflect current immigration policies, contexts, and service needs. As thousands of Latin American children arrive in the United States each day, increased awareness of common mental health outcomes can better equip nurses and other health care providers to deliver targeted assessments, timely referrals, and culturally responsive interventions that address the unique needs of this vulnerable population.
Footnotes
Authors’ Note
All identifying information related to the authors, institutions, funding sources, and approval bodies has been confined to this title page to preserve anonymity during the peer-review process.
Ethical Considerations
Ethical approval and informed consent were not required for this study as it is an integrative review of previously published literature.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.