
Abstract
In 2014, the U.S. Centers for Medicare & Medicaid Services (CMS) launched the Home and Community-Based Services (HCBS) Final Rule intended to improve the quality of HCBS for people with disabilities. The Rule focuses on improving outcomes through person-centered services and supports. These outcomes include privacy and dignity. This study reviewed state compliance with the Final Rule by examining statewide transition plans and investigating the Final Rule’s impact on privacy outcomes of adults with intellectual and developmental disabilities (IDD). We compared cross-sectional National Core Indicators® (NCI®) Adult Consumer Survey (ACS) 2012 to 2013 and Adult In-Person Survey (IPS) 2018 to 2019 data. Privacy (people letting them know before entering their home; being alone with friends/visitors at home) increased after Final Rule implementation. Individuals in the 2018 to 2019 group had 36% and 29% higher odds of being asked for permission to enter their home and of being alone with friends/guests, respectively. Age, gender, severity of intellectual disability, and several co-occurring conditions were also predictive of improvement in privacy.
Keywords
Most people with intellectual and developmental disabilities (IDD) who access U.S. community-based supports and services receive Home and Community-Based Services (HCBS) waiver-funded. Approximately 4.6 million individuals in the United States received HCBS with combined state and federal funding of $82.7 billion in 2017 (Musumeci et al., 2019). People with IDD typically receive their HCBS through the Section 1915 (c) waivers. Progress has been made in the United States in respecting the rights of people with disabilities, but many rights violations have been reported (Conrad, 2020). In 2014, the Centers for Medicare & Medicaid Services (CMS) issued the Final HCBS Rule (hereafter the Rule) designed for states to provide services so that they enhance community inclusion and respect for the human and civil rights of people with IDD.
Home and Community-Based Services Final Rule
Issued in January 2014, the Rule has been an important step toward improving the lives of people with disabilities receiving HCBS. The Rule’s intent was to provide guidance on maximizing access to living in the community, including receiving services in the most integrated settings. This policy was enacted to ensure that Medicaid funding met its obligations under the Americans with Disabilities Act (ADA, 1990) and the Supreme Court decision in Olmstead v. L.C., 527 U.S. 581 (Ginsburg & Supreme Court of the United States, 1998), and that service provider agencies achieve quality life outcomes. The Rule applies to all settings funded under Medicaid HCBS “authorities,” including the 1915 (c) Home and Community-Based Services (HCBS) waiver, 1915 (i) HCBS state plan option, 1915 (k) Community First Choice, and Section 1115 waiver. Settings include both nonresidential (e.g., adult day services) and residential (e.g., group homes). The Rule emphasizes autonomy, privacy, dignity, respect, meaningful community inclusion, and choice in HCBS.
Under the Rule, states were required to submit statewide transition plans (STPs) for approval to CMS (The Arc, 2014; Riesen & Snyder, 2019). The plans had to specify how each state will assess the extent to which its regulatory requirements ensure that settings, where people with disabilities receive services, comply with the Rule and describe steps toward compliance with these requirements, including timelines and deliverables. First, states submitted a plan for initial approval. Upon review, CMS either accepted the plan as proposed or requested clarifications/modifications. Upon approval of the revisions, the state plan is fully approved by CMS. As part of the approval process, each state is further required to identify settings that received institutional Medicaid funding. These settings subsequently undergo a heightened scrutiny evaluation to determine whether their approach to supporting people with disabilities complies with the Rule.
The original 2019 deadline for transition plan approval was extended first to 2022, and later to March 2023 (Friedman, 2020). As of September 2024, all but one state had received final approval from CMS for their transition plan. The remaining state had received initial approval and was working on accomplishing remaining milestones (Centers for Medicare & Medicaid Services [CMS], n.d.).
Privacy
The Rule includes guidance on the privacy of HCBS recipients, stating that the setting “ensures the individual has privacy in their sleeping or living unit including lockable doors” (Riesen & Snyder, 2019, p. 16). The setting should ensure that the resident controls their privacy and can opt to lock their bedroom door and the front door. Unless identified as a modification due to a specific individual need, staff should only access the person’s bedroom/unit to address health and safety concerns. In such cases, staff should request entry to a tenant’s bedroom/unit by knocking or requesting permission to enter. A person receiving HCBS has a right to have visitors, including family and friends, in a private space that is not a designated common area to be able to develop meaningful relationships.
Literature
Most definitions of privacy include the opportunity to be free from being observed or disturbed by other people. There are many contexts for privacy among people with IDD. This includes physical privacy or having spaces available to be away from others. Long and Averill (2003) cite many benefits of having time alone, including an opportunity for solitude, a sense of freedom, space for creativity, and uninterrupted time for spiritual activities. The lack of physical privacy also presents barriers regarding sexual intimacy. Evans et al. (2009) found that 25% of direct support professionals (DSPs) and 26% of family members were opposed to allowing people with IDD privacy with another person for fear of sexual activities. Furthermore, 69% of DSPs and 57% of family members felt that staff should notify families of intimate relationships, something not acceptable for people without disabilities.
McCarron et al.’s (2019) systematic review of deinstitutionalization found that moving to the community resulted in increased personal space and privacy, resulting in improved quality of life. Even so, Charitou et al.’s (2021) literature synthesis found that people with intellectual disabilities (ID) reported multiple organizational barriers and restrictions to sexual expression, such as limited privacy and strict regulations. Similarly, Hollomotz’s (2008) study on sexual relationships of people with intellectual disability (ID) in U.K. group homes reported that many homes did not provide private space in which they could explore sexual relationships in a safe and dignified manner.
Prohn et al. (2022) used U.S. National Core Indicators® (NCI) data to examine the relationship between privacy rights, community participation, everyday choice, and expanded friendships. They found the strongest association between privacy and everyday choice, arguing that if a setting (e.g., residential) has a culture of respect and access, then people will likely experience both the right to choose and the right to privacy.
People with IDD sometimes choose to keep information about their disability or support needs private (Evans, 2017; Harris, 2020). This may help avoid stigma and discrimination when applying for jobs, or even when developing a new friendship (Rocco, 2001). Living in segregated facilities for people with disabilities makes maintaining such privacy difficult.
Privacy may entail risks. There may be concerns about safety when left alone. Thus, many DSPs and family members let perceived risk overshadow the opportunities that come as people with IDD exercise greater control (Wiesel et al., 2020). For example, Stancliffe et al. (2022) found that 41.8% of U.S. adults with IDD were never allowed to stay home when others in their homes went out. Using smart-home technologies and providing training on what to do in an emergency can help alleviate these concerns (Stancliffe et al., 2022).
Brand et al. (2019) surveyed people with disabilities’ privacy concerns about smart-home technologies. Their findings were as follows: (a) smart-home data need to be stored in a way that ensures client privacy; (b) smart-home residents should be able to meet remote staff in person, making the technology less invasive; and (c) video cameras overlooking bedroom and bathroom entrances were of the greatest concern.
People with IDD may need support to learn what information is best to be kept private when independently using social media (Chalghoumi et al., 2019), or making online purchases.
In emergencies, people with IDD may not have their privacy respected, such as a physician sharing information with a DSP or family member that they would not share about a nondisabled patient (Rubin Law Firm, 2021). People with IDD may not be told “bad news,” such as their cancer diagnosis, that others in their lives are privy to (Tuffrey-Wijne et al., 2013). This is especially important because it often leads to people not being included in decisions about their own treatment plans (Tuffrey-Wijne et al., 2010). Privacy is protected as a human right for all people, including those with disabilities according to the Convention of the Rights of Persons with Disabilities (CRPD; United Nations, 2006, Article 22).
Study Purpose
This study’s purpose is to examine the impact of the implementation of the Rule on the experience of privacy of people with IDD receiving HCBS. We compare the privacy results from 2012 to 2013 and 2018 to 2019 NCI’s cross-sectional datasets. A related contextual purpose is to learn about the extent to which STPs are compliant with the Rule with respect to privacy. The research questions are as follows:
These research questions are being answered in the context of information reviewed in the state plans for compliance with the Rule specifically related to privacy issues.
Method
First, we reviewed the transition plans of the participating states to gain a more in-depth understanding of the extent to which these states addressed privacy issues as outlined in the Rule (e.g., being able to lock doors, securing space for personal items, etc.). This review provided an important policy context that assisted us with the interpretation of the National Core Indicator–In-Person Survey (NCI-IPS) results.
Review of STPs
We utilized information about STPs from the Medicaid.gov (https://www.medicaid.gov/medicaid/home-community-based-services/statewide-transition-plans/index.html) webpage. In early 2021, we reviewed state plans for all but two (their plans could not be located) of the 21 states that are included in the NCI portion of the study. For these 19 states, we examined state compliance with privacy issues, initial state actions to improve compliance, and tools the states developed for providers to assess their own compliance with the Rule (in our case specifically the items related to privacy).
Sample
State Selection
From 2012 to 2013, NCI data were collected from 25 states (National Core Indicators [NCI], 2014) and from 2018 to 2019 from 37 states (NCI, 2019a). To compare the results between both time points, the same states needed to participate in both survey cycles. Random selection of participants each year meant data were of different participants at the two time points. Twenty-one states were included in the final analyses, including 4 with final approval from CMS (AR, KY, OR, UT), 15 with initial approval (AL, CT, FL, GA, HI, IN, MO, NC, NH, NY, OH, PA, SC, VA, WI), and 2 with no approval (NJ, TX). From 2018 to 2019 NCI-IPS data were used, and approval status was determined based on June 30, 2019, which was the end of that NCI data collection period. The NCI-IPS (formerly known as the Adult Consumer Survey [ACS]) is a component of a national NCI initiative focused on quality enhancement/assurance of state DD systems. The initiative is a collaboration between the National Association of State Directors of Developmental Disabilities Services, the Human Services Research Institute, and participating state DD systems.
Within-State Sample Selection
Random selection of participants was implemented within each state’s population of adults age 18 years or older, and receiving home-based, community, or institutional services through the state DD system or receiving some subgroup of these to determine the state samples. Some states placed additional restrictions on their samples (e.g., recipients of HCBS only). For each state’s specific sampling strategy, see Appendix C in NCI’s 2012 to 2013 ACS Final Report (NCI, 2014) and Appendix B in NCI’s 2018 to 2019 IPS Final Report (NCI, 2019b). From 2012 to 2013, state sample sizes varied from 212 (HI) to 976 (PA) with an average of 367. From 2018 to 2019, state samples ranged from 164 (HI) to 1,427 (TX) averaging 441.
Instrument
Two versions of the same instrument were used for this study: the 2012 to 2013 NCI-ACS and the 2018 to 2019 NCI-IPS. The NCI data are the only quasi-national data on adults with IDD using HCBS IDD services. The 2012 to 2013 survey provided the most recent data before the Rule was promulgated in January 2014. The 2018 to 2019 NCI data was the most recent available data not affected by the pandemic. COVID-19 may have affected privacy practices and behavior. Additionally, COVID-19 impacted the 2019 to 2020 NCI data collection methods. The IPS is typically conducted face-to-face, but other modes were used due to the pandemic.
The 2012 to 2013 NCI-ACS has three sections. Data from all three sections were used in the study. The background information (BI) section includes questions about the participant’s personal characteristics, diagnoses, functioning capacities, health issues, service usage, employment, and residential status. These data come from existing administrative data. State data records, case managers or setting administrators, direct support providers, and sometimes family members or individual service recipients are the sources of these data. Section 1 asks about daily activities, home life, safety, friends and family, and satisfaction with services and supports. This information is obtained directly from the person receiving services. Section 2 seeks information on community inclusion, choice, rights (including privacy), and access to services. Information may be provided by the person receiving services or by a proxy (e.g., family/friend, staff, or other individual; NCI, 2014). From 2018 to 2019, the study used data from two of the three sections of the 2018 to 2019 NCI-IPS. The sources for these data are the same as described above. Both survey years required survey interviewers to participate in an NCI training program to ensure a consistent understanding of the survey and data collection procedures (NCI, 2014, 2019a).
Participants
The 21 states appearing in both survey years had randomly selected samples of 11,079 (2012–2013) and 13,467 (2018–2019). Regarding Rule approval status by June 30, 2019, 15.4% of participants were in states with no initial or final approval, 84.6% were in states with initial approval, and 13.8% were in states that also had final approval.
Variables
Demographic Variables
Residence Type Categories.
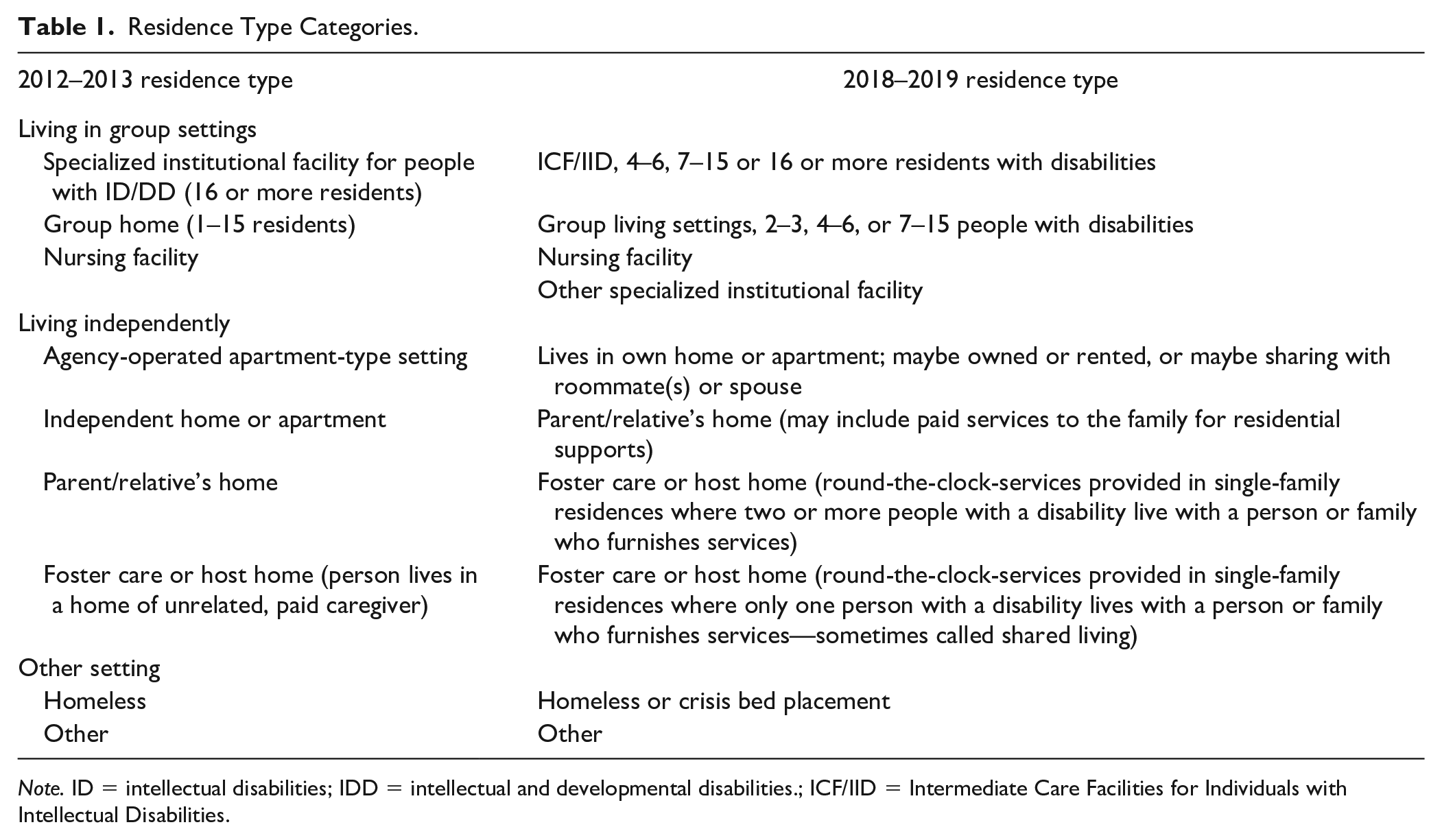
Note. ID = intellectual disabilities; IDD = intellectual and developmental disabilities.; ICF/IID = Intermediate Care Facilities for Individuals with Intellectual Disabilities.
Respect for Privacy Variables
Analyses
All analyses were conducted in STATA version 14 (Stata Corporation, 2015a). “Svy” commands were used to address sampling participants within the state. State was the primary sampling unit. This approach controls for the potential effect of state differences, such as sampling bias and differences in how the Rule was applied. Analyses were evaluated at alpha = .05. Frequency distributions provided descriptive statistics. Chi-square tests (χ2) were run to examine differences between participants from 2012 to 2013 and those from 2018 to 2019. STATA’s “svy” commands correct the Pearson chi square for the survey design using the second-order correction of Rao and Scott (1984) and converting it to an F-statistic. Pearson chi square statistic and the corrected F-statistic p-values are interpreted in the same manner. A t-test was run to compare age by wave of data. Given that STATA has no t-test command, the “means” command followed by the Adjusted Wald test provided an F-statistic. The square root of the F-statistic produces a t-value (Stata Corporation, 2015b). Lastly, for the privacy outcomes that were significant, logistic regression models were run to examine if relationships held up controlling for covariates.
Results
Review of STPs
Compliance
A first step was for states to systemically assess how well the state statutes and regulations and the ways in which they contracted for their services matched the new CMS requirements. For each provision in the Rule, states needed to report whether their systems were noncompliant (existing language either did not address or ran counter to the new regulations and needed replacement), partially compliant (existing language needed to be revised and strengthened), fully compliant (no or very minor changes were needed), or silent (nothing in statutes or regulations and completely new language and procedures were needed).
The Rule operationalized privacy at a minimum, meaning participants had privacy where they slept, locks on entry doors to their living space and bathrooms with only necessary staff having keys, a choice of roommate or to have a private bedroom, the ability to decorate and furnish their living space according to their personal preferences, a secure place to keep their personal items, and privacy in all areas where personal care is provided.
Our review of the 19 state plans focused on privacy issues and demonstrated a range of specificity, with some areas of privacy explicitly mentioned more consistently than others. Some states operationalized privacy at a higher level, without providing specificity on the subtypes. As shown in Table 2, most state plans focused only on door locks, choice of roommate, and decorating and furnishing one’s living space as desired.
State Compliance With Privacy Issues in HCBS Programs for People With IDD.
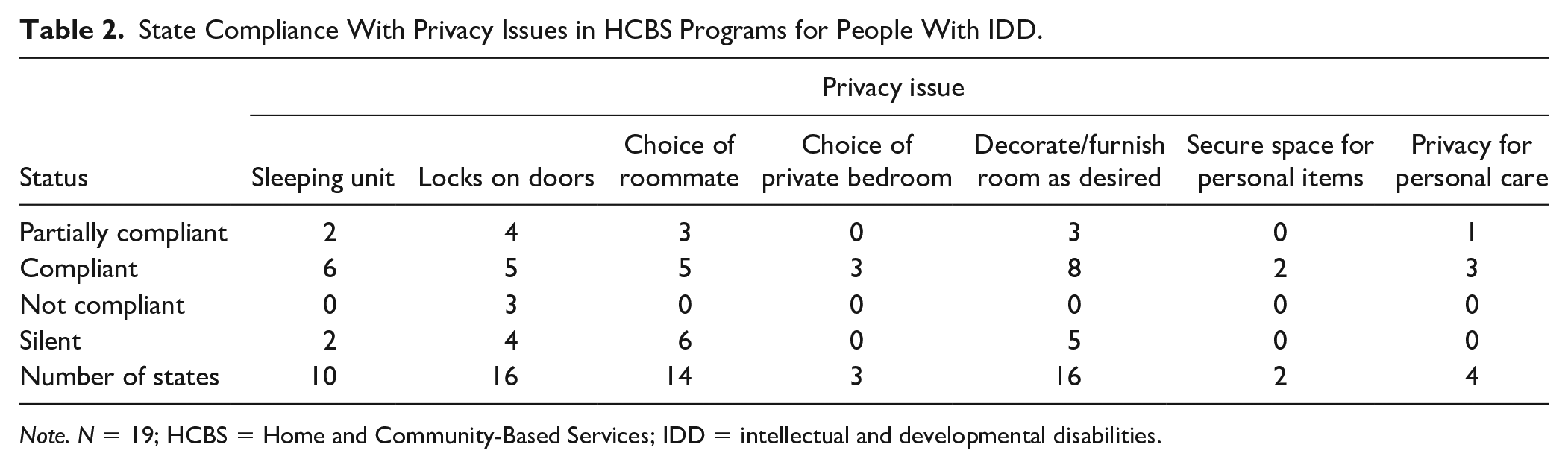
Note. N = 19; HCBS = Home and Community-Based Services; IDD = intellectual and developmental disabilities.
Initial State Actions
Most states developed a combination of both training and technical assistance to support providers to become compliant with the Rule, plus new certification requirements and ongoing regulations for which providers were accountable.
Eleven of the 19 state plans included information about specific actions assuring service recipients’ privacy. Of those 11 states, five (45%) made changes to regulations that providers were accountable for, four (36%) reported providing training and technical assistance to providers, three (27%) made changes to how providers were certified, two (18%) made changes to statutes, two (18%) added new tools to use in evaluating providers, and one (9%) made changes to provider manuals.
Provider Self-Assessment Indicators Related to Privacy
The Rule required states to ask all HCBS providers to self-assess their compliance with its stipulations. The results were used to sort individual settings into three categories:
The setting was fully compliant with the Rule
The setting could become compliant but needed to make some changes, or
The setting could not become compliant and participants should be offered better options.
Four state plans included the tool created for providers to use in completing their self-assessments. Each of these states made some attempt to measure the degree to which the setting supported the participants’ right to privacy.
Four (100%) asked whether participants had a choice of roommate, and one also asked if participants knew how to request a change of roommate.
Three (75%) asked about locks on bedroom doors. Two also asked about locks on bathroom doors, and the other asked about a lock on the outside door.
Three (75%) asked if staff knocked and waited for a response before entering a bedroom, and one also asked if there were circumstances when staff would use a key or code to enter a locked private living space (residence door, apartment, bedroom, bathroom, etc.).
Two (50%) asked if participants could have their own phone, and one also asked whether there was a private area for phone calls.
Two (50%) asked whether the furniture was arranged to allow for private conversations.
Two (50%) asked about having areas available that allow privacy with visitors.
One (25%) included problems with staff discussing private information openly, whether or not individuals could decorate and furnish their bedrooms as desired, and whether there was any use of video cameras.
National Core Indicator–In-Person Survey Data Analysis
Demographics
Demographic variables were examined by survey year. As seen in Table 3, there were significant differences in autism diagnosis, p < .001, with 2012 to 2013 having a lower percentage of autism (12.3% vs. 21.0%) compared to 2018 to 2019. Additionally, there were significant differences, p = .020, on the ID level. Those from 2012 to 2013 had a lower percentage without ID (5.8% vs. 12.1%), a higher percentage of severe ID (15.1% vs. 12.6%), and a higher percentage of profound ID (11.8%, vs. 8.6%) compared to 2018 to 2019. Mental health issues, p < .001, and behavior challenges, p < .001, differed significantly. Individuals from 2018 to 2019 had higher percentages of mental health issues (41.4% vs. 33.5%) and behavior challenges (32.8% vs. 15.7%). There were no significant differences in type of residence, gender, having a guardian, mobility, and age.
Demographic Comparisons From 2012 to 2013 and 2018 to 2019 Survey Years.
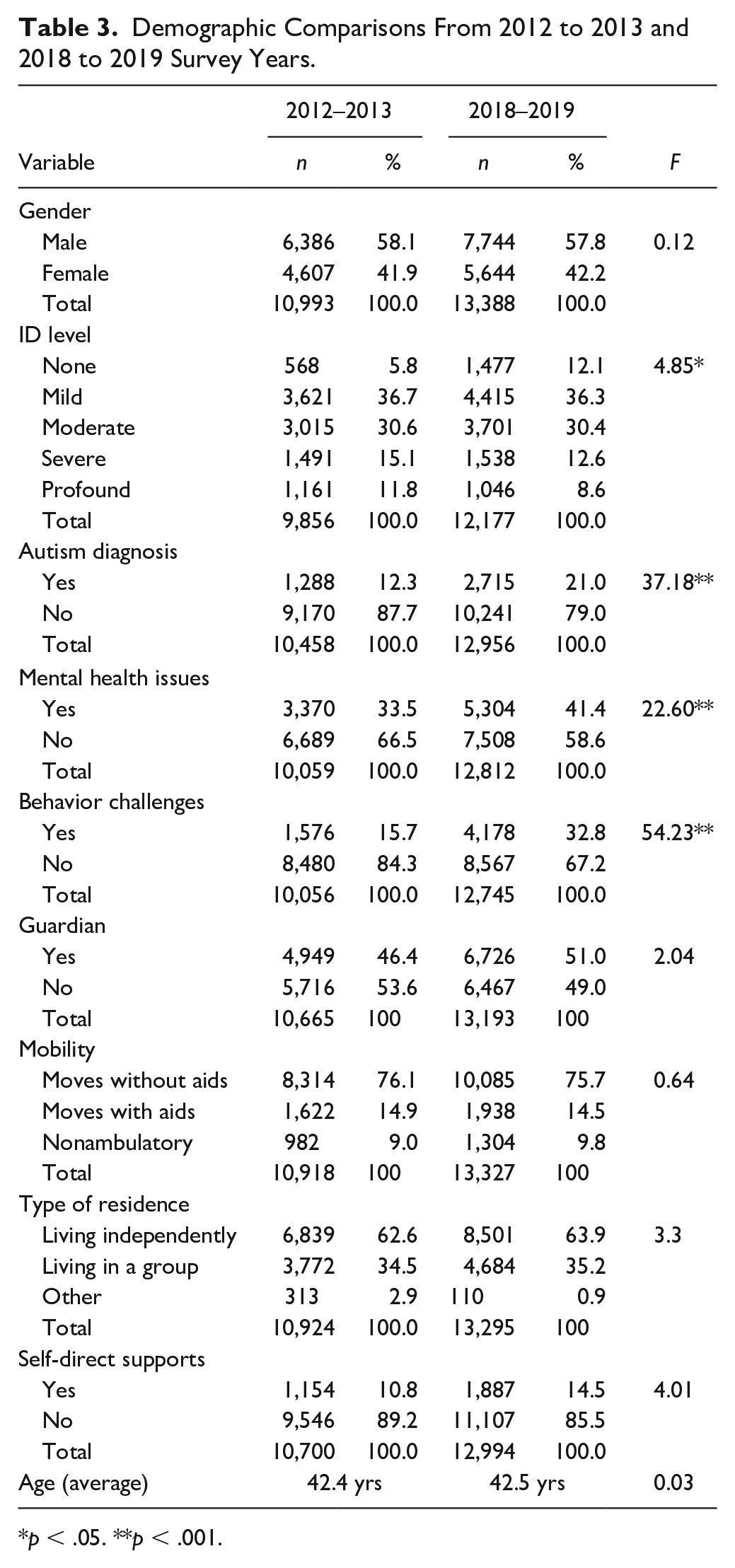
p < .05. **p < .001.
Respect for Privacy
For analyses on respect for privacy, only participants with valid responses to the respective items were included. From 2012 to 2013, 9,535 participants had valid responses to at least one item, and from 2018 to 2019 there were 9,261 (see Table 4).
Respect for Privacy From 2012 to 2013 and 2018 to 2019 Survey Years.
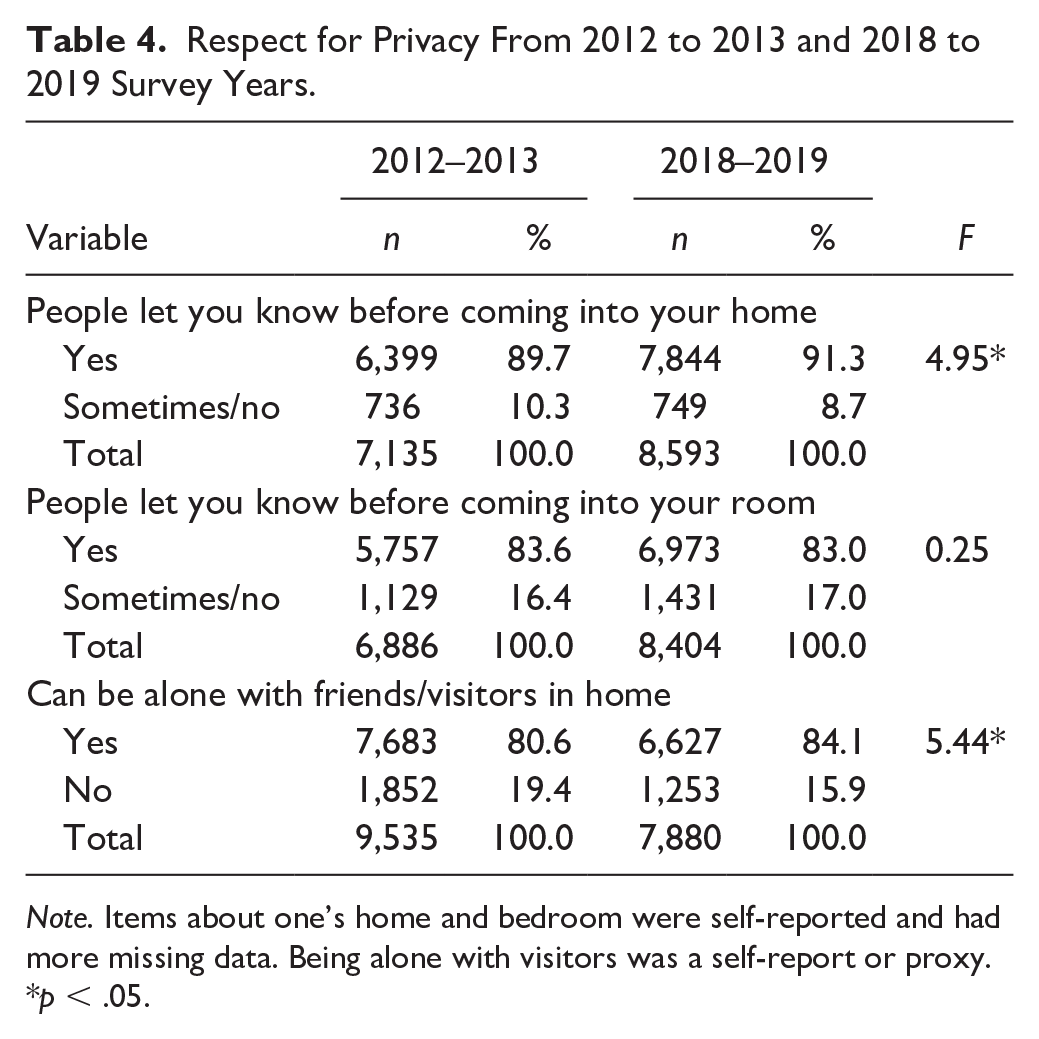
Note. Items about one’s home and bedroom were self-reported and had more missing data. Being alone with visitors was a self-report or proxy.
p < .05.
Table 4 reveals significant differences by survey year on people asking before coming into participant’s homes, p = .032. Those in 2018 to 2019 had higher percentages who asked (91.3% vs. 89.7%). There were significant differences in being alone with friends/guests in one’s home, p = .025. More in 2018 to 2019 could be alone with friends/guests at home (84.1% vs. 80.6%). There were no significant differences in people asking before coming into the individual’s bedroom.
Multivariate Examination of Respect for Privacy
Three logistic regression models were used to examine the relationship between Rule approval status, the wave of data, and the privacy variables (people asking permission to come into one’s home, one’s bedroom, and being allowed to be alone with guests or visitors) while controlling for covariates (age, gender, ID level, autism diagnosis, mental health, behavior challenges, and receiving self-directed supports).
As seen in Table 5, after controlling for other variables, the effects of Rule approval status and the wave of data differed depending on the aspect of privacy. The wave of data (2012–2013 vs. 2018–2019) was significant for asking permission to come into the individual’s home and for being allowed to be alone with friends/guests. Those in 2018 to 2019 had 36% and 29% higher odds of being asked for permission to come into their home, odds ratio (OR) = 1.36, p = .001, and for being allowed to be alone with friends/guests, OR = 1.29, p = .007. Initial approval of the Rule was significantly related to being asked permission to come into the individual’s bedroom, OR = 1.44, p < .001, and being allowed to be alone with guests/visitors, OR = 1.69, p = .009. Individuals in states that had initial Rule approval had 44% and 69% higher odds of being asked permission to come into their bedroom and being allowed alone with friends/guests, respectively. Final approval of the Rule was not significantly related to any of the privacy outcomes.
Logistic Regression Analysis of Respect for Privacy.
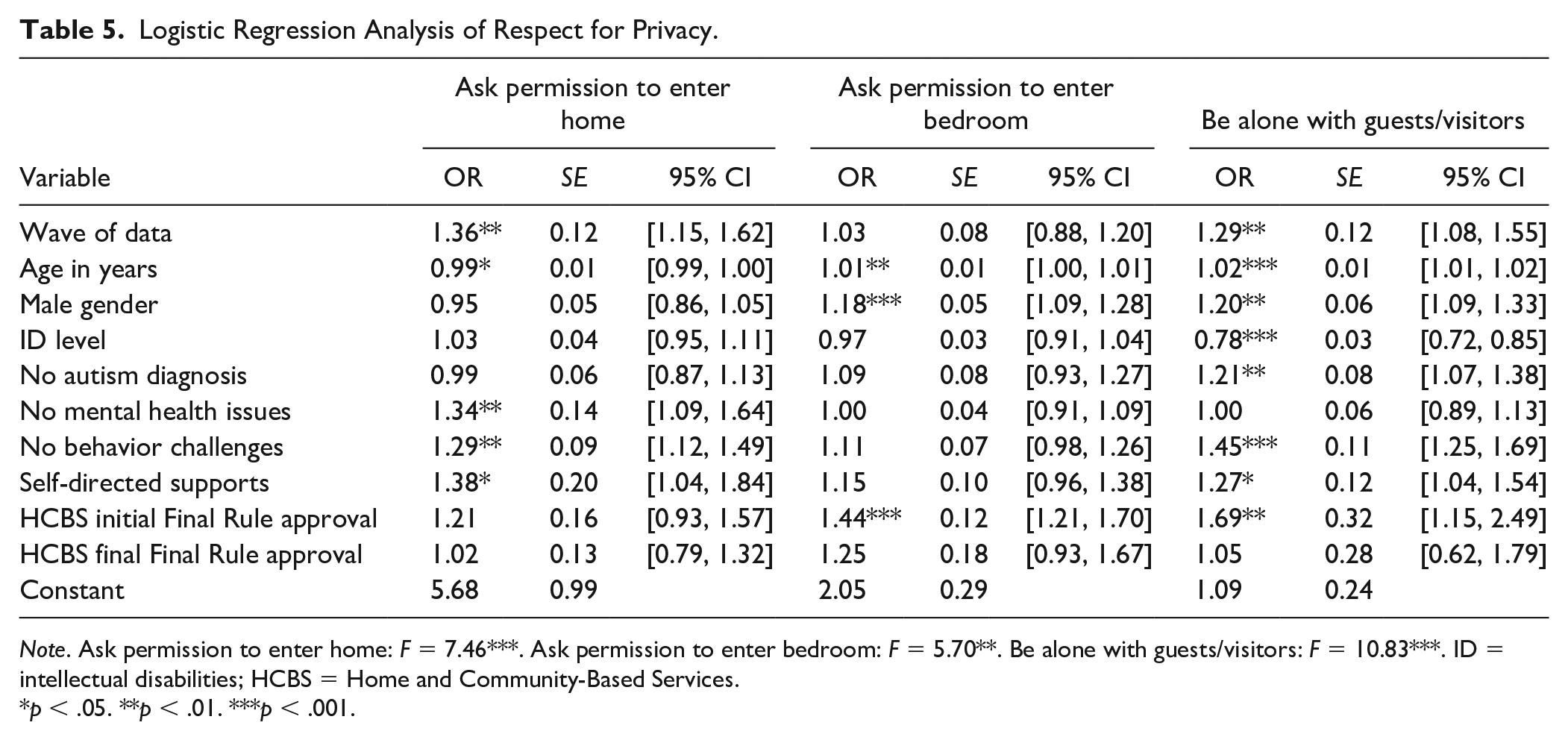
Note. Ask permission to enter home: F = 7.46***. Ask permission to enter bedroom: F = 5.70**. Be alone with guests/visitors: F = 10.83***. ID = intellectual disabilities; HCBS = Home and Community-Based Services.
p < .05. **p < .01. ***p < .001.
For demographics, age was a statistically significant predictor for all three privacy outcomes. Gender was significant, with males having 18% and 20% higher odds of being asked for permission to come into their bedroom. The effects of disability-related variables also differed depending on the aspect of privacy. Intellectual Disability level had a strong negative effect on being allowed to be alone with friends/guests. Those without an autism diagnosis had 21% higher odds of being allowed to be alone with friends/guests. Those without mental health issues had 34% higher odds of being asked permission to come into their home, whereas individuals without behavior challenges had 29% and 45% higher odds of being asked permission to come into their home and being allowed to be alone with friends/guests. Individuals with self-directed supports had 38% and 27% higher odds of being asked permission to come into their homes and being allowed to be alone with friends/guests.
Discussion
The HCBS Final Rule that came into effect in early 2014 was designed to increase autonomy, respect, choice, privacy, and meaningful community inclusion for people with disabilities. This much-needed regulation is intended to expedite the provision of more person-centered and community-based services and reduce institutionalization and segregation. While policies are necessary ways of making change, the extent to which change is actually taking place needs to be examined. Privacy is a basic right as indicated in CRPD and HCBS Final Rule.
We reviewed 19 state plans to determine how privacy was addressed. The plans differed in their conceptualization of privacy, the detail with which they addressed it, and the ways in which they evaluated compliance with the Rule, including in the domain of privacy.
Most state plans focused only on door locks, choice of roommate, and decorating/furnishing one’s living space as desired. Few plans dealt with having a secure place for personal items, a choice of a private bedroom, or privacy for personal care. All states (three) that reported having a choice of a private bedroom demonstrated compliance. All states (two) that reported having a secure space for personal items were compliant. Eleven of the 19 states noted an initial action for improvement, ranging from making changes to regulations that providers were accountable for and providing training and technical assistance, to changing the manuals guiding service provision. Most states had some limited way to measure participants’ privacy, but it often only involved asking one question on discussing private matters openly, having cameras in the space, or knocking before entering a bedroom.
Clearly, many states were either not compliant with or not reporting on several key issues of privacy. This state-plan information provided a context in which to interpret the results of the analysis of 2012 to 2013 and 2018 to 2019 NCI data. Overall, the plans indicated that most states have attended to a few of the aspects of privacy specified in the Rule, but much remains to be done. Therefore, improvements in privacy likely will be patchy and inconsistent. Nevertheless, the few states that achieved full compliance indicate what is possible and provide a benchmark for other states to emulate.
To examine the change in the privacy of people with IDD before and after the enactment of the Rule, we conducted a trend analysis using cross-sectional NCI data from 2012 to 2013 and 2018 to 2019. In the absence of a national longitudinal database of outcomes for people with IDD in the United States, the cross-sectional NCI data provided us an opportunity to compare aspects of privacy in the same 21 states with two random samples of individuals with IDD after 6 years have passed. While this type of analysis does not allow us to examine individual longitudinal changes, it lets us examine trends in the outcomes over time.
Significantly more people with IDD reported that people asked before entering their homes in 2018 to 2019 as opposed to from 2012 to 2013. Similarly, significantly more respondents from 2018 to 2019 reported that they could be alone with friends or guests in their homes. These differences were evident for both univariate and multivariate analyses, the latter controlling for important demographic and disability-related differences between waves of data.
Initial approval of the STPs, unlike the final approval, was significantly related to being asked permission to enter the individual’s bedroom and being allowed to be alone with friends/guests. This finding suggests that developing a transition plan may influence providers’ awareness of and compliance with privacy requirements.
These findings of improvement in respect of privacy over time echo findings from a review by McCarron et al. (2019) indicating as people with IDD move from institutionalized settings to more community-based residences, their right to privacy to more respected. At the same time, these findings also provide evidence for Charitou et al.’s (2021) conclusions on prevailing barriers to privacy, indicating a need for continued work in this direction. Moreover, focusing on relocating people with disabilities to more community-based settings, however, is not a guarantee for an increased level of privacy or other rights. Based on the findings by D. S. Evans et al. (2009) indicating that about a fourth of DSPs, as well as family members, were opposed to respecting privacy related to intimate relationships, there needs to be a call for education of service providers and caregivers on the rights of adults with IDD, including for respect for privacy.
As states work toward compliance with the Rule, including the right to privacy, our results contribute to understanding this important issue. There is an encouraging trend toward an increased respect for privacy for adults with IDD over time. Service providers and policymakers should pay special attention, however, to how privacy is respected for older vs. younger adults with IDD, their gender, level of support needs, as well as comorbidities. Such findings also have implications for considering alternative support options for certain populations such as the use of smart living technologies, especially at this time of staff shortages.
While not conclusive due to its research design, this study provides preliminary evidence of the Rule’s potential to make a positive impact on the privacy of people with IDD.
Recommendations
More studies with rigorous inferential (hopefully including longitudinal) methodologies are needed to investigate the impact of the Rule on the full range of outcomes it covers. Research is also needed on the comprehensiveness, data quality, and effectiveness of various instruments used by states to evaluate services and outcomes for people with IDD. A wider distinction between residential settings would provide a clearer picture of the impact of the Rule on people in different living arrangements. The full range of privacy issues should be included in future analyses to increase the accuracy of conclusions about changes in privacy as a construct.
Limitations
This study has several limitations. There is a standardized approach for survey administration that does not provide the opportunity for deeper exploration into issues examined or the process of decision-making used by participants as they responded. Race/ethnicity was not included in these analyses because the relevant NCI questions from 2012 to 2013 were notably different from 2018 to 2019. In addition, due to incomplete data, the logistic regression analyses resulted in a loss of individuals which threatens the validity of the results. A cross-sectional approach was taken; therefore, causation should not be inferred. The concept of privacy was reduced to the variables that were available in both datasets, thereby limiting the scope of our privacy analyses.
Conclusion
The deadline for full state compliance with the Rule is fast approaching (March 2023), so it is important that all stakeholders have confidence that compliance with the Rule will lead to significantly improved outcomes for people with IDD. This study is one small step in demonstrating the potential positive impact of the Rule, specifically approval of the initial compliance plan with the Rule, for at least two aspects of privacy: being asked for permission to enter their home and the opportunity to be alone with friends/guests in their home.
Footnotes
Acknowledgements
The authors would like to thank Dorothy Hiersteiner and Stephanie Giordano from HSRI for their input into this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Development of this article was supported by Grant #90RTCP0003 to the Research and Training Center for Community Living from the National Institute on Disability Independent Living and Rehabilitation Research, U.S. Department of Health and Human Services. Grantees undertaking projects under government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not therefore necessarily represent official NIDILRR policy.