
Abstract
Long COVID is an emerging public health issue that may be disproportionately impacting adults who had disabilities before the COVID-19 pandemic. We use data from the 2022 National Health Interview Survey to conduct multivariate analyses to compare the odds of having Long COVID among four different disability subpopulations and their working-age reference groups: (1) working-age Medicare beneficiaries, (2) single working-age adults without children who were receiving Social Security Disability Insurance (SSDI) and/or Supplemental Security Income (SSI), (3) adults who had disabilities before the age of 22; and (4) adults with Veteran’s Administration disability ratings. We find that people with disabilities who started before the age of 22 had significantly higher odds of ever having Long COVID (odds ratio [OR]: 2.030, p = .007) compared to their reference group, holding all else constant. We did not find significant differences in the odds of ever having Long COVID for the other three subpopulations we identified. These findings point to the importance of ensuring that the systems that support the economic security, education, employment, and health care of people with disabilities with an onset before age 22 address this newly emerging concern.
Keywords
Introduction
The aim of this paper is to provide estimates of the prevalence of Long COVID among United States (U.S.) adults who had pre-existing (non-COVID-related) disabilities. In 2019, prior to the COVID-19 pandemic, an estimated 41.2 million people with disabilities were living in U.S. communities (Paul et al., 2020). These individuals had lower employment rates, higher poverty rates, and higher rates of involvement with public programs that supported their economic security, educational, employment, health care, and independent living needs than people without disabilities (Paul et al., 2020). Although the pandemic has subsided, Long COVID remains a concern and may exacerbate these aforementioned disparities for people with pre-existing disabilities.
Nationally, an estimated 6%–7% of noninstitutionalized U.S. adults have ever had Long COVID (Adjaye-Gbewonyo et al., 2023; Ford, 2024). Long COVID can result in chronic symptoms that impair daily functioning or worsen existing disabilities and so may place additional pressure on the systems that support people with disabilities. If certain subpopulations of people with disabilities are more likely to have Long COVID, the demand for long-term medical care, rehabilitation services, or Social Security disability benefits may increase. Having Long COVID may restrict education or employment participation for people with disabilities or increase the need for accommodations within those spheres in response to episodic conditions like Long COVID. There is a lack of concise data about the prevalence of Long COVID among people with disabilities, however.
The information presented here will therefore be useful to policymakers and practitioners who are serving people with disabilities so they can understand whether the populations they serve are at increased risk of having Long COVID.
Literature Review
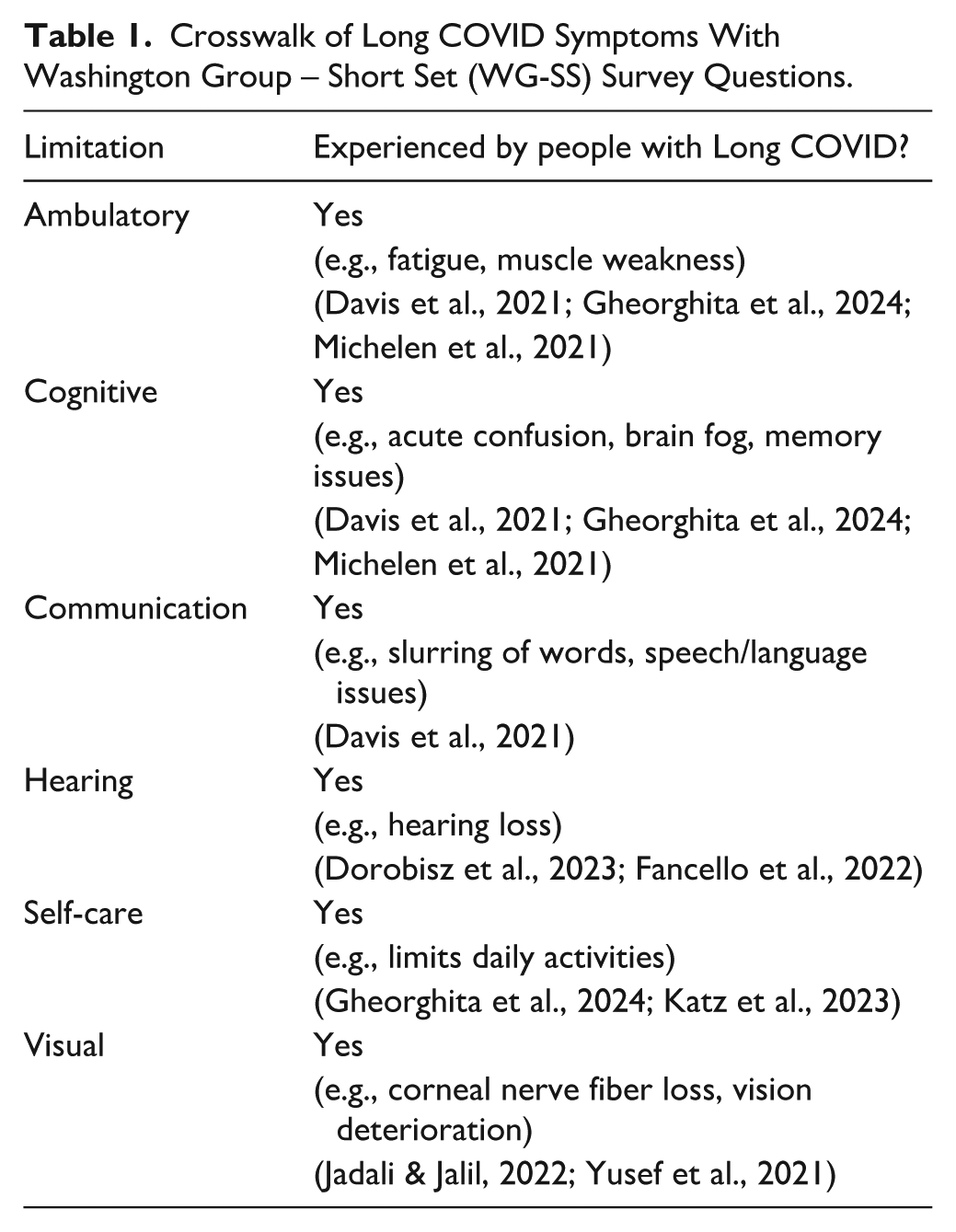
Long COVID refers to a constellation of symptoms that arise from COVID-19 infection and persist for 3 months or more. Fatigue, postexertional malaise, and cognitive dysfunction (e.g., acute confusion, brain fog, memory issues, slurring of words, and speech and language issues) are common symptoms of Long COVID (Michelen et al., 2021). Long COVID may also cause problems with hearing (Dorobisz et al., 2023; Fancello et al., 2022) or vision (Jadali & Jalil, 2022; Yusef et al., 2021). Long COVID may involve multiple organ systems and may present in a relapsing-remitting pattern or may progress or weaken over time. In some instances, the recovery timeline may exceed 35 weeks (Davis et al., 2021; Michelen et al., 2021) or have severe life-threatening consequences months or years after the initial infection (U.S. Department of Health and Human Services, 2026). Long COVID may cause disability, limiting a person’s ability to perform day-to-day activities and employment, increasing their risk of other health conditions and use of primary and short-term health care services, and having a negative association with household financial stability (Katz et al., 2023). Long COVID can also increase pre-existing mental health conditions (Hovagemyan et al., 2023).
Estimates of the percent of U.S. adults who have experienced Long COVID vary by data source and population of interest. In 2022, approximately 6%–7% of noninstitutionalized U.S. adults ever had Long COVID (Adjaye-Gbewonyo et al., 2023; Ford, 2024). Data from the 2022 National Health Interview Survey (NHIS) suggest that while nearly 7% of U.S. adults ever had Long COVID, only 3.5% were experiencing current symptoms (Adjaye-Gbewonyo et al., 2023). Overall, an estimated 15% of U.S. adults with a prior positive COVID-19 test develop symptoms of Long COVID. Much is still unknown about the biological pathways that increase the risk of Long COVID at an individual level (Krishna et al., 2023). Certain subpopulations, however, including people who are older, females, people with lower levels of education, and people with more comorbidities (e.g., hypertension, obesity), are more likely to experience Long COVID (Cohen & van der Meulen Rodgers, 2024; Durstenfeld et al., 2022; Song & Giuriato, 2023). Adults who have completed a primary vaccination series prior to infection are less likely to report Long COVID symptoms (Perlis et al., 2022).
U.S. adults with disabilities face health disparities, which may have increased their risk of getting COVID, developing Long COVID, or dying from COVID. People with disabilities have an increased risk of chronic conditions (Dixon-Ibarra & Horner-Johnson, 2014), a lack of access to culturally sensitive health care (Kennedy et al., 2017; McBride-Henry et al., 2023), and increased out-of-pocket costs for health care (Goyal et al., 2023). Adults with disabilities who are from other subpopulations that also face health disparities, including persons from racial/ethnic minority groups (Goode et al., 2014; Shenk et al., 2023; Yearby, 2018), persons who live in poverty (Goyal et al., 2023; Price et al., 2018), and persons who identify as nonstraight gender identities (Mulcahy et al., 2022; Ruedas et al., 2021), may face the multiplicative effects of the intersectionality of these disparities.
Our interest here is in expanding the recent literature about the prevalence of Long COVID among people with pre-existing disabilities. Cohen and van der Meulen Rodgers (2024) used cross-sectional data from the U.S. Census Household Pulse Survey to estimate rates of Long COVID among different subpopulations, including persons they defined as having pre-existing disabilities. While they noted that persons with pre-existing disabilities had higher rates of ever having Long COVID compared to persons with disabilities, their definition of persons with pre-existing disabilities likely overlaps with persons experiencing limitations due to Long COVID. They defined persons with pre-existing disabilities as those who responded affirmatively to having one of six limitation questions (ambulatory, cognitive, hearing, independent living, self-care, and vision), which we would argue are not distinct from symptoms experienced by persons having Long COVID.
Hall et al. (2024) used data from the National Survey on Health and Disability (NSHD) to estimate rates of Long COVID among people with pre-existing disabilities. They compared these rates to findings about the general population from the U.S. Census’ Household Pulse Survey (HPS). The NSHD, an online survey that only includes people with disabilities, has the benefit of gathering detailed data about the date of disability onset so that the data can be used to identify people who had disabilities prior to the COVID-19 pandemic. Hall et al. (2024) estimated (from the NSHD) that 10.4% of people with pre-existing disabilities and (from the HPS) and 7.5% of the general population had Long COVID symptoms in 2022. However, the NSHD survey is not nationally representative, is weighted to represent nonelderly adults, and does not include people without disabilities as a possible reference group. Comparing results from that survey to results from the general population surveyed in the HPS (which includes people with and without disabilities) can bias the findings.
As Long COVID can cause disability, it can be difficult to identify, in cross-sectional population-level data, people who had pre-existing disabilities and then were impacted by Long COVID. Many nationally representative surveys that are fielded by federal agencies, for example, use a set of six questions to identify people with disabilities. The NHIS, for example, uses six disability constructs that are included in the Washington Group – Short Set (WG-SS) to measure limitations in ambulation, cognition, communication, hearing, self-care, and vision. Persons responding as having some or a lot of difficulty in these areas are commonly denoted as having a disability. As shown in Table 1, however, Long COVID can cause limitations in each of these areas. Other research attempts to measure the population with disabilities using cross-sectional data, and these questions may be conflating these two populations (Nguyen et al., 2024).
Crosswalk of Long COVID Symptoms With Washington Group – Short Set (WG-SS) Survey Questions.
We take a different approach in our cross-sectional analysis by using a nationally representative household survey, the NHIS, that includes adults with and without disabilities and by crafting four different unique definitions of disability that can be used to identify persons who had disabilities prior to the pandemic. We estimate the prevalence of ever having Long COVID for four groups of persons with disabilities: (1) Working-age Medicare beneficiaries, (2) Single working-age adults without children who are receiving Social Security Disability Insurance (SSDI) and/or Supplemental Security Income (SSI), (3) People who reported that they had a disability prior to age 22, and (4) People with a Veteran’s Administration (VA) disability rating.
Each of these groups represents people who likely had disabilities before the pandemic. These populations interact with a range of different service systems, which may all need information about how Long COVID is impacting their service populations. Such information can inform policy and practice that can better support the needs of people with disabilities who have Long COVID by increasing access to necessary health care and by considering how programs might need to be adapted for people who are now experiencing Long COVID symptoms. We further explain our rationale and limitations for identifying these groups in “Measures” section.
Method
Data
Conducted by the U.S. Centers for Disease Control and Prevention, the NHIS is a cross-sectional, nationally representative, household interview survey that collects data on health and health care experiences from the civilian noninstitutionalized population residing within the 50 states and the District of Columbia. Each year, the NHIS gathers information from approximately 27,000 adults and over 9,000 children across roughly 35,000 households. For this study, we use data from the 2022 adult sample NHIS file (unweighted n = 27,640), as this was the first year that the NHIS included questions about Long COVID. We restricted our data set to adults aged 18 and older. Data are publicly available and include appropriate sample weights. Cases with missing data were dropped from our analyses. All analyses were conducted in Stata and/or R.
Measures
Within the NHIS, the measurement of Long COVID is a sequential process. First, to determine if a person ever had COVID-19, the NHIS asks individuals if they either underwent testing or were told by a doctor or other health professional that they likely had coronavirus or COVID-19. Next, if individuals answer yes to either of these questions, they are asked about how severe their symptoms were. If a respondent states that they had mild, moderate, or severe symptoms of COVID-19, they are asked: “Did you experience any symptoms lasting 3 months or longer that were not present prior to contracting COVID-19?” Survey interviewers could provide the following language if needed: Long term symptoms may include tiredness or fatigue, difficulty thinking, concentrating, forgetfulness or memory problems, sometimes referred to as ‘brain fog’, difficulty breathing or shortness of breath, joint or muscle pain, fast-beating or pounding heart (also known as heart palpitations), chest pain, dizziness on standing, depression, anxiety, mood changes.
As stated earlier, we cannot rely on standard disability measures within the NHIS to identify people with pre-existing disabilities who also ever had Long COVID. Instead, we created four different measures of disability that were unrelated to COVID. Our first measure is persons who were working-age Medicare beneficiaries (persons age 18–65 who were receiving Medicare). These are likely people who qualified for Medicare due to receiving disability benefits from the Social Security Administration (SSA), which requires that a beneficiary have a 2-year waiting period before receiving Medicare, and so the disabling condition would have occurred well before the pandemic. Our second measure is single working-age adults without children who were receiving either SSDI or SSI due to disability. For both programs, the application and award process can take a year or more. Restricting this second measure to single adults without children ensured that we were capturing benefit receipt of the single adult (rather than other family members), as benefit receipt is only captured at the family level within the NHIS. Focusing on single adults implies that we are capturing a single adult with a disability that was severe enough to receive SSA disability benefits. Third, we identified a group of people who stated that they had a disabling condition that began before age 22 and restricted analyses using this measure to persons age 25 and older (in 2022) to ensure that these people had a disability prior to the start of the pandemic in 2020. This ensures that the disability or limitations the respondent was referring to were not caused by COVID-19. Fourth, we created a measure of people who had a VA disability rating, which would identify people with a service-connected disability. As of 2022, Long COVID was not considered a service-connected disability.
As a comparison in our initial set of descriptive tables, we include estimates of the proportion (unweighted and weighted) of adults who had disabilities according to the WG-SS questions included in the NHIS. We measured this using the reported level of difficulty respondents report in six functioning domains: cognition (remembering or concentrating), communication (understanding or being understood by others), hearing, mobility (walking or climbing stairs), seeing, and self-care (washing all over, dressing). Persons who responded that they experienced “a lot of difficulty” or “cannot do at all” to at least one limitation question were considered to have a WG-SS disability.
We also included sociodemographic characteristics in our final analyses as covariates. Age was measured as an interval measure. Race was measured as non-Hispanic white or not. Sex was measured as male or female. Gender was measured as straight or not. Educational attainment was measured as having at least a high school education or not. Metropolitan status was measured as living in a large central, large fringe, medium, or small metro area or not. The region was defined as Northeast, North Central/Midwest, South, or West. Overweight was measured as overweight or obese, according to self-reported Body Mass Index categories included in the NHIS. The usual source of health care was measured as having one or more usual sources of care or not. Hypertension was measured as ever having been told that a respondent had hypertension or not. COVID vaccine receipt was measured as having had at least one COVID vaccine.
Analytical Approach
We first present unweighted and weighted sample sizes for the population that ever had Long COVID and the different disability measures. Next, we present a cross-tabulation of the disability measures with ever having Long COVID, testing for differences between groups using chi-square. Finally, we conduct sequential regressions to estimate the association of disability status with the odds of ever having Long COVID. Please note that these analyses do not consider mortality and are conditional on people surviving COVID. The first regression estimates the risk of ever having COVID based on age, race, sex, gender, educational attainment, metropolitan status, region, being overweight, having a usual source of health care, having hypertension, and receipt of any COVID vaccine. The resulting estimates are included as a variable in the second logit, which estimates the odds of Long COVID, controlling for risk of ever having COVID, disability status, and the sociodemographic characteristics included in the first regression.
Results
Table 2 shows the unweighted and weighted numbers of adults who ever had Long COVID and the numbers of people within our different subpopulations of people who had a disability. Overall, nearly 7% of the U.S. adult population, or more than 17.6 million Americans, ever had Long COVID in 2022, which on its own may be disabling. Our pre-existing disability subpopulations represent smaller proportions of the overall adult population. When weighted, these proportions range from slightly over 1% (for working-age single adults without children who are receiving SSDI and/or SSI) to slightly over 3% (working-age Medicare beneficiaries). These estimates are substantially lower than the proportion of the adult population that is identified using the WG-SS (over 9%), although, as noted earlier, the WG-SS measure likely includes a mix of people with pre-existing disabilities and people who are currently experiencing symptoms associated with Long COVID.
Number of Adults With Long COVID and Number of Adults With Disabilities Within 2022 NHIS (Unweighted N = 27,640).
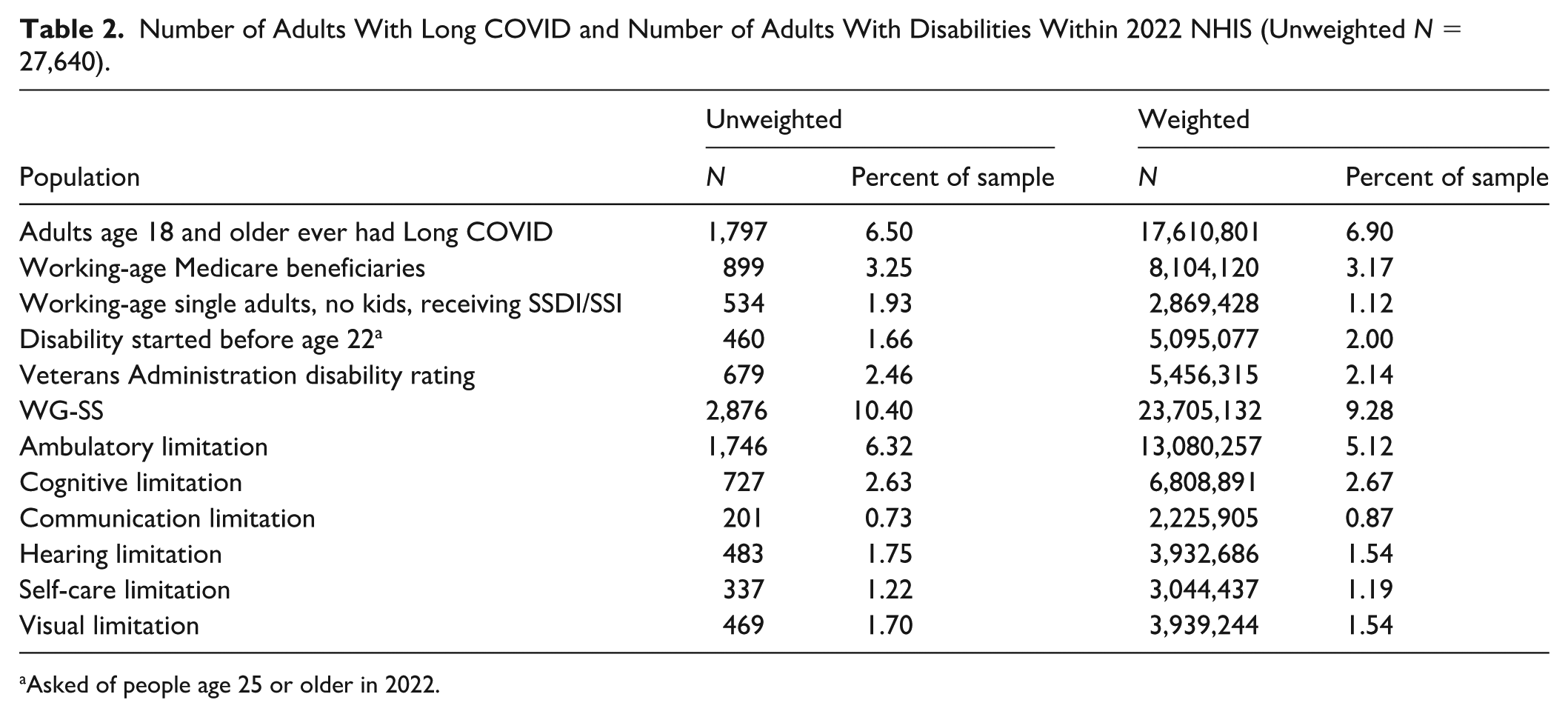
Asked of people age 25 or older in 2022.
Table 3 presents our bivariate analyses, showing the percentage of adults who ever had Long COVID for each of our pre-existing disability populations and the p-value results of the chi-square test for significant differences. Although our estimates of ever having Long COVID range from 6% to 9% among the different pre-existing disability populations, these percentages are not significantly different from their reference groups.
Percentage of Adults who Ever had Long COVID by Disability Status 2022 NHIS (Unweighted N = 27,640).
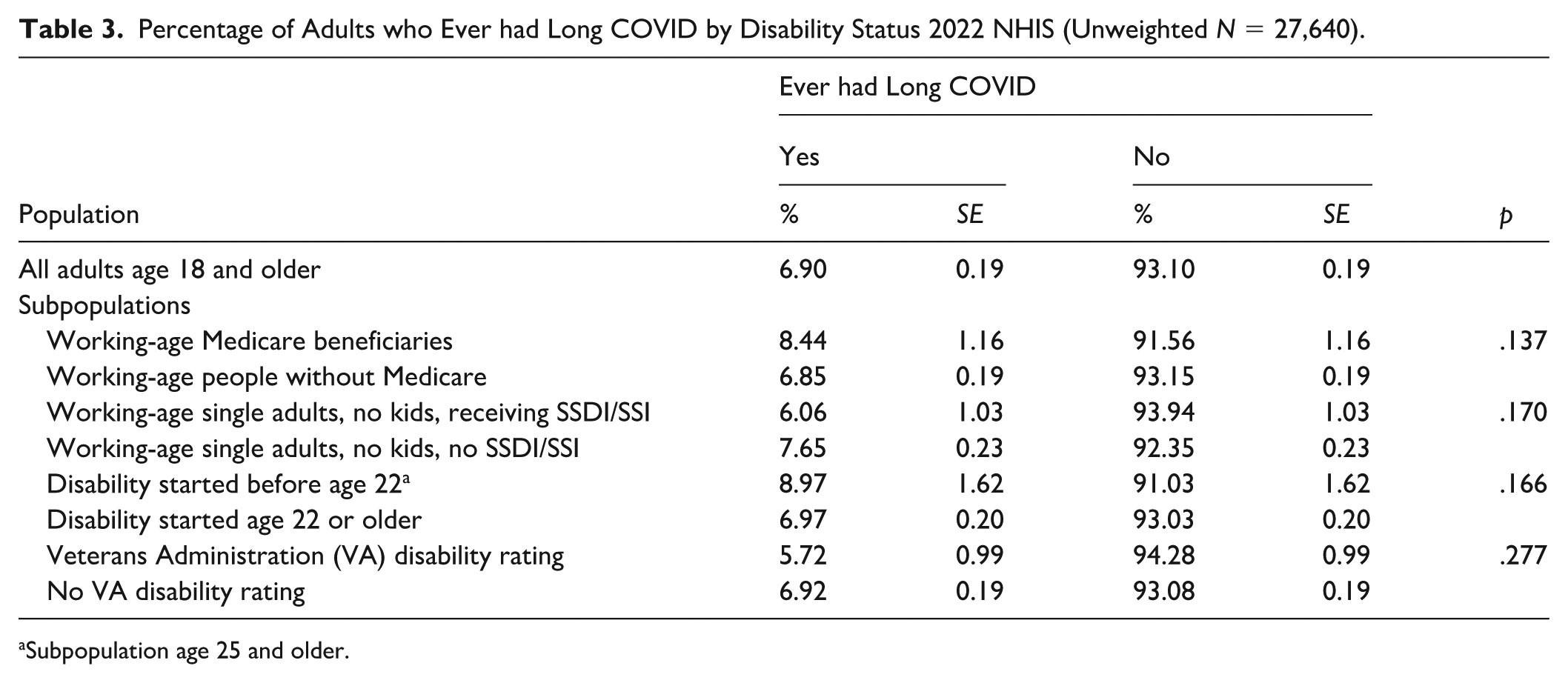
Subpopulation age 25 and older.
Table 4 shows the adjusted odds ratios of ever having Long COVID by pre-existing disability status. Adults who had a disability that started before the age of 22 were significantly more likely to have Long COVID than adults who did not have a disability before age 22 (odds ratio [OR] = 2.030, p = .007). No other significant differences between disability subpopulations were found.
Adjusted Odds Ratios (ORs) of Ever Having Long COVID Among Adults Age 18 and Older, By Pre-Existing Disability Status, 2022 NHIS (Unweighted N = 27,640).
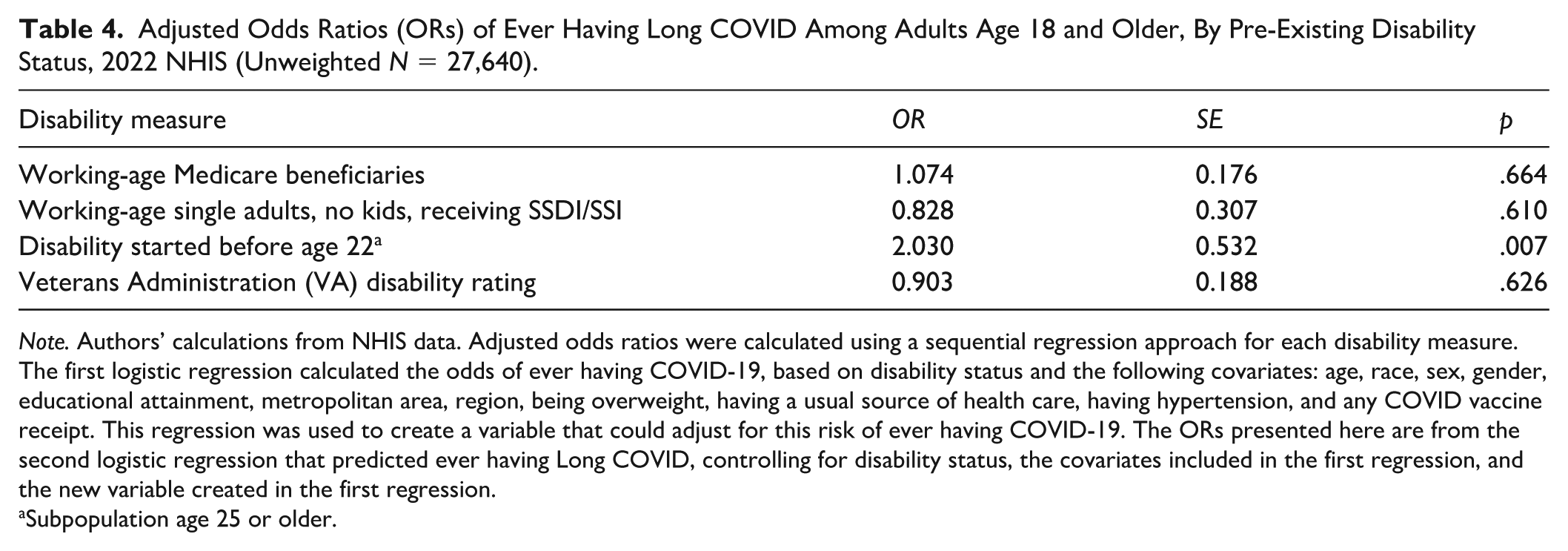
Note. Authors’ calculations from NHIS data. Adjusted odds ratios were calculated using a sequential regression approach for each disability measure. The first logistic regression calculated the odds of ever having COVID-19, based on disability status and the following covariates: age, race, sex, gender, educational attainment, metropolitan area, region, being overweight, having a usual source of health care, having hypertension, and any COVID vaccine receipt. This regression was used to create a variable that could adjust for this risk of ever having COVID-19. The ORs presented here are from the second logistic regression that predicted ever having Long COVID, controlling for disability status, the covariates included in the first regression, and the new variable created in the first regression.
Subpopulation age 25 or older.
Discussion
This paper makes key contributions to the literature about Long COVID among people with disabilities by estimating the odds of having Long COVID among different subpopulations of adults with pre-existing disabilities. In sum, we find a strong association between having a disability before age 22 and having Long COVID, but we do not find significant associations for the other disability subpopulations. Two of the underlying factors that might account for this difference relate to the likelihood of contracting COVID and the likelihood of vaccine receipt. While not shown in “Results” section (but available from the authors), the preliminary analysis that we conducted related to these two factors found variations across subpopulations. People with disability onset before age 22 were the only subpopulation that had similar risks of ever having had COVID compared to others (34% compared to 39%, p > .05) coupled with a statistically significantly lower likelihood of having received any COVID vaccine (74% compared to 80%, p < .05). For comparison, working-age Medicare beneficiaries had statistically lower likelihoods of ever having COVID and equal likelihoods of receiving vaccines compared to others; working-age single adults without kids receiving SSDI/SSI had statistically lower likelihoods of contracting COVID and statistically lower likelihoods of receiving vaccines compared to their reference group; and people with VA disability ratings had equal likelihoods of contracting COVID but statistically higher rates of receiving vaccines than their comparison groups. As no group had a higher likelihood of ever having had COVID compared to their reference groups, vaccine receipt appears especially important for reducing the risk of Long COVID. People with disability onset before age 22 faced a distinct disadvantage in terms of Long COVID, given the same general risk of contracting COVID but lower vaccine receipt.
The systems that support people who have disabilities that were acquired before age 22 include a mix of public and private economic security, educational, employment, independent living, and health care programs that were primarily designed to address the needs of people with intellectual and developmental disabilities (IDDs). Whether and how these systems are adapting to the additional burden of Long COVID is unclear. Given the findings presented here, however, it is important that these systems develop and implement evidence-based methods of serving people with IDD who are also experiencing symptoms of Long COVID. These Long COVID symptoms may, as referenced earlier, limit ambulation, cognitive ability, communication, hearing, self-care activities, and vision and may also be intermittent. Accommodating people with IDD who have Long COVID within existing systems may require rapid innovation. In addition, it is important that public health agencies should treat people with disabilities with onset before the age of 22 as a high-risk group for Long COVID and include them in targeted surveillance and outreach efforts.
While the findings presented here may be particularly relevant to policymakers and practitioners that serve people who acquired disabilities before age 22, others may find utility in these findings as well. Even though we did not find increased odds of having Long COVID compared to the reference groups for the other three measures of pre-existing disabilities, having equal odds of having Long COVID suggests that these other subpopulations are also experiencing Long COVID. Each of the individuals included in these other subpopulations may be interacting with different service delivery systems. For example, working-age Medicare beneficiaries and working-age single adults who are receiving SSDI/SSI may be interacting with SSA as well as employers or vocational rehabilitation services as they attempt to balance work and benefit receipt. SSA, employers, and vocational rehabilitation services therefore need to understand how to accommodate people with disabilities who now have Long COVID and its associated symptoms. As one example, these systems need to ensure that applications for benefits or services are accessible to people who have brain fog symptoms, which may mean simplifying application requirements, shortening any required eligibility or intake meetings.
Future research should aim to delve more deeply into how the multitude of systems that are serving people with disabilities are adapting their policies and practices to address the impact of Long COVID. Long COVID may be an additional concern for people who have other types of disabilities and may also be moving more people, including those who did not have pre-existing disabilities, to seek disability-related services and support. Improving data collection in nationally representative datasets to more clearly identify people with pre-existing or non-COVID-related disabilities as well as people who have disabilities related to Long COVID would help move this future research forward.
Limitations
Our findings should not be construed to imply that the overall risk of having adverse effects from COVID-19 is similar among these populations, as we do not account for mortality impacts in these basic descriptive analyses. As the analyses described here rely on nationally representative household survey data, it is important to recognize that such analyses are simply descriptive. Such data cannot be used to estimate the overall risk, or increased likelihood, of having Long COVID among the entire adult population who had pre-existing disabilities, as nationally representative household survey data do not allow for consideration of the mortality impacts of COVID. Measurement is a large barrier to effectively assessing differential rates of COVID-19 mortality by disability status, as this characteristic is not captured on mortality files or death records the way that gender and race more readily are. Future analysis can utilize population-level data to understand whether patterns of COVID-19 mortality are higher in communities with higher rates of disability so that more effective and inclusive public health strategies can be developed.
Conclusion
People who have acquired disabilities before the age of 22 have increased odds of having Long COVID, which may be increasing disparities in economic security, education, employment, health care, and independent living for this population. Policymakers and practitioners who support people with early-onset disabilities in these realms must adapt to this new concern to ensure that their systems remain effective.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this paper were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90DPEM0007-01-00). NIDILRR is a center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this paper do not necessarily represent the policy of NIDILRR, ACL, or HHS, and you should not assume endorsement by the federal government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.