
Abstract
Child welfare workers (CWWs) face challenges to engaging families, including initial parental resistance, service plan noncompliance and other barriers. Adopting a motivational interviewing (MI) framework may improve engagement and collaboration between CWWs and parents, thereby leading to better child welfare (CW) outcomes. This comprehensive narrative review identifies the use of MI in CW, the outcomes of MI use and the gaps in the literature. Of the 16 articles that met inclusion criteria for our search, 12 suggested MI’s value in parenting skills, parent/child mental health, retention in services, substance use, and CW recidivism. Four of these studies specifically focused on CWW. Future studies should examine specific CW outcomes such as reunification, parent/child relationships, recidivism and parent/child mental health.
Keywords
Successfully working with families in the child welfare (CW) system involves an understanding of practices that help parents find internal motivation to make changes while engaging with the child welfare worker (CWW). Yet caseworkers have noted challenges with engagement, citing their inability to motivate client change as their greatest deficit (Forrester, Westlake, & Glynn, 2012; Pecora, 1989). One way to overcome this deficit is to invest in CWW engagement, which ultimately results in better outcomes for families (Cheng, 2010). A number of factors have been cited as barriers to parent engagement (Iannos & Antcliff, 2013), but perhaps one of the most challenging may be the power differential between the CWW and parent (Dumbrill, 2010). Since power differentials often create problems and limitations in the relationship between CWWs and parents (Dumbrill, 2010), we believe that motivational interviewing (MI) practice, which emphasizes collaboration, partnership, and empowerment, should be the future foundation of effective CW practice with families.
MI, consistent with the strengths-based social work model (Manthey, Knowles, Asher, & Wahab, 2011), is one approach for CWWs to enhance engagement with parents. Adopting a spirit of partnership, acceptance, compassion, and evocation to enhance parent self-efficacy may result not only in improved relationships with parents but also in better CW outcomes. MI is defined as a “person-centered counseling style for addressing the common problem of ambivalence about change” (Miller & Rollnick, 2013, p. 29).
Use of MI in CW settings or populations is likely to increase due to growing evidence of its value with a number of presenting problems (Lundahl, Kunz, Brownell, Tollefson, & Burke, 2010). The process of changing any behaviors can be difficult but especially so for CW families. Parents within this system face numerous obstacles, including shame (McConnell & Llewellyn, 2005; Scholte et al., 1999); experience in the CW system in their own childhood (Kim, 2009); low income and education (Coulton, Crampton, Irwin, Spilsbury, & Korbin, 2007); mental health, domestic violence, substance use, unemployment, and homelessness (D’Andrade & Chambers, 2012); and poor understanding of service plan requirements and access to resources (Estefan, Coulter, VandeWeerd, Armstrong, & Gorski, 2012).
As highlighted by Hohman (1998), MI could be a particularly useful tool for engaging CW-involved parents with substance use problems—problems that account for 61% of out-of-home placements for infants and 41% for older children (Wulczyn, Ernst, & Fisher, 2011). Substance use is one of the most common parental concerns and frequently results in slower reunification or higher rates of recidivism (Ryan, Victor, Moore, Mowbray, & Perron, 2016). MI has been identified by the Children’s Bureau (2014) as a tool to promote parental engagement with substance abuse treatment. Since MI has been established as an evidence-based treatment for substance use (Burke, Arkowitz, & Menchola, 2003; Hettema, Steele, & Miller, 2005; Lundahl et al., 2010), it may be a valuable skill for CWWs to acquire. MI could be used by CWWs to understand the obstacles faced by each family and collaboratively work with families to overcome these challenges as part of the change process.
The California Evidence-Based Clearinghouse for Child Welfare (2017) rates MI as well-supported by research evidence but only of moderate relevance to CW practice. Moreover, it references only studies related to substance use in its summary statement. No reviews have formally evaluated the use of MI in the CW system, but such a review could inform practitioners, researchers, and administrators about MI’s potential utility and the existing gaps in research that require further study. Implementing MI with CW clients could result in improved parent engagement and save CWWs time over the course of the case. Using a comprehensive narrative review approach, this article summarizes research studies addressing how MI is being used in CW settings.
Method
Little information has been consolidated on how MI has been used within CW settings or populations. Therefore, we chose to be broad in our inclusion of studies, including any studies examining the use of MI alone or in combination with another intervention.
Inclusion Criteria
We included papers that (a) were studies of MI with clear descriptions of the intervention, (b) were prospective studies with outcome data (quantitative and qualitative), (c) included parents involved with the CW system or CWWs, (d) were written in the English language, and (e) were peer-reviewed.
Exclusion Criteria
We excluded papers that were (a) not studies of MI, (b) conceptual, (c) reviews, (d) not CW populations or settings, (e) case studies, and (f) not empirical.
Search Strategy
Our search strategy along with search terms are detailed in Figure 1 in a flow diagram of the reviewed studies. In addition to database searches of manuscripts published until February 2018, we examined the references of relevant review articles as well as studies from the California Evidence-Based Clearinghouse for Child Welfare. During database searches, the title and abstract were screened for eligibility. If the article could not be included or excluded based on this information, the full article was obtained and reviewed for inclusion. Two researchers reached a consensus on each study to determine inclusion.
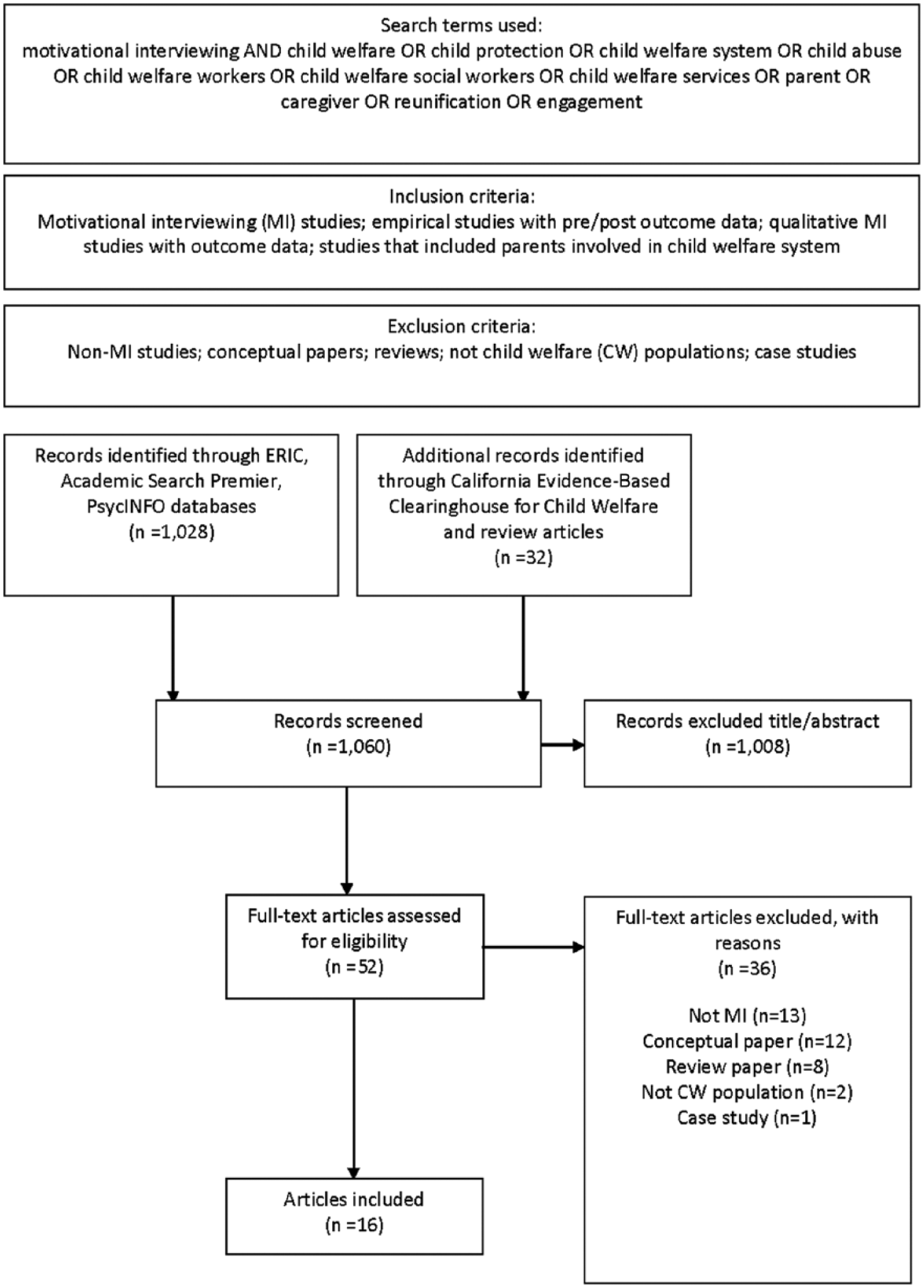
Flowchart of inclusion/exclusion criteria and included/excluded studies.
Results
A total of 1,060 studies were identified through database searching and additional sources (see Figure 1). Of these studies, 1,008 were initially excluded, leaving 52 articles to be assessed for inclusion. Ultimately, 36 articles were excluded and 16 were included. Two of the included articles discussed the same study but reported different outcomes. See Table 1 for a summary of the study’s samples and designs. Eleven studies used only CW samples or CWWs, while part of the samples of four studies were in the CW system. Four studies evaluated CWW use of MI and outcomes for social workers (SWs), including skill development, self-efficacy, team culture, and engagement. Two of the studies evaluated both parent outcomes and CWW fidelity with MI. Of the studies, only four reported CW-related outcomes (e.g., recidivism, days of out-of-home placement, new child abuse reports). Some studies reported multiple types of outcomes:- three studies reported child mental health-related outcomes, five reported mental health or substance use outcomes, and six reported parenting outcomes. The MI intervention was part of a parenting intervention in six studies, family preservation in one study, substance use referral/treatment in two studies, CW case work in one study, and family intervention for parents abusing substances for one study (Multisystemic Therapy Building Stronger Families).
Summary Information of Identified Studies Involving MI in a CW Setting.
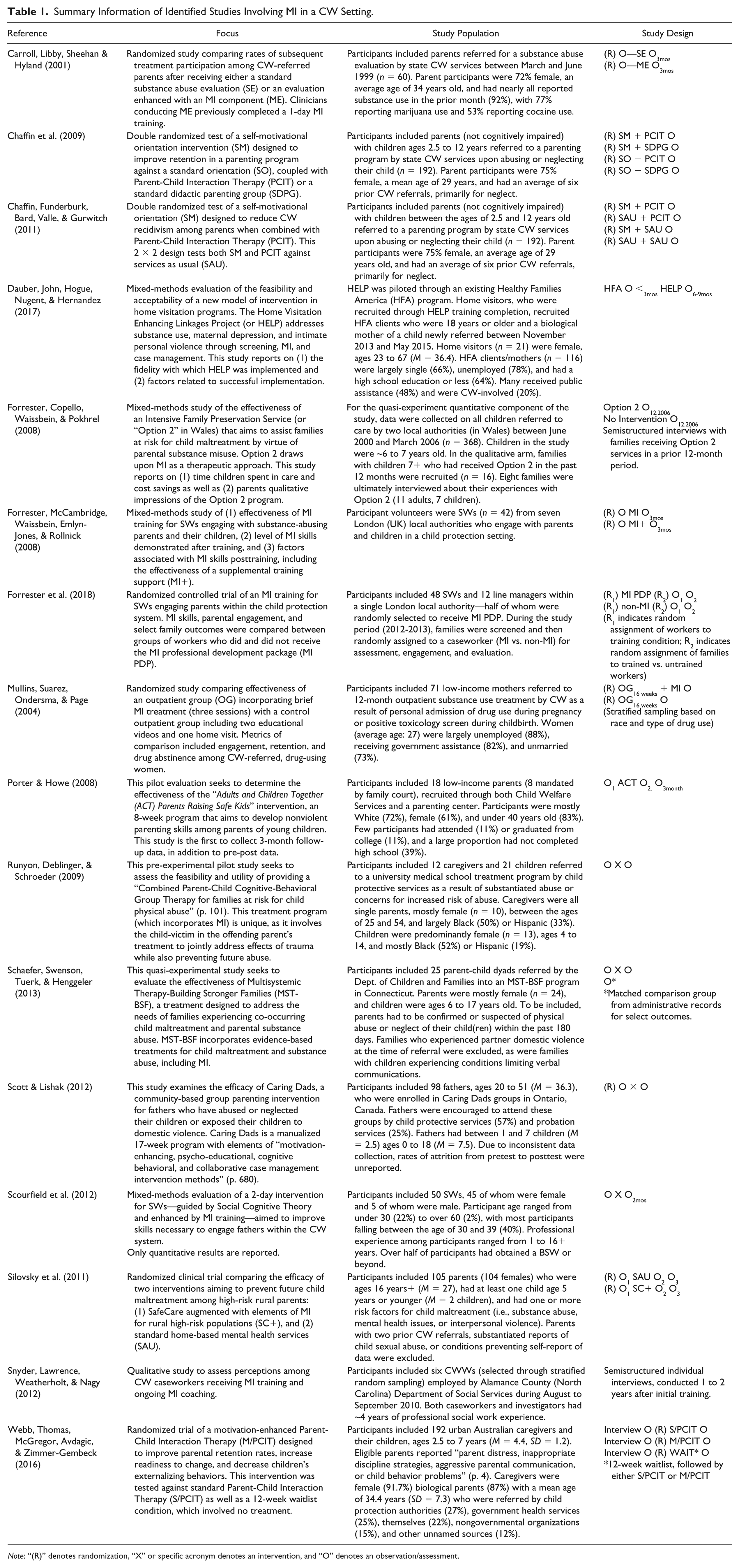
Note: “(R)” denotes randomization, “X” or specific acronym denotes an intervention, and “O” denotes an observation/assessment.
MI Combined With an Intervention
MI was combined with Parent Child Interaction Therapy (PCIT; n=3), cognitive behavioral therapy (n=3), case management (n= 1), multisystemic therapy (n=1), intensive family preservation (n=1), CW case work (n=2), CW interviewing (n =1), substance use assessment (n=1), and other nationally recognized programs (Caring Dads, Adults and Children Together/Parents Raising Safe Kids, and Safe Care, n=3). The next section describes these studies in detail, paying particular attention to the benefits of using MI in CW settings.
CWWs and MI
Initial research has uncovered the value of adding MI to interventions in the CW setting for both the client and the CWW. According to qualitative interviews with family assessment CWWs, implementing MI with continued coaching of CWWs to ensure treatment fidelity led to improved engagement and cooperation of families (Snyder et al., 2012). MI can be successfully implemented if ongoing supports are made available to caseworkers based on a typological analysis. As indicated in prior literature, caseworkers benefited from frequent skill-building sessions/workshops where they could receive live feedback and have the opportunity to model responses. Caseworkers may require 1 year or more to develop comfort with these skills, which is notable given the high turnover rates within CW (Kim & Kao, 2014).
MI training improved SW engagement with fathers in a residential setting (Scourfield et al., 2012). SWs showed significant increases in self-efficacy as well as improvements in team culture with increased comfort working with fathers and as a team. Also, SWs had significant increases in engagement with fathers (both residential and nonresidential) who they deemed to not be a risk to their children yet did not increase engagement with fathers whose behavior posed a risk to their children.
Similarly, in a study of the effectiveness of a 2-day MI training for CWWs engaging with substance-using parents (Forrester, McCambridge et al., 2008), CWWs reported increased reflexive listening skills and willingness to let the clients take the lead. For 85% of CWWs engaging in simulated interviews, only two demonstrated sufficient skill in MI (through observed skill ratings); another eight were borderline competent, while nine demonstrated no MI skills despite the 2-day training. After low uptake of MI+ supports (which included three individual and two group-supervision sessions in the months following the MI training), participants in the two conditions (MI and MI+) failed to differ significantly in MI skills at 3-month follow-up; however, while not statistically significant, participants receiving MI+ supports had a tendency to demonstrate high levels of MI skills compared to participants receiving only the 2-day MI training. Clearly, findings from this study suggest the value of ongoing training.
To evaluate the benefits of more supportive training, Forrester and colleagues (2018) examined the effectiveness of the MI Professional Development Package (PDP) for CWWs in improving MI skills, parental engagement, and other select family outcomes within the child protective system in a randomized controlled trial. The PDP included 2 days of a standard MI training workshop, 1 day of MI for complex child protection interviewing, eight weekly supervisions sessions, 1 day of MI in child protection, and one supervision session for 6 months. No statistically significant gains were noted in parental engagement or other outcomes for families assigned to MI PDP-trained CWWs as compared to families assigned to untrained workers. Yet group differences in MI skills (collaboration and evocation, specifically) were detected in which CWWs trained with MI PDP were slightly more skilled than their untrained counterparts (Cohen’s d=0.201). Forrester, McCambridge et al. (2008) note that CWWs did not have many sessions in which to meet with clients, and these sessions were focused on administrative or logistic matters rather than client change, perhaps accounting for the weak findings in outcomes. There was also wide variability in MI skills among the CWWs at baseline, which could affect the ability to understand skill improvements. We would add, based on our own experience delivering MI, that it may take many years of skill practice prior to proficiency. Therefore, these findings combined with our experience lead us to recommend that training in MI begin as early as college and that it would be more potent when delivered more frequently in CW services like intensive family preservation.
In an evaluation of the Home Visiting Enhanced Linkages Program (HELP), the frequency of MI implementation and case management components was examined (Dauber et al., 2017). Mothers were referred to HELP only if they endorsed mental health or substance use concerns during screening. It appears that home visitors used MI at a lower than expected rate but that they did use MI more with mothers in treatment who already had high levels of motivation. It was noted that some mothers may not have reported problems (e.g., mental health or substance use) during the initial screening due to concerns about CW repercussions. Two components of HELP (MI and case management) were offered to less than half of the sample. Yet home visitors reported high levels of implementation of general supportive services. In examining factors associated with implementation, quantitative findings revealed that home visitors’ attitudes toward evidence-based practices as well as the treatment model were relatively high when compared to prior studies. Qualitative findings revealed barriers to implementation including client reluctance to engage due to stigma and fear related to CW involvement as well as personal, logistical, and systemic barriers to accessing treatment. While home visitors were generally satisfied with the HELP protocol, some noted frustration with their perceived limitations to provide assistance to clients in need.
Parenting and MI
Silovsky and colleagues (2011) found that rural parents were much more likely to enroll, be retained in treatment, and be engaged if randomized to a skills-based parenting program enhanced with MI (MI+P) rather than to standard home-based mental health services. Fewer domestic violence-related CW reports were also reported. Parents assigned to MI+P were more engaged and satisfied with services compared to parents receiving mental health services. While group differences across other CW outcomes were not noted, MI-enhanced parenting trended favorably.
A large field trial of MI combined with a hands-on parent-child interaction program resulted in lowered CW reports (29% recidivism; Chaffin et al., 2011) compared to only motivation (34% recidivism), only parenting (47% recidivism), and only services-as-usual (41% recidivism). The MI+P was associated with a better retention rate (85%) than the other three treatment conditions (~61%). This combined program has found improved retention rates in parents with low-to-moderate initial motivation but lower retention in those with higher motivation (Chaffin et al., 2009). The findings suggest the importance of gauging early motivation and tailoring interventions based on initial assessments.
In a study by Webb et al. (2016), parents receiving PCIT with a three-session motivational enhancement showed no difference in study retention over parents receiving standard PCIT. However, those with the motivational enhancement showed increased levels of readiness to change, which should be further explored. Child externalizing declined most notably within the MI+PCIT and PCIT groups. Child internalizing behaviors declined in both the MI+PCIT and PCIT groups but not in the waitlist group. Similarly, child behavior (intensity and frequency) declined most notably within the MI+PCIT and PCIT groups but not the waitlist group. Parent stress (child- and role-related) declined in both the M/PCIT and S/PCIT groups but not in the waitlist group. The strength of this study lies in assessing both child and parent outcomes; which would be valuable for future MI research.
Substance Use and MI
In a study testing an intervention for parents with co-occurring child maltreatment and substance abuse, multisystemic therapy enhanced with MI led to lower recidivism over 24 months (Schaeffer et al., 2013). These families fared better than those referred to community services with fewer substantiated maltreatment reports and children requiring fewer days of CWW care. Pretest and posttest differences were noted primarily for mothers, who experienced positive treatment outcomes for alcohol and drug use, depression, psychological aggression, and nonviolent discipline (effects [d] ranged from .45 to .95). Youth also experienced a reduction in anxiety (d=.42). These findings suggest that combining MI with other therapeutic approaches can result in vigorous and long-lasting benefits.
Additionally, Carroll et al. (2001) demonstrated that CW parent participants receiving a motivationally enhanced (ME) substance abuse evaluation were more likely to initiate treatment (59%) than those receiving the standard substance abuse evaluation (SE; 29%). More participants completed three or more treatment sessions after receiving ME (30%) compared to SE (17%), yet this finding was not statistically significant (Carroll et al. 2001). However, these results begin to suggest the value of adding MI even to the evaluation process.
When adding a very brief MI intervention for mothers in a substance use treatment, outcomes have not been as promising. Mullins et al. (2004) randomized participants to view educational videos or attend two sessions of MI. There appeared to be no difference in the number of group sessions, program completion, or drug abstinence on urine test outcomes. Perhaps more sessions would have resulted in better outcomes.
Families and MI
MI has also been used as a tool within violence prevention programs for parents, which aim to reduce the incidence of child victimization among high-risk CW populations. In an evaluation of the “ACT: Parents Raising Safe Kids” violence prevention program, Porter and Howe (2008) demonstrated reductions in parent-reported physical punishment of children, hostile attributions of child behavior, and attitudes about spanking children. Upon completion of ACT, parents’ opinions of the value of social skills were also increased, relative to pre-program assessments (Porter & Howe, 2008). Of 18 participants, only 6 completed the 3-month follow-up. Positive parenting, anger management, and misdirected frustration showed no change, as did media literacy, family connection/affection, and beliefs about crying/screaming child. Similarly, no changes were noted when examining child observational outcomes using the Behavior Assessment System for Children (BASC-2).
Similarly, the Caring Dads program, which incorporated MI, improved engagement and reduced parental resistance (Scott & Lishak, 2012). Concerning anger (Buss-Perry Aggression Questionnaire), significant small-effect (d=~0.2) reductions were noted on two subscales: Hostility and Verbal. On the Parenting Scale, a significant medium effect (d=0.3 to 0.4) was noted for the Overreaction subscale, and small-effect reductions were noted for the Laxness and Hostility subscales. Lastly, the father’s perception of co-parenting measured with the Parenting Alliance Measure demonstrated significant medium-effect improvements in both domains (Communication and Respect). This suggests the potential for adding MI to mandated parenting classes.
A pre-experimental study of Combined Parent-Child Cognitive-Behavioral Group Therapy demonstrated pretest and posttest differences for child-reported PTSD symptoms, parent- and child-report of corporal punishment, as well as parental anger (measuring behavior and intensity; Runyon et al., 2009). The effects of these significant clinical improvements were large (d=0.85 to 1.33). This pilot study successfully demonstrated both the feasibility and utility of this novel therapeutic approach to family treatment in cases of child physical abuse. Future studies of this type of intervention should track child maltreatment/neglect outcomes to determine the impact of this intervention on CW outcomes.
Forrester, Copello et al. (2008) also found MI to be a beneficial approach when implementing intensive family preservation services. Within a quasi-experimental study, this MI-enhanced service (MI+IFS) reduced the number of days children were in care and, thereby, the total costs of care (Forrester, Copello et al., 2008). However, there was no reduction in the likelihood of a child entering care when compared to the comparison group. Lastly, a greater proportion of children receiving MI+IFS (68% vs 56%) were residing at home at the time of follow-up. Qualitative interviews with parents and children involved with MI+IFS provided positive accounts of the program. With parents, six strengths of the program were identified: (1) a “non-judgmental and understanding approach”; (2) “good open communication between the worker and the family”; (3) “availability, reliability and high frequency of contact”; (4) “suggesting helpful strategies and offering practical support”; (5) “support with substance problem”; and (6) “help with family relationships” (Forrester, Copello et al., 2008, pp. 417-418). Child interviews suggested increased confidence leading to better outcomes with school and friends. A strength of this study is the focus on parent, child, and CW outcomes. Family preservation is an ideal environment for MI to be incorporated.
Only four studies with CW populations could be located in which outcomes were mixed or poor (Dauber et al., 2017; Forrester et al., 2018; Mullins et al., 2004; Webb et al., 2016). Aside from these noted departures, initial studies suggest the potential value of incorporating MI with CW populations to improve parent engagement, improve relations with the CWWs, and/or improve maltreatment outcomes. See Table 1 for a summary of these studies.
Discussion
The current article reviewed the use of MI in CW settings given its potential for growth. Based on the review, MI appears to be a promising intervention for CW-involved families. This review also identifies gaps in the literature that could be used to guide further research. Of interest would be research that helps develop an understanding of how MI may impact CW-specific outcomes, including family functioning, reunification, child maltreatment/neglect, and recidivism. Also of value would be the experiences of parents and children as well as CWWs attempting to incorporate MI into their practice.
This narrative review of the literature was an attempt to synthesize some of the information on MI. Some papers may not have been identified through our search approach, as they did not adequately describe interventions and may not have used the terms MI or used the term in only a cursory fashion. For example, Family Drug and Alcohol Courts (FDACs) are an increasingly important venue within the CW landscape. While these courts draw explicitly upon “therapeutic jurisprudence,” which is informed by techniques closely related to MI (Harwin, Alrouh, Ryan, & Tunnard, 2013, p. 462), these connections are not explicitly defined in ways that allow drawing conclusions that any outcomes of FDACs are attributable to MI components of the general FDAC model. While outside of the scope of the current review, this discussion of the role of FDACs relating to CW outcomes can be followed elsewhere (e.g., Harwin et al., 2018).
Currently, CWWs experience significant burdens in the form of high caseloads and stressful work conditions, often while feeling inadequately supported professionally, emotionally, or financially (e.g., Griffiths & Royse, 2017; Griffiths, Royse, Culver, Piescher, & Zhang, 2017; Kim & Koa, 2014). It would be interesting to know if CWWs found the approach valuable in improving engagement with families, decreasing parental resistance, enhancing collaborations, decreasing burnout and turnover rates, and decreasing CWW time commitments or stress. This information would be important for CWWs to understand before they invest the time and resources to learn and incorporate MI into practice.
Use of MI in CW settings or populations is likely to increase due to growing evidence of its value with a number of presenting problems (Lundahl et al., 2010). Barth, Lee, and Hodorowicz (2017) suggest that training CW SWs in MI may be an approach to improve child well-being, an idea that is currently being evaluated by the National Center for Evidence-Based Practice in Child Welfare. The prioritization of teaching an evidence-based practice by a coordinated number of programs could lead to novel approaches to train CW students. Some graduate-level social work programs are already training students for MI practice (Barth et al., 2017; Iachini, Lee, DiNovo, Lutz, & Frey, 2018; Pecukonis et al., 2016), which may reduce the cost of training those entering the CW workforce. Two successful models of MI training within social work education include Pecukonis and colleagues’ (2016) training of CW students in MI using live simulation of standardized clients under the supervision of an MI supervisor as well as Iachini and colleagues’ (2018) seamless integration of MI training into field education and community practice opportunities.
The incorporation of training for the CW workforce and incoming workforce could be accomplished through a combination of additional approaches. Some training programs have MI elective courses (e.g., University of Buffalo School of Social Work), standard curriculum courses (e.g., University of Illinois), skills lab courses (e.g., University of Alabama School of Social Work), certificate programs (e.g., University of Maryland), digitally available case simulations to practice MI skills (www.kognitocampus.com), and continuing education opportunities for workforce training. A number of social work programs across many states have had the opportunity to receive Screening, Brief Intervention, and Referral to Treatment training funding through the Substance Abuse and Mental Health Services Administration to provide MI training to students, faculty, and clinical providers in the community, creating opportunities for dissemination on multiple levels. There are also available textbooks and workbooks on the use of MI in social work (Corcoran, 2016; Hohman, 2012). In addition, there are videos specific to training MI in CW developed by the University of Minnesota and University of California, Davis (Hall & Hohman, 2012). Moreover, collaborative partnerships similar to those described by Iachini and colleagues at the University of South Carolina (2018) could be developed with Motivational Interviewing Network of Trainers, which hosts live and self-paced online training courses.
Systemic and organizational factors could impact the delivery of MI and should be considered during implementation. MI might best be seen as a practice that needs to permeate an organization, from uppermost administrative personnel to frontline caseworkers, as suggested by Dauber and colleagues (2017). To do so, the spirit of MI should be applied at all levels of a CW agency: between the director and supervisors, between supervisors and CWWs, and between the CWWs and families. Without ongoing modeling from CWWs’ supervisors, MI practices may be less likely to be implemented into practice (Dauber et al., 2017). Forrester et al. (2018) trained both child protection workers and their line managers as part their most recent study on implementing MI in CW settings. The next step would be to apply this to all levels. Clarke and Giordano (2013) recommend incorporating the MI spirit to engender an “accepting, collaborative, and compassionate atmosphere” (p. 256). They also suggest using the four MI processes “to create a person-centered style” (p. 249) in supervision with the goal of developing strong worker and supervisor alliances. This could lead to staff retention, which is important in CW agencies (Kim & Kao, 2014).
An initial two-day MI training workshop can introduce administrators and CWWs to MI and allow preliminary practice of MI skills, while ongoing coaching can encourage retention and adoption of skills. Ongoing use of a manual for training clinicians in MI, Motivational Interviewing Assessment: Supervisory Tools for Enhancing Proficiency (Martino et al., 2006), can offer opportunities for CWWs to become more comfortable with MI. Concurrently, coaching or additional supervision by an MI trainer or expert can aid in implementing the MI approach. Based on a meta-analysis of post-MI training (Schwalbe, Oh, & Zweben, 2014), four coaching sessions at a minimum are needed for retention and skill acquisition along with the preliminary workshops. Dauber and colleagues (2017) expressed that some of these approaches may be used to improve the implementation in future trials. For example, Hall and Hohman (2012) provide a manual specifically on applying MI to CW settings, which is available at no cost along with corresponding videos online. Given the results of Forrester et al. (2018), more research is needed on the amount of MI training and supervision needed to improve skills as well as possible CW outcomes. One must also consider the complex nature of CW work in examining best training strategies and their outcomes.
In many cases, CWWs are struggling to help parents address more addictive drug use alongside mental health problems with constrained community resources (Mowbray et al., 2017). As one part of this complicated process, MI has the potential to strengthen the relationship between parents and CWWs, which in turn would reduce CWWs’ time and stressful interactions while potentially improving outcomes for children and their families.
Footnotes
Disposition editor: Sondra J. Fogel
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.