
Abstract
Nearly ten years ago, Families in Society published an article (Kim, Smock, Trepper, McCollum, & Franklin, 2010) that discussed the empirical status of solution-focused brief therapy (SFBT) and its progress toward being accepted as an evidence-based intervention in the United States. In the last decade, new growth of experimental design studies using SFBT with diverse populations has occurred. The current article provides an update on the evidence-base of SFBT, showing favorable results on emotional, behavioral, and interpersonal issues. Resources for practitioners on SFBT training are also included.
Keywords
Introduction
Developed in the early 1980s, solution-focused brief therapy (SFBT) evolved out of the brief family therapy models by an interdisciplinary team of therapists, led by two social workers, Steve de Shazer and Insoo Kim Berg (Lipchik, Derks, LaCourt, & Nunnally, 2012). SFBT is widely taught and used in social work practice (Franklin, 2015), and it is therefore very timely that this article will appear in the 100-year anniversary of Families in Society that celebrates family-centered social work and the contributions of social work practice. SFBT is a therapy model whose core therapeutic processes are working with the co-construction of meaning, the strengths of the client, the establishment of a cooperative helping relationship, setting collaborative goals with client, the use of positive emotions (i.e., hope), and working with clients to build their own solutions (Franklin, Zhang, Froerer, & Johnson, 2017). The purposeful use of language and how to ask questions are very important for how SFBT works and are interrelated with the co-construction process, cooperative helping relationship, and solution-building (Berg & De Jong, 1996; De Jong & Berg, 2001). For example, social workers using SFBT facilitate conversations with clients that describe, in great detail, what their life will look like when the problem is no longer present in their lives. SFBT became known for questions such as the miracle question, scaling questions, best hopes, and relationship questions that were used to facilitate the relationship and the co-construction process with clients.
In the beginning, SFBT was studied in a family services agency where clinicians were trying to discover the best brief therapeutic techniques for client change. It was in this spirit of inquiry that the first small scale qualitative observations, program evaluations, and quasi-experimental studies were completed on SFBT (Lipchik et al., 2012). Over the past 15 years, however, more rigorous quantitative research methods using randomized controlled trials (RCTs) have greatly increased, resulting in SFBT being recognized as an evidence-based intervention. The empirical evidence on SFBT moved forward quickly as more researchers across disciplines became interested in SFBT. Hastening research was the evidence-based practice movement in mental health and psychotherapy, which emphasized empirically supported treatments. A decade ago, we set out to describe an evaluative process for how SFBT was considered for inclusion in three national evidence-based practice (EBP) registries in the United States. At that time, it was unclear to us how therapy models and programs were deemed evidence-based and how SFBT would be rated by some of the recently developed U.S. evidence-based registries. This seemed to us to be very important larger systems work that would benefit social workers and other clinicians who were worried that SFBT sessions would not be reimbursed by funding agencies and that they may not even be allowed to use SFBT with clients. This culminated in the first article published in Families in Society by Kim, Smock, Trepper, McCollum, and Franklin (2010) that explored whether SFBT was evidence-based and also reported what we learned from our work in having SFBT submitted to U.S. federal registries.
It has been 10 years since we began submitting SFBT research studies to evidence-based registries and almost 10 years since the publication of our original study, and much has changed since that time both in the evidence-based status of SFBT and on the U.S. national front concerning the evidence-based registries. Thus, the aim of this article is to update the status of SFBT as an empirically recognized evidence-based intervention and revisit the question, “Is SFBT evidence-based?”.
State of SFBT Research
Since our initial article in 2010, several RCTs and quasi-experimental studies have been completed on SFBT; the addition of these studies and their overall positive results continue to increase our confidence in the evidence base of SFBT. Take, for example, the growth of SFBT research from 2000 to 2013 as demonstrated by two narrative reviews of SFBT outcome studies. Gingerich and Eisengart (2000) could only identify 15 outcome studies that were completed with experimental designs. Of these studies, the authors were hard pressed to find quality studies of any sort and few RCT studies. They rated the studies with five receiving a strong rating, four receiving a moderately strong rating, and six receiving a weak rating. In comparison, Gingerich and Peterson (2013) identified 43 SFBT outcome studies that met the criteria for their review. This was both a sizable change in number and quality of the studies. These authors indicated that (74%) of the studies reported significant positive benefit from SFBT.
It is also important to note that several RCT studies have been conducted across different populations and countries than are reported in these reviews. Unfortunately, many studies are not in English and are not available for inclusion in systematic reviews. An evaluation list of published studies, however, identified 143 randomized clinical trials on SFBT as of March 2017 (http://blog.ebta.nu/wp-content/uploads/2017/12/SFTOCT2017.pdf). The substantial growth in experimental design studies makes it advantageous to study SFBT using meta-analysis methods that may also help researchers better communicate to practitioners the overall efficacy of SFBT.
Meta-Analysis Studies on SFBT
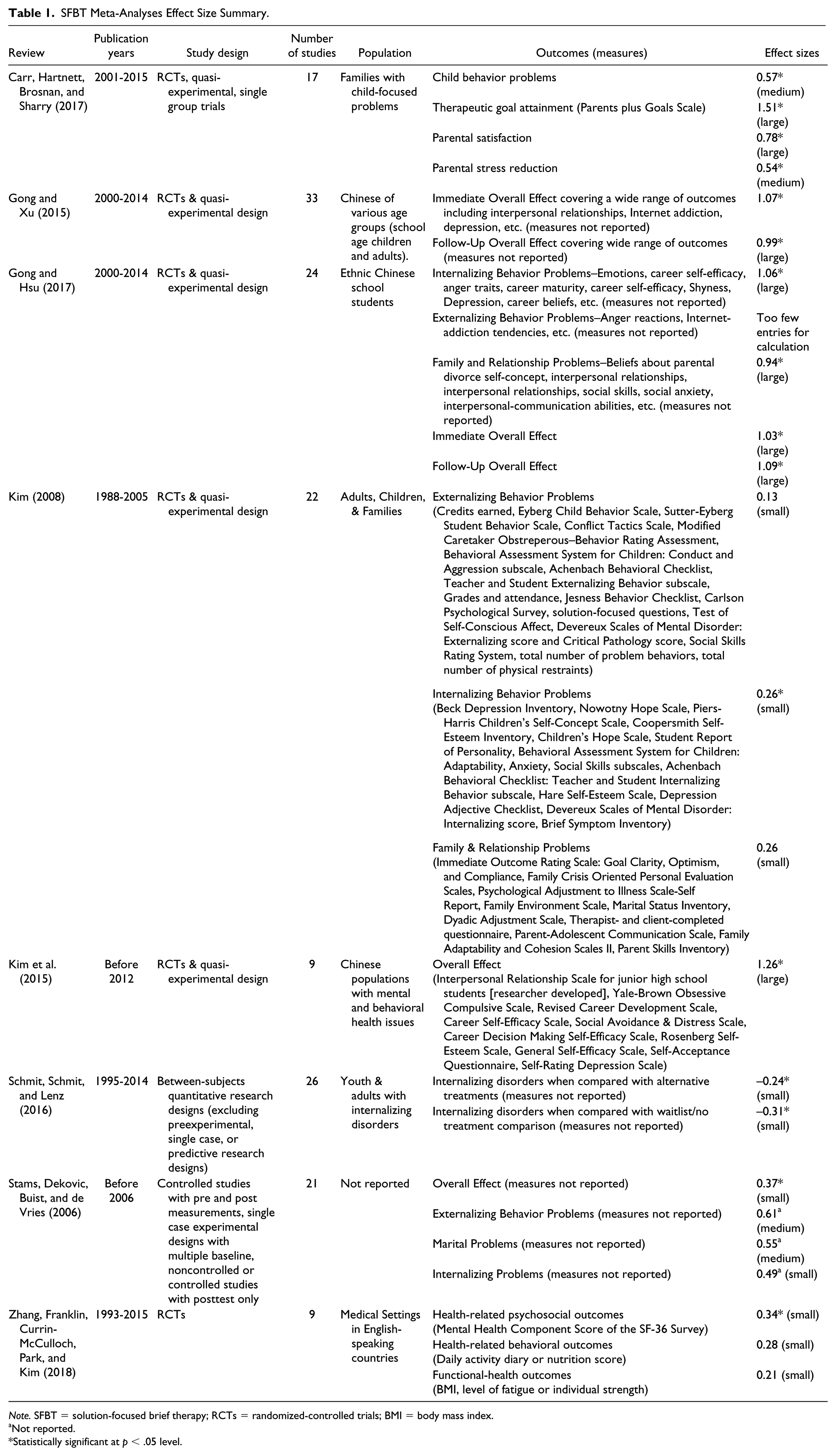
Meta-analysis is a secondary data analysis method where researchers systematically collect data from multiple outcome studies that answer a specific research question (e.g., how effective is SFBT with internalizing mental health outcomes?) and offers an effect size, a quantitative number that statistically calculates how large of a treatment effect the intervention (e.g., SFBT) has on identified outcomes (Franklin, 2015). One important benefit of meta-analysis is the interpretation of the effect size, which is usually described as being small, medium, or large, as well as whether the difference between the groups is statistically significant. Practically, when therapies are effective, it is not uncommon to find a small effect size in effectiveness trials conducted with community-based samples and large effect sizes in controlled efficacy studies (Kim, 2008). What is most important, however, is for the therapy to be able to show a positive effect across multiple studies on similar populations and outcomes. It is equally important to judge the quality of the studies, and RCTs are the gold standard for evaluating whether a therapy is evidence-based. In Table 1, we briefly describe eight meta-analyses that have been completed on SFBT, and overall these studies provide support for the effectiveness of SFBT. The table may also help practitioners better understand the evidence base of SFBT with different populations and outcomes.
SFBT Meta-Analyses Effect Size Summary.
Note. SFBT = solution-focused brief therapy; RCTs = randomized-controlled trials; BMI = body mass index.
Not reported.
Statistically significant at p < .05 level.
Results from Table 1 show that most SFBT studies were conducted in applied, community settings even when the purpose of the individual study was to test its efficacy. The individual meta-analysis studies analyzed a range of outcomes studies from nine to 33 across the different meta-analyses. The overall effect sizes for studies ranged from small to large indicating that in general SFBT was an effective intervention with study populations. Populations varied from families, children, adolescents, and adults and included diverse nations and populations including Chinese, Korean, North American, Europeans, Latino, and African Americans in study samples. This indicates that SFBT is feasible to use with a broad range of clientele. Researchers in the United States and China worked to have some of the Chinese studies that were reviewed in these tables translated and reviewed in English (Kim et al., 2015), and some Chinese researchers have also translated some of the studies for us (Gong & Xu, 2015). Certainly, more of this translation work will lead to an even greater appreciation for the broad evidence base of SFBT.
There were also several different outcomes measured within the meta-analyses including those associated with depression, stress, anxiety, behavioral problems, parenting, substance use, and psychosocial and interpersonal difficulties. One meta-analysis also looked at outcomes when being used in health care and had effective results for health-related psychosocial outcomes (Zhang, Franklin, Currin-McCulloch, Park, & Kim, 2018). These problem areas are all clinically significant areas of importance to most social workers and other clinicians. While the measures used across the studies for the same types of outcomes are different, and not necessarily comparable, some trends can be observed. SFBT has been frequently studied with internalizing mental health outcomes such as depression, stress, and anxiety with consistent results across many of the meta-analyses despite the variance in measures used to evaluate outcomes. One meta-analysis study was specifically focused on the symptoms of internalizing disorders and showed that SFBT had a small effect size (Schmit, Schmit, & Lenz, 2016). However, studies from China also showed that it had a very large effect size (Kim et al., 2015), and this difference might suggest a population effect or a setting effect, or may highlight other cultural factors that contribute to the difference in the size of the effect. Several of the meta-analyses also show that SFBT is effective when behavioral problems and substance use are outcomes, but there appears to be more mixed results with externalizing outcomes in comparison to internalizing outcomes.
Interestingly, few studies on SFBT have measured changes in substance use and this is despite its noted use in clinical practice with clients who use substances and the frequent co-morbidity of substance use with depression and anxiety disorders (Reddy, Bolton, Franklin, & Gonzales, 2018). In addition, SFBT is studied in school settings across different countries, as well as outpatient mental health and community agencies that serve youth and families.
Feasibility and Effectiveness of SFBT in Community-Based Settings
Important to the developing evidence base of SFBT is the fact that it has proven to be an intervention that can effectively be used by social workers in community-based settings. For example, SFBT has accumulated research from schools and is an intervention that is used by school social workers (Kim, Kelly, & Franklin, 2017). Garza High School in Austin, Texas, was the first school in the United States to implement a school-wide solution-focused approach as a way to help at-risk students. Garza High School has now sustained the solution-focused approach for 17 years and has become a model alternative school program, demonstrating the feasibility and effectiveness of the use of SFBT with at-risk youth in public schools. Studies on Garza High School range from quasi-experimental, qualitative, concept mapping, and program evaluations focused on the longitudinal analysis of on-time graduation rates and college readiness of at-risk students (Franklin, Streeter, Belcuig, Webb, & Szlyk, under review; Franklin, Streeter, Kim, & Tripodi, 2007; Lagana-Riordan et al., 2011; Streeter, Franklin, Kim, & Tripodi, 2011; Szlyk, 2018). Garza High School was also selected by the U.S. Department of Education as one of the top dropout prevention and academic success programs (Franklin, Streeter, Webb, & Guz, 2018).
In another community-based example, Broward County, Florida, has embraced the PROMISE program (a SFBT founded program for “targeting both short- and long-term academic success, aligning best practice models and Restorative Justice principles, and developing pro-social and resilience skills”) as a community partner (PROMISE Program, 2017). In 2014, the program was awarded the Community Partner of the Year award for the dramatic decrease in juvenile arrests and school expulsion recidivism rates from above 35% (2012-2013) to between 8% and 13% for 3 consecutive years (2013-2016).
SFBT Federal Registry and State Evidence-Based Ratings
Federal agencies and states have evaluated research studies on SFBT and provided some rankings toward its evidence-based status. As discussed in our first article, Kim et al. (2010), we submitted SFBT research studies to three national evidence-based registries in the United States based on the submission criteria for evaluation. The three registries were Office of Juvenile Justice and Delinquency Prevention (OJJDP) Model Program Guide, SAMHSA National Registry of Evidence-Based Programs and Policies (NREPP), and U.S. Department of Education What Works Clearinghouse (WWC). Since this time, two of the registries have discontinued due to withdrawing of federal funds (OJJDP & NREPP), and one registry has ceased reviewing almost all of their topic areas (WWC).
Table 2 provides a current overview of SFBT by national registries. As is indicated in the table, we have submitted different studies on SFBT to four national registries and the intervention was rated as promising by two of the registries. SAMHSA’s National Registry of Evidence-Based Programs and Practices and OJJDP rated the intervention promising. In a submission to the California Evidence-Based Clearinghouse for Child Welfare (CEBC), a SFBT intervention in child protective services was reviewed as being a highly relevant topic but not yet rated, waiting for further data to be presented from the ongoing SFBT studies. However, in a submission to the CEBC by another research team, Solution-Based Casework, which incorporates elements of SFBT, was rated as a promising intervention (Antle, Barbee, Christensen, & Martin, 2008).
National Registries of Evidence-Based Practices.
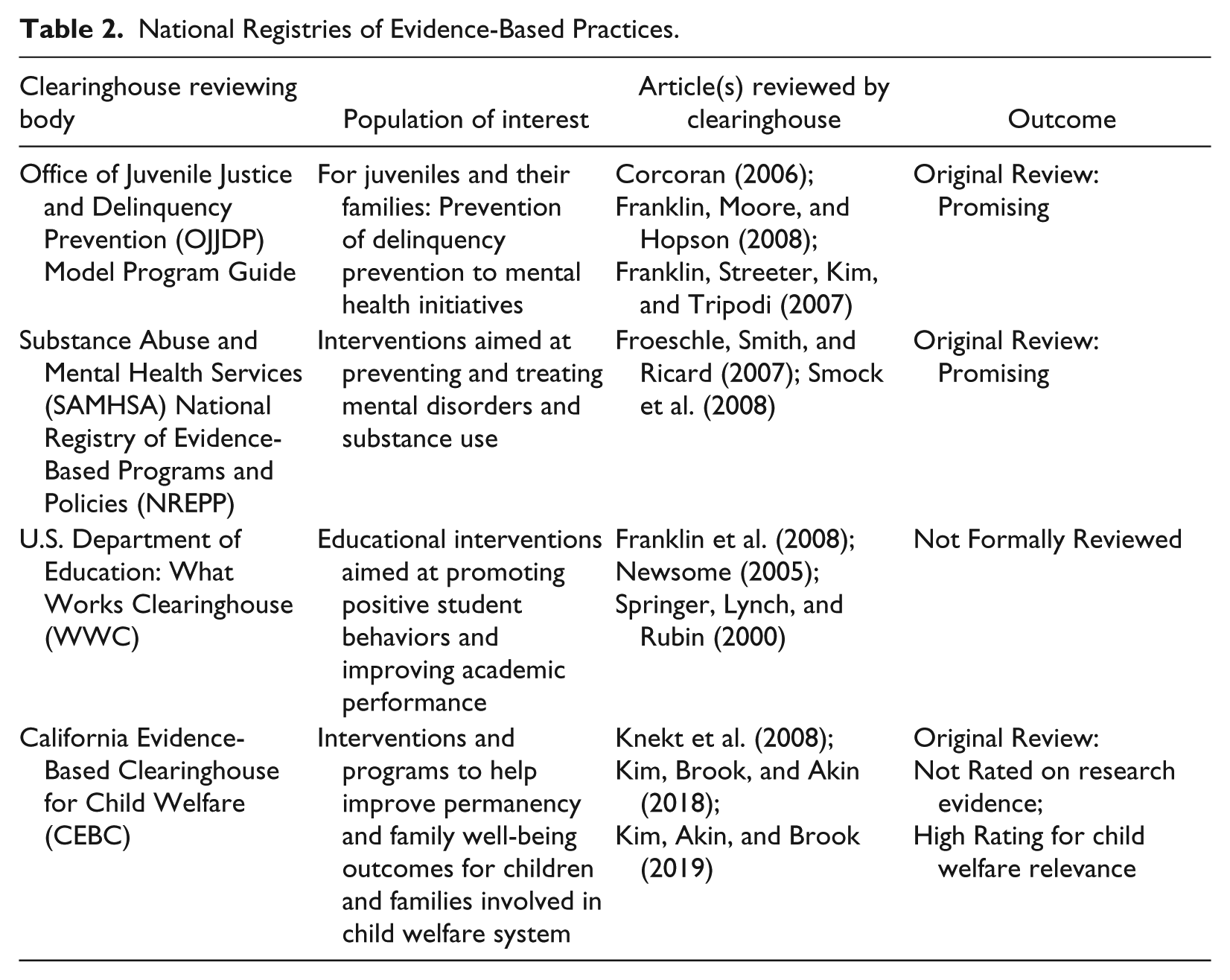
Current SFBT studies have recently been funded by federal agencies to study the efficacy of SFBT in child protective services (Kim, Akin, & Brook, 2019; Kim, Brook, & Akin, 2018). In addition to those mentioned, there are other studies that are currently being funded by federal agencies on the Signs of Safety measures (https://www.signsofsafety.net/). When current studies are finished, and have undergone peer review, we will be able to better evaluate the evidence base of SFBT within child protective services.
Beyond the federal registries, two states in the United States have also included SFBT on their websites as evidence-based interventions. Oregon’s Addiction and Mental Health Services Department lists various treatment approaches as evidence-based for addiction and/or mental health disorders, co-occurring disorders, or prevention approaches. Currently, SFBT is listed as evidence-based for mental health disorders (Oregon Health Authority: Addictions and Mental Health Services, 2017). Similarly, the state of Washington has listed solution-based casework as an evidence-based practice through the Washington State Department of Social and Health Services: Children’s Administration (2017).
Implications for Practice
The process of evaluating an intervention as evidence-based is an ongoing and evolving process. Since the first article that appeared in Families in Society, Kim et al. (2010), SFBT has made big strides by increasing the number of rigorous outcome studies and appearing on OJJDP MPG and SAMHSA NREPP as a Promising intervention. Recently, SFBT as an intervention for child welfare–involved families has been reviewed by CEBC and listed on their website with a High child welfare relevance rating but received Not Able to be Rated for scientific rating. These ratings by CEBC can change as researchers submit additional SFBT outcomes from ongoing studies focused on child welfare. For example, a recently published study by Kim et al. (2019) has been submitted to CEBC as additional empirical support on SFBT and is currently being reviewed. A forthcoming follow-up study to Kim et al. (2018) is under journal review and will also be submitted as additional empirical support for the effectiveness of SFBT with families involved in child welfare.
While national registries like SAMHSA NREPP and CEBC are one way to gauge whether an intervention or program is evidence-based, examining the overall body of empirical support provides a more robust perspective. Thus, a decade later we revisit our original question about whether SFBT is evidence-based by examining the growth in outcome studies that use experimental designs. Based on the progress SFBT has made, we assert that SFBT is a practice that is based on evidence. As indicated by the eight meta-analyses reviewed, the numbers of experimental design studies on SFBT have increased, providing us greater confidence in the evidence base of SFBT for treating internalizing symptoms, behavior problems, and social and interpersonal difficulties. SFBT studies also show the applicability of SFBT in the community across schools, mental health clinics, and health care settings, as well as the feasibility of its use with diverse populations and age groups.
Researchers across several different countries have worked together to make the SFBT research more accessible to all clinicians (Franklin, Trepper, Gingerich, & McCollum, 2012). Even with these efforts, however, the spread of SFBT and its use across the globe challenges researchers to be able to improve and assess all the SFBT research. There is now a large number of RCTs written in several different languages (Mandarin, Japanese, Korean, Persian, Spanish, Dutch, etc.), and this makes across-country comparisons important to be able to synthesize all the studies for practitioners. One limitation of the international SFBT meta-analysis studies not published or translated into English is our limited ability to review the methodological rigor of the studies.
Our best hopes are that as this research is more widely available, clinicians and clients will have a greater ability to choose SFBT as an approach that is right for them. We hope the update in this article has provided the foundation for practitioners to use SFBT because we believe there are many benefits to continuously improving practice and working within an evidence-based framework. Spring (2007) outlined several benefits from working from an evidence-based perspective such as (1) improving quality and accountability, (2) keeping treatment costs low, (3) fulfilling our ethical mandate to do our best for clients, and (4) empowering practitioners and consumers. Although implementing evidence-based practice is important, there are some potential barriers that may impede practitioners from utilizing this evidence-based practice.
Generali, Foss-Kelly, and McNamara (2011) reported that lack of training, limited access to treatment manuals, inadequate research and evaluation skills, and limited professional supervision are all obstacles to EBP. SFBT has taken steps to mitigate several of these barriers. There are several training institutes within the United States and across the globe that provide ongoing training. For example, the Institute for Solution-Focused Therapy (https://solutionfocused.net/) that provides a certification program, the research and training consortium (SFBT Consortium on Implementation, Training, & Evaluation) between the University of Denver and the Steve Hicks School of Social Work at The University of Texas at Austin that provides ongoing training for research projects and community agencies (https://socialwork.du.edu/node/1606). In addition, BRIEF International (2017), International Alliance of Solution-Focused Teaching Institutes (IASTI; 2017), Denver Center for Solution-Focused Brief Therapy (http://denversolutions.com), and the Solution Focused Institute of South Africa (2017) provide both training and SFBT certification processes. There are also several national and international organizations that hold regular training events and conferences (i.e., Solution Focused Brief Therapy Association [SFBTA; 2017], European Brief Therapy Association [EBTA; 2017], and Australasian Association for Solution-Focused Brief Therapy [AASFBT; 2017]). In addition to these ongoing training opportunities, the SFBTA has published a free downloadable treatment manual (Solution-Focused Brief Therapy Research Page, 2017) that is accessible to all professionals.
To further address the barriers to using EBP, the SFBTA research committee has continued to get SFBT recognized and included on national registries (as noted in this paper above). Alastair MacDonald in the United Kingdom began maintaining an ongoing list of research from around the world that illustrates the current research available regarding the outcomes of SFBT (MacDonald, 2017). This comprehensive list makes finding research easy for all users and is now being updated by SFBTA and EBTA. The SFBTA has also attempted to address the limited supervision barrier by including a mentoring section on their website (SFBTA, 2017). Clinicians can sign up to receive mentoring from experienced clinicians. Solution Focused University (2017) has also been established to provide ongoing collaboration, consultation, and networking opportunities for SFBT clinicians across the globe.
Conclusion
Over the past 10 years, SFBT research has grown, and these studies have produced considerable evidence that have increased its worldwide recognition. This article summarizes the status of SFBT as an evidence-based intervention via research studies that are summarized in meta-analyses. Practitioners can take confidence in the growing evidence base of SFBT and use it when it is a good fit with their client and clinical context. Now, there are also a number of training resources available for practitioners to learn and gain competencies in SFBT, and this is also a step forward in enhancing SFBT for use in practice. To keep moving forward with the evidence base of SFBT, researchers need to work together and with clinicians to improve outcome studies. It is important for studies to build on one another using similar measures, populations, and study designs because this has not been done in the past. To improve our confidence in the evidence base of SFBT, it is important to continue to produce more rigorous research designs that match high standards for RCT studies.
Future studies need to include methods such as randomization, intent-to-treat analysis, long-term follow-up, and blinding methods. Most of the SFBT studies are from small community samples and need to be scaled up to larger clinical trials. This is beginning to happen now on studies conducted within child welfare and criminal justice but needs to extend to other areas where SFBT has shown effectiveness. The studies also need clear documentation for treatment fidelity and program dissemination materials. Finally, it is important not only for the studies to improve but also for researchers to continue to analyze SFBT outcomes studies with high-quality meta-analytic studies and to make those reviews available to practitioners and policy makers.
Footnotes
Disposition editor: Sondra J. Fogel
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.