
Abstract
Non-medical opioid use (NMOU) has had a devastating effect on families. Affected families may experience interpersonal and financial problems and self-stigma that can impede help-seeking and self-care. This study aimed to identify recommendations for families affected by opioids given by those with lived experience. Adults with a family member with NMOU (N = 299) completed a survey that included an open-ended question asking for advice for other families similarly affected by opioids. Data were coded independently by research team members using an iterative approach to thematic analysis. Themes included seeking support, seeking education, and managing relationships with the loved one and others. Results highlight avenues for helping families cope while supporting a loved one who uses opioids, including contact with others with shared experience and access to educational resources. Families affected by opioids can provide valuable insights that should be considered when designing supports for families.
Introduction
Non-medical opioid use (NMOU) 1 and opioid overdose are significant public health burdens that have had devastating effects on families. In 2021, nearly 108,000 drug overdose deaths occurred in the United States, with most involving opioids. As NMOU and opioid overdose have escalated, it has been increasingly common for Americans to be personally affected. A Pew Research Center survey (2017) indicated that 46% of Americans had a family member or close friend with a drug or alcohol addiction. Having a loved one who uses drugs can be highly stressful (Fraser et al., 2009). In families with non-medical substance use, substance use often becomes a significant focus within the family (Daley et al., 2018). The consequences of non-medical substance use often extend past the individual to their family members, affecting relationships, finances, daily routine, and leisure activities (Nebhinani et al., 2013; Sharma et al., 2019). Family members of people with substance use disorders (SUDs) experience higher rates of depression, anxiety, stress, trauma, and suicidality (Ray et al., 2009; Richter et al., 2000). Non-medical substance use is also associated with marriage instability and interpersonal violence (Godleski & Leonard, 2019).
Family members of people who use drugs are further affected by courtesy stigma, or stigma due to their association with their relative who uses drugs (Goffman, 1963). A national survey found that public stigma toward family members of people with SUDs exceeds that toward families affected by other health conditions (Corrigan et al., 2006). Family members are often blamed for the onset of their relative’s substance use (Corrigan et al., 2006). Qualitative studies indicate that public stigma drives shame, hopelessness, and isolation among family members, which can impede help-seeking and self-care (McCann & Lubman, 2018a, 2018b; O’Shay-Wallace, 2020).
The relationship between substance use and family functioning is reciprocal; just as NMOU can affect family functioning, family members can influence their loved one’s treatment and recovery trajectory. Family conflict, low family support, and substance use among family members have been associated with poor treatment outcomes, including delayed initiation, poor retention, and increased substance use following treatment (Rowe, 2012). Conversely, family involvement can increase treatment initiation and engagement and improve recovery outcomes (Hogue et al., 2021). Many affected family members (AFMs) regularly have contact with their loved one who uses drugs. A survey of AFMs involved with a family support group found that half reported daily contact with the loved one and an additional third reported weekly contact (Bagley et al., 2015). Information and support for AFMs can potentially have a substantial impact.
Given the bidirectional link between substance use and the family, family-centered interventions are among the most effective approaches for caring for people with SUD (Hogue et al., 2018; Rowe, 2012). Relative to individually focused treatment, treatment approaches that integrate family members are associated with greater reductions in substance use and related problems, with positive effects retained 12 to 18 months post-treatment (Ariss & Fairbairn, 2020). However, health care and treatment providers often overlook the potential for family members to affect the success of treatment outcomes; family members are often excluded from the treatment process or even blamed for their loved one’s non-medical substance use (Ventura & Bagley, 2017). Experts are calling for the substance use treatment system to move toward a more strengths-based, family-centric approach (Dopp et al., 2022; Ventura & Bagley, 2017). Providers should engage family members in treatment and recovery services and be knowledgeable about the various supports available to AFMs. Family centric approaches that consider the needs of both the individual with NMOU and their AFMs may be more effective for the individual with NMOU.
Previous Studies and Research Gaps
Previous research on family members of individuals with NMOU has focused primarily on AFMs’ experiences of having a loved one with an opioid use disorder (OUD; McCann & Lubman, 2018a, 2018b; O’Shay-Wallace, 2020) and the role of family members in their loved one’s opioid use (Khan et al., 2019; Robertson et al., 2022). While previous research on the experiences of AFMs identified stigma (O’Shay-Wallace, 2020), stress (McCann & Lubman, 2018), and barriers to help-seeking (Nebhinani et al., 2013) as significant burdens, we are unaware of research that qualitatively examined support needs and advice from the perspective of AFMs offering advice to other AFMs. Two recent studies examined interventions to increase the well-being of AFMs. Dilkes-Frayne and colleagues (2019) found positive results from online counseling for AFMs while others (Kelly et al., 2017) found positive results for AFMs from a structured and free peer-support program. It is likely, however, that AFMs need various types of formal and informal support across the many domains of their lives, much more than discrete interventions can provide. AFMs who have experienced having a loved one with NMOU can provide valuable insights that should be considered when designing supports for families. The advice AFMs give to others can be indicative of what services they find helpful or unhelpful and areas where further support is needed.
Study Aims
Little research to date has examined or identified the distinct and specific needs of AFMs, nor has previous research identified the specific types of support that AFMs experience as most helpful. Therefore, the aim of this study was to understand the specific needs of AFMs, distinct from the needs of their family members with NMOU, by examining what AFMs would advise others going through similar experiences. The primary research question guiding this study was: What recommendations do AFMs have for other families dealing with a close family member with NMOU from the perspective of their own lived experience? Study findings may support providers serving people with NMOU and their families.
Method
Adults with close family members with NMOU (N = 299) were recruited to complete a web-based survey about their experiences. Publicly funded treatment providers in Michigan and support groups for family members (e.g., Families Against Narcotics) shared recruitment materials through social media and email. Information was also shared on a university social media platform. Participation was limited to those with a close family member with NMOU (i.e., parent, stepparent, child, stepchild, sibling, stepsibling, or spouse).
The survey asked questions about demographic information (i.e., age, gender, race, education, and income) and about the participant’s loved one(s) who used opioids. These included questions about their relationship, OUD diagnosis, intravenous drug use, overdose history, and whether their loved one died by overdose. The survey also included an open-ended question asking, “What advice do you have for other families seeking support for themselves?” Over two thirds of survey participants (205 out of 299 or 68.56%) answered this open-ended question. Although individual incentives were not provided, all participants could enter a gift card drawing. Data collection took place from November 2018 to February 2019. The Wayne State University institutional review board approved all study procedures.
Data Analysis
Descriptive statistics were examined for demographics and questions about the participant’s loved one(s). Chi-square tests and t-tests were used to compare the respondents who answered the open-ended question to the full sample of survey participants.
For the qualitative analysis, we explored participant responses to the open-ended question about advice for other families seeking support using inductive thematic analysis (Braun & Clarke, 2022). Our experiential approach aimed to capture and explore people’s own meanings and understandings (Braun & Clarke, 2022). This approach was a flexible method for identifying, analyzing, and reporting patterns within the data through a systematic process. The systematic process includes familiarizing ourselves with the data, generating initial codes, searching for themes, reviewing themes, and producing the report (Braun & Clarke, 2022).
Three research team members independently read and reread participant responses and noted initial themes. As coding and analysis continued, the research team met multiple times to refine the codebook. During these meetings, the research team reviewed the corpus of data to gain a thorough understanding of the data, identify a final set of themes, and find confirming and disconfirming evidence to determine whether each theme was warranted. Themes were revised or eliminated based on evidentiary adequacy until well-warranted assertions remained. The final set of themes that were well-supported by the data is presented in the next section. Example quotes do not represent the only evidence for each theme.
Results
Sample Characteristics
Characteristics of the sample are presented in Table 1. Results of bivariate analysis indicate no significant differences in the demographic characteristics of those who did and did not complete the open-ended question. Participants who completed the open-ended question (n = 205) ranged in age from 18 to 65, with a mean age of 45.88 years (SD = 15.14). More than three quarters of these respondents identified as women (80.5%). Although the majority of respondents who answered the open-ended question self-identified as white (85.4%), a smaller proportion self-identified as Hispanic/Latinx (4.5%), Black or African American (3.5%), or other races or ethnicities (1% Asian, 1% Arabic/Middle Eastern, 4% American Indian, 3.5% Multiracial, and 1.5% other races/ethnicities).
Participant Demographic Characteristics.
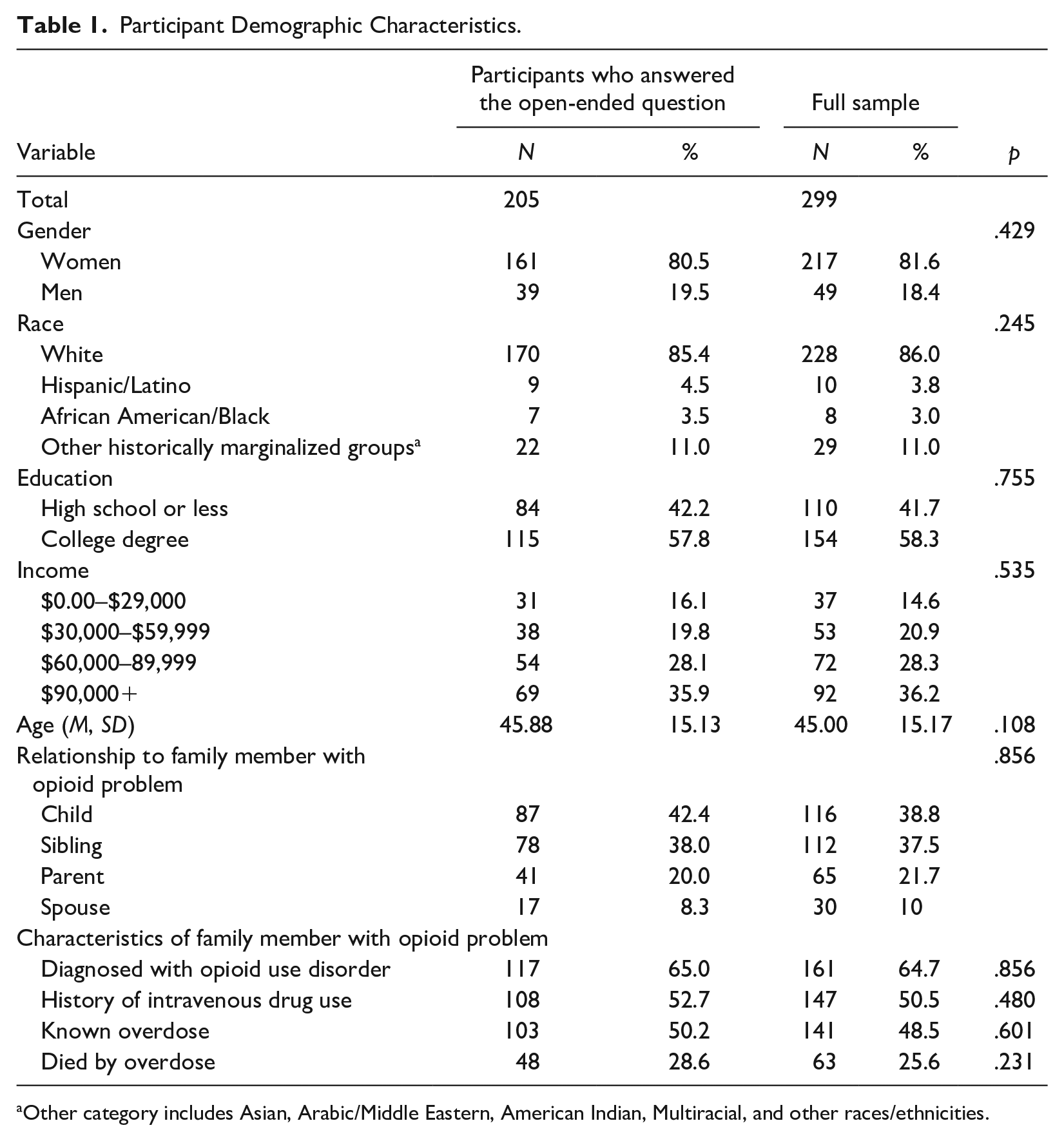
Other category includes Asian, Arabic/Middle Eastern, American Indian, Multiracial, and other races/ethnicities.
Respondents had children (42.4%), siblings (38.0%), parents (20.0%), and spouses (8.3%) who engaged in NMOU. Nearly a third (30.1%) had more than one close family member with NMOU and 65% of respondents reported their family member had been diagnosed with an OUD. About half reported their family member used opioids intravenously (52.7%) and half were aware that their family member had overdosed on opioids (50.2%). Over a quarter (28.6%) reported that a family member died from an opioid overdose.
Open-Ended Responses
For the 205 responses to the open-ended question “What advice do you have for other families seeking support for themselves?,” the mean word count per response was 29.1 words (SD = 36.6). Although some responses (n = 14) were quite brief (e.g., “You need community,” “Families Against Narcotics”), over half of the responses were at least 19 words long (up to 300 words). The advice given by respondents was grouped into nine broad themes (Table 2). Six of these themes were further broken down into subthemes. Eight comments that were either brief or vague were not coded (e.g., “I wish I knew!,” “I don’t really know,” “none”).
Advice for Families of People With Opioid-Related Problems (n = 197).
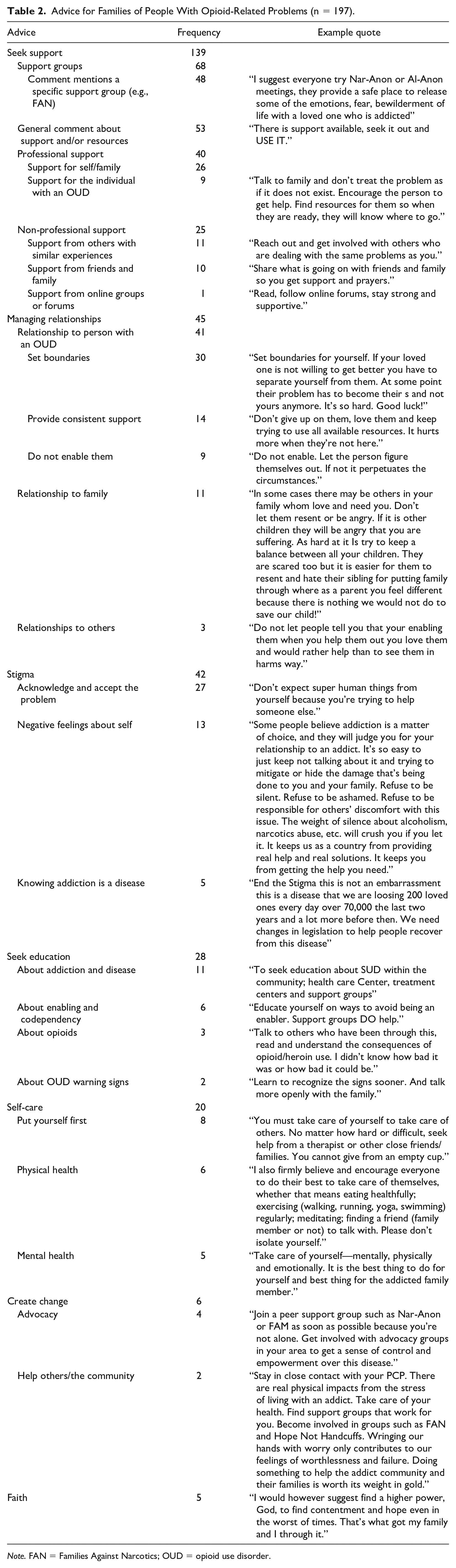
Note. FAN = Families Against Narcotics; OUD = opioid use disorder.
Seek Support
Respondents most commonly advised other AFMs to seek support. Seeking support was mentioned by 68% (n = 139) of respondents. Subthemes included seeking support from support groups, professionals (e.g., therapists, counselors, social workers), and non-professionals. Most responses about support seeking advised AFMs to join a support group. Some respondents named specific groups such as Families Against Narcotics (FAN), Families Anonymous, The Addict’s Mom, and Al-Anon. For example, one respondent shared their experience with support groups by commenting, “Al-anon was the best thing to ever happen to me. It helped me understand that the drugs were not my fault in any way, and that I was being an enabler. Once I established boundaries, I healed a lot.” Other participants noted that social media groups on Facebook were helpful.
Advice to seek professional support included suggestions to speak with a therapist, doctor, primary care physician, family therapist, or family recovery coach. Respondents recommended seeking professional support for individual family members or the whole family. One respondent wrote, “Seeking help from a therapist for yourself is extremely helpful and needed for your own mental health.” Other respondents recommended seeking professional support for the individual with NMOU. Such recommendations included, “The sooner a family member gets into treatment the better they can help themselves, which will also help the family member struggling with addiction.”
Most advice about non-professional support focused on seeking support from friends, family, or others with similar experiences. For example, respondents commented, “Reach out to others that have experienced the same situations,” and “There is no shame in asking friends or family for help.” One individual advised finding support online: “Read, follow online forums, stay strong and supportive.” Respondents also made general comments about support and resources. General comments about support and resources did not specify a form of support. Such statements included, “There is support available. Seek it out and USE IT,” and, “Support is a very important aspect of the recovery process.”
Managing Relationships
The second most common theme of the advice offered by respondents pertained to managing relationships. Managing relationships was mentioned by 22% (n = 45) of respondents. Subthemes included managing the relationship with the individual with NMOU, relationships with other family members, and relationships with non-family members. Responses about managing the relationship with the individual with NMOU gave advice on interacting and setting boundaries with this individual. Advice on setting boundaries included physically separating oneself from the individual and not blaming oneself for the addiction. One respondent summarized this well by stating: “Set boundaries for yourself. If your loved one is not willing to get better, you have to separate yourself from them. At some point their problem has to become theirs and not yours anymore. It’s so hard. Good luck!” Advice on managing the relationship with the individual with NMOU also included not enabling them: “It’s up to the afflicted to help themselves. Be cautious in enabling the afflicted party’s unhealthy behaviors.” Although some respondents advised families to set boundaries and avoid enabling, others advised families to provide consistent support to their loved ones: “This is not a tough love situation. Never turn your back on your loved one. Fight for your loved one . . . ”
Responses about managing relationships with other family members advised others to consider the impacts of opioid use on the family. Effects of opioid use included stress and stigma. One respondent stated, Being the ex-wife of an addict is embarrassing and degrading. There is nothing worse than lying. Addiction affects EVERYBODY in the family. And it was so stressful and difficult trying to display being a normal mom and wife even though his addiction was so obvious.
Some respondents offered advice from their perspectives as a parent of multiple children. One parent stated, “With a child in addiction, it’s important for the parents to present a united front and support each other. If there are other children in the home, remember that they deserve your time and attention, too.”
Three respondents (1.5%) commented on managing relationships with non-family members, including responding to unsolicited advice. For example, one respondent suggested, Learn how to set boundaries and learn how to politely decline advice. Every person out there has an opinion on what you should or should not be doing, only you (or immediate family) can make the best decision for your situation.
Another respondent encouraged others not to be burdened by the attitudes of non-family members, stating, “Refuse to be ashamed. Refuse to be responsible for others’ discomfort with this issue.”
Stigma
About 20% of AFMs (20.5%, n = 42) mentioned stigma or shame. Experiencing stigma can decrease help-seeking and self-care behavior. Subthemes included acknowledging and accepting the problem, negative feelings about oneself, and understanding addiction as a disease. Advice coded as “acknowledge and accept the problem” encouraged family members to talk openly about having a family member with NMOU and accept the circumstances as a way of coping. One respondent summarized this well in their comment: “Talk to family and don’t treat the problem as if it does not exist. Encourage the person to get help. Find resources for them so when they are ready, they will know where to go.” Other respondents advised, “Don’t keep things bottled up. It’s important to find someone you trust to talk about the way you’re feeling,” and, “Everyone makes their own choices. Don’t blame yourself for a family member’s choices.” Respondents encouraged AFMs not to hide this aspect of their life from others.
Other respondents encouraged AFMs not to feel embarrassed or ashamed. Some respondents directly related shame to help-seeking and self-care. For example, one respondent generally commented, “Self-care is very important. Do not be ashamed.” Other family members said, “Don’t be embarrassed. Don’t try to hide it,” and “Please do not let stigma get to you.” Another participant, who was a Black woman, stated, “Don’t be ashamed or afraid. If you feel you need support get it. I tend to see where African-Americans shy away from seeking support, some because they have in the past and have been turned away.” Five respondents commented on the need to view addiction as a disease to reduce stigma. One respondent conveyed this well by advising others, To know they are not alone and there is no shame and to be a part of changing the stigma. This a chronic disease and should be treated that way. This is not a moral failing and addiction does not discriminate.
Seek Education
Nearly 15% of respondents (13.7%, n = 28) advised others to seek education about relevant topics, including “opioids,” “addiction,” “enabling and codependency,” and “the warning signs of an opioid use disorder.” For example, one parent whose child overdosed and died encouraged other families to “read and understand the consequences of opioid/heroin use. I didn’t know how bad it was or how bad it could be.” Another parent encouraged families “to seek education about SUD within the community—health care centers, treatment centers and support groups.” Although mentioned less often, several AFMs commented on education related to “enabling and codependency.” For example, a participant whose sibling had been treated for OUD encouraged other families to “Educate yourself on ways to avoid being an enabler. Support groups DO help.”
Some advice on seeking education was geared toward protecting and helping AFMs. One respondent felt that education may help family members with coping: “The more you learn about addiction, the better you can deal with your loved one’s choices.” Another respondent encouraged others to seek education about the signs and symptoms of SUDs. One woman whose husband had opioid-related problems wrote, Learn about the indicators of substance abuse. I was a stay-at-home mom with two young girls. I didn’t know what was happening with our finances. I realized that expensive belongings began to disappear as well as medication I had been prescribed from a severe injury.
Self-Care
One in 10 respondents (19.8%, n = 20) offered advice on self-care. This advice focused on putting themselves first or prioritizing their well-being. For example, one respondent who had multiple family members who used substances commented, “Worry more about helping yourself than the one with the problem. More often than not, they won’t recognize they even have a problem. Especially if it’s prescribed to them. You can’t help anyone if you can’t help you first.” Other comments about self-care focused on physical health and mental health. One respondent whose child used opioids wrote, “I also firmly believe and encourage everyone to do their best to take care of themselves, whether that means eating healthfully, exercising (walking, running, yoga, swimming) regularly, meditating, finding a friend (family member or not) to talk with.”
Create Change
A small proportion of respondents (2.9%, n = 6) advised family members to create change through advocacy or by helping the community and others affected by substance use. Some respondents based this advice on their own experiences leading community-based projects. One respondent shared, Our son passed in 2011—there was no FAN for support, education, services, etc. in our county. We created one after his death—today, there are over 20 chapters in the state. Seek out a chapter for support—and live their motto—help us help yours and then come back and help us help someone else.
Others commented on the need to change laws. Interestingly, one respondent seemed to favor laws providing substance use recovery services. This respondent stated, “We need changes in legislation to help people recover from this disease.” In contrast, another respondent seemed to favor less legal protection for individuals struggling with addiction. This respondent stated, Drug addicts are protected by too many laws. Those laws hurt them much more rather than help them. Those laws that protect the rights of drug addicts are now causing more sickness to the rest of the family as well as allowing the sick to stay sick. Change the laws and you will see less drug abuse.
Faith
Finally, five respondents (2.4%) mentioned how faith affected their experiences having a family member with NMOU. Four of these comments mentioned prayer, and one respondent advised, “I would however suggest find a higher power, God, to find contentment and hope even in the worst of times.”
Discussion
AFMs can experience high stress and public stigma, which can lead to shame, hopelessness, and isolation. This, in turn, can negatively affect help-seeking and self-care behaviors. Support for families affected by opioids is important for family members’ well-being and for the individual with NMOU. Just as they are affected by their loved one’s substance use, family members can also affect the trajectory of their loved one’s treatment and recovery. For example, family involvement has been linked to increased treatment initiation, treatment engagement, and better recovery outcomes. For this reason, family-centered interventions may be more effective for treating SUDs than individually focused interventions. Despite such research, providers largely focus on the individual in substance use treatment and neglect the positive impacts that family involvement can have on treatment outcomes. Although the relationship between family involvement and treatment outcomes has been established, few studies have explored how family members can be best supported. The goal of this study was to identify recommendations for family members affected by NMOU, from the perspective of individuals with lived experience. Understanding the perspectives of those with lived experience can contribute to our knowledge of best practices for supporting affected families, which in turn improves outcomes for individuals with NMOU or OUD.
In this study, respondents most commonly advised families to attend a support group. Prior studies have similarly demonstrated the benefits of mutual aid among families affected by substance use. For example, Kelly et al. (2017) evaluated Learn to Cope, a support network for family members of a loved one addicted to opioids or other drugs. Participating family members reported the group offered them information and directions from others, a sense of group cohesion, or a sense of group universality. Findings from the current study suggest that affected families find support through speaking to others with shared experience and seeking education, both of which can be indicative of group cohesion and gaining information from others. Together with the current study, this growing body of evidence suggests that support groups can benefit families affected by opioids (Bagley et al., 2015; Kelly et al., 2017). However, more research is needed to further determine which group characteristics make the greatest impacts. Such characteristics may include contact with others with shared experience and access to education. It is also important to note that support groups are a widely known resource for affected families, which may play a role in how many respondents mentioned support groups.
A critical difference between the current study and past research is that this study asked AFMs to share advice on any form of support rather than exploring the role of support groups only. In addition, this sample included family members who were not involved in a support group and may therefore experience greater stigma and isolation. Including a broader range of perspectives in studies of families affected by NMOU is necessary, as there are multiple avenues for supporting families and alternatives to groups should be explored.
Although few studies have examined how alternatives are perceived by family members, researchers have made important recommendations for practice outside of support groups. For example, Lander et al. (2013) recommend that social workers understand the family structure and provide referrals for family members to family therapy, couples therapy play therapy, or other professionals as appropriate. These recommendations are reflected in our findings, as almost 20% (18.7%, n = 26) of respondents in the current study who advised families to seek support also recommended seeing a therapist, recovery coach, or other professional. Similarly, experts recommend educating families on substance use (e.g., treatment options, to correct myths and misconceptions) and helping families maintain their emotional, physical, and spiritual health (Substance Abuse and Mental Health Services Administration [SAMHSA], 2020). In comparison, 14% (n = 28) of current study respondents advised seeking education and one in 10 (10.2%, n = 20) mentioned the importance of self-care, including physical and mental health. Our findings provide support for these recommended strategies as one of the first studies to confirm the acceptability of various services and supports for AFMs.
Other recommendations by SAMHSA’s Center for Substance Abuse Treatment pertaining to support for families include identifying and utilizing family strengths and helping family members address difficult feelings surrounding SUD with a counselor. Identifying and utilizing family strengths may be related to managing the relationship to the individual with NMOU or with other family members, which was mentioned by over one quarter (26.4%, n = 52) of family members in the current study. Our findings in this area highlight the need for professional support for family members as they cope with their loved one’s opioid use and navigate family relationships simultaneously.
Some respondents (4.6%, n = 9) who offered advice on managing the relationship to the loved one with NMOU recommended avoiding “enabling.” Respondents also encouraged others in their situation to seek education about “enabling” and “codependency.” Concerns about codependency and enabling are rooted in 12-step philosophy. From this perspective, “codependent” relationships with loved ones may prevent a person from hitting the “rock bottom” necessary to motivate recovery; family members are instead encouraged to deliver “tough love” to prevent contributing to their loved one’s continued use (Szalavitz, 2016).
While these concepts are deeply engrained in treatment and recovery culture, they are not supported by research. In fact, people with fewer resources and less support are significantly less likely to initiate and maintain recovery; social support, safe housing, employment, and physical and mental health are associated with increased likelihood for success in recovery (Evans et al., 2014; Laudet & White., 2008; Sahker et al., 2019). In addition, 7% (n = 14) of respondents in the current study advised that others provide consistent support to their loved one, which contrasts tough-love-based approaches to recovery. The mixed advice given about managing relationships with their loved one (e.g., tough love or consistent support) suggests that families do not always know how to best help their loved one and protect themselves at the same time (Laudet & White, 2008).
Family members need to protect themselves and their children from the chaos that can result from a loved one’s opioid use. About 15% of respondents recognized this and offered advice on setting boundaries. Counselors and social workers can play an important role in supporting family members as they set firm boundaries while maintaining a relationship with their loved one. This may entail helping clients to identify strategies for self-care, which many family members considered essential to maintaining their own health and wellness as they cared for their loved one.
The terms “codependent” and “enabling” have also been described as labels that are stigmatizing to family members (Wilkens & Foote, 2019). Addressing stigma experienced by family members is critical as it can lead to poorer physical and mental health outcomes, social isolation, and reduced help-seeking. One in 10 family members (8.6%) mentioned stigma in their advice to others. Some family members advised others to not feel stigmatized because addiction is a disease. However, research suggests that conceptualizing addiction as a disease does not necessarily decrease stigma and may reduce hope for recovery (Kelly et al., 2021; Rundle et al., 2021). Further research is needed to identify conceptual frameworks that more effectively reduce stigma toward NMOU among family members. Other studies have found family members often manage stigma by avoiding it rather than by challenging or confronting it (McCann et al., 2017; O’Shay-Wallace, 2020). Although limited, these findings further suggest that stigmatizing concepts remain deeply engrained in approaches to recovery and family support but do not actually serve families and their loved ones (McCann et al., 2017; Sahker et al., 2019).
To mitigate the negative impacts of experiencing stigma, researchers have suggested implementing evidence-based family approaches to recovery, challenging stigma, and addressing stigma within the family unit. In addition, Ashford and colleagues (2019) have suggested that engaging in recovery-related advocacy can reduce stigma among individuals in recovery. This positive impact of engaging in recovery-related advocacy may also be present for AFMs. In fact, seven respondents (3.6%) in the current study advised others to create change surrounding substance use issues and four (2.0%) specifically mentioned participating in advocacy.
Strengths and Limitations
While this study offers novel findings from an understudied population, several limitations should be considered. While the findings are based on over 200 responses, they reflect answers to a single open-ended question. Research using different methodologies, including in-depth interviews with probing, may provide more detailed information on how to best support families affected by opioid use. Still, the current study is one of few studies that explored advice from AFMs and findings can be used to guide further research.
Second, there were no limitations on the number of individuals that could participate from one family unit. It is possible that some repeating themes emerged because respondents from the same family reported similar experiences. However, it is also possible that individuals from the same family have different experiences and would benefit from different forms of support. Future research should explore how effective support for individual family members may differ within a single-family unit, for example, by characteristics such as gender, age, or relationship to the loved one with NMOU (parent, sibling, or other).
Third, respondents could participate in this study even if they did not currently have a family member who is using opioids. Some respondents may perceive their experiences and support needs differently now than they did when their family member was actively using opioids. Support needs may also change if the loved one moves forward in recovery or passes away. Future research should explore how family members’ needs for support change with the trajectory of their loved one’s opioid use and recovery.
Fourth and finally, while this sample of AFMs included a broad range of perspectives in terms of exposure to support groups, stigma, and isolation, most respondents identified as women (80.5%), white (85.4%), and highly educated (57.8%). Future studies should examine the experiences of men, historically marginalized racial groups, and people from different educational backgrounds.
Implications for Practice
The advice shared by AFMs highlight the importance of providing support for families affected by opioid use and the importance of the perspective of individuals with lived experience. Although many respondents advised participating in a support group, our findings suggest that family members feel most supported by their relationships and exchanges with other people, on a professional and non-professional level. Support groups that promote the development of supportive relationships within and outside of the group may be particularly helpful in supporting AFMs. This may include facilitating linkage to counseling professionals and discussing strategies to improve relationships with friends and family.
Increased efforts are needed to link AFMs to professional and non-professional support groups and services. Information about support services needs to be accessible outside of OUD treatment centers, as not all individuals affected by opioid use have a loved one who is currently in treatment. This may include providing information and guidance in accessing services at community centers, online, and at a primary care physician visit. More research is needed to determine how to reach AFMs most effectively and engage them in support groups. OUD treatment providers (such as social workers, substance use counselors, and physicians) can also play an integral role in linking families to support groups when they engage in family-centered therapies. It is important that providers are aware of support groups for AFMs, the positive impact groups can have, and how to link AFMs to groups.
Providers can further support affected families by discussing difficult topics such as managing the relationship to the loved one or other family members, acknowledging and accepting circumstances, and managing stigma. Findings from this study also suggest that the importance of self-care for family members should be emphasized in practice. Providers should aid individuals in finding and engaging in useful and effective forms of self-care.
As providers can play a key role in supporting AFMs, it is important that AFMs are connected to these professionals. Again, future research should explore strategies to reach affected families whose loved one is not currently in treatment or who are not attending a support group themselves. Avenues for connecting families to providers may be established through community centers, online platforms, public service announcements (such as on TV or radio), family medicine settings, or schools. As we continue building knowledge of how to support families affected by opioids, it is equally important to understand how to connect AFMs to such support.
Footnotes
Disposition editor: Cristina Mogro-Wilson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Michigan Department of Health and Human Services under the State Targeted Response to the Opioid Crisis Grant (#TI083298). The Michigan Department of Health and Human Services approved the study design and assisted with recruitment. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funders. The authors would like to thank Families Against Narcotics for assisting with recruitment.