
Abstract
Latina young people report high levels of mental health problems and low levels of help-seeking compared with their white peers, but little research has examined factors influencing their mental health views. Inductive analysis of 25 participants’ narratives revealed that Latina young people described three stages in the development of their mental health-related beliefs, attitudes, and behaviors: undergoing a process of family mental health socialization, suffering in silence, and attaining a new perspective. Within each of these phases, participants shared stories that attest to their agency and resilience. This research uncovers a novel theoretical construct, “family mental health socialization,” which elucidates how young people internalize mental health-related beliefs, behaviors, and norms within their cultural and family context. Implications for social work practice include the need for culturally sensitive, family-centered interventions that promote open communication about mental health.
Latina young people are less likely to seek mental health services than their white peers, despite reporting persistently high levels of depressive symptoms, suicidal ideation, and suicide attempts (Price & Khubchandani, 2017; Stafford & Draucker, 2020). Research has shown that several factors contribute to Latina youth’s underutilization of mental health services, including practical or logistical barriers, negative health care experiences or concerns about treatment, and personal health-related beliefs and attitudes (Lightfoot et al., 2019; Stafford & Draucker, 2020; Wang et al., 2020). Stigma plays a significant role in shaping Latina young people’s perspectives on mental health, as studies have found that Latinas hold negative views about mental illness and mental health treatment (Cheng et al., 2013; De Luca et al., 2015; Stafford & Draucker, 2020) and that mental health stigma uniquely predicts their help-seeking attitudes (Mendoza et al., 2015). Lack of mental health knowledge and perceived lack of support for mental health treatment also inhibit Latina young people from seeking and/or engaging in treatment (Stafford & Draucker, 2020; Stafford et al., 2019; Szlyk et al., 2019; Wang et al., 2020).
Research suggests that family and culture contribute to Latina young people’s decreased help-seeking norms (De Luca et al., 2015). Mental health seems to be taboo within Latinx families due to cultural scripts that prescribe silence around sensitive topics (Stafford et al., 2019; Szlyk et al., 2019; Wang et al., 2020) and an emphasis on family privacy in Latinx cultures (Nolle et al., 2012; Valdivieso-Mora et al., 2016). These factors likely contribute to Latina young people’s tendency to conceal symptoms of mental distress, rather than seek mental health treatment (Stafford et al., 2019; Szlyk et al., 2019). Despite the recognition that socialization processes are influential in shaping young people’s attitudes, beliefs, and behaviors, this is the first study to explore how family socialization processes contributed to Latina young people’s views and experiences related to mental health and help-seeking.
Health Socialization Theory
Socialization theory seeks to explain the processes by which attitudes, values, and norms related to particular spheres of behavior are transmitted between generations. While there are multiple agents of socialization throughout the life course, research examining the socialization of children and adolescents tends to focus on the influential role of the family context as the primary agent of socialization during the early stages of life. Researchers have applied socialization theory to various behavioral realms to understand how young people develop attitudes and behaviors related to sex/sexuality (Warner et al., 2020), political beliefs and ideologies (Bañales et al., 2021), racial/ethnic identity (Ayón et al., 2020), and health behaviors and identity (Stanley & Stanley, 2017). This body of scholarship has shown that through their everyday interactions and communication with young people, families transmit what they understand to be culturally appropriate norms, attitudes, and behaviors within various behavioral realms, thereby shaping young people’s understanding of these topics through the socialization process.
This study builds upon the theoretical concept of health socialization to explore how Latina young people developed their perspectives on, attitudes toward, and behaviors related to mental health. Health socialization helps explain how children acquire health-related attitudes and behaviors, recognizing the particularly influential role of family relationships in this process (Tinsley, 1992). From a health socialization perspective, health-related attitudes like beliefs about control over health and perceived vulnerability to illness, and health-related behaviors such as seeking health care and participating in health-promoting or health-damaging activities, are shaped by the familial and sociocultural environment in which children are embedded (Kendall & Li, 2005; Singh-Manoux & Marmot, 2005; Tinsley, 1992). A substantial amount of scholarship has demonstrated that families are a significant agent of health socialization, impacting children’s health-related attitudes and behaviors into adulthood (Grey et al., 2022; Lees & Tinsley, 1998; Tinsley, 1992). Among Latinx families specifically, numerous studies have explored how the family socializes young people with regard to sexual, reproductive, and menstrual health (Aragón & Cooke-Jackson, 2021; Aragón et al., 2023; Schiffner et al., 2017). However, researchers have only recently begun to explore family communication about mental health and its impacts on young people (Dorri et al., 2023; Flood-Grady & Kellas, 2018; Yasui et al., 2023) and no studies have examined socialization processes related to mental health within Latinx families. To fill this gap, this study explored how Latina young people developed their mental health-related beliefs, attitudes, and behaviors with a focus on the family context.
Method
Research Purpose and Design
The purpose of this study was to theorize how the family system influenced the development of Latina young people’s mental health-related perspectives, attitudes, and behaviors by answering the following research questions: What messages about mental health did Latina young people receive from their families growing up? What impact did those messages have on Latina young people? How do they make sense of these messages? To answer these questions, this study analyzed a subset of data collected as part of a larger exploratory, qualitative research project called Health Opportunities for Latina Adolescents and Young Adults (HOLA), the purpose of which was to elicit and analyze the retrospective narratives of Latina young adults to gain empirical insights about their mental and sexual health experiences during adolescence. Mental and sexual health were the foci of HOLA to better understand the well-documented health disparities in these areas (Centers for Disease Control and Prevention [CDC], n.d.) from Latinas’ firsthand perspectives. Findings related to sexual health were analyzed and reported separately (Lilly, Emerick, & Pace, 2023; Lilly, Pace, & Emerick, 2023; Pace et al., 2023).
HOLA employed a narrative research design (Kim, 2016) to gather and analyze the firsthand accounts of 25 Latina young people. Narrative methodologies use stories as data “to provide explanatory knowledge of human experiences, which allows the portrayal of rich nuances of meaning in emplotted stories” (Kim, 2016, p. 13). This methodology was deemed appropriate because it focuses on people’s lived experiences and perspectives of daily life and considers “the feelings, goals, perceptions, and values of the people whom we want to understand” (Kim, 2016, p. 13). Thus, a narrative research design offered a holistic approach to exploring and contextualizing Latinas’ lived experiences of mental and sexual health in adolescence and understanding how they made meaning of those experiences.
Research Setting and Participants
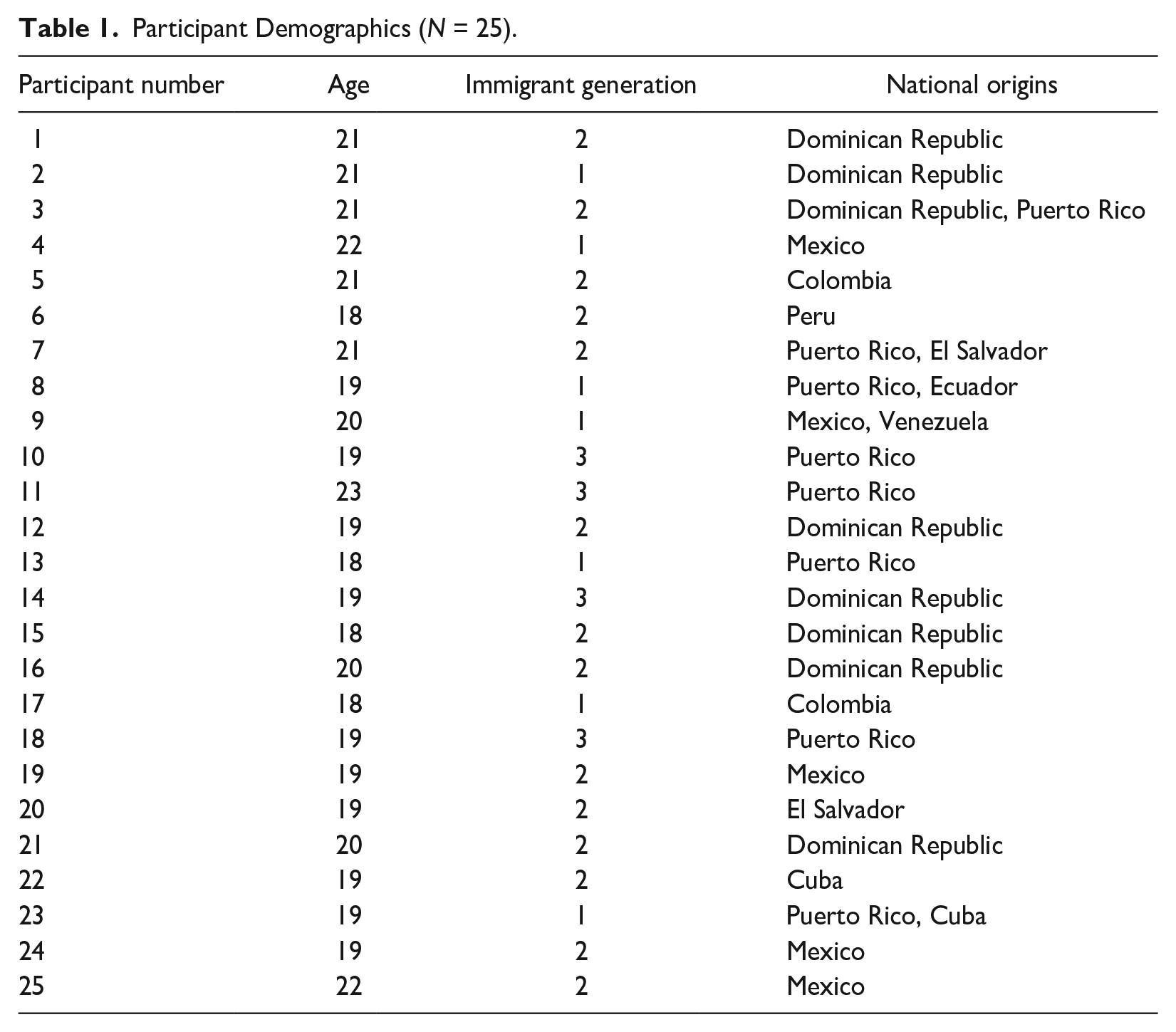
We recruited a purposive sample of 25 Latina young adults (aged 18-25) who resided in the New York City (NYC) area after obtaining university IRB approval. NYC was chosen as the research setting due to its sizable and diverse population of Latinx residents, the largest contingents of which are Puerto Rican, Dominican, and Mexican (Bergad, 2022). Potential participants were recruited using network sampling techniques by disseminating our call for participants through university- and community-based groups and organizations working with Latina young people. Research team members did not work directly with these groups or organizations but had contacts within them and/or were subscribed to their email lists or social media accounts. Potential participants were asked to complete an online screening form (see Appendix A) to assess eligibility. The screening form was completed by a total of 33 eligible potential participants, the first 30 of whom were invited to participate via their preferred contact method (text, call, or email) by the Principal Investigator (PI). Five of the 30 invitees did not respond, yielding a sample size of 25 participants that reflects the diverse national origins of Latinx peoples in NYC. Table 1 provides demographic information about the 25 participants. “Latina” identification was defined as having at least one biological parent of Latin American heritage. Three participants had one Latinx parent and one white parent, and two participants identified as Afro-Latina.
Participant Demographics (N = 25).
Data Collection
To minimize barriers to participation associated with COVID-19 and transportation, the Zoom platform was used to virtually conduct interviews. Each participant was interviewed by the PI of the HOLA project (the author), a white female university professor who is well-versed in qualitative interviewing, is fluent in Spanish, and has previous experience working with Latinx communities as a social work practitioner and researcher. Prior to beginning the Zoom interview, the PI introduced herself, explained the purpose of the research, and asked participants if they had any questions about their involvement in the study. Then, the PI obtained oral consent to participate in the study and to record the interview from each participant, using an IRB-approved consent script. Interviews were conducted in the Spring of 2022 and lasted 59 min on average. Participants received a US$50 Amazon e-gift card following the interview.
Interviews employed a life history narrative approach that afforded participants control over the telling of their stories. A flexible, semistructured interview guide (see Appendix B) was used to guide the conversation. Participants were asked to narrate their mental and sexual health experiences during middle school and high school, using interview questions designed to elicit stories, such as: How do you think your family has impacted your views on mental health? What conversations about mental health do you remember having with family members? What are some of the most memorable events related to your mental health in middle school? How did your mental health in high school differ from middle school?
Data Analysis
The PI led the research team in an iterative, collaborative approach to data analysis to strengthen the integrity of our interpretations (Church et al., 2019). The team consisted of the PI and four research assistants—three Master of Social Work (MSW) students (two of whom are Latina) and one social work doctoral student. All research assistants had previously completed coursework in qualitative research and were trained by the PI in the specific methodologies and methods used for the HOLA project. We used NVivo software to process and organize data throughout the analysis process. Interview audio files were transcribed using NVivo automated transcription software. Then the research team listened to each audio file while checking the interview transcripts for accuracy, immersing ourselves in the data through this process.
We used both holistic-content and categorical-content approaches to narrative analysis, allowing global impressions and themes to emerge inductively from the data (Lieblich et al., 1998). Holistic-content analysis considers each participant’s entire narrative with a focus on its content, while categorical-content analysis identifies categories or themes in excerpts of the text within and across narratives (Lieblich et al., 1998). We employed these approaches to narrative content analysis sequentially. First, our holistic-content analysis proceeded through the following steps as delineated by Lieblich et al. (1998): (a) we read each interview transcript multiple times to allow a pattern to emerge; (b) we recorded our global impressions of each participant’s individual narrative; (c) we determined themes to follow within each narrative; (d) we read the narrative separately and repeatedly for each theme and marked them in the text; and (e) we noted our conclusions and discussed each case as a group. Then, the PI and one MSW research assistant engaged in categorical-content analysis (i.e., content analysis). First, all content related to mental health was selected from the transcripts, yielding a total of 888 unique references. Then, the PI read through the selected subtext to define major content categories and subcategories through an open reading of the text that allowed empirical categories to emerge inductively, as described by Lieblich et al. (1998): “in practice, it is a circular procedure that involves careful reading, suggesting categories, sorting the subtext into categories, generating ideas for additional categories or the refinement of existing ones, and so on” (p. 113). Major content categories represented cross-cutting themes identified within all 25 participants’ narratives and included as many subcategories as needed to represent the content universe. Examples of major content categories and subcategories include family factors that impacted mental health (subcategories: family attitudes toward mental health, adverse events in the family system, family dynamics, family roles, and family values) and mental health management (subcategories: coping mechanisms, exercise, help-seeking, medication, self-expression, and self-care practices). Next, the PI and research assistant sorted the material into the content categories independently, which allowed us to calculate interrater reliability to ensure a high level of agreement (Kappa’s coefficient 0.88). Finally, we met several times to discuss our conclusions and refine our interpretations (Lieblich et al., 1998). These meetings allowed us to identify the categories that appeared most frequently, write analytic memos that provided a complete description of the content universe within each category, and discuss and determine relationships between categories. This informed the author’s process of formulating and writing the findings.
Evaluative Criteria
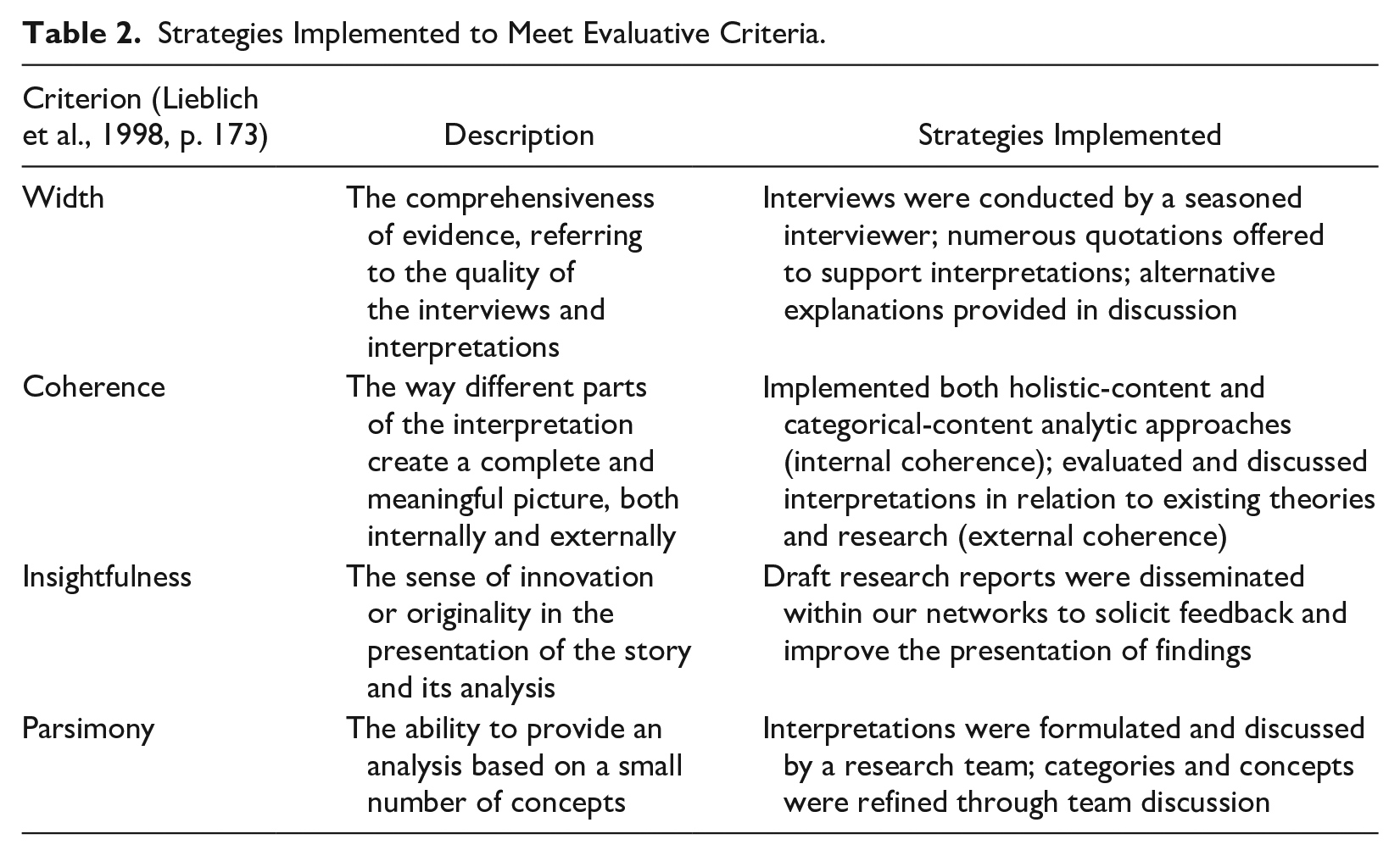
In alignment with the interpretive epistemological standpoint of narrative methodologies, which “asserts that narrative materials—like reality itself—can be read, understood, and analyzed in extremely diverse ways” (Lieblich et al., 1998, p. 171), this study attended to the criteria for evaluation of narrative research outlined by Lieblich et al. (1998), as described in Table 2. We also implemented several strategies aimed at “sharing one’s views and conclusions and making sense in the eyes of a community of researchers and interested, informed individuals” (Lieblich et al., 1998, p. 173), which is highly valued in narrative research. These strategies included writing reflexive memos throughout the data collection and analysis process to make team members’ own views and conclusions clear; sharing our findings with research participants and soliciting their feedback (i.e., member-checking); and presenting our findings to other researchers to engage their questions and understandings.
Strategies Implemented to Meet Evaluative Criteria.
Findings
A rigorous, inductive analysis of participants’ narratives revealed that Latina young people described three significant stages in the development of their mental health-related beliefs, attitudes, and behaviors which were labeled: undergoing a process of family mental health socialization, suffering in silence, and attaining a new perspective. During the first stage, undergoing a process of family mental health socialization, Latina young people learned and internalized their family members’ predominantly negative views about and attitudes toward mental health and help-seeking. The next phase, suffering in silence, was characterized by Latina young people suppressing and/or concealing their mental distress and help-seeking experiences. During the final phase, attaining a new perspective, participants were able to make sense of the messages about mental health they received in their families growing up and formulate their own viewpoints. These phases are presented sequentially with representative quotes from participants to illustrate identified themes within each phase. Within each of these phases, participants shared stories that attest to their agency and resilience, which are summarized at the end of each phase. These stories not only highlight the strengths of Latina young people in the face of challenges but also provide a nuanced and holistic view of the diversity and complexity of their stories.
Undergoing a Process of Family Mental Health Socialization
In their narratives, Latina young people described how ideas about mental health were transmitted to them through their interactions with and observations of their family members. Participants’ stories conveyed that growing up in a family environment characterized by predominantly negative views of mental health and help-seeking influenced the development of their initial perspectives on mental health. We categorized the messages about mental health Latina young people received from their family members as serving three overarching functions: stigmatizing, minimizing, and silencing.
Stigmatizing Messages
Messages that perpetuated mental health stigma were the most frequently described by participants. 72% of participants (18/25) reported receiving stigmatizing messages about mental health within their families growing up. One of the most common stigmatizing messages was that therapy is only an acceptable option for very extreme cases of mental illness, and those who needed mental health services were considered “crazy.” Participant 3 described how this attitude was conveyed in her family, stating: I just feel like in general, mental health and getting help and things like that is generally frowned upon, especially in the Latino culture. I definitely had a lot of negative reactions from my family. Like even my dad, when he found out that I wanted to go to therapy . . . I know he means well, he loves me, but he’s like, “Oh, that’s for weak-minded people. I didn’t know you were a weak-minded person.”
A common message received was that therapy was only needed for severe mental illness, and those who sought such services were perceived in a negative light. Participant 1 recalled: My aunt had an accident and she lost her leg. And when that happened, she voiced out, “I really need to go to therapy. I really want to see hope for myself.” Because it was a traumatic event and no one told her to go seek help. Everyone was just like, they didn’t tell her anything . . . So if I do it, “Oh, is there something wrong with me?” That’s what my family has made her think. Like if you seek therapy, something is wrong, mentally wrong with you. You have to be, I don’t know, harmful, you have to do something terrible, you have to be a threat to seek therapy. Like if you’re a psychotic. It has to be extreme in order for them to think that it’s okay to seek therapy.
Several participants also reported receiving the message that mental health concerns should only be discussed within the family. Participant 7 received this message in adolescence: When I was younger, I would have kind of mini panic attacks in terms of school, especially in the beginning of the school year when things were new. I was definitely not a big person on acclimating to new things. And I remember having my mom come and talk to me. But it wasn’t a full-on, like “Oh, let’s reach out and get help for you.” It was more like, “I’ll take care of it within the home behind doors.”
Another stigmatizing message received suggested that if a person’s needs are met, they should not suffer from mental health concerns or require mental health services. Participant 4 shared a story of a time she received this message from her father: A couple months ago, I had a blow out fight with my dad, and I said to him, “This conversation is going to send me back to therapy!” Because I started going on my own through [university]. And then my dad was like, so upset. And he was like, “What have I ever done in my life? We’ve given you a good life. Why would you need therapy?”
Minimizing Messages
Messages that served to minimize mental health concerns were also prevalent in participants’ narratives. In all, 68% of participants (17/25) described receiving mental health messages that were categorized as serving a minimizing function. One of the minimizing messages commonly received was that people often exaggerate mental health issues and participants just needed to be tough enough to overcome any difficulties. Participant 3 recalled receiving this message from her maternal aunts: My mom’s side of the family, they grew up with this strict structure. And to them, that’s [mental health concerns] just something that’s like, you know, you got to brush it off, you know? Like, “Oh, people go through things, you’re going to experience stress. It’s life.” My aunts on my mom’s side would always say, “Oh, life is hard. That’s life. It’s hard, it’s not easy. You’re going to go through things.” . . . And they’re just like, “You have to have thick skin like me.”
Participants’ narratives also revealed the message that young people today have it easier than their parents, thus their mental health issues are not worthy of concern compared to the struggles of previous generations. As Participant 22 described: Your emotions and your sadness don’t really matter because you’re in this country, right? Your parents, it’s always the notion in your head of your parents came from so much worse and so much harder, where it’s like me sitting here being like, “Oh, I feel kind of depressed today” versus like, I don’t know, my grandfather struggling to immigrate here, my father struggling to immigrate here. It’s like a different sense of relativity of it all. My emotions aren’t really that valid. And I think my parents intentionally want to perpetrate, put that emotion onto me.
A third minimizing message that was found in participants’ narratives was the idea that mental health concerns could be alleviated through faith and religious practices, which were considered the best means of coping. Participant 13 described receiving this message from her mom: I feel like my whole life, every time I’ve told my mom, “I have really bad anxiety,” it’s like, “Just trust God and breathe and it’ll all be okay.” Like no, that does not work. But definitely growing up in the Latino community, they don’t believe in mental health. It’s kind of just like, trust God.
Participant 13’s mom might have felt she was providing emotional support by encouraging her daughter to trust God, but Participant 13 did not feel that her anxiety was taken seriously.
Silencing Messages
Silencing messages, which functioned to shut down conversation or encourage silence about mental health concerns, were identified in 56% of participants’ narratives (14/25). The most frequently described silencing message was that mental health and mental illness are foreign constructs or uniquely American phenomena that Latinx people do not acknowledge. When asked about her family’s attitudes toward mental health, Participant 6 recounted: It wasn’t a thing. It wasn’t a thing you discussed. Like, anxiety, depression, those were just terms of this American—something that’s American. That’s not something that happens to us. Like, yeah, we have anxiety, yeah, we have depression, but, it’s not, like an actual mental disorder. It was just something that, yeah, you can experience, but not in the long run. That’s not a thing. That doesn’t happen to us. That’s the kind of mentality they had. And so that’s why I kind of felt like I couldn’t talk about it to anyone, either.
Similarly, Participant 8 explained how the very idea of being “mentally unhealthy” was inconceivable in her family, stating: I didn’t know anything about it [mental health] because it’s kind of like, how can you be mentally unhealthy? You know, that’s more like, matters of health are supposed to be physical, not mental. You’re supposed to be all right upstairs.
Another message that served a silencing function conveyed that mental health communication was unwelcome, as Participant 2 explained: You feel like you bringing up your problems is just, like, the other people are just going to be like, “Oh.” We just disregard it. That’s like one of the major issues I’d say. We just push it to the side.
The general disregard for mental health within the family made it difficult for participants to talk about it with family members, as Participant 1 recalled: I’ve tried going to my parents and telling them [about my mental health problems] and it’s just like, they’re like, “I don’t want to hear about this.” Like, “Why are you telling me?” Like, it’s just completely either blocked or just ignored, like put to the side. Like, they don’t want to hear the conversation.
Highlighting Strengths
Although participants’ stories highlighted the central role of the family as a source of mental health socialization, Latina young people were also influenced by and proactively sought out other sources of information about mental health. Participants described learning more about mental health by turning to social media, engaging in conversations with peers, and accessing school resources. Participant 23 shared that she turned to social media to learn about mental health: “I watched a lot of YouTubers, I would say, growing up, and most of them openly spoke out about mental health. So, it was pretty positive . . . it would be speaking out about it or offering advice.” Participant 16 shared that she talked about mental health with a friend: My best friend at that point also had a lot of anxiety I would say, like worse than me. But we talked about it a lot. And I guess that kind of helped me, probably because she was kind of my support system, like we were together all the time. And I guess having someone there, like I could talk to her about it, like if I was feeling stressed or anything, and she would always sympathize with me.
A few participants were interested in engaging in mental health services as early as middle school and requested their parent’s permission to do so; however, parents were rarely supportive of this idea. When parents denied their daughters the opportunity to seek help, it sent them a clear message about the family’s negative attitudes toward help-seeking. However, two participants shared that their mothers facilitated their engagement in mental health treatment at an early age and reported gaining a lot of insight and coping skills from the experience, while still understanding that therapy might be frowned upon by other family members.
Suffering in Silence
As a result of the messages about mental health transmitted by their families, almost all participants (23/25) shared that they learned to suppress their emotions and/or conceal mental distress and related help-seeking.
Suppressing
Most participants (21/25) described how they suppressed or “bottled up” difficult emotions so that they could keep going in life. Choosing to focus on educational pursuits rather than attending to mental health concerns was frequently discussed. As Participant 2 shared: So, when I was in middle school, I was kind of having the same perspective [as my family]. I was just like, “Yeah, I just need to push it away. I just need to push through it, bottle up my little emotions.” And stuff like that. Like, “Those don’t matter right now. Let me just focus on getting that education so that we can, you know, prosper.” That was the whole mentality that was ingrained in my brain. And that’s what I went through the entire time to the detriment of my whole mental health.
Participant 22 explained that she also focused on school while neglecting her mental health, so much so that she deceived herself, stating: I do have a very “get through it” attitude in the sense that even in the worst weeks of my life, I always get my stuff done. My assignments are always turned in. My work is always finished. My reports are sent. Like I definitely have internalized that I will keep on going no matter what happens. But I think I learned to bottle up my feelings from a young age and deeply invalidate the way that I feel all the time, like almost gaslight myself into being like, “Oh, it’s so great. This is fine.” And that has not benefited me at all now.
Concealing
Many participants (17/25) hid their mental health concerns and help-seeking efforts from their parents and other family members. One reason participants concealed their mental health problems was because they did not want to burden their family members, especially when the family system was already experiencing other stressors. Participant 7 shared: Sophomore year, I knew that my family was going through a lot of stressors themselves in terms of having my mother go through this stroke where she was handicapped. I knew that I didn’t want to add on stressors to my father or to my mother, or any family member. Because I knew that what my mother had gone through was a big issue, especially because she was a primary person, like the go-to person in my family. And so, to have her go through that, a lot of people were dealing with stressors, and I remember not wanting to add on to that, so I usually kept things to myself.
Describing a similar situation, Participant 9 shared that she felt unable to confide in her parents after her mother was diagnosed with breast cancer: I didn’t want to talk to my parents about, like, my emotions at all because I was like, “They have so much going on on their plate right now. Like, I don’t need to add to this.” So yeah, we just didn’t really talk about how we were feeling during that time, but I was definitely really struggling.
Participants also chose not to disclose their mental health experiences out of fear of being misunderstood by their parents or other family members. Participant 3 expressed fear of misunderstanding if she talked about her mental health within her family: I would never really speak up—I was scared to because, you know, I can’t really tell you why. I was just scared to say how I was feeling. I guess because I’m the child under the adult . . . So, yeah, I was just more like, I can’t really say anything because if I say something, I’m talking back or I’m being disrespectful or like, if I say something, they’re not going to understand and we’re going to get in a disagreement and it’s not going to go the way that I want it to. So, I would just stay quiet about it.
After trying to talk with her parents about her depression initially, Participant 21 avoids those conversations now because she has reason to believe they won’t understand: I hesitate to tell them [parents] things now regarding my mental health. I hesitate to tell them how I’m feeling . . . Every time I try to talk to them about mental health or what I’m going through, it is scary because from the first reactions, it just kind of stuck with me. So, I’m just like, “Nope, nope, they’re not going to believe you. They’re not going to really care. Or they’ll just, like, question you.” So, I’d rather stay away from that.
Participants also described concealing their efforts to engage in mental health services from their family members. Participant 7 recalled: “I always understood that there is this need to talk about mental health. I would seek out services in school and I really wouldn’t tell my parents about it.” Participant 8 also sought the support of her guidance counselor in school, which allowed her the opportunity to talk about her mental health without her parents’ knowledge: I was a depressed little shit, let me tell you. I was going through it for some reason, and I was talking to my friends, talking to my guidance counselor at my high school . . . because I was so afraid to tell my parents.
Having access to confidential services was important to many participants, who were fearful of their parents finding out they were seeking or receiving mental health care. Participant 6 also sought support in secret due to this fear: I put in a request for [university counseling services] for a couple of sessions . . . But it’s like, I don’t know how my parents would react, so I—that’s why I kind of wanted to do it at [college], so it could kind of be a little hush-hush type of situation. But then I got scared. And then it was like, what if it gets out?
As these excerpts illustrate, participants often suffered in silence when dealing with mental distress because they believed that suppressing and/or concealing their experiences was an appropriate way to manage them.
Highlighting Strengths
While suffering in silence, participants displayed several notable strengths that helped them get through difficult times. First, participants frequently described using positive distractions to cope with mental distress. Rather than acting out or engaging in vices as a means of escape, Latina young people tended to focus their energies on learning and performing well in school. Second, participants showed concern for other family members when describing why they felt they had to conceal their mental health experiences. Although concealing behaviors may have been detrimental to participants’ mental health, they were willing to sacrifice their own needs to prioritize the well-being of both individual family members and the family unit. Third, participants exercised agency in choosing not to disclose their mental health struggles and related help-seeking to family members. This choice helped protect participants from negative reactions and misunderstandings while their mental health was in a vulnerable state. Fourth, many participants did seek help when they felt they could no longer manage symptoms on their own. Help-seeking was particularly courageous for those who felt the need to conceal it from their families because they knew it would not be received well. In addition, some participants shared that they engaged in journaling and artmaking, which provided a vehicle for venting and processing emotions. When asked what helped her manage mental distress, Participant 14 shared: “I used to draw. When I had my first depressive episode, I drew.” Participant 23 described how journaling provided an outlet for her: When I started getting into journaling and actually writing down any thoughts that I had that were like bothering me and not allowing me to sleep, then I realized like, wait, that’s so good to just be able to get rid of all of this and not have to talk about it.
Participants also shared stories of navigating toward trusted, supportive peers to discuss mental health concerns. As Participant 6 expressed: “I said to myself, ‘Okay, I’m going to talk to this person today.’ . . . Because talking with people really, really helps me relieve stress.”
Attaining a New Perspective
Participants’ narratives also described a third phase in the development of their mental health-related beliefs, attitudes, and behaviors—attaining a new perspective. During this phase, participants made sense of the messages about mental health they received from their families growing up and formulated their own understandings of mental health and help-seeking. Latina young people frequently described a desire to break the intergenerational patterns that stigmatize, minimize, and silence mental health within Latinx family systems.
Participants’ narratives displayed two ways of understanding their family’s views toward mental health and help-seeking: generational differences and projecting an image of family strength. Many participants (14/25) shared the viewpoint that the stigmatizing, minimizing, and/or silencing messages about mental health they heard in their families growing up could be attributed to the conceptualizations of and attitudes toward mental health and help-seeking in Latin American countries of origin that had been passed down through the generations. Participant 12 shared: I see that my older family members, they say that it [mental health] is stigmatized. They say, “Oh, you’re alive and you have a roof over your head, why are you worried? Why do you have mental health issues?” It’s not something they really talk about. They try to avoid it . . . In all honesty, I think they’re very instilled in their old ways—what their parents taught them, what their grandparents taught them—and it’s just an old way of thinking from where we come from. And they’re very embarrassed. It’s always a matter of being embarrassed and proving to yourself and others that nothing is wrong.
Similarly, Participant 1 explained how older generations learned not to talk about mental health: In the Caribbean, no one is talking about mental health, it’s not a thing. It doesn’t exist. But here, because it exists and you’re trying to talk to your parents more about it, it’s like they just don’t get it because it hasn’t been in their culture. So, you can’t even expect them to understand when they’ve spent all these years knowing that it’s not a thing.
Thus, negative attitudes toward and messages about mental health were perceived as stemming from older generations’ experiences growing up in Latin America.
Participants also came to understand that their family’s negative attitudes toward mental health and help-seeking were rooted in a need to project an image of family strength and well-being. Acknowledging or seeking help for mental health struggles might make the family seem vulnerable or weak and/or invite scrutiny or judgment from outsiders. Participant 6 shared: They never, never allow themselves to be vulnerable . . . Everything needs to be kept in, nothing can get out. Like, they just don’t want to seem vulnerable at all. So, something like [depression], you can’t say outside.
Participant 7 explained that it was important to preserve an image of family strength: Within the Hispanic culture, it’s keeping things within the family in order to have this persona that we’re fine and that our family is fine. So, I think just trying to be strong and trying to have that persona, it’s where we don’t really talk about mental health.
Participant 22 emphasized how shame and stigma caused family members to keep mental health matters private so as not to seem weak: I think that there’s a lot of shame for anybody who’s struggling . . . And it’s like a very public community in the sense that everybody is kind of up in each other’s business. And so, I think if you were to be publicly struggling or tell your friends that you were struggling, it’s like, “Oh my God,” like other families in the neighborhood are going to call and know that you’re struggling. I think it’s like a social fear of stigma or being seen as weak or not being able to provide for your family.
As these examples illustrate, participants understood that family members felt it was important to appear strong and healthy, which contributed to their tendency to stigmatize, minimize, or silence mental health issues.
Participants also shared stories of how they formulated their own ideas about mental health, often intentionally moving away from the attitudes and beliefs they learned from their families. Participants mentioned several influences outside the family that helped them attain a new perspective. Participant 22 shared how her exposure to social media and another family’s dynamics helped change her ideas about mental health and help-seeking: I would say the media had a decent amount of influence, social media especially . . . for me personally, it was really helpful in helping me figure things out . . . And then also, I think seeing my parents struggle and not really doing anything about it . . . So I think their not handling their trauma and handling their issues deeply impacted the reasons why they’re not really together anymore. And so, I think that was kind of jolting in a sense. I was like, “Well, I’m seeing all of these things that they do and the way that they make me feel, and I’m seeing the things that I’m starting to do the same and it’s making me not feel great.” It’s like, why would I keep kind of contributing to these like patterns? . . .And then I went to Macedonia [for study abroad]. . .I lived with a host family there and I observed the dynamics of their family and I was like, “What? Wait a damn minute. Like, everything that I grew up with was so not normal” . . . And so I think that was kind of like the light bulb that went off in my head was like observing other people’s dynamics with their families living in another person’s family . . . I think the fact that I started to realize, I was like, “Damn, I’m really going to end up like my parents if I don’t go to therapy.”
For Participant 9, working with a therapist helped her re-examine her beliefs, as stated: I think now looking back, it was very cathartic to talk about it and have someone validate like, “Oh, that was something tough,” when I had been minimizing it. I’d be like, “Oh, it was tough, but it was fine, whatever.” But she [therapist] really pushed me to be like, “No, it was really difficult, but I’ve grown from that, and I’ll get through whatever next challenge comes up.” So, I did appreciate it.
Participant 10 also articulated that her views about mental health are now different from what she learned from her family, thanks to a process of self-reflection. She explained: I think it [mental health] is not the lack of being sad or anything like that. I feel like it’s more the ability to work through your emotions. It’s not the absolute absence of any negative emotion. It’s when you encounter something that’s negative, you can work through it and you’re not just taken down and inundated with these feelings. You know how to positively cope with them and deal with them and work through them so that you can get back to the positive emotions. But I also think there’s a certain level of self-reflection and stuff like that that does go into a positive mental state . . . With mental health, there’s a certain level of, like, the person who’s having poor mental health or needs to improve their mental health, they have to actualize it. Like, you can lead a horse to water, but you can’t make it drink. But back then, I wasn’t even before the water. Like, as the horse, I was just in a pasture, just chilling, eating grass. Like there was no river, there was no lake. Like, I did not know there was water to be drinking. I didn’t even realize I was very thirsty if that makes sense.
Not only did participants tell stories of how they were able to attain a new perspective, but some participants also shared that their experiences in their families growing up motivated them to work to change mental health attitudes within their families and the broader Latinx community. Participant 2 shared how she was actively engaging her family members in conversations about mental health: In families, we just don’t talk about mental health, or at least that was my experience growing up. But in recent years, though, it has been becoming a little bit more accepted, I’d say. Like I’ve really tried to communicate with my family like, “All your emotions are important too,” like, “We should discuss them as a family and that will get us closer” and stuff like that, through that aspect. Kind of like for us to start having conversations about mental health.
Participant 3 also shared a story of helping to change her mom’s attitudes toward mental health by involving her in a therapy session. She stated: It was hard for my mom to kind of grasp the fact that I needed therapy and was feeling these things because her growing up, she grew up with a strict father. Her father was a politician, my grandfather was a politician. So, in DR, your status and the way you come out to the world is a number one priority. So, I think those conversations around mental health weren’t normalized in my mom’s upbringing, so to her, it was just like a whole new world, you know? She was confused, she couldn’t understand it. But I feel like now she’s gone to therapy with me. She did go to therapy and she spoke to the therapist with me and now, I feel like she understands and she can be of help, you know?
Participant 7’s mental health struggles inspired her to pursue a psychology degree so she can help others in similar situations: My goal is to become a guidance counselor because I understood the importance of having someone talk to you, in terms of, if a student is facing any difficulties, just having that person that’s going to sit down and really talk through it without deflecting your feelings and pushing them aside. So that’s how I got into psychology.
Similarly, Participant 1 shared a desire to encourage help-seeking within Latinx cultures, stating: In all those countries [in Latin America], there’s this same belief that mental health is such a bad thing, and we shouldn’t be trying to do anything about it . . . That’s why personally, I want to become a psychologist or do something in counseling. I want to change that stereotype that it’s like, “Oh, it’s bad.”
Participants’ narratives demonstrated that they made sense of the predominantly negative messages about mental health they received within their families growing up, drew upon internal resources and other sources to formulate new perspectives, and in some cases, are actively striving to promote mental health and related help-seeking in their families and communities.
Highlighting Strengths
Participants’ agency and resilience were readily apparent in their stories of “attaining a new perspective.” During this phase, participants realized their own power to interpret and make meaning of the messages about mental health they had received within their families, displaying critical awareness of the social forces that influenced their family members’ beliefs and attitudes. Participants also engaged in self-reflective practices that helped them gain new understandings of mental health and help-seeking, choosing to formulate their own views rather than accept those they had been socialized to adopt. Having critically reflected on and learned from their family’s attitudes toward mental health, participants actively sought to promote positive changes within themselves, their families, and their communities.
Discussion
The Latina participants of this study provided detailed, insightful narratives of their mental health experiences during adolescence and young adulthood, offering empirical insight into the messages about mental health they received within their families growing up, the impacts of those messages on their mental health-related behaviors, and how they made sense of and advanced beyond those messages. A rigorous, inductive analytic process revealed that Latina young people received several stigmatizing, minimizing, and silencing messages about mental health within their families, which led them to suppress or conceal their mental distress and related help-seeking experiences. Latina young people made sense of these messages by acknowledging generational differences in understandings of mental health and the family’s desire to project an image of strength and well-being and engaged in reflective practices to formulate their own perspectives on mental health and help-seeking.
These findings suggest that participants’ mental health experiences and perspectives were shaped by a process of family mental health socialization—a new theoretical construct that explains the process through which young people learn and internalize the mental health-related beliefs, behaviors, norms, and expectations of the cultural and family context in which they grow up. In their narratives, Latina young people described “undergoing a process of family mental health socialization”—the first phase in the development of their mental health-related beliefs and attitudes. During this phase, participants recounted that they learned that family members held stigmatizing attitudes toward mental health and related help-seeking, tended to minimize their own and others’ mental health struggles, and/or prescribed silence around mental health issues. Participants conveyed that growing up in a family environment characterized by predominantly negative views of mental health and help-seeking influenced the development of their own perspectives on mental health.
Participants’ stories showed how these ideas about mental health were transmitted to participants through their interactions with and observations of their family members. Although parents were most frequently described as influential agents of mental health socialization, participants also shared stories of how aunts, uncles, cousins, and grandparents were influential in the family mental health socialization process. While research with other groups has examined “parental mental health socialization” (Yasui et al., 2023), the findings of this study indicate that parents and other members of the family system were influential in shaping Latina young people’s views about mental health. This suggests that for Latinx families, it is important to examine mental health socialization processes at the family level. Participants’ narratives demonstrated that various members of the family system acted as agents of mental health socialization, leading Latina young people to internalize their family’s beliefs about and attitudes toward mental health.
The family messages about mental health described by Latina participants are similar to those Chinese American young people described receiving in their families (Yasui et al., 2023), suggesting that they may be tied to the immigrant experience, likely due to differences in cultural beliefs about mental health in the United States as compared with immigrants’ native countries (Mascayano et al., 2016). Previous research has found that length of time in the United States is positively associated with Latinx parents’ communication with service providers about their child’s mental health, suggesting that greater acculturation to U.S. culture increases Latinx parents’ willingness to discuss mental health (Cook et al., 2014). However, acculturation is also a source of stress and a predictor of mental illness in Latinx adults and adolescents (Alegria et al., 2007; Cervantes et al., 2011). It is also important to consider Latinx people’s perceptions of and experiences with the clinically oriented U.S. mental health care system to understand their attitudes toward mental health and related help-seeking. Despite recent progress, clinical mental health services are limited in Latin America (Caldas de Almeida, 2013) and more informal approaches to mental health management, such as talking to family members, religious leaders, or God (through prayer), are often preferred in Latinx communities (Moreno & Cardemil, 2013). Previous research has found that Latinx people in the United States face barriers to accessing mental health care, such as language, immigration status, and mental health literacy (Bledsoe, 2008). When they are able to access these services, Latinx people often report negative experiences that lead them to disengage from treatment (Montalvo, 2009; Stafford & Draucker, 2020). Thus, systemic factors associated with the marginalization of Latinx people’s ethno-racial and immigrant identities likely influenced the attitudes toward and beliefs about mental health and related help-seeking that family members transmitted to the Latina young people involved in this study.
As a result of the family mental health socialization process, Latina young people behaved in ways that conformed with family norms by suppressing and/or concealing negative emotions and other mental health symptoms. During this phase of “suffering in silence,” participants described suppressing emotions by bottling them up and focusing on academics instead. Rather than seek support within their families, participants chose to conceal their mental health struggles because they didn’t want to contribute to family stress. Fear that family members wouldn’t be supportive or understanding also inhibited participants from disclosing their mental health issues and related help-seeking. These findings are supported by previous research on the mental health and help-seeking behaviors of Latina young people. For example, research with Latina young people with depressive symptoms found that they initially hid their depression from family members, peers, and mainstream authorities (Stafford et al., 2019) and research with Latina young people who had a history of suicidal behavior found that familial codes of secrets and silence contributed to their suicide attempts (Szlyk et al., 2019).
Analysis of participants’ narratives also revealed the many strengths that they possess and demonstrated throughout the three stages. Latina young people exercised agency in actively seeking mental health information and treatment, used positive distractions, found outlets for creative expression to cope with their emotions, and formulated their own perspectives on mental health. These notable strengths demonstrate that family mental health socialization is not a passive process—rather, Latina young people were actively engaged in interpreting the messages about mental health they received in their families growing up and making agentic choices to navigate toward needed sources of support.
A critical analysis of participants’ narratives also suggests that there were not just familial forces at play in Latina young people’s mental health socialization—sociocultural forces are also influential in shaping the perspectives, attitudes, and behaviors of Latina young people and their family members. Latinx cultures and family environments tend to be highly patriarchal, prescribing masculine ideals that prohibit vulnerability for men and feminine ideals that encourage self-silencing and selflessness for women (Nuñez et al., 2016). As an ethnic minority group in the United States, Latinx peoples are also subject to other forms of oppression including racism and nativism, which perpetuate harmful stereotypes that criminalize and/or blame immigrants for social problems (Kilty & Haymes, 2000). Within this context, the adverse attitudes toward help-seeking behaviors exhibited in Latinx families and the tendency for Latina young people to suffer in silence may be considered adaptive (Ronningstam, 2006), serving a protective function for Latinx families who cannot risk being rendered more vulnerable than these intersecting systems of oppression already make them. By avoiding the topic of mental health, discouraging help-seeking, and modeling silencing behaviors, Latinx families may be jeopardizing their mental well-being for the sake of safety, security, and well-being in other aspects. However, the participants of this study demonstrated that it is possible to recognize and resist the impacts of these oppressive systems while working to transform the prevailing negative beliefs about mental health in the Latinx community so that mental health is prioritized as vital to working through life’s challenges.
This research centered the perspectives of Latina young people to deepen understanding of mental health experiences during adolescence through their richly detailed, firsthand accounts. However, the findings of this qualitative, exploratory research should not be generalized beyond the participants involved in this study. Although narratives were analyzed using both holistic and categorical content approaches, the presentation of results offers only a fragmented representation of participants’ stories that fail to preserve the context needed to understand how the identified stages play out and vary within each participant’s unique narrative. Furthermore, the findings present only the participants’ views on mental health attitudes and norms within their family systems. Future research that captures the perspectives of parents and other family members and/or observational research is needed to triangulate these findings. We specifically focused on Latina young people to gain insights from their past experiences with mental health and related help-seeking. This retrospective approach has the advantage of allowing participants to reflect on and derive meaning from their experiences over time. However, this approach relies on participants’ memory recall, which is fallible. In addition, participants’ narratives might be influenced by social desirability bias. Interviews were conducted by a non-Latina researcher, which may have affected participants’ responses.
Implications
These findings have the potential to inform future research, enhance theoretical frameworks, and guide more culturally sensitive and effective approaches to improving the mental well-being of Latina young people and their families. This research expands upon the theory of health socialization by introducing the concept of family mental health socialization, underscoring the need to incorporate family dynamics and cultural influences into theories of mental health development, especially for ethnic minority groups. By highlighting the strengths of Latina young people, this study emphasizes that individuals actively interpret and respond to family messages about mental health. Future research should explore the applicability of family mental health socialization to other cultural groups and the nuances within them while accounting for individuals’ ability to make choices and formulate their own viewpoints. Future research is also needed to delve deeper into how familial, cultural, and sociocultural forces (including intersecting systems of oppression) impact mental health attitudes and behaviors in Latinx communities and other marginalized groups.
Gaining a better understanding of family mental health socialization processes offers new knowledge about the various contextual factors that influence young people’s attitudes, beliefs, and decisions about mental health and help-seeking, information that can be useful in promoting behavior change to reduce mental health disparities within this population. As the findings highlight the role of various family members as agents of mental health socialization, social service practitioners should consider involving multiple family members in interventions, recognizing that change within the family system is vital for improving mental health outcomes among Latina young people. Building on Latina young people’s strengths, practitioners can also work to empower this population to seek mental health information and treatment and encourage open dialogue within Latinx families about mental health. The three-stage model of undergoing a process of family mental health socialization, suffering in silence, and attaining a new perspective may be clinically useful in providing mental health services to Latina young people experiencing mental distress. Intersectional frameworks are also needed to contextualize Latina young people’s unique challenges and address not only their mental health but also other social determinants of health, such as racism and nativism, in a holistic manner. Finally, community engagement and education efforts focused on reducing stigma and encouraging mental health dialogue are needed to transform negative beliefs about mental health within the Latinx community—as several of the Latina young people involved in this study are already doing.
Conclusion
In conclusion, this study offers a profound understanding of the mental health experiences of Latina young people, unveiling the intricate web of influences that shape their beliefs, behaviors, and attitudes toward mental health. Through their detailed narratives, participants illuminated the profound impact of family mental health socialization—a novel theoretical construct—on their mental health beliefs, behaviors, and attitudes. Importantly, this research underscores the resilience and agency of Latina young people; their journeys through family mental health socialization illuminate the capacity for individuals to challenge and reshape deeply ingrained beliefs. The findings of this study emphasize the need for intersectional, culturally competent mental health services, family-centered interventions, and empowerment strategies that honor the strengths and agency of Latina young people.
Footnotes
Appendix A
Appendix B
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Fahs-Beck Fund for Research and Experimentation Faculty Research Grant, the Fordham University Faculty Research Grant, and the Fordham University Graduate School of Social Service Faculty Research Development Fund.