
Abstract
The purpose of the present study is to analyze the potential impact of a custodial grandchild receiving mental healthcare on grandparent caregivers’ psychosocial functioning. Findings suggested that grandparents of grandchildren who had received some form of mental healthcare were more personally distressed, experienced less social support and more parental strain/stress, and were less resilient. Such grandparents were also less attached to their grandchildren and had grandchildren who were experiencing more emotional/behavioral difficulties. They were, however, more open to receiving psychological help. Findings also revealed that such effects were mediated by resilience, social support, and, to an extent, by parental self-efficacy. These data indicate that raising distressed grandchildren takes its toll on grandparents and that they are especially vulnerable, even if such grandchildren are receiving help.
Keywords
The Experience of Raising Children Who Are Distressed Among Birth Parents
Most adults can attest to the fact that good parenting requires both time and effort. Recent work, however, suggests that parenting children who are experiencing physical, social, or psychological difficulties is more challenging, wherein raising such children is associated with personal distress in birth parents, even if such children are receiving professional help (Boyden et al., 2022; Jin et al., 2021; Mastorakos et al., 2021; Muscara et al., 2015; Patel et al., 2022). Indeed, the severity of a parent’s distress co-varies with the course of a child’s therapy over time, as does the parenting stress they are experiencing (Friedman et al., 2020; Mastorakos et al., 2021; Sperling, 1997). In addition, over the course of a child receiving help, the parent’s ability to tolerate the child’s distress and the quality of the parent-child relationship change (Selles et al., 2018).
While there is evidence that grandchildren raised by grandparents face numerous adjustment-related challenges, some of which likely warrant help from a mental health professional, there is virtually no work that explores the potential impact that getting such help has on grandparents themselves. The present study builds upon the limited research that explores this issue, important to the mental health of both grandchildren and grandparents.
The Impact of Adjustment Difficulties Among Grandchildren Being Raised by Their Grandparents
In light of the aforementioned work exploring the relationship between child difficulties and parental distress among birth parents, it may also be that this would be the case among grandparents raising grandchildren. Indeed, raising grandchildren is associated with more psychosocial distress among grandparents than among age peers who are not raising a grandchild (see Dunifon, 2018; Kelley et al., 2021; Smith & Palmieri, 2007; Smith & Ricjardson, 2008; Smith et al., 2008). Underscoring the impact of grandchild difficulties on grandparents, previous work (Hayslip et al., 1998) found that grandparents who were raising grandchildren with emotional/behavioral problems experienced the most personal distress, the least role satisfaction and role meaning, and the most negative grandchild relationships, relative to grandparents raising grandchildren with few such problems.
In this light, the behavioral, social, and emotional challenges experienced by many, but not all, children raised by their grandparents may be due in part to long-standing problems in their families of origin or to challenges in adjusting to a newly formed full-time parental relationship (Hayslip et al., 1998; Pilkausakas & Dunifon, 2016; Smith et al., 2019; Xu et al., 2022). Such adjustment difficulties likely contribute to the distress that grandparent caregivers feel and most likely elicit thoughts of getting help for oneself and/or the grandchild. That grandchildren’s adjustment difficulties may persist into adulthood is supported by the work of Nadorff et al. (2022) who report greater evidence of anhedonia and suicidal ideation among adults who had been raised by their grandparents than among those raised by their biological parents; more frequent attendance at religious activities and greater household income did, however, mitigate such difficulties.
Seeking Help for a Distressed Grandchild
Based on the aforementioned grandfamily literature and that pertinent to the impact of raising a distressed child among birth parents, it would not be surprising to find that grandparents would be negatively impacted by the parenting challenges associated with the adjustment-related difficulties their grandchildren are experiencing. Relatedly, we might expect that grandparent caregivers would face distress in dealing with the ensuing process of overcoming barriers in getting help for their grandchildren (Hayslip et al., 2022). Such grandparents may also have to cope with the stigma of raising a distressed grandchild in need of help as well as difficulties in getting information about such help (Carr et al., 2012; Hayslip et al., 1998, 2020).
In this context, there is little literature focusing on the impact on grandparents with regard to their grandchildren receiving any form of mental health care. Montoro-Rodriguez et al. (2012) found among custodial grandchildren a 37% utilization rate of community-based services and a 51% rate of school-based services and that a grandchild’s externalizing symptoms as well as the presence of grandchildren with medical or psychiatric diagnoses in the home predicted service use. Dare et al. (2020) cite evidence (as reported by grandparents) of the benefits of a residential camp on grandchildren in terms of increased resilience, less isolation, and greater peer acceptance. Fruhauf et al. (2020) reported preliminary findings based on a multi-focus program (GRANDcares) that suggested programmatic gains in grandchild emotional regulation and communication skills. Significantly, none of these studies explored the impact of grandchildren getting some form of mental healthcare assistance on grandparents.
In the lone published study (Hayslip & Shore, 2000) exploring the potential impact of a grandchild receiving some form of mental health care on grandparent caregivers, nearly half (45%) of such grandparents in the sample of 102 stated that they had sought some form of help to assist them with their caregiving responsibilities or regarding behavioral or emotional difficulties experienced by their grandchildren. Importantly, those who, generally speaking, had sought help for the grandchild or for themselves were raising grandchildren with more emotional or behavioral difficulties, derived less meaning and less satisfaction from grandparenting, and experienced more emotional distress and poorer grandchild relationship quality. Yet, distinctions between seeking help for oneself or one’s grandchild were not made in this study (Hayslip & Shore, 2000). In addition, the sample itself was comparatively small. Indeed, comparably few grandparents, (between 8% and 10% of those raising problem-free grandchildren, between 10% and 30% of those raising grandchildren with problems) had ever sought any kind of professional help for themselves or the grandchild. In this context, however, recent work suggests that openness to seeking psychological help is key to understanding relationships between mental health attitudes and the use of mental health services among grandparent caregivers (Hayslip & Maiden, 2023).
Purposes of the Present Study
The present study is unique in building on the very limited literature exploring the potential impact of a grandchild receiving some form of mental healthcare on grandparents. Our work has several goals, all pertinent to grandfamilies’ mental health and adjustment. First, relying on cross-sectional/descriptive survey data gathered across the United States and Canada, we explore grandparent- and grandchild-related factors associated with a grandchild receiving mental healthcare. This will be accomplished by statistically (e.g., via analyses of variance [ANOVAs]) comparing survey data among those grandparents raising such grandchildren versus those that were not. Such surveys were completed by grandparent caregivers who were recruited primarily through announcements about the project and, to a limited extent, through contacts with undergraduates at the first author’s university. Second, again relying on cross-sectional/descriptive data and utilizing structural equation modeling as an analytic strategy, we examine relationships between grandchild and grandparent-related characteristics and several indices of grandparent adjustment among those families who had or had not sought mental healthcare for a grandchild. This analysis targeted resilience and social support as mediating influences, where resilience (Hayslip et al., 2013) and social support (Hayslip et al., 2015; Whitley et al., 2016) may each mitigate the otherwise negative impact on grandparents whose distressed grandchildren are receiving some form of mental healthcare. Third, we use 1-year longitudinal data in understanding the predictive role of a grandchild receiving help in accounting for grandparent caregiver adjustment, relying on both correlational analyses and repeated-measures ANOVAs to do so.
Method
Data Collection Procedures
After approval by the first author’s university institutional review board, participants were recruited within and around the Dallas/Ft. Worth, Texas, area as well as from other states and Canada, using available resources that included national organizations serving grandparents and grandparent caregivers (e.g., American Association of Retired Persons (AARP), Generations United, Grandparents.com), grandparent support groups, the community at large, and in a very small number of cases, contacts through undergraduate students. Most surveys were mailed to participants who expressed an interest in the project, which dealt with grandparent caregiving (Hayslip et al., 2013), and were returned to the first author. Originally, 270 survey packets were mailed to potential volunteers, and 239 participants returned the survey (88.1% response rate). Grandparents received no incentive for their participation. They did however receive a feedback letter detailing the original project’s findings. In the case of grandparents who were recruited via contacts through undergraduates, strict rules were enforced to ensure the reliability of such data, where surveys were sealed and signed by the participant with contact information included. Grandparents were then contacted by phone and their participation verified.
The data pertinent to the grandchild receiving mental healthcare were collected in 2012, but until the present article, they remained unanalyzed. With respect to the grandparent caregiving literature, it is important to note that these data are unique in their focus on the potential impact of a grandchild receiving mental healthcare on his or her grandparents. The present study reflects data gathered from a larger sample than the aforementioned 2000 study, utilizes a wider variety of grandfamily outcome measures, and incorporates longitudinal data to explore predictive relationships over time between grandchildren receiving help and grandparent functioning.
Cross-Sectional Sample
Participants qualified for the study if they were currently caring for a grandchild on a full-time basis. Participants were either in skipped-generation grandfamilies, (where the child’s biological parents are not currently residing with the grandparent and child) or they were in a co-parenting grandfamily (where the biological parent lived with them but was not the primary caretaker). Although we did not collect such data per se here, an independent study (Hayslip et al., 2021) of 109 of the 239 grandparents in this sample indicated that over 90% were raising a grandchild without any assistance from the child’s biological parent.
The sample consisted of 42 male and 196 female participants; one survey omitted gender. Seventy-nine percent of the sample was white, with African Americans being next most common, making up 13.8% of the total sample. Participants’ age ranged from 38 to 90 years, with the mean age being 58.06 (SD = 8.17). The number of grandchildren being cared for by a grandparent caregiver ranged from 1 grandchild to as many as 13, with the average number of grandchildren being cared for being 1.61 (SD = 1.19). The mean age of the grandchild in care was 9.44 (SD = 4.65) and ranged from less than a year to 24 years of age. The average length of time that a grandparent had been caring for his or her grandchild was 6.44 years (SD = 4.68, range = less than a year to 24 years). Annual household income ranged from less than $10,000 to over $60,000: 13.1% reported annual incomes up to $20,000; 24.3% had annual incomes between $20,000 and $40,000; 28.7% reported incomes between $40,000 and $60,000; and 33.9% reported earning over $60,000 annually.
One-Year Longitudinal Sample
The one-year longitudinal sample consisted of 86 caregiving grandparents (Mage = 59.39, SD = 7.79, range = 43–73; 83.7% women) who had full-time responsibility for their grandchildren (Mage = 9.66, SD = 4.29; 44.2% girls, years of care M = 5.86, SD = 4.36). The racial/ethnic composition of the longitudinal sample was 89.2% white, 6% African American, and 4.8% Hispanic. The majority (66.7%) of these grandparents reported being married, 17.8% were divorced, 10.7% were widowed, and 4.8% were single. Thirty-seven percent of grandparents were working full-time, 18.5% worked part-time, and 44.5% were retired. Grandparents reported caring for up to four grandchildren under the age of 18 years who currently lived with them; 66.7% were raising one grandchild, having been the primary caregiver for between 1 and 24 years. The annual household income (based on an n of 75) ranged from less than $10,000 to over $60,000: 9.9% reported annual incomes up to $20,000; 27.2% had incomes between $20,000 and $40,000; 27.1% reported incomes between $40,000 and $60,000; and 35.8% reported earning over $60,000 annually. For data analytic purposes, in both the initial and longitudinal samples, income was coded along a continuum of increments of $10,000 annually, ranging from 1 to 7, with higher values indexing greater annual income. Grandparent caregivers who participated in the longitudinal study (n = 86) were older and had more grandchildren living at home (p < .05) than those who did not participate.
Measures
A variety of measures were completed by participants in a survey format. Each survey took approximately an hour to complete. These measures assessed grandchild adjustment/difficulties, grandparent resources and help-seeking attitudes, grandchild relationship quality, parenting demands, and grandparent adjustment. They have been utilized in grandparent caregiving research for several decades and cut across many domains of custodial grandparenting (see Dunifon, 2018; Kelley et al., 2021; Xu et al., 2022). In this study, we utilized multiple indicators of the following: Grandparents’ health, grandchild distress, parenting demands, grandparent adjustment, and grandchild relationship quality (all reported by grandparents, see below). In addition, and relevant to a grandparents seeking help for a distressed grandchild or oneself, grandparents completed a measure of openness to seeking help and a measure of social support. Unless the grandparent was caring for a single grandchild, grandparents selected a given child under the age of 18 whom they were raising who had been in their care the longest and answered any questions pertinent to a grandchild with this grandchild in mind.
Openness to seeking psychological help was assessed via a list of 24 problems such as deep depression, forgetfulness, loneliness, trouble sleeping, and arguments with children (Hayslip & Maiden, 2023). Participants were asked whether they would seek help from a mental health professional for each problem. The number of items each participant endorsed was summed to give an Openness score, wherein higher scores indicated greater openness toward seeking mental health services. The alpha coefficient for Openness in the present sample was 0.89.
Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) is a 12-item measure of perceived social support from family, friends, and significant others. For example, “There is a special person who is around when I am in need.” Each item is scored on a Likert-type scale, where 1 = very strongly disagree to 5 = very strongly agree, and higher overall scores reflect more perceived social support. The alpha coefficient for the MSPSS is 0.95 in the present sample.
Grandparent Health: Short Form-36 General Health Survey
The Short Form-36 (SF-36; Ware, 1993) is a 36-item self-report measure that was used to assess physical health. The SF-36 has scales measuring physical functioning, role disability due to physical health problems, bodily pain, general health perceptions, vitality, social functioning, role disability due to emotional health problems, and general mental health. We used a 16 item assessing health limitations, 9 item assessing pep/vigor, and 4 items assessing self-rated health to assess multiple dimensions of overall physical health in this sample, where all items were drawn from the SF-36. These were totaled to yield an overall measure of physical health (alpha = 0.93), where higher scores indexed better overall physical health. This multi-faceted index of health has been used to explore relationships with both social support and well-being among grandparent caregivers over time (Hayslip et al., 2014, 2015).
Grandparent Health: Overall Self-Rated Health
To reflect the fact that the aforementioned measure of physical health had a substantial amount of missing data (22 cases), we also constructed a second 4-item measure of self-rated health (3 missing cases, alpha = 0.79), where items reflected self-rated sickness relative to others, perceptions of one’s health worsening, perceived excellence of health, and self-rated health relative to others. Higher scores indexed better overall self-rated health.
Grandchild Distress: Strengths and Difficulties Questionnaire
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001) consists of 25 items rated by the grandparent along a 3-point Likert-type scale, with 1 = not true and 3 = certainly true, and is used to assess the psychological adjustment of children and adolescents. The 25 items are divided into five difficulty subscales that look at prosocial behavior, emotional symptoms, conduct problems, hyperactivity-inattention, and peer problems. For purposes of the present study, an overall index of grandchild difficulties was created by summing the items comprising the aforementioned subscales (alpha = 0.87); higher scores reflected more such difficulties.
Grandchild Distress: Grandparent-Rated Grandchild Problems
To supplement the SDQ, grandparents rated the extent to which they felt their grandchild (1 = no problem to 5 = severe problem) was experiencing each of nine different difficulties (e.g., abuses alcohol, hyperactivity, depression) that reflected both internalizing and externalizing behavioral/emotional difficulties (alpha = 0.72). Higher total scores reflected greater grandparent-rated grandchild problems.
Parenting Demands: Parental Role Strain
Custodial grandparent’s parental role strain was assessed via a 17-item measure derived from the Structure of Coping Scale (Pearlin & Schooler, 1978) and used to identify potential strains in grandparent’s roles as parents, as well as to identify emotional stress experienced by grandparents connected to this role. Each item is scored on a 4-point scale, where 1 = never to 4 = very often. Higher scores indicted the grandparent experienced more strain associated with the caregiving role (alpha = 0.89).
Parenting Demands: Grandparent Parental Role Stress
A 12-item measure assessed (grand) parenting stress (Abidin, 1990), where higher scores (1 = not at all to 4 = very) reflect higher levels of such stress in the grandparenting role (alpha = 0.89). Exemplar items are, for example, “I feel trapped by my responsibilities as a parent,” “I am not as interested in people as I used to be,” “Since having my grandchild I feel I am almost never able to do the things that I like to do,” and “I find myself giving up more of my life to meet my grandchild’s needs than I ever expected.” Higher scores indexed greater parental role stress.
Parenting Demands: Parental Self-Efficacy
To measure parental self-efficacy, a nine-item scale (Bachicha, 1997) assessed grandparents’ perceptions of their ability as parents to solve problems and understand their grandchild. Each of the nine items were answered on a 5-point Likert-type scale, where 1 = strongly disagree to 5 = strongly agree. Higher scores indicated a lessened parental self-efficacy (alpha = 0.88). This scale has been successfully used to assess the impact of a psychosocial intervention targeting grandparent caregivers (Hayslip, 2003).
Grandparent Adjustment: Grandparenting Satisfaction
As utilized by Thomas (1990), satisfaction with grandparenting was assessed via 15 questions (alpha = 0.79). Each question was answered on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree), and higher scores reflected greater role satisfaction.
Grandparent Adjustment: The Resilience Scale
The Resilience Scale (RS, Neill & Dias, 2001) is a 15-item self-report survey modified from the resilience measure of Wagnild and Young (1993) that was used to assess themes of resilience. All items are worded positively, and responses are on a 4-point Likert-type scale. Concurrent validity has been supported by significant correlations between RS scores and measures of morale, life satisfaction, and depression (Neill & Dias, 2001; Wagnild & Young, 1993). Its Cronbach’s alpha is 0.91, and higher scores represent higher levels of resilience.
Grandparent Adjustment: Psychological Well-Being
Psychological well-being (Liang, 1985) was assessed via 15 items that measure respondents’ feelings about their lives. Exemplar items are “As I look back on my life I am fairly well satisfied” and “I feel very lonely” (reverse scored). Higher overall scores indexed greater well-being. Its alpha coefficient in the present sample was 0.90.
Grandparent Adjustment: Center for Epidemiologic Studies Depression Scale
Psychological distress/depression was assessed via the 20-item Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) measuring one’s current level of depressive symptomatology with an emphasis on depressed mood. Participants were asked to endorse the response that best described how often they felt a particular way in the past week. Questions were answered on a 4-point Likert-type scale, where 1 = rarely or some of the time to 4 = most or all of the time. Its alpha coefficient in the present sample was 0.89. CES-D responses were coded so that higher scores indexed less depressive symptomology.
Grandchild Relationship Quality: Attachment to the Grandchild
Participants completed a 28-item measure of grandparent-grandchild emotional and behavioral attachment (Armsden & Greenberg, 1987) reflecting a grandparent’s emotional and behavioral orientation to a specific target grandchild, that is, the child they knew the best (alpha = 0.88). Exemplar items include “I sense when my grandchild is upset about something” and “When we discuss things, I respect my grandchild’s point of view.” Higher scores (1 = strongly disagree to 5 = strongly agree) indexed lesser attachment to the grandchild.
Grandchild Relationship Quality: The Positive and Negative Affect Scale
This is a 19-item measure representing the respondent’s levels of positive and negative affect. It includes nine items (1 = none to 5 = a great amount, alpha = 0.89) and negative affect (10 items, 1 = never to 5 = very often, alpha = 0.65) with regard to one’s grandchild, where again, grandparents reported on same target grandchild, that is, the grandchild that they knew best. In an independent study using the Positive and Negative Affect scales, alphas exceeded 0.92 (Hayslip et al., 1998). Exemplar items on the Positive Affect scale are “How much affection do you feel your grandchild has for you?” and “How much do you trust your grandchild?” Those for Negative Affect are “How often do you find your grandchild’s tone of voice irritating?” and “How often do you and your grandchild show anger and dissatisfaction with each other?” Higher scores indexed less positive affect and greater negative affect toward the grandchild (Bence & Thomas, 1988).
Analytic Plan
Utilizing descriptive/cross-sectional data, we first explored differences in the aforementioned grandfamily measures as well as sociodemographic characteristics as a function of whether grandchildren had (yes) or had not (no) received mental health services/counseling to deal with his or her behavioral difficulties, as reported by the grandparent. To assess such between-group differences, we used a one-way multivariate analysis of variance (MANOVA), with univariate analyses as appropriate (p < .05). A subsequent discriminant function analysis explored the best linear combination of grandfamily measures differentiating each group of grandchildren. To examine the longitudinal relationship between grandchildren having received counseling or not at Time 1 and the aforementioned grandfamily measures data collected 1 year later as dependent variables, a two (grandchild help) by two (occasion) MANOVA was also carried out, with univariate analyses performed as appropriate. The current analyses included those grandparent caregivers with data collected at both the initial assessment and at one-year follow-up. Missing data across variables were minimal (less than 4% of the sample), with most missing data being related to income (n = 8), attachment (n = 8), and social support (n = 7).
Structural Equation Analysis
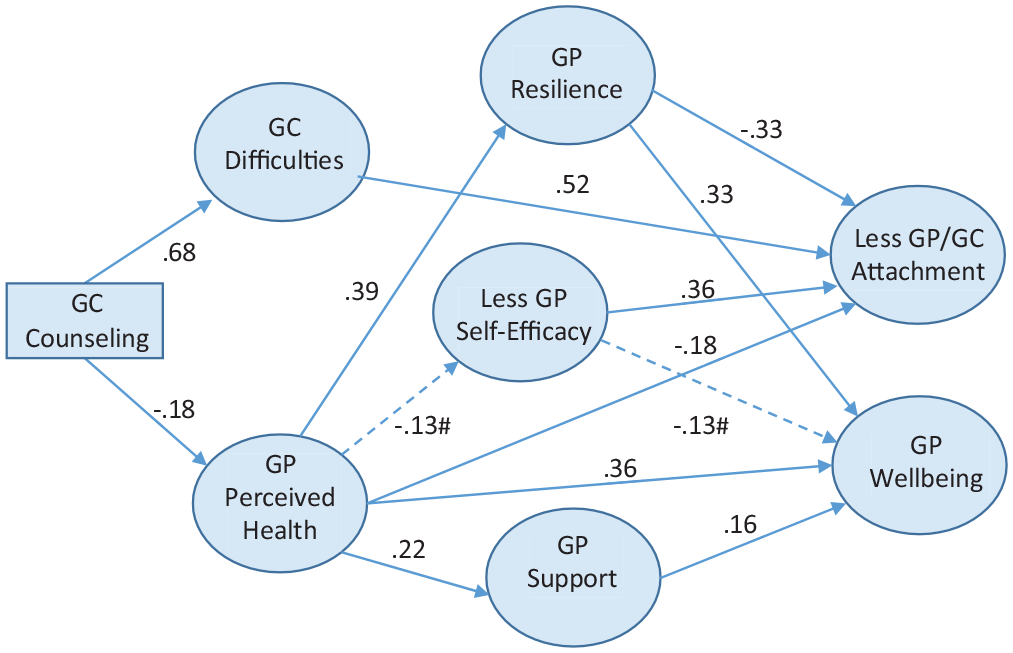
To explore relationships between grandchildren receiving help and relying on multiple measures of grandfamily functioning, we tested a structural equation model. This structural equation analysis enabled us to explore individual differences in relationships between grandchildren receiving mental healthcare, their distress, and grandparent functioning as predictors and both grandparent-grandchild relationship quality/attachment and grandparent well-being as outcomes. This model represents resources and coping mechanisms of both grandparents and their grandchildren (see Figure 1) and parallels a process approach to caregiving (Pearlin et al., 1990) specifying antecedents, mediators, and caregiving outcomes.
SEM Findings: Direct and Indirect Influences of Grandchild Counseling Help on Grandparent Attachment and Wellbeing.
This model centralized the roles of health, social support, resilience, and parental efficacy as mediators/links in understanding the relationships between the effect of distressed grandchildren receiving mental health care/assistance on grandparent well-being and grandchild attachment. These mediators and outcomes have received a great deal of attention in understanding grandparent caregiving over the last two decades (Hayslip et al., 2013; Hayslip & Fruhauf, 2019; Park & Greenberg, 2007) and thus were logical candidates for the structural model we tested here.
Description of the Model
The following variables (see Figure 1) were included in the model: (a) Use of counseling for the grandchild, a dichotomous group variable (received/not received), where receiving such help was coded as “2,” and not receiving such help was coded as “1”; (b) Grandchild difficulties, represented as a latent variable measured by four items using a 4-point scale to indicate the overall level of difficulties categorized as emotions, concentration, behavior, and relationships (SDQ); (c) Self-rated health, a latent variable measured by four items using a 5-point scale (SF-36 Health Interview) to represent grandparent level of health; (d) Perceived social support, represented as a latent variable measured by three parcels derived from the aforementioned 12-item measure (Multidimensional Scale of Perceived Social Support); (e) Parental self-efficacy, represented as a latent variable measured with three parcels formed from the above nine-item scale; (f) Personal resilience, a latent variable measured with three parcels from the 15-item scale assessing themes of resilience; (g) Attachment to the grandchild, a latent variable measured with four parcels derived from the above 28-item measure of grandparent emotional and behavioral attachment to the grandchild; and (h) Psychological well-being, a latent variable measure derived from three parcels from the aforementioned 15-item self-report scale measuring respondents’ feelings about their lives. Of central interest here were both grandparent well-being and attachment to the grandchild as outcomes (see Figure 1). These relationships were also explored longitudinally via correlational analyses.
Specifying the Model to Be Tested
The model included direct and indirect paths from the use of mental health services by grandchildren to all other variables in the model. Co-variances were allowed between the two dependent variables (attachment with grandchild and parental well-being), mediators (resilience, parental self-efficacy, social support), as well as grandparent physical resources (self-rated health) and grandchild-related stressors (grandchild difficulties). The model exploring predictors of well-being and quality of grandchild/grandparent relationship outcomes was tested using Amos Version 28 (Arbuckle, 2022).
To specify and test the model, parcels were derived for most latent variables using the original scale items to reduce the number of variables in the analysis, for example, if a scale had 15 items, three parcels were created assigning the first five to that partial and so on. Parcels are useful tools and have the potential to enable a clear and interpretable test of a research hypothesis (Little et al., 2013).
Results
Grandchildren’s Distress: Descriptive Findings
Eighty grandchildren were reported by the grandparent to be receiving some form of counseling/mental health services, while 159 were reported as not receiving such services. When asked regarding what emotional/behavioral problems the grandchild was being treated for, the most commonly reported difficulties were learning problems (n = 50), hyperactivity (n = 42), depression (n = 33), and oppositional behavior (n = 27). None of the remaining problems (alcohol abuse, drug abuse, sexual identity, mental retardation, breaking the law) were reported frequently (ns < 7).
When asked an open-ended question regarding treated grandchild problems, issues pertaining to the grandchild’s reactions to abandonment, anger, anxiety, attachment, or trauma were mentioned most often (n = 25), followed by attentional difficulties/hyperactivity (AD/ADHD, n = 14), being physically or emotionally abused (n = 4), Asperger’s syndrome (n = 3), bipolar disorder (n = 3), and autism (n = 3).
Comparisons Across Grandchildren Receiving or Not Receiving Mental Healthcare
The MANOVA (complete data for 206 grandparents, 68 receiving help, 138 not receiving help) exploring differences in grandfamily constructs across the presence/absence of receiving mental healthcare/counseling or treatment was statistically significant (F20,182 = 10.39, p < .01, η2 = .53). Univariate ANOVAs indicated that grandparents raising grandchildren receiving some form of mental health counseling/treatment (ps < .05) had more grandchildren under the age of 18 living with them, were raising grandchildren who were older, reported less social support, were less resilient, and reported more parental role strain and role stress (see Table 1). In addition, such grandparents experienced more negative/less positive affect regarding the behaviors of the grandchild, were less strongly attached to the grandchild, were less satisfied with the grandparent role, reported poorer overall self-rated health, and were raising grandchildren with more behavioral, emotional, and social-relational difficulties (see Table 1). On the other hand, they were more open to seeking psychological help. There were no differences across grandchildren groups (receiving help or not) regarding grandparent well-being, depression, grandparent age, duration of care, income, or parental self-efficacy. Moreover, such groups did not vary by either grandparent or grandchild gender (see Table 1).
Grandfamily Constructs and Grandchildren Receiving Help (Time One).
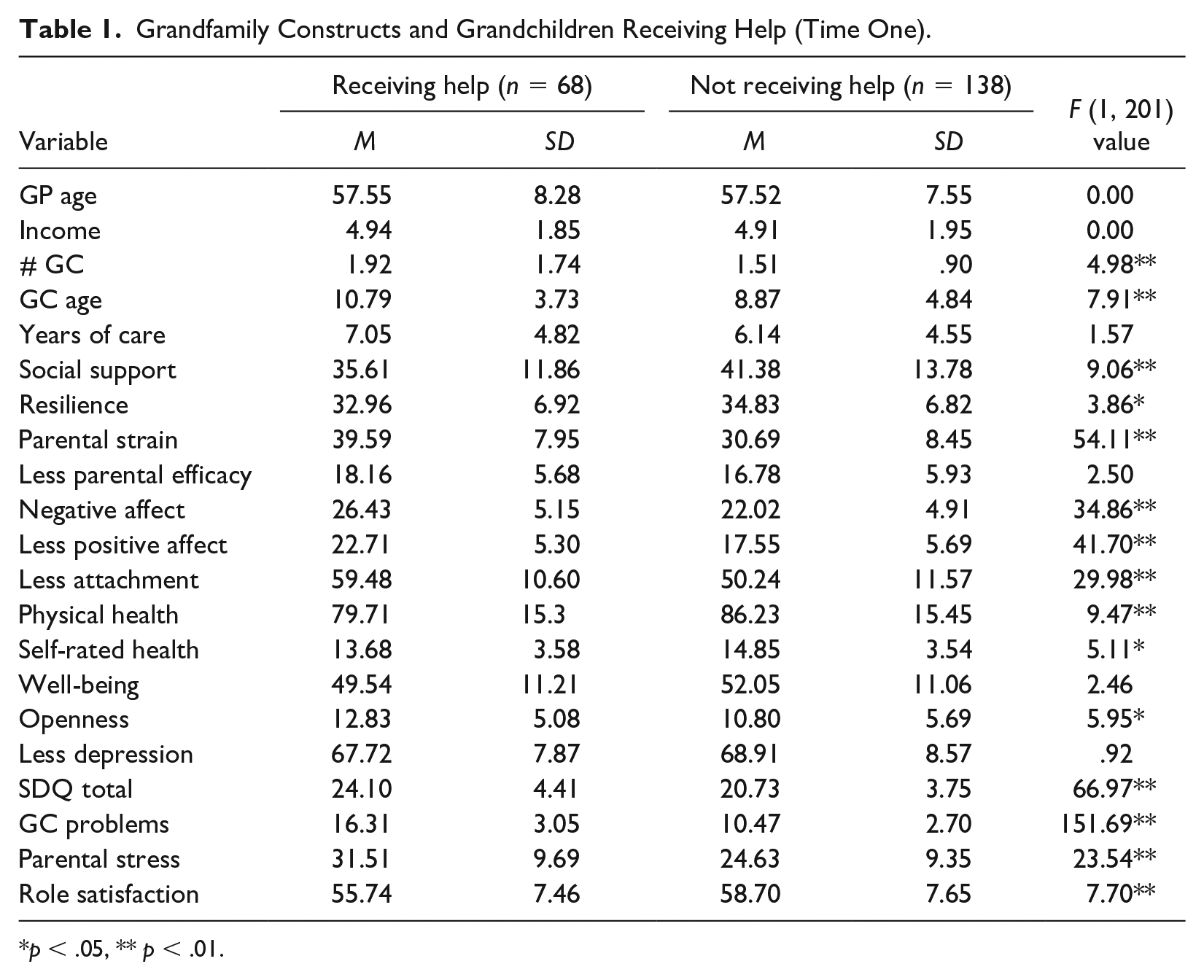
p < .05, ** p < .01.
Factors Having the Most Salient Relationships With Grandparent Functioning Across Grandchildren Receiving Help Groups
To identify the most important factors impacting the differences between grandparents whose grandchildren were or were not receiving help, we performed a discriminant function analysis. This yielded a single such function (Wilks’ Lambda = .467, χ220 = 145.48, p < .01) that accurately classified 89.7% of cases. Variables with the most salient discriminant function coefficients were grandparent-rated grandchild problems (.86), parental stress (.38), less positive affect (.32), openness to seeking help (.22), role satisfaction (.20), parental self-efficacy (−.16), well-being (.18), and number of grandchildren (.16).
Longitudinal Findings: Grandchildren Receiving Help at Time One and Grandparent Functioning at Time Two
An initial MANOVA indicated that participants who participated in the 1-year longitudinal follow-up (n = 86) were not different (p > .05) from those who did not do so for the aforementioned measures as a set. For the 1-year longitudinal sample, analyses then explored whether grandchildren receiving help or not at Time 1 (complete data for n = 82, with 33 grandchildren receiving help and 49 grandchild not receiving help) co-varied with the aforementioned grandfamily measures over time, that is, 1 year later.
A repeated-measures MANOVA of the 1-year follow-up data by whether or not grandchildren were receiving counseling assistance/help at Time 1 indicated that for the variables as a set, the effects of having earlier received help were statistically significant (F13,66 = 2.09, p < .03, η2 = .29). At the univariate level, findings indicated (p < .05) that grandparents whose grandchildren had earlier been reported as receiving help, 1 year later, experienced poorer health, more parental stress and parental strain, more depression, and more negative affect/less positive affect associated with the behavior of the grandchild (see Table 2). At Time 2, there were no between-group differences regarding having received help or not a year earlier in role satisfaction, well-being, social support, resilience, attachment, and parental self-efficacy. That only five grandchildren received help for the first time at Time 2 precluded an examination of the impact of grandparent constructs at Time 1 on grandchildren receiving help at Time 2.
Grandfamily Constructs at Time 2 and Grandchildren’s Receiving Help at Time 1.
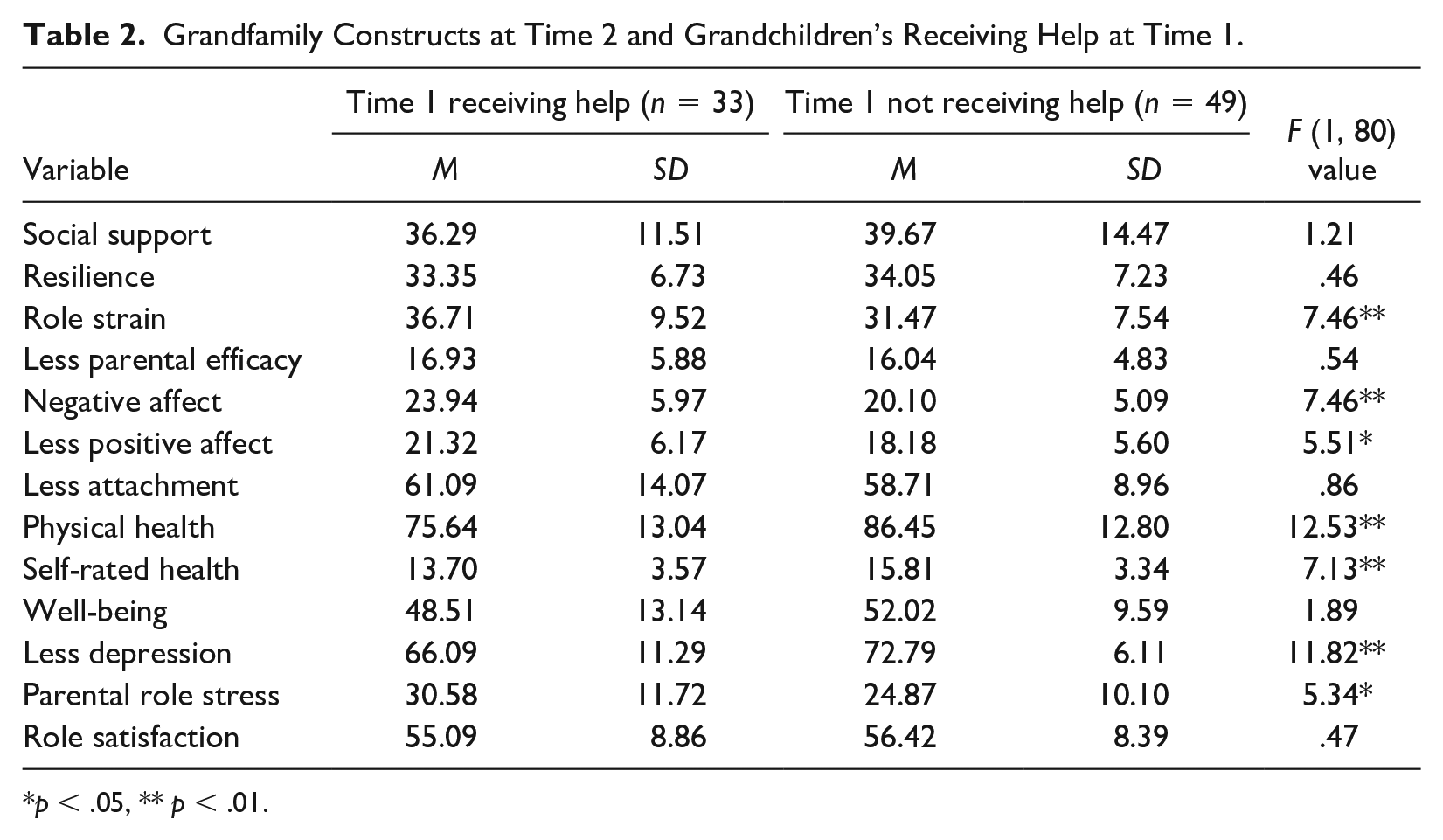
p < .05, ** p < .01.
Grandparent Functioning Over Time and Grandchildren’s Receiving Help
We then conducted an analysis of whether grandfamily variables changed over time and whether such changes varied by whether the grandchild had received help at Time 1 or not. Repeated-measures ANOVAs indicated that, irrespective of grandchildren receiving help, overall physical health improved over time (Mtime1 = 77.95, Mtime2 = 87.00, F1,82 = 7.50, p < .01). For attachment (where higher scores indexed less attachment), scores declined over time (Mtime1 = 54.06, Mtime2 = 59.63, F1,80 = 23.98, p < .01). In addition, the grandparent’s rating of the grandchild’s difficulties (Mtime1 = 13.38, Mtime2 = 12.51, F1,77 = 5.86, p < .05) lessened over time, as did negative affect toward the grandchild (Mtime1 = 24.40, Mtime2 = 21.21, F1,83 = 28.87, p < .01). None of these changes over time interacted with grandchild counseling status.
In contrast, for the total Strengths and Difficulties score, while we found that such scores declined over time (Mtime1 = 21.86, Mtime2 = 16.96, F1,84 = 66.37, p < .01), the grandchild counseling by time interaction modified this pattern (F1,84 = 6.28, p < 01), where overall Strengths and Difficulties scores for those grandchildren receiving help earlier declined moderately over time (Mtime1 = 23.97, Mtime2 = 19.94). In contrast, for grandchildren not having earlier received help, declines in Strengths/Difficulties scores over time were of greater magnitude (Mtime1 = 20.77, Mtime2 = 13.16). The grandchild counseling by time interaction was also statistically significant for grandparent depression (where higher scores indexed less depression) (F1,82 = 4.27, p < .05). For grandchildren having earlier received help, grandparent depression worsened over time (Mtime1 = 67.76, Mtime2 = 65.32), while for those grandparents whose children had not earlier received help, emotional distress/depression improved (Mtime1 = 70.96, Mtime2 = 72.94).
Structural Equation Findings: Relationships Between Grandchildren Receiving Mental Healthcare and Grandparents’ Well-Being and Attachment to the Grandchild
Results indicated overall good model fit, χ2/df = 1.41, comparative fit index (CFI) = 0.968; Tucker-Lewis Index (TLI) = 0.959; root mean square of approximation (RMSE) = 0.04. Findings suggested that grandchildren’s use of mental health services influenced both the quality of their relationship to the grandparent as well as the well-being of the grandparent, as mediated primarily through two different coping mechanisms (grandparent resilience and social support). While receiving mental healthcare had no direct effects on well-being and attachment, the use of such services significantly impacted the level of the grandchild’s emotional/behavioral difficulties (beta = .68), which in turn had a direct impact on the quality of the relationship between grandparent and grandchild, as indexed by attachment (beta = .52).
Receiving mental healthcare also had a direct effect on the grandparent perceived health (beta = −.15), which in turn had a direct impact on attachment (beta = .18) and well-being (beta = .33) and an indirect impact on well-being through the grandparent’s social support and resilience. The total standardized effect of receiving counseling on attachment was 0.28, and for well-being, it was −0.12. Grandparents’ self-rated health had the highest total effect on their well-being (0.55), as did grandchildren’s behavioral difficulties on the quality of the relationship with/attachment to the grandparents (0.54). Results indicated a moderately high adjusted R2 for grandparents’ well-being (55%) and attachment (51%). Finally, two additional paths, although not statistically significant, were nonetheless somewhat substantial: the influence of grandparents’ health on their parental self-efficacy (p < .08) and the impact of parental self-efficacy on grandparents’ well-being (p < .08; see Figure 1).
Longitudinal Correlational Findings
That the longitudinal sample was comparatively small (N = 86) and the number of free parameters to be estimated was large precluded the estimation of a stable model via structural equation modeling (Kline, 2011).
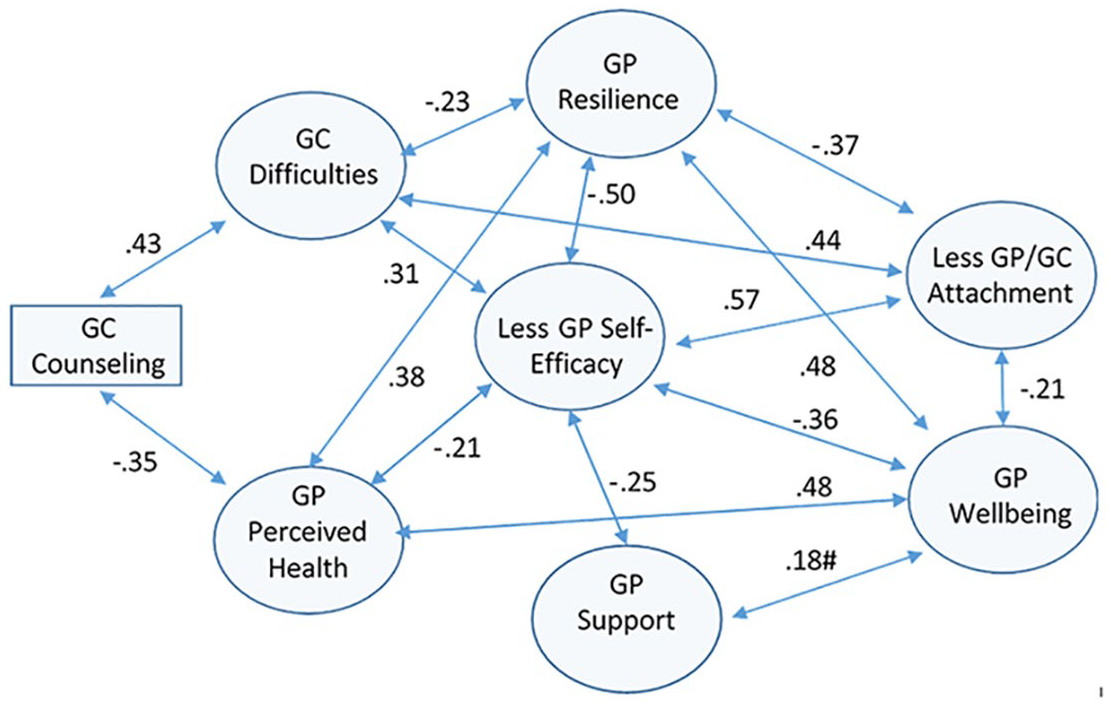
For this reason, we instead computed Pearson Product Moment correlations between grandchildren having had/had not received mental health care at Time 1 and both grandchild-related (difficulties, attachment) and grandparent-related variables (resilience, parental self-efficacy, social support, health, well-being), all at Time 2 (see Figure 2). Findings indicated that the influence of grandchildren receiving help at Time 1 on both grandparent-grandchild attachment and grandparent well-being at Time 2 was mediated by/linked to both resilience and parental self-efficacy and, to an extent, (p < .10) by social support via their relationships with either grandchild emotional/behavioral difficulties or grandparent self-rated health.
Correlations Between Grandchild Counseling Help at Time 1 and Grandparent-Related Constructs at Time 2.
Discussion
Our purpose here was to explore indices of grandparent functioning that are potentially impacted by the fact that the grandchildren they are raising are receiving some form of psychological help/counseling to assist them in coping with a number of psychosocial difficulties. Such problems may have manifested themselves prior to coming to live with the grandparent, arising out of adjustment problems experienced by grandchildren-linked parental divorce, drug abuse, death, parental incompetence, and/or abandonment (Hayslip et al., 1998; Hayslip & Fruhauf, 2019). Such difficulties complicate the grandchild-grandparent relationship and likely exacerbate a grandparent’s distress.
The present study breaks new ground in the grandfamily literature building upon limited earlier work (Hayslip & Shore, 2000) in (a) not only targeting mental healthcare for the grandchild, but also (b) relying on a larger sample of grandfamilies and (c) in encompassing a wider array of measures related to not only grandparent distress but also grandparent-grandchild relational characteristics and parenting attributes. It is important to note that this study’s uniqueness is further enhanced via its longitudinal nature and the use of SEM to explore relationships between grandchildren receiving help and a variety of grandchild/grandparent characteristics. In this respect, we note that other models could be developed that might also fit the data (Kline, 2011).
Cross-Sectional Comparisons Across Grandchildren Receiving or Not Receiving Help
The between-group comparisons indicate that grandparents raising grandchildren receiving some form of mental health counseling/treatment (ps < .05) had more grandchildren under the age of 18 living with them and were raising grandchildren who were older. Importantly, they reported less social support, more parental role strain and role stress, and experienced more negative/less positive affect regarding the behaviors of the grandchild. They also were less strongly attached to the grandchild, were less satisfied with the grandparent role, reported poorer health, and were raising grandchildren with more behavioral, emotional, and social-relational difficulties (see Table 1). On the other hand, they were more open to seeking psychological help.
These between-group comparisons suggest that grandparents whose grandchildren were receiving help were indeed more distressed, paralleling work with birth parents (see e.g., Boyden et al., 2022). More importantly, we found that not only did these children evidence more emotional and behavioral difficulties as reported by the grandparent but that among such grandparents, the quality of their relationships with the grandchildren they were raising was also undermined. This may be due to the challenges of parenting such children (who were also more distressed) who likely posed greater demands on grandparents.
These between-group findings seem to parallel those of Baker and Silverstein (2008) who found grandparent caregivers to prioritize their grandchildren’s health concerns behind those of their own. To the extent that grandparent caregivers are experiencing personal distress, either driven by the demands of raising a grandchild (see Pilkausakas & Dunifon, 2016; Smith et al., 2019) or by the difficulties associated with raising a distressed grandchild (Hayslip et al., 1998), such concerns seem to lead to seeking help for such a grandchild. It is also possible that despite being open to seeking help, the stigma and/or lack of knowledge about childhood adjustment problems, each associated with raising and seeking help for an emotionally/behaviorally challenged child, contributed to the distress associated with that child receiving help among grandparent caregivers. Answers to these questions warrant future research.
Longitudinal Findings: The Potential Impact of Grandchildren Receiving Help on Grandparents
Longitudinally, this pattern was for the most part replicated, and over the 1-year timeframe, grandparents whose grandchildren had earlier been reported as receiving help reported subsequent poorer health, experienced more parental stress and parental strain, reported more depressive symptoms, were less strongly attached to their grandchildren, and reported more negative affect associated with the behavior of the grandchild (see Table 2). The repeated-measures findings indicating that grandchild problems (Strengths/Difficulties scores) declined to an extent yet depression worsened over time among grandparents raising grandchildren receiving help at Time 1 are consistent with the negative impact of grandchildren receiving help on the grandparents caring for them.
Mediators of Relationships Between Grandchildren Receiving Help and Grandparent Functioning
The structural equation findings (see Figure 1) suggest that the impact of grandchildren receiving mental healthcare is secondarily mediated by a grandchild’s emotional/behavioral difficulties, grandparent health, and to an extent, (grand) parental self-efficacy. Ultimately, however, they suggest that grandparent resilience and social support are key mediators of the relationship between grandchildren receiving help and grandparents’ well-being and attachment to the grandchild, as they relate to a grandchild’s emotional/behavioral difficulties and the grandparent’s health (see Figure 1).
This may suggest that raising a grandchild with behavioral and/or emotional problems and/or the state of one’s health lays the groundwork for the mitigating roles of personal resilience, the availability of social support, and to an extent, the development of parental self-efficacy as coping mechanisms in raising a grandchild who is experiencing behavioral or emotional problems. This pattern is consistent with the protective effects on well-being of both resilience (Hayslip et al., 2013) and social support (Whitley et al., 2016). Nevertheless, future work is warranted exploring both grandchild and grandparent functioning as well as the relational dynamics between grandparent and grandchild over the course of the grandchild receiving help. These may be further clues to the roles many factors might play in explaining the potential impact of grandchild difficulties on grandparent caregivers.
The correlational patterns in Figure 2 are, for the most part, consistent with the aforementioned Time 1 structural equation findings in Figure 1. They moreover support the possibility of multiple longitudinal paths of the potential causal influence of grandchildren receiving help on both grandparent-grandchild attachment and grandparent well-being, as mediated by resilience, parental self-efficacy, and to an extent (p < .10), social support via their relationships with either grandchild emotional/behavioral difficulties or grandparent health (see Figure 2). These longitudinal correlational patterns are thus valuable in identifying multiple indirect patterns of potential causal influence between grandchildren receiving mental healthcare and grandparent well-being and attachment to the grandchild.
Limitations: Concerns Regarding Causality
Although these cross-sectional comparisons are novel, we urge caution in interpreting the relationship between grandchildren receiving help and grandparent functioning as causal in nature, that is, those pertaining to comparisons across grandchild receiving help groups. Indeed, the between-group (receiving help/not receiving help) differences we found here may reflect pre-existing patterns of grandchild and/or grandchild adjustment, where grandparents who are already more psychosocially vulnerable may be predisposed to having more difficulty coping with a grandchild’s distress. That this may be a possibility is reflected in the work of Smith et al. (2023) who found relationships between self-reported adverse childhood experiences (ACEs), that is, a history of physical or emotional abuse, and custodial grandmothers’ physical and emotional well-being. Likewise, grandchildren who have been emotionally abused or experienced family trauma leading to the divorce of their parents may be predisposed toward emotional or behavioral difficulties (Hayslip et al., 1998). This is consistent with the pattern of emotional, psychosocial, and behavioral difficulties among such grandchildren ultimately giving rise to the need for mental healthcare. Moreover, the presumably direct relationship between grandchildren receiving help and grandparent functioning is in fact an indirect one, mediated principally by both social support and resilience and, to an extent, parental efficacy, as per our SEM findings.
The aforementioned cautions not withstanding, the longitudinal findings bear out the relationship between a grandchild receiving help at Time 1 and subsequent changes over time in grandparent functioning. This might imply a causal relationship between the two, although this could be mediated by heretofore-unidentified factors. Such influences could reflect the psychosocial context in which grandparent caregivers find themselves in facing isolation or discrimination from others (Hayslip et al., 2019; Hayslip & Fruhauf, 2019). Nevertheless, they should be replicated with other samples of custodial grandchildren and grandparent caregivers, as should the between-group comparisons. The longitudinal findings here thus suggest the potentially causal role that a grandchild receiving help plays in contributing to not only grandparental distress but also to less-positive relationships with a distressed grandchild (see Dunifon, 2018; Hayslip et al., 2019; Kelley et al., 2021). Although it could not be longitudinally examined here, it is also possible that a grandparent’s personal distress, child relationship difficulties, or ineffective parenting practices give rise to the grandchild’s difficulties, leading to the decision to seek help for a grandchild.
Additional Limitations of the Present Study
Although the patterns of relationships between variables over time (see Figure 2) are, for the most part, consistent with the structural equation findings, they are nonetheless influenced by measures’ relationships to one another. Thus, they may be somewhat less informative versus the SEM findings, where such relationships are taken into consideration in estimating a final model whose fit to the data is good (Kline, 2011). At the minimum, these findings suggest the need for longitudinal data utilizing a SEM approach exploring potential causality over time. It also remains to be seen what other, yet to be identified, factors (e.g., isolation, poorer health, difficulties in accessing services, worsening grandchild functioning) might account for the longitudinal relationship between grandchildren’s receiving help and grandparent functioning one year later.
Despite our work’s novelty and contribution to the grandfamily literature, there are other limitations to be acknowledged here. Over and above the aforementioned discussed concerns about causality, we know nothing about the nature of the mental health assistance grandchildren were receiving as reported by the grandparent. Thus, we are limited to not only grandparents’ reports on their grandchildren’s emotions and behavior but also to their reports of the grandchild receiving help. Nor do we know anything about the duration or efficacy of this help. Yet, as one might expect, at both Time 1 and Time 2, there were substantial relationships between grandchildren receiving mental healthcare and the extent to which they manifested emotional, interpersonal, or behavioral problems, as measured by the SDQ (rs of .68 at Time 1, .43 at Time 2, both p < .01).
Despite the aforementioned limitations, it is significant that we found that the Strengths/Difficulties scores for those grandchildren receiving help declined moderately over time. However, as might be expected, for grandchildren not receiving help (who were less distressed), declines in Strengths/Difficulties scores over time were of greater magnitude. This pattern might suggest that receiving help was somewhat beneficial for grandchildren. Significantly, however, for grandchildren receiving help, grandparent depression worsened over time, while for those grandparents whose children were not receiving help, emotional distress/depression improved.
Implications for Practice
These findings underscore the negative impact on grandparents whose children, being more distressed, are getting help to alleviate this distress. This pattern may reflect the interaction of both grandparent and grandchild functioning with the course of therapy/treatment/counseling, where previous work has found that for the most part, parent distress, parenting distress, and relationships with a child improve over the course of treatment (Friedman et al., 2020; Mastorakos et al., 2021; Selles et al., 2018). Because the overall picture (via both between-group comparisons and longitudinally) here was negative regarding the impact of grandchildren receiving help on grandparent functioning and grandchild relationship quality, we might infer that most grandchildren who were receiving help had just begun or were in the early phases of treatment. Yet, because we do not know where grandchildren were in terms of their treatment, it is difficult to precisely specify the nature of treatment’s impact on grandparents. Clearly, the present study’s findings regarding the nature of child mental healthcare warrant cross-validation with other samples of grandchildren and their grandparent caregivers. A more intensive look into the impact over time of the child progressing through therapy on grandparents is also warranted.
The present findings mirror work suggesting that parenting children who are experiencing physical, social, or psychological difficulties is more challenging and that raising such children is associated with personal distress among birth parents, even if such children are receiving professional help in coping with such problems (Boyden et al., 2022; Jin et al., 2021; Mastorakos et al., 2021; Patel et al., 2022; Selles et al., 2018).
These novel findings lay the groundwork for the implementation of programs and interventions targeting the development of personal resilience and social support as coping mechanisms to deal with the demands of raising a distressed grandchild, wherein one is challenged in maintaining a meaningful relationship with that child yet simultaneously having to care for oneself. Practitioners therefore should empathically stress the development of personal resilience: having a positive view of oneself and one’s coping skills, setting meaningful goals for oneself, being hopeful about the future, taking a proactive approach to solving problems, and being solution-focused rather than problem-focused (Montoro-Rodriguez et al, 2021; Hayslip et al., 2022). Likewise, these findings highlight efforts by practitioners to link grandparent caregivers to sources of both emotional and instrumental support, therefore avoiding isolation from others and poorer physical and mental health borne of a lack of self-care.
Footnotes
Disposition editor:
Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.