
Abstract
This study examined the relationship between the timing of childhood maltreatment and depression and anxiety in adolescents. Using prospective data from 867 children and their caregivers from the Longitudinal Study of Child Abuse and Neglect (LONGSCAN), the effects of early childhood maltreatment (ages 0–5.99) and middle childhood maltreatment (ages 6–11.99) on depression and anxiety at age 16 were compared. Early childhood and middle childhood maltreatment were measured in three ways, including latent class analysis. Findings from multiple regression analysis revealed that only early childhood maltreatment significantly increased adolescents’ depression and anxiety, even after controlling for multiple covariates such as negative life events, social support, and caregiver depression. Strategies to improve early childhood maltreatment prevention and reduce adolescents’ depression/anxiety are also discussed.
Keywords
Depression and anxiety disorders are among the leading causes of global health burden (COVID-19 Mental Disorders Collaborators, 2021), and these two disorders and their symptoms are highly comorbid (Kalin, 2020). Depression and anxiety disorders commonly begin during adolescence, although anxiety disorders often precede depressive disorders (Kalin, 2020). Evidence suggests that depression and anxiety disorders share genetic and nongenetic risk factors, including early-life adversities (Kalin, 2020) such as child maltreatment (Li et al., 2015). Despite the well-established relationship between childhood maltreatment and late-life depression and anxiety (Baldwin et al., 2023), findings on the specific timing of childhood maltreatment before adolescence or adulthood that has the most negative effect on later-life depression and anxiety are mixed (Duggal et al., 2001; Dunn et al., 2013; Harpur et al., 2015; Keiley et al., 2001; Li et al., 2022; Mueller-Pfeiffer et al., 2013).
Some studies suggest that early childhood is a critical period for later-life depression and anxiety, whereas others report that childhood maltreatment in middle childhood is more detrimental (Li et al., 2022). The early years of life form the foundation of emotional regulation, self-concept, and brain development, and disruption in this period has a lifelong impact (Cicchetti, 1989; Lynch & Cicchetti, 1991). However, when children are older and have greater cognitive capacity, the negative effect of maltreatment is maximized, as they can conceptualize the meaning of their experiences (Russotti et al., 2021).
Depression and anxiety that emerge in adolescence tend to become chronic and severe in adulthood (Kessler et al., 2001) with long-term adverse consequences such as poor physical health and poverty (LeMoult et al., 2020). This highlights the need to understand the relationship between the timing of childhood maltreatment and adolescent depression and anxiety to develop effective prevention strategies. However, there are insufficient studies to draw unequivocal conclusions about the timing of childhood maltreatment and adolescent depression and anxiety. The majority of existing studies on childhood maltreatment and adolescents’ depression and anxiety do not differentiate between the timing of maltreatment, specifically early and middle childhood maltreatment (As-Sanie et al., 2014; Blanchard et al., 2002; Courtney et al., 2008; Haapasalo & Virtanen, 1999; Lee et al., 2012). In addition, there are more retrospective studies relying on self-reported and memory-based accounts of childhood maltreatment than prospective studies (Li et al., 2022). Fewer studies have also paid attention to neglect and emotional abuse compared to physical and sexual abuse when examining the impact of childhood maltreatment on later-life depression and anxiety (Li et al., 2022). In this context, this study aims to fill the gaps in previous research, attributable to the methodological limitations, and compare the impact of early childhood maltreatment (ages 0–5.99) and middle childhood maltreatment (ages 6–11.99) on depression and anxiety in late childhood or adolescence (age 16). Furthermore, this study tries to consider the occurrence of multiple types of childhood maltreatment in addition to the timing, using prospectively collected data.
Timing of Childhood Maltreatment and Later-Life Depression and Anxiety
The limited number of studies on the timing of childhood maltreatment and its psychological outcomes present different perspectives and empirical findings. Some researchers underscore the importance of early childhood experiences. Infancy marks the period when children develop attachments with caregivers, laying the foundation for self-worth and trust in others (Lynch & Cicchetti, 1991). Between ages 2 and 7, self-esteem and a sense of control over oneself and the environment develop, and any disruptions during this phase can have severe long-term effects (Cicchetti, 1989). Kaplow and Widom (2007) found that early maltreatment predicted more symptoms of anxiety and depression in adulthood, even when controlling for abuse reports after early childhood. Keiley et al. (2001) similarly reported that physical abuse in early childhood (ages 0–5) predicted more internalizing problems in early adolescence compared to abuse occurring later (after age 5). Dunn et al. (2013) highlighted the critical nature of early childhood, showing that for sexual abuse, the first occurrence during infancy (ages 0–2) had the greatest impact on depression at age 18, while for physical abuse, the first occurrence during preschool (ages 3–5) had the greatest impact. G. W. Brown et al. (2013) found that experiencing maltreatment by age 8 was associated with chronic depression in adulthood. These studies suggest that attachments and brain development in early years establish the foundation for cognitive functioning and emotion regulation. Disruption in socio-emotional development and changes in brain structure may impede recovery from chronic depression in adulthood (G. W. Brown et al., 2013; Kaplow & Widom, 2007; Lynch & Cicchetti, 1991).
However, childhood maltreatment can be more detrimental for older children because they have greater cognitive capacity to conceptualize their adverse experiences (Russotti et al., 2021). Empirical findings suggest that the effect of early childhood maltreatment is not necessarily greater than that of maltreatment occurring in other childhood periods. For instance, Duggal et al. (2001) found that early childhood maltreatment (up to 64 months) had no significant effect on adolescent depression (around ages 16–17 years), with only an immediate effect observed on depression around children’s first to third grades. Similarly, Harpur et al. (2015) found that depressive symptoms at age 14 were directly predicted by maltreatment at ages 10 to 12, but not by earlier maltreatment at ages 0 to 4 or 6 to 8, despite maltreatment at ages 10 to 12 being associated with earlier childhood maltreatment. In a prospective study, Huang et al. (2021) found that physical punishment at age 5 only indirectly increased depressive symptoms at age 15 through bullying victimization at age 9. Other studies have reported no significant effects of maltreatment in early childhood, middle childhood, or adolescence on adulthood depression (Mueller-Pfeiffer et al., 2013).
In a recent meta-analysis on the timing of childhood maltreatment and depression, Li et al. (2022) analyzed 58 studies and found that childhood maltreatment during middle childhood (ages 6–13) explained depression the most. However, the authors noted that the majority of the sample studies were retrospective and there was a lack of studies on early childhood maltreatment between the ages of 0 and 6 years. With a retrospective design, it is challenging to ensure that child maltreatment incidents occurred prior to the appearance of developmental outcomes. Unlike those without symptoms, adolescents with symptoms of depression and anxiety may perceive their childhood experiences as maltreatment. However, in a prospective study, early and middle childhood maltreatment was measured chronologically first, followed by adolescents’ depression and anxiety. Ensuring the time order between child maltreatment and the outcome helps strengthen confidence in the findings of the causal relationship between childhood maltreatment timing and adolescent outcomes (Fitton et al., 2020; Shadish et al., 2002).
Factors Associated with the Development of Depression and Anxiety among Adolescents
Depression is multifactorial in that a variety of biological and environmental factors play a role. Several individual, familial, and social factors are interconnected, resulting in the development of depression and anxiety among adolescents (Carson et al., 1997; Lu, 2019).
Studies have reported that female adolescents are likely to have higher depression/anxiety levels, both in the general population (Lu, 2019) and among those experiencing child maltreatment (Godinet et al., 2014). Female adolescents are at three times higher risk of major depressive episodes than their male counterparts (Lu, 2019). Among boys with early childhood maltreatment, the negative impact on internalizing problems during ages 0 to 4 faded over time; for maltreated girls, the negative impact during ages 0 to 4 became more pronounced around adolescence (Godinet et al., 2014). This may be because of hormonal changes during puberty or the disadvantaged social status of female adolescents, which leads to increased exposure to stress and poorer mental health (Adkins et al., 2009). Findings on race/ethnicity and adolescent depression and anxiety are mixed (Daly, 2022; Lu, 2019). However, similar to gender discrepancies in social status, ethnic minorities may face more disadvantages and stress and have poorer mental health (Adkins et al., 2009). In addition, minorities have access to fewer resources to address mental health problems (J. S. Brown et al., 2007).
Multiple familial factors can affect depression and anxiety in adolescents. Families’ low socioeconomic status (SES), such as caregivers’ income and education (Adkins et al., 2009; Shore et al., 2018), and single parenthood (Lu, 2019) were among the risk factors. Similar to gender and race/ethnicity, the disadvantaged social location of adolescents with low SES and single parenthood can increase stress exposure and vulnerability, and as psychological responses, depression and anxiety can develop (Adkins et al., 2009). Single parenthood due to divorce, separation, or partner incarceration can also be considered a part of adverse childhood experiences (ACEs), which are known risk factors for long-term mental health problems, including depression/anxiety (Elmore & Crouch, 2020; Felitti et al., 1998).
Other ACEs that are risk factors for depression/anxiety include childhood maltreatment and family dysfunction, such as mental illness, substance abuse, and domestic violence (Felitti et al., 1998). Both the accumulated ACEs and different categories of ACEs are associated with depression and anxiety (Elmore & Crouch, 2020). The relationship between caregiver depression and adolescent depression is well-established in previous research (Sanders et al., 2005). When caregivers experience depression, it can be genetically inherited by adolescents. Adolescents can also be exposed to negative affect and behaviors directly from caregivers as well as more stressful environments such as caregivers’ marital discord or family poverty (Goodman & Gotlib, 1999). Caregivers’ substance use is also considered an ACE that increases the risk of depression and anxiety. Caregivers’ dependence on substances can diminish parenting capabilities, such as caring for basic needs and interacting with children with responsiveness and warmth (Carson et al., 1997; Miller et al., 2014; Restifo & Bögels, 2009; Yap et al., 2014). When adolescents are treated with inconsistent and indifferent attitudes from caregivers and are expected to take over their parents’ role instead of their caregivers, it can lead to more stress and make them vulnerable to depression and anxiety (Miller et al., 2014).
Negative life events are risk factors for depression and anxiety. Among negative life events, child abuse, domestic violence, and the death of family members significantly predicted higher levels of depression among children and adolescents (LeMoult et al., 2020). Negative life events related to peer relations and family circumstances are especially important sources of psychological distress (Kim, 2021). For adolescents with childhood maltreatment, additional victimization can exacerbate the negative outcomes of childhood maltreatment (Carson et al., 1997).
Perceived social support from familial and nonfamilial adults or peers can play a protective role in both the general population and victimized adolescents (Rueger et al., 2016; Scardera et al., 2020). Social support can reduce depression by improving self-worth. It can also mitigate the negative effects of adverse life experiences on depression by providing hope for controlling these experiences and ensuring that they do not blame themselves for the occurrence of negative events. Social support may occur in school or community settings as well as in families through individuals, including parents, relatives, teachers, and peers (Carson et al., 1997; Rueger et al., 2016).
The magnitude of the relationship between social support and depression varies according to the source of support. The association between support from family members and depression among adolescents with child maltreatment experiences was relatively weak in the meta-analysis. This might imply that when adolescents and their support source share stressors, as in child maltreatment, the quality of social support is compromised, and support outside the family might be more important for the victims (Rueger et al., 2016).
Limitations of Previous Studies
Although previous studies have contributed to a better understanding of childhood maltreatment and its long-term effects on depression and anxiety, they have some limitations. First, as mentioned earlier, many existing studies were retrospective (Lee et al., 2012). When they defined childhood maltreatment that occurred before adolescence, typically around the age of 12 to 15 years, they did not differentiate early childhood maltreatment from middle childhood maltreatment (As-Sanie et al., 2014; Blanchard et al., 2002; Courtney et al., 2008; Haapasalo & Virtanen, 1999; Lee et al., 2012). Retrospective studies depend on the participants’ recall of childhood maltreatment, making it challenging to specify the exact timing, especially when it occurs during the earlier years of life. Conducting prospective studies over a long period is not easy. However, the timing of child maltreatment can be specified, and the time order of child maltreatment incidents and the appearance of the outcome can be ensured. This makes prospective studies more useful for exploring the causal relationship between the timing of childhood maltreatment and depression and anxiety among adolescents. However, in retrospective studies, adolescents’ reports of early and middle childhood maltreatment based on memory can be biased, and the time order of child maltreatment incidents and adolescents’ depression/anxiety is not ensured, which makes it more difficult to reveal causal relationships (Fitton et al., 2020; Shadish et al., 2002).
Second, previous research has focused on the impact of physical and sexual abuse, whereas research on emotional maltreatment and neglect is lacking (As-Sanie et al., 2014; Blanchard et al., 2002). However, to fully understand the consequences of maltreatment, it is necessary to consider multiple dimensions, including the subtype and timing. In reality, victims often experience multiple types simultaneously, and considering the complexities of maltreatment, researchers recommend moving from a focus on a single maltreatment type and its impact to capturing real-life experiences (Rivera et al., 2018; Warmingham et al., 2019). In recent years, latent class analysis (LCA), a person-centered approach, has been widely used as it moves from examining the relationships among variables to identifying subgroups of individuals considering multiple variables simultaneously (Rivera et al., 2018). In other words, the LCA enabled us to identify subgroups of children with different combinations of the four maltreatment subtypes. It can inform us of victims’ real-life experiences with co-occurring maltreatment subtypes. Only a few studies have used LCA to examine the consequences of child maltreatment (Warmingham et al., 2019). LCA, a person-centered approach, should be used to examine the impact of multidimensional child maltreatment experiences on adolescents’ depression and anxiety.
Third, although previous studies have tried to control for factors related to the development of adolescent depression among victims of childhood maltreatment (Dunn et al., 2013; Godinet et al., 2014; Harpur et al., 2015), more risk and protective factors can be considered. Since familial or social environments can affect depression/anxiety, moderating or exacerbating the consequences of childhood maltreatment, the occurrence of additional child maltreatment after childhood, family dynamics, and the social context of victims must be considered to fully understand the impact of childhood maltreatment on adolescents’ depression and anxiety (Carson et al., 1997). Having more covariates will help strengthen the validity of the causal relationship when examining the relationship between maltreatment timing and adolescent depression/anxiety (Shadish et al., 2002).
Fourth, the timing of childhood maltreatment must be differentiated from its onset at a certain period. Some studies have used onset interchangeably with timing (Dunn et al., 2013). However, as maltreatment can be either chronic or episodic after onset, depending on its recurrence, more specific information on onset and duration is needed when examining the impact of child maltreatment timing on adolescents’ depression/anxiety.
This study attempts to fill the gaps in previous studies and contribute to the understanding of the timing of childhood maltreatment and its impact on adolescents’ depression and anxiety. Specifically, this study uses prospective data from the Longitudinal Study of Child Abuse and Neglect (LONGSCAN) and considers both the specific timing and types of maltreatment by utilizing LCA. In addition, the analysis will control for maltreatment occurring after childhood, as well as other familial and social risk factors for adolescents’ depression and anxiety.
Method
Participants
This study used secondary data from LONGSCAN, a consortium consisting of five independent prospective studies conducted at different sites that shared the same methodology for data collection through the Coordinating Center except for participants’ recruitment criteria (LONGSCAN Coordinating Center, 2014). The studies recruited children aged 0 to 4 years at various risk levels of childhood maltreatment and followed them for up to 18 years at regularly scheduled intervals (every 2 years) to investigate the antecedents and consequences of child maltreatment based on the ecological-developmental theory. LONGSCAN is useful for exploring the long-term consequences of child maltreatment due to its longitudinal design and data on children, maltreatment experiences, and environments with at-risk children. It tried to incorporate various protective and risk factors, developmental outcomes, and different dimensions of child maltreatment, including timing, duration, and subtype.
LONGSCAN’s five sites include urban, suburban, and rural areas. All research procedures, including child and caregiver interview protocols, were approved by local institutional review boards (IBRs) and the IRB of the coordinating center. Caregivers and children were contacted to collect data on children and their environments. Caregivers provided informed consent while children provided assent from age 8 through 16 for their participation in interviews (Kaferly et al., 2020). Child Protective Services (CPS) records and written teacher reports on child outcomes are also data sources (LONGSCAN Coordinating Center, 2014). This study used data from the children, caregivers, and CPS records.
The samples differed across five sites, including children with various risk statuses and levels of exposure to maltreatment (LONGSCAN Coordinating Center, 2014). Low-income families were recruited from primary health care clinics in the East (EA) site. One-third were CPS-reported, and among non-CPS-reported children, half were at risk, and half were controls. At the Midwest (MW) site, the CPS recruited young children and matched non-CPS controls. Among the CPS-reported children, half received comprehensive services, and half received only CPS interventions. At the Northwest (NW) site, all children in the sample were reported to have CPS by age 5 but were divided into substantiated and unsubstantiated. At the South (SO) site, among high-risk infants, CPS-reported and nonreported children were recruited by matching with a 1:2 ratio at age 4 (LONGSCAN Coordinating Center, 1998). Children with out-of-home placement with a relative or foster family due to maltreatment were recruited from the Southwest (SW) site. By the age of 4, one-third of them returned home, and one-fifth were adopted. Whether they remained in foster care, returned to their families, or were adopted, LONGSCAN followed them up to the age of 18 (Runyan et al., 1998). Among the 1,354 children who participated in LONGSCAN at baseline, those who participated in interviews at age 16 and responded to the outcome variable of depression were included in the final study sample. The final sample included 867 children and their caregivers. The dropout participants were not significantly different from the final sample of this study regarding maltreatment experiences or other variables.
Variables
Dependent Variable
Depression/anxiety was measured by caregivers using the Child Behavior Checklist (CBCL) at age 16. Caregivers were asked to report their children’s symptoms in the last 6 months (LONGSCAN Coordinating Center, 2010). The CBCL is widely used to measure emotional and behavioral problems (Éthier et al., 2004; Shaffer et al., 2008) and has established reliability and predictive validity (Achenbach, 1991). The CBCL has two broad groups of syndromes (externalizing and internalizing scales) comprising eight constructs: social withdrawal, somatic complaints, aggressive behavior, and anxiety/depression. The current study used 14 anxiety/depression items, and Cronbach’s α for reliability was .87. Each item had three categories (0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true). T-scores based on the children’s gender and age were used in the analysis.
Independent Variable
The timing of childhood maltreatment was measured in three ways. First, early childhood maltreatment from ages 0 to 5.99 and middle childhood maltreatment from ages 6 to 11.99 were measured as the number of CPS allegations. Second, for early and middle childhood maltreatment, the number of CPS allegations was counted, respectively, for 2-year intervals. For early childhood maltreatment, childhood maltreatment allegations were measured at ages 0–1.99, 2–3.99, and 4–5.99. For middle childhood maltreatment, childhood maltreatment allegations were measured at ages 6–7.99, 8–9.99, and 10–11.99. Third, for early and middle childhood maltreatment, four types of allegations (physical, sexual, emotional maltreatment, and neglect) were measured (yes = 1, no = 0) for each of the three 2-year intervals. Accordingly, for early childhood, 12 indicators were created to measure the four types of allegations for each of the three intervals: 0 to 1.99, 2 to 3.99, and 4 to 5.99. For middle childhood, 12 indicators were created to measure the four types of allegations for each of the three intervals: 6 to 7.99, 8 to 9.99, and 10 to 11.99.
In LONGSCAN, trained observers at five sites reviewed CPS records regularly (every 2 years) and collected information about child maltreatment. They categorized allegations into subtypes according to a modified version of the Maltreatment Classification Scheme (Barnett et al., 1993) and specified the timing. More details of the review process are described in previous studies (English et al., 2005). This study used any alleged CPS reports as child maltreatment, regardless of the substantiation status, based on the findings of previous studies. Earlier research on LONGSCAN participants found similar developmental and behavioral outcomes among children with substantiated and unsubstantiated CPS reports (Dubowitz et al., 2016; Hussey et al., 2005). Other researchers also suggested that it is not useful to make a distinction between unsubstantiated and substantiated reports (Drake, 1996; Dubowitz et al., 2016; Kohl et al., 2009; Leiter et al., 1994; Palmer et al., 2021).
Covariates
Negative life events included childhood maltreatment and victimization by peers after the age of 12 years and witnessing violence against familial and nonfamilial members by the age of 14 years. Childhood maltreatment after age 12 (12–16) was measured as the total number of CPS allegations based on CPS records. Peer victimization was measured using one item: “Since you turned 12, about how often did any kids pick on you by chasing you, trying to scare you, threatening you, grabbing your hair or clothes or forcing you to go somewhere, or do something, you did not want to do?” (0 = never, 1 = 1 time, 2 = 2–3 times, and 3 = four or more times). Witnessing violence on family members and nonfamily members was measured using the same eight items from the History of Witnessed Violence Scale. The items included the total number of times the participant witnessed eight types of violence against family or nonfamily members in their lives, including someone being arrested, slapped/hit, shot, stabbed, killed, raped, a gun being pulled on someone, or a knife being pulled on someone (0 = never, 1 = once, 2 = 2–3 times, and 3 = more than 3 times). The Cronbach’s α of the eight items was 0.54 for family members and 0.75 for nonfamily members, and the scores ranged from 0 to 24, respectively.
Social support included the friendliness of peers and having adults to go to for help. Friendliness of peers at school was measured with one item, “How many of the other kids at school are friendly toward you?” (4 = almost all, 3 = most, 2 = about half, and 1 = almost no one). Having adults to go to for help was measured with four items: “Is there an adult (or adults) you can turn to for help if you have a serious problem?,” “Could you go to a parent or someone who is like a parent, with a serious problem?,” “Could you go to another relative (not a parent), with a serious problem?,” “Could you go to another adult (not a relative) with a serious problem?,” and “Has there ever been an adult outside of your family who has encouraged you and believed in you?” (yes = 1, no = 0). The total score was used in the analysis, and the scores ranged from 0 to 5.
Caregiver depression was measured at 16 years of age using the Center for Epidemiologic Studies Depression Scale (CES-D). The CES-D consists of 20 Likert-type items that reflect dimensions of depression (0 = rarely or none to 3 = most or all the time). The Cronbach’s α of the 20 items was 0.90, and the scores ranged from 0 to 60.
Other covariates included family income (1 = less than $5,000 per year, 2 = $5,000–$10,000 to 11 = more than $50,000), caregiver education (high school or above = 1, less than high school = 0), five dummy variables for sites (EA, MW, NW, SO, and SW), caregiver marital status (married = 1, not married = 0), three dummy variables for child race/ethnicity (White, Black, and others), and child sex (female = 1, male = 0), other category of race/ethnicity included Hispanic and other minorities.
Analysis
First, a LCA was conducted to identify subgroups of victims of childhood maltreatment during early and middle childhood. LCA is useful in identifying unobserved subgroups of individuals by classifying them using observed indicators (Lazarsfeld & Henry, 1968). To identify subgroups of victims with early childhood maltreatment experiences, 12 indicators were used: four types of allegations (physical, sexual, emotional maltreatment, and neglect) for each of the three 2-year intervals (0–1.99, 2–3.99, and 4–5.99). To identify subgroups of victims with middle childhood maltreatment experiences, the same 12 indicators were used: four types of allegations (physical, sexual, emotional maltreatment, and neglect) for each of the three 2-year intervals (6–7.99, 8–9.99, and 10–11.99). These indicators had no missing values; therefore, 867 children in the sample were used for the LCA.
Multiple model fit indicators were used to determine the number of subgroups that best fit the data (Nylund-Gibson & Choi, 2018), including the Bayesian Information Criterion (BIC), adjusted BIC, Akaike Information Criterion (AIC), Vuong-Lo-Mendell-Rubin likelihood-ratio test (VLMR LRT), Lo-Mendell-Rubin adjusted likelihood-ratio test (LMR A-LRT), and entropy. Smaller values of the BIC, adjusted BIC and AIC indicated a better model fit. The VLMR LRT or LMR A-LRT estimates the log-likelihood difference distribution to obtain p-values, indicating if the k − 1 class model should be rejected or not against the k class model. The p-values of VLMR LRT and LMR A-LRT <.05 indicate that the k class model fits data significantly better than the k − 1 class model, so the k − 1 class model is rejected in favor of the k class model. The p-values of VLMR LRT and LMR A-LRT >.05 indicate that the k class model fits data no better than the k − 1 class model. An entropy closer to 1 indicates a better model fit (Nylund-Gibson & Choi, 2018; Yampolskaya et al., 2014).
After identifying subgroups of childhood maltreatment victims during early and middle childhood, descriptive analysis was conducted to examine the overall sample characteristics regarding the dependent, independent, and control variables. Finally, a multiple regression analysis was conducted to examine whether early or middle childhood maltreatment predicted depression in adolescents. Multicollinearity was checked through the variance inflation factor (VIF) and no concern was found. Other assumptions of multivariate regression analysis, such as the independence of errors, normality of errors, and homoscedasticity of variance, were also checked and satisfied. Prior to multiple regression, multiple imputation was used to handle missing data for some variables, ensuring that all observations in the sample could be used for the regression analysis (Yuan, 2011). Ten imputed datasets were used to produce the parameter estimates.
Results
In the LCA, the LRT results supported four classes of early childhood maltreatment (see Table 1) and three classes of middle childhood maltreatment (see Table 2) because the p-values of the LRT results on the five-class model of early childhood maltreatment and the four-class model of middle childhood maltreatment were >.05. While not all other model fit indicators aligned with the LRT results, it is common for multiple fit indices not to converge on a single model (Nylund-Gibson & Choi, 2018). Class models were selected based on class size, interpretability, and fit indices.
Model Fit Indices by the Number of Classes for Early Childhood Maltreatment.
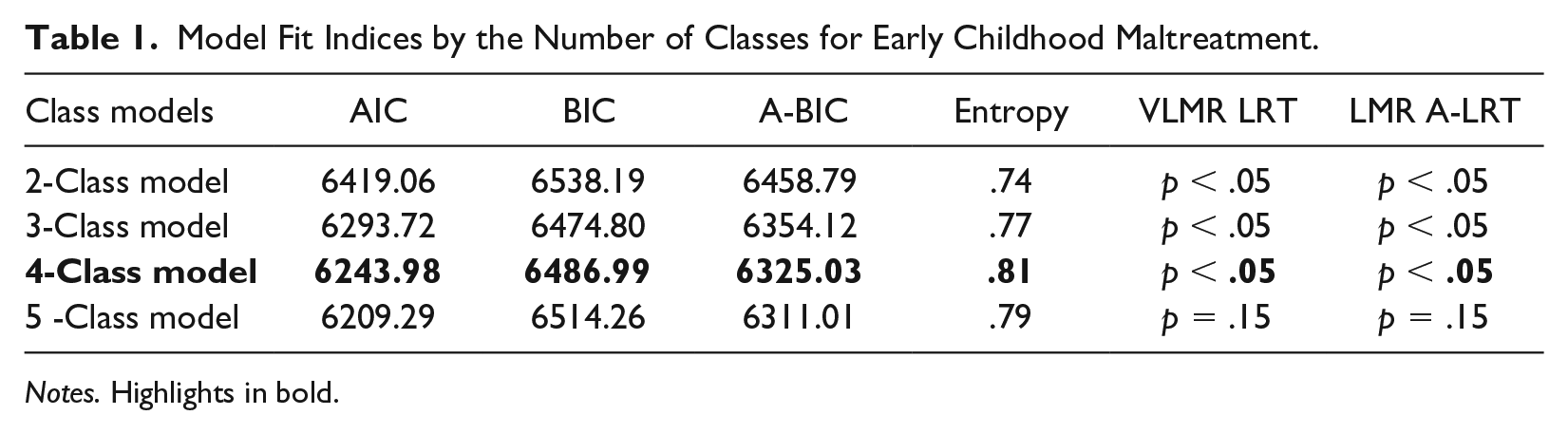
Notes. Highlights in bold.
Model Fit Indices by the Number of Classes for Middle Childhood Maltreatment.
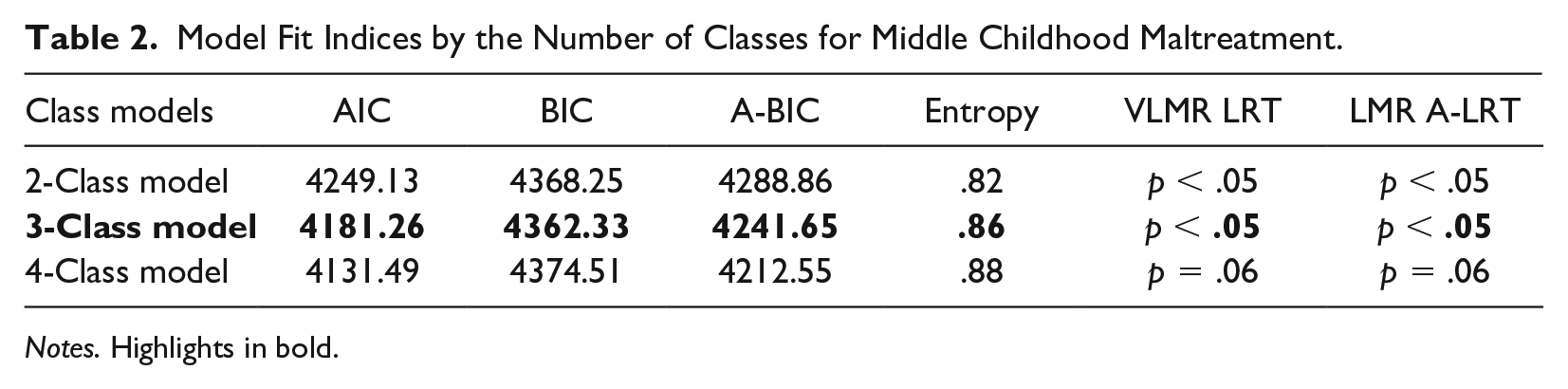
Notes. Highlights in bold.
The item probabilities in Tables 3 and 4 indicate the probability that children in a given class experienced a particular maltreatment subtype during a specified period (Yampolskaya et al., 2014). Regarding early childhood maltreatment subgroups, as shown in Table 3, Class 1 is a group in which children had a high probability of experiencing neglect (87%) and emotional maltreatment (66%) at ages 0 to 1.99. In Class 2, children had a high probability of experiencing neglect (77%) at ages 4 to 5.99. Class 3 represents a group in which it is likely that children did not experience maltreatment. Class 4 is a group in which children have a mid-to-high probability of experiencing physical abuse (54%), neglect (72%), and emotional maltreatment (54%) at ages 2 to 3.99.
Item Probabilities by Class for Early Childhood Maltreatment (N = 867).

n=125. bn=129. cn=564. dn=49.
Notes. Highlights in bold.
Item Probability by Class for Middle Childhood Maltreatment (N = 867).
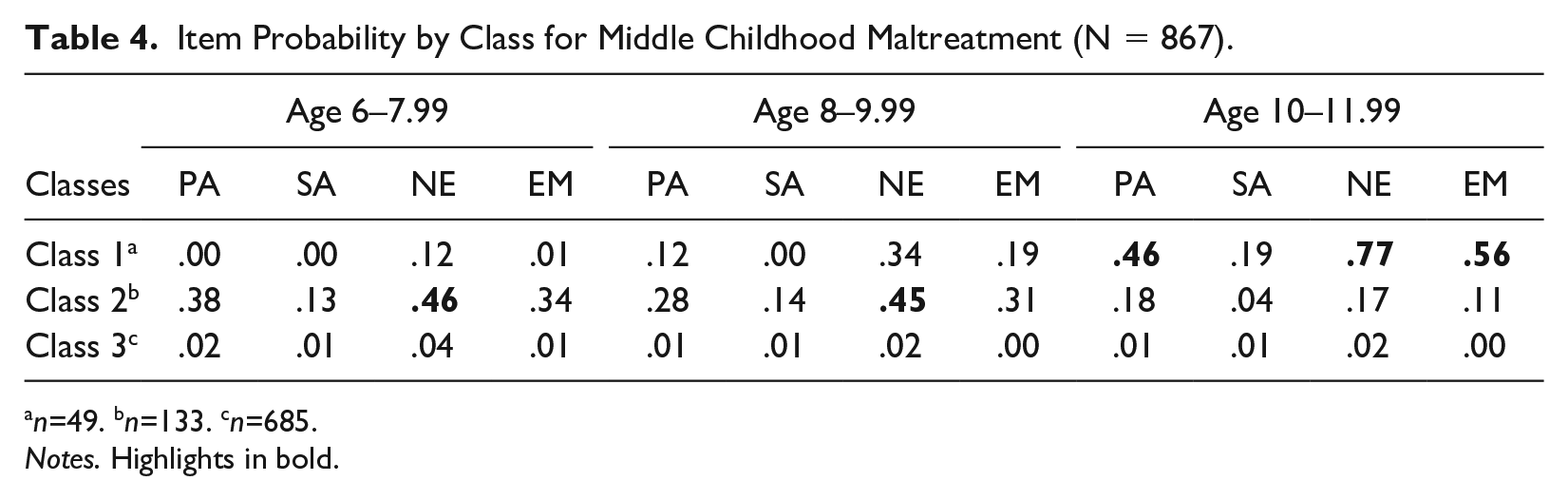
n=49. bn=133. cn=685.
Notes. Highlights in bold.
Regarding middle childhood maltreatment subgroups, as shown in Table 4, Class 1 is a group in which children had a mid-to-high probability of experiencing neglect (77%) and emotional maltreatment (56%) at ages 10 to 11.99. Class 2 is a group in which children had a moderate probability of experiencing neglect (45%–46%) at ages 6 to 7.99 and 8 to 9.99. Class 3 represents a group in which children did not experience maltreatment.
Table 5 presents the sample characteristics of the variables used in the multivariate model. The mean T-score of adolescents’ depression/anxiety was below the clinical range of over 70. Child maltreatment was more frequent in early childhood (age 0–5.99) than in middle childhood (age 6–11.99) or adolescence (age 12–16). Table 6 shows the results of multiple regression analysis examining the relationship between childhood maltreatment and adolescent depression/anxiety. The results indicated that while early childhood maltreatment significantly predicted adolescents’ depression/anxiety, middle childhood maltreatment did not.
Descriptive Results of Sample Characteristics (N = 867).

n = 662. bn = 761. cn = 807. dn = 690. en = 759. fn = 798. gn = 865. hn = 862. in = 863. jn = 757.
Timing of Childhood Maltreatment and Adolescent Depression/Anxiety (N = 867).

p < .05. **p < .01. ***p < .001.
In Model I, childhood maltreatment during ages 0 to 5.99 increased depression/anxiety (β = 0.08, p < .05), but childhood maltreatment during ages 6 to 11.99 did not. In Model II, the number of alleged childhood maltreatment cases at ages 4 to 5.99 significantly predicted increased depression/anxiety (β = 0.21, p < .05), but other childhood maltreatment variables did not. In Model III, Class 4 of early childhood maltreatment significantly increased depression and anxiety (β = 2.27, p < .05). In Model III, Class 3 was used as a reference group for early childhood maltreatment and middle childhood maltreatment since children in these groups rarely experienced child maltreatment. In summary, among the variables related to maltreatment during early and middle childhood, only those related to childhood maltreatment were significant. In addition, in all three models, childhood maltreatment during ages 12–16 significantly predicted depression/anxiety (β = 0.55~0.58, p < .001).
Among other control variables, caregiver depression (β = 0.17, p < .001) significantly increased depression/anxiety in all three models, whereas caregiver substance use did not. Other family and caregiver characteristics, such as marital status, income, and high school degree, were not significant. On the other hand, peer victimization emerged as a significant factor in all three models (β = 0.59~0.60, p < .05) along with peer friendliness (β = −0.64 to −0.62, p < .05). Witnessing violence toward family or nonfamily members and support from adults were insignificant. Black and other (Hispanic/other) children were not significantly different from white children. Female adolescents were not significantly different from male adolescents. LONGSCAN sites were significant predictors; compared to the Southwest site, all four other sites reduced depression/anxiety (β = −2.65 to −1.60, p < .01–.05).
Discussion
This study aimed to examine the effects of childhood maltreatment during early and middle childhood on adolescent depression and anxiety. In the three multiple regression models with different measures of childhood maltreatment, only early childhood maltreatment predicted increased levels of depression and anxiety among adolescents.
First, an increase in allegations of childhood maltreatment during ages 0 to 5.99 predicted higher levels of depression compared to middle childhood maltreatment allegations. Second, when childhood maltreatment allegations were measured at 2-year intervals from ages 0 to 12, a higher occurrence of childhood maltreatment at ages 4 to 5.99 was associated with increased depression/anxiety in adolescents, while other childhood maltreatment-related variables did not show this association. Third, in the latent class model, only Class 4 was a significant predictor of depression and anxiety in early childhood. Class 4 represents a group in which children have a high probability of experiencing all four types of maltreatment at ages 2 to 3.99. In addition, the most recent childhood maltreatment allegations, which occurred between ages 12 and 16, were significant predictors in all three models with different measures of early and middle childhood maltreatment.
These findings imply that early childhood maltreatment has a long-term negative effect on adolescents’ depression and anxiety, in addition to the effects of more recent maltreatment. These findings supported that early childhood is a critical developmental period. During this period, children develop attachment to caregivers, which is the foundation of their self-concept and emotion regulation (Lynch & Cicchetti, 1991). In addition, brain development occurs rapidly, and disruption during early childhood can have long-lasting mental and physical effects (Cicchetti, 1989; Lynch & Cicchetti, 1991).
Despite the importance of early childhood, specifying the exact timing of maltreatment that has the most detrimental effect on adolescents’ depression/anxiety is challenging. Without considering maltreatment type, an increase in maltreatment allegations at ages 4 to 5.99 was found to be significant. However, when considering both maltreatment types and timing, multiple maltreatments during ages 2 to 3.99 (Class 4) were significant. This suggests that the occurrence of multiple maltreatment may result in depression/anxiety in later life, although the negative impact on depression/anxiety may not solely be attributed to the occurrence of multiple types of maltreatment.
During middle childhood, in Class 1, multiple types of maltreatment occurred at ages 10 to 11.99, but this was not a significant predictor of adolescents’ depression/anxiety. Similarly, during early childhood, in Class 1, children had a high probability of experiencing neglect and emotional maltreatment at ages 0 to 1.99, yet being in this group did not increase depression/anxiety at age 16. Thus, not only multiple types of childhood maltreatment but also the timing between ages 2 and 5.99 years might have detrimental long-term effects. Compared to infancy or early teenage years, ages 2 to 5.99 could be particularly important for psychological development, possibly due to the development of self-esteem and a sense of control over the environment and self between ages 2 and 7 (Cicchetti, 1989). With victimization during this time, children may blame themselves by attributing the maltreatment to their faults. With the inconsistent and unpredictable behaviors of caregivers, young children may feel unsafe and powerless without feeling control over the environment. In the long term, victims can develop symptoms of depression/anxiety when they reach adolescence, a period of physical change and more stressful life experiences. Compared to children aged 2 to 5.99, infants aged 0 to 1.99 may have less developed cognitive abilities to attribute maltreatment to their faults and may not pursue developmental control over the environment. However, infancy is also a critical period for the development of a secure attachment to caregivers, which is related to emotion regulation and psychological distress (Kaplow & Widom, 2007). Although a few previous studies have shown that adults with child maltreatment during preschool years have higher levels of depression and anxiety than those with infancy maltreatment (Kaplow & Widom, 2007), further studies are needed to confirm the current findings on the long-term impact of child maltreatment during infancy.
The findings of this study diverge from certain previous studies suggesting that childhood maltreatment is more detrimental for older children (Duggal et al., 2001; Harpur et al., 2015; Huang et al., 2021; Mueller-Pfeiffer et al., 2013), who are better able to comprehend and interpret their experiences (Russotti et al., 2021). While childhood maltreatment between ages 12 and 16 was associated with depression/anxiety at age 16, middle childhood maltreatment did not significantly predict these outcomes, unlike early childhood maltreatment. This discrepancy could stem from LONGSCAN’s recruitment criteria, which targeted children at risk of or exposed to early childhood maltreatment, potentially resulting in less frequent and severe maltreatment experiences in middle childhood. In addition, certain covariates, such as substance use or witnessing violence, were more closely associated with middle childhood maltreatment. Substance use was measured at age 8, and adolescents’ self-reports of lifetime violence exposure might overlook experiences from early childhood due to limited memory. Another possibility is that early childhood is more developmentally critical than middle childhood.
In this study, child maltreatment was measured using CPS records. With self-reported data on early and middle childhood maltreatment experiences, findings on the relationship between childhood maltreatment timing and depression and anxiety may differ. As self-reported child maltreatment usually has a greater impact on mental health (Negriff et al., 2017), and it is easier to recall middle childhood memories than early childhood memories, the relationship may change.
Peer victimization after age 12 and child maltreatment between ages 12 and 16 significantly increased adolescents’ depression and anxiety at age 16. Victimization by peers or caregivers is considered a negative life event and a known risk factor for negative mental health outcomes (LeMoult et al., 2020). Witnessing violence against family members is also considered a negative life event (LeMoult et al., 2020) but was insignificant in this study. Items to measure violence against family members in this study included severe incidents, such as being arrested, shot, stabbed, killed, and a gun being pulled, and the mean frequency was low overall. Items including psychological aggression and minor physical violence may have produced different results. Witnessing violence against nonfamily members also included items on severe physical violence, and it had a relatively higher mean score of frequency but was not a significant predictor. The impact of negative events involving nonfamily members may depend on their relationship with them or their perception of events rather than merely on the number of events. Further studies with different measures of witnessing violence are needed to confirm our findings.
Caregivers’ substance abuse was not significant, and it might be that a one-item measurement at the age of 8 years was not sufficient to collect data on adverse familial experiences associated with adolescents’ mental health. Caregiver depression was a consistently significant predictor, aligning with previous studies reporting the negative impact of caregivers’ mental health, including depression, on children’s behavioral issues (Carson et al., 1997; Du & Kim, 2020). Depressed caregivers can exhibit more negative behaviors or affect their children, resulting in depression in adolescents. In addition, as adolescent depression and anxiety were reported by caregivers in this study, caregivers’ depression may have influenced the way they viewed their children’s behavior.
Peer friendliness was significantly associated with decreases in depression and anxiety, whereas support from adults was not. Perceived support from peers is a known protective factor against depression and anxiety in adolescents (Carson et al., 1997; Rueger et al., 2016). Adult support is also a protective factor, but for adolescents with child maltreatment experiences, support from outside family members can be more important (Rueger et al., 2016). The current sample included those at various risk levels for childhood maltreatment; however, the social support items asked about support from both familial and nonfamilial adults. In addition, the items to measure support from adults did not ask about the quality of support and simply asked if adolescents had adults go for help. However, different measurements may produce varying results.
Caregivers’ marital status, income, and educational level were not significant. Single parenthood, low income, and education can increase children’s stress exposure, and as a response, depression and anxiety can develop (Adkins et al., 2009). However, in this study, it is possible that as other family-related vulnerabilities such as caregiver depression, substance abuse, and violence against family members were controlled for, SES and marital status were not significant. Compared with White children, Black and other minority children did not exhibit higher levels of depression in this study, and previous studies have not yielded consistent findings regarding racial disparities in adolescent depression (Lu, 2019). Being female was also not significant, although previous studies reported higher levels of depression and anxiety among female adolescents (Godinet et al., 2014; Lu, 2019). The stress process model explains that ethnic minorities or female adolescents face more disadvantages and stress, which can lead to poor mental health (Adkins et al., 2009). In this study, it is possible that as other family-related vulnerabilities such as family dysfunction, SES, and protective factors were controlled for, ethnicity and sex were not significant. Further studies are needed to examine the effect of race/ethnicity and sex on adolescents’ depression and anxiety. Compared to the SW site, the other sites were associated with lower levels of depression. Children from the SW site were in foster care during early life, and out-of-home placement can be a risk factor for mental health problems, including depression and anxiety (Pilowsky & Wu, 2006), as it can be traumatic and lead to insecure attachment (Pilowsky & Wu, 2006).
Implications for Practice
The current findings emphasize the importance of preventing early childhood maltreatment, particularly among children aged 2 to 5.99, including the prevention of multiple instances of maltreatment. Many existing home visitation or center-based programs target young, at-risk children and their caregivers beyond the pre- and postnatal periods to prevent early childhood maltreatment. These programs aim to facilitate children’s healthy development by supporting and engaging caregivers, and they usually have a parent education component. Through skill modeling, practice, and feedback, parents learn how to discipline children appropriately, provide a safe and healthy environment, and interact positively with their children (Silovsky et al., 2023). Although these programs are generally effective in reducing child maltreatment (Chen & Chan, 2016), there is room for improvement (Silovsky et al., 2023). Since families at risk of early childhood maltreatment often face more challenges related to basic needs or behavioral problems due to poverty and drug use than those with older children (Palusci, 2011), these programs should be more flexible in addressing families’ needs beyond parental education. Strategies that target poverty, substance abuse, and unstable housing can also be beneficial (Maguire-Jack et al., 2018) as they are risk factors for early child maltreatment. Prevention programs for young children and their caregivers can become more effective when addressing the multiple challenges faced by families.
The study findings also underscore the importance of assessing and responding to the co-occurrence of multiple instances of childhood maltreatment between the ages of 2 and 5.99. CPS workers must maintain comprehensive records of the adverse experiences of young victims of maltreatment. Families with young children experiencing multiple types of maltreatment often exhibit several risk factors, as each type of maltreatment has both shared and distinct risk factors (Younas & Gutman, 2022). As such, these families should be prioritized for intervention. In addition, families experiencing a single type of maltreatment should be prevented from experiencing additional types. Practitioners need to undergo training to conduct thorough investigations and assessments to determine the current and potential future threats to children’s safety within families. They should understand the antecedents and consequences of the occurrence of multiple maltreatment and provide tailored services to meet the specific needs of each family.
Young children who have experienced maltreatment require access to mental health treatment throughout their development. Evidence suggests that mental health services for children involved in CPS are not always as effective as expected (Fong et al., 2015) and that children often have low rates of therapy completion (McPherson et al., 2012). Thus, based on comprehensive mental health screening for victimized young and older children with early childhood maltreatment experiences, those in need of mental health services should be thoroughly identified and provided with high-quality mental health services. Services should also be engaging and motivating in order to achieve high completion rates. In particular, those with early life foster care experiences need special attention from practitioners regarding mental health service needs and service receipt, whether they returned home, were adopted, or remained in foster care, as being placed out of home at an early age exposes children to the risk of insecure attachment and trauma due to separation (Pilowsky & Wu, 2006).
In addition, services for caregiver depression should be accessible and efficacious along with services for children. A more family-centered approach is needed to address adolescents’ depression and anxiety. With adolescents developing symptoms of depression and anxiety, caregivers’ mental health needs to be checked, and appropriate services need to be provided. Caregivers’ depression or mental health service receipt are important factors influencing adolescents’ depression/anxiety and the effectiveness of services for adolescents (Du & Kim, 2020; Fong et al., 2015).
Efforts to strengthen positive peer relations and prevent peer victimization are important. Evidence-based peer relation and peer victimization prevention programs should be provided based on schools or community institutions. Peer relations programs can strengthen positive peer relations by improving self-concept and mental well-being and by practicing social skills through role-plays or group tasks (Pollak et al., 2023). Effective peer victimization prevention programs can help increase conflict-resolution skills, social competencies, and help-seeking behaviors (Hoglund et al., 2012).
Limitations
Although this study contributes to a deeper understanding of the timing of child maltreatment and adolescent depression/anxiety, it has a few limitations. First, the sample consisted of at-risk children, so generalizing the findings to the general population may be limited. LONGSCAN recruited CPS-reported children, including those with a history of out-of-home placement, and matched them with low-income children. As a result, the sample characteristics and life trajectories of the children in this study may differ from those of the general population.
Second, the study did not consider the severity of childhood maltreatment, focusing instead on maltreatment type and timing. Future studies should incorporate additional dimensions of childhood maltreatment, such as severity, frequency, and chronicity. Furthermore, future studies could use adolescents’ self-reported lifetime child maltreatment when examining their mental health, as it is not always congruent with CPS reports regarding frequency and association with outcomes (Negriff et al., 2017). Third, the control variables selected may not have been comprehensive. Information on substance abuse and social support from peers is limited to this dataset. Additional ACEs or negative life events were not included in the analytical models. In addition, certain variables in this study were measured with only a single item or a few items that may have insufficiently captured the aspects of caregivers’ and children’s lives. However, compared to previous studies, this study progressed by controlling for more potential confounding variables. Despite these limitations, the findings of this prospective study contribute to current knowledge of the timing of childhood maltreatment and its association with adolescent depression. Based on these findings, efforts to prevent early childhood maltreatment should be more effectively integrated into child welfare policies and practices.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.