
Abstract
This study examines the effects of the kinship navigation program at Michigan’s Kinship Care Resource Center (KCRC) on caregivers’ depression, self-care practices, and children’s behavioral issues. This study analyzed survey data of kinship caregivers in Michigan using propensity score matching and inverse probability weighting with regression. We found that children in the care of caregivers who used KCRC had fewer behavioral issues (β = −0.281, p = .024). The effect of KCRC on self-care practice among caregivers is significant at .01 level (β = 0.309, p =.055). This study contributes to the understanding of how navigation programs for kinship caregivers affect both children and caregivers’ outcomes. It suggests expanding these programs to encompass a broader spectrum of behavioral health services for children, which could ease the caregiving load. The research also provides novel data on kinship caregivers’ self-care practices, a previously underexamined issue due to the focus on children.
Keywords
Introduction
According to the KIDS COUNT Data Center (Children in Kinship Care, 2024), about 2,426,000 children lived in kinship care arrangements in the U.S. from 2021 to 2023. In Michigan alone, the number of children who were in kinship care arrangements was 53,000 in 2022 (Michigan Department of Health & Human Services [MDHHS], 2025). Kinship care occurs when children and youth are raised by family members, including grandparents, aunts, uncles, siblings, and extended relatives (Child Welfare Information Gateway, 2025). Kinship care arrangements can be categorized as formal (within the child welfare system) or informal (outside the system). The majority of kinship caregiving arrangements are informal. Nationwide, for every child in formal kinship care arrangements, about 20 children are being raised by kin informally without the child welfare system’s oversight (Child Trends, 2025). Formal kinship caregivers (licensed relative foster parents) typically have greater access to resources and support services through child welfare agencies, whereas informal kinship caregivers often must manage with far fewer formal supports (Child Trends, 2025).
Despite the type of arrangement, kinship caregivers have widely varying needs and challenges. The most salient need/challenge of kinship caregivers is financial stress, given the cost of child care and compromised work time (Kiraly et al., 2021). Many kinship caregivers also have health needs, requiring support for physical and mental health (Burke et al., 2023; Lee et al., 2016). Although cash assistance and health insurance for eligible families who are providing kinship care under the federal poverty level are available, kinship caregivers often do not apply for these supports due to barriers such as uncertain guardianship agreements and limited knowledge of accessing health insurance (Rubin et al., 2017). As challenges and needs across a wide range of domains for kinship caregivers become more widely identified and understood, the solution to fulfill those needs becomes essential.
One key solution to the above challenges is kinship navigation programs. Available in many states of the United States, kinship navigation program has shown promising evidence of effectiveness in meeting kinship caregivers’ needs (Shao et al., 2025). In this study, a kinship navigation program is defined as a service that assists kinship caregivers in accessing resources and support to create stability for families in need and help connect caregivers with both public and private resources (Day et al., 2024).
The Family First Prevention Services Act of 2018 (FFPSA) established kinship navigator programs as a reimbursable service under Title IV-E, positioning them as a core prevention strategy within child welfare policy. Against this backdrop, states are incentivized to expand navigator services and invest in rigorous evaluation (FFPSA, 2019). From caregivers’ perspectives, those who attended kinship navigation programs (including navigator services, support groups, and caregiver training programs) were associated with improved well-being through enhanced social support and reduced caregiver burden. For example, caregivers using a support group were associated with better kinship caregivers’ social connectedness (Strozier, 2012). In addition, utilizing one-on-one navigator assistance was associated with a lower rate of caregivers’ stress-related health problems (Monahan et al., 2013). Kinship-specific parenting interventions have shown potential to strengthen caregivers’ parenting skills and their ability to manage child behaviors (Wu et al., 2020). For example, participants in the attachment and trauma-focused program “Connect for Kinship Parents” demonstrated reductions in parenting stress and use of harsh discipline, although such outcomes may vary across contexts and programs (Pasalich et al., 2021). Some kinship navigation programs also aim to empower caregivers by elevating their voices and promoting self-advocacy. The Oregon Kinship Navigator Program, for instance, incorporated caregivers’ cultural input and created opportunities for them to advocate for their own needs (Rodriguez-JenKins et al., 2021).
From the children’s perspective, children may also benefit from kinship navigation programs, although the evidence is still developing. Children in kinship care often face behavioral or emotional challenges stemming from prior adverse experiences, such as trauma or parental substance use (Xu et al., 2023). Therefore, supporting these children is a key concern for kinship caregivers, and many kinship navigator initiatives have been found to yield positive outcomes. For instance, the Kin as Teachers (KAT) 2.0 program was associated with improvements in children’s communication, motor, problem-solving, and personal-social skills, as well as greater home safety (Littlewood et al., 2023). Similarly, the Children’s Home Network Kinship Navigator Program in Florida showed improvements in protective factors such as family functioning and resilience, social-emotional support, concrete support, knowledge of child development, and nurturing and attachment (Littlewood et al., 2021). While these findings suggest potential benefits for children, results vary across programs, and additional rigorous evaluations are needed to determine the extent to which navigator programs consistently improve child well-being.
Although many positive outcomes have been observed for both caregivers and children, prior evaluations of kinship caregiver programs have also yielded mixed results. For example, Lin (2014) examined a kinship navigation program that offered mental health services but found no significant difference in caregiver stress at program completion. This finding suggested that stress is multiply determined (e.g., financial insecurity, caregiving demands, and children’s behavioral needs) and not easily shifted by short-term supports.
Similarly, Hawkins and Bland (2002) reported inconsistent effects of kinship programs on child well-being (e.g., child’s social, educational, and developmental functioning) when evaluating the Comprehensive Relative Enhancement Support and Training Project. While overall ratings were positive, kinship workers reported lower scores (7.5/10) than caregivers (8.9/10) and child welfare workers (8.7/10), highlighting inconsistencies in perceived impact. Taken together, these studies suggest that program effects vary by need and context, including the severity of children’s prior adversity and the types, intensity, and duration of supports provided.
Emerging literature indicates that racial and ethnic differences in kinship caregiving experiences and outcomes are driven largely by structural context rather than inherent group characteristics (Washington & Despard, 2024; Washington et al., 2024). African American families are disproportionately represented in kinship care and more often provide informal care, a pattern tied to long-standing responses to racial and economic oppression. In this context, caregivers face elevated structural risks such as lower income, less education, unemployment, and poorer health, which heighten stress and constrain time and resources for self-care. Moreover, because informal caregivers do not receive benefits available to formal foster placements, stress is disproportionally heightened among African American kinship caregivers (Washington & Despard, 2024; Washington et al., 2024).
From the above literature, navigator models vary widely, despite one common goal of connecting kinship families to services specified under the Family First Prevention Services Act of 2018. Some operate primarily as referral hubs (e.g., Ohio’s Kinship Care Navigator), while others, such as Oregon’s model, incorporate more intensive elements such as culturally responsive engagement, advocacy, and caregiver education. The Kinship Care Resource Center (KCRC) in Michigan offers a hybrid model providing individualized navigation assistance and direct caregiver support (training, legal assistance, and advocacy). This positioning places KCRC within the national landscape as a comprehensive program that moves beyond referral to include capacity-building for kinship families.
For this study, Family Stress Theory (McCubbin et al., 1980) provides a useful framework for understanding these challenges of kinship caregivers and the potential impact of the kinship navigation programs. According to this model, economic hardship and financial strain serve as primary stressors for low-income parents, potentially leading to increased psychological distress and reduced parenting quality (Conger et al., 1992). For example, caregivers in kinship navigation programs often started caregiving responsibilities with limited financial resources, placing them at heightened risk of material hardship (Washington & Despard, 2024). Such economic strain has been shown to exacerbate psychological distress, including symptoms of depression and anxiety, among kinship caregivers (Xu et al., 2020). The adverse effects of financial hardship can extend beyond caregivers themselves and may directly affect the developmental well-being of children in their care. Prior research indicates that caregiver anxiety and depression are associated with lower levels of children’s cognitive development (e.g., reading and math skills) as well as socio-emotional outcomes, including both internalizing and externalizing behavior problems (Harris & Santos, 2020). To address these interrelated challenges, kinship navigation programs in the theoretical framework serve as a protective mechanism. By providing financial guidance, emotional support, and linkage to community resources, such programs may buffer the negative consequences of the financial strain and mitigate both caregiver psychological distress as well as children’s behavioral difficulties (Masarik & Conger, 2017). Moreover, grounded in Family Stress Theory, we included caregiver self-care practice as a key outcome variable because it served as an adaptive coping resource in the stressor-strain adjustment pathway. Although not testing the effectiveness of self-care practice on kinship caregivers’ outcomes, prior work showed that self-care among kinship caregivers mediates the association between children’s behavioral problems and caregiver depression, significantly attenuating depression linked to child behavior (Shao et al., 2025). Therefore, we considered kinship caregivers’ self-care as a proxy of broader caregiver well-being in this study.
Current Study
For this study, we examined the effect of the Kinship Care Resource Center (KCRC), known as a kinship navigation program in Michigan, on kinship caregivers’ depression, self-care practices, and behavioral issues of their children in care. KCRC offers a comprehensive range of services to support kinship caregivers across Michigan. Through personalized assistance from trained kinship navigators, caregivers receive information and referrals to local and statewide resources including child care, legal support, financial aid, housing, and health services. KCRC also facilitates caregiver support groups to reduce isolation and foster peer connections and organizes regular trainings and workshops on topics such as parenting challenges, trauma-informed care, and navigating state systems. In addition, the center maintains an extensive online resource library covering education, legal issues, self-care, state assistance programs, and more (KCRC, 2025).
This study addressed several gaps in the existing literature. First, most existing research on kinship navigation programs focused exclusively on either children’s or caregivers’ outcomes, but not both. This study addressed this gap by examining outcomes for both kinship caregivers (depression and self-care) and the children in their care (behavioral issues). Second, although self-care is often mentioned in qualitative studies or reported as a secondary outcome, few studies have quantitatively measured kinship caregivers’ self-care practices. Drawing on Family Stress Theory, self-care can be conceptualized as a protective coping strategy that buffers the negative effects of economic strain and caregiving demands on psychological well-being. When kinship caregivers have limited time or resources for self-care, they are more likely to experience stress and burnout (Harding et al., 2018). KCRC’s navigation, information, and respite supports are designed to reduce demands and increase access to resources, thereby creating conditions that enable caregivers to engage in self-care. Finally, although kinship caregivers represent an increasingly important caregiving population, localized studies that use Michigan’s data are essential to capture the unique features and impacts of community-based navigation programs. We have made the following hypotheses: compared to those who did not use KCRC, caregivers in Michigan who used KCRC (a) would have lower levels of behavioral issues of children; (b) have lower levels of depression; and (c) engage more in self-care.
Method
Data and Sample
The potential kinship caregivers in Michigan were identified through existing administrative records and referrals from the community including self-referrals and referrals from KCRC’s service network. In addition, flyers for recruitment were widely shared in the KCRC’s social media and among its service networks. KCRC maintains an internal database of kinship caregivers who have sought services, participated in past programs, or were referred to the KCRC by partner organizations. Kinship caregivers in the database were informed and agreed to KCRC outreach. This database functions as an active case management and outreach tool, allowing KCRC to maintain updated contact information, track service provision, and identify emerging needs among caregivers. Using this record as a recruitment source ensured that invitations were extended to caregivers already connected with KCRC, increasing the appropriateness and feasibility of recruitment.
We successfully recruited 136 initial participants to join the online Qualtrics survey. Among them, 16 did not finish the survey. Ultimately, 120 surveys were completed, and a final sample of 118 unique kinship caregivers in Michigan completed the survey after 2 duplicate entries were removed. Participants were kinship caregivers residing in Michigan, and the sample included both formal and informal kinship caregivers. The survey did not explicitly ask caregivers to indicate their formal or informal status as long as they self-identified as a kinship caregiver. Caregivers’ relationships to the children in their care varied: the majority were grandparents raising grandchildren (consistent with the mean caregiver age in the mid-50s), with others being aunts, uncles, or other extended family members. Each caregiver reported on one child in their care when answering questions about child outcomes. If a caregiver was caring for multiple children, they were instructed to respond regarding a focal child (the survey did not collect data separately for each child in the household). Each participant received $25 as compensation for their involvement. This study received approval from a University Institutional Review Board for conducting research involving human subjects.
Measurement
Treatment: KCRC
The intervention under examination is the utilization of the kinship care navigator service (coded as 0 for “No” and 1 for “Yes”), which is offered by the University Kinship Care Resource Center (KCRC). This data was sourced from the administrative records of the KCRC, and it was restricted to KCRC staff only. These records enhanced internal validity and reduced self-reporting bias by confirming whether each participant had accessed any KCRC services prior to completing the survey, allowing for accurate classification into treatment and control groups. While detailed usage data (e.g., visit counts and service types) were not available, this approach provided a reliable and objective indicator of program exposure.
Control Variables
In this study, we incorporate a range of control variables, primarily about kinship caregivers’ characteristics. These variables encompass age, race, gender, education level, and income inadequacy. Race categories were defined as follows: 1 for white/Caucasian, 2 for African American. Gender was coded as 0 for Female and 1 for Male. Education level was assessed by querying the highest educational attainment, with options being 1 for high school and below, 2 for some college, and 3 for a bachelor’s degree or higher. Income inadequacy was gauged by participants’ perception of affording basic monthly living expenses, graded on a scale of 1 for “Not difficult” to 4 for “Very difficult.” In addition, participants provided information on their age in 2022 and this was treated as a continuous variable.
Outcomes
Children’s Behavioral Issues
We utilized behavioral issue indicators for children sourced from the Child Welfare Information Gateway (2025). Caregivers were asked to report whether their child exhibited five specific problems: smoking or drinking, truancy or school skipping, violent behaviors, depression (defined here as potential trauma experienced by children), and drug use. Responses were rated on a scale ranging from 1 for “Never” to 4 for “Often.” A mean score was calculated, and a composite variable was constructed based on these measures. In our sample, this five-item composite had a Cronbach’s alpha of 0.80.
Kinship Caregivers’ Depressive Symptoms
The level of depression among caregivers was assessed using items adapted from the Center for Epidemiologic Studies Depression (CES-D) scale (Radloff, 1977). Employing a 5-point Likert-type scale ranging from 1 for “Never” to 5 for “All the time,” five questions were administered to gauge the caregiver’s depressive symptoms. These questions included statements such as “I could not seem to experience any positive feelings at all,” “I found it difficult to work up the motivation to do things,” “I felt that I had nothing to look forward to,” “I felt that I wasn’t worth much as a person,” and “I was unable to become enthusiastic about anything.” Subsequently, we calculated the mean score of the summed items for use in the analysis. This short CES-D subset showed good internal consistency in our sample (Cronbach’s α = 0.81), and composite scores ranged from 1 to 5 (higher values indicate more frequent depressive symptoms).
Kinship Caregiver’s Self-Care Practice
The self-care practices perceived by caregivers were assessed using the adapted Mindful Self-Care Scale (Bellone et al., 2023). Two specific questions were chosen to evaluate caregivers’ self-care activities over the previous 12 months: “How frequently do you feel capable of taking time for yourself when necessary?” and “How often do you feel you have the opportunity to engage in activities you enjoy?” Responses to these questions were provided on a 5-point Likert-type scale, ranging from “1=Never” to “5=All the time.” An average score was calculated for this variable, with higher scores indicating better self-care practices observed by participants during the past year. Although only two items, they were significantly correlated (r = 0.65, p < .05) in this sample, justifying their combination into a single index.
Analytical Strategies
To test the effect of KCRC on kinship caregivers’ depression, self-care practice, and their children’s behavioral issues, we utilized inverse probability weighting (IPW) and regression to create a propensity score model. This way, we can compare the weighted averages of each outcome for kinship caregivers who used or did not use KCRC, removing the selection effect due to factors such as gender and race (Shiba & Kawahara, 2021). In other words, IPW helps address selection bias by creating a synthetic sample in which the distribution of covariates is independent of treatment assignment (the use of KCRC = 0 or 1). First, a propensity score was estimated using a logistic regression model with the use of KCRC and all control variables. Second, we created IPW for the use of KCRC (0 = No and 1 = Yes), using the propensity scores we just estimated. The inverse probability weights (IPW) equals: the probability of using KCRC divided by (1-probability of using KCRC). When weights are working correctly, the means of the two groups, 0 = control (not use KCRC), 1= treatment (used KCRC), on all covariates are approximately equal (the standardized differences of <10% between the means of the two groups) (Austin & Stuart, 2015). Finally, we used regression with newly created IPW and all covariates to estimate the effect of KCRC with outcomes added. For each outcome, we performed IPW regression analysis predicting caregivers’ depression, child behavioral issues, and caregivers’ self-care by the use of KCRC. All quantitative analyses were conducted using Stata (Version 17).
Findings
Descriptive Results
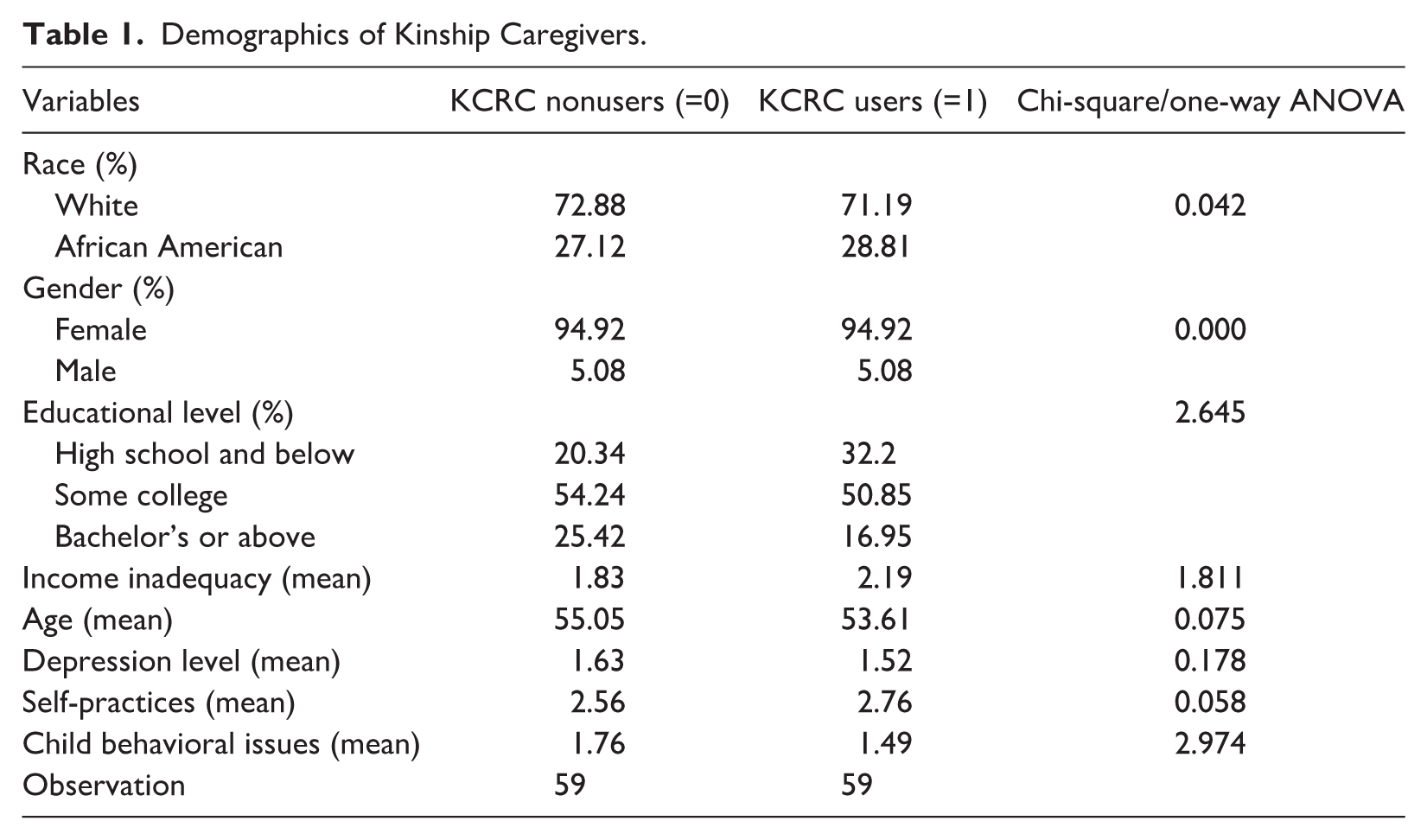
Table 1 describes the demographic information of kinship caregivers and the use of KCRC. According to Table 1, 71.19% of white and 28.81% of African American caregivers had used KCRC before. The proportion of caregivers who have not used KCRC is similar, including 72.88% of white and 27.12% of African American caregivers who have not used KCRC. Most (94.92%) of them were female caregivers. In terms of the education level of caregivers, over 50% of caregivers had some college education for both KCRC users and nonusers. Non-KCRC users had lower mean scores on income inadequacy compared to KCRC users (mean = 1.83 and 2.19) out of 5. The average age for both groups (non-KCRC users & KCRC users) is 55.05 and 53.61, respectively. To continue comparing the mean scores, KCRC users had lower scores on depression (mean = 1.52), higher scores on self-care practices (mean = 2.76), and lower scores on their children’s behavioral issues (mean = 1.49). None of the differences in demographics or baseline outcomes between KCRC users and nonusers were statistically significant (see Table 1).
Demographics of Kinship Caregivers.
IPW Results
Post-IPW adjustment, covariate balance was achieved, as indicated by Table 2. The weighted mean characteristics of KCRC users and nonusers became approximately equivalent. As a rule of thumb, standardized mean differences less than 10% indicate adequate balance, suggesting our propensity weighting succeeded in creating comparable groups (Chesnaye et al., 2021).
The IPW Results on Covariates Balance.
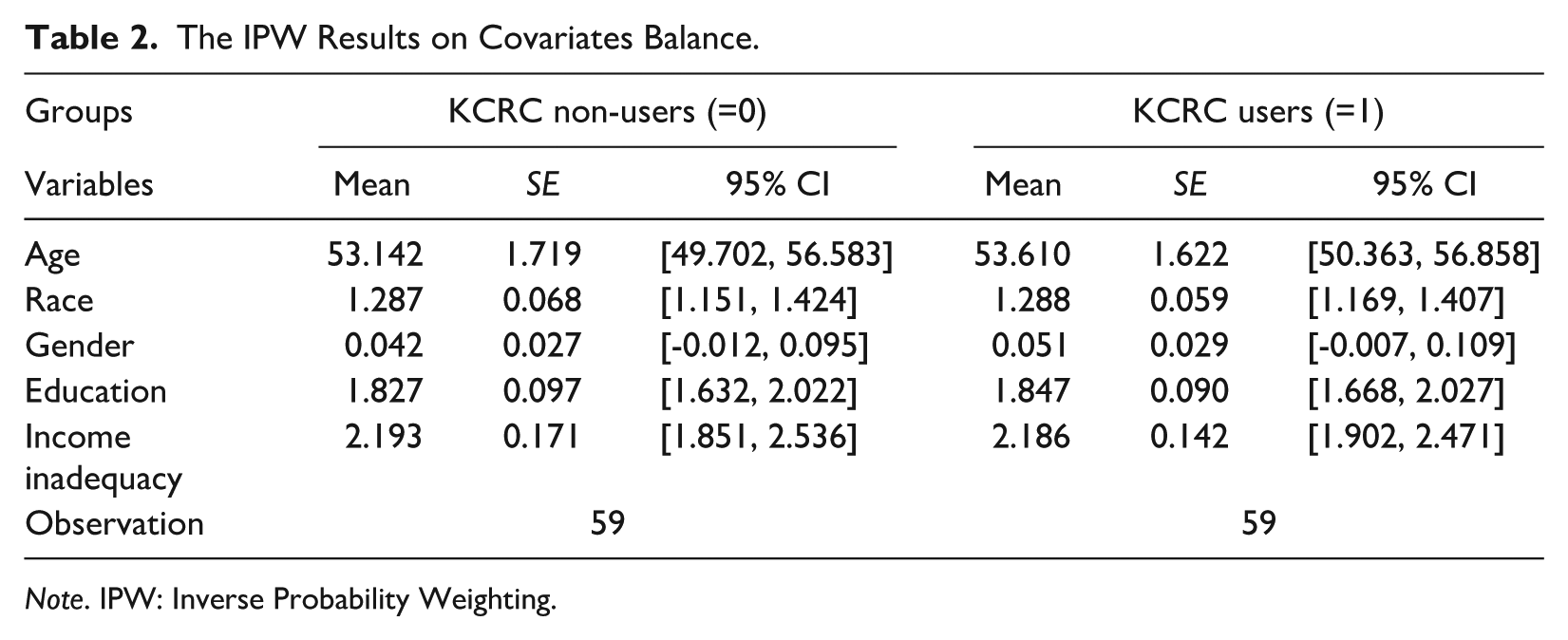
Note. IPW: Inverse Probability Weighting.
Regression Results
Children’s Behavioral Issues
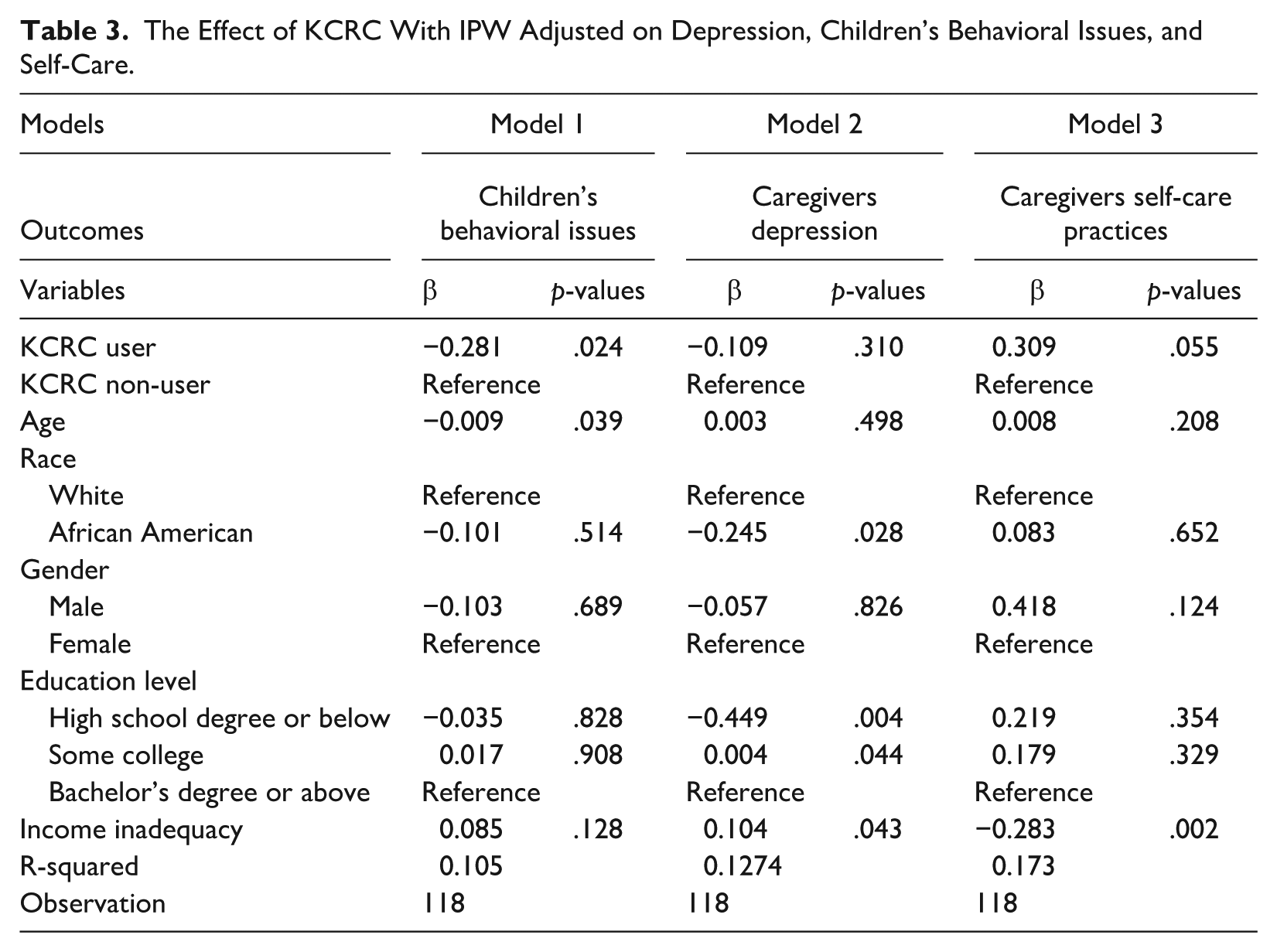
Model 1 examined the main effect of the use of KCRC on children’s behavioral issues (adjusted IPW). We found that children in the care of caregivers who used KCRC had fewer behavioral issues (β = −0.281, p = .024). This finding suggests that KCRC use was associated with an improvement in children’s behavioral issues. One significant demographic variable associated with children’s behavioral issues was caregivers’ age. Younger caregivers reported their children in care had higher scores in behavioral issues (β = −0.009, p = .039).
Kernel matching estimates revealed a statistically significant and meaningful reduction in children’s behavioral issues associated with KCRC use. Among KCRC users, child behavior scores were lower by an average of 0.35 points when estimating the average treatment effect on the treated (ATT) (β = −0.351, p = .012), even after adjusting for caregiver characteristics. The effect was consistent across all treatment effect estimates (ATE and ATC), underscoring the potential impact of kinship navigation services on child behavioral outcomes.
Caregiver Depression
As we examined the main effect of KCRC on caregivers’ depression, the linear regression analysis (adjusted for IPW) indicated that those who used the KCRC program did not differ significantly in the level of depression from those who did not use KCRC (β = −0.109, p = .310) (see Model 2 in Table 3). Caregivers who were African American and who had a high school degree or below had lower levels of depression after using KCRC (β = −0.245, p = .028; β = −0.449, p = .004). However, caregivers who had some college education and who had a higher score of income inadequacy had higher depression scores after using KCRC (β = 0.004, p = .044; β = 0.104, p = .043). In a sensitivity analysis using kernel propensity score matching, we estimated the average treatment effect on the treated (ATT) for caregiver depression. The results indicated that KCRC users had lower depression scores (β = −0.13, p = .271), though the effect was not statistically significant. These findings are consistent with those in the IPW model, suggesting robustness of the estimated treatment effects across methods.
The Effect of KCRC With IPW Adjusted on Depression, Children’s Behavioral Issues, and Self-Care.
Self-Care Practice of Caregivers
Model 3 in Table 3 examined the main effect of KCRC on caregivers’ self-care practices. The effect of KCRC on self-care practice among caregivers approached the statistical significance at a .05 level (β = 0.309, p =.055). The use of KCRC was associated with high levels of engagement in self-care. Caregivers with higher income inadequacy had lower engagement in self-care practices (β = −0.280, p = .002). The sensitivity analysis using kernel propensity score matching indicates a consistent positive association between KCRC participation and kinship caregivers’ self-care engagement (β = 0.26, p = .118), although not significant.
Discussion
This study assessed the impact of a kinship navigation program on the well-being of children and their kinship caregivers. The results indicate promising evidence of enhanced self-care among caregivers and a decrease in behavioral issues among children in kinship care. Using Lin’s (2014) hierarchy of evidence-based intervention effectiveness, which is categorized as (a) superior, (b) effective, (c) efficacious, (d) emerging, and (e) concerning. We classify the KCRC program as efficacious (Level 3), following Lin’s framework, based upon a single study design with a nonequivalent control group and nonrandomization.
Interpreting these results through the lens of Family Stress Theory provides additional insight. This framework posits that a major caregiving stressor such as assuming the care of a relative’s child can push a family toward crisis if it is not buffered by adequate resources and coping abilities (McCubbin et al., 1980). In our study’s context, the KCRC program likely functioned as an external resource that bolstered kinship caregivers’ capacity to cope, thereby mitigating the impact of caregiving demands on the family. By accessing the support, knowledge, and respite offered by KCRC, caregivers probably experienced reduced stress and were better equipped to meet their children’s needs. Such outcomes align with Family Stress Theory’s prediction that strengthening family resources and coping strategies will lead to improved adaptation and fewer stress-related negative effects (McCubbin et al., 1980).
One primary finding suggests that caregivers who utilized the services of KCRC reported fewer behavioral issues among the children in their care. The KCRC facilitated access to an array of support services, including counseling, educational resources, and community referrals. These services equipped kinship caregivers with the necessary tools to forge connections with peer caregivers, facilitating invaluable social support. Such support is crucial for addressing risk factors that exacerbate children’s behavioral challenges (Littlewood et al., 2012). For example, these services contributed to better communication between caregivers and children. By learning effective communication techniques and building stronger bonds, caregivers could create a supportive environment where children feel understood and valued, potentially reducing the occurrence of behavioral issues. This is also found in Gunderson et al.’s (2022) study on children with autism. KCRC empowered kinship caregivers by providing them with knowledge, resources, and a sense of community related to kinship care. With supportive resources, participants may feel more confident and develop greater self-efficacy, improving their caregiving (Arenella & Steffen, 2020). Increased self-efficacy of caregivers to adopt more effective parenting strategies, resulting in more constructive interactions with children (Factor et al., 2023).
Despite these resources being pivotal for managing children’s behavioral challenges, we also hypothesize that caregivers’ augmented self-care routines post-KCRC participation significantly contributed to their adeptness in managing these issues. Enhanced self-care practices corresponded with reduced caregiver stress (Washington et al., 2024), and the alleviation of stress among kinship caregivers was linked with positive behavior in children (Lin, 2018). Therefore, another key outcome of this study highlighted the influence of the KCRC on advancing caregivers’ self-care practices. This result aligns with the findings of Carter et al. (2023), whose research demonstrated that kinship caregivers engaging in a peer-supported and culturally sensitive navigation program—aptly named “Time for Me.” This program enhanced caregivers’ self-care knowledge in areas such as sleep, exercise, monitoring, medication, and coping strategies. In addition, the participants in the “Time for Me” program reported improvements in self-care practices, particularly in sleep, diet, and physical activity. Our study diverges from that of Carter et al. (2023) in that we did not categorize self-care practices into specific domains like eating, sleeping, or exercising, nor did we assess the improvement in knowledge about self-care. While Carter et al. (2023) noted significant enhancements in self-care among the “Time for Me” program participants, their conclusions were largely based on self-reported data concerning the actual self-care activities of kinship caregivers.
Our study did not corroborate the improvement of mental health among kinship caregivers through participation in care navigation programs, as the KCRC’s main effect on reducing depressive symptoms was not statistically significant (refer to Table 3). This is contrary to the findings of previous research (Monahan et al., 2013; Pasalich et al., 2021). The possible reasons for nonsignificant results are as follows. First, each participant was exposed to a varied intensity or duration of the KCRC program. If a participant had a short-term exposure, the effect of the KCRC on mental health may not have been shown. In other words, even caregivers in KCRC were in great distress, they may not experience immediate relief. Second, KCRC participants could have varied levels of mental health challenges, and a one-size-fits-all program may not address the needs of those with severe depression. Finally, we want to emphasize that the aim of KCRC is not about alleviating depression but more about peer support (e.g., emotional support, peer network, and social service support).
Practice Implication
We also have practical implications based on the study’s findings. A Kinship Care Resource Center rooted in the community can expand its services to include more support groups tailored to meet the parenting needs of caregivers. These groups could offer information sessions designed to enhance the parenting abilities of kinship caregivers. In addition, the program should aim to allocate additional spaces within the center for kinship caregivers and their children, fostering an environment conducive to quality interactions.
Furthermore, the implementation of community-based practices can be considered. For instance, each visit to the agency could begin with a self-care activity for caregivers, who would also be encouraged to maintain a record of their self-care routines. Agency staff could then follow up on these records to track and discuss progress. An example of such a self-care activity could involve music and dance: caregivers could be guided to create and practice dance moves coordinated with their favorite songs. These movements should be simple enough to be easily learned and performed either at home or in a park.
It is important to acknowledge certain limitations within our study. First, the sample size of male caregivers was notably small, which prevented specific analyses if based on gender groups and may affect the generalizability of our findings. A larger and more diverse sample could potentially lead to different insights regarding the three examined outcomes. Second, our study relied on self-reported data for self-care practices. There is a possibility that caregivers’ subjective assessments (for instance, their feelings about self-care) may not accurately represent their actual practices. Consequently, the extent of self-care activities might not be fully captured, potentially compromising the precision of the findings. Third, the assessment of children’s behavioral issues might be more pertinent to older children, as some of the behaviors assessed were quite severe that may not be applicable to younger children. This could restrict the scope of our findings to a narrower age range than initially intended. In addition, we acknowledge that the survey instrument did not capture detailed metrics such as frequency, duration, or intensity of KCRC participation. This limits our ability to differentiate effects by dosage or specific program components. Moreover, although we included race as a covariate, further subgroup analysis was not designed in our model because of a lack of power. Future work should examine potential race/ethnicity differences in kinship caregiving outcomes associated with service use. Finally, the reliance on a self-selected sample recruited largely through KCRC social media and networks raises the possibility of selection bias, which likely limits generalizability. In addition, nonresponse bias may exist as 16 individuals started but did not complete the survey.
Conclusion
This study contributes to the growing literature on kinship navigation programs by examining both caregiver and child outcomes using propensity score matching. Participation in the KCRC was associated with fewer behavioral issues among children and improved caregiver self-care practices, although no significant effects were found for caregiver depression. These findings highlight the promise of community-based kinship supports while underscoring the challenges of addressing complex caregiver mental health needs. For practice, the results suggest that kinship navigation programs may be most effective when they combine caregiver-focused supports, such as self-care promotion, with child-focused behavioral health resources. For policy, the findings reinforce the role of kinship navigator services under FFPSA and underscore the importance of continued investment in sustainable, evidence-informed models that serve both formal and informal caregivers. Future research should extend this work by using larger and more diverse samples and employing longitudinal designs. Such efforts will help clarify for whom and under what conditions kinship navigation programs are most effective and guide both program development and policy decision-making.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.