
Abstract
Our aim was to qualitatively explore LGBTQ+ parental experiences, including stress and support, while having a newborn in the NICU. Using a community-engaged approach, we collaborated with a community advisory board of (a) LGBTQ+ parents with infants in the NICU and (b) NICU health care providers who work with LGBTQ+ parents to create semi-structured interviews exploring the NICU experiences of LGBTQ+ parents in the United States. We interviewed 10 LGBTQ+ parents who had a NICU experience within the past five years. We engaged in inductive, reflexive thematic analysis with a strengths-based, constant comparative approach and generated seven themes. Participants experienced both stress and support (queer-specific and general) in the NICU and provided valuable recommendations for LGBTQ+ parents and NICU health care providers.
Having an infant in the Neonatal Intensive Care Unit (NICU) represents a departure from the usual entry to parenthood and can be a source of heightened anxiety, stress, and trauma for parents (Ghorbani et al., 2014; Janvier et al., 2016). Parents of infants in the NICU may be at heightened risk for depression and post-traumatic stress syndrome (Roque et al., 2017). These challenges may impact parental well-being, parent–infant bonding, and infant development (Vance et al., 2020). For the approximately 4 million parents who identify as lesbian, gay, bisexual, transgender, queer, or other sexual and gender minority identities (LGBTQ+) in the United States (U.S.; Flores & Conron, 2023; Wilson & Bouton, 2024), fear of discrimination due to sexual orientation, gender identity, or gender expression (SOGIE) may make the NICU experience even more stressful and lead to health disparities (Sigurdson et al., 2018).
Infants may be admitted to the NICU for a wide range of conditions, including preterm birth (before 37 gestational weeks), withdrawal from substances, infections, or a genetic or other health condition present at birth (March of Dimes, 2025). These conditions range from benign diagnoses simply needing extra observation and support for a day or two to life-threatening conditions that require a stay of 6 or more months (Lee et al., 2016). For very premature/low birthweight infants, mortality rates range up to 75%, and morbidity is also high (Edwards et al., 2024). NICU care frequently includes administration of medicine as well as surgeries and procedures, sometimes multiple painful procedures in a single day (Kassab et al., 2017). Infants in the NICU often have feeding problems, which may initially require IV nutrition or tube feeding. Respiratory conditions such as neonatal respiratory distress syndrome are not uncommon and may require administration of oxygen via machines (e.g., continuous positive airway pressure (CPAP) or a mechanical ventilator; March of Dimes, 2025).
Although health care professionals in the NICU provide support for parents to learn to care for their infants in the NICU and after discharge, many parents experience stress due to observed or presumed discomfort their child is experiencing, their own lack of confidence in caring for an infant with complex health needs, and the many inherent unknowns about their infant’s present and future health (Gooding & Yinger, 2023). Hospital social workers play an active role in supporting NICU families, typically serving as a link between the family and the medical team. Although there are numerous ways in which social workers assist NICU families, supporting the family emotionally, service linkage, and advocating for the family are some common actions the social workers may take directly. Indirectly, social workers may assist with informing policies and practices within the NICU setting, including policies and practices that affirm LGBTQ+ families.
LGBTQ+ parents may be more likely to experience an infant in the NICU due to assisted reproductive technology or adoption (Ibi & Takahashi, 2023; Marcellus, 2004; Patterson et al., 2021). In addition, LGBTQ+ parents are more likely to experience negative health outcomes (Assink et al., 2022) in large part because of stigma, discrimination, and denial of their civil and human rights based on SOGIE (US Department of Health and Human Services, 2022). Unfortunately, these discrimination experiences are widespread. A 2020 study found that 15% of LGBTQ+ participants indicated they had postponed or avoided medical treatment due to fear of discrimination (Center for American Progress, 2020). It is likely that these experiences extend to avoidance or postponement of prenatal and perinatal care (Goldberg, 2022; Ross & Goldberg, 2016), which could lead to negative infant and parent health outcomes.
As LGBTQ+ families grow (Wilson & Bouton, 2024), there is a need to examine their NICU experiences, since limited understanding of the unique needs of these parents—including what is specifically perceived as supportive and helpful by LGBTQ+ parents—may sustain non-inclusive hospital policies. Here, framed by ecological systems and minority stress theories, and using a community-engaged, qualitative, and strengths-based approach, we explored stress and support among LGBTQ+ parents with NICU experiences in the past 5 years.
Theoretical Framework
According to minority stress theory (Brooks, 1981; Meyer, 2003), people with minoritized identities, including LGBTQ+ individuals, experience stress due to stigma and discrimination at interpersonal and institutional levels. However, when applying a minority stress framework, it is important to avoid an exclusively damage-centered lens (Tuck, 2009) and also consider positive qualities, experiences, and strengths that LGBTQ+ people and their families possess to fully recognize them as having power, agency, resources, and hope (Levitt et al., 2023). It is crucial for researchers, clinicians, and policymakers to remember that in spite of pervasive stigma, discrimination, and health disparities, LGBTQ+ people show resilience to adversity and often find unique sources of support. For example, many LGBTQ+ people lean on their “chosen” families (Farr et al., 2022; Weston, 1991), find belonging within the LGBTQ+ community (Lin & Israel, 2012), integrate positive LGBTQ+ identities (Siegel et al., 2022), and gravitate toward LGBTQ+ affirming climates (National Academies of Science, Engineering, and Medicine [NASEM], 2020). We draw on queer family resilience (Farr et al., 2022; Prendergast & MacPhee, 2018) that contributes to the positive adjustment and well-being that LGBTQ+ people, including parents and children, demonstrate in spite of stigma and discrimination. In doing so, we recognize and highlight the individual characteristics (e.g., flexibility, adaptability), behaviors (e.g., coping strategies), and relational processes (e.g., family communication, LGBTQ+ parent family socialization) that help lead to healthy functioning (Farr et al., 2022) despite minority stress, or as assets that are adaptive products of experiencing minority stress (Cipollina et al., 2024; Levitt et al., 2023).
Our research also draws on ecological systems theory (Bronfenbrenner, 1979), which emphasizes people’s interactions within their environment at multiple levels. LGBTQ+ parents and their infants in the NICU are likely to be influenced by microsystems (e.g., relationships within the immediate family), mesosystems (e.g., interactions between the family and hospital staff), exosystems (e.g., hospital policies), and macrosystems (e.g., the broader sociopolitical milieu for LGBTQ+ families in a particular geographic location). Risks, including stigma and discrimination, exist for LGBTQ+ families at the exo- and macro-levels, which influence interactions at the micro- and meso-levels in unique ways, contributing to stress but also resilience. Social support, including emotional, instrumental, or informational assistance or protection (Langford et al., 1997), is an important contributor to resilience for parents (Lapidus et al., 2023), particularly LGBTQ+ parents (Farr et al., 2022). We recognize the importance of an intersectional approach (Crenshaw, 1991) to understand health equity for LGBTQ+ families. We acknowledge the many compounded social inequities experienced by the LGBTQ+ community, particularly parents who are transgender and/or Black, Indigenous, or other People of Color (BIPOC; Chan & Henesy, 2018), and those who do not conform to traditional gender expression.
Many LGBTQ+ parents face obstacles with health care practitioners in the NICU (Yinger et al., 2024). Given increases in LGBTQ+ parents, the well-documented stressors associated with the NICU experience, and the additional minority stress in health care settings, research on LGBTQ+ parents’ experiences in the NICU is critically needed. Without better understanding, hospital policies and provider training may fail to adequately support these parents.
The Current Study
Our purpose was to explore LGBTQ+ parents’ experiences in the NICU, with a focus on sources of stress and support. Our broad research question was: How do LGBTQ+ parents who have had infants in the NICU describe their experiences? Specifically: (a) What do they identify as sources of stress? (b) What do they identify as sources of support? (c) What recommendations do they have for LGBTQ+ parents with infants in the NICU and for NICU health care providers?
We had a few general expectations and questions for exploration. We expected parents to describe a range of experiences (some discriminatory, some supportive) related to their infant’s NICU stay. We queried whether parents with multiple marginalized identities (e.g., BIPOC and gender diverse) among LGBTQ+ participants would be particularly vulnerable to negative NICU experiences. This includes consideration of LGBTQ+ parents who may be more readily “visibly queer” (i.e., gender-nonconforming) in presentation, further away (“disruptive”) from various accepted cultural and social norms (Farr et al., 2025; Silver, 2020). In contrast, we anticipated that parents who described having interacted with LGBTQ+ affirming providers would be likely to describe positive experiences in which they felt supported in their LGBTQ+ parent identities.
Method
All study protocols for human subjects research were approved by the University of Kentucky Institutional Review Board. We used a community-based, qualitative, inductive approach, which is vital to advancing research about LGBTQ+ parent families and conducting culturally sensitive research with underrepresented samples to avoid problematic assumptions (i.e., damage-centered research) inherent to standardized questionnaires not previously validated among specific populations (Cipollina et al., 2024; Jones et al., 2024; Tuck, 2009). Qualitative findings can yield a comprehensive, strengths-forward understanding of experiences (Prendergast & MacPhee, 2018) and better address the needs of LGBTQ+ families who have had an infant in the NICU. Our interviews were informed by a Community Advisory Board (CAB) of LGBTQ+ parents whose infant had a NICU stay and LGBTQ+ (and allied) NICU health care providers (the development of our CAB is described in Jones et al., 2024).
Recruitment
We recruited participants through professional and personal networks, the CAB, online advertising via social media and our university’s research recruitment website, and by posting flyers at local LGBTQ+-affirming businesses. When establishing our CAB, there were several interested parents whose infants were born within the past 5 years who gave us permission to email them about future research; we sent recruitment emails to these LGBTQ+ parents. We also used snowball sampling, a widely used method in qualitative research (Parker et al., 2019; Patton, 2002), by asking participants to share recruitment materials with their personal networks. Our recruitment materials directed interested participants to a pre-screening survey administered via Qualtrics, which consisted of questions that determined whether participants met inclusion criteria and demographic questions (location/geographic area, gender identity, sexual orientation, race/ethnicity, income, and SSS). We continued recruitment until data saturation was achieved through the semi-structured interviews. See Figure 1 for a flowchart of participant inclusion.
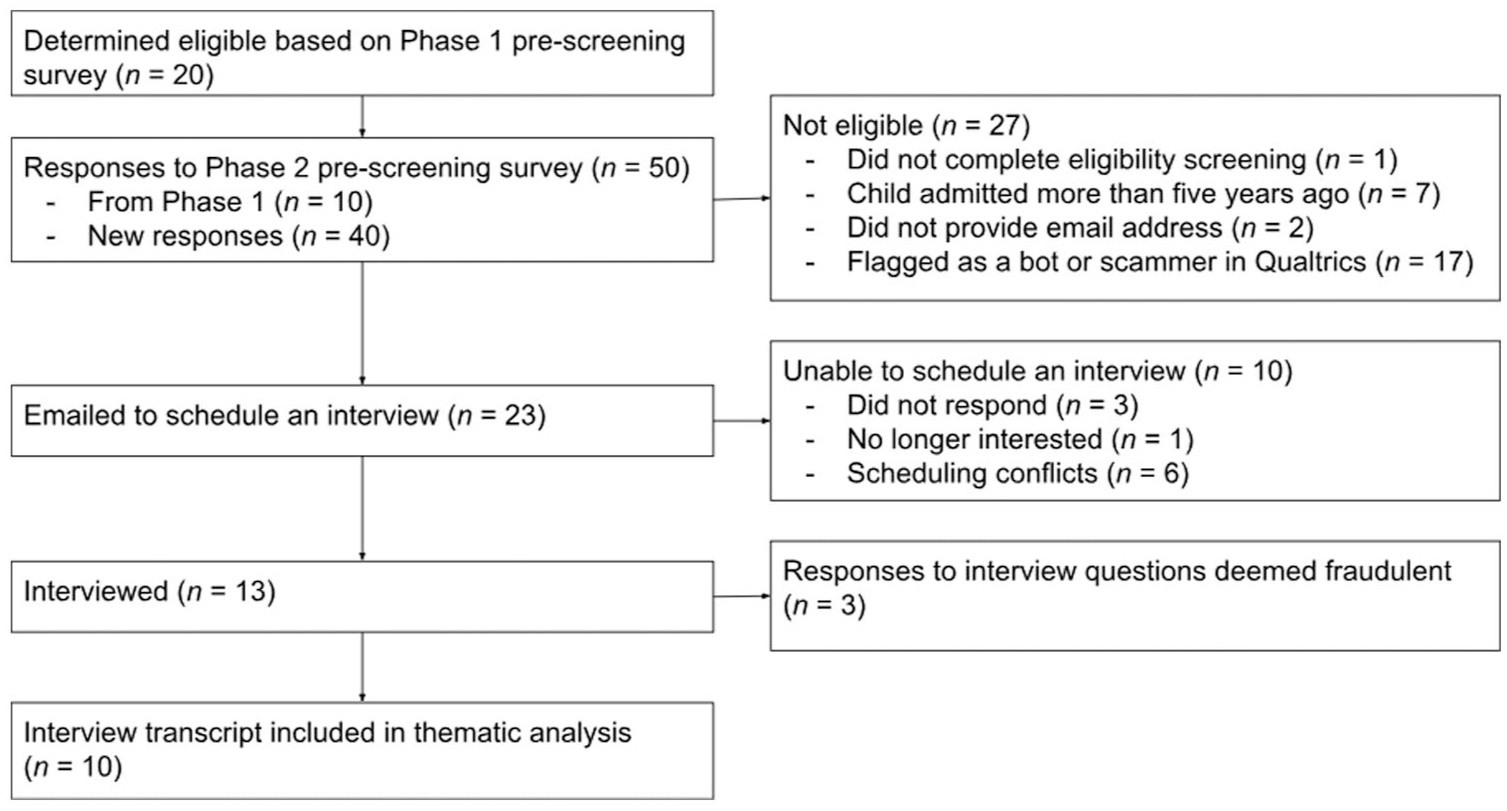
Participant Inclusion Flowchart.
Participants
Participants were parents (N = 10) who were over the age of 18, self-identified as LGBTQ+, and had a newborn child admitted to the NICU in the United States within 5 years of the time of data collection. Our rationale for these inclusion criteria was that this group of LGBTQ+ parents would not overlap with our CAB, whose infants were admitted to the NICU more than 5 years prior to the time of data collection. We also wanted to learn about the perspectives of parents whose experiences had occurred fairly recently. This was important due to changes in the legal landscape (with implications for hospital policies) for LGBTQ+ parents after several U.S. Supreme Court (SCOTUS) cases. This included the 2015 Obergefell v. Hodges ruling that made same-sex marriage (and adoption of children) legally available in all 50 states, as well as rulings that provided legal pathways for same-sex partners to be listed on children’s birth certificates (regardless of biological or adoptive parenthood) across the United States (Farr & Goldberg, 2018).
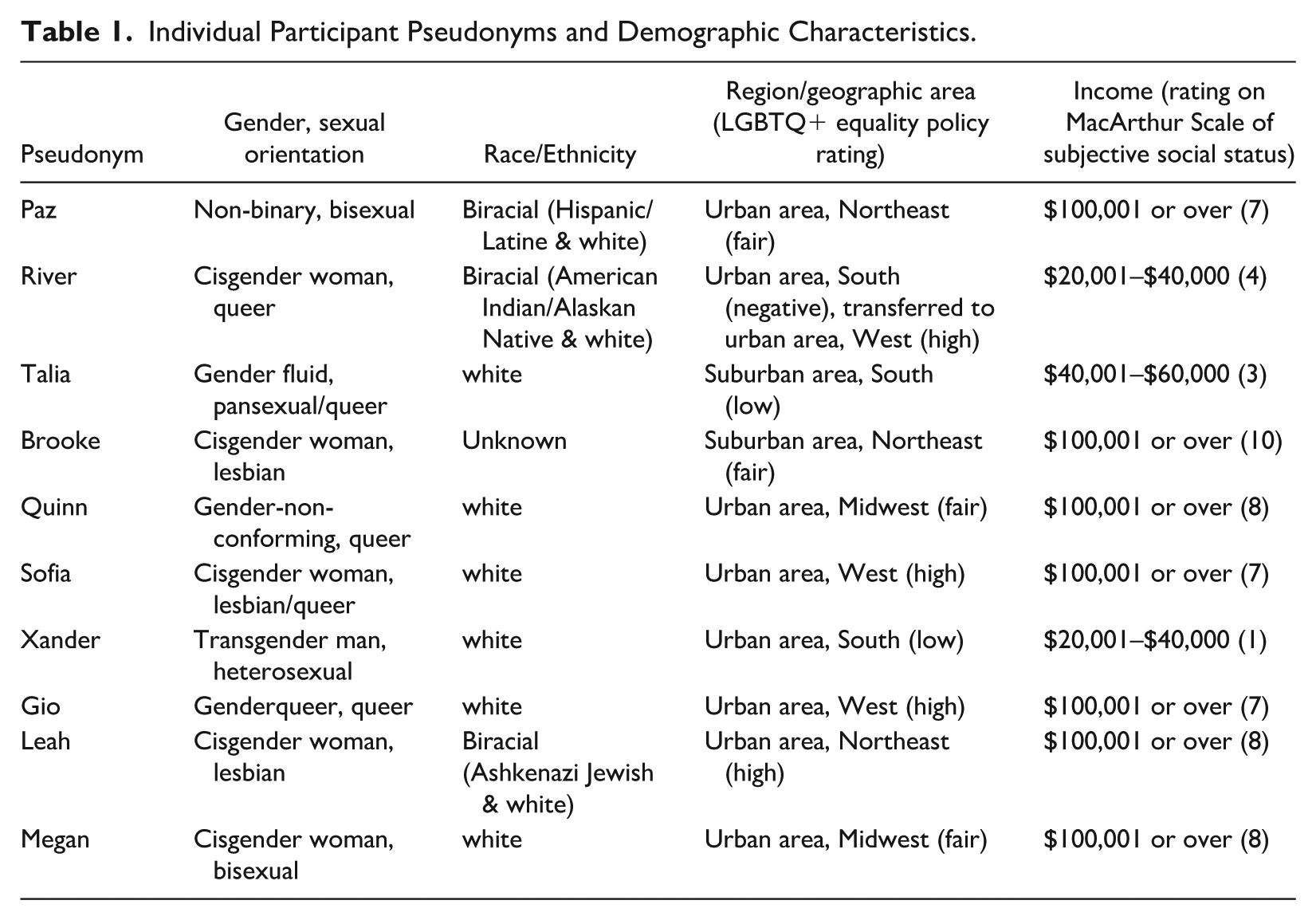
The sample included 10 participants who resided in various regions of the United States, with three families from the Northeast, three from the West, two from the Midwest, and two from the South. Five participants identified as cisgender women, one as a transgender man, and the remaining four participants identified as non-binary, genderqueer, gender fluid, or gender non-conforming. Of the nine participants who reported their race/ethnicity, six identified as white and three identified as biracial. Seven participants reported a subjective social status (SSS) of 7 or higher on the 10-point MacArthur ladder scale (where higher scores reflect greater perceived social status; Adler et al., 2000), whereas three participants reported a score of 3 or below. Four participants reported living in states with high LGBTQ+ equality policy ratings, whereas four were in states with fair ratings and two were in states with low ratings. One participant lived in a state with a high rating, but abruptly gave birth in a state with a negative rating, later moving to a NICU in their home state. Table 1 shows participant demographic characteristics and pseudonyms.
Individual Participant Pseudonyms and Demographic Characteristics.
Measures
In collaboration with our CAB members (n = 6), we developed a semi-structured interview guide (Moore et al., 2024). Research assistants conducted mock interviews with CAB members to practice and refine the questions. Ultimately, the interview guide consisted of 19 questions and nine additional probes. Some interview questions were about parents’ demographic information (e.g., SSS; Adler et al., 2000), NICU experience in general (e.g., journey to becoming a parent, how they fed their infant in the NICU), whereas other questions were about how the NICU experience impacted parents (e.g., meaningful moments, empowering experiences, impacts of the NICU stay on their family, positive and negative impacts of hospital policies). Other questions focused on parents’ LGBTQ+ identities (e.g., how being “out” impacted NICU experience, challenges faced as LGBTQ+ parents). We asked parents what advice and resources they would share with other LGBTQ+ families in the NICU, as well as NICU health care professionals working with LGBTQ+ parents.
Procedure
After determining eligibility through the pre-screening survey, a member of our research team reached out to eligible participants via email to schedule Zoom interviews. Three student research assistants conducted the interviews, which occurred from October 2023 to April 2024. Interviews lasted from 14 minutes to 1 hour 22 minutes in duration, with an average length of 46 minutes. Each participant received a $30 gift card via email after their interview. Interviews were transcribed by Landmark Associates, an IRB-approved and HIPAA-compliant third party. After research assistants checked transcriptions for accuracy, they deleted video recordings and retained audio recordings in a password-protected file accessible only to the study team.
Analysis
We employed an inductive, reflexive thematic analysis with a constant comparative approach to analyze data (Braun & Clarke, 2006, 2021), winnowing codes and consolidating into themes and subthemes. Following Braun and Clarke’s (2021) six-phase approach to reflexive thematic analysis, we analyzed data beyond the initial round of coding through an iterative, flexible, reflexive process. We engaged in regular memo writing and peer debriefing while exploring and refining interpretations of the data. Phase one began with a close reading of transcripts by two members of the research team, accompanied by memo writing using Dedoose and via individual and collective shared Google documents. In phase two, we coded transcripts inductively. To establish consensus, the research team members reviewed the preliminary coding and collaboratively coded two transcripts, refining and expanding the coding structure. We then developed a codebook to document codes, definitions, and example quotes. Two researchers independently coded the remaining transcripts and then reviewed each other’s coding, identified discrepancies, and resolved differences through discussion until consensus was reached. Phase three involved refining codes, organizing them into categories, and discussing connections, which allowed initial themes to emerge. In phase four, we further refined the themes by revisiting the research questions, consolidating and reorganizing codes and categories as needed. Phase five involved selecting final themes that best represented the data. The final phase entailed writing the analytic narrative. Although these phases were structured sequentially, they remained dynamic, with ongoing revisions and reflections throughout analysis. The codebook and interview materials are available via Open Science Framework (Moore et al., 2024).
Reflexivity, Positionality, and Trustworthiness
The research team (who come from diverse methodological backgrounds and have extensive collective experience conducting mixed-methods, descriptive, and participatory research) employed techniques to demonstrate trustworthiness through reflexive memoing and discussion, member-checking, interrater reliability, and by using audit trails during the analysis process. The coding team consisted of six of the authors of this manuscript, representing different career stages and disciplines. All members of the coding team identify as members of the LGBTQ+ community. Although three members of the coding team are parents, none have had a child in the NICU. However, one member of the coding team has worked in the NICU, three have experience working with CAB members, and three conducted the interviews.
Results
We first summarize the context of each of our 10 participants’ NICU experiences (all names are pseudonyms). Then, we describe the seven themes and corresponding 29 subthemes that emerged in analysis, illustrating the themes with exemplar quotes from LGBTQ+ parents.
Participant Summaries
Brooke’s wife, Janelle, conceived their child with sperm from a donor via intrauterine insemination (IUI) at home with a midwife. Their son was transferred to the NICU at a different hospital hours after birth due to an unexpected defect in his colon. He stayed in the NICU for almost a month and had one surgery while he was there. Brooke shared that although Janelle initially planned to breastfeed her son, this was not possible at first due to his gastric condition, so Janelle exclusively pumped for about six months before switching to exclusively nursing.
After Gio’s wife, Vanessa, experienced the loss of a pregnancy, she waited two and a half years before trying to conceive again via IUI with sperm from a donor. Gio explained that this tragic loss deeply informed their experience of becoming parents. Gio and Vanessa chose to change insurance plans so they could go to a different hospital as a result of a negative experience they had as a queer couple with their previous hospital. Vanessa was hospitalized for a week due to preeclampsia and delivered their daughter at 34 weeks, at which point she was admitted to the NICU for oxygen and feeding support, given her premature birth and small size. Gio and Vanessa’s daughter was able to go home from the NICU after 3 weeks. Vanessa initially tried to breastfeed her daughter, but ultimately decided to pump exclusively for 16 months, since her daughter had difficulty latching. Gio was a graduate student when their daughter was in the NICU. They felt that being in school gave them a great degree of flexibility to be at the hospital.
Leah and her wife, Deb, became parents through adoption after trying for several years to conceive via IUI and in vitro fertilization (IVF). They went through a private adoption agency to adopt their daughter and, 4 years later, their son. Both children were in the NICU, but their daughter’s NICU stay was only one night. Their son was estimated to have been born at 33 weeks and was in the NICU for 2 weeks, where he received formula via nasogastric tube until he was ready for bottle feeding. Although he was readmitted to the hospital due to breathing issues after being home for 5 weeks, his readmissions during his first 6 months were to the pediatric intensive care unit (PICU) rather than the NICU.
Megan and her wife, Cara, talked to many people in their community about queer family making before ultimately deciding to use sperm from a sperm bank to help Megan conceive via IUI. At 31 weeks, Megan was admitted to the hospital due to preeclampsia, which led to other health complications for her. After delivery via C-section at 32 weeks, their son was transferred first to the high-risk NICU, and then 2 weeks later, to the intermediate care NICU. Although Megan wanted to breastfeed her son, she was frustrated that a lactation consultant pushed her to begin pumping breast milk while she was still recovering from her C-section and groggy from medications. Nevertheless, she was able to pump breastmilk for her son while he was using a feeding tube and later to breastfeed him during his month-long NICU stay.
Paz stopped taking testosterone temporarily to conceive a child using sperm from a relative of their wife, Felicia. At 39 weeks, Paz experienced a blood pressure spike and was induced due to preeclampsia. Although their son was full-term, he was small for his gestational age and was admitted to the NICU to increase his blood sugars intravenously. Paz had had top surgery and was concerned they would not be able to produce enough milk to feed their son, so Felicia began taking medication to induce lactation when Paz was 12 weeks pregnant. Felicia provided milk she had pumped and was ultimately able to breastfeed their son in the NICU.
Quinn’s wife, Heather, became pregnant with triplets via IVF. Heather was placed on bed rest at 20 weeks and gave birth via emergency C-section at 24 weeks. One of their infants died within the first few weeks in the NICU, and another was life-flighted to a hospital across the state, which caused strain for the family since their two sons were more than 5 hours apart. Their sons stayed in the NICU for more than 100 days before they were able to go home.
River’s wife, Nadia, gave birth to their first child, and 3 years later, River became pregnant with their second child via at-home insemination. While she was pregnant, River expressed concerns about her pregnancy that her providers dismissed as anxiety. At the recommendation of her health care providers, to try to alleviate some of River’s anxiety, River, Nadia, and their daughter took a vacation to visit family in the southern United States toward the beginning of River’s third trimester. While on vacation, River went into labor and had a traumatic birthing experience at 23 weeks in a state far from her home that she and Nadia had left specifically because they did not feel they would be affirmed as queer parents in this state. Once her son was stable, he was able to be transferred back to the NICU in River’s home state.
Sofia and her wife, Wendy, lived in an urban western U.S. area when Sofia became pregnant via IUI. After a relatively typical pregnancy, her full-term son was delivered via emergency C-section with a hypoxic brain injury and pneumothorax. Sofia had serious medical complications requiring hospitalization, so she did not meet her baby until about 24 hours later.
Because Talia and their husband, Kevin, were in a heterosexual-presenting relationship, they assumed that most health care providers saw them as a straight, cisgender woman. Talia described two experiences of giving birth to infants who received NICU care. Talia experienced complications during both pregnancies that caused them to be hospitalized prior to birth. Both of their children were born prematurely and admitted to the NICU for breathing and feeding support, the first one prior to the COVID-19 pandemic, and the second one during the pandemic.
Xander’s wife, Zoe, was already pregnant when he met her on a dating app. Xander was with Zoe throughout her pregnancy, including during her emergency C-section to deliver their son at 35 weeks. Their son was admitted to the NICU for breathing support for 1 week.
Theme 1 (4 Subthemes): Cis/Heteronormative Microaggressions, Bias, and Discrimination Are Pervasive
This theme focuses on instances of microaggressions, bias, and discrimination that participants experienced based on their LGBTQ+ identity and/or family status. These experiences pertain to relevant paperwork like birth certificates, dismissive behavior by medical team members (seemingly motivated by LGBTQ+ identity or family), not being recognized as a family, and other cis/heteronormative assumptions and microaggressions.
Subtheme 1.1 was Birth Certificates, where parents described experiences filling out birth certificates, often being asked or required to change labels or wording. Megan recalled:
On our paperwork . . . they only had an area for mother and father . . . then there was something on there that said . . . “if there’s perjury on this document, you’ll be fined $10,000” . . . We were asking people . . . “we literally don’t know how to fill this out because there isn’t a spot for my wife on here . . . if we put her name in father, we don’t wanna get charged $10,000.” We’re asking all these people, and they’re like . . . “We don’t know what you’re supposed to do.” . . . We contacted a lawyer, who specializes in queer rights . . . We contacted somebody who was connected to us . . . in [state] records who does this . . . everybody was like, “Just put Cara’s name in the father . . . and it will be okay.”
Paz described:
The only thing that I didn’t know was gonna happen—when you fill out the notice of birth and all the applications for social security . . . ours had said “Parent 1” and “Parent 2,” which was great—but they ask you for your maiden name or any previous names. I didn’t change my name when I got married. My wife has my last name, but I changed my birth name, previously. And so I put my old name as a previous name, and then when the birth certificate came, it had my old name on it, which was really annoying.
Xander said:
They allowed [Zoe] to sign the affidavit stating I could be on my son’s birth certificate . . . we both signed the paperwork in front of the notary. The notary signed it . . . I watched her put it in his file. When I ordered the birth certificate, I am not on [certificate] whatsoever.
Bias-based Dismissive Behavior was Subtheme 1.2, where parents describe how the medical team treated their concerns or input in a dismissive manner. Xander said,
I don’t think they knew how to address me as an individual . . . they weren’t rude or foul . . . they didn’t deadname me or anything, but they just wouldn’t try . . . to call me Xander . . . they were more accessible to my wife when they would talk. River explained: One other really unique thing to being a queer couple is that when [my infant] started to breastfeed, chest feed, and drink out of the bottle, we wanted assistance, and we needed approval by the neonatologist to do SNS [supplemental nursing system], which we had done with our first child. And we wanted my wife to have the experience of latching and possibly have support producing milk-inducing lactation from a non-maternal parent. And they shut that down pretty immediately and told us that that would never happen and that it’s not safe for him to receive fluids at an uncontrollable frequency, and that they would not support us in that, which was . . . kind of like a slap in the face. . ..I, at that point, said that they would offer those services to mothers who nursed or who their child wasn’t ready to latch onto a bottle or they weren’t producing enough milk through chest feeding . . .there were situations where they allowed that for other women who were the maternal parent of that child, and that we felt like we were being discriminated against because we asked for those same services for the non-maternal, the non-gestational parent.
Subtheme 1.3 was Not Recognized as a Family, involving instances where parents described a struggle to be seen as a family by hospital staff (i.e., a non-gestational parent being called a friend or sister rather than wife/mother). This subtheme often involved parents having to assert the existence and validity of their family structure. River reflected:
. . . it was also challenging to be recognized as both being parents to our child . . . within the first month, it was constant. They would recognize me as a femme-presenting partner in our partnership as the mother . . . we would always have to explain who my wife is, who is masculine presenting, her role as not my sister, not a friend, but the second parent . . . second mother of this child . . . somebody with equal say over care.
Subtheme 4.4 was Other Cis/Heteronormative Assumptions and Microaggressions, involving instances where parents, through interactions with staff, perceived how the hospital environment and NICU operating procedures appeared to be built for cis/heteronormative families. Brooke shared, “. . . one time on the phone someone was like, ‘When you’re gonna park, have your husband park the car in that garage.’” Even some relatively positive experiences revealed the pervasiveness of these cis/heteronormative “scripts” during patient interactions in the NICU. Megan said,
But also we were there during Mother’s Day, which was also a really interesting thing cause I do feel like on the one hand, they made us both something, but I think there were some weirdness around, like, I think that they weren’t really used to that, and they were trying to figure out, like, “What do we do with them?”
Theme 2 (4 Subthemes): Despite Difficulties, Positive Experiences Along the Way
This theme includes positive experiences in the context of adversity described by participants. Subthemes relate to the presence of LGBTQ+ people and allies among the medical staff (nurses, doctors) and also normalcy when experiencing their baby’s developmental milestones or due to the hospital environment, policy, and staff. Additional subthemes include positive emotions (joy, relief), and also strength, endurance, resilience, and coping (including establishing boundaries) experienced across the experience of having a baby in the NICU.
Subtheme 2.1, Presence of LGBTQ+ Staff (Doctors, Nurses), and Allyship, referred to when parents discussed positive experiences of LGBTQ+ doctors and nurses and ally-identified staff members who provided a sense of safety and other positive feelings. Parents often described trusting these staff members to be open and honest with them about certain choices and procedures. River shared: “I think that we lucked out—there was one openly gay neonatologist on the staff. I think—he probably advocated us for behind the scenes” and also explained:
We first came to the hospital . . . they had their rounds to say who was born that night, where they came from, they did introduce us as two moms . . . [A nurse] automatically jumped up and asked to be assigned to us because she knew that we were going to need support from within our community to feel safe there . . . We developed . . . a very loving, trusting, friendship and professional relationship with her where she helped us understand the process of the NICU, the trajectory of where he is . . . the likelihood of him continuing care and getting better, in a way that we could understand . . . we trusted her to tell us hard things, hard truths, because we are both queer . . . she also was really adamant about teaching us how to care for, touch, and bathe our very sick and fragile child with compassion and dignity . . . we will be forever grateful for that.
Subtheme 2.2 (Normalization) consisted of instances where parents felt normalcy through events such as progress in their baby’s development, through positive hospital environmental factors, or through being “treated like everyone else.” Baby milestones included instances where parents described how their baby’s developmental milestones (i.e., being able to get rid of certain equipment or reaching a certain weight) were positive experiences. River noted:
. . . the second-most memorable time is . . . after he had been on the conventional ventilator for a while, still intubated, . . . they hadn’t told me yet, and when I walked in, he was on the CPAP . . . it was the first time that I saw him not intubated . . . it was really just nice to walk in and have that surprise . . . he also had clothes on. They had dressed him for me . . . that was the first time I felt like I saw him as a real baby.
Participants also experienced normalization through the hospital environment, including when they could stay the night with their baby or have a room with certain accommodations like a window, shower, bed, or TV that helped them feel humanized. Nurses providing care and support also contributed to this experience of a more positive environment. River offered:
Every room was a private room . . . and there was a foldout bed and a TV and big, giant picture windows that looked out. And we were allowed to sleep. And they had showers and bathrooms. And that really was a gamechanger for us where we felt like we weren’t just watching—sitting there, staring at a sick baby. We felt humanized more where we could sit there and watch TV while we were holding the baby and look out of a window, spend the night, wake up with him in the middle of the night, and . . . it normalized it.
Being “treated like everyone else” was also core to Normalization and involved instances where parents described interactions with and expectations from medical personnel aligning with how any other parent would be treated. Quinn shared:
They didn’t care what you looked like, where you came from, who you were married to. They just wanted to make sure that they could contact you . . . that you were there for your child . . . they were there for your child . . . for us, too.
Subtheme 2.3 (Positive Emotions) encapsulated instances where parents described events that revolved around or caused positive emotions such as joy or relief. Brooke shared: “. . . very joyous and happy—big relief to get home,” and Quinn said, “going home, you have so much joy.”
Subtheme 2.4, Strength, Endurance, Coping (Boundaries), and Resilience, involved instances of parent skill development or engagement of resilience and endurance. Parents described developing and enacting certain coping strategies like setting boundaries. Leah noted:
I can be a very anxious person, but there’s actually a way that it forces you to be present because—you never know what you’re gonna get . . . people sometimes think bad about adoption, but the truth is if you give birth, you don’t know what you’re getting, either. There are so many unknowns. I say that because, yeah, I think it forced me to—I mean resilience is a bit of an overused word, but . . . you have to cultivate a bit of a calm strength, and patience, and just being like ‘I am not the boss.’ You can’t make it go faster. You can’t know what the outcome is. You just can’t really know, right?
Theme 3 (6 Subthemes): Considerations of Context Are Vital
This theme encapsulates participant experiences that illustrate important contextual details surrounding their infant’s stay in the NICU. This included considerations related to perceived privilege afforded by certain aspects of identity, the type of hospital and/or NICU, participants’ geographic location, relevant pregnancy and birth circumstances, whether this was a first birthing experience, and how the COVID-19 pandemic may have been relevant.
Subtheme 3.1, Identity Significance and Intersectionality, regards the role of identity and intersectionality of identities for participants. This subtheme involved instances where parents reflected on how specific privileged or marginalized identities that they hold impacted specific abilities to connect with providers and/or support. Megan noted the role of cis-privilege: “my friends who are trans. . . I feel like they experience. . . more challenges than my cis-queer friends.” Talia did not feel like they faced challenges related to their LGBTQ+ identity during their NICU stays because, in their words, “I wasn’t very out . . . I’m in a heterosexual-presenting relationship, so I think most people just assume I’m a woman, a heterosexual, cisgendered woman.” However, experiencing the erasure that comes with those assumptions seemed uncomfortable, since their first piece of advice to health care providers was “don’t make assumptions that you know how people identify, that you know what their relationship is to their partners.”
Sofia offered: “We had some privilege just because we were both in the medical field. And so there was probably more sort of peer-level conversations happening at times.” Relatedly, having familiarity with medical terminology, health care settings, or the NICU itself seemed to help some participants feel less stressed during their infant’s NICU stay. Several participants (e.g., Brooke, Gio, Megan, Paz, Quinn, and Sofia) reported that they and/or their spouse worked in health care or a helping profession, such as social work, psychology, nursing, or medicine. Sofia and Paz reported that they had worked in the hospitals where they gave birth. In contrast, participants who were less familiar with medical settings frequently felt overwhelmed. Quinn described that even as a nurse, the NICU was a setting that their family was not familiar with.
Leah had two children who experienced the NICU and one who also experienced the PICU. Leah and her partner became adoptive parents to these two children through two paths (public and private). Thus, as another example of identity significance and intersectionality, Leah described her family’s experiences with the legal and policy aspects that were unique and offered how intersecting identities of being queer and adoptive parents came into play.
Subtheme 3.2 refers to the type of hospital and NICU that participants experienced, and included instances where parents described these features of their stay (e.g., hospital was religiously affiliated or “baby-centered”). River said: “We were also in a Catholic hospital—and in that hospital, they had the right to refuse service to us, and that’s something that we knew.”
Subtheme 3.3 pertains to the role and impact of geographic location (e.g., city, state) of participants’ NICU. Gio noted:
. . . policies about birth certificates . . . just being politically a blue state was really reassuring. We’ve lived in Texas before . . . we wouldn’t have done that in Texas. We would’ve moved to do that . . . I think just the overall inclusive policy of the state was absolutely necessary for us to feel comfortable and . . . willing to do that.
Pregnancy and birth experiences comprise Subtheme 3.4. Included here are participants’ descriptions of pregnancy or birthing events or circumstances that contextualize their NICU stay. Sofia explained,
I was induced at 39 weeks . . . ended up having arrested descent and . . . an emergency C-section. He came out not breathing . . . he had a hypoxic brain injury and a pneumothorax . . . he ended up being in the NICU for treatment of those.
Subtheme 3.5, Parental Status, is characterized by whether the NICU experience reflected parents’ first-time becoming parents or whether this was a subsequent pregnancy, birth, or parenting experience. About their NICU stay and transition to parenthood, Megan said: “We were first-time parents, so we were like, ‘We don’t know what we’re doing.’”
Parents whose NICU stays took place during the COVID-19 pandemic (e.g., Brooke, Paz) reported different experiences than those whose NICU stays took place before (e.g., Gio) or after the height of the pandemic, encapsulated by Subtheme 3.6 (COVID-19), where parents noted instances of the impact of COVID-19 on their NICU stay. COVID-19 presented an added challenge in preparing for, and then experiencing, the birth of their child (including limitations on who could be with the baby or birthing parent, and when), which furthered feelings of isolation and anxiety. The notion of COVID-19 reverb, or ripple effects from the pandemic, was evident in these families’ lives. Brooke remembered:
It was May 2020, so during the birth and postpartum, we couldn’t leave the room. Everyone was wearing masks. Visitors were very restricted. Certain things that might have been open like restaurants or takeout places weren't open . . . once we brought our child home, we continued to be fairly isolated.
Theme 4 (5 Subthemes): Negative Experiences Are Common
This theme encapsulates participants’ described experiences of Negative Emotions (Subtheme 4.1). These emotions named or referred to can include fear, anger, overwhelm, anxiety, uncertainty, grief, (self-)blame, guilt, and others. Xander expressed such fear in saying, “It’s scary ‘cause you don’t know if the baby’s gonna make it day to day.” River described the host of negative feelings that arose across the experience: “At that point, I started to be self-deprecative and blame myself for not advocating for myself early on in the pregnancy and not having the foresight to recognize that something was wrong with me.”
This theme also includes reference to Harmful Stress as Subtheme 4.2 (to make distinct from experiences of stress that can be constructive, productive, or even positive). Subtheme 4.2 involves different types of harmful stress that can result from financial, practical (e.g., related to baby care, parenting, job/career, etc.), and medical (the baby and/or parent) concerns. Gio discussed financial stress (i.e., instances where parents discuss stress due to financial strain or concerns):
I think logistically . . . you’re thinking about insurance and costs. We were racking up a million-dollar bill and knowing that we were about to get slapped with . . . our whole deductible . . . thinking about logistically what that meant . . . logistics of insurance are stressful.
Leah described other practical stress (i.e., instances where parents discuss stress over issues like baby care, job/career, parenting, etc.): “It affected us logistically for sure in that way—and we were both trying to work, and it was just kind of really crazy juggling.” Leah noted stress about medical concerns that necessitated a feeding tube:
Seeing the tube, it’s kind of scary . . . he pulled the tube out once, so they had to do it again . . . that’s a little bit stressful when you see that for . . . such a tiny baby . . . he was so, so tiny . . . he feels precarious to hold.
In addition, this theme of negative experiences includes participants’ feelings regarding control, and often the loss of it. Subtheme 4.3—(Loss of) Control—includes instances where participants describe grappling with feelings about having no control or losing control while in the NICU. Talia recalled:
. . . the nurses directed his feedings . . . his bathing . . . I know why that happened, but it’s really stressful . . . to feel like you have so little agency in your child’s care . . . the biggest thing is . . . feeling out of control of the decisions that were bein’ made for him.
Subtheme 4.4 (Trauma) pertained to parent trauma during the NICU stay. Talia noted:
. . . the trauma of feeling like I couldn’t bond with him . . . even when I started to feel like he was mine, I felt like he was on loan from the hospital because the nurses were so confident when they were handling him. On top of birth trauma . . . the trauma of feeling like this isn’t really my kid.
Subtheme 4.5 (Hit on Mental Health) captures the negative impact the NICU experience had on participants’ mental health. River described:
. . . all-encompassing, full-body, debilitating amount of stress . . . could not have my anti-depressants re-prescribed to me out of state and had no help with that, so I was experiencing extreme post-partum depression, physical malaise, and exhaustion. I was pumping every 3 to 4 hours for the first 3 months . . . often, I felt like I was a shell of a person. I completely shut down. I could not talk to anybody outside of the NICU team . . . it was really not great for my mental health, but I felt like it [pumping] was the only empowering way that I could protect my child and help in his healing.
Theme 5 (4 Subthemes): There Is a Ripple Effect of NICU Impact on Family
This theme describes the broader impact of the NICU experience on LGBTQ+ parents’ family members, including partners, children, and extended family. Subthemes consider intersections of family structure and parenting status (i.e., first or subsequent child or birth), as well as geographic location (i.e., city, state) in relation to experiences of harmful stress.
Subtheme 5.1, Partner Relationship, referred to the impact of participants’ NICU stay on their partner relationship. River expressed:
It impacted my relationship with my partner where I was coming out of a traumatic birth, postpartum depression, pumping full time . . . I was always afraid that we we’re going to lose [our child], so my wife and I—we became ships in the night. One of us would spend half of the day there, and then we would switch.
Subtheme 5.2, Other Children, reflected instances of impact for some parents’ NICU stay on other children. Talia said:
[Older sibling] had to be in care of other family members for almost two weeks . . . I think it changed the dynamic . . . I think we, maybe, have corrected for that now. But for a long time, I think it was a lot harder for him to bond with his brother.
Subtheme 5.3 (Extended Family) included instances where parents described the impact of their NICU stay on family members (e.g., their own parents). Talia expressed:
Both of our NICU stays were hard on our families . . . they didn’t understand why we were so protective of both children, being scared that they would get something that would put them back in the hospital or would harm them majorly . . . our family didn’t understand what we had been through in the NICU and how scary that is. It was a lot scarier with our first. Our second . . . he mainly just needed to eat a little and make sure he was okay . . . with our 1st, I think family thought that we weren’t wanting to share our baby.
Subtheme 5.4 (Intersections of Family Structure and Geographic Location) focused on instances where parents detail how location (i.e., city or state) intersected with their family structure (i.e., the presence of other children) to create new stressors and challenges. Quinn described:
. . . one of our little guys was life-flighted . . . across the state, five hours away, and one of them stayed here. One of them passed away . . . that was probably the hardest part, is that we were split up as a family, as a team . . . how do we make it work and still be there for our kids?
Theme 6 (3 Subthemes): Many Forms of Support Are Needed and Valued (To Support Those Positive Experiences Despite the Difficulty of a NICU Stay)
This theme refers to the many forms of support that are needed and valued by participants to facilitate and sustain the most positive possible experience and outcome for their families. Subthemes relate to support and lack thereof, as well as (queer-specific) advocacy, particularly personal (e.g., by partners, extended family, friends), professional (e.g., among medical staff), institutional (e.g., via hospital policies), and self-advocacy.
Subtheme 6.1 is Resources, including any instances where parents described how certain outside groups and materials facilitated aspects of their NICU stay. This subtheme comprised parent descriptions of support through LGBTQ+ or NICU parent groups, or both. Parents often got involved with certain support organizations or charities. Brooke said, “We had like a queer young parents group that we would meet with every Friday. We started that before actually he was born, but we continued to do that. And that was a good form of support.” Resources came in the form of those online (i.e., instances where parents found support and knowledge through things such as informative websites, social media pages, and virtual support groups), in-person support groups and organizations, as well as books and material resources. Regarding online resources, River reflected: “I would say there’s two micro-preemie Facebook pages on there. I think that it was helpful, logistically, to figure out what was wrong with my son and crowdsource other people’s experiences to kind of see where he was at.” Parents also read books or other materials to gain knowledge during their NICU stay. Quinn remarked: I had actually bought a book on my phone. It was called “The Preemie Primer.”
Subtheme 6.2 is Lack of Sufficient Support is Common. Parents described that the support or resources available were insufficient to fully help during their NICU stay. River noted:
. . . we didn’t see ourselves in the parents in the NICU, so we did not feel comfortable joining the NICU support group there. It was very heteronormative, run by a Catholic charity . . . we did not feel safe or welcomed in that environment. We really lacked that support while we were there to connect to other parents who were going through some of the same things. Those support services were just really lacking.
Subtheme 6.3, Advocacy, involved instances where parents discussed support (including queer-specific support) from people and groups during their NICU stay and the transition home.
Personal advocacy consisted of instances where parents described emotional and logistical support from friends, family, or their partner during their NICU stay. Leah noted:
We had two friends in particular who spent time with us there who were able to come in, meet [infant], hold him. Even though they were mostly there to help with our daughter, they were able to sort of be part of the support team in that way. Having a chosen family and having friends . . . that was really an outside resource that was invaluable because it was like they could take my daughter to the playground or the pool.
Queer-specific advocacy reflected instances where parents felt a sense of support in the NICU due to items such as affirming pins, flags, signage, or hospital policies, as well as staff microaffirmations. Paz commented on queer-specific advocacy:
I had a really good doc, so it was very obvious in the chart. . .what name I was using . . . I was going by Dad, and my pronouns, and kind of what our family structure was, and who was breastfeeding and who carried . . .
When describing professional advocacy, parents shared how members of the NICU team (especially doctors, nurses, or specialists) advocated for parents and supported them through certain decisions. Talia said,
[Our doula] was able to advocate in those moments when we weren’t, because she wasn’t . . . having an epidural, being under anesthesia, being the . . . supportive partner who is just wanting to make sure that their child and partner comes out of this alive. Having a doula was a huge difference for us on the second time. She was able to advocate and ask questions with the staff when I didn’t . . . she understood more of what was going on . . . at one point, they gave me fentanyl during my surgery . . . they said, “We’re gonna administer this,” and she said, “Before you do that, is that compatible with breastfeeding?.” . . . so that I can make an informed decision. Whereas before, I don’t know that I could’ve asked those questions. I don’t know that I had the wherewithal or . . . the presence of mind . . .while you’re actively having surgery . . . I don’t know that my partner had the knowledge either or the presence of mind. . .having a third party who is there just to advocate for you, who knows some of the systems and the language and the implications of different decisions, who can say, “Here’s the full understanding,” so that I could give informed consent.
Advocacy also included instances of institutional advocacy, or times where parents described how certain hospital policies were beneficial toward better treatment. Sofia explained, “we were very, very lucky that the NICU was able to provide him with donor milk. I don’t know that all full-term babies necessarily have that benefit, but luckily, we were able to get that.”
Advocacy occurred through Self-advocacy as well (i.e., instances where the parents advocated for themselves, such as making sure their thoughts were known among the staff or by insisting on trying other care strategies or getting new staff involved). Quinn remarked:
It took a lot for me, as a parent, to speak up for my kid, and I’m so glad that I did because if I wouldn’t have, I really feel like he would have been reintubated and we would’ve been kinda taking these huge steps backwards. That was huge for me to be like, “Okay. You do know your kid. You do know this.” That was very impactful and very empowering for me as a parent to recognize that, but not easy to stand up.
Theme 7 (3 Subthemes): What Worked and What We Needed (Advice/Recommendations)
This theme conveys specific advice and recommendations from participants, particularly for LGBTQ+ parents with NICU infants and health care professionals who work with them. Subtheme 7.1 focused on recommendations for parents. Participants gave advice that would be helpful for other LGBTQ+ parents who will have a baby in the NICU to know. Sofia offered:
You’re your best advocate and your child’s best advocate . . . I think just being upfront about . . . this is your family . . . Once we corrected people once or twice . . . people weren’t assuming . . . baby had some absent dad who wasn’t coming in and that my wife was . . . aunt or something like that. Obviously, it depends on where you are, and people have their safety concerns, too. But, if that’s something you feel safe doing . . . you are entitled to . . . acknowledgement of your family. Advocate for yourself and your relationships.
Gio advised:
Find a doctor and team that’s inclusive and affirming, and making sure your insurance is . . . taken at hospitals . . . that are outside of religious hospital systems . . . you might have more barriers in that way than you might not in another system.
Megan recommended: “For LGBT parents, I think I would say it for any parent . . . try your best to lean on your community . . . having additional queer community can be an additional buffer.” Speaking of the importance of queer community, River suggested:
Find other queer parents that have been through that same experience . . . Find anything that you can, even if the google search is “queer NICU.” . . . find those people . . . hear their stories . . . get those support systems . . . Find any queer person that works in that hospital who sees value in your relationship and who you are and can validate your experience and help you advocate for yourself.
Subtheme 7.2 refers to recommendations for hospital staff who work with LGBTQ+ parents with NICU infants. Participants described what NICU medical care providers (doctors, nurses, other staff, specialists) should know or do when working with LGBTQ+ parents. Leah said: “People should always know that it’s very rude to make assumptions about people’s families . . .not asking. . .where the father is or where your husband is, or vice-versa.” River said:
I want them to know and acknowledge the fact that queer families exist . . . we deserve representation in hospitals even if we are the minority population . . . signage that is welcoming to queer people. Even if we saw a rainbow flag . . . it would have changed our perception walking in there, as welcoming . . . to educate their staff that . . . “these people are both moms . . . this is . . . mom, this is mama.” This is what “they’ve told us” and then make sure that that is in every file, it’s visible for any nurse coming in to take care of that baby who these parents are, what their titles are, and that they are valid, meaningful . . . should be respected . . . It’s not optional . . . You’d have to validate that and accept that. Whether you have indifference to queer identities or not, it should be policy.
Subtheme 7.3 is about recommendations for resources and groups. Parents described resources, like Reddit, local groups, or action plans that were helpful or would be helpful in the future. These can apply to various groups such as researchers and policymakers too. River said,
I really wish that there was a online Zoom queer parent support group that I could have joined at that time . . . people need to recognize that not all identities are going to be supported in internally offered NICU support groups . . . they should have the resources to find other avenues for parents from marginalized communities to access those resources in ways that are affirming to their identities.
Discussion
In this study, we used an intersectional (Chan & Henesy, 2018; Crenshaw, 1991), strength-based (Farr et al., 2022; Prendergast & MacPhee, 2018), and community-engaged approach (Key et al., 2019; Newman et al., 2011) to interview 10 parents who identified as LGBTQ+ and who had an experience of an infant in the NICU within the last 5 years. Guided by ecological systems (Bronfenbrenner, 1979) and minority stress theories (Brooks, 1981; Meyer, 2003), we wanted to understand more about LGBTQ+ parents’ experiences of stress and support in the NICU, with the goal of informing future scholarship and praxis. Using qualitative, reflexive thematic analysis (Braun & Clarke, 2006, 2021), we identified seven themes with 29 subthemes. We describe how themes address specific research sub-questions about stress, support, and recommendations for LGBTQ+ parents and providers alike in NICU settings.
In connecting the seven themes to our overarching research question, Themes 1 and 3-5 (Cis/heteronormative microaggressions, bias, and discrimination are pervasive; Considerations of context are vital; Negative experiences are common; There is a ripple effect of NICU impact on family) relate to what participants identified as sources of stress. They identified sources of support via Themes 2 and 6 (Despite difficulties, there were positive experiences along the way; Many forms of support are needed and valued). Recommendations from participants to parents and providers were both encapsulated by Theme 7 (What worked and what we needed).
Importantly, some themes and subthemes appeared universal, at least among these 10 participants. All 10 had experiences captured in five of seven themes; subthemes described by all participants were: 2.2 (hospital policy and environment), 2.4 (strength, endurance, coping, and resilience), 3.4 (pregnancy and birth), 4.1 (negative emotions), 6.3 (professional advocacy), 7.1 (recommendations for parents), and 7.2 (recommendations for providers).
Our findings underscore the duality of stress and support in NICU contexts for LGBTQ+ families. Consistent with minority stress theory (Brooks, 1981; Meyer, 2003), participants described multiple sources of stress, including loss of control, negative emotional experiences, ripple effects on family systems, and cisheteronormative microaggressions and discrimination. These were particularly stressful if NICU experiences happened with a first child and transition to parenthood and if medical and health care settings were less familiar to participants. At the same time, participants articulated sources of resilience, including coping strategies, positive interactions with providers, and multiple forms of formal and informal support. These results reflect a “both/and” perspective: NICU experiences for LGBTQ+ parents involve significant challenges (vulnerabilities and risk), but also opportunities for affirmation, advocacy, and resilience (Prendergast & MacPhee, 2018).
All participants seemed eager to make parent and provider recommendations given their direct experiences, especially since needed resources and support were often lacking. Participants frequently emphasized the importance of visible and tangible signs of queer affirmation like inclusive paperwork, gender-affirming language, and LGBTQ+ symbols in health care settings. Our findings align with prior work documenting how queer visibility and representation foster safety and belonging in health care (e.g., Dua et al., 2025; Nelson, 2020). Conversely, cis/heteronormative assumptions—including misrecognition of parental roles or erasure of bi- and pansexual identities via assumptions about heterosexual-presenting relationships—were experienced as stressful or invalidating, echoing prior research on LGBTQ+ health disparities in perinatal contexts (Sigurdson et al., 2018; Yinger et al., 2024).
As we anticipated, parents described a range of experiences (some discriminatory, some supportive) related to their infant’s NICU stay. We were not able to ascertain whether BIPOC parents were more vulnerable to negative NICU experiences because all of our participants identified as white or biracial, with white as one of the races identified. However, Talia’s experience of having no challenges related to LGBTQ+ identity because they were in a cis/straight passing relationship provides support for our prediction that parents who were readily “visibly queer” (i.e., gender-nonconforming) in presentation would be more vulnerable to negative NICU experiences (Farr et al., 2025; Silver, 2020). Contrasting the largely positive experience of Paz (whose experience was in an openly LGBTQ+-affirming hospital in a state with high LGBTQ+ policy ratings) with the negative experiences of River (whose experience was in a NICU in a Catholic hospital in a state with negative LGBTQ+ policies) supports our expectation that that parents who interacted with LGBTQ+-affirming providers would likely describe positive experiences where they felt supported in their LGBTQ+ parent identities. Despite overall negative experiences described by River, they noted the positive impact of their queer-identified nurse in the NICU.
Participants highlighted the centrality of support networks. Formal supports included affirming nurses, physicians, and social workers, while informal supports included partners, family members, and online communities. These findings are consistent with evidence that social support buffers the effects of minority stress and enhances parental coping (Edwards et al., 2024; Veldhuis, 2022). Importantly, participants differentiated between coping strategies used to manage their own emotions and systemic supports provided by institutions, suggesting that resilience is promoted via a variety of internal and external mechanisms.
Strengths and Limitations
The intent of this research was to develop a deeper understanding of LGBTQ+ parents’ experiences in the NICU and not to universally explain or draw conclusions. Our study has limitations that must be considered. While our sample size (N = 10) is similar to other qualitative studies (Hennink & Kaiser, 2022), it is still limited. All resided in urban or suburban areas; none were from rural areas. Our CAB consisted of women, so our interviews may have missed specific questions unique to experiences of people with additional and different gender identities. We also do not have consistent information about whether participants’ NICUs specifically recommended supportive online or material resources; this is a question in future research.
Despite limitations, our study contributes to scant literature about LGBTQ+ parents’ NICU experiences. Even with a small sample, different parenthood pathways and sexual, gender, and racial/ethnic identities were represented among our participants. Our participants also came from a variety of different geographic regions across the United States. Second, our study was informed by a CAB (Jones et al., 2024) of people who identify as LGBTQ+ parents and LGBTQ+ affirming NICU employees. This is the first study to our knowledge using a community-engaged approach to address this research area. Continued community-engaged research here is needed.
Implications for Future Research, Practice, and Policy
Our findings demonstrate the value of community-engaged approaches. The involvement of our CAB not only informed study design and interpretation but also ensured that LGBTQ+ parent voices shaped dissemination. Future work should continue to build on community partnerships while expanding to include more diverse geographic regions and family structures, including parents from rural areas and those with varied gender identities.
NICUs often strongly emphasize breastfeeding (Wight, 2015). This may pose challenges for LGBTQ+ parents who chestfeed, induce lactation, or use donor milk (Ferri et al., 2020). Greater awareness of these complexities in research, coupled with gender-affirming lactation support, is needed to reduce stress and support parent–infant bonding for LGBTQ+ parents.
Our findings have implications for NICU practice and policy and will inform our research team’s creation of a toolkit for LGBTQ+ parents and practitioners who work with them in the NICU. Theme 7 comprised participant recommendations for both parents and providers. For parents, advice included: (a) advocating for oneself and one’s child, (b) asking questions of NICU staff, (c) preparing for possible challenges, and (d) prioritizing self-care by seeking support for your own needs. For providers, participants suggested (a) explicit training in LGBTQ+ family competence, such as understanding that two married same-gender parents can be listed on a birth certificate, (b) recognition of diverse pathways to parenthood, and (c) adoption of queer-affirming hospital policies and practices, including providing explicit queer-affirming signage and paperwork. These insights reinforce prior calls for family-centered care that is explicitly inclusive of LGBTQ+ families (Sigurdson et al., 2018). Visible signs of inclusion (e.g., inclusive forms, queer-affirming signage, explicit non-discrimination policies) may help with recognition and respect during an already stressful time. In improving inclusivity in family-centered NICU care, the well-being of LGBTQ+ parents and their infants will be supported.
Conclusion
Research is vital to better understand and support the experiences of LGBTQ+ parents of infants in the NICU, given that the transition to parenthood is stressful even in the best of circumstances and LGBTQ+ parents face unique stressors due to stigma and discrimination. We found that LGBTQ+ parents described a complex interplay of both stress and support from a variety of sources. Our results are consistent with existing literature on the challenges faced by all parents with a baby in the NICU, but extends them to LGBTQ+ parents specifically. Our strengths-based findings highlight the supports that may minimize difficulties for parents and children who have experienced the NICU. Some may be specific to LGBTQ+ parents, like advocacy, affirmation, and allyship. Our results inform theory and research, as well as practice among health care professionals and the diverse families they work with in NICU settings.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding for the NICQu Families Study was provided by UL1TR001998/University of Kentucky (UK) Center for Health Equity Transformation (CHET) & Center for Clinical and Translational Science (CCTS) pilot grant. Supported by the National Center for Research Resources & Center for Advancing Translational Sciences (NIH). Additional funding was provided by the UK UNITE Research Priority Area, the UK College of Fine Arts Faculty Research Support Grant, and the UK University Research Professor Award.