
Abstract
This scoping review aimed to summarize the perspectives of survivors of intimate partner violence (IPV) seeking help in rural North America. Using five databases (CINAHL Plus with Full Text, Criminal Justice Abstracts and Full Text, Medline, PsycINFO, SocINDEX), 14 peer-reviewed empirical articles published in English from 2015 to April 2025 were identified. Included articles captured more barriers (e.g., concerns about privacy in rural communities) and fewer facilitators (e.g., experienced providers) to accessing services for IPV. A limited number of articles captured survivors’ perspectives on remote services. More research is needed to understand the experiences of survivors of IPV seeking help in rural areas, especially related to facilitators of accessing services and how remote services impact this experience.
Introduction
Intimate partner violence (IPV) is a significant, worldwide, public health issue. In the United States, over 1 in 3 women report experiencing physical violence, sexual violence, or stalking by an intimate partner in their lifetime (Smith et al., 2018). In Canada, 44% of females aged 15 and over who have ever been in an intimate partner relationship reported experiencing some form of relationship abuse in their lifetime (Cotter, 2021). The impact of IPV across the lifespan has been well documented (Bell et al., 2024), with chronic physical and mental health issues that persist during and after exposure to IPV. Past incidents of IPV and residing in a rural area have both been associated with increased risk of suicide (Stacy et al., 2022). In addition, exposure to IPV is a risk factor that is believed to adversely affect aspects of child development, including executive functioning (Clark et al., 2022). Research on IPV is a vital pursuit due to the prevalence of abuse in relationships and the severe impact IPV has on those who experience or witness it. For this study, the term “survivor” will be applied to anyone who has experienced IPV in the past or present.
The challenges to leaving an abusive relationship are vast, such as the increase in danger when one leaves an abusive relationship, overcoming the subsequent isolation from friends and family during an abusive relationship, and a lack of resources to leave (Women Against Abuse, 2025). While making decisions about how to address violence in a relationship is challenging for survivors in any situation, survivors in rural communities may face unique hurdles. Challenges such as getting help in a geographically isolated community, gaps in resources and services, limited second-stage housing options (i.e., living arrangements between emergency shelter and permanent housing), concerns about confidentiality within small communities (Zorn et al., 2017), and limited availability of needed bandwidth to access supports via the internet (Ndungu et al., 2022) are often reported. Rural providers face challenges related to having smaller budgets, fewer staff, and less access to volunteers than their urban counterparts (Edmond et al., 2020). As such, urban models of care should be adopted with caution in rural areas, given significant environmental differences (Neill & Hammatt, 2015). Further research is needed to understand rural survivors’ experiences of accessing services.
Perceptions of community social norms may affect how individual community members respond to domestic and sexual violence within their communities (Banyard et al., 2020). Compounding factors may challenge accepted community social norms in rural areas, such as increased vulnerability and the risk of comorbid substance misuse (Shannon et al., 2016) among survivors. Ultimately, residing in a rural area may limit a survivor’s ability to end the relationship due to limited support for this decision within their support network (Renner & Hartley, 2022). Thus, more research is needed to understand the barriers and facilitators to accessing services among survivors of IPV in rural areas.
A variety of efforts have been made to facilitate access to services, including the use of trained forensic nurses in underserved communities (Sheeran et al., 2022), the use of interdisciplinary collaboration (Neill & Hammatt, 2015), having staff with sufficient time to build relationships and connections with clients (Rizkalla et al., 2020), and the presence of safe spaces in the community where survivors can disclose their experiences and access support (Beebe et al., 2018). Some professionals believe that the expanded use of telehealth (O’Briant & Clements, 2024), along with other modes of technology, such as phone, email, or messaging (Cortis et al., 2021), and the development of safe online spaces (Ndungu et al., 2022), offer viable solutions to expand access to support in rural communities. However, such technology may present unique challenges, including difficulties assessing the risk of potentially dangerous situations when using remote service delivery methods (Cortis et al., 2021). Other potential challenges include difficulty for older individuals in accessing online sessions (Kautz et al., 2024), challenges in developing rapport remotely (Ndungu et al., 2022), and risks to confidentiality when family members may overhear conversations (Kautz et al., 2024). Yet, more research is needed to understand the impact of the shift toward telehealth and related services from the point of view of survivors of IPV in rural communities.
Findings relevant to IPV, rurality, and barriers and facilitators to accessing support are embedded in the current literature, which suggests these are important yet underexplored topics. While many of the barriers and facilitators may be reflected in the broader literature, it is crucial to recognize how rurality may influence survivors’ help-seeking. To the authors’ knowledge, no reviews capture the current state of the literature on this topic. As a first step, this study conducted a scoping review to answer the research question: In the current literature, what barriers and facilitators are identified for survivors of IPV residing in rural regions of North America to access formal support?
Method
Following Arksey and O’Malley’s (2005) process for scoping reviews, this study is reported in accordance with the PRISMA extension for scoping reviews (PRISMA-ScR; Rethlefsen et al., 2021; Tricco et al., 2018) guidelines. Due to the scoping nature of this review, it was not registered prospectively with PROSPERO (Schiavo, 2019). Guided by the research aim, the related literature was searched for relevant articles, using Covidence (2025) to organize and analyze pertinent data for this scoping review. Included articles were then summarized in Table 1 (Arksey & O’Malley, 2005; Levac et al., 2010). An internal review protocol was developed, shared with the team, and reviewed by a librarian (KK) who provided feedback on the search strategy. Due to the nature of scoping reviews (i.e., an emphasis on providing an overview of the available literature rather than critically assessing it), the quality of the articles was not assessed (Munn et al., 2018). The choice to capture both barriers and facilitators was modeled after a related but distinct review (Muth et al., 2024). In Muth et al. (2024), the authors conducted a scoping review, where they identified barriers and facilitators to implementing harm reduction procedures within shelters, coded them, and further categorized them into subcategories. This study followed a similar analysis plan, extracting barriers and facilitators to survivors’ access to formal supports and further categorizing them. This also guided the presentation of our findings.
Article Characteristics.
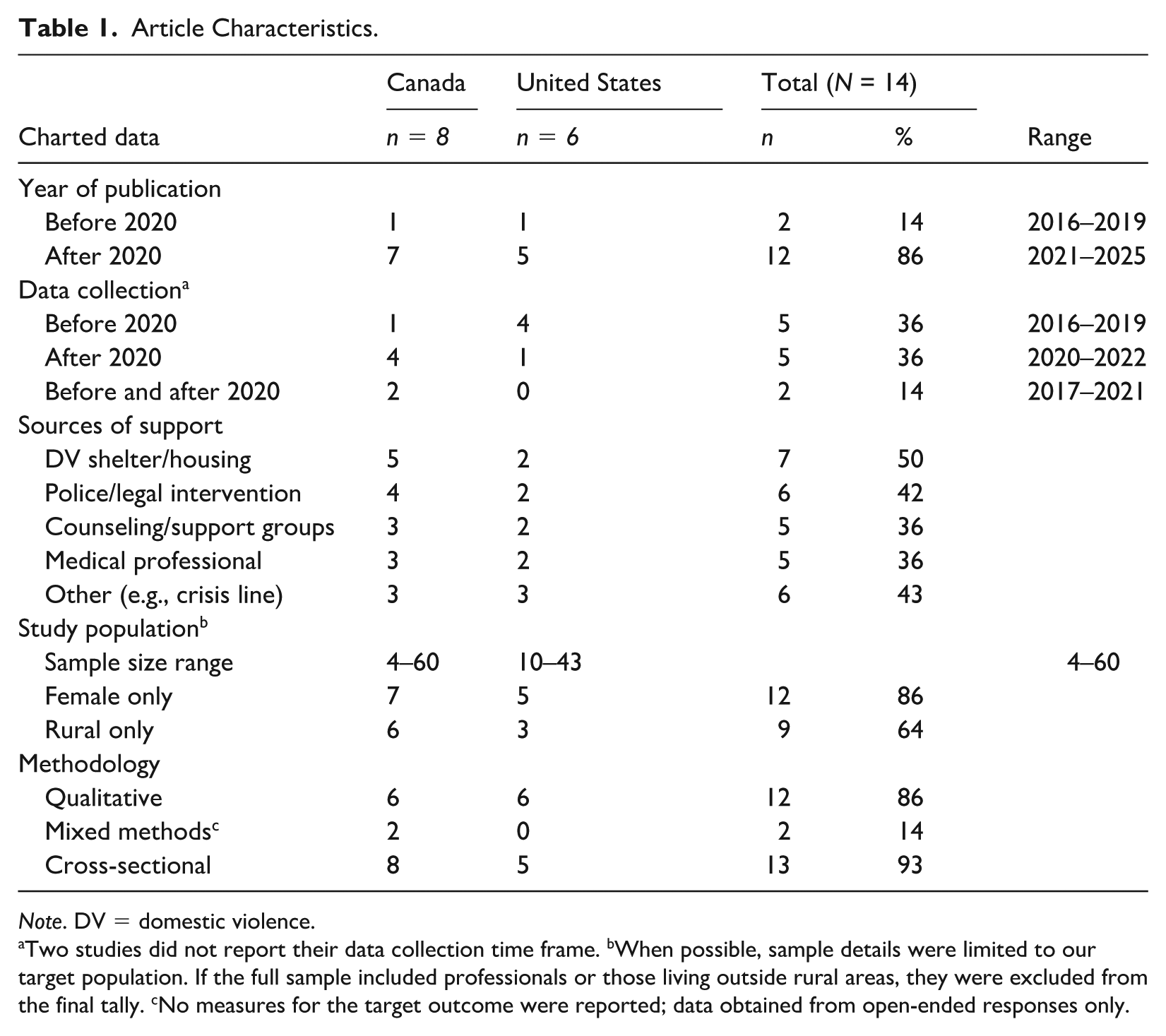
Note. DV = domestic violence.
Two studies did not report their data collection time frame. bWhen possible, sample details were limited to our target population. If the full sample included professionals or those living outside rural areas, they were excluded from the final tally. cNo measures for the target outcome were reported; data obtained from open-ended responses only.
Search Strategy
Five electronic bibliographic databases (CINAHL Plus with Full Text, Criminal Justice Abstracts and Full Text, Medline, PsycINFO, SocINDEX), which capture a broad range of scholarly literature from related fields of study, were searched using the EBSCOhost platform in April 2025. Reference lists of articles that met all inclusion criteria but were systematic reviews were excluded, and the remaining articles were manually screened to identify any additional relevant articles not captured by the original search. To maximize the capture of pertinent literature, search terms were developed using key terms from related literature (e.g., Muth et al., 2024), Boolean operators, and consultation with a librarian (KK) to finalize the search strategy. Key search terms were related to IPV, rural location, and intervention: (“domestic violence” or “domestic abuse” or “intimate partner violence” or “partner abuse” or “intimate partner aggression” or “IPV” or “DV” or “relationship violence” or “dating violence” or “spousal abuse” or “battered women” or “battered wife” or “wife abuse” or “battered females” or “gender-based violence” or “marital violence” or “violence against women” or “sexual violence”) AND (“rural” or “remote” or “isolated” or “regional” or “small town” or “township” or “village” or “countryside”) AND (“interventions” or “strategies” or “best practices” or “treatment” or “therapy” or “program” or “management” or “telehealth” or “telemedicine” or “telemonitoring” or “telepractice” or “telenursing” or “telecare”). Search terms were broad to maximize the capture of relevant articles and allow for flexibility in finalizing the inclusion and exclusion criteria.
Additional filters were applied depending on the database: CINAHL Plus with Full Text, Medline, and PsycINFO were limited to English, academic journals, and years 2015 to present; Criminal Justice Abstracts and Full Texts and SocINDEX were limited to English, academic journals, reviews, and years 2015 to present. The search was limited to English due to the study team’s language fluency. Citation types (e.g., academic journals) were limited to exclude sources that were not empirical or peer-reviewed, such as magazines and guidelines. The search was limited to publications from 2015 to the present to reflect the changing landscape of intervention in rural areas over the last decade, including the expansion of telehealth services and the impact of COVID-19. Duplicates were removed using Covidence (2025) and manually during screening.
Inclusion and Exclusion Criteria
To be included at the screening level, the title/abstract had to (a) be focused on a sample that had experienced IPV, (b) be focused on the experience of the sample with help-seeking and/or related interventions, and (c) be located in a rural area. Rather than setting parameters for what is considered rural, this review included any study that identified a rural population in its dataset. Citations were excluded if they were (a) conducted outside of the United States or Canada to reflect the team’s expertise working with IPV (i.e., all authors are located in North America, with familiarity and expertise in either the United States or Canadian service systems) and benefit comparison across articles (i.e., samples will interact with similar service landscapes), (b) not focused on experiences from a rural setting (i.e., either such geographic details were not reported or findings for a rural sample could not be distinguished), (c) not focused on the survivor’s experience getting support, such as articles focused only on prevalence of IPV were excluded, (d) not describing any barriers or facilitators to getting support, (e) published before 2015, (f) not in English, or (g) not peer-reviewed (e.g., book) or empirical (e.g., commentary) to benefit summarization across a broad range of study designs in a review type that does not appraise the quality of the evidence (Pollock et al., 2023).
Screening and Data Extraction
The inclusion and exclusion criteria were entered separately into Covidence (2025) eligibility criteria, and each citation was screened at the title and abstract levels. The full text was reviewed when inclusion could not be determined at the title and abstract levels. When full text was unavailable, the citation was requested through interlibrary loan at Case Western Reserve University. Each citation was screened by at least two screeners (SB, KK, AW, LJ). Discrepancies at the screening level were reconciled in accordance with the research question and inclusion/exclusion criteria, as guided by the first authors (KK, SB). Once screening was completed, full-text articles of included citations were uploaded into Covidence (2025) and reviewed for eligibility by the first authors (SB, KK).
The data extraction template was developed, pilot-tested, and finalized using Covidence (2025). The data extraction template captured the author, year of publication, study location, details about the study population, aims of the study, methodology, a description of the open-ended questions/measures related to this review’s outcome of interest (i.e., accessing support), and any relevant results for each included citation (Arksey & O’Malley, 2005, p. 27), such as key findings related to a survivor of IPV receiving services. In addition, barriers (i.e., anything that prevents survivors of IPV from receiving help) and facilitators (i.e., anything that supports survivors of IPV in receiving help) of survivors receiving services or seeking help were also tracked. Extraction was conducted independently by three reviewers (SB, KK, AW) and focused on the abstract, methods, and results sections of the included articles. Extraction forms were reviewed by the first authors (KK, SB) before completion. Barriers and facilitators were grouped into levels, categories, and defined, and charted in Table 2, and also summarized narratively. The levels were based on the interaction between the survivor and the surrounding environment. For our review, we group barriers and facilitators into the individual, service, community, and system levels. The individual level reflected barriers and facilitators centered on the survivor’s characteristics or beliefs. Service-level barriers and facilitators related to services available in their community, including the quality of those services. Community-level barriers and facilitators reflected the physical and social environments survivors experienced in their communities. Systems-level barriers reflected the infrastructure that influenced survivors’ experiences seeking formal support for IPV.
Barriers and Facilitators to Accessing Services in Individuals Experiencing Intimate Partner Violence in Rural Areas Across Included Articles (N = 14).
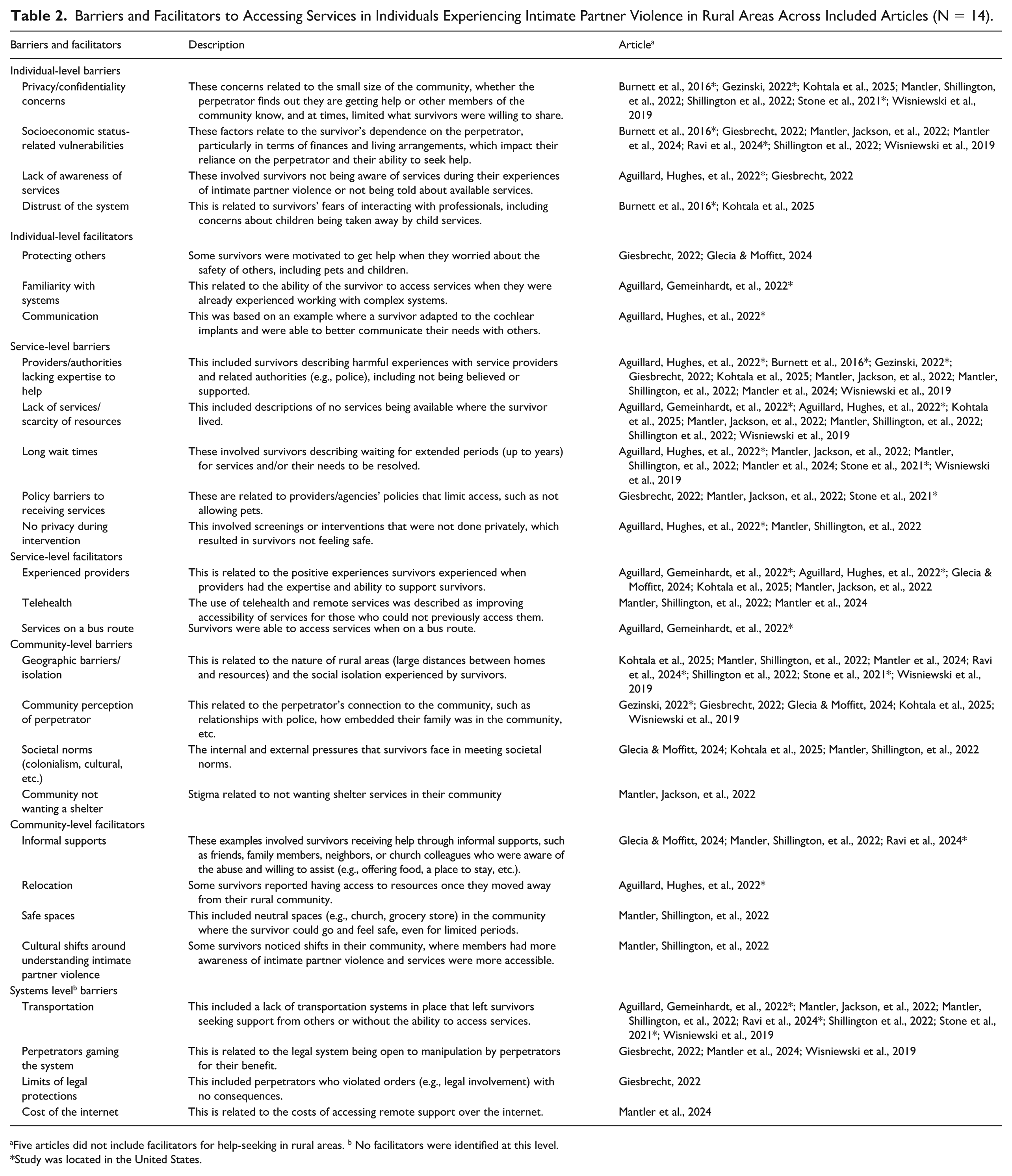
Five articles did not include facilitators for help-seeking in rural areas. b No facilitators were identified at this level.
Study was located in the United States.
Results
A total of 3,463 citations were retrieved from the five databases. See Figure 1 for the PRISMA flow diagram. After applying the inclusion and exclusion criteria, 14 peer-reviewed articles remained. Two sets of articles were based on the same samples (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022; Mantler, Shillington, et al., 2022; Mantler et al., 2024). See Table 1 for a summary of the included articles.
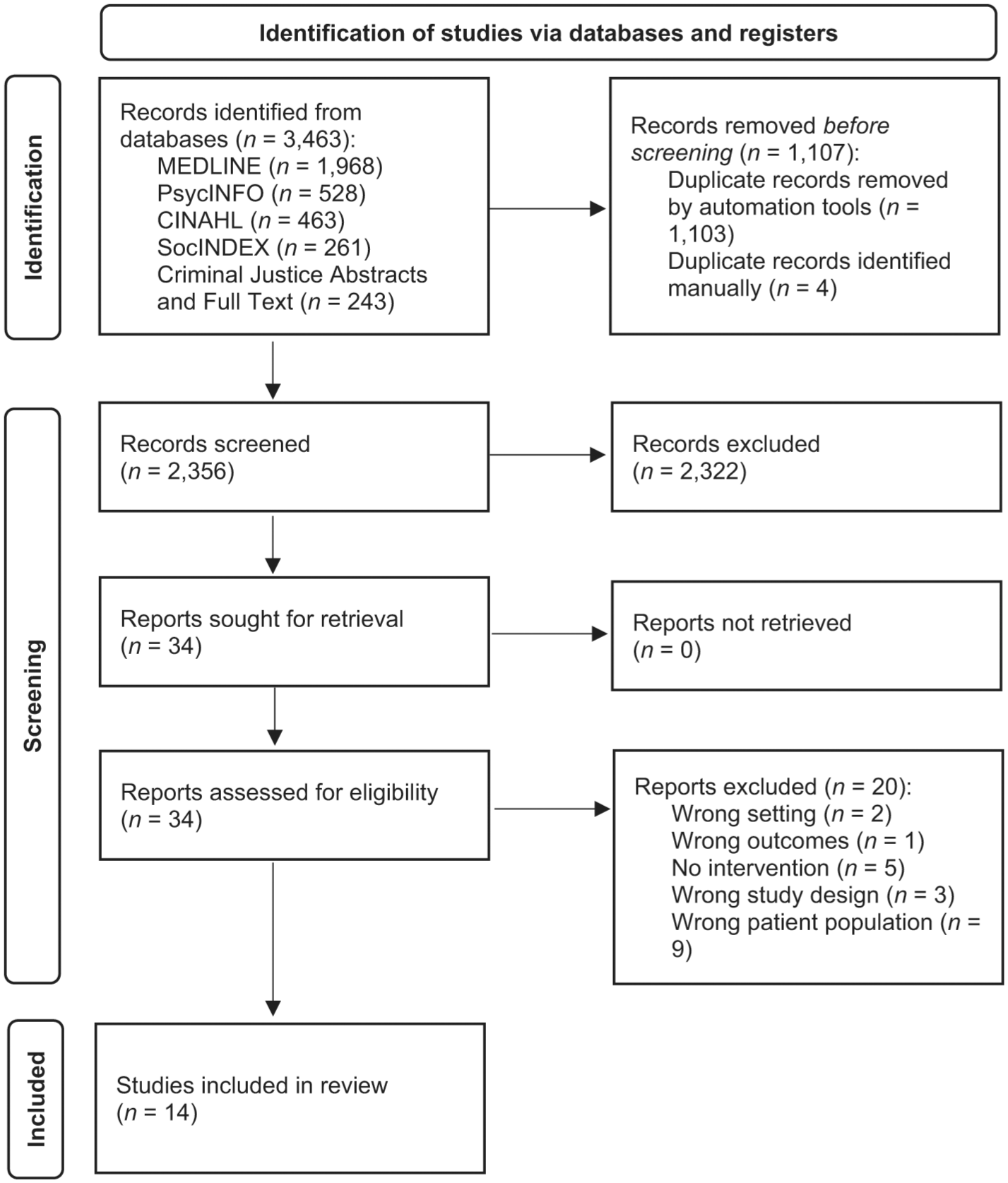
PRISMA flow diagram (Page et al., 2021).
Summary of Included Articles
While most articles (n = 12, 86%) were published after 2020, only seven articles (50%) included data collected after 2020. Only one of these articles captured data from the United States (Ravi et al., 2024). The sample size ranged from 4 (Wisniewski et al., 2019) to 60 participants who had experienced IPV (Giesbrecht, 2022). Most of the included articles (n = 9, 64%) focused on a rural-only sample (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022; Burnett et al., 2016; Glecia & Moffitt, 2024; Kohtala et al., 2025; Mantler, Jackson, et al., 2022; Mantler, Shillington, et al., 2022; Mantler et al., 2024; Wisniewski et al., 2019). Only six of the included studies defined what rurality meant, including four studies that referenced specific population limits of 30,000 people or less 1 (Gezinski, 2022; Mantler, Jackson, et al., 2022; Shillington et al., 2022; Wisniewski et al., 2019) and two mixed sample studies that included communities as small as having 2,000 people (Mantler et al., 2024; Mantler, Shillington, et al., 2022).
The findings summarized and reported in this study were limited to samples that had experienced IPV and were from rural areas. For example, only results under “rural context” were included in the analysis from Shillington et al. (2022) since there was no way to distinguish other findings between their urban and rural subsamples. Sources of formal support varied across articles, with the most common being domestic violence and related housing services (Giesbrecht, 2022; Glecia & Moffitt, 2024; Mantler et al., 2024; Mantler, Jackson, et al., 2022; Mantler, Shillington, et al., 2022; Ravi et al., 2024; Stone et al., 2021).
Most articles were qualitative (n = 12, 86%) and cross-sectional (n = 13, 93%). Two Canadian articles featured mixed methods (Giesbrecht, 2022; Shillington et al., 2022). However, the findings in this study were sourced from the open-ended response data in these mixed methods articles, based on relevance to our study. One article from the United States employed a longitudinal study design (Burnett et al., 2016). Burnett et al. (2016) conducted a qualitative study of 10 rural women who completed six interviews, capturing their lived experiences of IPV during pregnancy and for 2 years postpartum.
The reporting of additional sample details varied across articles. All articles described survivors as either a majority or an all-female sample. One article with a 98% female sample reported one male participant (Giesbrecht, 2022). Two additional articles described their sample as having three “transwomen” (Ravi et al., 2024) or one respondent who “identified as transgender, gender nonbinary, or gender queer” (Stone et al., 2021). Two articles did not describe any further sample details beyond gender (Shillington et al., 2022; Wisniewski et al., 2019). In articles that reported age (n = 11, 78%), ages ranged from 16 to 72. Most articles did not report whether survivors remained in abusive relationships. In the four articles that did, about one in three were still partnered (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022; Burnett et al., 2016; Mantler, Jackson, et al., 2022). Of articles that reported (n = 6, 43%), about half to all survivors reportedly had children (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022; Burnett et al., 2016; Glecia & Moffitt, 2024; Mantler, Jackson, et al., 2022; Stone et al., 2021). Among those who reported (n = 6, 43%), employment ranged from 20% to 75% of the sample (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022; Burnett et al., 2016; Mantler et al., 2024; Mantler, Jackson, et al., 2022; Mantler, Shillington, et al., 2022). Of the two articles that did report sexuality, the majority (65-74%) were heterosexual (Gezinski, 2022; Mantler et al., 2024; Mantler, Shillington, et al., 2022). Except for one article focused on Indigenous mothering (Glecia & Moffitt, 2024), the articles that reported race (n = 11, 78%) were mostly white samples (66-86%). Only two articles from the same study, which explicitly focused on a sample with disability, discussed disability status (Aguillard, Gemeinhardt, et al., 2022; Aguillard, Hughes, et al., 2022).
Barriers and facilitators to formal support are described at the individual, service, community, and systems levels. See Table 2 for a summary of these barriers and facilitators. The individual level describes characteristics of the individual (e.g., lack of awareness of services), including aspects related to their concerns (e.g., distrust of the system) or motivations (e.g., protecting others). The service-level concerned any barriers or facilitators related to services (e.g., experienced providers) or access to services (e.g., long wait times). The community level was related to aspects of the community, including the physical location (e.g., safe spaces) and the people who shared the space (e.g., the community’s preference for not having shelter). System-level barriers concerned aspects of survivors’ experiences that extended beyond service providers or communities to larger systems, such as transportation infrastructure in rural areas. Some barriers and facilitators were related across levels, which reflects the complexity survivors of IPV face as they seek help. Barriers and facilitators are bolded.
Barriers
All articles included a description of barriers to IPV services in rural areas. The most common barriers were identified across locations and encompassed individual, service, community, and system levels.
Individual-Level Barriers
At the individual level,
Service-Level Barriers
At the service level, in cases where
Community-Level Barriers
In addition to the barriers discussed above (i.e., the relationship to individual-level barriers), the impact of
System-Level Barriers
Many survivors described how
Facilitators
Most articles (n = 9; 64%) included a description of facilitators to IPV services in rural areas. Five articles did not highlight facilitators (Burnett et al., 2016; Gezinski, 2022; Shillington et al., 2022; Stone et al., 2021; Wisniewski et al., 2019). However, Stone et al. (2021) did note that when they asked survivors (i.e., participants) about possible solutions, “. . .participants described desiring a group living situation for women in recovery, preferably with supportive IPV services” (p. 40). Facilitators were identified across locations, but only at the individual, service, and community levels.
Individual-Level Facilitators
Only four articles described individual-level facilitators to help-seeking behaviors. This included survivors’ motivation to
Service-Level Facilitators
The most common facilitators were at the service level.
Community-Level Facilitators
At the community level, survivors shared stories of help they received from
Discussion
This scoping review explored barriers and facilitators experienced by survivors of IPV seeking services in rural North America. This review highlighted several key findings. Despite a broad search, only 14 articles were identified that captured perspectives from survivors of IPV in the context of help-seeking experiences. This likely reflects the limited number of studies conducted from the perspective of the survivor on help-seeking and in rural areas, thus highlighting an area of interest that may be understudied. The available literature captured more barriers to help-seeking than facilitators (see Table 2), suggesting a potential need for more emphasis on facilitators to access services in rural areas. Although fewer facilitators were reported, several appeared to directly counter some of the barriers (further described below). However, only two articles captured any related barriers and facilitators to remote services, suggesting more research is needed in this population to understand the impact of telehealth in rural areas. Finally, the diversity in the samples across articles was limited, suggesting a gap in findings for males and certain racial, sexual, and gender minorities in rural areas.
Barriers and Facilitators
Confidentiality concerns, the lack of privacy when seeking help, and geographic location, where everyone knows everyone’s business, were related barriers in rural communities. Some potential related facilitators to overcome these barriers included relocating and telehealth services. While the ability to relocate may be limited, telehealth services have been supported as a viable option in rural areas (O’Briant & Clements, 2024). However, they also come with their own limitations, including privacy and costs. While more nuanced discussions on the pros and cons of telehealth exist (e.g., Jack et al., 2021), this study only identified the costs of internet (Mantler et al., 2024) as a systematic barrier that survivors face in rural communities. Thus, infrastructure is needed to expand access to the internet in rural communities, such as the U.S. ReConnect Program or the currently closed Canadian Universal Broadband Fund, which supported the development of broadband access or high-speed internet in rural areas without access (Government of Canada, 2025; U.S. Department of Agriculture [USDA], 2025). In addition, more investment is needed in programs like the former U.S. Affordable Connectivity Program, which previously increased access to the internet for those struggling to afford it (Consumer and Governmental Affairs Bureau, 2024).
While not specific to rural areas, some efforts were made to adapt existing programs to online formats during the COVID-19 pandemic. Emsley et al. (2023) detailed this process in the United Kingdom, sharing that the efforts widened access to services but also may have reduced engagement. They also noted additional concerns related to safety in IPV situations (Emsley et al., 2023). Similarly, the ADAPT-ITT (assessment, decisions, administration, production, topical experts, integration, testing, training) framework was used to adapt current guidelines for telehealth use to safely recognize and respond to IPV (Jack et al., 2021). Jack et al. (2021) identified a number of ways to prioritize individual physical and emotional safety, which they summarized in Table 3 (p. 594). For example, when scheduling and confirming a telehealth visit, it is suggested to “ask the patient if there is a time when they have access to a quiet, comfortable and private space where other people cannot overhear the conversation. Be prepared that they may not” (p. 594). This preparation may involve alternative ways or places to meet. Guidance for nurses on how to recognize and respond to IPV during telehealth was also provided in Table 4 (pp. 595–596), such as normalizing “the discussion about relationships and health” (p. 595). This suggestion aligns with the National Health Resource Center on Domestic Violence recommendation to conduct universal education and screening for all patients focused on health outcomes related to domestic violence (e.g., CUES; Futures Without Violence, 2025).
The confidentiality concerns described may further relate to the barrier, lack of awareness of services, as survivors may struggle to know who they can privately ask about potential resources in their community. The related literature suggests practices around screening may be helpful, such as making it standard practice to screen all patients in a hospital setting rather than waiting for patients to bring it up or having medical professionals only ask when they have concerns about IPV (Moyer, 2013; US Preventive Services Task Force et al., 2025). In fact, a study focused on rural settings found that health care providers’ knowledge and attitudes did not increase the likelihood of IPV screening, but rather the number of hours of training on abuse and organizational protocols increased the likelihood of IPV screening (Bender, 2016). Thus, emphasis on more training for rural professionals may be one avenue of investment to identify those in need and raise awareness of available IPV services in the community.
In addition, a related facilitator was that survivors with previous familiarity with other complex service systems may be at an advantage in navigating IPV resources in their community. Communities may consider using a resource and referral software system (e.g., Unite Us) that allows direct referrals to nearby agencies serving specific social needs to further facilitate survivor referral needs. Thus, potentially connecting IPV-related services to other service systems in the community could be another way to raise awareness and familiarization with accessing such services. Lack of awareness of services may further be connected to issues of geographic location in a rural area, and the real possibility of a lack of services available. Thus, alternative services such as telehealth and mobile units may be an important way to address this barrier. For example, programs like Ohio Domestic Violence Network’s (ODVN) Care Connection received funding to expand behavioral health referral services for survivors in underserved areas (Ohio Domestic Violence Network [ODVN], 2024).
SES vulnerabilities were related to the essential supports needed as survivors left their abusive relationships in which they had been dependent on their abuser (e.g., Burnett et al., 2016). Those who were reliant on their abuser for transportation often struggled in rural areas that lacked the infrastructure for accessible alternatives (e.g., Mantler, Jackson, et al., 2022). As Aguillard, Gemeinhardt, et al. (2022) explained, this left survivors reliant on others when they “would have preferred to access counseling online, through telehealth, because she had to rely on her family to drive her to appointments, and she was not always able to attend consistently” (p. NP15607). For those who lived in an area with a bus system, finding services on their bus route was essential (Aguillard, Gemeinhardt, et al., 2022). Alternatively, mobile advocacy units may be another option for addressing barriers to services. Mobile advocacy involves meeting survivors in the location of their choosing (Atkinson & Vagi, n.d.; Washington State Coalition Against Domestic Violence [WSCADV], 2025), which can be one way to overcome transportation and related barriers to accessing services.
Some felt stigmatized related to their SES (Burnett et al., 2016), which contributed to further distrust of the system, and struggled to overcome related policy barriers to receiving services (e.g., providing certain documents to access housing supports; Mantler, Jackson, et al., 2022). One facilitator identified that may overcome this barrier was to rely on informal supports; for example, one study of Indigenous women highlighted how informal supports played roles in survivors’ pursuit of safety (Glecia & Moffitt, 2024). Further, programs that tailor services to meet participants’ needs may foster further buy-in to services. For example, Bagwell-Gray et al. (2021) described the adaptation of a web-based safety planning intervention for Native American women exposed to IPV. This online resource could be a useful tool in rural areas and by adapting it to specific populations, it may ensure a more diverse group of survivors can be reached.
For programs that cannot develop their own adapted safety planning tool, practitioners may be able to utilize comprehensive and individualized safety planning tools provided by the National Domestic Violence Hotline (2020), which can be completed with or by a survivor. The most commonly identified facilitator was the impact experienced providers had on the service experience (e.g., Aguillard, Gemeinhardt, et al., 2022). However, many articles described the barriers to providers and authorities in rural areas lacking the expertise to help, which had high consequences, including instances where perpetrators manipulated authorities to their advantage (e.g., Wisniewski et al., 2019). This suggests more training is needed related to understanding the nuances of IPV and also supports the need to expand access in rural areas to providers with the needed expertise, including the possibility of mobile advocacy units that travel farther as well as telehealth services. In addition, these efforts to expand access to services could also potentially address the long wait times that survivors in rural areas experience.
While it was not detailed on how it was accomplished, one article highlighted the benefits a survivor was experiencing due to a cultural shift in their community related to more awareness and understanding of IPV (Mantler, Shillington, et al., 2022). Such shifts in awareness of IPV may potentially address barriers such as community positive perception of perpetrators, cultural norms that pressure survivors to stay in abusive relationships, and communities that push back on having a shelter in their neighborhood.
Strengths and Limitations
As with any scoping review, the interpretation of findings is limited due to the nature of scoping review methodology, which aims to summarize the breadth of evidence on a topic, rather than assess the quality of evidence (Arksey & O’Malley, 2005; Pollock et al., 2023) that is part of other systematic review methodologies. Subsequent reviews may employ other types of review methodology to further evaluate the evidence and capture different facets of related inquiry. In contrast, a strength of this scoping review is that it is believed to be the first review on this topic. Thus, capturing the scope of the available literature can be useful for subsequent scholars to understand the current state of the literature and identify gaps for future research.
Another strength of this review is the use of a team of scholars and practitioners, including scholars with experience conducting scoping reviews (e.g., WW), or expertise in IPV (e.g., AW), as well as current practitioners working with clients experiencing IPV in Canada (i.e., KK) and the United States (e.g., KC). Of particular interest to the team was the impact of telehealth on receiving help in rural areas. This review captured only a small number of articles, which may reflect the inclusion criteria and the goal of focusing on more recent evidence related to the enhancement of remote interventions during COVID-19. Despite this effort, only two articles mentioned telehealth services from the survivor’s point of view in rural areas (Mantler et al., 2024; Mantler, Shillington, et al., 2022), which suggests a gap in the literature on this topic. Thus, more research is needed to understand both the barriers and facilitators to remote services in rural areas from the point of view of survivors of IPV.
The articles in this review capture findings available in English from North America (i.e., Canada and the United States). As a result, findings may not represent barriers and facilitators to receiving help in rural areas in other countries. Subsequent reviewers may consider capturing evidence from a global sample or a broader set of countries. Further, the sample diversity was limited to largely white, non-Hispanic, heterosexual, cisgender females, suggesting findings may not accurately capture the experiences of other identities or cultural contexts. This is an important finding because different communities may have different needs. For example, a related systematic review found that social isolation, a pervasive issue in rural areas, was exacerbated in rural Hispanic American women, resulting in a call for action for the creation of more evidence-based tools to address IPV in underserved communities (Sawin et al., 2017). Therefore, another strength of this scoping review is the identification of this gap in understanding the experiences of rural survivors from diverse backgrounds in the literature. Future studies should consider efforts to capture more diverse samples, including racial, sexual, and gender minorities and males experiencing IPV and living in rural areas.
While some barriers and facilitators may apply to both rural and urban areas, further research is needed to understand the differences between geographic locations. Researchers can support this effort by emphasizing differences in findings between urban and rural areas as well as conducting future research that further captures such differences. This may also include a subsequent systematic review that compares the barriers and facilitators between urban and rural areas to determine differences when overlap exists. Additional longitudinal studies may capture the changes in needs over time, including the impact that variations in funding and services can have on rural communities.
Implications for Practice
While more research is needed, this scoping review suggests some possible implications for practice. Practitioners (e.g., social workers and other professionals working in the field of domestic violence) may consider flexibility in meeting locations, such as having satellite offices in discrete locations (e.g., a doctor’s office) or mobile advocacy units that meet clients at their desired location to increase access and support survivors’ anonymity when receiving services within a rural community. Satellite offices may also offer opportunities to collaborate with an interdisciplinary set of professionals (e.g., physicians, nurses, teachers, ministers of religion) who may serve as first points of contact in rural settings. Due to socioeconomic status (SES) vulnerabilities that act as barriers to treatment, practitioners may need to offer domestic violence housing first/flexible funding initiatives for survivors seeking support to build financial independence from the abuser. Points of first contact and/or social services providers lacking the expertise should either get additional training or refer clients to existing related services, including confidential virtual support groups to provide support/validation for survivors while maintaining privacy. Social workers may advocate for the expansion of private screenings and relevant information provided at all doctor offices, other agencies (e.g., Job and Family Services), schools, motel/hotel rooms, or posted in public restrooms to raise awareness of available services. Social workers may provide generalized education on IPV, such as topics like “how to support a survivor of abuse,” at the community level to contribute to cultural shifts and the potential for more chances of informal support being experienced by survivors. Practitioners should be required to have protocols in place and have alternative providers available to refer potential survivors to in cases where a significant other is also seeking services.
Conclusion
This review highlighted a number of gaps in the literature that can be addressed by future research, including the general need for more research on barriers and facilitators to accessing formal supports with this population, greater attention to facilitators in particular, and investigation with more diverse rural populations. A key finding from this review was the limited peer-reviewed research related to the implementation of remote interventions in rural areas from the perspective of survivors of IPV. Remote services have the potential to address many of the barriers described in rural areas (O’Briant & Clements, 2024). Some included articles also mentioned that survivors wanted access to more telehealth/remote services (e.g., Aguillard, Hughes, et al., 2022). More research in this area could support the development of evidence-informed practices and better implementation of remote services to increase access for more survivors in rural areas. By capturing the perspectives of survivors, it could also capture aspects of implementation that may be missed by professionals and other advocates of remote services.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.