
Abstract
Families face significant barriers to pediatric mental health care due to marginalization and disparities. AI chatbots offer a promising, accessible solution, particularly for underserved areas. However, AI must be integrated as a complementary tool to enhance, not replace, human clinical interaction. AI can mitigate barriers related to social determinants of health, but its adoption requires ethical scrutiny regarding data security, transparency, and biases in training data. Social workers are essential, bringing expertise in program evaluation and clinical service delivery to ensure equitable and culturally responsive implementations. This article proposes an integrated practice-oriented model that positions AI as an associated, provider-driven tool rather than a human replacement. Social workers must take a pivotal role in shaping policies that promote justice, relationality, and systemic change within AI-augmented environments.
Introduction
Child and adolescent mental health have become a substantial public health concern with high rates of clinical mental health diagnosis and suicide-related behaviors continuing to rise. Current data describe 17.4% of youth ages 2–8 years have a diagnosed mental, behavioral, or developmental disorder (National Library of Medicine, 2022). In 2023, data from the National Survey of Children’s Health indicated that the prevalence of diagnosed mental or behavioral health conditions of high school students increased 35% from their previous reporting year (Sappenfield et al., 2024).
Compounding this crisis are significant barriers to accessing care. A shortage of mental health professionals, long wait times, high costs, and social stigma prevent many children from receiving timely and effective treatment (Gallegos et al., 2024; Tingley, 2025). These challenges are often insurmountable for adolescents in rural or underserved areas. Pediatricians provide referrals for mental health services, but many local counseling offices are not accepting new patients (Gallegos et al., 2024; Whitney & Peterson, 2019). The gap between need and access creates an urgent demand for innovative solutions that can provide scalable, immediate, ethical, and evidence-based support. Artificial intelligence (AI), particularly in the form of natural language processing conversational chatbots, has emerged as a promising tool to bridge treatment gaps (Heinz et al., 2025; Inkster et al., 2018; Mehta et al., 2021). A chatbot can simulate human conversation with some designed to connect users with a human resource. Chatbots connect with youth through text, voice, images, or a combination of these methods. There is positive evidence for the use of these tools. Chatbots can provide immediate engagement, act as a steppingstone for youth resistant to traditional therapy, and deliver accessible, evidence-based coping skills around the clock (Hasei et al., 2025). Evidence is emerging suggesting therapeutic chatbots can reduce mild symptoms of depression. Woebot used as a fully automated cognitive-behavioral therapy tool which produced a reduction in depression and anxiety in college age students (Fitzpatrick et al., 2017). Wysa, a mental health support chatbot, demonstrated significant mood improvements among adult users (Inkster et al., 2018). Most evidence within meta-analytical studies focus on young adult or adult populations, creating a paucity of research for pediatric mental health. As recent American Psychological Association (APA) congressional testimony highlights, the integration of chatbots is increasingly viewed as inevitable, making it timely for the field to intervene, assess, and address potential areas of harm to effectively meet youth behavioral health needs (Prinstein, 2025). There is a growing number of accounts where minors have died by suicide following their interaction with chatbots who claimed expertise in mental health to assist these youth (Barry, 2025). Litigation cases involving AI activating self-harm or homicidal ideation, or for causing hypersexualized behaviors within youth using unvetted platforms lacking supervision, regulation, or oversight are occurring (Allyn, 2024; Gold, 2025; Yang et al., 2025). AI offers a solution to the rising need for access to behavioral health in youth, yet caution is needed considering the limited regulation safeguarding the use of this technology in vulnerable populations.
This article argues that AI should be viewed as a complement to human clinicians, a tool that requires careful development with ethical implementation. The primary objective of this article is to provide a practice-oriented framework for ethical AI integration that addresses the current gap in the literature regarding the ethical integration and operationalization of AI in pediatric behavioral health settings. Rather than viewing AI as an autonomous intervention, instead the author identifies the human-in-the-loop model where the practitioner remains central as a facilitator of care. Use of AI within pediatric mental health has become not a question of “if” but a question of “when” and most importantly “how.” It is imperative that social workers foresee the rapid integration of this technology into pediatric health care. Social workers must uphold their ethical responsibility to the profession by advocating for clear, rigorous standards of practice (National Association of Social Workers, 2021). The article identifies strategies to extend a clinician’s reach through an integrated provider-led AI framework, outlining developmentally tailored visual and auditory interventions for emotional literacy, and emphasizing the necessity of preserving the irreplaceable human element in service delivery. Social workers promote human rights and the realization of social justice (National Association of Social Workers, 2021). Without a framework guided by principles of social justice and relationality, AI usage carries significant risks with creating a two-tiered system of care, where marginalized youth receive less developed and monitored algorithm-driven support, while more affluent families gain access to higher quality AI tools combined with access to human practitioners (Victor & Goldkind, 2025). Framed by Bronfenbrenner’s (1979) ecological systems theory, integrated provider-led AI recognizes that children exist within a complex microsystem where parents and caregivers actively seek quality health and social services from the broader community and ecological environment. The interconnectedness of these systems suggests that when AI is integrated as a supportive mezzo-level tool, linking home-based interventions with clinical oversight, it reinforces the protective factors necessary for healthy child development and systemic resilience. The article addresses the need for social workers to play a pivotal role in shaping an AI-augmented future, ensuring that technology enhances rather than replaces the developmentally tailored, culturally responsive care that is fundamental to pediatric mental health.
Implications for Practice: Improving Accessibility and Engagement
AI chatbots offer a multifaceted approach to addressing the systemic challenges in mental health care delivery. The most immediate benefit of AI chatbots is their ability to transcend the geographic and logistical barriers that plague traditional care models. Chatbots can be accessed via smartphone, offering an immediate bridge to care while youth wait for an appointment with a human care provider or as a tool during hours where mental health providers are routinely inaccessible (Tingley, 2025). This 24/7 availability bridges accessibility for a crisis response as the chatbot does not adhere to a standard business schedule. AI is serving as a tool to offer support during hours where mental health providers are routinely inaccessible, positioning chatbots in a support role to reduce Emergency Department admissions bridging care until youth can access their routine care provider. AI also has the position to engage adolescents who are resistant to traditional therapy. Some youth find it easier to be vulnerable and honest with a nonjudgmental and predictable AI, more so than with an adult where they may fear disapproval or misunderstanding (Kitroeff, 2025; Mahajan et al., 2026). AI interaction can provide an emotional vocabulary, building confidence, potentially serving as a steppingstone toward more open communication with a human therapist.
Delivering Evidence-Based Interventions
Generative AI creates distinctive responses with original content, benefiting youth who enjoy created images that bring abstract concepts into concrete forms, supporting a connection with tailored psychoeducation (Sezgin & McKay, 2024). Images within these generative AI models can be personalized to the child, therefore the AI generated imagery can help youth better understand the connection among their thoughts, emotions, and behaviors, assisting the child with new strategies.
AI’s advancements in machine learning (ML) can employ advanced algorithmic methods to solve problems and engage in complex analysis quickly through deep learning. This subset of ML is based on multi-layered artificial neural networks giving rise to promising methods for more accurate diagnosing across health care platforms (Bohr & Memarzadeh, 2020). ML is now being implemented to process massive amounts of intake data to support the provider in making more accurate diagnoses (Char et al., 2020). AI support in data analysis of diagnostic decision-making streamlines documentation for mental health providers as they navigate the demands of higher caseloads.
Modern mental health chatbots are not merely conversational partners; they are increasingly designed to deliver structured, evidence-based therapeutic interventions. Many AI platforms like Woebot, Tess, and Wysa are built on principles of cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), and acceptance and commitment therapy (ACT), teaching users to identify negative thought patterns, practice coping skills, and regulate emotions (Malik et al., 2022; Tingley, 2025). Some generative AI can create visual aids tailored to a child’s specific needs, such as images depicting facial expressions to support emotional literacy building or virtual scenarios for gradual exposure therapy targeting specific phobias or anxiety conditions. Concurrently, parent consultation appointments can be assisted by AI tools to increase parent education and skill building at home. AI can create unique and contextually relevant exercises within child and family therapy making interventions more targeted, accessible, and effective, thereby aligning with the therapeutic goal of personalizing care.
Augmenting Human-Led Care: Integrated Provider-Led AI Framework
Rather than replacing clinicians, AI should function as a powerful assistive tool for pediatric providers. Pediatric mental health service delivery can model integrated provider-led AI frameworks designed to both enhance provider care while tailoring information service delivery to patients (Fawzy Eid, 2024). AI becomes a clinical extender, not a replacement, with its effectiveness entirely dependent on oversight from the social worker. Everyday tasks could be delegated to an AI assistant, allowing a health care provider to focus on more complex clinical tasks, evaluation of data sets, or research evidence-based interventions for integration into upcoming appointments. A chatbot in a united model can help clients with simple supports like remembering to practice skills between sessions, tracking moods, and identifying triggers. This augmented approach views technology as an extension of the clinician’s cognitive and therapeutic capacity, not a substitute (Altamimi et al., 2023). This symbiotic relationship leverages the strength of both AI (scalability, data processing, constant availability) and the human factor (empathy, clinical judgment, relationality) to optimize clinical outcomes.
Social workers can strategically use AI to strengthen the protective factors known to improve adolescent mental health. A social worker could both support development of chatbots which incorporate pillars of health and utilize these chatbots to help a teen set and track goals related to sleep hygiene, nutrition, or other activities of daily living targeting goals which improve a healthy lifestyle for mood regulation. AI-driven role-playing scenarios can be employed to help teens practice communication skills with their parents, strengthening family connection, while simultaneously infusing parental monitoring. AI can become a tool supporting wellness and resilience within the adolescent’s existing social ecosystem.
Integrated provider-led AI frameworks function as a feedback loop where the social worker is the main architect with a clear practitioner role acting as a human-in-the-loop, responsible for content validation, monitoring algorithmic bias, and interpreting AI-generated data through a clinical lens. Social workers review and monitor system-level safeguards ensuring ethical technical requirements are met such as end-to-end encryption, automated alerts for safety concerns, and the integration of AI transcripts into legal health record keeping for transparency. Finally, an integrated provider-led framework maintains rooted social work values, implementing social justice and relationality to prevent a two-tiered system where technology replaces human care for marginalized youth.
Ethical Imperatives and the Role of Social Work
Despite its potential, the deployment of AI in pediatric mental health is fraught with ethical challenges that align directly with the core tenets of social work: Social justice, the dignity and worth of the person, confidentiality, and the importance of human relationships (National Association of Social Workers, 2021).
The Risk of a Two-Tiered System: Social Justice
Deepening health disparities due to unregulated AI adoption is a real concern (Novak et al., 2018). A divided digital redlining system is emerging where affluent families retain access to superior, specialized human practitioners, while marginalized populations are relegated to lower-quality automated service models driven by algorithms (Victor & Goldkind, 2025). Social work, with its mandate to challenge social injustice, has an ethical obligation to advocate for policies and implementation frameworks that prevent this digital stratification of care (National Association for Social Workers, 2021).
Bias, Privacy, and Safety
Bias
AI systems are only as good as the data they are trained on. If training datasets are not representative of diverse populations
Privacy & Safety
The National Association of Social Work (2021) clearly identifies ethics of care for social workers, driving their responsibility to clients and the broader society. Social workers must act to advocate for policy changes which aide developers in strengthening encryption options to prevent unauthorized access to personal health information (Reamer, 2025). Many AI systems do not adequately address how sensitive user data will be used, raising concerns about protected health information becoming exploited for commercial purposes (Gallegos et al., 2024). Alongside privacy, safety is a critical issue. While some apps have protocols to detect suicidal ideation and provide crisis resources (Esmaeilzadeh, 2025), the protocols are not consistently applied, and many AI tools lack the ability to identify homicidal ideation and mandatory reporting concerns (White, 2018). Open AI, which oversees the programming of ChatGPT, describes protocols and safeguards specifically for teens who are experiencing suicidality (Altman, 2025). Yet crisis support for suicidality is often nuanced and not easily coded with simple identification words or phrases. In addition, loopholes embedded within AI systems have allowed teens to discover very detailed information about suicide methods, while failing to encourage the teen to seek support from family members (Clark, 2025; Kitroeff, 2025). This type of engagement with a client would be unconscionable for a health care professional. The loophole clearly violates core social work ethical principles regarding client safety and the worth and dignity of a human life (National Association of Social Workers, 2021). These gaps highlight the danger of relying on automated systems in crisis situations where nuanced human judgment is indispensable.
The Irreplaceable Human Element
At its core, psychotherapy is a deeply human endeavor built on trust, empathy, and the therapeutic alliance. AI, in its current form, attempts to simulate these qualities, creating an illusion of compassion or empathy. Large language models have a history of sacrificing truthfulness to align with a user’s viewpoint or perspective, turning a conversation toward a sycophantic exercise, rather than challenging a client’s thinking (Kitroeff, 2025; Naddaf, 2025). This is particularly critical in pediatrics, where a clinician must provide developmentally tailored interventions, build rapport with both the child and their caregivers, and navigate complex family systems to challenge and reshape behavior within the micro and mezzo level. The social work profession’s emphasis on relationality and a person-in-environment perspective underscores that effective care cannot be decontextualized or reduced to an algorithm. Rather, the child’s experience of connection with their provider who is bearing witness to verbal or nonverbal creative expression serves as the driving protective resource for posttraumatic growth and resilience (Pliske et al., 2021).
A Framework for Ethical AI Integration: The Social Worker as Architect and Evaluator
Harnessing AI’s benefits while mitigating its risks requires social work to take an active role in the design, evaluation, and oversight of these technologies. The goal is not to resist innovation but to steer it toward equitable and humane outcomes. One viable path forward is an integrated model where AI serves as a powerful tool actively employed by a human provider. The integration of AI into pediatric health care can be modeled after pioneering educational frameworks like Khanmigo, which utilizes a Socratic, human-in-the-loop approach to ensure the technology functions as a scaffold for child development rather than a replacement for professional expertise (Khan Academy, 2025). Just as Khanmigo empowers educators by automating administrative tasks while requiring them to audit and validate AI-led student interactions, the pediatric social worker acts as the clinical architect, ensuring AI remains a transparent, safe, and developmentally appropriate adjunct to the therapeutic process. This framework has the provider remain the central facilitator of care, supervising the AI integration. For example, social workers can employ expressive arts through generative AI to create personalized visual or auditory props for younger learners to better integrate emotion regulation into daily experiences. Client use of the AI is reported directly back to the clinician, ensuring necessary oversight. Technology harnessing the power of AI has the potential to help the social worker engage in research informed practice through collecting client data to inform treatment planning or assist in thematic analysis of client work.
Program Evaluation and Policy Advocacy
AI in pediatric settings necessitates policy on how to evaluate its interactions with young users. Youth development is deeply rooted in social context. The thoughts, behaviors, and emotions a child carries into adulthood are forged through interpersonal exchanges during childhood (Prinstein, 2025). Consequently, policy frameworks must adopt an integrated, provider-led approach that views AI not as an autonomous agent, but as a monitored mezzo-level tool designed to bolster the human connections between parents, peers, and clinicians that drive a child’s maturation. Developing clear guiding principles for ethical guardrails, policies, and systematic evaluation of the implementation of AI programs positions AI as a supplement, not a substitute, allowing the clinician to maintain the therapeutic relationship while leveraging technology to extend their reach and enhance their effectiveness. Pediatric clients interacting with AI chatbots independently, without oversight or guidance from a clinical care team, risk the AI’s known problems of hallucinations and spiraling as long conversations unfold between the user and large language model chatbot (Hatem et al., 2023; Jones, 2025; Kitroeff, 2025). Social work can lead committees charged with establishing governing policy and procedures around pediatric AI use. A standard of care with guidelines for ethical AI use in clinical practice requires knowing how the tools function over time. This monitoring of a program’s safety simultaneously gathers insight for legislative policies to build regulatory action.
Some states are already acting to respond with legislation identifying safety concerns of AI within pediatric behavioral health. Illinois and Nevada have both passed legislation prohibiting or limiting AI use in mental health and behavioral health care (Assembly Bill 406; Wellness and Oversight for Psychological Resources Act, 2025). A code of ethics governing behavioral health would orient its practice around beneficence. Considering many AI models are owned by corporations who have a vested interest in profitability, behavioral health can be at odds with both the process and product of this technology. The capability of developing an AI model approved by health care professional organizations working within the confines of new and upcoming legislation can be integrated within already existing electronic record keeping platforms. Integration of a pathway toward ethical review, safety, and data security solutions is a first step. Social workers must assess the benefits and risks of technology by evaluating service delivery functions and their impact on clients. Consequently, practitioners must remain increasingly cognizant of state-level AI regulations, particularly when providing care across state lines through licensing compact agreements (National Association of Social Workers et al., 2017).
Integration of AI into an established health record keeping system can offer tools for ease of clinical record keeping, currently allowed in all U.S. states. Social workers may decide to offer the use of large language models or other generative AI tools within their practice settings, however additional safeguards including an AI alert to the health care team regarding client use and concerns related to their safety is warranted. Transcripts uploaded of the encounters between the client and AI platform will support documentation and charting practices of the AI team member within the legal record, giving greater transparency to the health care community regarding how the AI is conversing with and potentially advising their patients.
Privacy and Confidentiality
Regulations for AI usage in behavioral health need a diverse set of developers including experts from public health, social work, computer science, engineering, organizational payer administrators, and patients or guardians. More than 30 years ago, the U.S. Congress needed to act to create a law regulating confidentiality standards in the health care setting (Health Insurance Portability and Accountability Act (HIPAA), 1996). These HIPAA protections served to safeguard data transmission and confidentiality for patients in health care settings. Considering the concerns raised regarding data privacy in AI applications (Balthazar et al., 2018; Luxton, 2014) and confidentiality (National Association of Social Workers et al., 2017; Yew, 2021) social workers can engage developers in legislative action which supports AI implementation and usage within vulnerable populations. These frameworks must mandate data security, require transparency in how algorithms work, and create reimbursement mechanisms that incentivize integrated, human-led care rather than a complete substitution with cheaper, automated solutions.
Integrated Provider-Led AI Framework: Guiding Principles
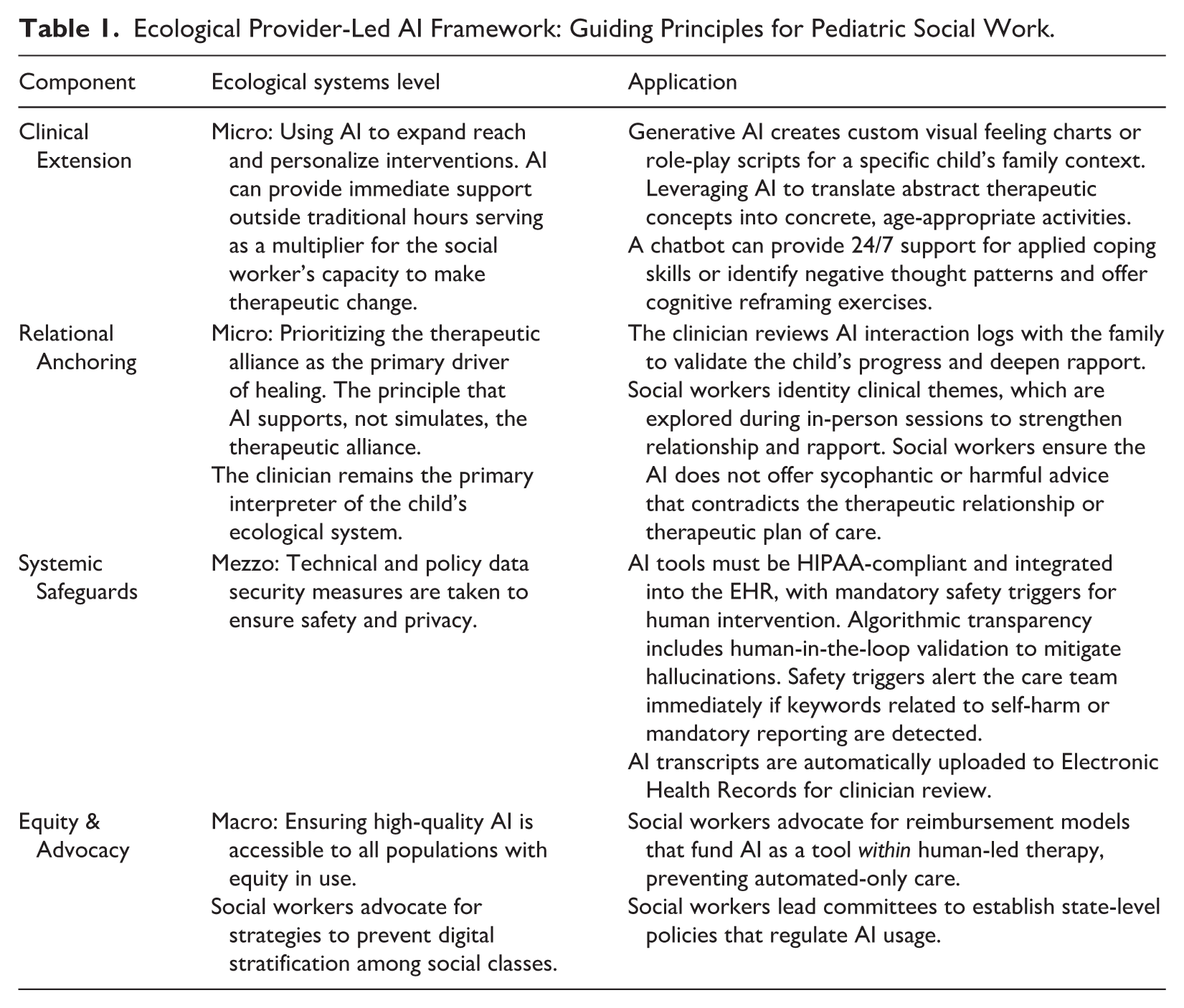
An ecological provider-led AI framework (see Table 1) can guide decision-making and application. A child presenting with emotional dysregulation can have personalized visual aids created by the mental health provider in partnership with their AI tool during the session to ground abstract concepts in concrete exercises. Between sessions, the AI functions as a digital bridge, tracking the child’s mood and providing evidenced-based coping skills. If the AI detects high-risk language, a predefined safeguard triggers an immediate alert to the clinician, ensuring that a human expert, not an algorithm, manages the crisis response. Finally, social workers need to maintain oversight of quality and compliance in technology-based record keeping, while actively advocating for regulatory frameworks (National Association of Social Workers et al., 2017).
Ecological Provider-Led AI Framework: Guiding Principles for Pediatric Social Work.
Discussion and Future Directions
AI is poised to transform the landscape of pediatric mental health. Chatbots and other AI iterations present a powerful opportunity to democratize access to care, engage youth on their own terms, and deliver personalized, evidence-based support at an unprecedented scale. However, this technological promise is shadowed by profound ethical risks, chief among them the potential to create a digital divide that leaves the most vulnerable youth with substandard, algorithm-driven care. AI chatbots should not be viewed as a replacement for professional human providers but as a tool to augment their work. The future of effective and just mental health care lies in a collaborative, human-in-the-loop model that marries the efficiency of AI with the irreplaceable empathy, wisdom, and relational skills of the clinical social worker. To achieve this, the social work profession must move beyond the role of a passive user and become an active architect of this new reality. This requires urgent, organized efforts among clinicians, researchers, academic institutions, and funding agencies to conduct rigorous, long-term research on AI’s effectiveness and to develop robust ethical guidelines and policies that protect patients. By embracing this role, social workers can ensure that technology serves as a force for equity, connection, and healing, shaping a future where every child has access to the high-quality mental health care they deserve.
Footnotes
Disposition editor: Cristina Mogro-Wilson
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.