
Abstract
Objective:
To evaluate cannabidiol (CBD) in pediatric patients with autism spectrum disorder (ASD), fluent verbal language and an estimated full-scale IQ of 80 or above.
Background:
Preliminary evidence suggests CBD may ameliorate challenges associated with ASD. Whether CBD benefits pediatric ASD without accompanying intellectual or language impairment remains unknown.
Methods:
We enrolled 23 participants, ages 7.8–17.8 (Mean [M] = 11.3 ± 2.8) with ASD and IQ ≥ 80 in a 6-week Phase-2 open-label trial of ≥98% CBD (Epidiolex®, 100 mg/mL) at 3, 6, or 9 mg/kg/day using a Bayesian optimal interval dosing design. The primary endpoint was the CBD dose associated with the highest response rate (i.e., Clinical Global Impression Scale-Improvement [CGI-I] score = 1 or 2) on a target symptom domain designated individually based on informant report, standardized scales, and clinical observation. Secondary endpoints were effect sizes of changes from baseline in measures assessing ASD core and associated symptoms, and global functioning. Adverse events (AEs) were assessed weekly. Plasma CBD levels and clinical labs were obtained at the final visit.
Results:
All 23 enrolled participants completed the trial. The highest response (62%) was observed at 9 mg/kg/day (N = 8). Overall, 10 of 23 patients (44%) were responders. Response varied across domains: Irritability/Tantrums (N = 5, 60%), Social (N = 8, 50%), Anxiety (N = 5, 40%), Restricted, Repetitive Behaviors (N = 4, 25%), and Sleep Problems (N = 1, 0%). Dose correlated with individualized CGI-I (r = −0.42, N = 23, p = 0.04).
Individualized domain CGI–Severity scores improved from pre-(M = 4.6 ± 0.5) to post-(M = 3.9 ± 0.8) treatment, t(22) = −4.36, p ≤ 0.001; d = 0.91; 95%CI [0.37,1.03]. Social Responsiveness Scale-2 Total-Score (SRS2-T) had the largest effect size (p ≤ 0.001; d = 1.36, 95% CI [0.78–1.93]).
Of 222 reported AEs, 27 unique AEs were considered treatment-related. Most AEs (93%) were mild and expected (82%); none was severe. The most frequent related AEs were increased salivation (30%), increased sleep duration (39%), sleepiness/sedation (26%), increased dream activity (35%), and polyuria (22%). Vital signs, physical exams, weight, liver function tests, and complete blood counts were unaffected. CBD plasma levels did not correlate with response.
Conclusions:
In this preliminary study, CBD was well tolerated; AEs were mild–moderate. Mean SRS2-T and subscores decreased significantly with large effect sizes, shifting from the severe to the moderate range.
Clinical Trial Registration:
ClinicalTrials.gov Identifier NCT03900923.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by social communication challenges and restricted, repetitive behaviors (Lord et al., 2018) with an estimated prevalence of 1 in 31 children (Shaw et al., 2025). There are no evidence-based pharmacologic treatments for core ASD symptoms. Aripiprazole and risperidone are FDA-approved to treat irritability, but can cause substantial adverse events (AEs) (Farmer et al., 2013). Anxiety and sleep difficulties are also common and burdensome. ASD often co-occurs with intellectual disability, speech and language delays, attention-deficit/hyperactivity disorder, and depression (Hodges et al., 2020). Given the substantial clinical needs, polypharmacy is common despite a lack of supporting evidence (Ritter et al., 2021).
Cannabidiol (CBD), a nonpsychoactive derivative of the Cannabis sativa plant, may be a promising treatment for core and associated ASD symptoms. CBD is FDA-approved to treat seizures in patients with Lennox–Gastaut syndrome, Dravet syndrome, and tuberous sclerosis complex based on pivotal Phase 3 placebo-controlled clinical trials in which common adverse events were generally mild-to-moderate in severity. CBD targets mechanisms implicated in ASD, including synaptic excitatory/inhibitory imbalance (Pretzsch et al., 2019; Rosenberg et al., 2023; Nelson and Valakh, 2015; Tsien and Rosenberg, 2025; Zhang et al., 2023). CBD reduced anxiety-like behaviors in mice (Assareh et al., 2020) and decreased public speaking-related anxiety in healthy human adults (Bergamaschi et al., 2011; Zuardi et al., 2017). In a retrospective study, CBD improved communication, anxiety and disruptive behaviors in children with ASD (Aran et al., 2019). In a double-blind trial of 20:1 CBD:tetrahydrocannabinol (THC) in 150 children with ASD and moderate or severe behavioral problems, CBD-THC produced a significant benefit on Clinical Global Impressions Scale-Improvement (CGI-I) but not on the other primary outcome measure, the Home Situations Questionnaire-ASD (Aran et al., 2021). This ambiguous result, concerns regarding potential deleterious effects of THC in youth, and the availability of an FDA-approved pharmacologic grade CBD prompted us to assess this formulation in children with ASD. A review of all trials to treat ASD patients listed in ClinicalTrials.gov (August 2024) found insufficient evidence of efficacy and safety for most trialed compounds, including CBD (Persico et al., 2025). A double-blind crossover placebo-controlled trial of pharmacologic-grade CBD in 39 autistic boys with severe behavior problems found 2/3 improved on CBD, but a strong placebo response obviated statistical separation of the treatments (Trauner et al., 2025). In both CBD–THC and CBD controlled trials (Aran et al., 2021; Trauner et al., 2025), study medication was generally well tolerated. Here, we assessed children or adolescents with Level 1 ASD who were verbally fluent, had an estimated IQ > 80 and no seizures to limit heterogeneity and avoid confounding from possible improvements in seizures. Our aims were to address feasibility/tolerability, dose-finding, and preliminary signals by symptom domain for future trials. Families identified their preferred primary treatment target. Given possible inverted-U dose-dependent effects of CBD in other contexts (Bergamaschi et al., 2011; Zuardi et al., 2017), we sampled several doses in this pilot open-label trial.
Methods
Study design
This was a single-center, single-group, open-label, Phase-2 clinical trial in ASD patients aged 7–17.9 years old with fluent verbal speech, and an estimated full-scale IQ ≥ 80. The study protocol was approved by the NYU Langone Institutional Review Board to consent up to 30 participants. The trial was conducted at the NYU Langone Child Study Center from January 2020 to May 2023 and was completed in accordance with the Declaration of Helsinki. Written informed consent and assent were obtained from all caregivers and participants, respectively. We recruited through IRB-approved electronic communications to parents of children diagnosed with autism in the NYU Langone Health database and by posting the study on ClinicalTrials.gov (NCT03900923).
Total duration of subject participation was 8–10 weeks, with telephone prescreening, screening visit, and a treatment phase of 6 weeks. Except for the first participant, who completed treatment before the COVID-19 shutdown, in-person visits were limited to initial and close-out visits, with other visits conducted via secure email and/or phone (on alternating weeks) to assess for adverse events. Figure 1 details the study design.
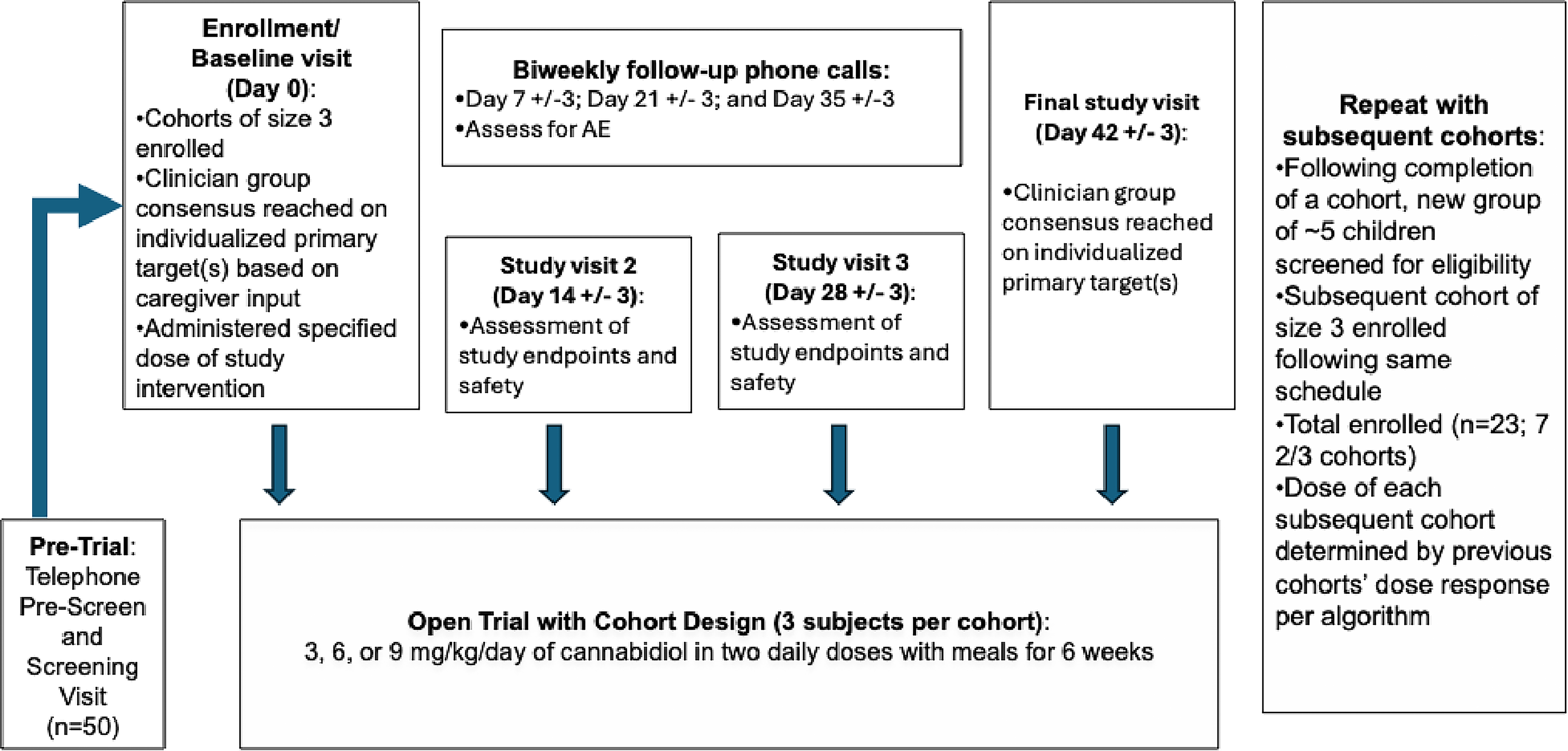
Open-label cannabidiol study design. Study flow chart and design.
We administered ≥98% pure CBD 100 mg/mL oral solution, Epidiolex®, provided at no cost by Jazz Pharmaceuticals, Inc. Adherence to treatment protocol was assessed by participant drug log with dose and time of administration recorded by the caregiver. Caregivers were counseled to administer CBD at meals (breakfast and dinner) with preferred foods with ample fat content to improve CBD absorption.
An adaptive Bayesian optimal interval (BOIN) design was used to increase sensitivity in capturing a nonlinear dose response (Yuan et al., 2016). Participants were assigned to cohorts (N = 3), which received doses of 3, 6, or 9 mg/kg/day for 6 weeks, depending on the treatment response of prior cohorts. The “optimal” dose was defined as the dose at which the largest proportion of participants responded (detailed in Supplementary Data).
Participant eligibility
Inclusion criteria
Eligible participants were male or female pediatric outpatients with a Level 1 ASD diagnosis confirmed by either the Childhood Autism Rating Scale Second Edition, High Functioning Version (CARS-2-HF) (Schopler et al., 2010) or the Autism Symptom Interview (ASI) (Bishop et al., 2017), and DSM-5 criteria (American Psychiatric Association, 2013) ascertained by licensed clinical psychologists with substantial expertise in ASD evaluation (P.E.C., R.A.S.). Participants were required to have verbal fluency, normal physical exam, laboratory tests of hepatic (alanine aminotransferase, aspartate aminotransferase and γ-glutamyl transferase) and hematologic (complete blood count) functioning within normal limits for age, estimated IQ score ≥80, Social Responsiveness Scale, Second Edition (SRS-2) Total T-score ≥66, and a CGI-S (Busner and Targum, 2007) score ≥4 on an individualized target symptom domain identified at baseline by clinician consensus from informant report, rating scales, and clinical observation.
Exclusion criteria
An active seizure disorder, history of epilepsy, known genetic developmental disorder (e.g., Rett Syndrome), Childhood Disintegrative Disorder, bipolar disorder, psychosis, schizophrenia, post-traumatic stress disorder, active suicidality, pregnancy, lactation, drug abuse (e.g., cannabis use) in past 3 months, or any other condition impacting participation ability, interfering with study conduct or confounding data interpretation, or endangering well-being were exclusionary.
We excluded patients using any medication metabolized primarily by CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP3A4, or CYP2D6 isoenzymes, exposed to any investigational agent in the 30 days before trial initiation, or cannabinoid treatment within 2 months. Subjects were ineligible if they underwent changes in nonexclusionary psychotropic medications, allied health therapies, behavioral or educational interventions within 4 weeks prior to trial initiation. Laboratory screening was conducted to exclude those with evidence of impaired liver dysfunction, pregnancy, or urine drug screen positive for THC, opiates, methamphetamine, or cocaine.
Lifestyle considerations
During the study, participants were asked to refrain from changing allied health therapies, behavioral or educational interventions, and any nonexclusionary psychotropic medication regimen. They were also required to abstain from illicit drugs and agree to use contraception if sexually active.
Data collection
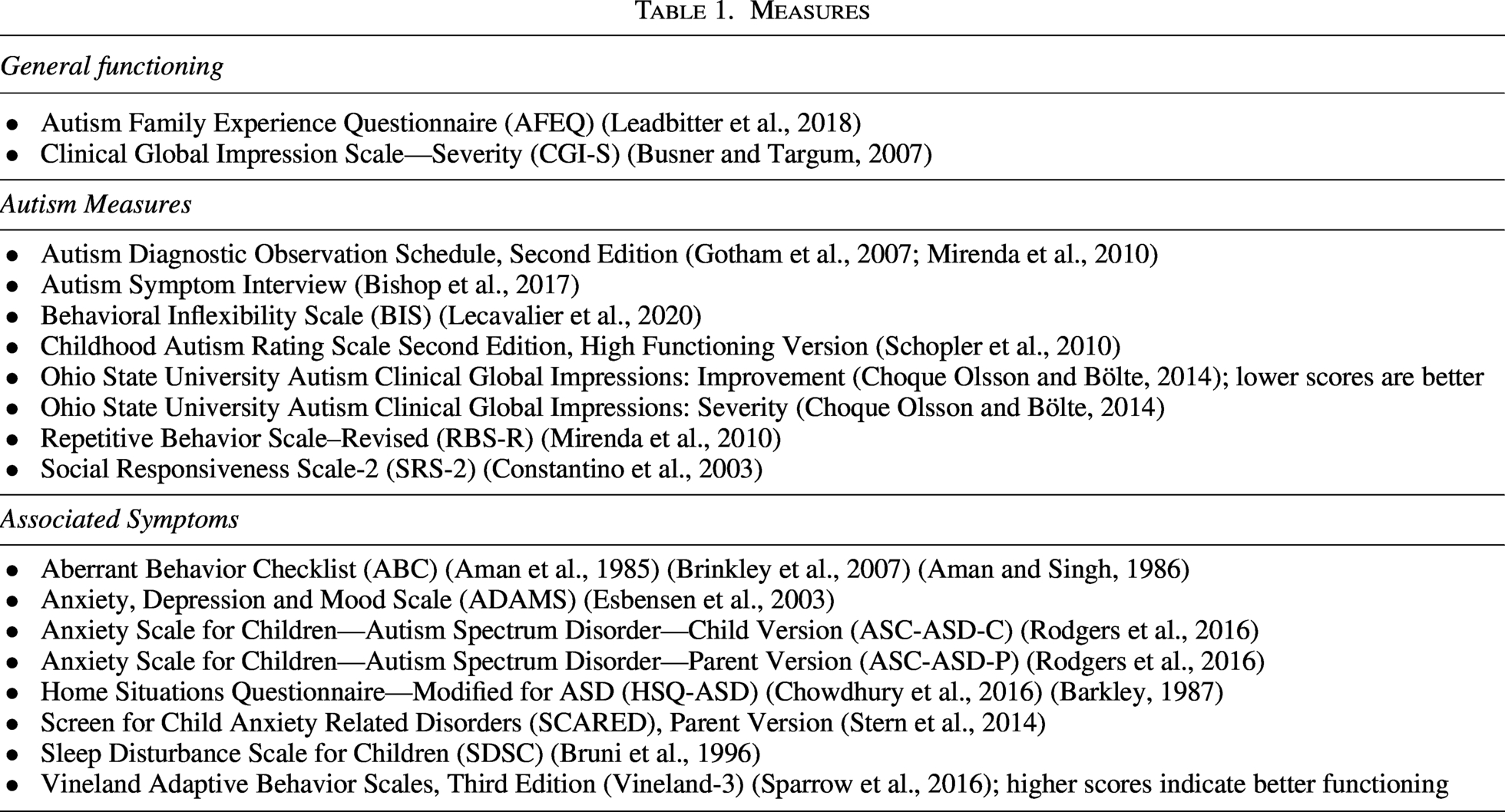
Data collected at scheduled 2-week intervals measured core and associated ASD symptoms and assessed drug safety (weekly) (See Table 1). A web application, Research Electronic Data Capture (REDCap), compliant with the U.S. Code of Federal Regulations, Title 21, Part 11, was used for data collection and management. In response to COVID-19, all screening procedures and assessments (excluding physical exams and blood testing to monitor safety) were conducted via secure virtual teleconferencing. Plasma CBD trough levels were obtained at approximately 5:30 pm at the end of the final in-person visit, that is, 9–10 hours following the final CBD morning dose, in the first 19 participants (analyses were conducted in the Cooper Lab at the Nathan Kline Institute for Psychiatric Research, which closed upon Mr. Cooper’s retirement).
Measures
Primary outcome
Treatment response was individualized for each participant, defined as change in a predetermined target symptom cluster considered most interfering at study outset. Participants who scored 1 or 2 (very much or much improved) on the Clinical Global Impression Scale—Improvement (CGI-I) (Busner and Targum, 2007) for their individualized primary outcome variable were classified as responders, whereas those who scored ≥3 (minimally improved, unchanged or worse) on the CGI-I scale were considered nonresponders. CGI-I scores were determined by clinician consensus (R.A.S., P.E.C., F.X.C.). Response rate was the proportion of responders.
Secondary outcomes
Secondary endpoints included scales assessing general functioning, core ASD symptoms, and symptoms associated with ASD (Supplementary Table S1).
Safety monitoring
Safety was assessed using AE reporting, the Columbia-Suicide Severity Rating Scale (C-SSRS) (Posner et al., 2011), and laboratory tests of hepatic and hematologic functioning at baseline and trial end. We assessed AE at weeks 1, 3, 5 by coordinator phone calls to parents, and at weeks 2, 4, and 6 via the UKU Side Effects Rating Scale—Patient Version-5 (Lindström et al., 2001) reported by caregivers and children to a licensed clinical psychologist. Clinician consensus determined the relatedness of AEs to treatment.
Statistical analyses
No statistical methods were used to determine the study sample size. All participants, regardless of treatment response, were included in the analysis datasets, to descriptively examine effects at varying doses as well as safety and tolerability across the entire sample. Demographic characteristics and baseline measurements were summarized using standard descriptive statistics. Cohen’s d effect sizes and 95% confidence intervals are reported for all measures at baseline and at final visit; there were no early terminations. We performed paired t-tests and Pearson correlations; p values < 0.05 were considered statistically significant, without correction for multiplicity given the preliminary nature of the study. Safety endpoints were analyzed as summary statistics. All AEs were analyzed and reported in terms of severity, frequency, and relatedness.
Results
Screening and enrollment
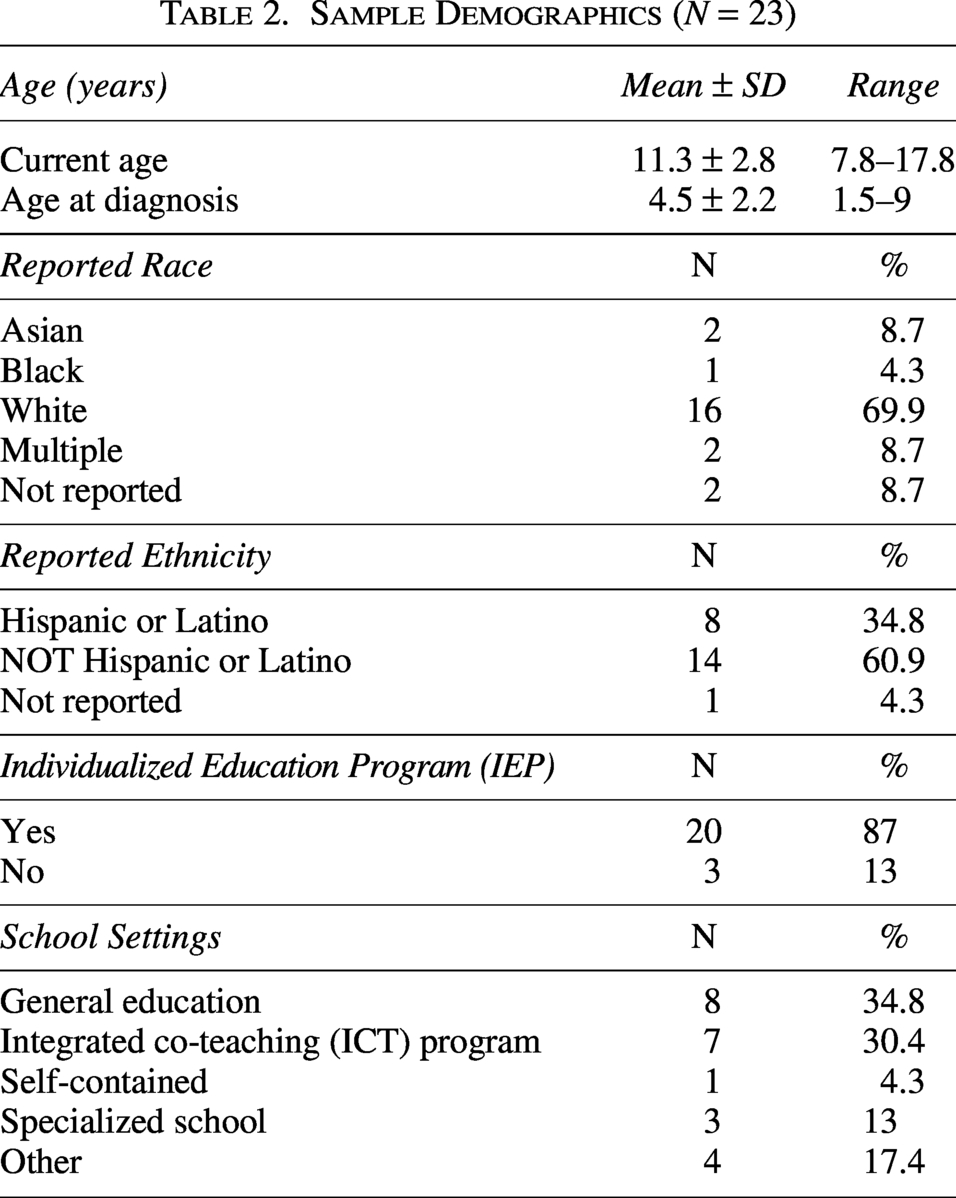
Thirty children were consented for screening with parental consent and child assent, as applicable. Three had SRS-2 Total T-Score < 66, three did not complete screening, and one declined hematologic testing. Twenty-three participants entered and completed the trial (22 males and 1 female; 21 met criteria for >1 additional psychiatric diagnosis [Table 2 summarizes demographics]).
Sample Demographics (N = 23)
Baseline measures
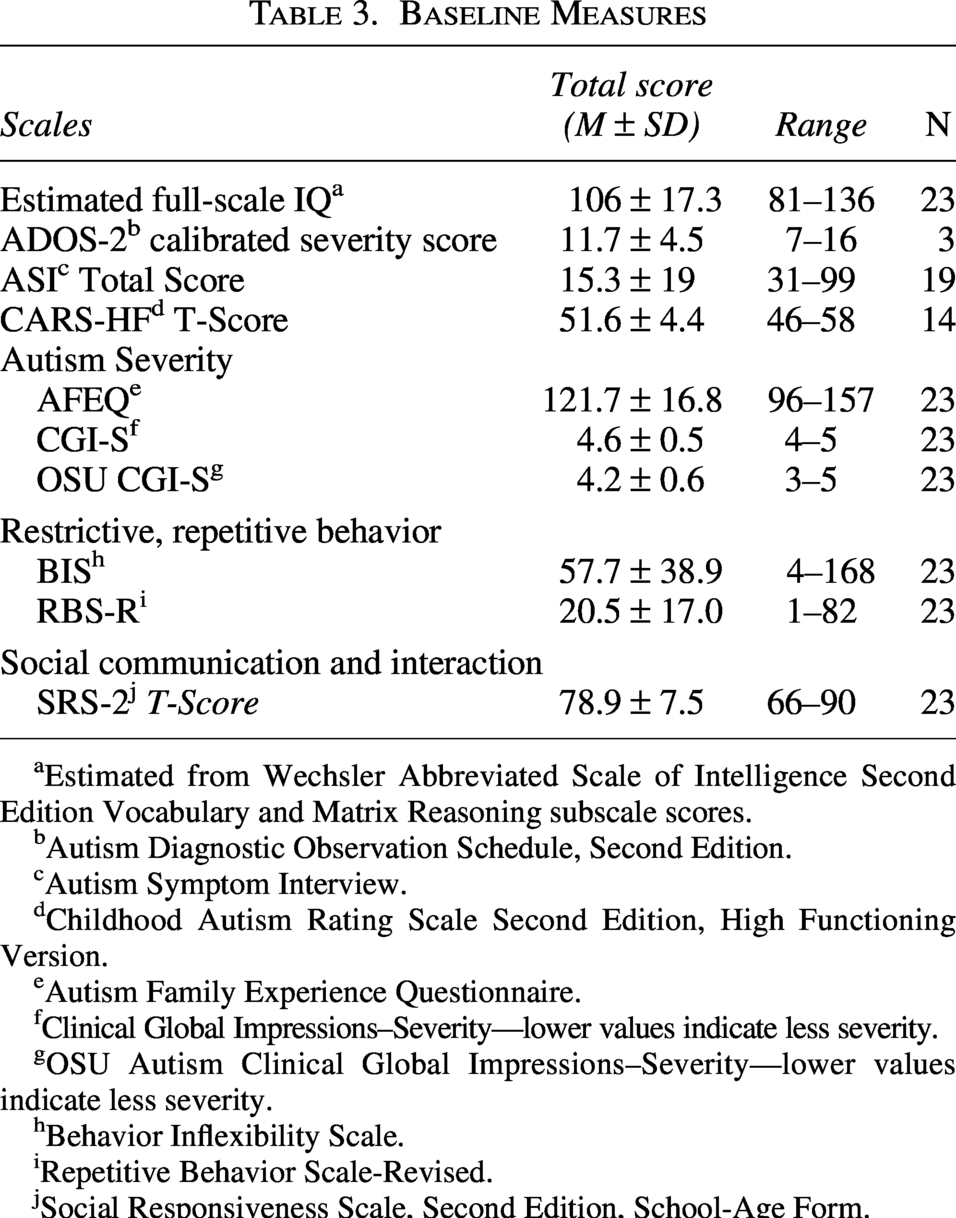
All participants met diagnostic criteria for Level 1 ASD by DSM-5 and ASI or CARS2-HF. At baseline (See Table 3), the average CGI-S score (M = 4.4 ± 0.5) on the individualized target domains reflected severity between 4 = moderately ill and 5 = markedly ill. OSU Autism CGI-S scores similarly placed the cohort within the moderate to moderately severe autism range. Regarding impact of participants’ symptoms on family experience and quality of life, initial AFEQ total scores (M = 122 ± 17) averaged below the scale midpoint (range 48–240, lower scores indicating better outcomes). Core ASD symptoms were measured using the RBS-R, behavioral inflexibility (BIS), and SRS-2. The average RBS-R total score (M = 20.5 ± 17) was low (scale range 0–229). Caregivers reported M = 11.8 ± 6.6 distinct repetitive behaviors for their child. The RBS-R Global Rating Score, assessing caregiver impressions of how these repetitive behaviors impact their child, averaged 55.5 ± 31, between “not a problem at all” (0) and “as bad as you can imagine (100).” Behavioral inflexibility, measured via the BIS (M = 57.7 ± 39), was in the lower end of the range (0–228, higher scores denote greater inflexibility), although values were widely distributed. Average baseline SRS-2 Total Scores (M = 78.9 ± 7.5) were in the “Severe” (T Score ≥ 76) range. Nine endorsed items on the baseline C-SSRS, including one who endorsed specific intent in the past six months. All were clinically evaluated and determined to be sufficiently stable to participate.
Baseline Measures
aEstimated from Wechsler Abbreviated Scale of Intelligence Second Edition Vocabulary and Matrix Reasoning subscale scores.
bAutism Diagnostic Observation Schedule, Second Edition.
cAutism Symptom Interview.
dChildhood Autism Rating Scale Second Edition, High Functioning Version.
eAutism Family Experience Questionnaire.
fClinical Global Impressions–Severity—lower values indicate less severity.
gOSU Autism Clinical Global Impressions–Severity—lower values indicate less severity.
hBehavior Inflexibility Scale.
iRepetitive Behavior Scale-Revised.
jSocial Responsiveness Scale, Second Edition, School-Age Form.
Primary target domains
The individualized target symptom domains identified for each participant were Social (N = 8, 35%), Anxiety (N = 5, 22%), Irritability/Tantrums (N = 5, 22%), Restricted, Repetitive Behaviors (N = 4, 17%), and Sleep Problems (N = 1, 4%).
Dosing
Per our BOIN design (see Supplementary Data), the first two cohorts (N = 6) trialed the median dose (6 mg/kg/day), yielding a 50% response rate. The next six participants trialed 3 mg/kg/day, attaining a 17% response rate. The fifth cohort (N = 3) was placed on the median dose (6 mg/kg/day); only one responded. With the two lower doses eliminated, the highest dose (9 mg/kg/day) was tested in subsequent participants (N = 8).
Treatment response
All 23 enrolled participants completed the trial. Ten were responders (44%), averaging 1.8 ± 0.1 on the individualized target domain CGI-I. For the overall sample, CGI-I scores (M = 2.6 ± 0.8, range = 1–4) averaged between 2 = much improved and 3 = minimally improved (See Table 4).
Treatment Response in Individualized Target Domains
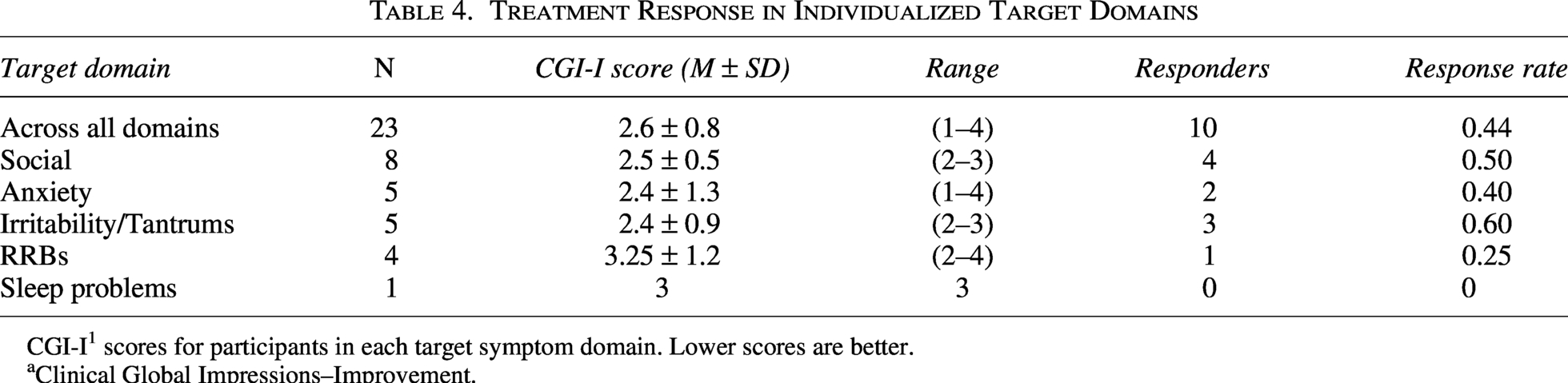
CGI-I1 scores for participants in each target symptom domain. Lower scores are better.
aClinical Global Impressions–Improvement.
Target domains varied in proportions of responders: Irritability/Tantrums (3/5, 60%), Social (4/8, 50%), Anxiety (2/5, 40%), Restricted, Repetitive Behavior (1/4, 25%), and Sleep Problems (0/1).
Categorical response rate was related to dose, ranging from 1/6 (17%) at 3 mg/kg/day, to 4/9 (44%) at 6 mg/kg/day, and 5/8 (62%) at 9 mg/kg/day. Dose was significantly associated with individualized CGI-I scores (r(23) = −0.42, p = 0.043) and OSU Autism CGI-I scores (r(23) = −0.62, p = 0.002) indicating greater improvement at higher dose levels. CGI-I mean ± SD and 95% confidence intervals by dose were 3.2 ± 0.3 [2.4, 4.0] at 3 mg/kg; 2.6 ± 0.3 [1.9, 3.2] at 6 mg/kg; and 2.2 ± 0.2 [1.7, 2.8] at 9 mg/kg.
Plasma CBD trough levels (9–10 hours after morning dose) after 6-week treatment were analyzed for the first 19 participants (Table 5). The analyzed subsample (N = 19) did not differ significantly from the entire sample in CBD dosage (Chi-square(2) = 0.96, p = 0.61). CBD plasma levels ranged widely (2.4–430.6 ng/mL) and were related to dose (r(19) = 0.46, p = 0.05), but not to individualized domain CGI-I score (r(19) = −0.19) or to categorical response.
Plasma Cannabidiol Trough Concentrations at End of Treatment (N = 19)
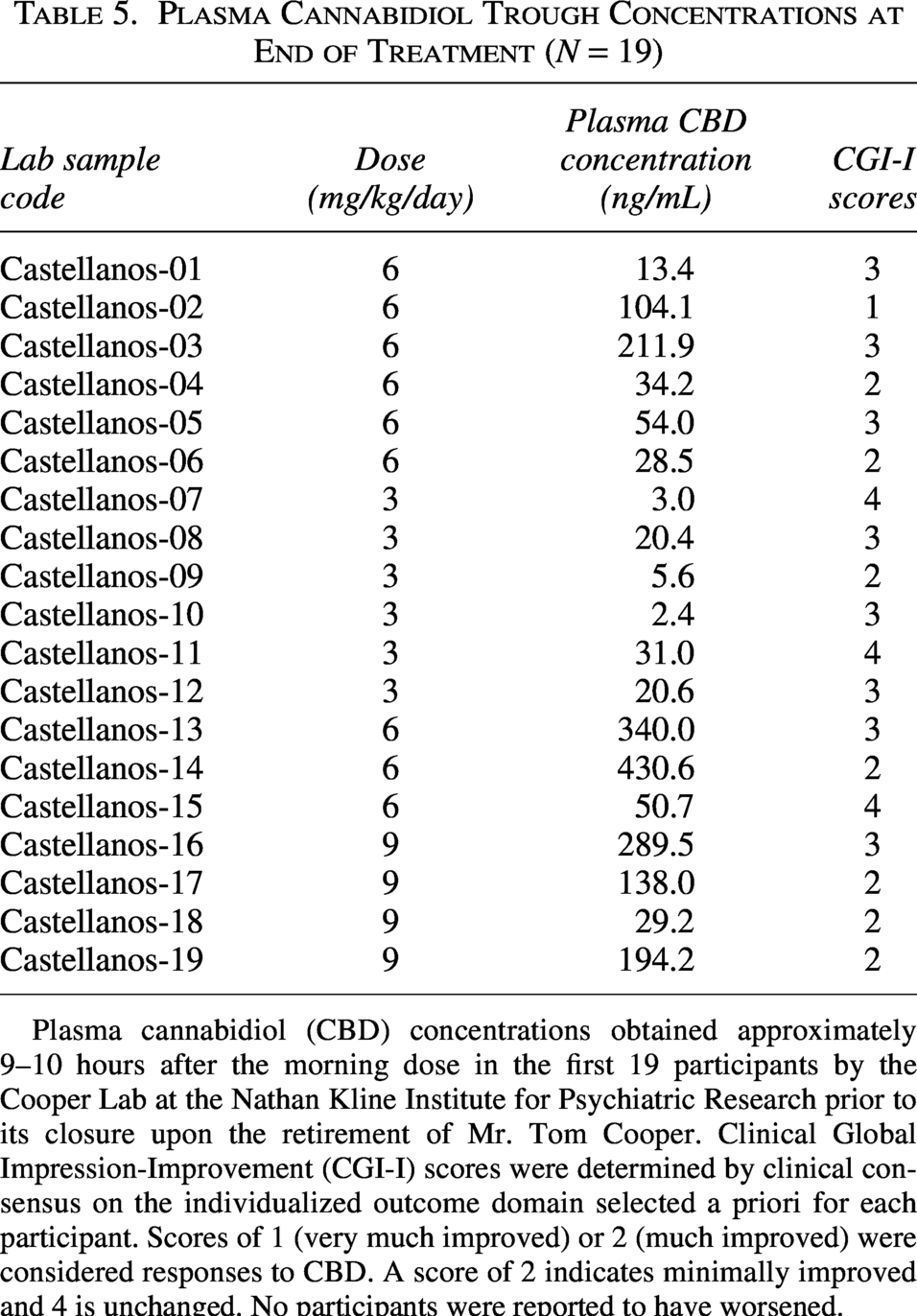
Plasma cannabidiol (CBD) concentrations obtained approximately 9–10 hours after the morning dose in the first 19 participants by the Cooper Lab at the Nathan Kline Institute for Psychiatric Research prior to its closure upon the retirement of Mr. Tom Cooper. Clinical Global Impression-Improvement (CGI-I) scores were determined by clinical consensus on the individualized outcome domain selected a priori for each participant. Scores of 1 (very much improved) or 2 (much improved) were considered responses to CBD. A score of 2 indicates minimally improved and 4 is unchanged. No participants were reported to have worsened.
Secondary endpoints
Severity
Table 6 shows individualized domain CGI-S scores changed significantly (p ≤ 0.001) with a large Cohen’s d = 0.91. By contrast, OSU (autism) CGI-S final scores were statistically unchanged.
Secondary Endpoints (N = 23)
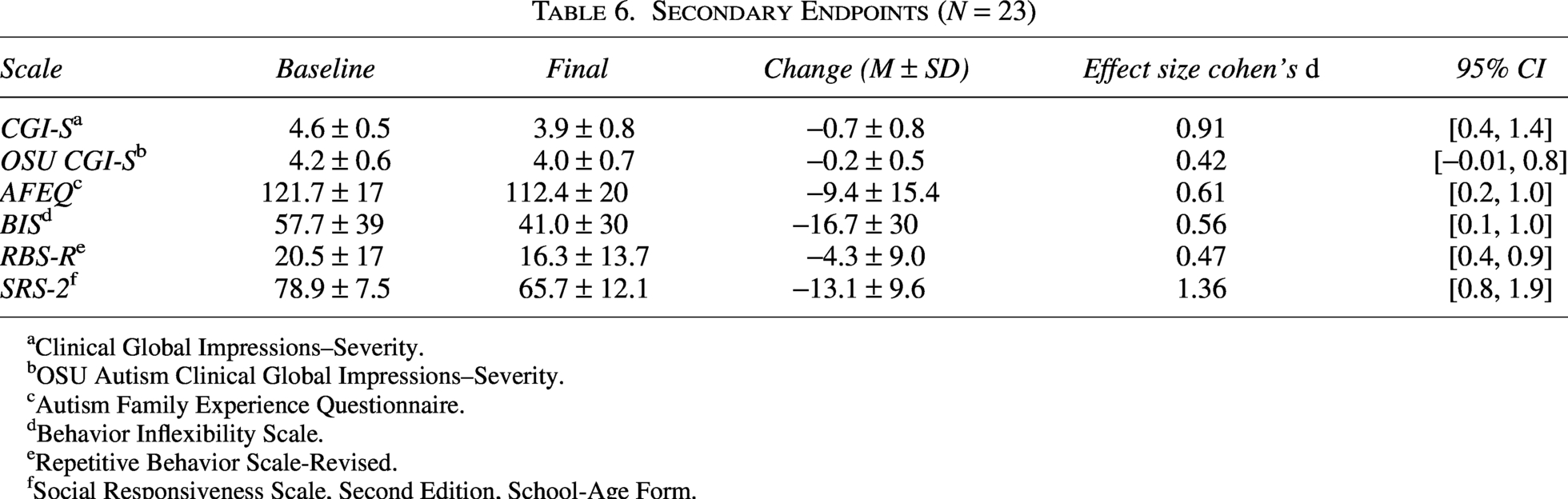
aClinical Global Impressions–Severity.
bOSU Autism Clinical Global Impressions–Severity.
cAutism Family Experience Questionnaire.
dBehavior Inflexibility Scale.
eRepetitive Behavior Scale-Revised.
fSocial Responsiveness Scale, Second Edition, School-Age Form.
Core ASD symptoms
Supplementary Table S4 shows that all SRS-2 subscales and total scores were significantly lower on CBD (p ≤ 0.001 for all), with large effect sizes (ranging from d = 0.93 to d = 1.74) except for Social Awareness (d = 0.65), corresponding to a mean change in SRS-2 Total-score from the Severe Range (≥76 T) to the lower end of the moderate range (66 T – 75 T) across all doses. This was most prominent on the highest dose (Supplementary Table S3), with the mean (59.5) nearly at the boundary of normal limits (≤59). Supplementary Table S5 shows that Total RBS-R score (p = 0.03, d = 0.47) and Stereotyped Behavior (p = 0.01, d = 0.56) decreased significantly on CBD with medium effect sizes. BIS also decreased significantly with a medium effect (p = 0.01, d = 0.56).
Anxiety
Most anxiety indices decreased with medium effects (Supplementary Tables S6 and S7). Child-rated ASC-ASD total scores were significantly lower (p = 0.005), as were caregiver ASC-ASD ratings (p = .01), SCARED–Parent Version total score (p = 0.01), subscales of Generalized Anxiety Disorder (p = 0.04) and Significant School Avoidance (p = 0.02). Somatic Symptoms/Panic Disorder, Separation Anxiety, and Social Phobic Disorder subscales did not change significantly.
Family and home experience
Caregiver-rated family experience and quality-of-life on the AFEQ were higher (t(22) = 2.93, p = 0.008). Child behavioral compliance at home on the HSQ-ASD was also higher (t(22) = 2.65, p = 0.02; see Supplementary Table S7). Both yielded medium effects.
Adaptive behavior
The Vineland-3 Adaptive Behavior Composite–Standardized Score was significantly higher (p = 0.003) with a large effect (d = 0.69; Supplementary Table S7). All three component domains, Communication (p = 0.008), Socialization (p = 0.007), and Daily Living Skills (p = 0.04) changed similarly albeit with medium effects.
Hyperactivity
The ABC Hyperactivity/Noncompliance subscale changed (p ≤ 0.001) with a large effect (d = 0.80) as did the ADAMS Manic/Hyperactive subscale (p = 0.02) with a medium effect (d = 0.55).
Mood and affect
ABC Irritability was lower (p = 0.002) with a large effect (d = 0.72). ABC Social Withdrawal was also lower (p = 0.047) but with a medium effect (d = 0.44). The ADAMS Depressed Mood subscale score was lower (p = 0.04) with a medium effect (d = 0.45).
Sleep problems
Sleep Disturbance Scale for Children (SDSC) total scores were significantly lower (p = 0.01) with a medium effect (d = 0.58). The Initiating Sleep subscale had the largest effect size (d = 0.74).
Dose effect on secondary endpoints
Bivariate correlations were tested between dose and change in total scores on all exploratory secondary endpoints. Dose correlated with change in SRS-2 Total T-Score (r(23) = −0.45, p = 0.03) and change in Vineland-3 Adaptive Behavior Composite Score (r(23) = 0.55, p = 0.007). Dose did not correlate significantly with change in SDSC total score or Initiating Sleep subscale. However, dose was associated with worsening on the Excessive Somnolence subscale (r(23) = 0.51, p = 0.01).
Safety
Physiological measurements
We did not observe any clinically relevant changes in vital signs or physical exam findings; neither weight nor BMI changed significantly. Laboratory parameters, including liver function tests and complete blood counts, were unaffected by CBD administration.
Adverse events
A total of 222 AEs were reported by 20 participants/caregivers across reporting methods;
Caregivers reported 143 AEs at study visits and via phone calls on weeks 1, 3 and 5; 73 AEs across 18 symptoms were considered related to CBD. Related AEs (mild, N = 68; moderate, N = 5) were reported in 15 children (65%). Moderate severity related AEs included headache, increased emotionality, greater oppositionality, sleep onset insomnia, and increased vivid dreams (all N = 5). Two events (mild skin rash, moderate headache) required over-the-counter medication to resolve. Most related AEs were expected (N = 60, 82%). Unexpected but related AEs (N = 14) included sleep-onset insomnia (6 reports, N = 2), greater oppositionality (3 reports, N = 1), and concentration difficulty (5 reports, N = 1). Two unexpected but related AE reports (sleep-onset insomnia, greater oppositionality) were rated as moderate in severity; the rest were mild.
At weeks 2, 4, and 6, the UKU Side Effects Rating Scale completed by participants and caregivers captured an additional 79 AEs. Of these, 55 reports (representing 13 symptoms, 9 not endorsed by other methods) were considered related to CBD treatment.
Across all methods, 27 unique AEs were considered treatment-related; 23 reached a frequency threshold > 5% (N ≥ 2 participants). The most frequently reported related AEs were increased salivation (N = 7, 30%), increased sleep duration (N = 9, 39%), sleepiness/sedation (N = 6, 26%), increased dream activity (N = 8, 35%), and polyuria (N = 5, 22%).
C-SSRS
Fifteen items were endorsed by 7 participants on the C-SSRS–Since Last Visit. Three participants experienced suicidal ideation during the trial, with intensity as “1—wish to be dead” for all three and “2—nonspecific active suicidal thoughts” for one. Four others endorsed non-suicidal self-injurious behavior, either “specific intent” (N = 2), “intent unknown” (N = 1), or both (N = 1). No reports of suicidal ideation or self-injurious behavior were determined to be study drug-related or resulted in discontinuation of study participation (Supplementary Table S9).
Discussion
Our study aimed to (1) assess a possible non-linear CBD dose-response in young autistic patients, (2) determine effect sizes of symptom changes from baseline to trial completion, using measures developed to assess core ASD symptoms, symptoms often associated with ASD, and global functioning, and (3) identify primary and secondary outcome measure(s) for subsequent double-blind placebo-controlled randomized clinical trials.
Dosages tested
We sought evidence of potential inverted-U dose-dependent effects (Kaplan et al., 2017; Zuardi et al., 2017). We hypothesized that moderate doses of CBD would be therapeutically beneficial for core and associated ASD symptoms and implemented the BOIN design to increase sensitivity accordingly. Instead, we found a monotonic relationship between dose and response within the dose range tested. The highest tested dose (9 mg/kg/day) yielded the highest proportion of responders (62%) and near normal SRS-2-Total T-scores, but also higher rates of AEs. Given study limitations, this observation should be considered preliminary and hypothesis-generating. Of note, pharmacologic grade CBD did not separate from placebo in autistic boys with substantial behavior problems even at 20 mg/kg/day (Trauner et al., 2025).
We defined response conservatively as “very much improved” or “much improved” on individualized symptom outcomes. The overall response rate (44%) (i.e., clinician-determined improvement in the symptom domain considered most interfering at study outset) was lower than what we had expected for an open-label trial (∼60%). Overall, the target domains with the highest proportion of responders were Irritability/Tantrums (60%), Social (50%), and Anxiety (40%), with minimal to no response in Restricted, Repetitive Behavior and Sleep Problems, respectively. However, participant distributions per domain and dose level were unequal, which prevents us from reaching clear conclusions regarding “optimal” target domains. For example, Irritability/Tantrums had the highest proportion of responders despite being tested only at 3 and 6 mg/kg/day. Most Social and Anxiety participants (12/13) were tested at 6 or 9 mg/kg/day, and the only participant reporting Sleep Problems received the lowest dose of 3 mg/kg/day.
Symptom changes
As SRS-2 Total-score ≥ 66 was an inclusion criterion, mean SRS-2 Total-score corresponded to the highest severity, as expected. The SRS-2 subscales showed strong effect sizes. This is not simply ascribable to regression to the mean, as baseline SRS-2 T-score did not correlate significantly with our primary outcome (r(23) = −0.20). By contrast, the standard measure of restricted, repetitive behavior (RBS-R) did not find strong evidence of effect across subdomains, which may reflect the overall lack of severity of restricted repetitive behaviors and behavioral inflexibility in our sample and also highlights that these instruments capture different constructs and may differ in sensitivity to rater-expectations and short-term change.
Given reported anxiolytic and prosocial effects of CBD, we expected improvements in these domains. Consistent with prior studies, we observed large treatment effects on scales measuring general anxiety and social communication/interaction. We also found that CBD had large effect sizes on subscales measuring hyperactivity, sleep, irritability, and adaptive behavior. However, all these observations are highly preliminary given our small heterogenous sample and open uncontrolled design.
Dose correlated with improvement on the SRS-2, suggesting an association between higher CBD doses and greater social responsiveness, although requiring an elevated SRS-2 Total-score for enrollment may have partially confounded this result. Of the secondary endpoints assessing associated symptoms, dose only correlated with the Vineland-3 Adaptive Behavior Composite, of which 2 of 3 domains (Socialization, Communication) measure core ASD symptoms.
We reiterate that all study endpoints are exploratory given our open-label design, small sample size and uneven distribution of primary domains and doses. However, measures of social communication and interaction changed substantially after six weeks of CBD treatment, regardless of response in overall target symptom domain, and the change was greater on higher doses.
Adverse events
CBD was well tolerated by participants with mostly mild adverse effects. Data from open-label and controlled trials of CBD in pediatric epilepsy found the most common AEs were somnolence, loss of appetite, vomiting, and diarrhea. In our sample, the most frequent AEs were related to sleep, mood/affect, salivation, appetite, and urine output.
Most sleep-related AEs (N = 9) reported somnolent effects: increased duration, sleepiness/sedation, and/or heavier sleep. Fewer (N = 4) reported insomnia (sleep-onset, shortened duration). Per the SDSC, sleep quality and quantity were higher with CBD treatment, with the largest effect in “Initiating Sleep.” We found a moderate positive significant correlation between dose and change in “Excessive Somnolence,” suggesting higher doses were associated with greater somnolence. Shortened sleep was an unexpected but related AE. Autistic youth are more likely to experience sleep problems compared to non-autistic peers (Johnson and Zarrinnegar, 2021). Interestingly, 2 of 4 participants reporting “decreased sleep duration” also reported “increased sleep duration” at other timepoints. This could indicate that CBD has inconsistent effects on sleep duration or could reflect preexisting sleep difficulties. The only participant with Sleep Problems as their target domain did not respond; however, this participant trialed the lowest dose.
The second most frequent sleep-related AE was “increased dream activity,” reported by eight, although they were not nightmares nor bothersome. Rather, they were often described as “vivid” with a pleasant connotation.
Weight/BMI
Given the substantial metabolic adverse effects from currently approved medications for irritability/aggression in ASD, we assessed changes in weight gain and appetite. Neither weight nor BMI changed significantly in either direction. Among AE, “increased appetite” and “decreased appetite” were reported in nearly equal proportions.
Limitations
Study limitations are numerous and inherent to its design, small sample size, and substantial heterogeneity. Our small sample size limits generalizability and diminishes our ability to detect meaningful effects. While our study sample spanned a broad age range, it was limited in other demographic measures (e.g., sex). Based on a male-to-female prevalence ratio for ASD without intellectual disability estimated at 3.8:1, we aimed to recruit ≥15% female participants; however, we only recruited one (4%). Even more problematically, uneven distribution of treatment domains and doses produced by our BOIN-based cohort design limit conclusions about “optimal” domains and doses. COVID-19 led to remote data acquisition procedures for all but the first participant. Our standard instruments were not validated for remote administration, potentially impacting reliability. We did not detect relationships between response and plasma CBD, which was highly variable. The broad range of plasma CBD levels may reflect inconsistent adherence (not independently verified), absorption differences (known to be large), or metabolic variation. We did not quantify CBD metabolites, which were related to outcomes and electrophysiological measures in boys with ASD (Cazares et al., 2026). Although the CGI-I is widely used, we did not institute structured anchoring or rater calibration procedures, which may have contributed to expectancy/observer bias. From an abundance of caution, we excluded potential participants to minimize risks of metabolic drug–drug interactions, which made our sample less representative. Additionally, pandemic-related changes in routine, social demands, or therapy access could have contributed to observed symptom changes. Finally, our requirement that children be verbally fluent with IQ ≥ 80 means that our results cannot be generalized to the broader ASD population.
Conclusions
In this hypothesis-generating study, CBD was associated with only mild-to-moderate AEs. Response rate (44%) was lower than expected a priori (∼60%); within the dose range tested, the highest observed responder proportion occurred at 9 mg/kg/day. However, somnolence was also greater at higher doses. Exploratory secondary analyses revealed large effect sizes in scales assessing social communication and interaction, adaptive behavior, irritability, and sleep. Clinical and laboratory parameters remained unchanged. These findings should inform the design and dose selection of future placebo-controlled trials.
Clinical Significance
This hypothesis-generating open-label Phase 2 clinical trial evaluated the safety and preliminary efficacy of CBD in autistic youth with fluent verbal language and IQ ≥ 80. Adverse effects were mild–moderate and CBD was deemed substantially helpful for nearly half of participants.
Authors’ Contributions
F.X.C., P.E.C., Y.Y., R.A.S., A.B.T., D.F., and O.D. were involved in study design. G.R.C., L.R., R.A.S., and P.E.C. were involved in data acquisition. L.R. and J.L., and F.X.C. performed data analysis/interpretation, and J.L., F.X.C., and R.A.S. drafted the article. All authors reviewed the final version and gave approval for submission.
Footnotes
Acknowledgments
The authors would like to thank study participants and caregivers for their time and effort, the Vulnerable Brain Project for funding support, and Jazz Pharmaceuticals, Inc. for providing Epidiolex® at no cost.
Author Disclosure Statement
There are no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.