
Abstract
Objective:
Use measurement-based care to assess symptom change across diagnostic categories for adolescents receiving acute-care psychiatric inpatient treatment including both psychopharmacology and dialectical behavior therapy.
Methods:
Adolescents were aged 12–17 and hospitalized on a coeducational, acute-care inpatient unit within a psychiatric hospital in New York City. We conducted a retrospective chart review to analyze symptoms across two or more timepoints from the first 15 days of admission using mixed effects regression models to estimate linear change on five outcome measures including Generalized Anxiety Disorder-7 (GAD-7), General Behavior Inventory-Mania subscale (GBI-10M), Patient Health Questionnaire-9 (PHQ-9), Prodromal Questionnaire Brief-21 (PQB-21), and Schwartz Outcome Scale-10 (SOS-10).
Results:
There were improvements on all five measures. For the GAD-7, GBI-10M, PHQ-9, and PQB-21, the change is negative, indicating a decrease in symptoms. For the SOS-10, the change is positive, suggesting an increase in well-being. The covariance parameters indicate that there is generally significant individual variation around the adolescent’s initial assessment as well as significant individual variation around the slope, suggesting that patients change at different rates. The Days × Intercept covariance parameter is generally negative, indicating that adolescents who started with higher symptom severity showed greater symptom reduction. For well-being, the negative change indicates that adolescents with higher well-being on the first assessment showed smaller increases in well-being over time.
Conclusion:
Adolescents experienced improvements in their symptoms of anxiety, mania, depression, psychosis, and well-being during acute psychiatric inpatient treatment. These are notable findings, particularly for demonstrating the impact of psychiatric inpatient treatment on improving symptoms/diagnoses.
Introduction
Background
It is widely recognized that psychiatric inpatient treatment is a crucial service on the continuum of levels of care designed to target the most severe and complex mental health challenges including suicidality, nonsuicidal self-injury, aggression, and homicidality for children and adolescents (Leffler et al., 2024). A 2023 systematic review evaluating 24 different outcome variables from psychiatric inpatient admission found positive outcomes, broadly speaking, in terms of biopsychosocial severity of mental illness, clinical improvements, and readmission rates, and underscored the increasing demands on and for psychiatric inpatient admissions (Hsu et al., 2024). Conversely, psychiatric inpatient treatment is considered a last resort option, and serious concerns have been raised in the field about the lack of established effectiveness and the potential iatrogenic effects (Zuccala et al., 2025). Indeed, there is a paucity of treatment outcome studies for psychiatric inpatient treatment, which limits the ability to identify and provide the best possible care for patients and to develop robust practice guidelines. Leffler et al. call for routine assessment and identifying and measuring target symptoms, and they highlight evidence-based interventions that are appropriate for inpatient services (Leffler et al., 2024). However, there remains a paucity of inpatient treatment outcome research.
Adolescents admitted to psychiatric inpatient care present with the most severe, persistent, and complex mental health disorders and symptoms (Kronström et al., 2016). Although psychiatric inpatient treatment has been shown to ameliorate crisis (Hayes et al., 2018) and to decrease unsafe behaviors while hospitalized (Tebbett-Mock et al., 2020), there remains a significant number of adolescents whose symptoms do not respond to inpatient treatment (Thompson et al., 2021). There is a gap in the literature about actual symptom improvement in the context of diagnoses, and there is a grave concern that conditions may worsen as a result of inpatient treatment (Zuccala et al., 2025). There are inherent challenges with studying inpatient populations, including the ethical concerns regarding randomization of patients and the fact that most inpatient youth, due to the complex clinical presentation, are excluded from randomized controlled trials (Gurtovenko et al., 2024). Examples of iatrogenic effects include adverse events associated with psychopharmaceutical treatment (Correll, 2011), the impact of experiencing containment practices (e.g., restraint, seclusion), or experiencing traumatic events which may in turn increase suicidality (Large et al., 2011), and the negative influence from peers (e.g., increase in nonsuicidal self-injury, social contagion for the spread of negative attitudes, behaviors, emotions) (Freemantle et al., 2012). There is limited albeit growing research within the field of acute-care inpatient for adolescents. Furthermore, outcomes have been mainly evaluated based upon indirect data including variables such as length of stay (LOS), readmission rates, the use of restraint, seclusions, and constant observation (CO), which does not measure symptom severity directly (Tebbett-Mock et al., 2020).
Dialectical behavior therapy
Dialectical behavior therapy (DBT) is one of the few psychological interventions that has an established body of literature on treatment outcome variables for inpatient adolescents. DBT is an internationally recognized, empirically supported treatment that directly addresses suicidal behavior and other forms of self-injury (Linehan, 1993) and has been adapted for adolescents (i.e., DBT-A) (Miller et al., 2007) with a range of psychiatric conditions across a range of levels of care (Boustani et al., 2026). A 2024 systematic review identified four studies evaluating DBT for inpatient adolescents (Waitz et al., 2021). Katz et al. conducted a nonrandomized controlled feasibility study and compared DBT to treatment as usual (TAU) on a unit with a mean LOS of 18 days for 62 adolescents and concluded that the group that received DBT had significantly fewer episodes of violent incidents on the unit compared with the group treated with TAU, and DBT showed a 100% retention rate of patients completing the DBT program, meaning that no patients crossed over into TAU or discharged early from their voluntary admissions (Katz et al., 2004). Tebbett-Mock et al. conducted a retrospective chart review for 425 adolescents receiving inpatient DBT and for a historical control group of 376 adolescents treated on the same unit before DBT was implemented, and they found adolescents who received DBT had significantly fewer CO hours for self-injury; incidents of suicide attempts and self-injury; restraints; and LOS days compared to patients who received TAU (Tebbett-Mock et al., 2020). Statistically significant differences were not found between DBT and TAU groups for number of CO hours for aggression, incidents of aggression toward patients or staff, seclusions, or readmissions (Tebbett-Mock et al., 2020). They also found that adolescents who received DBT had significantly lower clinician-rated depression scores and global impression scores upon discharge compared with patients who received TAU, but did not find statistically significant differences on levels of mania, symptom severity or aggression between the two groups (Saito et al., 2020; Tebbett-Mock et al., 2020). Romani et al. reported that adolescents treated in acute-care inpatient receiving group therapy based on DBT have significant improvements on self-report of depression, anxiety, and anger, but a higher rate of staff injuries (Romani et al., 2024).
Measurement-based care
Although the aforementioned research includes important data that reflects outcomes, most of the inpatient literature focuses on unit-level variables (e.g., restraints, seclusions, CO) or administrative variables (e.g., LOS) that indirectly measure patients’ well-being and do not directly measure patient-level outcomes. These variables do not comprehensively reflect symptom improvement or severity of mental illness, are not well understood within the context of mental health diagnoses, provide marginal insight into psychological well-being (Oh et al., 2020), and are limited in generalizability for psychopharmacology and psychosocial interventions across other levels of care, such as outpatient. While the focus on evidence-based practice is becoming increasingly common across clinical settings, surveys of practicing clinicians have revealed that clinicians have not consistently used best-practice assessment guidelines to monitor therapeutic progress (D’Angelo and Augenstein, 2012).
Measurement-based care (MBC) is considered an essential feature of evidence-based practice according to the American Psychological Association (American Psychological Association Presidential Task Force on Evidence-Based Practice, 2006) and refers to the routine collection and use of outcomes data throughout the treatment process. MBC is an evidence-based, patient-centered approach that helps clinicians identify and track progress toward treatment targets (Lavender et al., 2022; Scott and Lewis, 2015). MBC is used to supplement initial patient assessments, to develop and adjust therapeutic goals and treatment plans, and to monitor patient progress throughout treatment (Connors et al., 2022). MBC is transtheoretical and transdiagnostic, allowing it to be used across different settings and populations (Lewis et al., 2019). Empirical literature demonstrating the effectiveness and relevance of MBC in adult populations has been established supporting MBC effectiveness for improving clinical outcomes, providers’ clinical judgment, and therapeutic alliance (Fortney et al., 2017, Lavallee et al., 2016, Lewis et al., 2019, Peterson et al., 2018). Yet, there are few studies that evaluate MBC with youth. A systematic review and meta-analysis of youth mental health services identified only 12 studies that evaluate the implementation and clinical use of MBC with adolescent patients (Tam and Ronan, 2017). Boyd et al. highlighted that more research on MBC for child and adolescent settings is crucial (Boyd et al., 2024). Of note, Waitz et al. highlighted the challenge of inpatient studies using widely diverse and numerous measures; at least 12 different measures were used across 4 studies on inpatient DBT with no overlap across studies (Waitz et al., 2021). Although Waitz’s study was a systematic review specifically of DBT for inpatient adolescents, this problem is pervasive and Waitz’s study highlights that the field does not have commonly agreed upon measures for inpatient care (Waitz et al., 2021).
Although the field of psychiatry recognizes the benefits of MBC and the focus on evidence-based practice is increasing particularly for inpatient psychiatric units (American Psychological Association Presidential Task Force on Evidence-Based Practice, 2006), unstructured clinical evaluations and reliance on clinical judgment are common (Lewis et al., 2019) within inpatient psychiatry. First, a meta-analysis demonstrated that unstructured clinical interviews yield different diagnoses than structured interviews (Rettew et al., 2009). Second, research demonstrates that unstructured clinical interviews yield fewer diagnoses and focus only on primary diagnoses (Costello et al., 2003). Third, research highlights that unstructured interviews commonly miss comorbid diagnoses leading to inaccurate diagnosis and treatment. Fourth, research shows that interrater reliability among clinicians is weak. In addition, there may be a potential bias by clinicians when using subjective ratings, clinical judgment, unstructured interviews, and unplanned assessment timepoints rather than objective measures, structured tools, and routine/scheduled measurement timepoints. Salmond et al. reported that the patient-reported outcome among adolescents did not match with clinician-rated positive outcomes among adolescents treated in the inpatient unit. Specifically, clinicians rated 72% of adolescents improved on anxiety, depression, and functioning, whereas adolescents self-reported no changes and some reported deterioration (Salmond, 2020).
The challenges that inpatient teams encounter when implementing MBC are summarized in Saito’s recent article, along with insight into who should report the outcomes, which ratings to use, and overcoming obstacles in the implementation process (Saito, 2025). This review highlights that clinician-rated measurement poses multiple obstacles (e.g., time to complete, training required), whereas patient-reported measurement can be a reliable and practical method to collect treatment outcomes among pediatric patients older than 5 years when rating scales are carefully selected. To date, preliminary research has been conducted on the feasibility and acceptability of MBC within inpatient psychiatry. Though time constraints remain a concern, clinicians continued to have a high interest in MBC, a positive shift in clinician attitude toward feasibility, and clinicians felt that MBC could promote patient progress (Lanca et al., 2025). Two studies conducted in adult inpatient settings underlined the feasibility of using patient-reported outcomes. More than 90% of patients completed the baseline assessment in both studies and among those who had a baseline assessment, had also >90% discharge assessment completion rate. They answered 45 or 94 questions and reported it took 5–60 minutes to complete (Puschner et al., 2009, Wong et al., 2022).
These authors seek to take a crucial step in the field to fill the gap in the literature by establishing the efficacy of psychiatric inpatient acute-care for adolescents by using MBC to assess symptom change across numerous diagnostic categories for adolescents receiving both psychopharmacology and DBT. These authors hypothesize that adolescents will exhibit symptom improvement across all outcome measures including measures assessing anxiety, mania, depression, psychosis, and general well-being.
Methods
Present study
This is a retrospective chart review on adolescents admitted to an acute-care inpatient adolescent unit. Adolescents in the current study were aged 12–17 and hospitalized on a coeducational, acute-care inpatient unit within a private, nonprofit, free-standing psychiatric hospital in a suburb of New York City. Adolescents were admitted to the inpatient unit either voluntarily or involuntarily via local emergency departments due to imminent safety concerns including danger to self or others, whereby they could not be safely maintained outside of the hospital. Involuntary admissions were defined as patients who were detained under civil commitment laws because they were judged to be a danger to themselves or others or were unable to function in the community, and their guardian was not present or did not consent to the admission.
Participants
The number of participants for each of the five analyses varied slightly due to missing data on different measures at different time points. Participants who completed only one time point on certain measures were included in the analysis of that measure when those same participants had more than one (generally 2) timepoints on other measures. However, when patients had only one assessment time on all the measures, they were excluded from analyses. Of note, including patients with only 1 time point in mixed effects regression analyses does not impact the slope parameter estimates. These five analyses were based on the following five measures Generalized Anxiety Disorder-7 (GAD-7), General Behavior Inventory–Mania subscale (GBI-10M), Patient Health Questionnaire-9 (PHQ-9), Prodromal Questionnaire Brief–21 (PQB-21), and Schwartz Outcome Scale-10 (SOS-10). For the following measures, the number of observations by adolescent inpatients is as follows: SOS-10 (n = 491), GAD-7 (n = 438), GBI-10M (n = 441), PHQ-9 (n = 443), PBQ-21 (n = 457). We collected sex, age, and race as additional demographic variables. Due to the variation in measure completion, describing “the” sample was challenging because for each measure, there were slightly different but highly overlapping samples. The sample for the SOS-10 was the largest, and the samples for the other four outcome measures were exactly or nearly proper subsets of the 491 patients who completed the SOS-10. For example, all the patients who completed the GAD-7 and the PHQ-9 also completed the SOS-10. For the GBI-10M and the PBQ-21, 97% and 98% of the patients who completed these measures also completed the SOS-10. For this reason, as well as due to space limitations, the patients’ electronic medical record sociodemographic characteristics for the SOS-10 were selected as the demographics to be reported. The sample includes 491 adolescents with a median age of 15 (SD = 1.6, 95% confidence interval [CI] = 14.73–15.01). Approximately 72% (n = 353) were biologically female, approximately 28% (n = 137) biologically male, and .2% (n = 1) indicated as unknown sex. Approximately 38% (n = 187) identified as White/Caucasian, approximately 30% (N = 147) as multiracial, 16% (n = 80) as African American/Black, 9% (n = 46) as Asian/Asian American, 5% (n = 27) as unavailable/unknown, and .8% (n = 4) as American Indian/Alaskan Native. The term “multiracial” was used for patients who identified with more than one race. The median LOS was 10 days (SD = 11.5; 95% CI = 11.83–13.86).
Procedures
The health system’s Institutional Review Board (IRB) approved this study as exempt. This was a retrospective study. All patient information was de-identified, and patient consent was not required. Data was extracted from the archived electronic medical record database by the Quality Management team of the hospital and by Krasnoff Quality Management Institute. Data included the following variables: age; gender; diagnosis; LOS; date and assessment time point; and scores on the following five measures GAD-7, GBI-10M, PHQ-9, PQB-21, and SOS-10. Age, gender, and race were self-reported by the patient at the time of admission and documented in the electronic medical record by the Central Intake department of the health system.
Regarding MBC, all patients were offered the opportunity to complete all five self-administered measures upon admission, weekly, and upon discharge. The initial MBC assessment was done within 72 hours of admission. Weekly measures were also completed within a 72-hour timeframe of the “week 1” timepoint. For example, “week 1” timepoint was completed within days 8–10. All five measures were completed by patients regardless of their history of diagnosis and presenting symptoms and problems. Measures were available on an iPad whereby a staff member navigated the iPad screen to start the measure and opened the specific patient’s episode, then handed iPad to that patient to complete questionnaires. Patients were encouraged to answer all five self-administered measures detailed below.
Of note, the five measures were selected to assess common psychiatric inpatient problems and are not intended to be a comprehensive or exhaustive psychosocial assessment, and they were selected because they have demonstrated sound psychometric problems and were understood to be available for use in the public domain and free.
Assessment measures
GAD-7: The GAD-7 is a 7-item questionnaire to identify the presence and severity of anxiety (Spitzer et al., 2006). Items are rated on a 4-point Likert scale yielding categories of anxiety based on total scores: 0–4 = Minimal, 5–9 = Mild, 10–14 = Moderate, and 15–21 = Severe.
GBI-10 Mania subscale (GBI-10 M): The GBI-10 M is a 10-item questionnaire to identify the presence and severity of manic and hypomanic symptoms (Youngstrom et al., 2021). Items are rated on a 4-point Likert scale yielding categories of mania based on total scores: 0–5 = None, 6–17 = Mild, 18+ = Clinically Significant.
PHQ-9: The PHQ-9 is a 13-item questionnaire used to identify the presence and severity of depressive symptoms. 9 of 13 items are rated on a 4-point Likert scale yielding categories of depression based on total scores: 0–4 = No/minimal, 5–9 = Mild, 10–14 = Moderate, 15–19 = Moderately Severe, and 20–27 = Severe (Spitzer et al., 1999).
PQB-21: The PQB-21 is a 21-item questionnaire developed from the original 92-item Prodromal Questionnaire. It consists of 18 positive symptom items and is designed as the first step in a two-stage screening process that relies on a clinician interview to obtain a diagnosis of psychosis (Loewy et al., 2011). Distress scores of 6 or greater indicate significant risk for psychosis.
SOS-10: The SOS-10 is a 10-item questionnaire developed as a brief, reliable measure of psychological health and general well-being for diverse patient groups receiving a variety of treatments in diverse settings (Blais et al., 1999). The SOS-10 was also validated among adolescents in the inpatient setting (Haggerty et al., 2013). Items are rated on a 7-point Likert scale yielding categories of life impairment based on total scores whereby higher scores indicate less impairment and lower scores indicate more severe impairment: 1–22 = Severe, 23–32 = Moderate, 33–39 = Mild, and 40–59 = Minimal.
Treatment
The inpatient unit was comprised of a multidisciplinary treatment team including 2–3 full time psychiatrists and/or psychiatric nurse practitioners (supervised by the attending psychiatrist) and 1–3 psychiatry trainees (i.e., residents, child and adolescent fellows) at a time, each working part time at 20–30 hours per week who rotated on a monthly basis; 2 full time psychologists and 6 psychology trainees at a time, including 3 externs in a 12 month position, 2 interns in a 6 month position, and 1 fellow in a 12 month position, each working part time for 20 hours per week (each were supervised by a licensed psychologist), 2 full time social workers, 2 full time psychiatric rehabilitation specialists (who were team members either at the BA or MA level but not necessarily professionally trained nor licensed mental health providers), 3 nurses per shift, and 3–4 mental health workers per shift. Upon admission, all patients participated in an unstructured diagnostic interview by members of the psychiatry team, and patients received medication management, as needed. All patients received case management and discharge planning. The unit consists of an efficacious, comprehensive DBT program (Tebbett-Mock et al., 2020,2021, 2022). Details of the DBT treatment and implementation to the unit are available in previously published literature (Tebbett-Mock et al., 2022). DBT included all functions and components of Linehan’s original model (Linehan, 1993), as well as adaptations for adolescents made by Miller, Rathus, and Linehan (Miller et al., 2007). All patients on the unit received DBT milieu treatment (i.e., DBT coaching, a token economy, an egregious behavior protocol to address incidents such as nonsuicidal self-injury or aggression toward others). All patients received a total of 10 DBT skill groups per week, including a DBT skill group each weekday targeting skill acquisition and a DBT skill group each weekday targeting skill strengthening and generalization. Groups included all five adolescent DBT skill modules (Miller et al., 2007). Patients received intensive psychotherapy, including individual and family sessions. Multidisciplinary team members met weekly for consultation team.
Data analysis
Analyses were conducted using SPSS version 31.0. Our analytic approach was mixed effects regression models to estimate linear change on five outcome measures (i.e., GAD-7, GBI-10M, PHQ-9, PQB-21, SOS-10) obtained longitudinally during the patient’s stay on the unit. We coded time naturally as “days since admission” with the day of admission coded as zero and the day each assessment was completed as the number of days that had passed from the initial admission. Based on this coding, the intercept of the regression equation is the predicted average score on the outcome measure when the patient was admitted, and the slope is the predicted average linear decrease in the score per day on the unit. We specified an unstructured variance–covariance matrix for the random effects that included the variance around the intercept, variance around the slope and the covariance between the intercept and slope. We restricted the analyses to data from the first 15 days since the patient’s first admission to the unit (recognizing that the data may have included patients with previous admissions) to avoid including data from other admissions, which would be inconsistent with the data from one admission period. Generally, we included data from patients with at least 2 time points of assessment. However, because not all measures were obtained at a given time point, some patients with only one time point may be included in an analysis. We included these patients so that the data for each measure would be obtained on roughly the same patients, which would justify comparisons between measures.
Results
Analyses of change on the outcome measures
Tables 1–5 summarize the mixed effects regression analyses for the five outcome measures to assess adolescents’ symptom change over time. As can be seen in each table, the intercept parameter indicates the estimated average score on the outcome variable when the patient is admitted and the slope parameter, which is the estimated average change per day on the outcome variable indicates. There were improvements from admission on all five measures over the course of the adolescents’ inpatient stay. For the GAD-7, GBI-10M, PHQ-9, and PQB-21, the change is negative, indicating a decrease in symptoms. For the SOS-10, the change is positive, suggesting an increase in well-being. In addition, the covariance parameters (random effects) indicate that there is generally significant individual variation around the adolescent’s initial assessment (UN 1,1) as well as significant individual variation around the change or slope (UN 2,2), suggesting that patients change at different rates. Finally, the Days × Intercept (UN 2,1) covariance parameter is generally negative, indicating that adolescents with high symptom severity on their initial assessment measures showed greater symptom reduction than adolescents with lower symptom severity on their initial assessment measures. For well-being, the negative change indicates that adolescents with higher well-being on the initial assessment showed smaller increases in well-being over time. These results demonstrate consistency between a positive measure of well-being and the four negative measures of symptoms.
GBI-10M Mixed Effects Regression
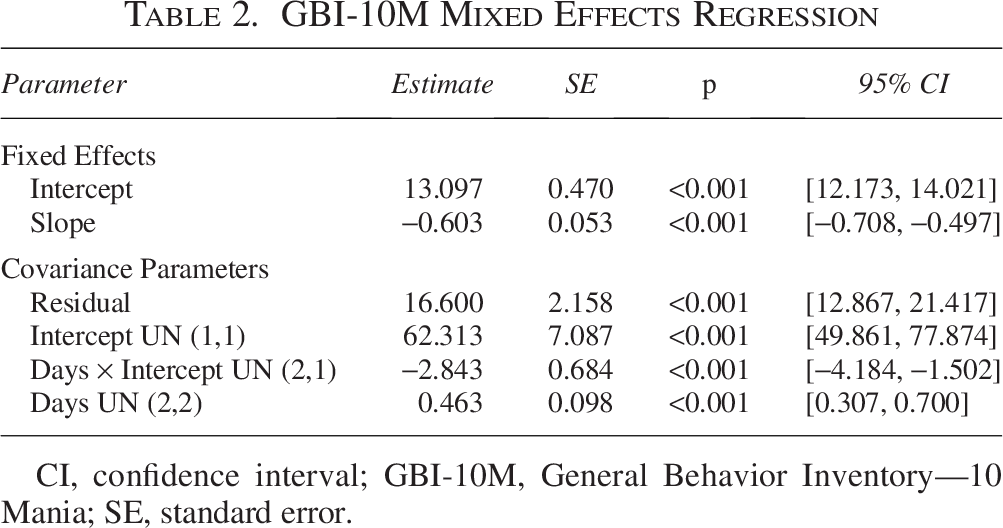
CI, confidence interval; GBI-10M, General Behavior Inventory—10 Mania; SE, standard error.
PHQ-9 Mixed Effects Regression
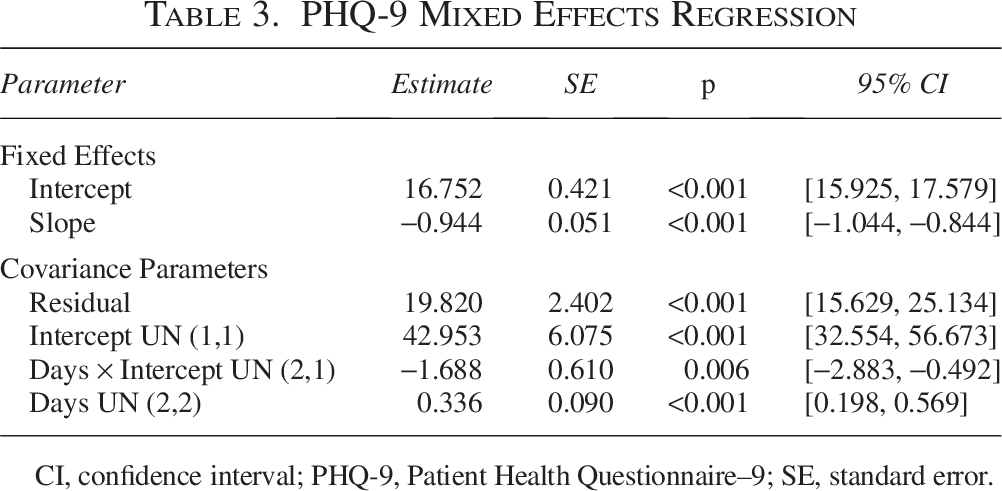
CI, confidence interval; PHQ-9, Patient Health Questionnaire–9; SE, standard error.
PQB-21 Mixed Effects Regression
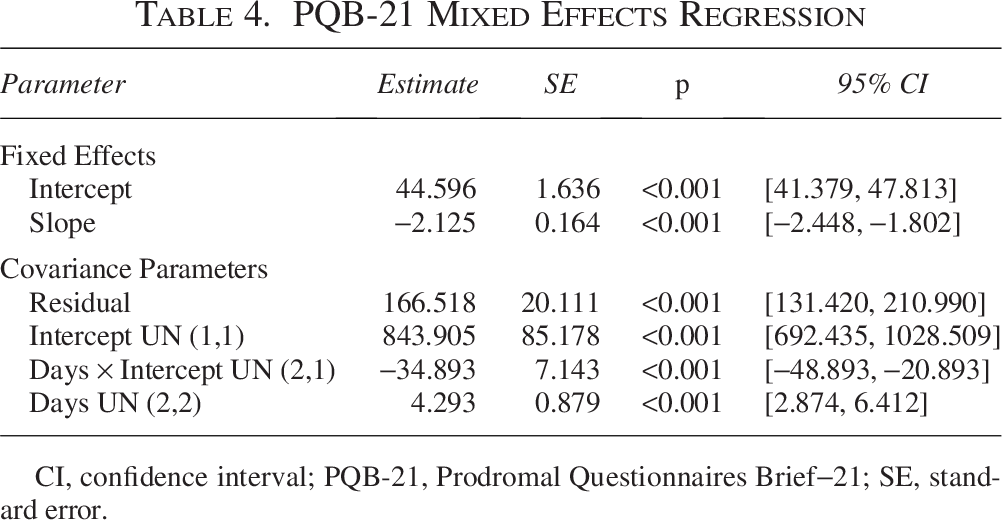
CI, confidence interval; PQB-21, Prodromal Questionnaires Brief−21; SE, standard error.
GAD-7 Mixed Effects Regression
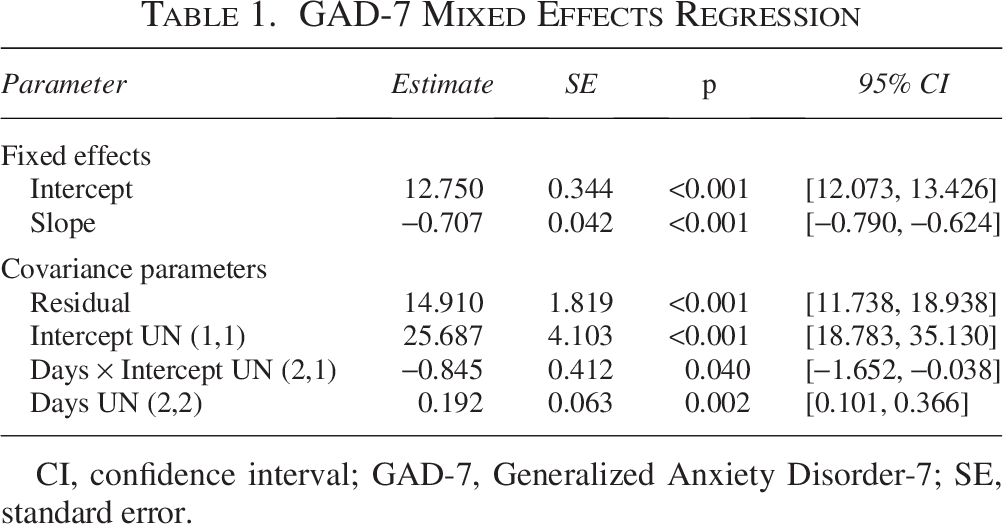
CI, confidence interval; GAD-7, Generalized Anxiety Disorder-7; SE, standard error.
SOS-10 Mixed Effects Regression
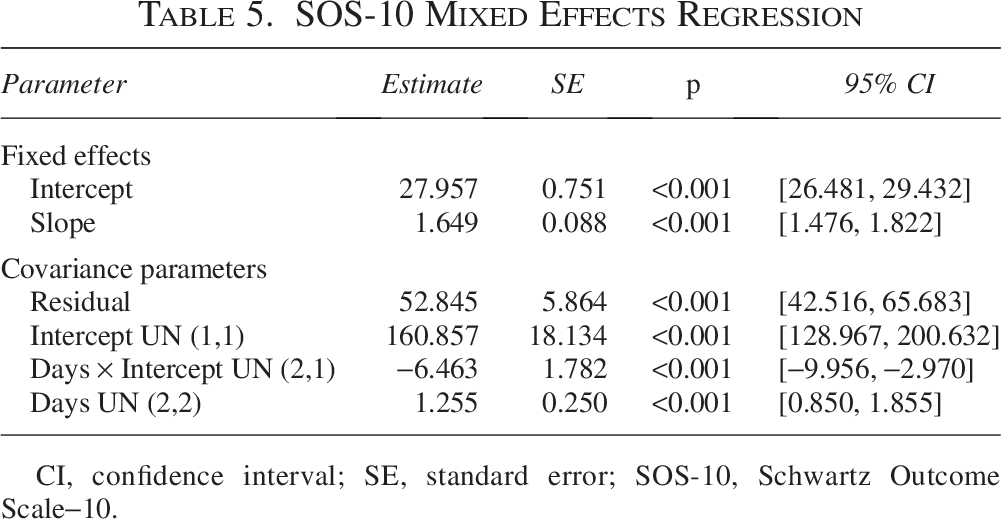
CI, confidence interval; SE, standard error; SOS-10, Schwartz Outcome Scale−10.
Discussion
Adolescents experienced significant improvements in their symptoms of anxiety, mania, depression, psychosis, and well-being during acute-care psychiatric inpatient treatment. These findings demonstrate the impact of psychiatric inpatient treatment on improving diagnostic symptoms, which is notable given that inpatient treatment is often recognized as only targeting crisis stabilization and for only assessing unit and administrative level variables. Furthermore, this study adds to extent literature because the findings examine both group and individual differences in symptom change. Although inpatient treatment is commonly viewed as necessary to provide safety for adolescents in acute crisis, research is limited on treatment outcomes pertaining to symptom improvement particularly according to MBC. Indeed, this study provides a foundation to demonstrate the potential benefit psychiatric inpatient treatment may have for treating anxiety, mania, depression, psychosis and well-being for adolescents presenting with imminent safety concerns. It is important to contextualize these findings in two keys ways— (1) this is an uncontrolled study so given it is without a comparison group, outcomes need to be interpreted with caution, and (2) findings are specific to 2 assessment timepoints within 15 days of inpatient treatment. Considering psychiatric inpatient treatment is often designed as acute-care, this study demonstrates benefits specific to acute care with an average LOS of approximately 2 weeks. Acute-care LOS varies nationally with some as short as 5 days, so our findings may suggest that 2 weeks is an adequate amount of time but may not generalize to shorter acute-care inpatient programs.
Psychiatric inpatient treatment is often indicated for adolescents with the most severe symptoms and safety concerns. Finding that patients with the more extreme symptoms at admissions show the greatest improvement is generally used as a classic example of “regression to the mean,” but in the context of this research study, this finding also reflects that patients in acute distress generally do not stay at that elevated level. Although perhaps driven at least in part by statistical regression effects and spontaneous improvement, it is still reassuring that the adolescents with the most severe symptom presentations experience symptom reduction in inpatient settings. This further lays a foundation for understanding who may benefit the most from psychiatric inpatient treatment, particularly when inpatient beds are limited throughout the United States. In turn, it is possible that adolescents presenting with the highest level of symptom severity were “flagged” by the treatment team and provided with the most intensive psychological services available within inpatient treatment such as more frequent individual and family therapy sessions and/or behavior plans, further aiding symptom improvement.
This study extends the body of research on MBC for inpatient adolescents as research on MBC within inpatient care has primarily focused on feasibility (Waitz et al., 2025). Acute LOS for inpatient adolescents necessitates outcomes data that are readily accessible to staff and intuitive so that clinicians can utilize data in real time. It is possible that there was a transactional effect whereby assessment information was provided to the patient and, in turn, led to greater symptom improvement.
Limitations
There are a number of notable limitations to this study regarding the interpretation and generalizability of our findings. First, these analyses were restricted to 15 days of inpatient treatment, representative of an acute length of stay, which was not necessarily the point of discharge for all adolescent patients. It is possible that symptom improvement may plateau or that symptoms may worsen with prolonged inpatient LOS or may continue a trajectory of improvement. Second, these findings demonstrate improvements within the context of inpatient treatment, and it is unknown if and how symptom improvements generalize post discharge. Waitz and colleagues assert that follow-up data after discharge would be beneficial in investigating the long-term impacts of psychiatric inpatient treatment including DBT (Waitz et al., 2021). Although follow-up can be challenging to conduct in clinical settings, it is an important piece in establishing treatment effectiveness for higher levels of care (Waitz et al., 2021). Third, while treatment likely had some impact on symptom improvement, this finding should be considered with caution given that there was no control comparison group. It is possible that the effect of time, rather than inpatient treatment and/or components of inpatient treatment (i.e., DBT, psychopharmacology) may be considerable factors leading to stabilization and driving symptom improvement.
Measurement was also limited in several ways. First, measurement only assessed symptoms of anxiety, mania, depression, psychosis, and well-being. Additional symptoms and related diagnoses would be beneficial to research including but not limited to post-traumatic stress disorder, attention deficit hyperactivity disorder, obsessive compulsive disorder, and personality disorders. Additional important domains of functioning to assess include emotion regulation, family conflict/environment, life problems, and ways of coping. Second, data were limited only to patient self-report. A multi-informant approach is commonly used in inpatient psychiatric settings to understand a patient’s overall functioning and to provide a holistic view of the patient. This was not feasible for this study due to limited resources; team members did not have time or capacity to consent caregivers for research or to collect assessment measures from them as they typically present for either a family therapy session or during visiting hours. Incorporating caregiver MBC of patients’ symptoms is important to obtain adequate assessments in adolescents. Caregiver-youth agreement is poor in most cases at the symptoms level, particularly for depression, suicidal ideation, anxiety, and conduct disorder, whereby caregivers under or overestimate this symptomatology (Lauth et al., 2010). Third, data did not include a tool to assess response bias so it is possible that patients may have “faked good” to facilitate discharge or “faked bad” as there may be secondary gains to continuing inpatient treatment.
Conclusions, Future Directions, and Clinical Implications
There are numerous important recommendations for future research directions and related clinical implications within inpatient psychiatric units for adolescents. First, it is strongly recommended that future research examine admission and discharge symptom improvement according to MBC. This study examined a timeframe of approximately 15 days, which was the average LOS but not specifically admission and discharge timepoints for assessment. Second, patients as well as hospital programs are often categorized as acute versus chronic or intermediate, and it is recommended that research examine these two different categories of patients and treatment to inform evidence-based practice for adolescent inpatient treatment and to further examine the potential for iatrogenic effects with prolonged length of stay. Related, there is variability within the definition of “acute” care, and future research should explore if admissions ranging from 5 to 7 days are comparable in treatment outcome findings to 10–14 days, for example. Such data can establish guidelines for decision making pertaining to admission to psychiatric inpatient treatment versus Emergency Department extended observation (e.g., Comprehensive Psychiatric Emergency Program) versus follow up with behavioral health urgent care clinics.
Third, it is indicated to expand measurement in a number of ways including additional diagnoses (e.g., post-traumatic stress disorder using the Child PTSD Symptom Scale [Foa et al., 2001]), symptoms (e.g., Emotion Regulation Questionnaire [Gullone and Taffe, 2012]), and domains of functioning (e.g., DBT Ways of Coping Checklist [Neacsiu et al., 2010]); caregiver report; and with using measures that are culturally tailored to meet the specific needs of the population recognizing that most outcome instruments are developed originally in English and based on Western cultural contexts (van Widenfelt et al., 2005). Including culturally supported, validated assessments is important for the most accurate and evidence-based treatment in youth who are psychiatrically hospitalized.
Lastly, we simply and strongly call for continued treatment outcome research for inpatient adolescents. Resources meant to guide practitioners providing inpatient treatment are increasing within the field, and the field is still in great need of more research and evidence-based treatment guidelines within inpatient psychiatric units for adolescents.
Authors’ Contributions
A.T.M. and E.S. contributed to this study with conceptualization, methodology, resources, data curation, writing original draft, and writing review and editing. S.G. and W.C. contributed to this study with methodology, data curation, formal analysis, writing original draft, and writing review and editing.
Ethical Considerations
This study received ethical approval from the Feinstein Institutes for Medical Research, Northwell Health, IRB (approval #X 23-0474) on February 11, 2025. The IRB indicated this study is approved as exempt. It is a retrospective study, all patient information was deidentified, and patient consent was not required. Patient data will not be shared with third parties.
Footnotes
Acknowledgments
The authors would like to thank their patients and patients’ caregivers for their engagement in treatment. The authors would also like to thank the full treatment team for their dedication and commitment to evidence-based practice.
Author Disclosure Statement
The authors have no financial interests, competing interests, or acknowledgements to report.