
Abstract
Background:
Sleep disturbance is common in youth with mood disorders and correlates with mood symptom burden. Insomnia polygenic risk scores (PRS), computed from adult genome-wide association study (GWAS) data, are associated with sleep disturbance among youth within the general population. However, no studies have examined insomnia-PRS in a clinical sample of youth with mood disorders.
Methods:
Participants included 374 youth aged 13–20 years, 247 with mood disorders (135 bipolar disorder [BD] and 112 major depressive disorder) and 127 controls. Insomnia-PRS was constructed using an adult insomnia GWAS (N = 360,738). Sleep disturbance was computed using the most severe lifetime insomnia and hypersomnia (i.e., excessive sleep) items from the Kiddie Schedule for Affective Disorders and Schizophrenia Depression Rating Scale. General linear models or logistic regressions examined main effects of insomnia-PRS on sleep disturbance and psychiatric characteristics (mood symptom severity, anxiety comorbidity, suicide risk, global functioning), controlling for age, sex, and genetic principal components.
Results:
Insomnia-PRS was higher in youth with mood disorders versus controls (p = 0.03, d = 0.24). Insomnia-PRS was associated with insomnia severity in youth with mood disorders (p = 0.03, ηp2 = 0.02), and with mania severity in youth with BD (p = 0.03, ηp2 = 0.03), although the insomnia severity finding did not survive Bonferroni correction. In sex-stratified analyses, insomnia-PRS was significantly associated with insomnia (p = 0.02, ηp2 = 0.03), depression (p = 0.02, ηp2 = 0.03), and mania (p = 0.02, ηp2 = 0.05) severity in females but not males. There were no significant findings for excessive sleep.
Conclusions:
This study extends prior findings linking adult-derived insomnia-PRS with insomnia in youth with mood disorders, with evidence of differences related to sex and BD. These preliminary findings suggest that sleep and mood in youth may be sensitive to adult-derived insomnia-PRS.
Introduction
Sleep is of central importance to adolescence, a key maturational period marked by significant changes in sleep architecture (Blake et al., 2018). Sleep disturbance is highly common and debilitating in youth, and is related to neurological development, physical health (e.g., obesity, diabetes), and psychological health (e.g., depression; Gariepy et al., 2020). There is well-established evidence of a bidirectional association between sleep disturbance and depression, such that sleep disturbance is both a prodromal symptom and clinical manifestation of depression (Li et al., 2016; Lovato and Gradisar, 2014). Depression, a characteristic of mood disorders including major depressive disorder (MDD) and bipolar disorder (BD), is the single leading cause of functional disability in youth (Gore et al., 2011). Sleep disturbance is associated with exacerbated symptom severity, episode relapse, suicidal thoughts and behaviors, and poorer functioning in both youth and adults with mood disorders (Comsa et al., 2022; Freeman et al., 2020; Lovato and Gradisar, 2014). It has also been suggested that insomnia within depression may comprise a biologically distinct subtype (Lamers et al., 2010). Despite clear influence from mood and environmental factors (e.g., early school start times, late bedtimes, social media use before bed) (Bartel et al., 2015; Gradisar et al., 2011), sleep disturbance often persists during periods of normal mood and appears to be partly driven by genetic factors (Pillai et al., 2011).
Insomnia is a type of sleep disturbance that appears to be both heritable and polygenic in nature. This is evidenced by twin studies yielding moderate heritability estimates (15–40%) and genome-wide association studies (GWAS) implicating a large number of single nucleotide polymorphisms (SNPs) significantly associated with insomnia (Jansen et al., 2019; Madrid-Valero et al., 2021). Several studies emphasize the association between genetic liability for sleep disturbance (i.e., insomnia, sleep duration) and mood disorders in adults. For instance, polygenic risk scores (PRS) for insomnia were associated with insomnia among adults with MDD, whereas similar associations were not observed for hypersomnia (Melhuish Beaupre et al., 2021). In another study, insomnia-PRS was not significantly associated with BD case status, but was significantly associated with BD subtype, particularly BD-II (Lewis et al., 2020). Interestingly, the genetic-sleep–depression association may be bidirectional, with several youth and adult studies demonstrating significant associations between polygenic risk for MDD and BD with insomnia and sleep duration (Dennison et al., 2021; Ohi et al., 2021; Pesonen et al., 2019; Wainberg et al., 2023). Together, these results lend support to the theory that genetic factors influence sleep and psychiatric health in adults with mood disorders.
Comparatively fewer studies have focused on the genetic underpinnings of sleep in youth. This is concerning, as sleep disturbance is strongly associated with suicide risk in youth, an age group for whom suicide is a leading cause of death (Liu et al., 2019). Sleep architecture undergoes distinct changes throughout adolescence (e.g., decreased slow wave sleep and circadian sleep phase delays), increasing risk for sleep disturbance and insomnia that persist throughout adulthood (Colrain and Baker, 2011; Johnson et al., 2006). Despite developmental changes, adolescent and adult insomnia are marked by similar psychological (e.g., negative cognitive styles, stress reactivity) and physiological (e.g., high-frequency cortical EEG activity, cognitive hyperarousal) vulnerability factors (Yuksel et al., 2022). Longitudinal twin studies further highlight that genetic factors explain most of the variance in the persistence of insomnia and sleep disturbance throughout adolescence (Gregory et al., 2009), estimates similar to those in adults (Barclay et al., 2015). To date, insomnia-PRS, derived from adult GWAS summary statistics, has only been explored in youth within the general population, with most reporting significant associations between adult-derived insomnia-PRS and sleep disturbance (Kocevska et al., 2024; Koshmanova et al., 2022; Ma et al., 2021; Zhang et al., 2025). Further, three studies in general population samples of youth of European ancestry demonstrate that higher adult-derived insomnia-PRS is associated with worse overall childhood psychopathology (Akingbuwa et al., 2020; Hernandez et al., 2023; Waszczuk et al., 2023; Zhang et al., 2025), with one study reporting positive correlations with internalizing symptoms in a large sample of over 42,000 youth aged 6–17 years (Akingbuwa et al., 2020).
Despite the well-established deleterious clinical correlates of sleep disturbance in youth with mood disorders, no studies have examined insomnia-PRS in relation to clinically validated measures (i.e., derived from structured psychiatric interviews) of sleep disturbance and psychiatric symptoms in this population. The current study aimed to examine adult-derived insomnia-PRS in a clinical sample of youth with mood disorders. For our primary analysis, we hypothesize that adult-derived insomnia-PRS will be associated with insomnia and hypersomnia symptoms. For secondary analyses, we hypothesize that insomnia-PRS will be associated with more severe psychiatric characteristics, as reflected by four themes: mood symptom severity, anxiety comorbidity, suicide risk, global functioning. Exploratory analyses will examine sex-related and diagnosis-specific effects.
Methods
Participants
This study included 374 youth aged 13–20 years, recruited through a subspecialty clinic at a tertiary academic health sciences center in Toronto, Ontario, Canada. Participants meeting criteria for a lifetime mood disorder were eligible. This included youth with MDD (unipolar depression), as well as BD (bipolar depression), if there had been a lifetime major depressive episode. Youth with BD-I, -II, or Other Specified Bipolar and Related Disorder (OSBRD; comparable to Bipolar Disorder Not Otherwise Specified [BD-NOS]) were eligible based on participation in the Center for Youth Bipolar Disorder’s clinical research registry. A control group was recruited from the community based on the following criteria: (1) no lifetime major psychiatric diagnoses (i.e., BD, MDD, schizophrenia); (2) no first- or second-degree family history of BD or other psychotic disorders. This study was approved by the institutional research ethics board, and written informed consent was provided by participants and at least one parent or guardian prior to study commencement.
Diagnostic and clinical interviews
All assessments were conducted by research staff trained and supervised by the senior author, and held at minimum a bachelor’s or master’s degree in a health science field. Youth and parent/guardian were interviewed to determine current and lifetime psychiatric diagnoses, including MDD and BD, using the Kiddie Schedule for Affective Disorders and Schizophrenia for School Age Children, Present and Lifetime Version (K-SADS-PL) (Kaufman et al., 1997). Diagnoses were made in accordance with DSM-IV criteria for data collected from September 2009 to June 2018, and DSM-5 criteria for data collected from July 2018 to 2024. Participants were diagnosed with MDD if they met criteria for a lifetime major depressive episode. Diagnoses were confirmed using all available information, including youth and parent interviews and any available medical records, and by consensus meetings with a licensed child and adolescent psychiatrist following interviews.
The K-SADS-PL Depression Rating Scale (DRS) and Mania Rating Scale (MRS) were used to determine most severe lifetime depression severity (“lifetime depression severity”) and most severe lifetime mania severity in youth with BD (“lifetime mania severity”) (Kaufman et al., 1997). As mania is a defining feature of BD that is not present in unipolar depression, lifetime mania severity was examined in youth with BD only. For secondary analyses examining insomnia-PRS in relation to depression severity, lifetime depression severity was determined based on a total score of all items within the K-SADS-PL DRS, with the exclusion of the DRS lifetime insomnia and hypersomnia items, adjusted by the number of items answered. Additional clinical characteristics examined in secondary analyses included global functioning, suicide risk, and lifetime anxiety diagnosis, measured as follows: the Children’s Global Assessment Scale was used to score youth’s global functioning during the most severe past mood episode, over the past month, and highest level of functioning over the past year (Shaffer et al., 1983). Lifetime non-suicidal self-injury and lifetime suicide attempt were gathered via the Adolescent Longitudinal Interval Follow-up Evaluation (ALIFE) Self-Injurious/Suicidal Behavior Scale interview and the Columbia Suicide Severity Rating Scale (C-SSRS), youth version (Keller et al., 1987; Posner et al., 2011). Suicide attempt was defined as a nonfatal self-injurious behavior carried out with at least some intent to die (Posner et al., 2007; 2011). Self-injurious behavior that did not meet the criteria of suicide attempt was defined as non-suicidal self-injury, deduced from the K-SADS-PL DRS or C-SSRS (Kaufman et al., 1997; Posner et al., 2007; 2011). Lifetime anxiety disorders were also gathered from the K-SADS-PL and combined into one “Any Anxiety Disorder(s)” variable, which encompassed generalized anxiety disorder, social anxiety disorder, separation anxiety disorder, agoraphobia, panic disorder, and any other specified/unspecified anxiety disorder. Socioeconomic status was evaluated from the Hollingshead Four-Factor Index (Hollingshead, 2011). Additional details regarding assessment of demographic and clinical characteristics are reported in Supplementary Data.
Characterization of sleep disturbance
Sleep disturbance was derived from the K-SADS-PL DRS item 11 “Insomnia” and item 12 “Hypersomnia.” For the purpose of this study, both sleep disturbance items were assessed during the most severe lifetime depressive episode. The insomnia item was rated on a scale from 1 to 6 with the following anchors: 1 “Not at all,” 2 “Slight,” 3 “Mild,” 4 “Moderate,” 5 “Severe,” 6 “Extreme.” A score of 3 is the cut-off for lifetime insomnia defined by the K-SADS-PL DRS scoring manual. The hypersomnia item was also rated on a scale from 1 to 6 with the following anchors: 1 “Not at all,” 2 “Occasionally sleeps more than usual,” 3 “Frequently sleeps at least 1 hour more than usual, or regularly sleeps much longer if not forced out of bed by parent or other authority,” 4 “Frequently sleeps at least 2 hours more than usual,” 5 “Frequently sleeps at least 3 hours more than usual,” 6 “Frequently sleeps 4 hours more than usual.” A score of 4 is the threshold cut-off for lifetime hypersomnia defined by the K-SADS-PL DRS scoring manual. The International Classification of Sleep Disorders—Third Edition categorizes hypersomnia associated with psychiatric disorders under the Central Disorders of Hypersomnolence, characterized by excessive daytime sleepiness not attributable to other neurological sleep disorders or circadian abnormalities (Sateia, 2014). Given the focus on extended sleep quantity in the DRS definition of hypersomnia, the term ‘excessive sleep’ will be used throughout to distinguish this score from the neurologically defined central disorders of hypersomnolence. Pittsburgh Sleep Quality Index (PSQI) data were available for a subset of participants and correlations of the PSQI subscales with DRS lifetime insomnia and excessive sleep severity items and insomnia-PRS were examined (Buysse et al., 1989).
Polygenic risk scores
Saliva samples (∼2 mL) were obtained from participants using an Oragene OG-500 DNA kit (DNA Genotek Oragene-500 kits; DNA Genotek Inc., Ottawa, Canada). Participants were instructed to abstain from chewing gum, eating, and drinking for 30 minutes before saliva collection. Detailed methods regarding DNA extraction, genotyping, genetic quality control, and imputation are shown in Supplementary Data. PRS for each participant in our sample was constructed using summary statistics from a recent insomnia GWAS in adults of European ancestry (PGS003328_hmPOS_GRCh37.txt.gz downloaded from the PGS catalogue) (Ma et al., 2022). Given that multi-ancestry GWAS are not yet available, the current sample includes only genetically European youth. Methods regarding genetics-based inclusion criteria can be found in Supplementary Data. The summary statistics for 960,097 SNPs had been adjusted by PRS-CS-auto, a Bayesian-based method that applies a continuous shrinkage prior on SNP effect sizes from the discovery GWAS summary statistics. The PRSs were subsequently calculated using PRSice2 and then standardized to mean of 0 and standard deviation of 1.
Statistical analysis
IBM SPSS version 27 (IBM Corp., Armonk, New York) was used to perform all statistical analyses. The Shapiro-Wilk test was used to assess normality for all continuous variables. Group differences in demographic and clinical characteristics were evaluated using t-tests for continuous variables and χ2 tests for categorical variables. An analysis of covariance (ANCOVA) was conducted to examine group differences in insomnia-PRS accounting for age, sex, and the first two genetic principal components. Mann–Whitney U-tests were used to assess group differences for variables that were not normally distributed. Statistical significance was set at p < 0.05. Spearman rank-order correlations assessed the correlation coefficients of the PSQI subscales with DRS sleep items and insomnia-PRS. General linear models (GLM) were used to examine the main effects of insomnia-PRS on sleep disturbance (DRS lifetime insomnia and excessive sleep severity items) as primary analyses. Secondary analyses included examining associations of insomnia-PRS with psychiatric characteristics using GLM for continuous variables (lifetime depression severity, lifetime mania severity [BD group only], global functioning) or binary logistic regressions for categorical variables (lifetime comorbid anxiety diagnosis, non-suicidal self-injury, active suicidal ideation, and suicide attempt). Exploratory analyses included examining insomnia-PRS effects in diagnostic (BD vs. MDD) and sex subgroups, and by incorporating an insomnia-PRS × sex interaction term into the primary models. All analyses controlled for age, sex, and the first two genetic principal components. Effect sizes were reported using partial eta squared (ηp2), an estimate of proportion of variance explained.
Correction for multiple comparisons was conducted for primary analyses examining insomnia-PRS in relation to sleep disturbance using Bonferroni correction on a family-wise basis (i.e., dividing the significance level by the number of primary statistical analyses, i.e., α = 0.05/2 = 0.025). Given the exploratory nature of the current study, we also report uncorrected p-values for secondary and exploratory analyses to inform future studies.
Sensitivity analyses were conducted for primary analyses including the following covariates in separate models: age of mood disorder onset, age of most severe lifetime depressive episode, body mass index [BMI], lifetime psychiatric medication use, and all 10 genetic principal components. A post-hoc sensitivity analysis using G*Power 3.1 (version 15) indicated a minimum detectable effect size of f2 ≥ 0.03 for a linear multiple regression model (F test; fixed model R2 increase), given the mood disorder sample size (n = 247), α = 0.05, one predictor, and four covariates.
Results
Demographic and clinical characteristics
The study sample included 374 youth: 247 with a lifetime mood disorder (112 MDD, 135 BD) and 127 controls. Demographic and clinical characteristics of the overall sample are presented in Table 1. Clinical characteristics of the mood disorder group are in Supplementary Table S1. In comparison to the control group, the mood disorder group was significantly older, had lower socioeconomic status, had a greater proportion of female participants, and had higher BMI. Demographic and clinical characteristics of youth with MDD vs. BD are in Supplementary Table S2. Relative to youth with MDD, youth with BD were more advanced in pubertal development, had more severe depression and mania symptoms, were more likely to use selective serotonin reuptake inhibitors (SSRIs), lithium, and second-generation antipsychotics (SGAs).
Demographic and Clinical Characteristics of Overall Sample
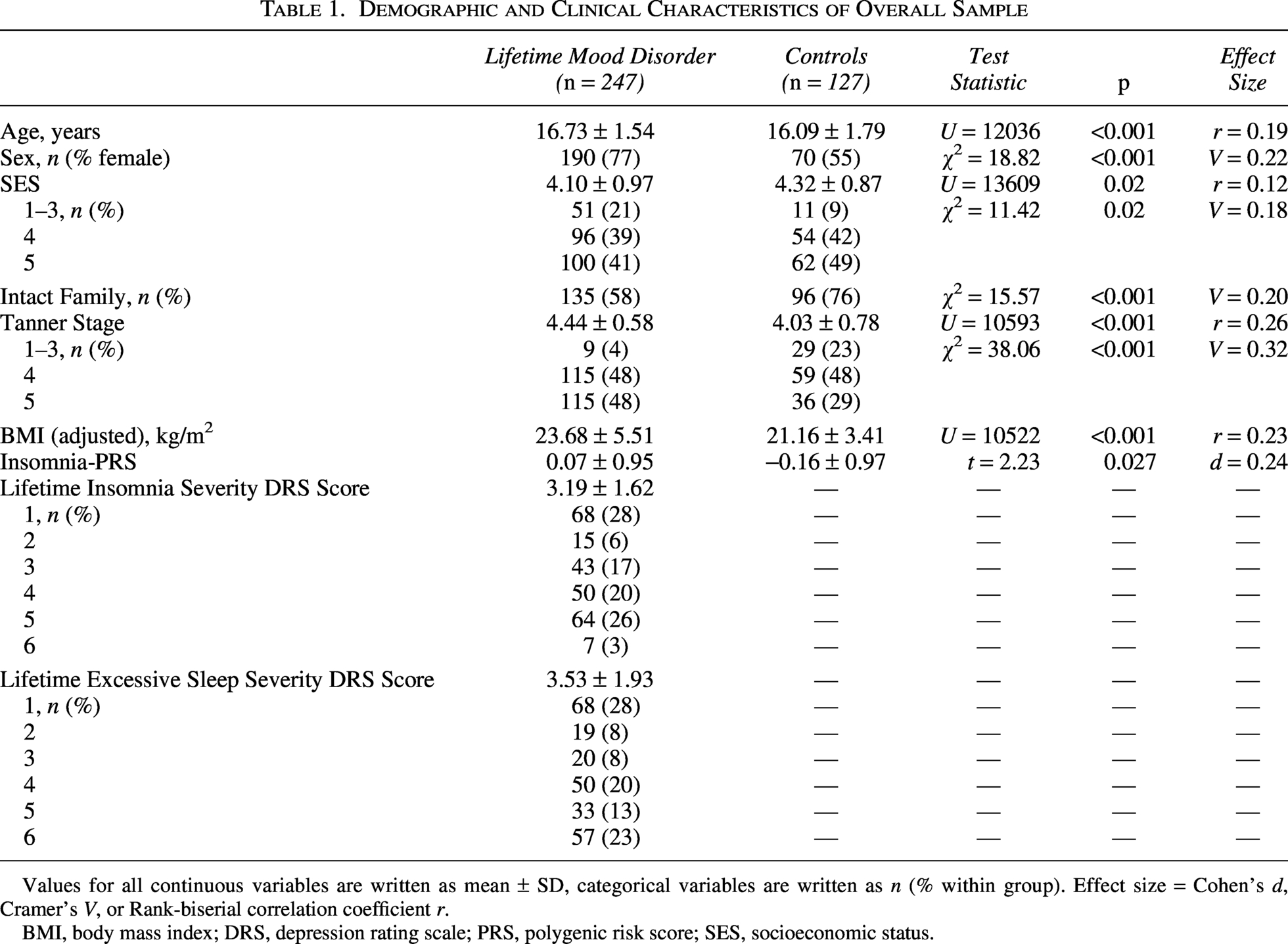
Values for all continuous variables are written as mean ± SD, categorical variables are written as n (% within group). Effect size = Cohen’s d, Cramer’s V, or Rank-biserial correlation coefficient r.
BMI, body mass index; DRS, depression rating scale; PRS, polygenic risk score; SES, socioeconomic status.
Group differences in insomnia-PRS
Youth with mood disorders had significantly higher insomnia-PRS compared to controls (p = 0.03, d = 0.24), which remained significant after controlling for age, sex, and the first two genetic principal components (F[1, 368] = 4.21, p = 0.04, ηp2 = 0.01). There were no significant differences in insomnia-PRS, insomnia severity, or excessive sleep severity based on sex or diagnosis (BD vs. MDD). Detailed information regarding sex and diagnostic differences in sleep disturbance characteristics and insomnia-PRS can be found in Supplementary Table S3 and Supplementary Table S4.
Correlation with PSQI subscales
The DRS lifetime insomnia severity item was significantly correlated with PSQI global score, subjective sleep quality, and sleep latency (Table 2). The DRS lifetime excessive sleep severity item was not associated with any PSQI subscale (Table 2). Insomnia-PRS was significantly correlated with PSQI global score, sleep duration, and sleep efficiency (Table 2). Given the limited sample with PSQI data, primary analyses continued to focus on DRS lifetime insomnia severity. Demographic and clinical characteristics of the PSQI sample are presented in Supplementary Table S5.
Correlations of Pittsburgh Sleep Quality Index (PSQI) Subscales with Lifetime Insomnia and Excessive Sleep Severity Depression Rating Scale Items, and Insomnia-PRS in Mood Disorder Sample
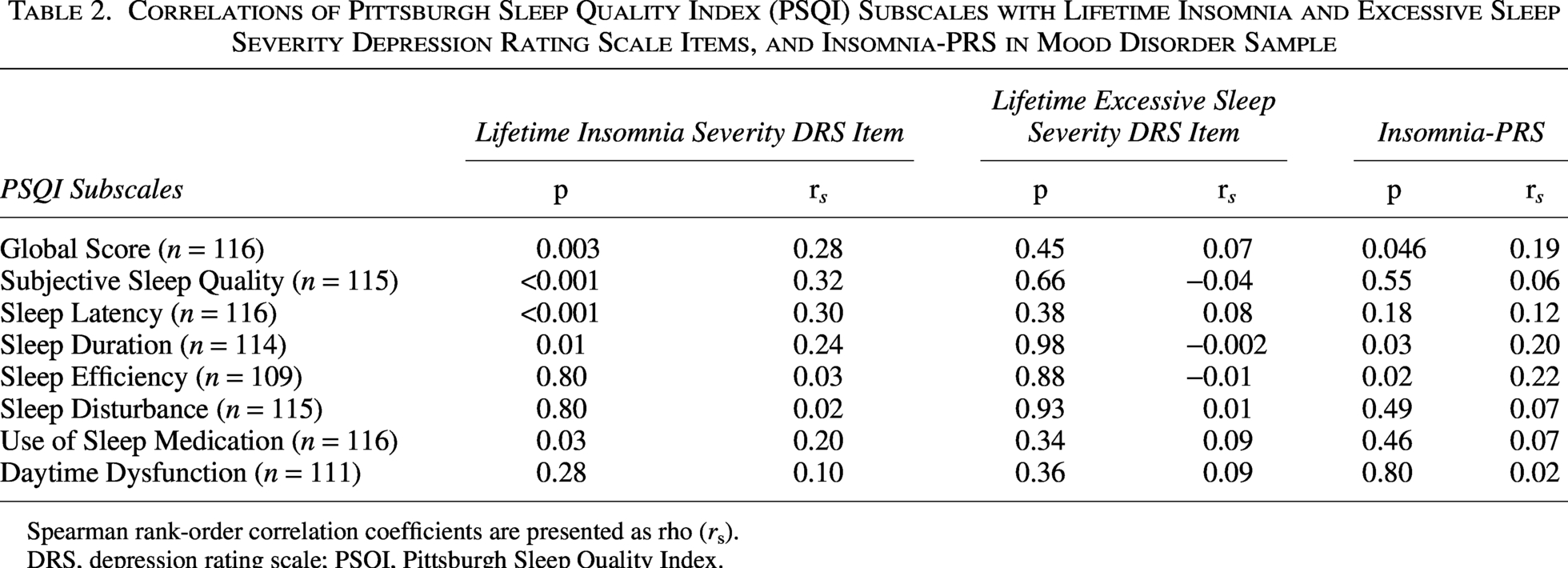
Spearman rank-order correlation coefficients are presented as rho (rs).
DRS, depression rating scale; PSQI, Pittsburgh Sleep Quality Index.
Insomnia-PRS and sleep disturbance
Insomnia-PRS was significantly associated with lifetime insomnia severity in youth with mood disorders (Fig. 1; B = 0.24, p = 0.03, ηp2 = 0.02). The insomnia-PRS explained 1.3% of variance in insomnia severity in youth with mood disorders. This association did not survive Bonferroni correction (α = 0.025). The association between insomnia-PRS and lifetime excessive sleep severity was not significant (B = 0.15, p = 0.26, ηp2 < 0.01). The association of insomnia-PRS with lifetime insomnia severity was significant in females (Fig. 2; B = 0.30, p = 0.02, ηp2 = 0.03) but not males with mood disorders (B = 0.01, p = 0.96, ηp2 < 0.01). There were no significant insomnia-PRS by sex interaction effects (insomnia severity: B = 0.26, p = 0.31, ηp2 < 0.01, excessive sleep severity: B = 0.11, p = 0.61, ηp2 < 0.01). In diagnostic subgroups, insomnia-PRS was not significantly associated with insomnia severity (BD: B = 0.26, p = 0.09, ηp2 = 0.02; MDD: B = 0.16, p = 0.35, ηp2 < 0.01) or excessive sleep severity (BD: B = 0.22, p = 0.24, ηp2 = 0.01; MDD: B = 0.06, p = 0.74, ηp2 < 0.01).
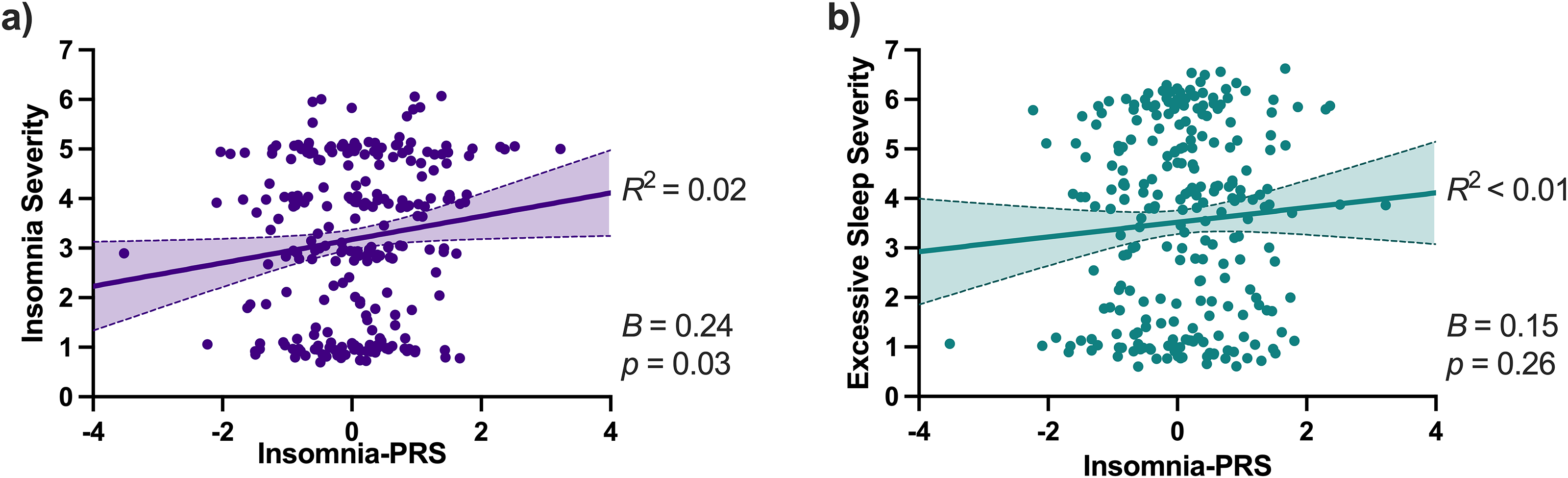
Associations of insomnia-PRS with sleep disturbance in youth with mood disorders. Note: Covariate-adjusted values plotted on both x- and y-axes. Higher insomnia-PRS was associated with
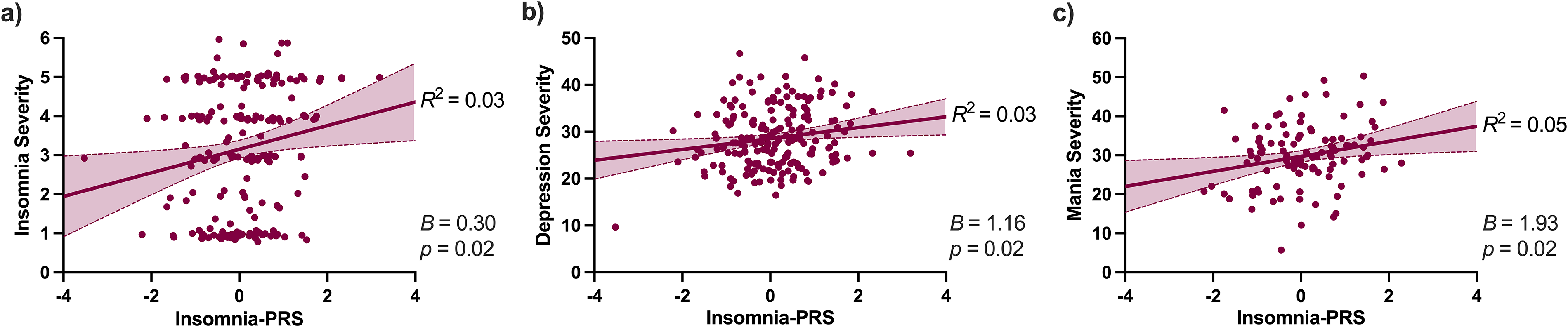
Association of insomnia-PRS with clinical characteristics in female youth with mood disorders (n = 190). Note: Covariate-adjusted values plotted on both x- and y-axes. Higher insomnia-PRS was associated with significantly higher
Psychiatric correlates of insomnia-PRS
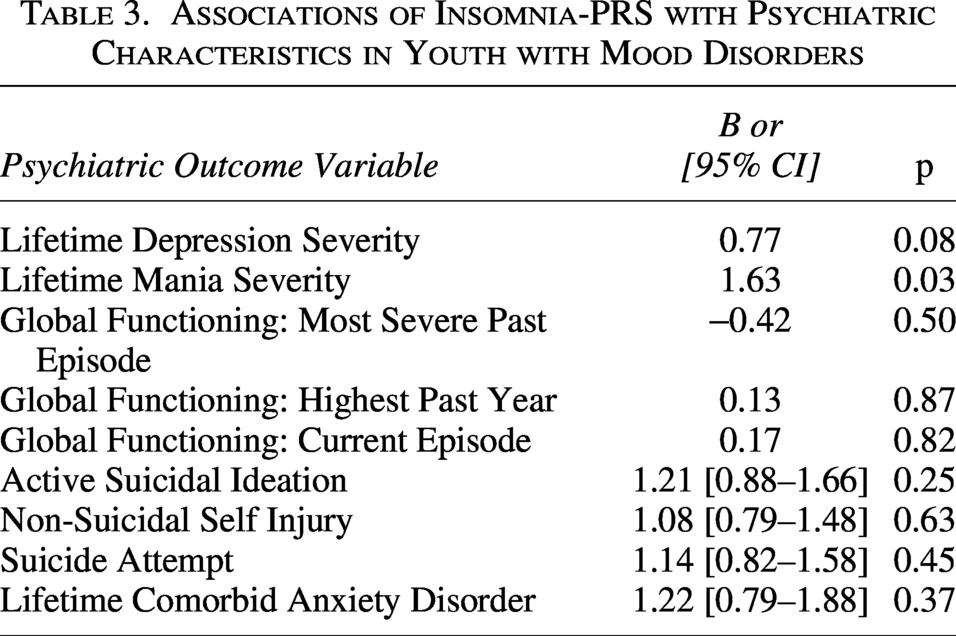
In youth with mood disorders, insomnia-PRS was not significantly associated with any examined psychiatric characteristic (Table 3); lifetime depression severity (B = 0.77, p = 0.08, ηp2 = 0.01), global functioning (during the most severe past mood episode: B = −0.42, p = 0.50, ηp2 < 0.01; highest past year: B = 0.13, p = 0.87, ηp2 = 0.00; current episode: B = 0.17, p = 0.82, ηp2 < 0.01), suicidal ideation (odds ratio [OR] 1.21, 95% CI 0.88–1.66), p = 0.25), nonsuicidal self-injury (1.08 [0.79–1.48], p = 0.63), suicide attempt (1.13 [0.82–1.58], p = 0.45), presence of lifetime comorbid anxiety disorders (1.22 [0.79–1.88], p = 0.37). In the BD only group (Fig. 3), insomnia-PRS was significantly associated with lifetime mania severity (B = 1.63, p = 0.03, ηp2 = 0.03). Sex Subgroups: In female youth with mood disorders, insomnia-PRS was significantly associated with lifetime depression severity (Fig. 2) (B = 1.34, p = 0.019, ηp2 = 0.03), and non-significantly associated with lifetime suicidal ideation (1.46 [0.99–2.15], p = 0.058). In the subgroup of female youth with BD (Fig. 2), insomnia-PRS was significantly associated with lifetime mania severity (B = 1.93, p = 0.020, ηp2 = 0.05). There were no significant psychiatric correlates of insomnia-PRS in male youth with mood disorders.
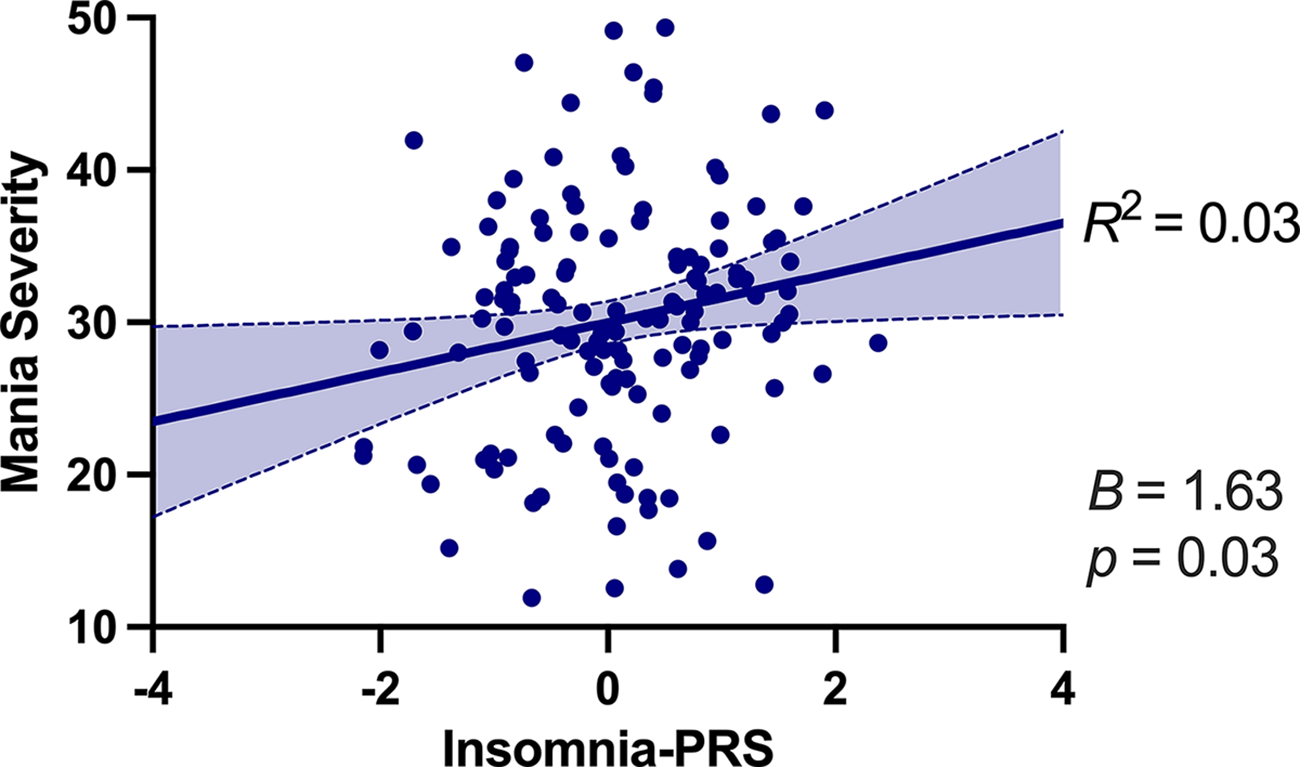
Association of insomnia-PRS with mania severity in youth with bipolar disorder. Note: Covariate-adjusted values plotted on both x- and y-axes. Higher insomnia-PRS was associated with significantly higher mania severity in youth with BD. PRS, polygenic risk score.
Associations of Insomnia-PRS with Psychiatric Characteristics in Youth with Mood Disorders
Sensitivity analyses
The association between insomnia-PRS and insomnia severity remained significant in sensitivity analyses controlling for age of mood disorder onset (B = 0.26, p = 0.02, ηp2 = 0.02), age of most severe lifetime depressive episode (B = 0.24, p = 0.03, ηp2 = 0.02), BMI (B = 0.30, p = 0.009, ηp2 = 0.03), lifetime psychiatric medication use (B = 0.18, p = 0.04, ηp2 = 0.01), and all 10 genetic principal components (B = 0.24, p = 0.03, ηp2 = 0.02).
Discussion
This study set out to examine associations of an adult-derived insomnia-PRS with sleep disturbance and psychiatric characteristics within a clinical sample of youth with mood disorders. We found that youth with mood disorders had elevated insomnia-PRS as compared to controls. Higher insomnia-PRS was associated with significantly higher insomnia severity among youth with mood disorders. These findings were independent of BMI and psychiatric medication use. While disrupted sleep is considered both a predictor and a consequence of mood symptoms, the current genetic findings provide preliminary evidence that insomnia severity among youth with mood disorders may be influenced in part by genetic factors.
The differences in insomnia-PRS between the mood disorder group and controls was anticipated. Sleep disturbance is a core symptom of depression based on DSM criteria and sleep disturbance is recognized as a criterion that distinguishes adolescents with depression from controls in population-based studies. Moreover, elevated insomnia-PRS has previously been reported in adults with MDD (Xu et al., 2025). Similarly, insomnia-PRS is associated with greater insomnia severity in population-based studies of youth (Kocevska et al., 2024; Ma et al., 2021; Madrid-Valero et al., 2024). The variance of DRS lifetime insomnia symptom severity explained by insomnia-PRS was comparable to, and in some cases larger than, the variance in sleep disturbance and mood disorders explained by either insomnia-PRS or MDD-PRS in prior youth samples (Kocevska et al., 2024; Ma et al., 2021; Ohi et al., 2021; Rabinowitz et al., 2020). While the effect sizes we observed were modest, this grounds our findings relative to existing literature. Nonetheless, it is important to note that, similar to other chronic diseases (Hughes et al., 2020), modest effect sizes already guide therapeutic treatment in youth with depressive symptoms (Eckshtain et al., 2020; Weisz et al., 2006; 2017).
The relative lack of psychiatric correlates in the current study was unexpected. We opted to examine well-established psychiatric correlates of sleep disturbance (e.g., mood symptom severity, suicide risk, and global functioning). However, prior studies have demonstrated associations between insomnia-PRS and broader indices of childhood psychopathology in community-based samples of youth (Akingbuwa et al., 2020; Hernandez et al., 2023; Waszczuk et al., 2023; Zhang et al., 2025). It is possible that insomnia-PRS may be more closely associated with other domains of psychopathology not examined in this study. Null findings may also reflect clinical heterogeneity or gene-environment interactions not captured in the present analyses (Madrid-Valero et al., 2024; Zhang et al., 2025). The association of insomnia-PRS with mania severity in the BD group was expected based on the fact that sleep disturbance is a well-established predictor of BD onset and mania in youth, alongside the known association of BD with circadian dysfunction. While present findings highlight only mania severity, other studies have demonstrated significant genetic correlations of insomnia with both BD and MDD (Baranova et al., 2022; O’Connell et al., 2021). Exploring circadian genes that are common to both insomnia-PRS and BD-PRS may give additional insight into mechanisms underlying the present findings regarding mania severity.
Study findings may highlight sub-populations in whom insomnia-PRS may be particularly relevant. Our exploratory analyses suggest that higher insomnia-PRS was significantly associated with higher insomnia, depression, and mania severity in female, but not male, youth with mood disorders. However, given the absence of significant insomnia-PRS by sex interaction effects, and the limited statistical power in the male subgroup, these results should be interpreted as hypothesis-generating rather than evidence of confirmed sex-specific effects. Future large-scale and prospective studies are needed to evaluate potential female-specific vulnerability to the negative clinical phenotypes associated with insomnia polygenic risk. While sex differences in insomnia genetic risk have yet to be fully explored in youth (Jansen et al., 2019; Madrid-Valero et al., 2021), there does appear to be a female preponderance of insomnia symptoms that emerges after puberty (Calhoun et al., 2014; Johnson et al., 2006). In addition, sleep disturbance in youth predicts future depression in females but not males (Conklin et al., 2018).
Several female-specific biological, cognitive, and psychosocial factors could be contributing to sex differences in sleep disturbance, such as pubertal development and menstrual hormone fluctuations (Manber and Armitage, 1999; Morssinkhof et al., 2020), as well as vulnerability to stress and negative cognitive styles (de Zambotti et al., 2018; Hamilton et al., 2015). Beyond the effects of sex, there are also youth-specific environmental mediators of the relationship between insomnia-PRS and sleep disturbance, including social jet lag, early school start times and later bedtimes, and artificial light at night (Bartel et al., 2015; Paksarian et al., 2020; Singh et al., 2023; Sun et al., 2025). Together, these data underscore the importance of early sleep-focused interventions among young females with mood disorders.
Limitations
This study has several limitations. First, sleep disturbance was ascertained from two sleep-related items from a diagnostic interview for depression, based on the most severe lifetime depressive episode. A more comprehensive sleep scale may have provided a more sensitive assessment. However, we observed significant correlations of DRS sleep items and insomnia-PRS with PSQI subscale scores, a validated sleep scale in adults and youth (de la Vega et al., 2015; Mollayeva et al., 2016; Raniti et al., 2018). Additional details regarding demographic and clinical characteristics of the PSQI sample are reported in Supplementary Table S5. As we continue to collect data, future analyses will examine PSQI subscales as a primary outcome. Moreover, because the sleep disturbance item was scored within the context of a depressive episode, we were unable to adequately assess sleep disturbance among controls and therefore limited analyses exploring sleep disturbance to the mood disorder group. This limited the ability to fully interpret the specificity of the observed associations between insomnia-PRS and sleep-related or clinical measures in the patient groups. Relatedly, we did not use gold-standard polysomnography given that the current study is a secondary analysis of a more broadly focused research project. This is important in light of evidence that there are discrepancies between objective and subjective sleep disturbance in youth (Munkhjargal et al., 2022). Power for the male subgroup analyses was limited by the comparatively small subgroup size. While effects within the mood disorder group were modest for both males and females, effect sizes were nonetheless larger in the female subgroup. Finally, our insomnia-PRS was derived from summary statistics of an insomnia GWAS conducted in adults of European ancestry. Therefore, the present insomnia-PRS may not be fully generalizable to youth with diverse ancestral origins (Ruan et al., 2022). Multiethnic GWAS are underway and will inform future studies.
Conclusions
This study extends prior findings linking adult-derived insomnia-PRS with insomnia symptoms in youth with mood disorders, with preliminary evidence of sex differences and differences related to BD. We found that insomnia-PRS is associated with insomnia severity in youth with mood disorders, particularly females, and is specifically associated with mania severity in youth with BD. Future prospective studies with repeated objective and detailed subjective sleep measures are needed to clarify sex and diagnostic differences in the sleep-depression interface in youth.
Clinical Significance
Exploring insomnia polygenic risk may offer insights into potential mechanisms underlying sleep disturbance, and if replicated, may eventually inform effective sleep and depression interventions that are specific to youth. Trials in adults show that mood disorder interventions influence sleep (Ballesio et al., 2018; DeMartinis and Winokur, 2007; Herrero Babiloni et al., 2021; Liu et al., 2025; Pu et al., 2023; Riemann et al., 2020), while youth trials show that improvements in sleep can predict improvements in depression (Courtney et al., 2022). Thus, optimization of sleep health may be a key therapeutic target. Consistent with this, sleep interventions reduce depressive symptoms in clinical adult and nonclinical youth samples (Gee et al., 2019). Upon validation in larger and multi-ancestral samples, insomnia-PRS may further inform clinical trial stratification and support sleep-focused interventions aimed at improving outcomes in youth with mood disorders.
Authors’ Contributions
A.A.P. contributed to conceptualization, data curation, formal analysis, visualization, and writing (original draft). M.M. contributed to conceptualization, data curation, formal analysis, supervision, and writing (reviewing/editing). M.K.D. contributed to methodology and writing (reviewing/editing). C.C.Z. contributed to data curation, formal analysis, methodology, and writing (reviewing/editing). M.I.B. contributed to writing (reviewing/editing). J.S.R. contributed to writing (reviewing/editing). B.I.G. contributed to conceptualization, funding acquisition, methodology, project administration, resources, supervision, and writing (reviewing/editing).
Ethical Considerations
Ethical approval was granted by Sunnybrook Research Institute Research Ethics Board (REB #230/2009 and #376/2010). All data were collected at Sunnybrook Research Institute. Subsequent to a move to the CAMH, where analyses were undertaken, ethics approval was also granted by the local Research Ethics Board (REB #148/2020 and #149/2020).
Consent to Participate
Informed consent was obtained from all participants and their parent and/or guardian prior to participating.
Data Availability
The datasets used and analyzed in this study are available from the corresponding author on reasonable request. This data is not publicly available due to privacy or ethical restrictions.
Footnotes
Acknowledgments
The authors would like to thank all study participants, their families, and staff for their contributions to this study.
Author Disclosure Statement
B.I.G. acknowledges research funding from the CIHR, Heart & Stroke Foundation of Canada, the CAMH Foundation, and the University of Toronto Department of Psychiatry Miner’s Lamp Fund Innovation fund. Outside of the submitted work, M.I.B. reports consulting fees and honoraria from Takeda, Lundbeck Pharmaceuticals, Jazz Pharmaceuticals, Paladin Labs, Eisai and the OntarioMD Peer Leader Program; travel support from McGill University; and receipt of sleep equipment or research support from Itamar Medical, Braebon Medical Corporation, and CGX. A.A.P., M.M., M.K.D., C.C.Z., and J.S.R. have reported no biomedical financial interests or potential conflicts of interest.
Funding Information
This study was supported by the Centre for Addiction and Mental Health (CAMH) Discovery Fund, philanthropic donations to the Centre for Youth Bipolar Disorder, and the Canadian Institutes of Health Research (CIHR) (L.T. Young, MOP 84414). Dr. Benjamin I. Goldstein acknowledges his position as RBC Investments Chair in Children’s Mental Health and Developmental Psychopathology at CAMH, a joint Hospital-University Chair between the University of Toronto, CAMH, and the CAMH Foundation.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.