
Abstract
Background:
Family promoting positive emotions (FPPE) is a dyadic, positive affect-focused preventive intervention shown to reduce perceived stress and emotional symptoms among children of mothers with elevated depressive symptoms, a population at heightened risk for psychopathology. Emerging evidence suggests that contextual disadvantages (e.g., socioeconomic, neighborhood) may shape vulnerability for major depressive disorder in children. The present study examined whether family- and neighborhood-level disadvantage moderated children’s response to FPPE relative to a psychoeducation comparison condition, with the goal of informing precision prevention efforts for high-risk families.
Methods:
Participants included 74 children (ages 8–12 years; 46.3% female) and their biological mothers with elevated depressive symptoms (i.e., Patient Health Questionnaire scores ≥ 8). Following random assignment, 47 dyads were assigned to FPPE, and 27 dyads were assigned to a written information psychoeducation condition. Neighborhood and family-level disadvantage was assessed using the Child Opportunity Index (COI) scores and family-level income-to-needs ratio (INR), respectively. Parent-reported child perceived stress and emotional distress (depressive, anxiety, and anger symptoms) were assessed pre- and post-intervention using the Perceived Stress Scale and Patient-Reported Outcomes Measurement Information System Emotional Distress Scales.
Results:
Family-level INR did not moderate intervention effects. Results revealed a significant time × group × COI interaction for child-perceived stress, such that greater neighborhood disadvantage was associated with a larger reduction in child-perceived stress pre-to-post intervention in the FPPE but not the written information group. No other significant effects emerged.
Conclusions:
FPPE was most effective in reducing perceived stress among children of mothers with elevated depression symptoms exposed to greater neighborhood-level disadvantage, suggesting that a positive valence system (PVS) may be a particularly sensitive and proximal preventive intervention target through which downstream reductions in stress occur. These findings suggest that youth facing both intergenerational and environmental risk may benefit the most from dyadic, positive affect-focused interventions to reduce stress. Research should test downstream effects of FPPE on clinical symptoms emerging over longer periods.
Keywords
Introduction
Psychiatric disorders affect approximately 16.5% of youth each year (National Alliance on Mental Illness, 2025), making the prevention of youth psychopathology an urgent public health priority. Children of mothers with elevated depressive symptoms are at higher risk for developing psychopathology and often exhibit earlier onset, greater chronicity, and poorer outcomes compared to their lower-risk peers (Bell et al., 2004; Goodman et al., 2011; Hammen, 2009; Murray et al., 2011; Weissman et al., 2016). Although preventive interventions show promise for supporting this higher-risk population, responses to such programs are likely to vary as a function of individual and contextual disadvantages (e.g., socioeconomic, neighborhood). Because maternal history of depression increases the risk of psychopathology in offspring, clarifying how disadvantage moderates the effectiveness of preventive treatment strategies may help prevent mental health problems in this higher-risk population.
Recent work by Burkhouse and colleagues (2023) offers promising initial evidence for a dyadic preventive intervention, family promoting positive emotions (FPPE), aimed at reducing risk for the emergence of clinical symptoms in offspring of mothers with elevated depressive symptoms. Given evidence that high-risk youth frequently exhibit blunted reward responsiveness, a pattern associated with later depressive symptom onset (Burkhouse and Kujawa, 2023; Kujawa and Burkhouse, 2017) and heightened stress reactivity (Goldstein et al., 2020), FPPE was developed to target positive valence systems (PVS; Burkhouse and Kujawa, 2023; Kujawa and Burkhouse, 2017) functioning. PVS encompasses several neural and behavioral processes involved in reward anticipation, motivation, reinforcement learning, and the experience of pleasure (Cuthbert and Insel, 2013). Critically, alterations in PVS functioning may diminish youths’ ability to engage with positive environmental experiences and to draw on such experiences as a buffer against stress, thereby increasing vulnerability to psychopathology across development (Roberts et al., 2025). Thus, FPPE was designed to engage mothers with elevated depressive symptoms and their school-aged children in structured, skills-based activities aimed at enhancing positive emotions and reward responsiveness within the parent-child dyad.
In the initial pilot efficacy trial, compared to a written information (WI) comparison condition, participation in FPPE was associated with improvements in parent-reported child-perceived stress and symptoms of depression, anxiety, and anger (Burkhouse et al., 2023). Youth in FPPE also exhibited relative increases in daily ratings of positive affect, consistent with the intervention’s mechanistic focus on strengthening PVS-related processes. This preliminary study highlighted both the promise of mechanism-targeted, family-based prevention approaches and the need to identify predictors of intervention response. Clarifying individual and contextual factors that influence FPPE response may inform the refinement and personalization of preventive interventions for youth at elevated risk for depression.
Emerging evidence suggests that the effectiveness of early preventive interventions may be shaped by contextual factors that influence youth’s exposure to chronic stress and disadvantage (Mennis et al., 2022). Notably, disadvantage at both the family and neighborhood levels, including limited financial resources and reduced access to community and educational supports, has been shown to interact with maternal depression history to shape reward processing and may represent one potential moderator of FPPE response. For example, Granros and colleagues (2023) demonstrated that reduced reward responsiveness was most evident among offspring of mothers with a lifetime history of depression residing in more socioeconomically disadvantaged neighborhoods, suggesting that contextual disadvantage may exacerbate reward-related vulnerabilities conferred by maternal depression. Complementing these findings, Israel and colleagues (2025) showed that higher levels of neighborhood disadvantage were associated with reduced reward responsiveness in children, with effects particularly pronounced among those with a parental history of major depressive disorder. In addition, Roberts and colleagues (2025) recently found that blunted neural reward response predicted increases in depressive symptoms, with effects strongest for youth experiencing lower income-to-needs and higher neighborhood disadvantage. Together, this work indicates that disadvantage and maternal depression interact to heighten disruptions in PVS functioning, rather than operating as independent risk factors. These findings underscore the importance of examining disadvantage as a predictor of response to FPPE among offspring of mothers with elevated depressive symptoms. Understanding how contextual disadvantage shapes FPPE response may be critical for identifying which youth are most likely to benefit from PVS-targeted prevention efforts and for tailoring preventive interventions to specific populations.
Building on evidence that maternal depression and disadvantage jointly disrupt positive valence system (PVS) functioning (Granros et al., 2024; Israel et al., 2025), the present study sought to examine whether disadvantage shaped children’s response to FPPE among offspring of mothers with experiencing elevated depressive symptoms. To address this question, disadvantage was operationalized across multiple ecological levels, including family-level risk (income-to-needs ratio [INR]) and neighborhood-level opportunity (Child Opportunity Index [COI]). This multilevel approach allows us to determine which forms of disadvantage-related risk confer heightened sensitivity to a PVS-focused preventive intervention, thereby clarifying which youth derive the greatest benefit from FPPE and informing more precise targeting of preventive efforts.
Given mixed prior findings, we considered two possible patterns regarding the direction of moderation effects. On one hand, some work suggests that socioeconomic adversity imposes chronic stressors and time demands that may undermine engagement with preventive interventions (Castro-Ramirez et al., 2021). This outcome raises the possibility that greater disadvantage across INR and COI would be associated with outcomes for FPPE, but not the WI control condition. On the other hand, there is some evidence that interventions targeting PVS functioning may be especially potent for youth exposed to heightened environmental adversity (Mennis et al., 2022). Thus, this research raises the alternative possibility that greater disadvantage would be associated with larger improvements in perceived stress and emotional symptoms following FPPE, but not in the WI control condition.
Methods
Participants
Participants were recruited for a pilot randomized controlled trial of FPPE for mothers with elevated depressive symptoms and their 8- to 12-year-old children (Burkhouse et al., 2023). Recruitment strategies included outreach through local schools, community organizations, and nation-wide social media advertisements to identify interested mother–child dyads. All procedures were conducted through electronic questionnaires and video calls (i.e., Zoom), allowing for enrollment across the United States. Interested dyads completed screening, including assessment of maternal depressive symptoms, and baseline assessments prior to random assignment to either the FPPE intervention or a WI control condition. Eligible families included biological mothers reporting elevated depressive symptoms, defined as a score of 8 or above on the Patient Health Questionnaire (Kroenke, Spitzer, & Williams, 2001), and their children within the target age range (i.e., 8–12 years). Exclusion criteria were designed to ensure participants could engage meaningfully in the preventive intervention and included factors such as severe developmental or medical conditions that would interfere with participation. Significant developmental or intellectual disabilities, psychotic disorders, bipolar or mania, as well as current substance use problems were also exclusion criteria. To focus on prevention, mothers who reported current depressed mood or anhedonia in their child (present for more than half the days in the past 2 weeks based on the Diagnostic Statistical Manual of Mental Disorders, 5th Edition Level 1 Cross-Cutting Symptom Measure; Bastiaens and Galus, 2018) were excluded. Following screening, consent, and baseline assessment, 74 eligible participants were randomized to an intervention (47 FPPE, 27 to WI). Of these, 55 completed all intervention sessions and post-intervention measures (29 in FPPE, 26 in WI; see also Burkhouse et al., 2023, for full consort diagram).
As reported in the initial trial, youth were 43.2% girls, 55.4% boys, and 1.4% nonbinary, with a mean age of 9.68 years (SD = 1.24). In terms of race and ethnicity, 13.7% of children identified as Hispanic or Latinx, 16.4% as Black or African American, 1.4% as Asian, 72.6% as White, and 9.6% as another identity. Mothers were 38.20 years of age (SD = 6.03), and 9.5% identified as Hispanic or Latinx, 16.2% as Black or African American, 74.3% as White, 1.4% as Asian, 1.4% as Native Hawaiian/Pacific Islander, and 5.4% as Other or Biracial. Furthermore, 86.4% of mothers completed a college degree, and the median household income was $70,000–$79,999 (range: $0–$9.999 to $100,000+). Demographic characteristics of FPPE versus WI dyads are presented in Table 1.
Demographic Characteristics of Families Assigned to FPPE (n = 47) versus WI (n = 27)
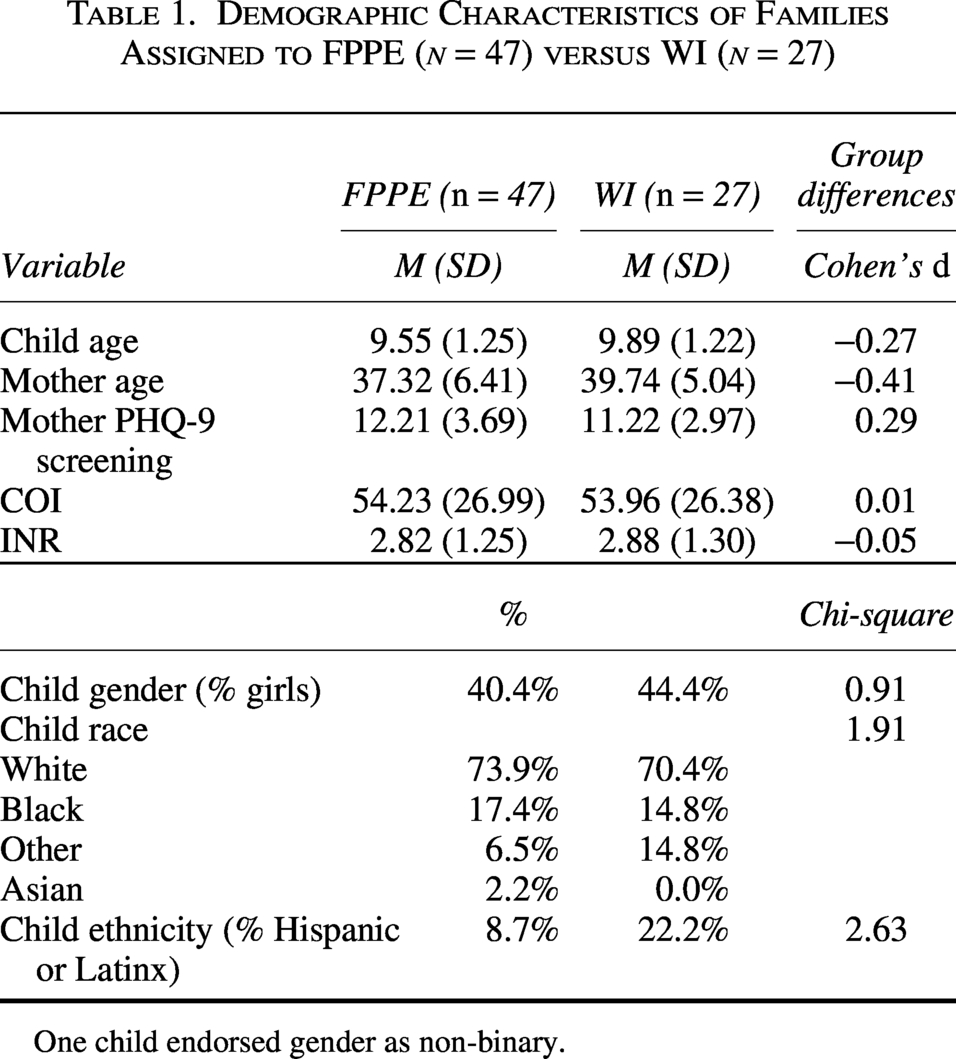
One child endorsed gender as non-binary.
Study procedures were approved by the
Procedures
Eligible mother–child dyads were randomized to either the FPPE group or the WI comparison group after completing baseline assessments. Measurements of child clinical symptoms included child-reported and parent-reported survey data. Surveys were completed by mothers and children electronically using REDCap. Symptom assessments (i.e., PROMIS Emotional Distress Scale measures, NIH Toolbox Perceived Stress Scale) were collected at baseline and post-intervention (8 weeks later). Given findings from the initial analyses of clinical outcomes, which demonstrated intervention effects only for parent-reported symptoms (Burkhouse et al., 2023), the current study focused exclusively on moderators of parent-reported change in child symptoms. This approach reduces the number of analyses and prioritizes the most robust indicators of FPPE response. Participants’ residential addresses were collected at baseline for neighborhood geocoding analysis.
Families assigned to FPPE participated in a structured, manualized eight-session preventive intervention designed to enhance positive emotions in high-risk children (Burkhouse et al., 2023). Sessions were administered by a masters- or PhD-level skills coach supervised by licensed clinical psychologists. Mothers first completed a brief orientation session with a skills coach to review session recommendations (e.g., minimizing distractions, offering praise). Each intervention session began with an icebreaker, followed by homework review with positive reinforcement, introduction of new content, dyadic practice, and collaborative goal setting. Participants received workbooks to summarize skills and track progress. For more details on session content, see Burkhouse and colleagues (2023). Families assigned to the WI control condition were sent materials weekly for 8 weeks. Materials included information about symptoms and signs of depression and coping skills for children and adolescents, as well as resources for mental health services.
Measures
Emotional distress
Measures of children’s emotional distress included the Patient-Reported Outcomes Measurement Information System (PROMIS). The PROMIS Emotional Distress scales assessed children’s symptoms of anxiety (e.g., “My child said that he/she felt worried”), anger (e.g., “My child felt mad”), and depression (e.g., “My child said that he/she felt sad”) over the past week. Each subscale (i.e., anxiety, anger, depression) includes 5–15 items rated on a 5-point scale. Each subscale was examined separately in analyses. Higher scores indicated higher levels of symptoms. These measures have been validated for youth 8–12 years old (Fries, Bruce, & Cella, 2005). Analyses focused on parent-reported anxiety, anger, and depression in children at baseline and post-intervention. Pre-intervention parent report was missing for one WI family.
Perceived stress
The NIH Toolbox Perceived Stress Scale (PSS) was used to measure children’s perceived stress levels. This validated measure includes 10 items describing subjective experiences of stress in the past month (e.g., “How often did your child appear nervous and “stressed”?”; Cohen, Kamarck, & Mermelstein, 1983; Kupst et al., 2015). Each item was scored on a 5-point scale. Higher scores indicated higher levels of symptoms. Analyses focused on parent-reported child perceived stress scores at baseline and post-intervention. The PROMIS subscales and PSS demonstrated acceptable to good internal consistency both pre- and post-intervention (Burkhouse et al., 2023).
Disadvantage
Two indices of disadvantage were used in analyses. First, neighborhood disadvantage was measured by the Child Opportunity Index (COI; version 3.0, 2020 census tracts), which is a validated, percentile-ranked index of neighborhood opportunity and resource availability comprised of publically available data on neighborhood education, health and environment, and social and economic opportunities from various sources (e.g., the American Community Survey, the Department of Education, the Environmental Protection Agency; Noelke et al., 2024). These factors are scored and averaged to calculate a COI composite index. Nationally normed COI composite indices (i.e., scored from 0 to 100) were used for analyses in the current study. Youth neighborhood COI was determined based on the census tract of their home address at the time of study enrollment. Of the 69 dyads with census tract data, all but two dyads (i.e., 97.10%) in this sample resided within different census tracts (i.e., defined geographic areas within counties). In the current sample, COI scores ranged from 1 to 96 (M = 54.13, SD = 26.56). Second, family-level disadvantage was measured by income-to-needs ratio (INR). INR was calculated as the total parent-reported family income divided by the federal poverty level based on family household size. Family income data were grouped into $10,000 increments, from “$0 to $9,999” to “$100,000 and above.” INR ranged from 0.23 to 5.80 (M = 2.84, SD = 1.26). INR and COI were significantly related (r = 0.40, p < 0.001).
Data Analysis
Given the proof-of-concept nature of the study and limited power in this pilot sample, we conducted intention-to-treat analyses, which preserve randomization and provide unbiased estimates of intervention effects under real-world conditions, including noncompliance and attrition. Primary analyses were conducted with all families enrolled in the study (FPPE n = 47; WI n = 27) (see supplement for analyses with only intervention completers, which demonstrated the same pattern of findings; FPPE n = 29; WI n = 26). First, independent samples t-tests were conducted in SPSS (version 31) to assess if differences in indices of disadvantage (INR or COI) were found between participants in the FPPE and WI groups at baseline. Of note, we had INR data for all 74 participants (FPPE n = 47; WI n = 27) but COI data only for 69 participants (FPPE n = 43; WI n = 26) given missing addresses or discrepancies in data. Second, mixed-design Analysis of Covariances (ANCOVAs) were conducted to test group (FPPE vs. WI) × time (pre- and post-intervention) × disadvantage (COI or INR) effects on primary outcome measures (parent-reported child emotional distress and perceived stress). ANCOVAS were run using restricted estimation maximum likelihood (REML) with the lme4 package in R, including all participants who completed intake measures and were randomized to an intervention (47 in FPPE, 27 in WI). REML estimation allowed us to include participants with missing census tract data. To interpret the directionality of effects, follow-up regression analyses included difference scores as the outcome. Regressions were estimated using full information maximum likelihood (FIML), which is well suited for regression models with incomplete data and allows inclusion of participants with partially missing data. The use of different estimators reflects differences in model type (mixed-effects vs. regression), rather than differences in analytic sample. Because neighborhood opportunity (indexed by COI) and household socioeconomic status (indexed by INR) represent related but distinct levels of disadvantage, models examining COI included INR as a covariate, and models examining INR included COI as a covariate, allowing us to estimate the unique contribution of each index of disadvantage (Taylor et al., 2020). For significant effects, we also evaluated whether significant findings were maintained when adjusting for child age, child gender, and maternal depressive symptoms. Child gender was examined using multiple coding schemes to ensure robustness of findings: (a) a binary variable excluding the nonbinary participant, (b) boy versus not boy, and (c) girl versus not girl.
Results
Descriptive statistics of parent-reported symptoms measures pre- and post-intervention are presented in Table 2.
Pre- (FPPE n = 47; WI n = 26) and Post- (FPPE n = 29; WI n = 26) Intervention Parent Report Measure
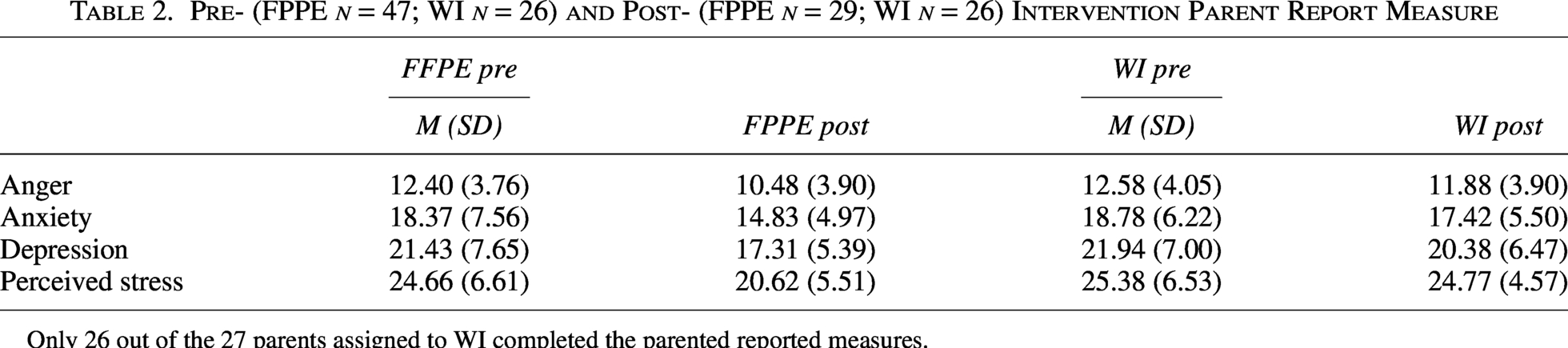
Only 26 out of the 27 parents assigned to WI completed the parented reported measures.
Group differences in neighborhood and family-level disadvantage
An independent samples t-test indicated no significant difference in COI between WI (M = 53.96, SD = 26.38) and FPPE (M = 54.23, SD = 26.99), t(67) = −0.04, p = 0.968, Cohen’s d = −0.01. Similarly, there was no significant difference in INR between WI (M = 2.88, SD = 1.30) and FPPE (M = 2.82, SD = 1.25) t(72) = 0.19, p = 0.851; Cohen’s d = 0.05.
COI and parent-reported child outcomes
As shown in Table 3, effects of time on parent-reported child-perceived stress, anger, anxiety, and depression were all significant (ps < 0.042). Results also revealed a significant main effect of time and time × group interaction for changes in parent-reported child perceived stress scores. These interactions were qualified by a time × group × COI interaction.
Main and Interactive Effects of Time, Group, and Child Opportunity Index on Child Outcomes
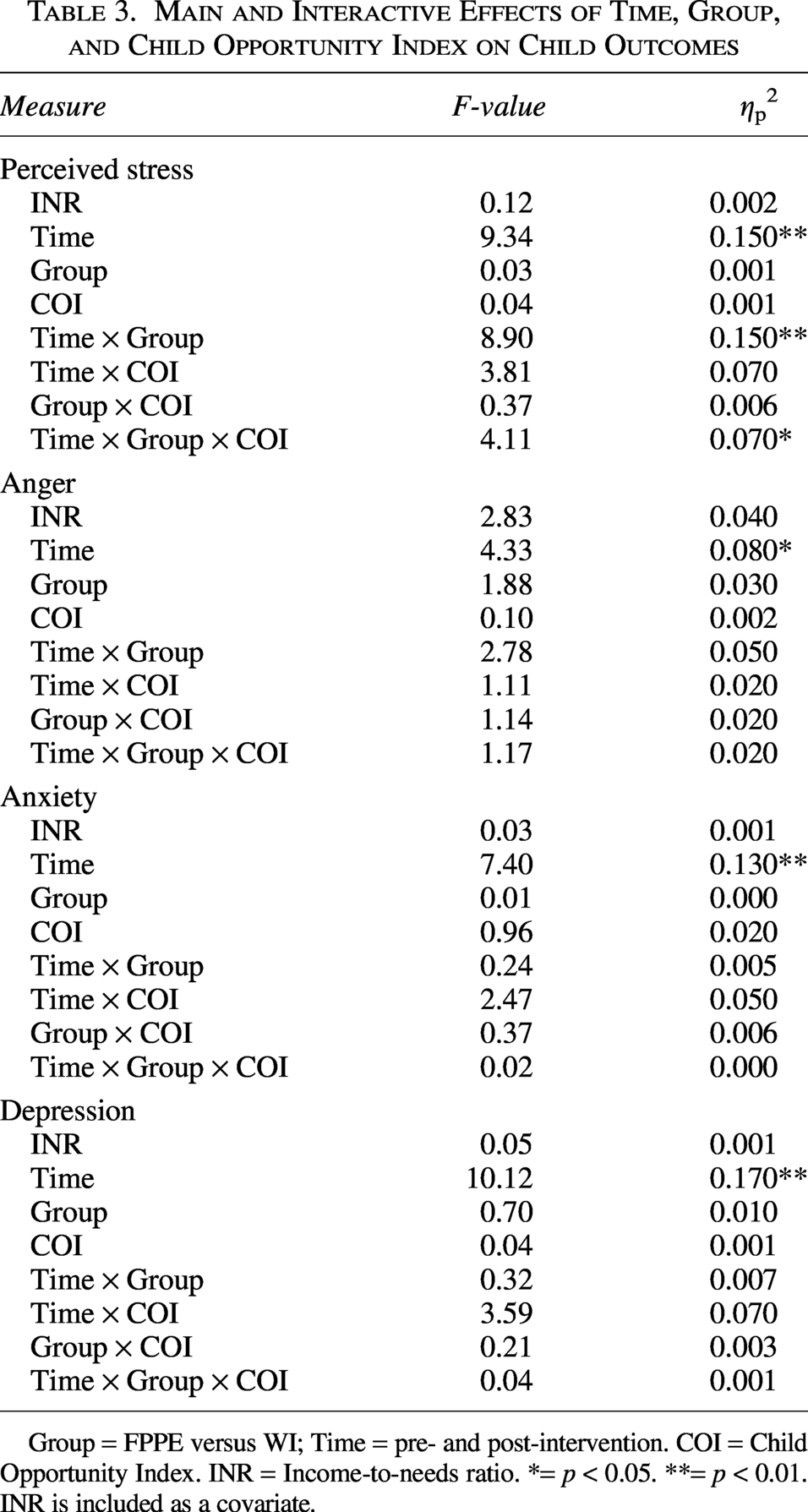
Group = FPPE versus WI; Time = pre- and post-intervention. COI = Child Opportunity Index. INR = Income-to-needs ratio. *= p < 0.05. **= p < 0.01. INR is included as a covariate.
To probe the time × group × COI interaction, we examined the time × COI interaction on perceived stress separately for group. Follow-up analyses revealed that the time × COI interaction on perceived stress was significant for families in FPPE, F(1, 30.67) = 7.58, p = 0.010, ηp2 = 0.20, but not for families in WI, F(1, 22.75) = 0.001, p = 0.980, ηp2 = <0.001.
To further characterize this effect, we conducted regression models predicting change in perceived stress (post minus pre scores; more negative scores indicate greater decreases) separately within each group, using FIML estimation and covarying for baseline perceived stress and INR. In the FPPE group, greater neighborhood disadvantage (i.e., lower COI) predicted greater decreases in perceived stress (i.e., more negative difference scores) over time (β = 0.32, p = 0.032; see Fig. 1). In contrast, COI was not predictive of perceived stress changes in the WI group (β = 0.09, p = 0.511; see Fig. 1).
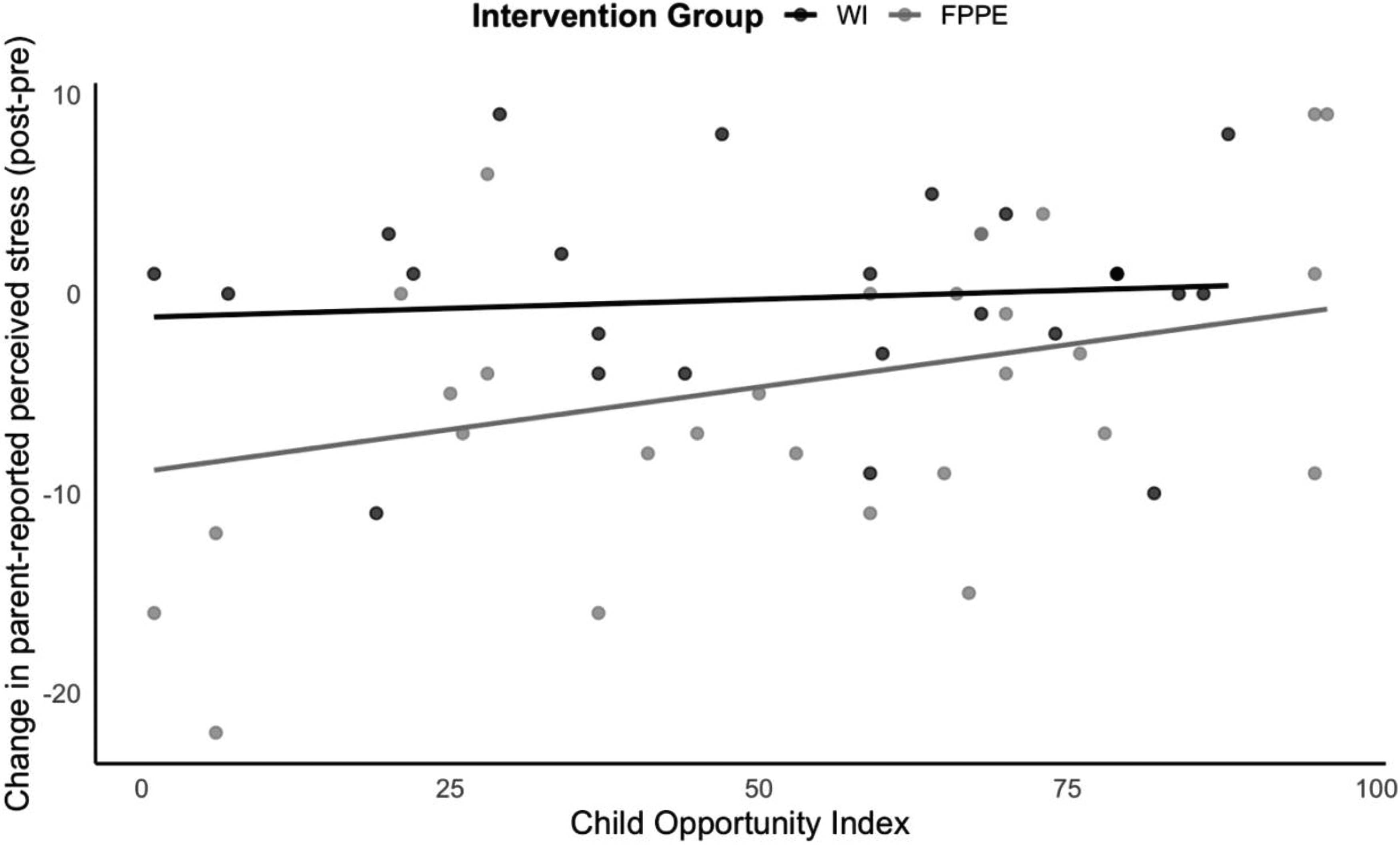
Scatterplot depicting the interaction between Child Opportunity Index (COI) and condition (FPPE vs. WI) on changes in parent-reported child perceived stress pre and post intervention. Child Opportunity Index (COI) is on the x-axis. Change in parent-reported perceived stress was measured as the difference between post intervention scores and pre intervention scores for parent-reported child perceived stress. More negative scores indicate greater decreases in symptoms.
The time × group × COI interaction for perceived stress remained significant when covarying for child age, F(1, 52.09) = 4.08, p = 0.049, ηp2 = 0.07; maternal depression scores at screening, F(1, 52.28) = 4.11, p = 0.048, ηp2 = 0.07; and child gender, regardless of coding scheme-binary (excluding the non-binary participant: F(1, 50.74) = 5.59, p = 0.022, ηp2 = 0.10; boy vs. not boyF(1, 52.19) = 4.24, p = 0.044, ηp2 = 0.08; and girl vs. not girl: F(1, 52.03) = 4.19, p = 0.046, ηp2 = 0.07).
INR and parent-reported child outcomes
As shown in Table 4, results revealed no significant main or interactive effects for time, group, or INR on parent-reported child outcomes.
Main and Interactive Effects of Time, Group, and Income-to-Needs Ratio
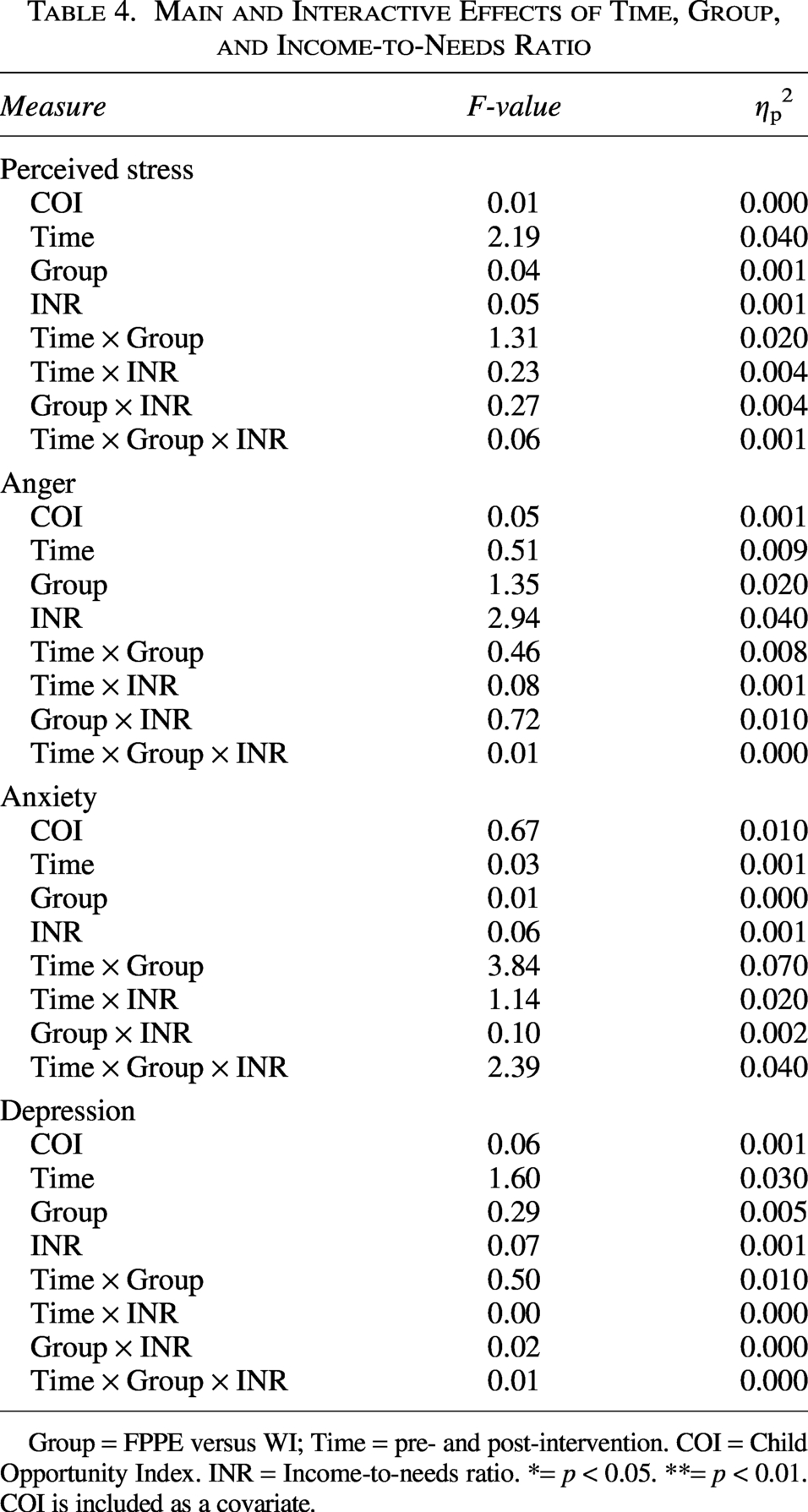
Group = FPPE versus WI; Time = pre- and post-intervention. COI = Child Opportunity Index. INR = Income-to-needs ratio. *= p < 0.05. **= p < 0.01. COI is included as a covariate.
Discussion
Building on evidence that disadvantage (e.g., neighborhood and family-level) and maternal depression jointly heighten disruptions in PVS functioning (Granros et al., 2024; Israel et al., 2025; Roberts et al., 2025), the present study tested whether contextual risk factors (i.e., family INR and neighborhood COI) moderated changes in children’s perceived stress and emotional symptoms in response to the FPPE prevention program. Prior analyses showed FPPE effects on reducing parent-reported perceived stress and emotional distress (Burkhouse et al., 2023). For the current study, we explored competing hypotheses regarding the direction of moderation effects. We found that neighborhood disadvantage emerged as a significant moderator of intervention effects on perceived stress, such that children residing in more disadvantaged neighborhoods showed greater reductions in perceived stress in the FPPE condition, but not in the WI control condition. These results highlight larger neighborhood context as a key factor shaping intervention response and point to FPPE as a potentially targeted prevention program for stress reduction among children facing elevated neighborhood disadvantage.
In prior research, stress has been linked to reduced PVS functioning, a core mechanism implicated in the development of psychopathology (Kujawa et al., 2020; Pizzagalli, 2014). Our findings suggest that neighborhood disadvantage may heighten children’s responsiveness to family-focused preventive intervention that explicitly target positive affect and reward processing. Emerging evidence indicates that neighborhood disadvantage is associated with blunted reward responsiveness, particularly among children of parents with a history of depression (Granros et al., 2024; Israel et al., 2025), a pattern directly aligned with the PVS processes targeted by FPPE. In this context, the observed moderation by neighborhood disadvantage suggests that children exposed to greater disadvantage may have more pronounced PVS-related vulnerabilities, rendering them especially responsive to preventive interventions designed to enhance individual and dyadic positive affect and behaviors. Consistent with this interpretation, perceived stress, an outcome closely linked to PVS functioning, showed intervention-specific reductions only among children living in more disadvantaged neighborhoods. Prior work demonstrates that perceived stress predicts diminished reward responsiveness even when accounting for anxiety and general distress (Pizzagalli et al., 2007), supporting the notion that stress may serve as a proximal indicator of PVS dysregulation.
A complementary explanation is that neighborhood-level disadvantage may shape the conditions under which FPPE exerts its strongest effects. Families facing elevated contextual stressors often report fewer positive experiences and diminished opportunities for reinforcing parent-child interactions (Ayoub and Bachir, 2025), which may impede the development of adaptive reward-processing systems in children. By explicitly targeting individual and shared positive affect and behaviors (e.g., shared pleasant activities), FPPE may provide compensatory support for families with fewer environmental resources, thereby enhancing the salience and impact of positive parent-child interactions. From a neurodevelopmental perspective, neighborhood disadvantage may heighten children’s sensitivity to improvements in positive caregiving, such that increases in warmth, reinforcement, and engagement more strongly influence reward responsiveness and stress regulation among higher-risk youth (Gee and Cohodes, 2023; Whittle et al., 2017). Thus, FPPE may be particularly effective in disrupting maladaptive responses to stress in the contexts of elevated adversity, leading to more pronounced reductions in perceived stress symptoms. Together, these findings suggest that positive emotion-focused family preventive interventions like FPPE may yield proportionally greater benefits for stress reduction among children exposed to neighborhood disadvantage.
Notably, family-level socioeconomic disadvantage, indexed by INR, did not significantly moderate intervention outcomes. One possible explanation is that neighborhood-level indices capture broader contextual exposures that shape children’s daily experiences beyond household economic resources alone. While INR reflects financial resources within the family, neighborhood context encompasses features such as community instability, access to recreational and educational resources, exposure to environmental stressors (e.g., crime, environmental hazards, and limited access to safe recreational and educational resources), and opportunities for social support. These broader contextual factors may more directly influence children’s stress exposure and the availability of reinforcing experiences in their larger environments, both of which are closely linked to PVS functioning. Consistent with emerging work suggesting that family- and neighborhood-level socioeconomic disadvantage may differentially interact with reward-related processes in predicting youth depression risk (e.g., Roberts et al., 2025), neighborhood-level disadvantage may represent a more ecologically proximal indicator of the environmental conditions. These conditions may interact with FPPE’s focus on enhancing positive affect and parent–child reinforcement. In contrast, family income alone may be less sensitive to the social and environmental processes that shape children’s responsiveness to interventions targeting reward processing and stress regulation.
Contrary to our initial hypotheses, we found limited evidence that disadvantage moderated pre-to-post changes in clinical emotional symptoms (i.e., anger, anxiety, or depression) following FPPE. In contrast, neighborhood-level disadvantage moderated intervention-specific reductions in perceived stress, highlighting perceived stress as being a particularly sensitive outcome of a PVS-focused intervention. Notably, neighborhood disadvantage was not associated with higher perceived stress at baseline (r = −0.13, p = 0.285), suggesting potential differences in responsiveness based on neighborhood context rather than pre-existing vulnerability. From a developmental and mechanistic perspective, perceived stress may represent an earlier-emerging indicator of change in reward processing, whereas changes in clinical symptomatology may require more sustained intervention effects or longer follow-up periods to become detectable. Reductions in perceived stress are theorized to precede downstream improvements in clinical symptoms because stress reduction may alter underlying stress-related biological and affective processes, creating a context in which broader emotional and reward-related functioning can improve over time (Slavich and Irwin, 2014). Indeed, longitudinal clinical work has shown that early decreases in perceived stress during psychotherapy predict later reductions in anhedonia, while anhedonia does not predict stress change, suggesting that perceived stress change can temporally precede and potentially facilitate broader symptom improvement (Phillips et al., 2023). Thus, the present findings suggest that FPPE may exert its strongest short-term effects on perceived stress, with potential cascading benefits for clinical symptoms that may emerge over time as stress-related vulnerabilities are reduced, though this needs to be tested in future work. Importantly, because this is a preventative study, effects on clinical symptoms may be expected to emerge over longer time horizons, reflecting the goal of preventing symptom onset rather than reducing existing symptom.
There were some notable limitations that should be considered when interpreting these findings, while also pointing to important directions for future research. First, the modest sample size and limited range of child ages limited statistical power to detect smaller moderation effects, particularly for changes in child emotional symptoms. Reductions in perceived stress may emerge earlier following intervention, with downstream effects on broader psychopathology becoming more apparent in larger samples. Second, the generalizability of these findings is limited to mother–child dyads, as fathers and other caregivers were not included, underscoring the need for future work to test FPPE across more diverse family structures. Third, although family-level (i.e., INR) and neighborhood-level (i.e., COI) indices provide useful proxies for disadvantage, they do not capture the full range of stressors and contextual adversities that may influence intervention response. In addition, another limitation is that the study relied on parent-reported measures of child emotional functioning, which helped maintain consistency with prior work but limited the number of analyses that could be conducted. Although reliance on maternal report may introduce shared-method variance, recent large-scale psychometric evidence suggests that maternal psychopathology does not bias parental report of child emotional problems (Olino et al., 2021), indicating that observed associations likely reflect true child functioning. Nonetheless, future studies should incorporate multi-informant (e.g., child or teacher report) and observational measures of child emotional functioning to further reduce potential reporting biases. Future research should examine the durability of FPPE effects over longer follow-up periods. In addition, future work should explore neural and physiological mechanisms linking disadvantage, parenting processes, and child outcomes to inform precision prevention approaches for families at highest risk. Finally, although the fully remote format reduced barriers related to transportation and driving time, this may have introduced other access-related challenges, particularly for families with limited access to reliable internet, electronic devices, or private space for participation. Future work should consider hybrid or flexible delivery models to ensure accessibility for families across varying socioeconomic contexts.
Conclusions and Clinical Significance
In conclusion, the present study provides evidence that FPPE may be particularly effective in reducing perceived stress among children of mothers with elevated depressive symptoms, with the strongest benefits observed for youth residing in more disadvantaged neighborhoods. These findings highlight the role of neighborhood context in shaping children’s responsiveness to preventive intervention, suggesting that neighborhood disadvantage may confer heightened sensitivity to family-based approaches that target positive emotional processes. More broadly, these results underscore the value of integrating contextual and neurodevelopmental perspectives into prevention efforts and support the promise of precision approaches that leverage neighborhood-level risk to identify children most likely to benefit from PVS-focused family preventive interventions.
Authors’ Contributions
J.Y. and E.F.C.: Conceptualization, investigation, formal analysis, writing—original draft, reviewing and editing. M.G., C.F., K.R.P., G.M., and A.S.: Data curation, investigation, writing—review and editing. A.K. and K.L.B.: Conceptualization, investigation, formal analysis, reviewing and editing.
Footnotes
Data Availability Statement
Data will be available on request.
Acknowledgments
The authors would like to thank all our participants, their families, and the staff at both the Vanderbilt Mood, Emotion, Development (MED) Lab and the Penn State Families, Affective, Neuroscience, and Mood Disorders (FAM) Lab.
Author Disclosure Statement
This research was supported by a John and Polly Sparks Early Career Grant from the American Psychological Foundation to A.K., Peabody Small Grant from Vanderbilt University to A.K., and in part by ULL1 TR000445 from NCATS. Study funders were not involved in the trial design, implementation of the project, or analysis/interpretation of results. The authors have no conflicts of interests.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.