
Abstract
Background. The prevalence of
Methods. A sample of 81 students on a healthcare campus completed a 30-item survey assessing
Results. The results revealed no differences between
Conclusion. Findings suggest that healthcare trainees who play
Background
An overwhelming amount of evidence demonstrates long-term exposure to violent video games leads to aggressive cognition, affect, and behavior (e.g., Anderson et al., 2010; Calvert et al., 2017; Dowsett & Jackson, 2019; Gentile et al., 2014, 2016; Groves et al., 2019; Mathur & VanderWeele, 2019; Teng et al., 2019). According to prior literature, aggressive behavior is usually preceded by an individual's own aggressive cognition (i.e., the hostile attribution bias which in this context, suggests an individual with a high hostile attribution bias may be more likely to interpret a benign and innocuous action as hostile; Anderson et al., 2010; Calvert et al., 2017; Gentile et al., 2014), and aggressive affect (i.e., trait anger, frustration, and levels of empathy; Anderson et al., 2010; Bavelier et al., 2011; Calvert et al., 2017; Gentile et al., 2014; Lei et al., 2019). A review of the literature suggests the theoretical underpinnings of aggressive behavior, affect, and cognition, as well as empathy and benevolence stem from desensitization (Brockmyer, 2015; Coyne et al., 2018).
Desensitization theory suggests repeated exposure to a situation provoking mild to moderate anxiety automatically and unconsciously reduces an individual’s cognitive, emotional, and/or behavioral responses to a stimulus (Brockmyer, 2015; McMullen et al., 2017). Violent games may act as a stimulus for desensitization which refers to the absence of a response (Brockmyer, 2015). Subsequently, individuals engaged in violent gameplay are frequently exposed to video game gore (e.g., blood) and aggressive interactions (e.g., fighting or weapon use), whilst making split-second decisions in real-time virtual combat. Coyne and colleagues (2018) noted previous authors have argued active engagement in video games differentiates video game players from individuals who passively watch television (as cited in Bryant & Oliver, 2009). Although violent images and/or graphics may initially be distressing to an individual engaged in gameplay, an increase in frequency or the continued exposure of gameplay may have a systematic desensitization effect on the player (Brockmyer, 2015; McMullen et al., 2017).
The Entertainment Software Association (ESA) conducted a survey consisting of over 4,000 Americans and found 65% of American adults who responded play video games (ESA, 2019). Of those who responded, the ESA (2019) reported the three most popular game genres include casual (71%), action (53%), and shooter (47%). With a large amount of the American population engaged in action or shooter type gameplay, possible concerns pertaining to empathy may arise (e.g., Anderson et al., 2010; Bavelier et al., 2011; Calvert et al., 2017; Gentile et al., 2014; Lei et al., 2019). Concerns surrounding empathy in gamers are particularly important for healthcare providers participating in gaming as empathy influences treatment outcomes, patient satisfaction, rate of medical errors, patient and staff wellbeing, and trust (Hannan et al., 2019; Panagioti et al., 2018; Sterkenburg & Vacaru, 2018). Physician burnout, specifically, has been tied to decreased empathy and increased personal distress, which can be a result of by emotional exhaustion, low satisfaction, lack of achievement, and depersonalization (e.g., Sterkenburg & Vacaru, 2018; Tei et al., 2014; von Harscher et al., 2018). As such, reduced empathy as a result of violent video game play may affect factors related to physician burnout and patient care (Bogiatzaki et al., 2019).
In accordance with desensitization theory, healthcare providers and trainees who engaged in violent video game play may experience a decrease in empathy. Thus far, research has primarily evaluated the effects of violent video game play on the general population and no research was found evaluating the effects of violent video games on empathy in healthcare providers. The purpose of this study was to examine if empathy in graduate-level healthcare trainees is affected by violent video game play. Based on previous literature, the authors hypothesized that individuals who played violent video games would report lower levels of empathy as compared to those who play non-violent video games or do not play video games at all.
Methods
To evaluate the effect of violent video game play on empathy in healthcare trainees, a descriptive-comparative study design was employed using a convenience sample of healthcare profession graduate trainees who were recruited in person to complete an online survey assessing video game habits and empathy. Empathy was divided into three domains: Personal Distress (PD), Empathic Concern (EC), and Perspective-Taking (PT) based on the Interpersonal Reactivity Index’s (IRI) original indices (Davis, 1983).
Sample
A total of 130 participants were recruited face-to-face by students in the clinical psychology graduate program at a graduate-only medical school campus in an urban area located in the Southwest United States. Results of a power analysis with the desired power set at .80 indicated a goal sample size of 50 per group. The sample included healthcare trainees in the following industries: Biomedical Sciences, Cardiovascular Science, Clinical Psychology, Dentistry, Occupational Therapy, Optometry, Osteopathic Medicine, Pharmacy, Physical Therapy, Physician’s Assistant, Podiatry, Nurse Anesthesia, and Veterinary Medicine. Individuals were not asked to disclose their program or demographic information to protect identifying characteristics; however, students on campus wore mandated badges to indicate student status.
Instruments
Participants completed two instruments to indicate game preferences, frequency of play, and an assessment of empathy. Instruments included a modified version of the Video Game Questionnaire (Anderson & Dill, 2000) and Interpersonal Reactivity Index (IRI; Davis, 1980)). Upon completing these measures, participants were presented with a screen thanking them for their participation.
Video Game Questionnaire
The video game questionnaire was adapted from Anderson and Dill’s (2000) framework, which includes two composite indices measuring video game violence: exposure and time spent playing video games. Participants reported their five favorite video games and rated how often they play these games on a scale from 1 (I never play these games) to 5 (I play these games every day). The original questionnaire included a 7-point scale that assessed each participant’s game play frequency, ranging from rarely to often (α = 0.84). In addition, the original questionnaire included participant’s perception of how violent the gaming graphics or content was, ranging from little or no violent graphics/content to extremely violent graphics/content (α = 0.86; Anderson & Dill, 2000). In the current study, this was adapted so that each video game reported was coded using a 5-point scale to correspond with Entertainment Software Review Board (ESRB) ratings of the video games (ESRB, 2019). Participants were also given the option to disclose that they do not play video games at all, which coded as a 0 (see Figure 1).
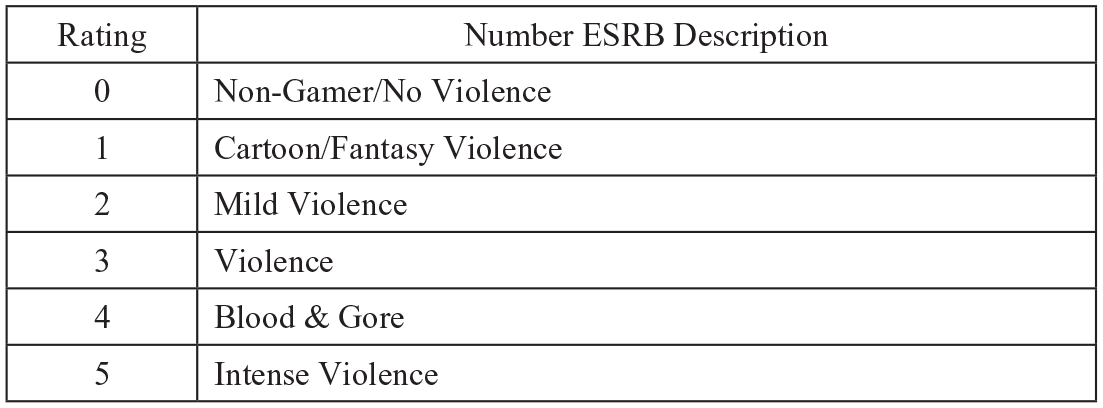
Violence rating numbers for individual games reported from participants based on the Entertainment Software Rating Board (ESRB) violence descriptors.
Interpersonal Reactivity Index
Participants also completed the 28-item Interpersonal Reactivity Index (IRI), which incorporates four scales of empathy including Perspective Taking (PT, α =.78-.75), Fantasy (FS, α = .78-.75), Empathic Concern (EC, α =.72-.70), and Personal Distress (PD, α =.78; Davis, 1980). Each question was rated using a 5-point Likert scale from 1 (Does not describe me well) to 5 (Describes me very well; Davis, 1980). The PT scale measures an individual’s ability to adopt another individual’s point of view (Davis, 1983). EC refers to an individual’s sympathy and concern towards another’s circumstances, while PD assesses an individual’s personal feelings of anxiety and discomfort when placed in tense or urgent settings (Batson & Shaw, 1991; Davis, 1983; Eisenberg & Eggum, 2009). For the purpose of the present study, the Fantasy (FS) scale, a measure of one’s ability to imagine themselves as fictitious characters in books, television, or plays, was removed due to the context of the questions and nature of the present study.
Research Protocol
The present study was approved by our own institution’s Institutional Review Board. Participants were recruited in-person in the common areas of a graduate-only medical school campus. Participants were handed a flier with a brief description of our study’s purpose, inclusion criteria, and a link to the survey (through SurveyMonkey). They were given a verbal overview of the study (i.e., the purpose and expectations), and informed that participation was voluntary. In an attempt to avoid selection bias, the flier included a statement indicating an individual did not have to play video games to participate. If preferred, participants were able to provide their email address on the flier provided to have the survey link sent directly. Before beginning the survey, participants agreed to a written informed consent presented at the beginning of the survey. The informed consent was emailed upon request. Participants did not provide any identifying information including program type and demographic characteristics. All participant email addresses were stored in a locked cabinet and destroyed upon the study’s conclusion. During the study, data was stored on a locked computer within a locked facility on the university campus.
Individual participants were sorted into one of three groups based off the level of violence depicted in their top 5 favorite video games and game play frequency. Ratings for violent content ranged from 1 (Cartoon/Fantasy Violence) to 5 (Intense Violence) and were based on the Entertainment Software Rating Board (ESRB) descriptors of violence (ESRB, 2019, see Figure 1). A rating of 0 was used to indicate no violent video game content (e.g., Solitaire) or non-gamers. Both non-gamers and those who play games with no violent content were given a code of 0.
Of the complete sample, 50% of individuals reported playing video games with high levels of violence, 15% reported playing games with mild to moderate violence, and 35% indicated playing video games with little to no violent content. Participants also responded to the frequency of their gameplay. 11% of the sample rated playing video games weekly or daily, 61% played approximately between two weeks and one month, while 28% indicated playing less than once per month.
Group 1 (n = 48) consisted of individuals who played violent video games (rating scores of 3 [Violence] to 5 [Intense Violence]) at least “rarely.” Group 2 (n = 14) was comprised of those who played games with mild to moderate violence (rating scores of 1 [Cartoon Violence] to 2 [Mild Violence]). Group 3 (n = 33) was made up of individuals who reported never playing video games or those who having had played video games in the past, but never play them currently (i.e, frequency rating at a 1). Each participant was sorted one of the three groups based off the level of violence depicted in their top 5 favorite video games and game play frequency. The process of group division is further explained in Figure 2.
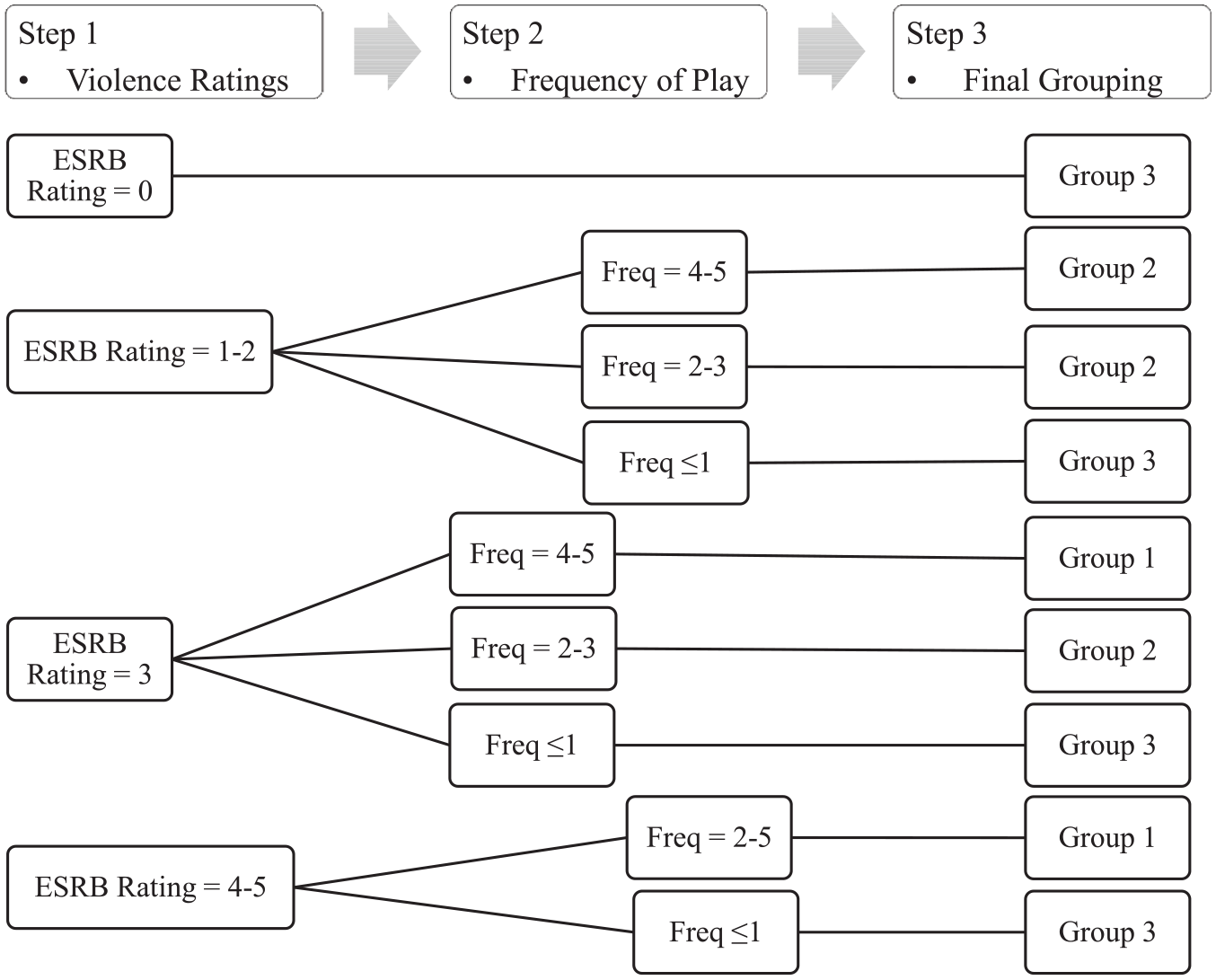
Process of group division.
After groups were divided, participants who rated mild to moderate violence (n = 14) were excluded from the final analysis as the study aim was to compare empathy levels between violent video game players and non-violent gamers/non-gamers. Therefore, a total of 81 participants were used to compare the effects of violent video game play on empathy levels in perspective healthcare providers. The Perspective-Taking, Empathic Concern, and Personal Distress scales from the IRI were totaled according to the scoring guidelines (Davis, 1980).
Statistical Analysis
The purpose of our study was to determine if the mean scores on ratings of empathy as measured by the Perspective-Taking, Empathic Concern, and Personal Distress scales on the IRI, differ based on whether a healthcare trainee engages in frequent violent video game play. A one-way multivariate analysis of variance (MANOVA) was run on SPSS software. A Tukey’s HSD post-hoc test was used to further examine between-subjects’ effects and to reduce the possibility of a Type II error (Chen et al., 2018).
Results
A total of 130 participants were recruited face-to-face on a medical school campus in an urban area located in the Southwest United States. Of the 130 original participants, 35 participants were removed due to fixed or incomplete responding, leaving 95 participants to be grouped for analysis.
Pearson’s R correlations were run to determine the relationship between game content and frequency of game play. Findings indicated video game violence ratings were positively correlated with frequency of play (r = .747, n = 95, p < 0.01), suggesting those who play violent video games tend to play video games more often.
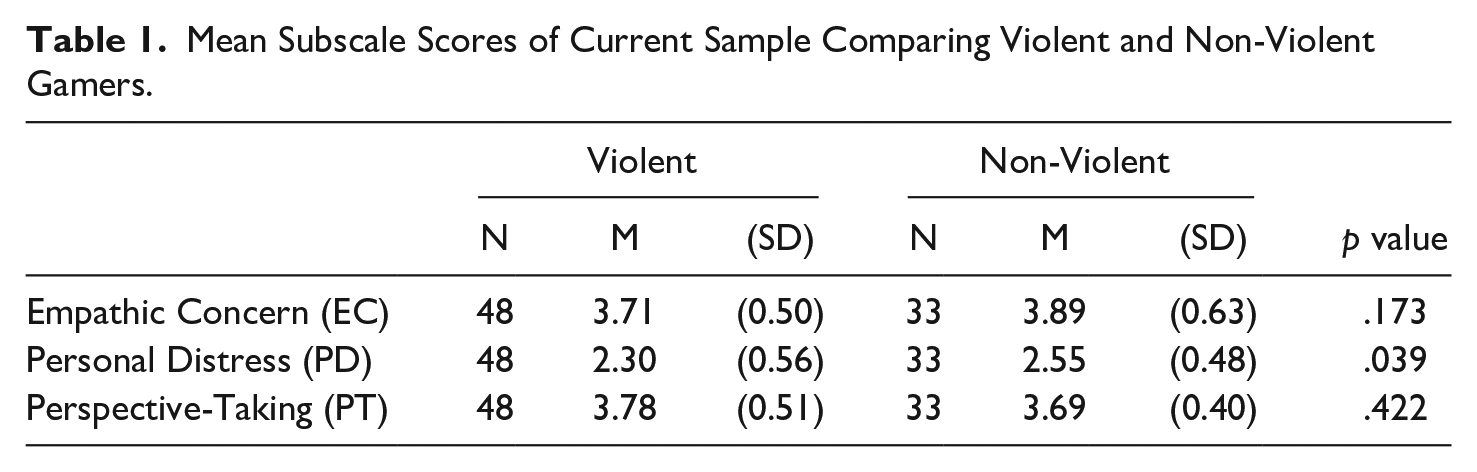
The results from the MANOVA are consistent with the null hypothesis (see Table 1), suggesting individuals frequently exposed to violent video games rated a similar level of Perspective-Taking, Personal Distress, and Empathic Concern, as compared to individuals who are not exposed to violent video games (F(3, 77) = 2.56, p > .05, Wilk’s Λ = 0.91). However, a Tukey’s HSD post-hoc test indicated a statistically significant difference between groups on Personal Distress (F(1, 79) = 4.42, p = .039). These findings suggest healthcare trainees engaged in violent video game play experienced significantly lower levels of Personal Distress.
Mean Subscale Scores of Current Sample Comparing Violent and Non-Violent Gamers.
Discussion
Results of this study suggest graduate-level healthcare trainees playing violent video games have similar levels of Empathic Concern and Perspective-Taking compared to those who do not play violent video games. More specifically, violent video game play does not appear to be related to Empathic Concern or Perspective-Taking and therefore, no notable differences in empathic patient care should be observed based on healthcare trainees’ video game habits.
However, post-hoc analyses revealed individuals who engaged in violent video game play were more likely to have lower levels of Personal Distress. This particular finding is consistent with desensitization theory because it suggests that individuals who engage in frequent violent video game play experience less Personal Distress when exposed to other’s discomfort, whereas non-gamers may experience a higher level of Personal Distress when exposed to another’s discomfort.
No prior literature has examined the effect of violent video game play on healthcare trainees, yet research has found increased stress is significantly related to depression in medical interns (Mata et al., 2016) and burnout in healthcare professionals (Montero-Marin et al., 2016). Similarly, in a sample of graduate level healthcare trainees, von Harscher and colleagues (2018) found higher levels of Personal Distress increased risk for burnout, which was measured by three dimensions (emotional exhaustion, depersonalization, and personal accomplishment). Specifically, increased emotional exhaustion and depersonalization with reduced personal accomplishment were indicated in trainees with high Personal Distress. In contrast, Empathic Concern was protective against burnout with lower levels of emotional exhaustion and depersonalization; and gave trainees a heightened sense of personal accomplishment. Taken together, these results suggest trainees with low Empathic Concern and high Personal Distress may be at higher risk for burnout (von Harscher et al., 2018).
Results from the present study indicate a reduction of Personal Distress in violent video game players as compared to non-violent players, suggesting engagement in violent game play may build tolerance and resiliency against stressors. These findings are corroborated by a study that evaluated whether a video game could improve empathy in 212 care providers who work with individuals with disabilities (Sterkenburg & Vacaru, 2018). Findings demonstrated small and non-significant improvements in empathy, and a significant decrease in Personal Distress. In addition, Personal Distress was shown to predict the increase in empathy (Sterkenburg & Vacaru, 2018).
Decreased Personal Distress has also been demonstrated to be adaptive in physicians when performing painful procedures as they may be better able to modulate their anxiety, which in turn may enhance their ability to focus and provide care to their patients (Cheng et al., 2007; Nielsen & Tulinius, 2009; Sterkenburg & Vacaru, 2018). For example, physicians displayed lower Personal Distress in the neural regions associated with emotional regulation in a functional magnetic resonance imaging (fMRI) when observing acupuncture videos as compared to a sample from the general population (Cheng et al., 2007). Seasoned physicians or healthcare workers exposed to frequent, highly distressing, emergent situations require higher tolerance to Personal Distress to successfully perform their daily responsibilities.
Arguably, this study suggests healthcare trainees who engage in violent video game play may be beneficial as they progress into their clinical career due to a lower level of Personal Distress. Decreased Personal Distress from violent video games again can be attributed to desensitization theory which poses repeated exposure to high stress video game environments reduces an individual’s perceived stress (Brockmyer, 2015). Theoretically, the fast-paced environments within a video game context may also be beneficial to healthcare trainees in emergency situations, because they are less likely to experience anxiety related to another’s distress or pain, which can positively influence judgement and decision-making (Wemm & Wulfert, 2017).
Improved decision-making and judgement coupled with reductions in stress, anxiety, and distress may aid providers in emergency scenarios by allowing them to focus on making accurate diagnoses and treatment plans, but also reduce outstanding anxiety and rate of errors (Hannan et al., 2019; Panagioti et al., 2018). With less errors, healthcare trainees may experience less emotional exhaustion and greater personal accomplishment. Therefore, it seems possible that regular exposure to high pressure violent video games could potentially improve a healthcare trainee’s future ability to modulate their emotional response to emergency or distressing medical situations, which may lead to improved medical care and therefore act as a protective factor for burnout as they become licensed, professional, healthcare providers (Nielsen & Tulinius, 2009; Thomas, 2013).
Limitations and Suggestions for Future Research
Results of this study are limited by the small sample size and sample population, which only included trainees enrolled in a healthcare-based graduate school program located in the Southwest United States; a lack of demographic variable collection; the examination of a single source of viewing violence (e.g., video games); unmonitored participants during response submissions; and a lack of validity and reliability scales included in the executive functioning measure. Additionally, we did not collect data assessing the reliability and validity of the Video Game Questionnaire modifications for this study. All identified fixed, random, or incomplete responses were reviewed and removed from the data. Due to the incomplete responding, the final sample size was below the goal of 50 per group. Future research should recruit a larger sample to ensure adequate power. It is also important to note the included self-report measures may not accurately reflect how empathy is reflected in patient care and professional development. Further, data is subject to selection bias, in that trainees who play video games may have been more inclined to participate in the study.
Follow-up research is necessary to determine if video game play affects healthcare trainee’s and professional provider’s empathy, error rate, and Personal Distress, along with patient satisfaction to obtain further information on whether regular exposure to high pressure, violent video games influence provider care, perceived Personal Distress, and patient care. Gender differences should also be considered within the healthcare population sample, as literature suggested males are more likely to play violent video games, as compared to females (Coyne et al., 2018; Read et al., 2016). Subsequently, females are more likely to display higher levels of empathy and prosocial behavior (Coyne et al., 2018). Studies should further assess participants viewing of violent television shows and movies to determine if there is a difference between engaging in virtual violence and passive viewing of violence in individuals in the healthcare field. Moreover, studies have been limited in evaluating how video game play affects healthcare providers across disciplines. Future research should address these limitations by collecting data from a larger number of students and ensuring that demographic data is collected in addition to video game habits and levels of empathy.
Conclusion
Our current study suggests healthcare trainees who play violent video games experience a similar level of Empathic Concern and Perspective-Taking as those who do not play violent video games but do demonstrate a reduction in their overall Personal Distress. Previous literature assessing the relationship between empathy and Personal Distress as it relates to physician burnout has indicated mixed results. However, high Personal Distress was identified as a risk-factor for burnout in graduate students (von Harscher et al., 2018) while other studies suggest low levels of Personal Distress are adaptive for healthcare providers (Cheng et al., 2007; Nielson & Tulinius, 2009; Sterkenburg & Vacaru, 2018). In the present study, Empathic Concern was comparable across both groups, while Personal Distress was lower in individuals who played violent video games. Though we cannot infer directionality in this relationship, this study adds preliminary findings to the desensitization theory framework in a new population. In addition, findings inform future research on the potential effects of video game violence exposure on healthcare trainees’ empathy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.