Abstract
Background
Management of in-hospital cardiac arrest includes many component skills that require considerable training in order to gain mastery. Practicing defibrillation skills in a simulated setting improves performance and time to shock delivery but is cumbersome and costly. Virtual reality (VR) simulation training may provide an alternative platform to help medical students learn and build confidence in the critical steps required to operate a manual defibrillator.
Intervention
We performed a pilot study to implement a VR simulation that trains learners on the stepwise operation of a manual defibrillator.
Methods
We conducted a cross-sectional survey that measured the feasibility, usability, and likeability of a VR simulation among fourth-year medical students at a large urban academic medical center. Secondary outcomes included self-efficacy with operating a defibrillator before and after the VR simulation, and time to defibrillation within the simulation.
Results
Twenty-six participants completed the VR simulation. The majority of participants found the VR simulation easy to use (71% agreed), liked the experience (96% agreed), found it realistic (87.5% agreed), and would recommend it to their peers (96% agreed). Most students (96%) agreed that the training improved their knowledge of how to use a defibrillator, and all (100%) students agreed that they were more confident than beforehand in using the defibrillator to defibrillate a patient with cardiac arrest. Self-reported knowledge and comfort with using the defibrillator significantly improved from before to after the VR training, as did average time to defibrillation.
Discussion
VR simulation for defibrillator training is feasible and well-liked by senior medical students and is associated with improved self-perceived knowledge and comfort with using a manual defibrillator.
Keywords
Background
In-hospital cardiac arrest is a common cause of morbidity and mortality impacting 9.7 per 1000 hospitalizations in the United States from 2008-2017 with poor survival outcomes (23.8%). (Holmberg et al., 2019; Chan et al., 2016; Larsen et al., 1993) The prompt identification of shockable rhythms and subsequent defibrillation can maximize odds of survival with a favorable neurologic outcome. (Chan et al., 2016) Deviation from the standards in Advanced Cardiac Life Support (ACLS) protocols reduces the patient’s chances of return of spontaneous circulation and survival to discharge. (Crowley et al., 2020) Unfortunately, despite regular mandated training and certification, trainees in a wide range of disciplines have reported low confidence in resuscitation management. (Barley, 2021; Lo et al., 2011; van Schaik et al., 2008).
Prior studies have demonstrated that practicing defibrillation skills in a simulated setting directly translates to an improvement in time to shock delivery during actual resuscitations. (Ericsson, 2004; Jeffers et al., 2016) Randomized controlled trials have shown that healthcare professionals trained on a defibrillator simulator demonstrated a statistically significant reduction in time to first shock delivery compared to those who did not receive simulation training. (Lemke et al., 2021) A comprehensive analysis of multiple studies investigating simulated defibrillator training consistently demonstrates improved time-to-shock delivery, emphasizing the effectiveness of simulated practice for developing defibrillation proficiency. (Yeung et al., 2011) These findings emphasize the importance of repetitive, high-fidelity simulation training to enhance clinical performance.
However, manikin-based simulation can be costly and requires significant human resources to operationalize. (Alaker et al., 2016; Nanji & Cooper, 2012; Sujatta, 2015) Opportunities for repeated practice to meet individual learning needs are further limited by time, equipment availability, or physical space constraints.
Virtual reality (VR) encompasses digitally-generated simulated environments experienced through head-mounted ocular displays or specially designed physical rooms (VR rooms/chambers) with advanced motion tracking and spatial mapping, allowing users to be fully immersed, physically interact, and explore the virtual world. (Sherman & Craig, 2018) These environments, when used for training, can offer an immersive experience with unique advantages that complement other immersive learning strategies such as manikin-based simulation. (Kuyt et al., 2021) VR can be conducted in solitude offering a psychologically safe space to practice, can hypothetically include unlimited simultaneous learners, and is optimal for simulating complex or large-scale scenarios that are less practical or even unfeasible in person (e.g., mass casualty events or operating room fires). (Jung, 2022) VR also has the potential to integrate and automate standard proficiency assessments, incorporate objective biophysiological feedback, and be programmed for an adaptive learning experience tailored to individual learners. (Plotzky et al., 2021; Chan et al., 2021) The concept of deliberate practice has been defined by Ericsson as “individualized training activities specially designed by a coach or teacher to improve specific aspects of an individual’s performance through repetition and successive refinement.” (Ericsson & Lehmann, 1996) One important aspect of deliberative practice in medicine is to define specific component tasks that can be refined, evaluated, improved and applied to patient care. VR technology allows repetitive practice in specific skills, with elements of immediate feedback during and after each training session. Therefore, VR can be a valuable, low-stakes component of deliberate practice by enabling individuals to repetitively and purposefully engage in skill training that is interspersed with other educational modalities as well as real-world experience. (Ericsson, 2004; Ericsson & Lehmann, 1996; Rodríguez-Matesanz et al., 2022; Semeraro et al., 2019)
Several studies have explored the successful use of VR in training high-quality cardiopulmonary resuscitation (CPR) and in adhering to ACLS algorithms, however, there remains an unmet need for step-by-step training in the critical actions needed to set-up and operate a manual defibrillator in VR. (Katz et al., 2020; Leary et al., 2019; Nas et al., 2022) Previous studies investigating VR training for CPR have primarily focused on broader CPR skills rather than specifically addressing the intricacies of defibrillator operation. While these studies have demonstrated the potential of VR training to enhance overall CPR performance, they have not fully addressed the specific needs and challenges associated with defibrillator usage.
This study aims to address this unmet need by evaluating a newly developed, immersive VR training experience targeting the essential steps involved in setting up and operating a manual defibrillator. The aim of this pilot study was to assess the feasibility, usability, and likability of a VR simulation as a learning tool for fourth-year medical students, specifically focusing on their ability to effectively set up and utilize the defibrillator during resuscitations. By focusing on the unique aspects and complexities of defibrillator usage within a virtual environment, this study intends to fill the gap in the existing literature and contribute to the development of more specialized and tailored training programs for healthcare professionals.
Methods
Study Design and Population
The study was pre-emptively approved by the Columbia University Institutional Review Board with written informed consent obtained from all participants. (Protocol #AAAT5978) In this mixed-methods pilot study, fourth-year medical students at a large urban academic medical center in New York City, USA were surveyed on their attitudes before and after experiencing a headset VR simulation on manual defibrillator operation. All fourth-year students participating in a month-long residency preparation course in the final quarter of the year were eligible for inclusion and recruited via a standardized email invitation. Since this study represents a feasibility pilot, no sample size estimation was performed. A convenience pilot sample of 26 participants was enrolled from an existing medical school course cohort with the aim of establishing a point estimate and confidence interval to inform the design and powering of future studies. Participants were informed, consented, and acknowledged the potential risks associated with the use of VR headsets, encompassing nausea, vertigo, and headaches triggered by visual effects.
Intervention
VR Development, Environment, and Training
A fully functional virtual replica of the Zoll R-series defibrillator (Chelmsford, MA) was created to use in a training simulation deployed on the Meta Quest 2 (Menlo Park, CA) using hand-tracking features. The VR simulation was written using Unity (Unity Technologies, San Francisco, CA) and deployed on the Meta Quest 2 in the fall of 2020 by a team of students and faculty from the Columbia Departments of Computer Science, Emergency Medicine, and Anesthesiology.
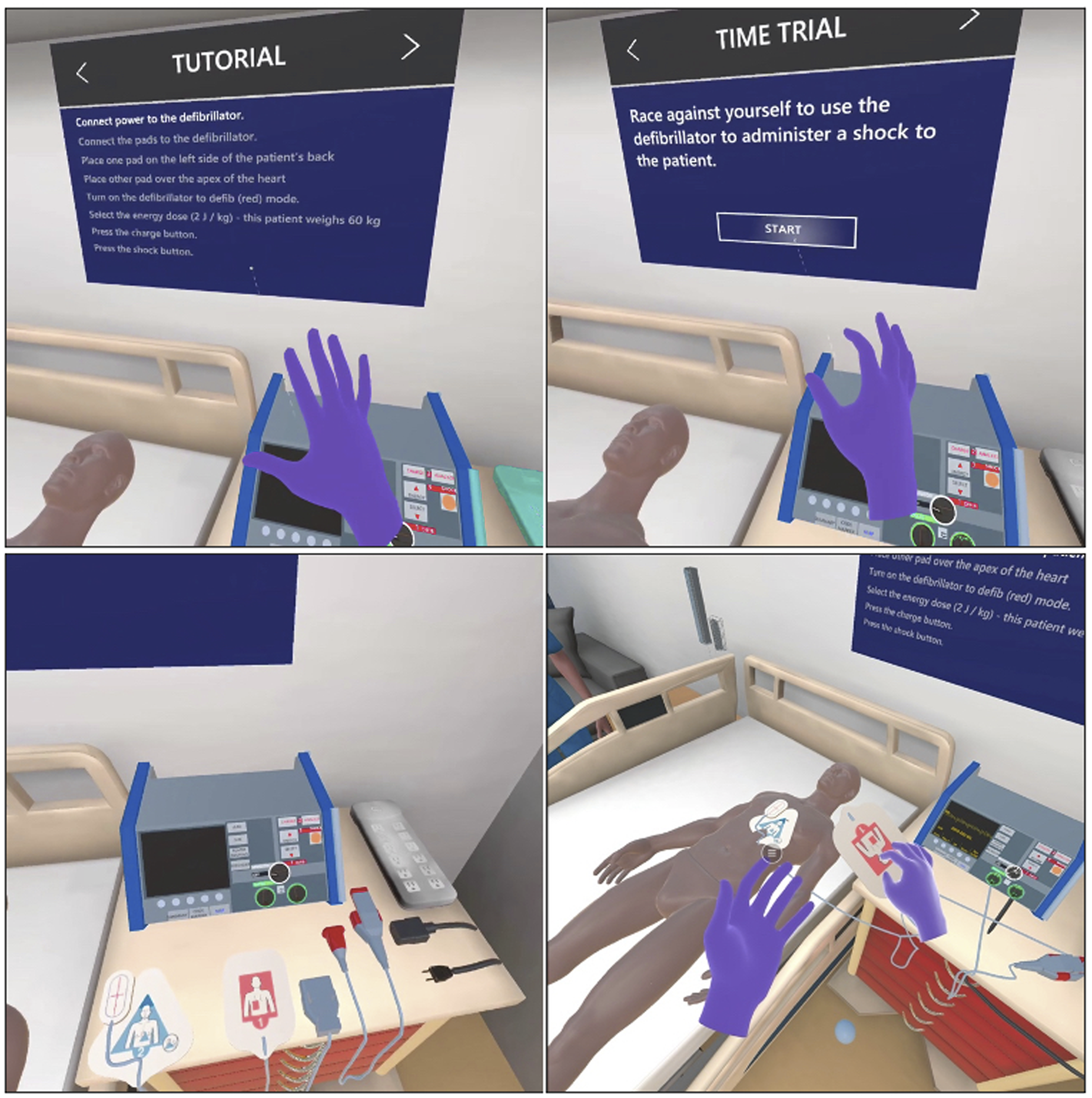
The VR simulation trains clinicians in operating a manual defibrillator Figure Appendix 1. In the virtual training environment, users begin at the patient's bedside in a hospital room with a nearby defibrillator on a code cart (standard equipment found in hospitals that house essential medical supplies and equipment for medical emergencies). The simulation guides the user through each step in setting up and operating the defibrillator, including plugging in components, using buttons and knobs, applying defibrillator pads correctly, and delivering a shock. The system provides a tutorial mode that guides participants through a well-defined sequence of actions as well as a timed mode for independent completion, functioning as a task that is repeatable until the participant successfully completes the exercise. (Appendix 1).
The VR simulation was conducted in an empty 5-meter by 5-meter room free of obstacles (see Appendix 3) with a study investigator present to address questions about operating the VR equipment or assist with technical difficulties. After reviewing the general study instructions, participants donned the headsets. They first completed Tutorial Mode, which guided the user on how to operate the defibrillator, correctly apply the pads, and select the appropriate amplitude of joules by sequentially highlighting each piece of equipment until the user engaged with it. To facilitate the process, the virtual room included a task board listing essential steps, where the highlighted items guide the user through each subsequent action. In instances where participants required technical assistance specifically related to the headset, such as troubleshooting or resolving technical issues, the study investigator provided necessary support during Tutorial Mode to facilitate the correct completion of each step by the student. It is important to note that this assistance focused solely on addressing technical aspects and did not involve teaching or providing instructional guidance.
Following Tutorial Mode, participants were instructed to proceed to Timed Mode, where no visual or verbal prompts were provided. Instead, participants were tasked with completing all steps in the correct order, while their progress was timed until the shock was delivered to the patient. During this mode, participants were able to view their time to shock directly within the VR environment. They were also specifically asked to record their own time as displayed by the VR system. The investigator guided participants to complete Timed Mode at least twice, with the goal of improving their score, while keeping track of both their initial attempt's duration and their fastest completion time.
Study Procedures
First, participants completed an online pre-study survey that collected demographic information and past training experience. This encompassed age, gender identity, recent American Heart Association (AHA) certifications (such as Basic Life Support and ACLS) held in the last five years, level of experience with video games and VR, experience, knowledge and comfort using manual-based defibrillators in simulated and clinical settings, experience, knowledge and comfort managing cardiac arrest in simulated and clinical settings, and susceptibility to motion sickness.
Next, participants were introduced to the VR hardware and software by reviewing instructions that were embedded in the online survey on how to wear and adjust the fit of the headset for comfort and how to navigate in the virtual environment (see Appendix 2). Participants then completed the VR activity as described above Figure Appendix 3.
Finally, participants completed an online post-study survey. Participants were asked to rate the usability and likability of the VR simulation, self-assess their knowledge and comfort relating to using the defibrillator and management of cardiac arrest, provide comments on what they liked best and what they would change about the experience, and report any side effects from using the headset along with a rating of the symptom severity. No formal feedback or instructor-led debriefing occurred, except for the features already automated and integrated into the experience.
Data Collection Tools
All survey instruments (including demographic data) were administered through the online survey platform, Qualtrics (Seattle, WA). To obtain information about the usability, likability, and perceived impact on knowledge and confidence, a survey was designed to elicit user experiences comprised of 6-point Likert style questions with answers ranging from “strongly disagree” to “strongly agree”. In addition, participants were asked two open-ended questions about what they liked best and what they would change about the VR simulation. The survey instruments were designed for this specific project and did not have previous evidence for validity or reliability tested.
Exploratory efficacy outcomes were collected to evaluate for point estimates and effect sizes on trainee improvement in self-assessed knowledge, self-assessed comfort, task performance within the simulation, and self-reported time to shock delivery in the VR simulation.
Potential harm to participants was evaluated by assessing frequency and severity of side effects reported after using the VR headset. Before the simulation, participants reported their propensity to motion sickness on a 10-point scale from “not at all” to “very prone”. After the simulation, participants were asked to report physical symptoms from using the headset as measured on a 5-point scale from “not at all” to “very much”. Finally, baseline propensity to motion sickness was compared to reported severity of physical symptoms from using the headset.
The data obtained from open-ended questions was presented without conducting additional analysis, with the intention of utilizing it for future iterative improvement of the VR training experience as a whole. The comments were compiled and presented in their original form, without any categorization or interpretation, to maintain the integrity of the user's feedback.
Statistical Plan
Descriptive analyses were performed; for categorical variables, frequencies and proportions were reported, mean values and standard deviations were reported for continuous data with comparisons made using the paired t-test, and median values and interquartile ranges were reported for ordinal data with comparisons made using the Wilcoxon signed-rank test. Spearman’s rank correlation was used to evaluate relationships between ordinal data. P values ≤0.05 were considered significant. Statistics were performed with Stata/SE 15.1 for Mac, (StataCorp LLC, College Station, TX). Open ended survey questions were reported in full as appendix materials.
Results
Participant Characteristics
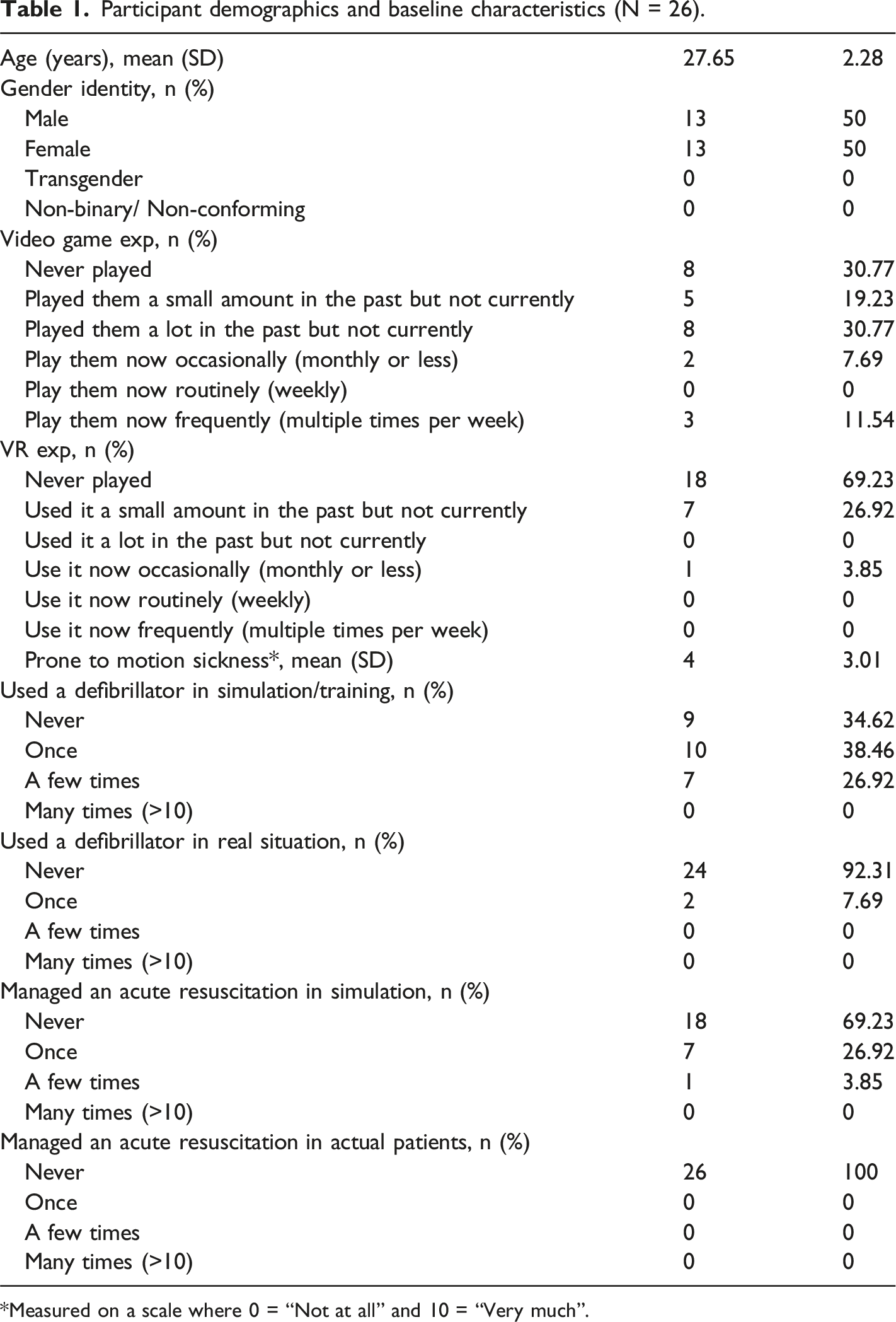
Twenty-six fourth-year medical students completed the VR simulation (see Figure 1). All participants were AHA certified in basic life support within the past four years, and none were ACLS certified. Eighteen participants (69%) had no prior VR experience. On average, baseline propensity to motion sickness was rated as a 4 out of 10. Only two participants (8%) had experience using a defibrillator in an actual resuscitation, while seventeen participants (65%) had used a defibrillator in a simulated setting (see Table 1). Out of the 26 students who participated in the training, two students did not complete the feasibility, usability and likability survey and three students did not complete the motion sickness survey nor the pre and post test surveys, resulting in a sample size of 23 for all componenets of the survey analysis. Study flow. Participant demographics and baseline characteristics (N = 26). *Measured on a scale where 0 = “Not at all” and 10 = “Very much”.
Feasibility, Usability, and Likability of the VR Simulation
Usability and Likability of the Virtual Reality Simulation (N=24).
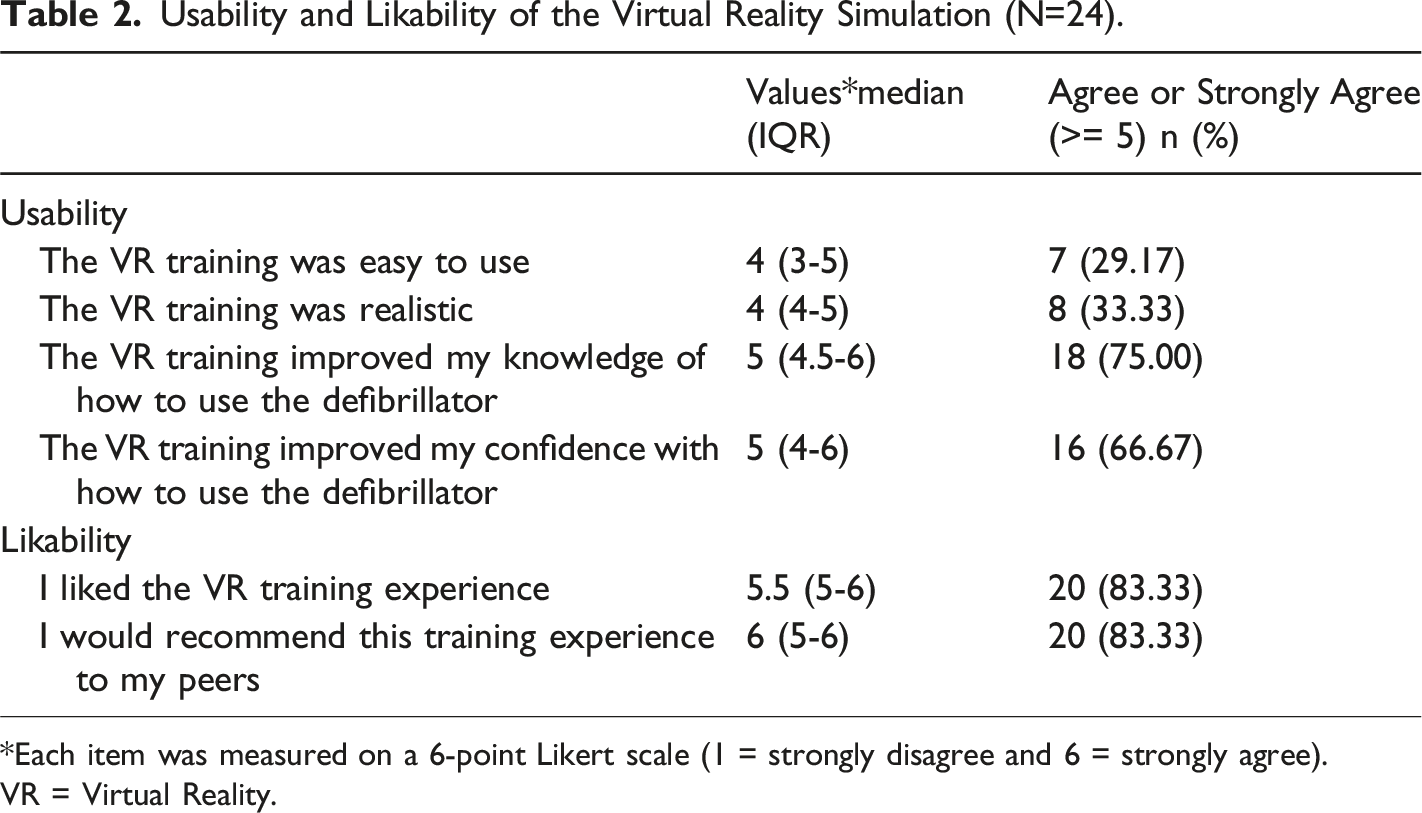
*Each item was measured on a 6-point Likert scale (1 = strongly disagree and 6 = strongly agree).
VR = Virtual Reality.
Motion Sickness
Self-reported Symptoms Immediately Following the VR Simulation (N=23).
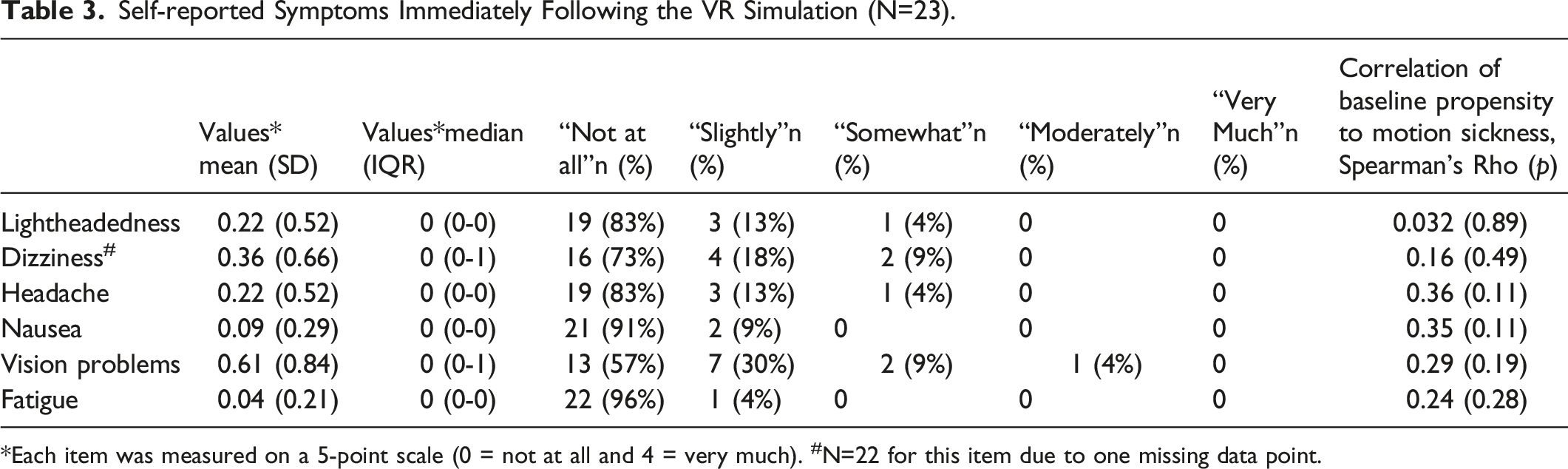
*Each item was measured on a 5-point scale (0 = not at all and 4 = very much). #N=22 for this item due to one missing data point.
Trainee Knowledge and Task Performance
There was a significant increase in self-reported trainee knowledge and task performance from pre- to post-VR simulation (see Figure 2). The greatest increase was in the proportion of participants who felt comfortable using a defibrillator in a cardiac arrest, which increased by 56% (from 40% to 96%). Overall, there was a 24% increase (from 76% to 100%) in the proportion of participants who felt comfortable that they knew how to use the defibrillator to defibrillate a patient with cardiac arrest after using the VR simulation. There was a significant improvement in the self-reported time to defibrillation within the VR simulation from first attempt (mean = 106.6 seconds, SD = 44.1) to the final or best attempt (mean = 67.1 seconds, SD = 33.6) by 38.9 seconds (p<0.01). After training, 76% of participants achieved a time to first shock below the American Heart Association recommended time of 90 seconds. Comparison of trainee knowledge and task performance before and after using VR simulation. Note: Each item was measured on a 6-point Likert scale (1 = strongly disagree and 6 = strongly agree). P values for each question item are listed; all pre-post study comparisons were significant (p<0.05). The question stems were: 1. I know how to turn on a hospital defibrillator. 2. I know how to connect the defibrillator pads to the patient. 3. I know how to connect the defibrillator pads to the defibrillator machine. 4. I know how to select the correct mode. 5. I know how to set the defibrillator to analyze the patient’s rhythm. 6. I know how to use a defibrillator to defibrillate a patient with cardiac arrest. 7. I feel comfortable using a defibrillator in a cardiac arrest. 8. I feel comfortable managing cardiac arrest.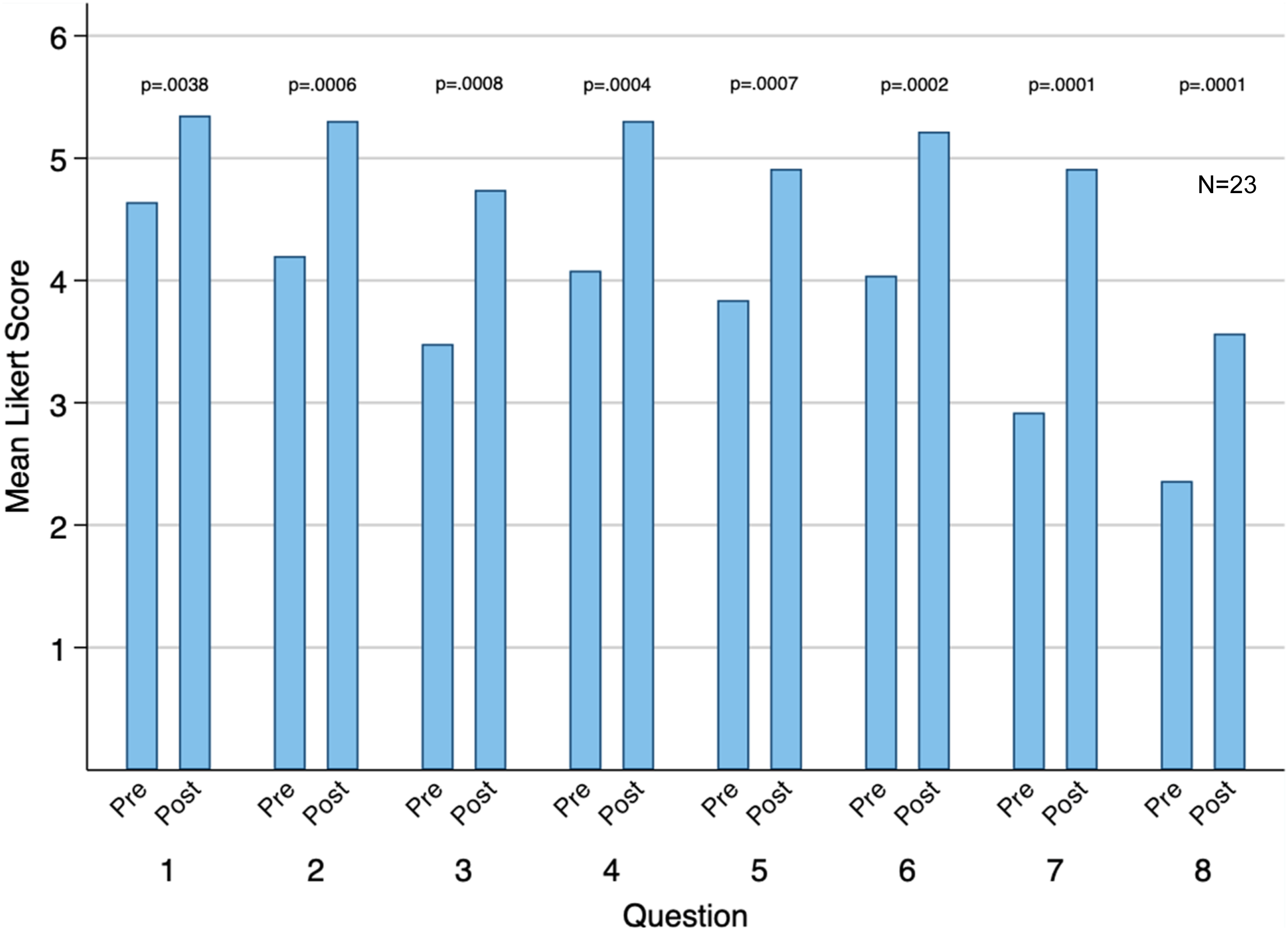
Selected Comments
Participants also described what they liked best and what they would change about the VR simulation. Participants wrote that they found the VR simulation to be novel and fun, the instructions on operating the defibrillator to be comprehensive, and the VR simulation to be realistic and immersive. They also commented on the low-stakes learning environment and the benefit of being able to repeat the simulation multiple times. Participants suggested the simulation could be improved by including more enhanced features, refining the controls and perceived glitches, and including additional instructions on how to initially navigate in a virtual environment. See Table Appendix 4 for all participant comments.
Discussion
Overall, the VR simulation was found to be feasible, usable, and well-liked by medical students, leading to improved self-perceived knowledge and comfort with using a manual defibrillator in a cardiac arrest. Participants had positive attitudes toward using VR in medical education despite very few having prior experience with the platform. Participants who used the VR simulation exhibited increased comfort and confidence in performing the critical action steps to execute successful defibrillation during a cardiac arrest in VR. This study demonstrated how technical skills and correct application of defibrillation can be successfully incorporated into a VR simulation case.
Past studies have shown that VR training improves performance in medical procedures by reducing errors and increasing speed to completion. (Gallagher et al., 2001; Gomoll et al., 2008) VR can improve performance in cardiopulmonary arrest and is comparable to manikin-based training, including adherence to protocols. (Nas et al., 2020; Siebert et al., 2017) The current study builds upon this knowledge by specifically focusing on VR simulation for the psychomotor practice of operating a manual defibrillator. While the current study did not involve direct patient outcome metrics, the surrogate measure of time to defibrillation was shown to decrease from before to after VR training. Use of a manual defibrillator is a component task in the broader context of CPR and requires specific psychomotor skills and practice. Use of a low-stakes VR training modality with repetitive practice and elements of immediate feedback may enable participants to develop and refine the psychomotor skills necessary for operating a defibrillator with precision and efficiency. This may in turn enhance overall resuscitation quality. (Wurmb et al., 2015).
VR integration into medical education offers the potential to enhance individual learning without requiring extensive physical resources. In our study, participants underwent equipment familiarization and engaged in multiple attempts of VR training, while requiring minimal time commitment and supervision. Consistent with previous reports, participants expressed a high level of interest in utilizing VR for medical simulation. (Setlur et al., 2022) Participants demonstrated improvements in self-perceived knowledge, comfort, and skills related to the practice of a high acuity, low-frequency procedure. The VR training was designed to facilitate repeated practice with gradually escalating difficulty from tutorial to timed mode and offered personalized feedback to assist participants in enhancing their skills in defibrillator use. This type of training could be incorporated as a component of a broader curriculum on cardiopulmonary arrest management in a wide range of medical disciplines and can help to facilitate deliberate practice.
The high level of fidelity of VR platforms like the one studied here provides an immersive and realistic experience that fosters engagement by enabling practical application and practice of technical skills. The clear task-oriented nature of VR simulation with focused content assists users in developing targeted competencies. In situations where real-world practice opportunities may be limited, VR offers an easily accessible and cost-effective means of employing spaced repetition to maintain skills and knowledge. This is particularly pertinent with ACLS and defibrillator use, as evidence indicates that knowledge of these skills tends to deteriorate over a period of 3-6 months, which can impact patient survival. (Smith et al., 2008).
Limitations
This study had several limitations. Firstly, as a small single-center convenience sample, the generalizability of our conclusions is limited. The study was not powered for inferential statistics or within-group comparisons such as the effect of past certifications on the acceptability of VR for training. All of the instruments used in this study to measure participant feedback on the experience were developed for this study and therefore lack prior validation or reliability data. Furthermore, data measures were self-reported, providing information about self-perceived knowledge and comfort but limiting inferences about actual learning impact. Understanding how skills learned in the VR environment are transferable to the clinical environment was beyond the scope of this study but would be beneficial to investigate further. Finally, physical discomfort and cybersickness are potential limitations of VR use and can negatively influence learner attitude toward the experience and thus the educational outcomes. VR applications involving simulated movement or rapid visual changes can induce nausea and dizziness. Despite this potential, these side effects did not seem to have a significant impact in this study cohort and there was no observed correlation between participants' self-reported propensity to motion sickness and the severity of symptoms experienced during the training. Furthermore, the reported symptoms of motion sickness were generally mild in nature.
Suggestions for Future Research
The data from this study will be used to further refine the VR simulation towards its final design state. Future research should employ instruments with greater validity evidence, such as the System Usability Scale or the simulator sickness questionnaire, to obtain more reliable data to interpret participant experiences. (Brooke, 1996; Sevinc & Berkman, 2020) This will be important prior to conducting comparative efficacy studies of VR to other simulation modalities.
This pilot study serves as a crucial guide for future work and plays a pivotal role in evaluating the implementation of a VR training application. Participant suggestions included incorporating enhanced features, refining controls, addressing glitches, and providing clearer instructions. In the context of this pilot study, gathering feedback from participants is necessary to refine and enhance future iterations of the VR program. Through active engagement with participants and careful consideration of their insights, developers and educators can iterate upon the software to ensure continuous improvement and alignment with the needs of learners.
Conclusion
A single institution mixed-methods pilot study on a newly developed VR manual defibrillator training application demonstrated feasibility for use of VR for component skill training in cardiopulmonary resuscitation, as well as decreased time to shock in the simulated environment and positive feedback from users. Future study will refine the VR training tool based on feedback from this pilot, compare educational outcomes between the VR application and other training modalities, and evaluate the impact of this type of VR training within a longitudinal training curriculum.
Footnotes
Acknowledgements
Thank you to Maneesha Aggarwal, Parixit Davé, John Martin, and the Emerging Technology Consortium sponsored by Columbia University IT for ongoing support with VR software development and logistics. Thank you to Matthew Kersey and Ray Li for initial software development, Woojin Shim for simulation and VR technical support, and Jonathan Amiel and the Office of Innovation in Health Professions Education for curricular strategic advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Participant view of VR simulation with the two game modes (top two panels) and virtual hospital defibrillator and pads (bottom two panels).