
Abstract
The issue of pregnant women’s exposures to everyday chemicals and the implications for the health of future children are receiving increased attention in popular media and in the academic press. In response, health profession organizations are developing clinical practice guidelines for warning pregnant women about the risks associated with exposures to certain toxics. We evaluate different sides of a risk-avoidance approach for pregnant women in the context of a hypothetical case study involving phthalates and women who work in nail salons. We consider the ubiquitous nature of low-dose exposures and both the positive aspects and limitations of promoting avoidance measures with respect to phthalate exposures. We conclude that a risk-disclosure approach has both practical limitations and equity dimensions which must be factored in to public health guidelines and messaging and the development of clinical practice guidelines. Upstream solutions including regulatory action on chemicals and heightened attention to environmental justice would result in optimal management of this issue.
Introduction
In an October 2015 statement to a congress of childbirth professionals, The International Federation of Gynecology and Obstetrics (FIGO) refers to exposure to toxic environmental chemicals during pregnancy and breastfeeding as “a threat to healthy human reproduction,” issuing a call to health professional societies “for timely action to prevent harm.” 1 They add, “we are drowning our world in untested and unsafe chemicals, and the price we are paying in terms of our reproductive health is of serious concern.” 2 Citing research by Woodruff et al., they note that “virtually every pregnant woman in the USA (United States of America) has at least 43 different environmental chemicals in her body.”1,3 The statement refers to the “tens of thousands of chemicals in global commerce … [for which exposure during pregnancy] can trigger adverse health consequences” for both the mother and the fetus. 1
The scientific research behind the notion that a pregnant woman’s exposure to a toxic substance could cause harm to her fetus is, historically, relatively recent. Today in North America, a woman’s experience of pregnancy has become far more public and under greater surveillance than in days past. What she eats, whether she exercises, whether and how much she consumes alcohol or caffeine, or if she smokes, are now seen as the business not only of her health care provider but the entire public health system.
Science has learned a great deal more about the vulnerability of the fetus in the last century. We now understand that the placental barrier has its limitations regarding exposure to toxic substances and endocrine-disrupting chemicals (EDCs). The umbilical cord transmits to the placenta not only the residue of tobacco and alcohol but also industrial chemicals, pollutants, and pesticides.
When science has a good understanding of the consequences of fetal exposure to certain substances, it can lead to crucial advice for women, and direct them toward effective behavior modifications in pregnancy, reducing morbidity, mortality, and other detrimental health outcomes. For example, smoking during pregnancy has been studied extensively and is linked with a host of adverse health consequences for both the women and the babies born of those pregnancies. Alcohol is another case in point.4,5 Where the science is clear and the advice is simple and practical (i.e. reduce or eliminate tobacco/alcohol), clinicians and public health agents can dispense information to pregnant women with some level of confidence that they are equipping individuals and communities with tools that will aid them in preventing harm.
With prescription medication, the legacy and lessons learned from the case of thalidomide resulted in significant changes to the way drugs are regulated in Canada and elsewhere.6,7 Today, a great deal more is known about the effects of many prescription medications on pregnancy outcomes, making another area where physicians working with pregnant women can provide them with clear directives, if not always easy choices.
It is from this history of a risk-based/information-providing approach with substances like alcohol, tobacco, and other drugs that childbirth professionals are navigating the challenge of exposures to everyday chemicals in pregnancy and preconception.1,8–11 Here, we discuss how, while beginning to address some of the harms posed by exposure to everyday chemicals, this approach has limitations as an overall public health strategy.
Clinical Practice Guidelines
How have western health professions involved in maternal–child health care (obstetricians, family doctors, midwives, obstetrics nurses) responded to the complexity of trying to protect future generations from harm due to toxic exposures?
In a 2008 editorial to her colleagues in American Family Physician, Schwarzman
9
notes [a]s physicians we will never have perfect information. However, widespread exposure to EDCs at doses linked to chronic health effects in animals, combined with significant barriers to establishing definitive evidence of human harm, warrant that physicians be educated about developmental exposures to EDCs.
In Canada, in November 2014, a group of organizations including the Canadian Partnership for Children’s Health and the Environment (CPCHE) and the Society of Obstetricians and Gynecologists of Canada (SOGC) held a Prenatal Environmental Health Education Forum aimed at finding strategies for educating prospective parents on the “negative effects of environmental exposures on fetuses and young children.” 12 Most recently, the aforementioned FIGO Statement continues to highlight this issue, but goes farther, calling for “timely action to prevent harm,” calling on health professionals to “advocate for policies to prevent exposure to toxic environmental chemicals and … to champion environmental justice,” and that “the potential health impact of a low-dose exposure to a toxic chemical is not the same for everyone.” 1 The statement recognizes that those who are most affected are often those with the least amount of power and personal agency.
The case has been put forward for the importance of counseling women on the best ways to minimize exposures in the preconception phase and during pregnancy.8,10,13 The Occupational Safety and Health Administration of the US Department of Labor provides numerous resource materials about chemical exposures and reproductive health, emphasizing that most research has not been conducted on humans, only animals. 14 European agencies such as HEAL (Health and Environment Alliance) have amassed substantial materials advising women on how to minimize their exposures during pregnancy. The list of resources is more extensive than this and growing. In support of this approach is evidence that when avoidance measures are put in place, exposure is lessened and that when provided with information about chemical exposures during pregnancy or preconception (e.g. through biomonitoring studies), women were not necessarily unduly alarmed.15–18
How realistic is it to rely on the behavior and purchasing practices of individual women to significantly alter the growing problem of toxic exposures in pregnancy? Sociologist Norah MacKendrick has documented the extent to which practices of “precautionary consumption” have been taken up by those with the financial, educational, and class positions to do so.19,20 In fact, there is a growing push to inform and educate not just pregnant women but all citizens about how they can reduce their exposures to toxic chemicals by reading labels, shopping wisely, and making less toxic choices, a practice MacKendrick calls “a form of privatized self-protection.” Citizen’s right-to-know campaigns by the David Suzuki Foundation (“Shopping with your dukes up”; “Five easy ways to go green at work”) and Canadian environmentalists Rick Smith (“Slow Death by Rubber Duck”; “Toxin, Toxout”) and Gillian Deacon (“There’s Lead in Your Lipstick”) promote actions that seek to empower consumers in the task of reducing their chemical body burdens.21–25 As a form of ecological citizenship, precautionary consumption has been recognized as relatively shallow. Its efficacy has also been questioned. 26
While these practices may change the situation for a select portion of the population, what of those who have some of the highest rates of toxic exposures and the least amount of agency to change their situation?
Phthalates and Nail Salon Workers
An examination of women who work in nail salons must be placed within the broader context of the study of women’s occupational health, an area largely neglected in health research until recently and, especially in regard to occupational reproductive hazards, fraught with methodological challenges. Messing 27 documents the resistance and challenges faced by occupational health researchers as recently as the 1980s and 1990s, when undertaking scientific study of pregnancy in the workplace. Messing et al. 28 have summarized that within occupational health research, hazards from women’s work have been underestimated and that assumptions about women in occupational settings have often been based on male-only research.
Women who work in nail salons—particularly those who work in discount salons—are exposed daily to hazardous chemicals found in the polishes, removers, gels, shellacs, disinfectants, and adhesives that are staples of their work. Phthalates, formaldehyde, and toluene make up what is known as “the toxic trio” of frequently-used chemicals in this industry. Exposure to chemicals from the toxic trio and beyond can occur through dusts and vapors; routes of exposure can be via skin, lungs, and blood. These chemicals may cause allergic reactions including asthma and allergic contact dermatitis. They may also be associated with certain cancers and adverse reproductive effects.29–37
Reproductive Health Effects of Chemicals Used in Nail Salons.
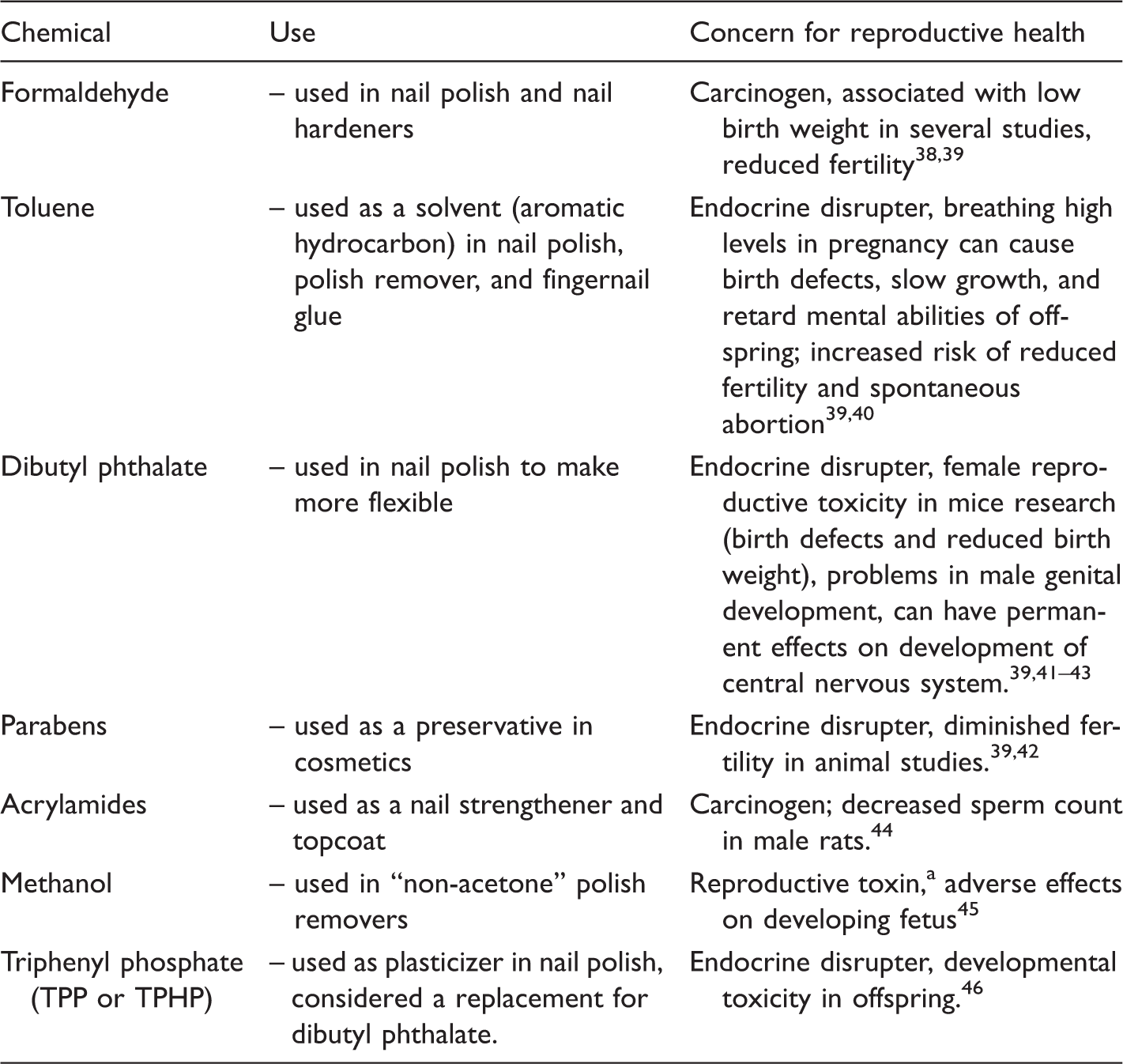
adverse effects on sexual function and fertility in adult males and females, as well as developmental toxicity in the offspring. The hazard class “reproductive toxicity” is differentiated into adverse effects on sexual function and fertility, or on development, and effects on or via lactation. 42
Nail salon workers in the Greater Toronto Area are primarily recent immigrants to Canada, speak limited English, and lack an understanding of and access to regulatory and health-care systems that may affect their work and their lives. 47 Quach et al. 48 note that new immigrant women make up a majority of nail salon workers in parts of the United States who “are drawn to this profession because it does not require long training or high English proficiency.” We assume that these same factors account for the high proportion of immigrant workers in nail salons in Canada. David 49 notes that nail technicians in Toronto who emigrated from China usually learn how to do nails on the job and without formal training. The most recent immigrants tend to be employed in discount salons where the cost of a manicure or pedicure can be kept low by using the cheapest, and generally most toxic, products. For the most part, this vulnerable group of workers earn low incomes and work in non-unionized environments. Market researchers for potential investors note that “the level of regulation is low, permitting easy entry by new operators.” 50 An investigative journalist with the Globe and Mail found that women working in this industry in Toronto did not want to be interviewed about their health for fear of repercussions stemming from their immigration status or from the owners of the salons where they worked. 51
Research on the effects of the in utero exposures on the children born to nail salon workers is not extensive. In one study that looked at a range of occupations where organic solvents were used, including nail salon workers, the children exposed to organic solvents in utero did more poorly on tests of auditory memory, general verbal information and attention when compared to a control group of children born of non-exposed women. 52 In a study of hairdressers and cosmetologists, the risk of babies being born small for gestational age and the risk of perinatal death were elevated for cosmetologists when compared to a control group of teachers. 36 Herdt-Losavio et al. 35 found a slightly increased risk for low-birth weight babies among cosmetologists compared to a group of realtors. 35 The risk was greater among non-White women in each comparison in the latter study.
Dibutyl phthalate, one of the most commonly found chemicals in this occupational setting, is incorporated into nail products as solvents and plasticizers and to strengthen the longevity of a polish application (i.e. to hold color and to prevent chipping). The family of phthalates is of particular concern to this discussion because of its endocrine-disrupting properties. As well as on the job, nail salon workers are additionally exposed to phthalates through widespread ecosystem contamination through releases in manufacturing, making their way into air, water, and food chains; food contact with plastics can also lead to human exposure. 33 Of environmental concern, phthalates in plastics also biodegrade very slowly. The chemical’s presence is considered ubiquitous.
Dibutyl phthalate is only one substance of a larger family of phthalates, a chemical grouping which has been the subject of some scrutiny of late, particularly due to concerns relating to developmental and reproductive effects. In Europe, where regulation of phthalates has been more robust, dibutyl phthalates have been banned in cosmetics and in children’s toys; some restrictions on use also apply in children’s toys in the United States. In Canada, a total of 28 phthalates are under review under the country’s Chemicals Management Plan. 53 Due to health concerns, a growing market for non-phthalate plasticizers has emerged. 54 While some show promise, others indicate similar problems to the original chemical; many are not yet well researched with respect to their effects on human health. 55
Phthalates in humans can cross the placenta to the developing fetus and be transmitted through breast milk to the growing child. 38 Negative reproductive outcomes such as preterm birth have been associated with phthalate exposure. 34 Quach et al. 56 found a significantly increased risk of diabetes, gestational diabetes, premature rupture of the membranes, and placenta previa among manicurists and cosmetologists compared with the general population for all races and for a subset of Vietnamese who were studied. When exposure occurs during the phase of fetal development when sexual differentiation happens (i.e. during the first trimester), malformations of the reproductive tract can occur.35,39,57,58 Particular malformations of the male reproductive system linked to phthalate exposure have been found in newborns.33,59
In the scenario below, we consider the promise and limitations of a risk-disclosure strategy for addressing the potential harms posed by exposures to these chemicals to a pregnant woman working in a nail salon.
Counseling for Risk Scenario
A young woman employed in a nail salon, a recent immigrant, learns that she is pregnant and visits a clinician for care. Imagine a clinical practice guideline exists, and that her clinician provides standardized information about the risks associated with low-dose exposures to EDCs. In our view, several limitations become obvious.
First, avoidance will likely be less effective when a woman is already pregnant. Timing of exposures is critical here: preventing future harm to a child would require parents to begin mediating their exposures prior to conception. Given that roughly 40% of all pregnancies in Canada are unplanned, a high proportion of women would not receive the appropriate messaging in time to prevent harm. 60 Compounding this, many women do not know that they are pregnant in the early weeks of gestation and thus will not likely visit a clinician for pre-natal care until organogenesis, considered a key period during which the embryo is susceptible to the effects of phthalate exposure, is completed. 61
In Canada, Sharma et al. 61 interviewed obstetricians, family physicians, and midwives about the availability of pamphlets in family physicians’ offices and postpartum care that might assist with risk management for subsequent pregnancies. While this kind of information disclosure might be useful to mitigate this problem in future pregnancies, it has limited usefulness for the already-pregnant woman who presents in this situation where, as is noted in the FIGO statement, “preventable exposures may have already occurred.” 1
Second, although phthalates are ever-present in a wide variety of settings, one may not know that they are being exposed because, like other chemical compounds used in the manufacturing of nail salon products, they are rarely labelled. In Canada, phthalates are largely unregulated and only specifically restricted for use in soft vinyl toys. 62 While some product information is available through organizations such as the Environmental Working Group’s Skin Deep database (http://www.ewg.org/skindeep/), sourcing this information assumes that one has the time and literacy competence to benefit from it.
Biomonitoring studies undertaken by Rudel et al. 16 found that when study participants’ diets were restricted to food with limited packaging, their exposure to phthalates and BPA were reduced. This is an important finding, particularly for those with the time and financial wherewithal to purchase unpackaged food, but how does this translate for the pregnant nail salon worker whose average income in Canada is $13 an hour?
In this context, what advice can a clinician offer? How could he or she identify products, behaviors or practices for the woman to avoid? One of the obstetricians in Sharma et al.’s 16 study highlights this difficulty: “… I still don’t know what to tell my patient … I can’t say … buy this and don’t buy that … people often do not have the resources to go the other way.” The highly ubiquitous nature of phthalates in our environments makes avoidance a near impossible undertaking, even for those with adequate resources. Exposure can certainly be minimized—with proper knowledge, the capacity to avoid critical environments of exposure, and the resources to purchase different products—but complete elimination is impossible.
Third, avoidance is a worthwhile goal but not entirely practical for women working in nail salons and related occupations. The precarious nature of their employment can make it challenging to avoid these exposures. Quach et al. 48 summarize the options for controlling exposures in this setting, including source reduction (i.e. using less-toxic products), improved ventilation (e.g. general and local exhaust ventilation that divert fumes at the point of generation), and the use of personal protective equipment (e.g. N95 masks—which protect against particulate matter in the air but not against vapors and fumes—and nitrile gloves). 48 These are all important measures and, in the absence of less toxic products being made available routinely, are worth pursuing.
However, convincing salon owners to invest in less-toxic alternatives can be difficult and potentially risky for employees, changes to ventilation are likely to be restricted because of cost, and wearing masks and gloves have other challenges.
63
Quach et al.’s
64
research based on focus groups with nail salon workers from 18 California nail salons found that “owners control the salon settings (e.g. products used and ventilation systems) and workers’ schedules (e.g. when breaks are allowed). Furthermore, owners can control the information that is given to workers.”
64
Kang’s
65
research of Korean nail salons in New York City showed that there is “often a wide gap between what manicurists know they should do and what they are actually able to do”. One of her study participants commented, When you use gloves, customers feel bad, so I don’t use them [and] … The owner doesn’t like it when you wear a mask with regular customers … because she wants you to talk to them. (p. 227)
The limitations to serious reduction in toxic exposures contribute to the basic problem associated with the risk-disclosure model: there is a lack of clear, effective, and practical advice available for clinicians to offer women concerning many EDCs. Additionally, physicians and other maternity care providers are not trained in toxicology or environmental science, and concepts such as “effects from low-dose exposures,” “windows of vulnerability,” and “multiple pathways of exposure” are complex notions to convey to patients.
Care providers already appreciate several difficulties with this risk-disclosure/avoidance approach. Sharma et al. 61 found that the care providers involved in her study “did not perceive engaging in the discussion of phthalate exposure in pregnancy as relevant.” A reason given for this view was discussed above: the clinicians would have already missed the opportunity to inform during the critical period of exposure in early stages of fetal development. Further, Stotland et al. 8 surveyed 2,514 US obstetricians on the topic of prenatal environmental exposure. 8 While they felt they could reduce patient exposures to environmental health hazards by counseling them, they also expressed fear of causing anxiety among patients.
The concern about fear and anxiety is a real one. Messing, 70 Altman et al., 71 Lee and Scott, 72 Mykitiuk and Scott, 73 MacKendrick,19,20 and Wiebe and Konsmo 74 have all argued against implementing policies and practices that contribute to a culture of blaming women for putting future children at risk through their behaviors and actions when pregnant and as mothers. This is particularly unfair to women who are marginalized for reasons of socioeconomic status, race, or occupational vulnerability, such as nail salon workers.
The risk disclosure model rests on the assumption that when given reliable information about risks, women will exercise agency and make choices in accordance with their own risk preferences. The model falls short when individual agency is conditioned by broader socioeconomic factors and structural inequalities. Even FIGO advocates that simply informing women is not enough, that “external factors may limit the capacity of individuals to make healthier choices” and that “improved public policy is essential to reducing exposure[s].” 1
Conclusions
Women’s exposures to toxic substances and EDCs during pregnancy and in the preconception phase are having harmful health impacts on their future children. In the absence of state regulation that would reduce or eliminate these exposures, women reach for whatever tools are available to protect themselves—and future generations—as best as they can. Beyond efforts to direct women to mediate their exposures to toxics through vigilant consumption, there is also a growing chorus of calls for clinicians to provide women with this risk information when they become pregnant or begin to contemplate a pregnancy. We have identified several shortcomings with this approach in practice, using the scenario of the pregnant nail salon worker. This area of practice would benefit from research data collected through in-depth discussions with maternity care practitioners to ascertain how they are coping with this new challenge and what solutions they might propose for moving forward for real change.
If a woman is planning to get pregnant or is pregnant, there is no question that avoiding or limiting exposure as much as one can is important. Childbirth health professionals should be encouraged to provide what information they can in as timely a manner as possible. A growing body of resources produced in North America and Europe can provide health professionals with some answers to the complexities that surround this issue when counseling their patients.
However, our analysis leads us to conclude that relying on this approach without considering other key strategies does not constitute healthy public policy. The approach for reducing harms to women and their children resulting from toxic exposures in pregnancy would ideally have three prongs.
Educate the public—via publicly funded education campaigns and clinical practices of childbirth health professionals—about toxic exposures and how to avoid them; such educational campaigns should be financed by public funds or by foundations that are not compromised by corporate donors. Advocate for change that would lead to the creation of policies that prevent exposures to toxic environmental chemicals including rules and regulations governing working conditions that put pregnant women at risk. Ensure that Canadian and other federal governments enact laws that mandate their chemical regulators to abide by the precautionary principle. Such laws should include the following provisions: (a) phasing out and ultimately removing those chemicals in commerce that are deemed toxic through a rigorous screening process, (b) requiring toxics use reduction and safe and tested substitutions while that phase-out process is occurring,
75
and (c) exercise more vigilance in not allowing any further problematic chemicals onto the market.
The FIGO statement acknowledges that “segments of [health professionals’] patient population likely bear a disproportionate burden of exposure to toxic chemicals” and that they should “champion policies and practices that secure environmental justice on a global scale.” 1 Those women who are most at risk of bearing the burden of toxic exposures that put their future children in harm’s way did not create the situations that put them at risk. When collective responsibility is assumed for rectifying this problem, all current and future pregnant women will benefit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anne Rochon Ford has been employed to conduct research with funding from the Institute for Human Development, Child and Youth Health (IHDCYH), Canadian Institutes of Health Research (CIHR). She has additionally received funding from the federal government (Health Canada) in her employment with the National Network on Environments and Women's Health and with the Canadian Women's Health Network. Dayna Nadine Scott has received research funding from the Institute for Human Development, Child and Youth Health (IHDCYH), Canadian Institutes of Health Research (CIHR), under grants RHF-100625 and RHF-100626.