
Abstract
Bloodborne pathogen exposures continue to be an occupational health concern of high importance. It is uncertain whether national regulations and enforcement have an impact on employer action for reducing risk. The goal of this research was to determine whether citations issued under the Occupational Safety and Health Administration’s Bloodborne Pathogens Standard changed over time given these changing risks and controls. Researchers analyzed 31,066 inspections. There were 77,142 citations issued between 1991 and 2015. The highest frequency is the time period just after revisions of the 2001 standard. There were striking levels of noncompliance, most evident in Exposure Control Plan and Recordkeeping violations. No other pattern or change was evident. In the time periods after 2005, numbers of citations remained steady or declined. As new bloodborne pathogens emerge annually, it is essential to continue to focus on enforcing the standard to keep employers in compliance and workers protected.
Keywords
Introduction
Bloodborne pathogen (BBP) exposures have long represented one of the signature occupational hazards in healthcare. Occupational Safety and Health Administration (OSHA) promulgated the Bloodborne Pathogens Standard (BBPS) in 1991 and engaged in additional rule-making after passage of the Needlestick Safety and Prevention Act (NSPA) in 2000.1,2 Since OSHA began enforcing NSPA changes fifteen years ago, global changes have risen in occupational risk from exposures to newer BBPs, including ebola and zika viruses. The hepatitis B and hepatitis C virus threats remain present because of increasing access to U.S. healthcare systems from infected populations both nationally and abroad. 3 Ensuring that workers are afforded a safe working environment with protections against BBPs requires ongoing vigilance, recognition of new hazards, and recognition of possible reemergence of old problems in new situations.
The healthcare industry has sought to improve quality and safety for both patients and personnel by examining performance, identifying practices, and trends. 4 Although enforcement agencies generally have some tradition of quality measures, internal auditing, and evaluation, few systematic reviews of enforcement actions and its impact exist. Data document the utility and beneficial consequences of enforcement actions for employer performance after inspections, but the traditional models of evaluation and action, i.e., quality management and improvement, whether early models (“plan-do-check-act”) or more sophisticated approaches (lean six sigma) have generally not been applied to enforcement.4–6 As it relates to documentation and improvement relative to occupational exposure to blood and other potentially infectious materials (OPIM), the employer’s Exposure Control Plan (ECP) functions as a comprehensive exposure assessment and details not only the controls put in place to prevent exposures but also serves as a facility-based model from which internal measures can be monitored, evaluated, and updated.
Few national surveys of occupational hazards relative to occupational exposure to BBP exist other than the International Safety Center’s Exposure Prevention Information Network (EPINet®) and the Association of Occupational Health Professionals in Healthcare EXPO-S.T.O.P (Exposure Survey of Trends in Occupational Practice).7,8 The National Institute of Occupational Safety and Health (NIOSH) has not funded the planned National Occupational Exposure Survey in follow-up to the National Occupational Hazard Survey of the 1980s. Data on healthcare hazards are sparse. Participation in NIOSH’s new Occupational Health and Safety Network (OHSN) targeted at healthcare is voluntary and as of 2019 will be defunded; currently available data are not expected to be shared publicly. Although they are not national in scope, both the Massachusetts Sharps Injury Surveillance System and the University of North Carolina Employee Occupational Health Service publish intermittent state-based or facility-based surveys that serve as reminders of the importance of preventing occupational exposures to blood and OPIM.9,10
OSHA inspections are not random because they occur in response to complaints or are targeted at high-risk employers. The analysis of OSHA inspection results therefore may not be representative of what is happening in all healthcare systems. Inspections are generated in two broad categories, i.e., triggered by employer-specific events or resulting from OSHA internal planned activities. Employer-specific triggers include worker complaints, hospitalizations, fatalities, and referrals from individuals (treating physicians, observers) or other agencies or accrediting bodies like the Food and Drug Administration or The Joint Commission. Planned inspections arise in systematic ways, i.e., national, regional, or local emphasis programs. They are designed to survey specific industries or specific hazards in defined geographic areas and are driven by interest in the Area Office, the Region, or OSHA’s National Office. Other inspections occur in routine follow-up to enforcement actions. States with OSHA-approved state plans have similar inspection programs. State plans are described more fully below.
OSHA and state OSHA inspections may therefore provide some indication of nationally representative distributions of hazards and controls. The authors explore what OSHA has found during its inspections for BBPs as they relate to the potential impact of policy implementation on occupational health and safety, e.g., revisions to the OSHA BBPS after the 2000 NSPA.
OSHA BBPS citations are issued to employers for violating specific provisions of that standard that are identified by numbered paragraphs and subparagraphs. State OSHA plans also issue citations for violating BBPS that are the same as or more effective than the federal standard. The provisions of those standards include, but are not limited to, the requirements to have the following in place: the use of engineering controls (e.g., safer medical devices); work practice controls; proper disposal of devices and regulated waste; labeling of biohazards; training; vaccinations; establishing and updating of the ECP; and maintaining a Sharps Injury Log. Failure to comply with any element identified during an on-site inspection by an OSHA Compliance Safety and Health Officer or state OSHA inspector (CSHO) may result in a citation. CSHOs propose and discuss citations with their supervisory chain and employers, and the OSHA Area Directors and their state equivalents issue corresponding citations and notifications of proposed penalties. In the states covered by federal OSHA, employers may contest citations and proposed penalties before the independent Occupational Safety and Health Review Commission, whose decisions may be reviewed by U.S. courts of appeals. In states with state plans, similar provisions for contesting citations and penalties are in place. This analysis excludes citations that are vacated.
This descriptive analysis explores how the number of OSHA inspections and subsequent citations changed over time in relationship to the promulgation of new BBPS requirements and ongoing awareness of the risk of not only bloodborne disease but also the availability of newer, safer medical devices and instrumentation available on the market. During the first twenty-five years of the BBPS, approximately seventy-seven thousand citations resulted from more than thirty-one thousand BBPS enforcement actions (inspections). The authors examined these actions with several goals in mind. The first was to document agency actions and experience in inspections. The second was to explore patterns of employer behaviors in program implementation that could become evident in changing patterns of violations. Finally, the authors wished to identify whether changes associated with or resulting from new law had an impact over time based on OSHA and state OSHA inspections and subsequent citations.
Methods
OSHA has relied on two major electronic systems for tracking its enforcement work; the Integrated Management Information System, in use until 2012 and the OSHA Information System since then, with some overlaps. OSHA covers private-sector workers in thirty-two states (the term “states” includes states, District of Columbia, and territories) and twenty-eight “State Plan States.”
A single file was assembled from OSHA’s data systems with a unique identifier for each inspection. Each citation from the same inspection received that one identifier. Separate inspections in the same facility at different times received separate unique identifiers. Inspections were assigned a date and year by the opening date of the inspection. Citation items were coded by the detailed paragraph of the BBPS, after realigning the different paragraph numbering in the various state standards. Those paragraphs were coded and assembled into two separate hierarchies, one by time period and the other by major paragraph of the standard, for example, ECP. Inspection data were not sorted by industry sector type; however, the majority of citations were in the healthcare sector.
Data were scrutinized by category of inspection, i.e., programmed/planned (i.e., triggered by an OSHA program) versus all others, triggered by outside questions, as these likely represent different categories, driven by OSHA priorities versus generated by specific employer- or facility-based problems. The first, programmed/planned, included the following codes from the OSHA Information System: POTH = Planned Other, PP = Program Planned, PREL = Program Related, M = Monitoring, and FU = Follow-up. The others, triggered from the outside, included the following: C = Complaint, F = Fatality, FC = Fatality/Catastrophe, REF = Referral, UNP = Unprogrammed, UNPREL = Unprogrammed Related, and UNPOTH = Unprogrammed Other.
Inspections were assigned a temporal grouping code, by five-year time periods (1) 1991–1995, (2) 1996–2000, (3) 2001–2005, (4) 2006–2010, and (5) 2011–2014. As OSHA issued the NSPA revisions in 2001, Time Periods 2 and 3 represent a major policy intervention.
Results
The agency data files contained records of 31,066 total inspections resulting in 77,142 citation items under the BBPS in Federal OSHA and State Plan states. Further references to OSHA combine both Federal OSHA and State Plan OSHA programs. Table 1 presents the number and percentage of total BBPS inspections for each five-year period. Each inspection represents a single facility at one point in time with at least one BBPS citation.
Total Number of Inspections by Time Period.
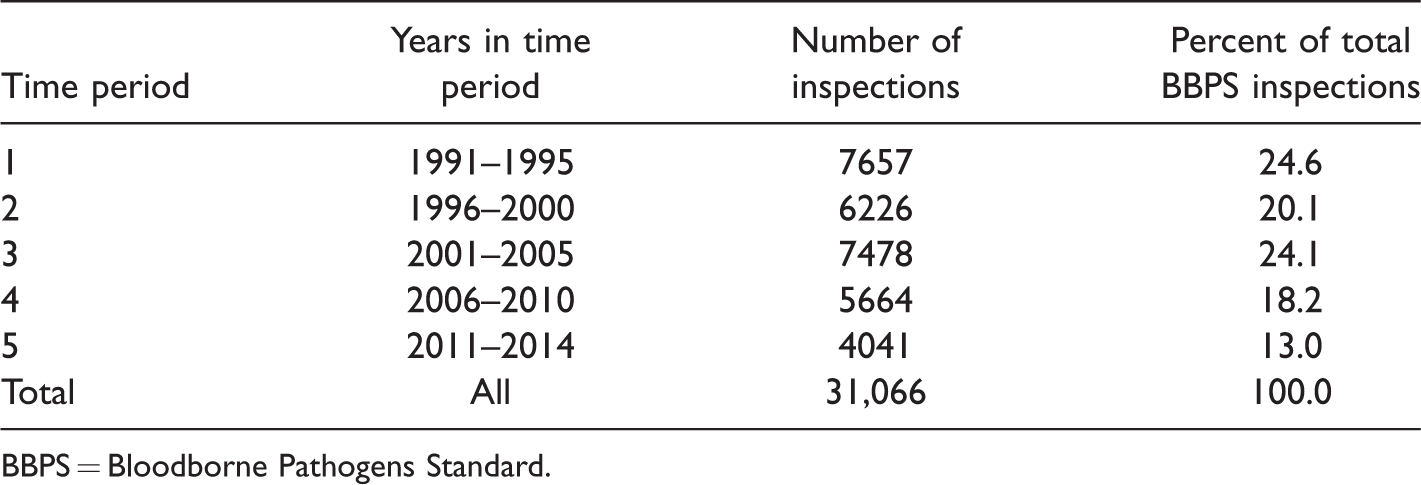
BBPS = Bloodborne Pathogens Standard.
The largest numbers of inspections were performed in the time period immediately after promulgation of the original standard and then again after the 2001 revisions to the standard required by the NSPA. Citation items issued during the most recent time period (2011–2014) represented the lowest total numbers of inspections.
Table 2 presents the number and percent of citation items under each major paragraph of the standard. Although the initial version of the standard required an ECP, the implementation of the NSPA in 2000, with the subsequent release of Center for Disease Control self-help manual (Workbook for Designing, Implementing, and Evaluating a Sharps Injury Program) in 2000, clarified those requirements and presented more detailed guidance. The majority of violations, and the majority of inspections with any violation, referenced the ECP, making up more than a third (33.99%) of all citation items. The requirements under the major paragraph for “communication of hazards to employees” encompass requirements for signage, labels, and color-coding as well as training. Methods of compliance include the use of engineering controls, such as safety devices, sharps containers, and regulated waste containers.
Total Number of Citation Items for OSHA Bloodborne Pathogens Standard by Major Paragraph, 1991–2014.
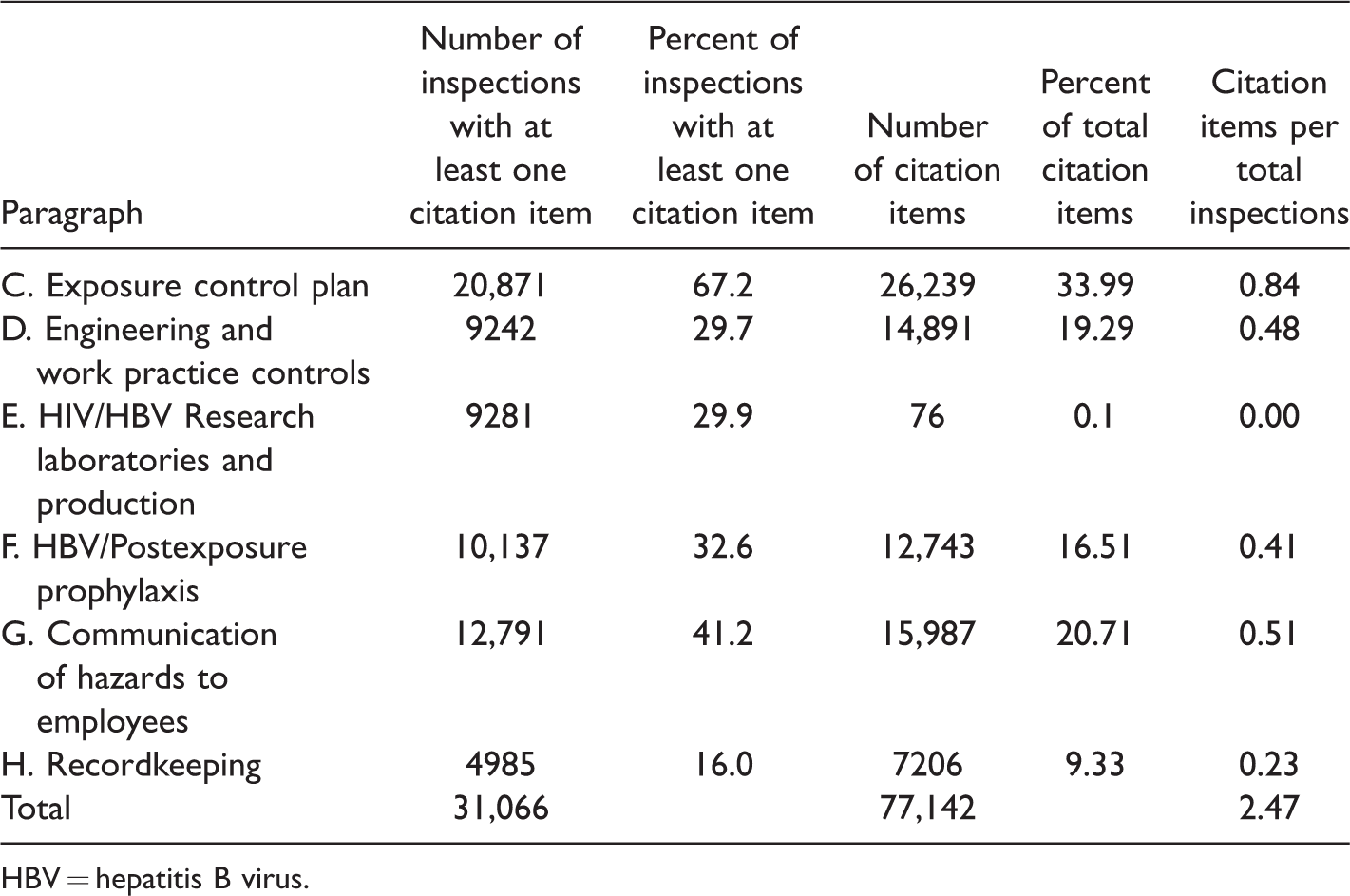
HBV = hepatitis B virus.
Clinical management of healthcare workers requires the offer of hepatitis B vaccinations. Failure to offer these vaccinations continues to be cited under paragraph (f) of the BBPS. 11 Other paragraphs remained relatively stable in the course of the twenty-five years, except for the new requirements required by the NSPA, including establishing and maintaining a Sharps Injury Log, nonmanagerial frontline employee feedback, and evaluation of engineering controls and work practices, and an expanded definition of engineering controls to include Sharps with Engineered Sharps Injury Protections (SESIPs) and needleless systems.
Of the total, 17,481 (56.3%) inspections arose from planned OSHA activities, and 13,585 (43.7%) resulted from outside triggers. Figure 1 presents the number of citation items by major standard paragraph for each of the five-year periods. The individual bars represent the proportion of inspections leading to at least one citation item under the major paragraphs presented separately by whether the inspection was triggered by an outside action or planned by OSHA. No category had a consistent decrease in citations over that time.
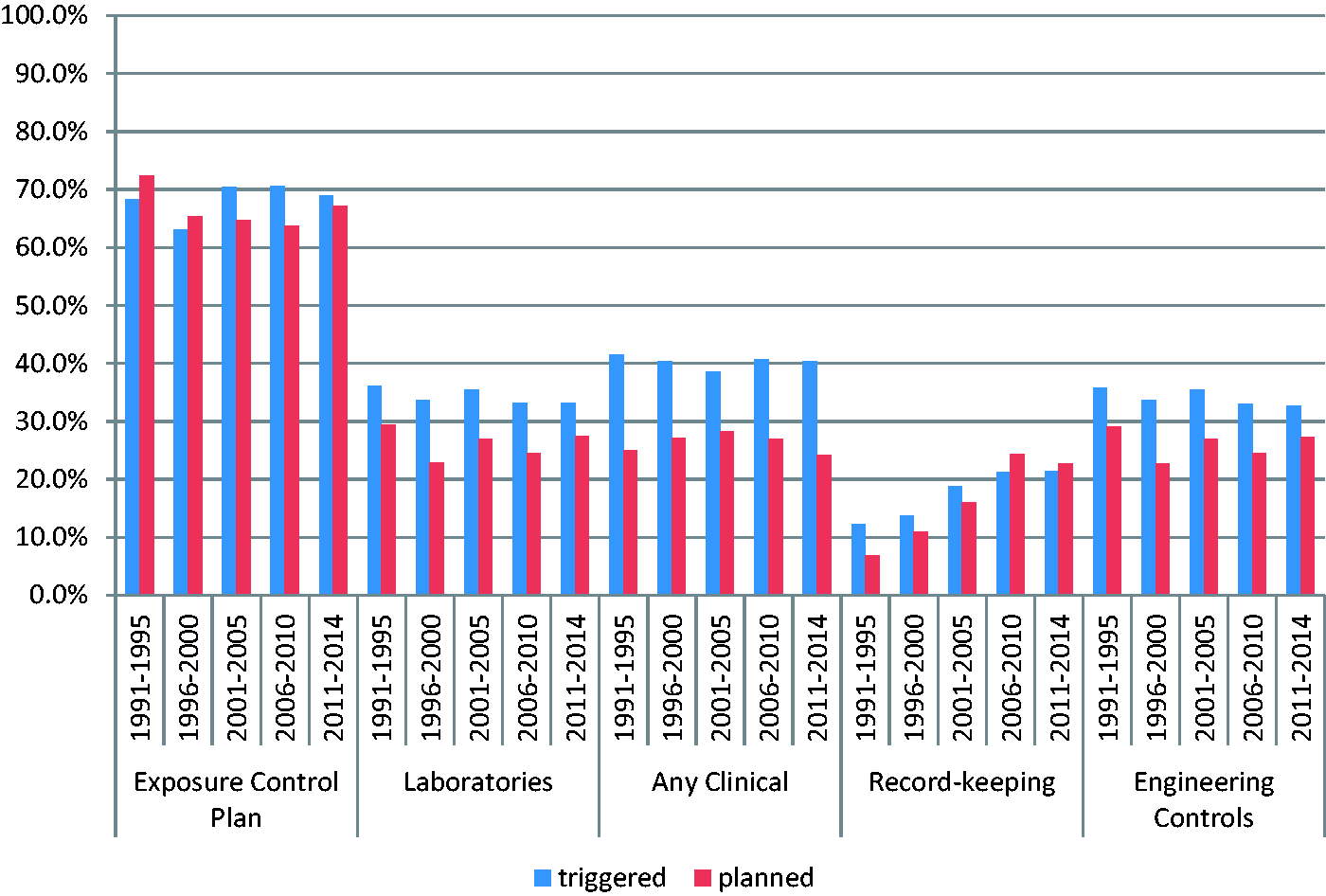
Percent of major paragraphs cited by time period—triggered versus planned inspections, 1991–2014.
Strikingly, BBPS recordkeeping violations almost tripled, from 9.8% to 22.2%. Scrutiny of the time pattern suggests that the new requirements in 2001 for employers to establish and maintain a Sharps Injury Log did not influence the rate of change, with the rate of increase slowing only after 2005. Exposure control plan deficiencies were noted without a major change across those five periods either. The persistent failure to review and document the ECP on an annual basis was striking.
When analyzing inspection data for each time period for inspection type (planned or triggered), there were notable differences for citation items for each paragraph during each time period. Triggered investigations led to higher rates of citation items than did OSHA’s planned actions but to no other obvious consistent differences.
As an example of detailed analyses, the proportion of inspections during which employers were cited for the failure to obtain signed confirmation that employees declined hepatitis B vaccination changed over time. This showed a dramatic increase shortly after the promulgation of the NSPA but has gradually declined since then, falling by slightly more than 2% over the last fifteen years.
As the evaluation and annual review of newly available engineering controls (safety devices, SESIPs) were new requirements of the NSPA, citation items were issued for those paragraphs of interest only in the three time periods after 2001. Of note, the use of engineering controls was an original requirement of the 1991 BBPS (paragraph (d) (2) (i)). However, because of the new provisions required by the NSPA, this provision was cited with greater frequency after the 2001 revisions. After this initial rise in 2001, the numbers of citation items remained similar over the subsequent time periods.
Discussion
The BBPS is now more than twenty-eight years old, and the NSPA was passed nineteen years ago. OSHA continues to encounter violations despite assumptions that healthcare employers should have adequate knowledge and commitment to adhere to those provisions. In fact, systematic review of the citation experience suggests that the overall frequency of most violations remained relatively constant, but one specific paragraph consistently fares worse now than in the 1990s, i.e., recordkeeping. This analysis examined all BBPS violations across industries, and the file did not contain industry codes. According to OSHA enforcement personnel, a vast majority of BBPS inspections occur in healthcare; however, no specific exploration of healthcare versus non-healthcare inspections was possible given the data set.
OSHA has encountered increasing difficulties with the recording of injuries on employer 300 and 300A Work-Related Injury and Illness Logs, mandated by OSHA’s Recordkeeping Regulation (29 CFR Part1904). In 2009, the Government Accountability Office suggested that employers were hiding events systematically and charged OSHA with examining the topic. The topic has been widely studied and data continue to suggest major underreporting, as has been documented for more than forty years.12–15 Similarly, OSHA’s National Emphasis Program on Recordkeeping documents that employers with lower-than-expected rates of injuries in high-risk industries do in fact have far more recordkeeping violations than those with higher rates. 16
There is widespread advertising of services to help employers reduce “OSHA recordable injuries,” but many seem to focus on reducing the rate of overall recordable injuries, rather than preventing the specific injuries and exposures themselves. The gradual progressive increase raises the question whether this will be in fact a long-term trend. Recent changes in recordkeeping requirements have generated multiple national discussions about whether electronic submission of records will be required, and the final outcome on improving recordkeeping compliance remains unclear.
Although this study did not compare citations issued under the general recordkeeping rule compared to the specific requirements to keep a sharps injury log as newly required by the 2001 standard, the substantial increase in BBPS recordkeeping citations appears directly related. The relationships between recordkeeping, citations issued for recordkeeping violations, and assessing if there is an impact on more accurate injury reporting, as defined in specific standards like the BBPS may be a fruitful topic of research.
The sustained consistently elevated frequency of ECP violations represents a surprising finding because the requirement to have an ECP in place is a foundation of any facility’s safety plan and was original to the 1991 standard. The mandate for an ECP changed dramatically in 2000 with the promulgation of the NSPA requirements. There was a clear rise (Figure 2) in the early years, followed by a sustained elevation. On the other hand, there has been a gradual though not dramatic decline in the failure to perform an annual review of the ECP. As the BBPS has been enforced since 1992, CSHOs are skilled at identifying employer weaknesses and failures to manage the documentation of device replacement appropriately, especially as they are relatively straightforward “paper-work” exercises that occur during an inspection where there are clear denotations in the written program plan for when, where, and how these reviews and device replacements are being conducted. CSHOs’ experience, tenure, and oversight have improved their ability to identify violations and “make them stick.” Recent publications suggest that facilities have grown inured or lax about the risk of bloodborne disease and subsequently the implementation of safety programs pertaining to sharps and that leadership may simply reallocate focus and resources to other nonoccupational reimbursement or quality initiatives. 17
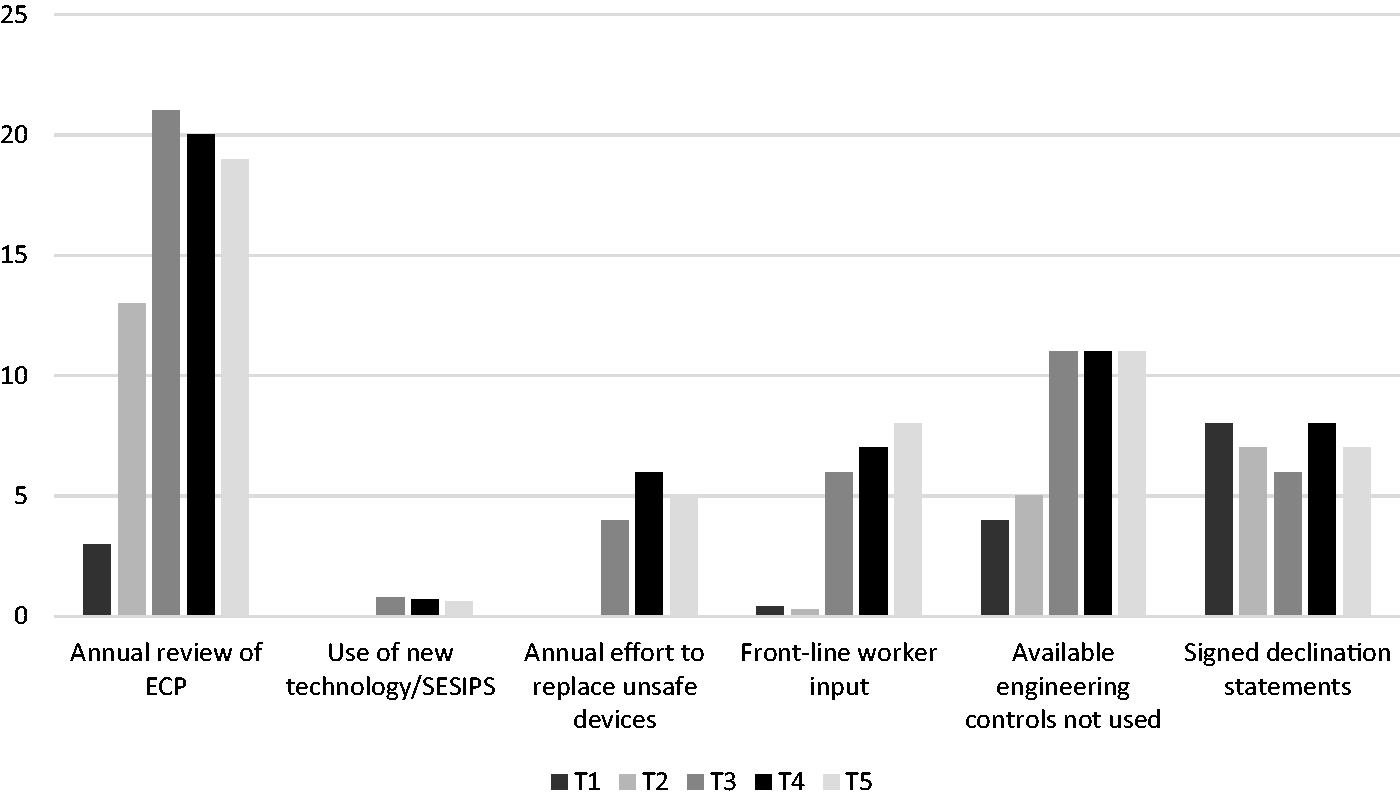
Percent change by Time Period* of Citations of High Interest, 1991–2014. *Time Period 1 = 1991–1995; 2 = 1996–2000; 3 = 2001–2005; 4 = 2006–2010; and 5 = 2011–2014 (SESIPs). ECP = Exposure Control Plan; SESIPs = Sharps with Engineered Sharps Injury Protections.
No trend in violation patterns over time was evident at the level of individual subparagraphs. Each paragraph lends itself to more discussions, but overall, this simply suggests an increasing overall failure to adhere rigorously to the standard rather than difficulties with any specific element. Healthcare facility staff and leadership turnover as well as “desensitization” to the risk of occupational bloodborne disease may represent the factors encountered in recent inspection and enforcement actions. Ideally OSHA standards, the “floor” for safe work requirements, become integrated into industry processes. In general, they do not become obsolete. The ongoing failure to adhere rigorously to elements of the standard echoes a broader failure in healthcare safety that has led to a focus on checklists and task performance.18,19
Results suggest ongoing difficulties with BBPS adherence and document the ongoing need for the standard and its enforcement. The BBPS has contributed, or at least paralleled, improvement in hepatitis B virus vaccination and the rate of bloodborne infections among healthcare workers has declined to well below that of the population at large. 3 In parallel, the proportion of employers cited for failing to offer the vaccine or have unvaccinated employees sign a declination statement has declined substantially. Nevertheless, according to the 2010 National Health Interview Survey, only 74.0% of healthcare workers with patient care experience, and, therefore at risk of hepatitis B, were fully vaccinated, with the prevalence among physicians (>80%) substantially higher than among nurses (<67%). 20 The BBPS remains important and has contributed to decreased incidence of occupational hepatitis B virus.
In many healthcare settings, a multiemployer environment exists, including permanent, temporary, contract, or agency-provided personnel. The groups range from environmental services personnel to subspecialty surgical groups, with implications for exposure prevention responsibility, and there are different and important requirements for what OSHA refers to as the creating, exposing, correcting, or controlling employers. 21 The standard requires that training on the prevention of exposure to BBPs must be provided to all workers with the sharing of BBPS responsibilities clearly defined in documents such as a contract or memorandum of agreement/understanding between the parties in a multiemployer environment.
Despite the twenty-five years since initial promulgation of the BBPS and the subsequent focus on “safer” devices under the NSPA, much work remains to ensure that healthcare facilities are not only in compliance with controls established in the standard but also that compliance is consistent over time. The data here suggest that the standard is still needed. It is uncertain if there will be lasting changes relative to ongoing enforcement and the issuance of citations in the future. As the provision of patient care environments continue to change and decentralize and as advancements continue in the medical device and equipment sector, it will be important to reevaluate this impact in the coming years.
The limitations of this study include the inability to randomly sample healthcare facilities themselves to determine if inspections were conducted based on compliance and to then contrast the facility type, geography, size, or specialty care of each facility. It is also not possible given the data set to identify if the citations issued at inspection time are illustrative of all of the shortcomings or safety control gaps that exist in a facility. Inspections driven by employee complaints are often limited to the scope of the complaint and not launched into full compliance inspections. In addition, unless a follow-up inspection occurred, the data do not allow for a prospective glimpse into the months or years ahead for a single facility to determine if the facility improved (or worsened) with respect to making its ECP actionable or maintaining more accurate records.
Conclusion
Overall, the researchers believe that OSHA enforcement of the BBPS is a necessary element in driving employers to provide the safest possible work environments to prevent illness and infection associated with BBPs like the hepatitis B and C viruses and HIV. It can also be a vehicle for promoting and ensuring measures for public health preparedness for globally emerging pathogens, like Zika and Ebola today, and whatever is to come in the future. As new clusters of BBPs emerge annually in communities, it is essential that we continue to have national, enforceable regulations in place that keep employers in compliance and ultimately that keep employees safe and well. Ongoing occupational surveillance in the form of incident reporting and recordkeeping is an important part of not only compliance but also to serve as methods to assess ongoing risk. This is a way for employers to assess if safety programs need to be improved or if there are improvements over time that have been more successful than others.
Future research of this type, using OSHA inspection data to translate compliance into a measurement of safety environment or safety climate, should focus on adjusting for some of the limitations noted above. This could include following single facilities and healthcare systems over time to identify improvements and the positive impact on recordkeeping or the Sharps Injury Log (decreased injury incidents) or comparing types of healthcare facilities based on size or geography to identify if there are differences in inspection practices or employer compliance. We lack evidence about whether workers identify BBP risk as seriously as physical or chemical hazards. Future research could compare the frequency of complaint-triggered inspections for the BBPS compared to complaint-triggered inspections other standards (e.g., hazard communication, means of egress, machine guarding, personal protective equipment). Given the changing nature of healthcare with growing decentralized administration of health services in a larger number of smaller, ambulatory centers including clinics and free-standing pharmacies, it will be important to identify whether new patient care environments impact enforcement on the national landscape as well as attention to compliance at the employer level.
Footnotes
Acknowledgments
This publication is dedicated to the late Gary Senatore, who spent considerable time ensuring accuracy of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.