
Abstract
Occupational asbestos exposure was prevalent in Taiwan, but asbestos-related diseases (ARDs) have rarely been recognized. We conducted in-depth face-to-face interviews with 16 patients with ARDs. All of them had worked in industries known for high asbestos exposure. However, only three patients had filed workers’ compensation (WC) claims, and of them, only two patients were approved. Reasons for the low compensation rate of ARDs could be divided into institutional barriers related to the flaws of the WC system and non-institutional barriers related to the knowledge status, causal interpretation, and social situations of individual workers. The Labor Occupational Accident Insurance and Protection Act passed in April 2021 has responded to the under-compensation of occupational diseases. However, the new act's effects toward improving the recognition of ARDs remain questionable. Our findings indicated that additional efforts are needed to remove non-institutional barriers hindering workers’ ability to ensure their compensation rights.
Introduction
Background
Extensive use of asbestos in many industrialized countries before the 1980s has resulted in drastic increases in the global burden of asbestos-related diseases (ARDs), including asbestosis, cancer of the lung, larynx, and ovaries, and also malignant mesothelioma (MM). MM is a rare but fatal type of neoplasm, often developed in the pleural or peritoneal linings and is known to be primarily caused by asbestos exposure. In many developed countries, asbestos use has been banned, but because of long disease latency, asbestos-related cancers are still increasing and have accounted for a sizable proportion of compensated occupational diseases.1–3
In Taiwan, asbestos ores were imported in large quantities in the 1970s and 1980s. During this period, asbestos was used in the manufacturing of building materials, thermal insulation materials, brake pads, gaskets, and other asbestos-containing products. Additionally, the shipbreaking industry used to be a significant source of asbestos exposure in Taiwan. From 1969 to 1988, guided by the economic policies at that time, some southern ports of Taiwan were turned into shipbreaking sites, processing up to 65% of abandoned ships worldwide. 4 Asbestos exposure occurred in the processes of dismantling and handling asbestos-containing insulation materials for resale purposes. The shipbreaking industry was finally shut down in 1988 after a severe industrial explosion, and since 1989, the imports of asbestos started to drop when the Environmental Protection Agency began to regulate its use. 5 However, asbestos use was not completely banned until January 2018, and asbestos-containing materials are still present in the built environment.
Given the historical asbestos exposure and an estimated disease latency of 30 to 40 years, Lin et al. 6 projected an uprising trend of ARDs in recent years. However, as shown below, ARDs have rarely been recognized as work-related and compensated in Taiwan. The low compensation rates of ARDs may be attributed to multiple factors, including health care providers’ limited knowledge and capacity in making precise diagnoses, cancer patients’ limited access to healthcare provisions, and difficulties in establishing disease causality due to long disease latency and lack of reliable information of past asbestos exposure. However, other factors would seem to suggest that ARDs should not be invisible in Taiwan. The healthcare system is considered advanced and people's access to healthcare is guaranteed by the universal coverage of the national health insurance program. Furthermore, as discussed below, numerous clinical reports and epidemiologic studies have been conducted, making medical professionals in Taiwan aware of the clinical features of ARDs.
Nonetheless, the under-recognition of occupational diseases is common around the world. It is well understood that the establishment of administrative procedures for reporting and compensating occupational diseases is unavoidably a social process. 7 Whether an illness of a worker is recognized as work-related and given workers’ compensation (WC) is influenced by many policy and social factors, which include the design of WC and reporting systems, knowledge status and interpretation regarding disease causation of the general public, workers’ knowledge regarding their compensation rights, workers’ motivation and capacity to exert such requests, as well as the attitudes of major stakeholders toward WC.8–10
We conducted in-depth interviews with patients diagnosed with ARDs to investigate the reasons for the under-recognition of ARDs in Taiwan. This collaborative research project was initiated by academic researchers and carried out jointly with Taiwan Occupational Safety and Health Link (Taiwan OSH Link), which is an independent non-governmental organization founded in 2013 by volunteer activists and academic scholars. Taiwan OSH Link provides consultation and assistance to injured workers and their families and engages in research and policy advocacy to promote workers' safety and health rights.
Population Incidence Rates and Clinical and Epidemiologic Studies on MM
We first reviewed the incidence rates of MM and clinical and epidemiologic studies conducted in Taiwan, specifically on MM. Based on data from the Taiwan Cancer Registry, incidence rates of lung cancer in the general population have increased steadily from 1980 to 2018; during the same period, incidence rates of MM, although much lower, had increased substantially by five-fold (Table 1).
Number of Incidence Cases and Age-Standardized Incidence Rates of Lung Cancer and Malignant Mesothelioma in Taiwan, 1980–2018.
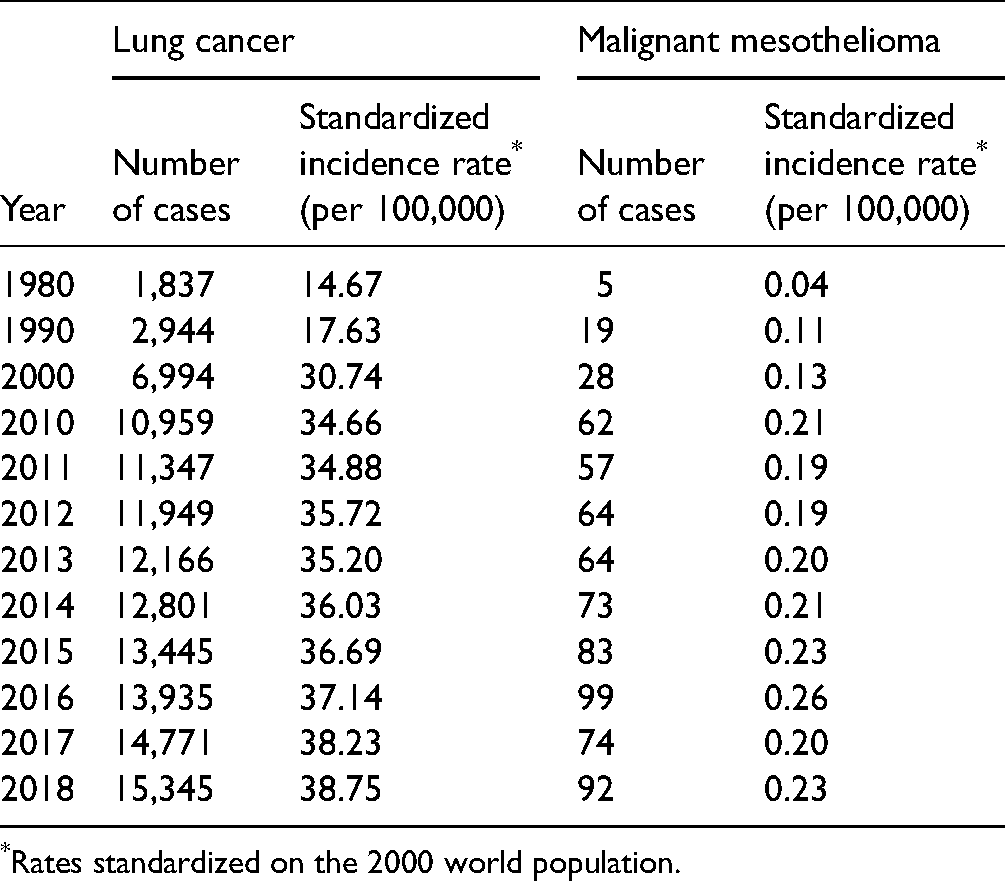
Rates standardized on the 2000 world population.
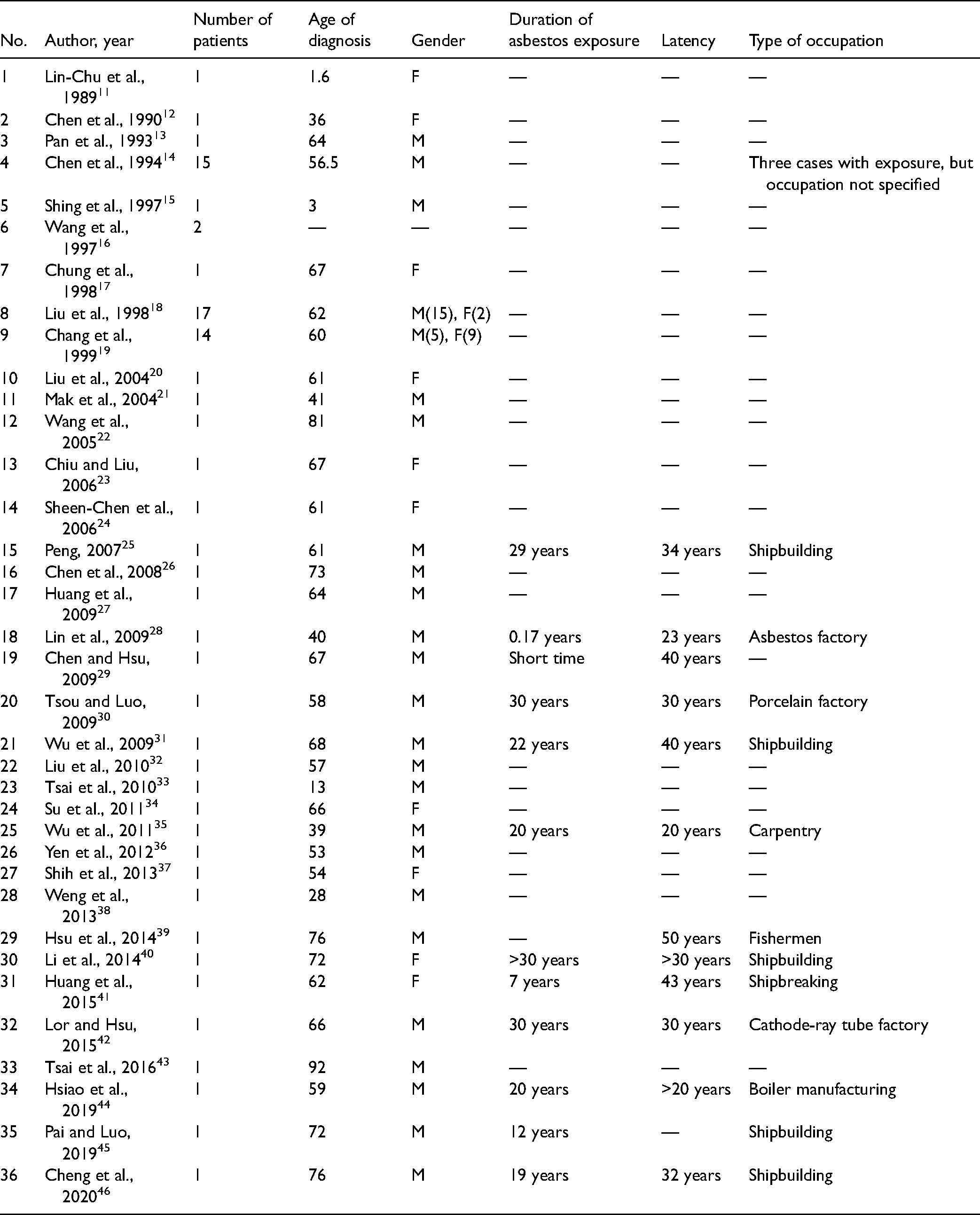
From 1989 to 2020, 36 clinical reports of MM were published (Table 2). We reviewed all these reports and identified 80 patients—57 males, 21 females, and two cases with gender not specified. Of these patients, 14 patients had a clear evident history of occupational exposure, and one patient had apparent environmental exposure to asbestos. Of the 14 patients with known sources of occupational asbestos exposure, six had worked in the shipbuilding or shipbreaking industries, and eight had worked in various manufacturing industries with substantial asbestos exposure. However, for the remaining 65 patients (81.3%), these studies focused on clinical features and did not address their asbestos exposure status.
Clinical Reports of Malignant Mesothelioma in Taiwan: 1989–2020.
From 2010 to 2019, eight epidemiologic studies were carried out to examine the associations between past exposure to asbestos and the incidence of MM (Table 3).
Epidemiologic Studies of MM in Taiwan: 2010–2020.
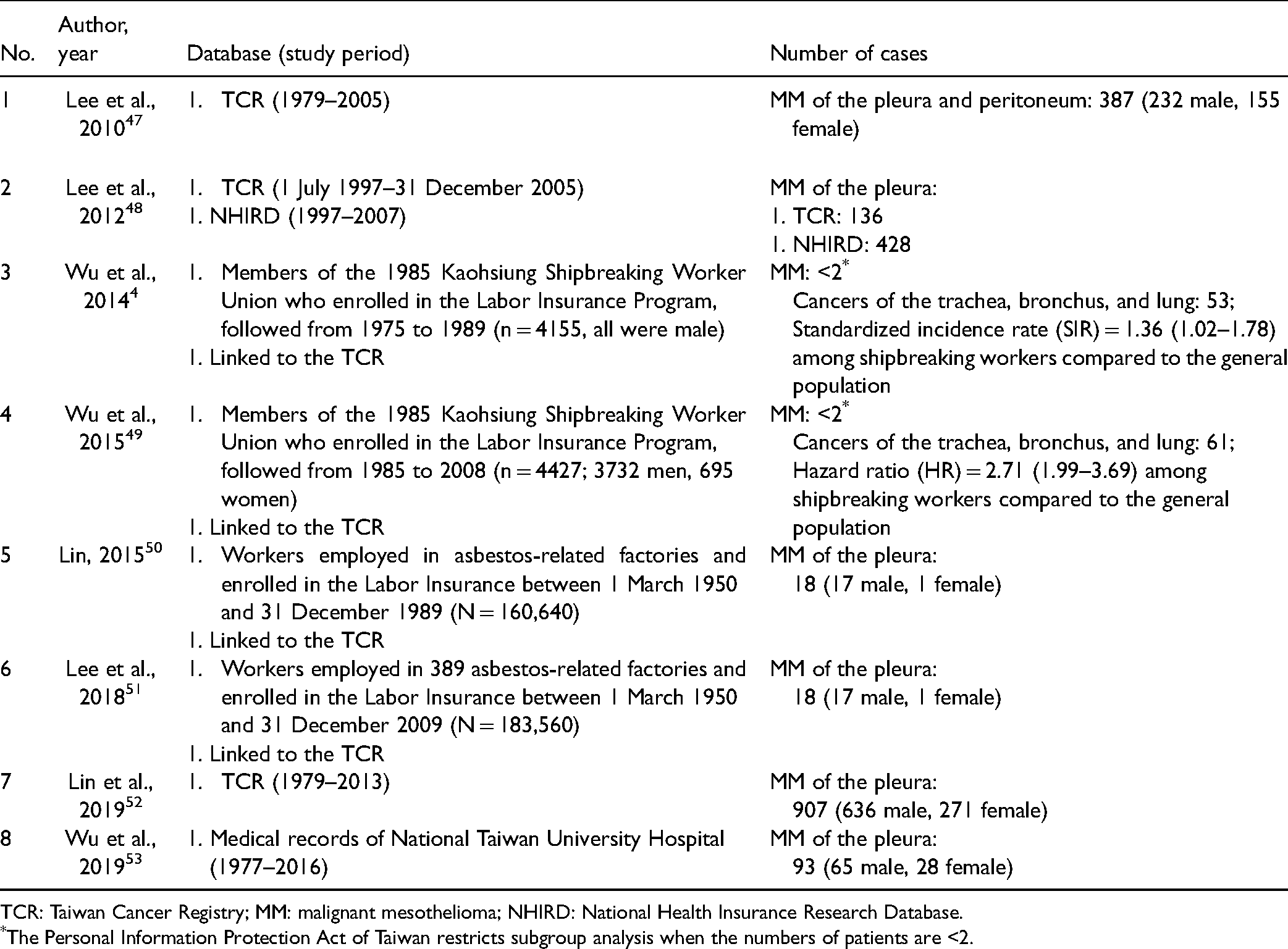
TCR: Taiwan Cancer Registry; MM: malignant mesothelioma; NHIRD: National Health Insurance Research Database.
The Personal Information Protection Act of Taiwan restricts subgroup analysis when the numbers of patients are <2.
Three studies (studies 1, 2, and 7 in Table 3) analyzed data of the general population. Of them, two studies by Lee et al.47,48 identified 387 cases of MM of the pleura and peritoneum from 1979 to 2005, and a study by Lin et al. 52 identified 907 MM of the pleura from 1979 to 2013. These studies also indicated that the incidence rates of MM of the pleura increased substantially during the studied period.
Four studies were conducted in specific working populations known for high asbestos exposure. The studies by Wu and colleagues4,50 found a significantly increased risk for neoplasms of the respiratory system in shipbreaking workers; however, the numbers of MM in their studies were too few for meaningful statistical analyses. Studies by Lin, Lee, and colleagues50,51 analyzed incidence rates of MM among factory workers of asbestos-related industries in different time frames and identified 18 cases of MM of the pleura (17 men and 1 woman) from 1980 to 2009.
In addition, one study 53 reviewed medical records of a single medical center and identified 93 patients (65 men and 28 women) with histologically confirmed MM of the pleura from 1977 to 2016.
In short, the literature review found no shortage of empirical evidence of MM occurrences in Taiwan. Reasons for the low compensation rate of MM and other ARDs are likely to go beyond diagnosis and healthcare issues.
Compensation of Occupational Diseases in Taiwan
At the time of writing this paper, regulations concerning the recognition and compensation of occupational diseases in Taiwan are stipulated in the Labor Insurance Act, which contains two categories of insurance – ordinary labor insurance (such as maternity benefits, sickness benefits, old-age benefits, etc.) and employment injury insurance. The latter provides four types of benefits – medical benefits, sickness (temporary disability) benefits, permanent disability benefits, and survivors’ benefits.
Despite that the Labor Insurance program had started to provide employment injury benefits in 1964, it was not until 1987 that statistics for compensation benefits of occupational disease became available. Yet, the types of occupational diseases were not distinguished until 1999. As shown in Figure 1, the number of occupational diseases rose sharply in the late 1990s. It was due to a series of protests mobilized by some labor organizers in this period. They demanded the government acknowledge the compensation rights of retired miners – many of whom suffered from pneumoconiosis. Under social pressure, the Bureau of Labor Insurance (BLI) relaxed the criteria for identifying occupational diseases after workers retire, resulting in a sharp increase in the cases of compensated occupational diseases. However, controversies surrounding malingering and financial deficits rose, prompting the BLI to tighten the criteria around 2001.
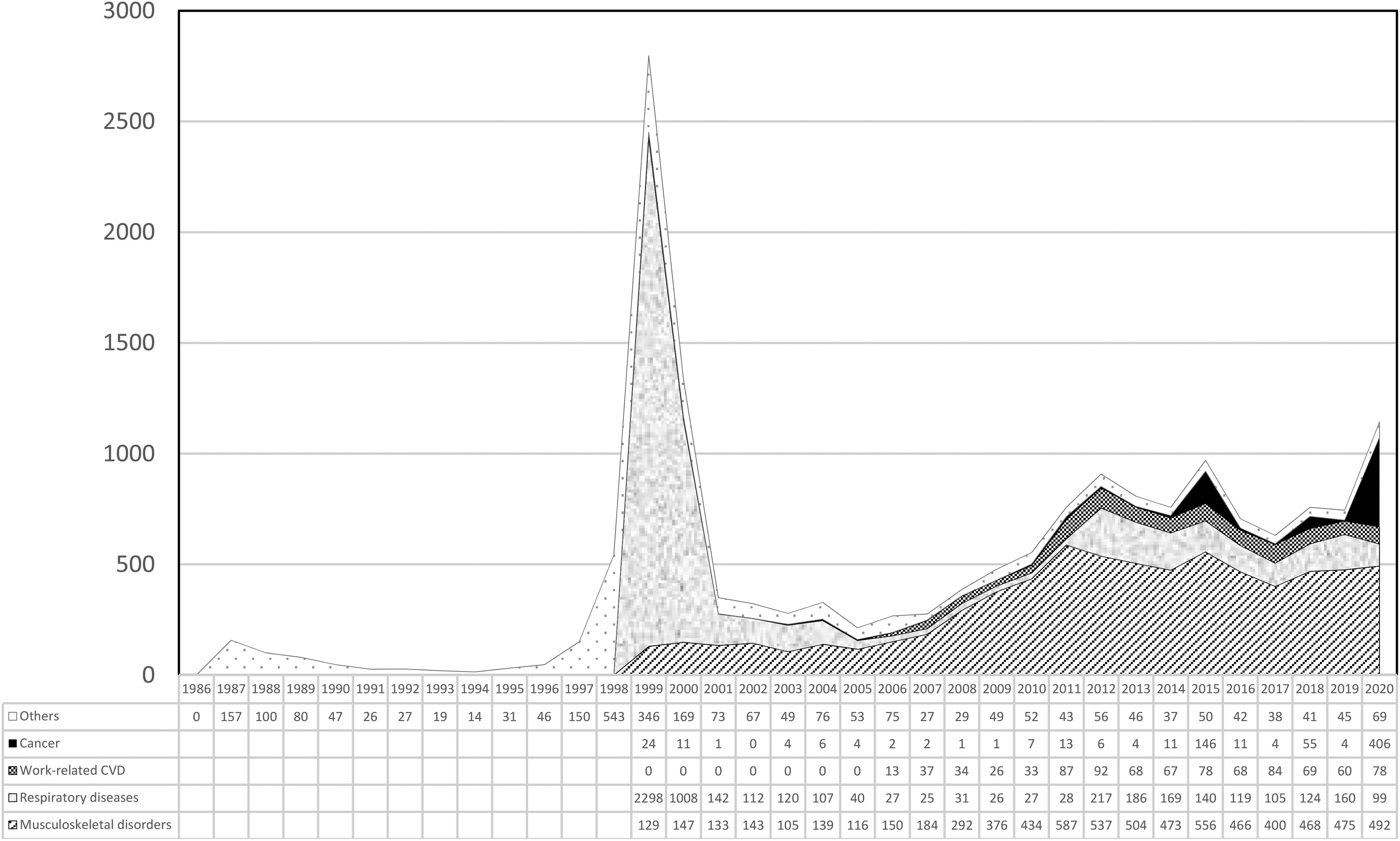
Numbers of compensated occupational diseases in Taiwan: 2001–2020.
After a low in 2005, the compensation rate for occupational diseases increased steadily from 2006 to 2012. This rising trend was attributed to many reforms initiated by Mr Huan-Ran Fuh, who was the director of the occupational safety and health division of the Council of Labor Affairs (later upgraded and restructured as the Ministry of Labor (MOL) in 2014) from 2006 to 2013. On the other hand, there were fluctuations in the compensation rates of occupational diseases from 2012 onwards. This was attributed to leadership changes in compensation affairs inside the labor authority.
From 2011 to 2020, on average, 818 cases of occupational diseases were compensated per year in a working population of approximately 11.9 million. The compensation rate was far below the levels of most of the developed countries. As seen in Figure 1, the predominant types of occupational diseases in Taiwan have been musculoskeletal disorders. In contrast, fewer than 10 cases of occupational cancer have been compensated per year. Except in 2015, 2018, and 2020, there were 146, 55, and 406 cases of occupational cancers, respectively.
The reason for these exceptional rises in the number of occupational cancers in these specific years was due to a long-lasting class-action lawsuit brought forward by workers against Radio Corporation of America (RCA) over multiple cancers allegedly caused by exposure to organic solvents, including trichloroethylene and tetrachloroethylene. These two chemicals are classified as known and probable human carcinogens by the International Agency of Research on Cancer, respectively. After years of litigation, the courts ruled in favor of diseased workers. The MOL followed court rulings and granted the diseased workers WC benefits in an exceptional manner. Accordingly, the BLI compensated 139 and 52 cancer cases in RCA workers in 2015 and 2018. Similarly, hundreds of RCA workers were compensated in 2020, following consecutive court rulings issued at the end of 2019 and in 2020; however, the exact number of compensated cases was not officially disclosed.
The WC insurance program developed on a non-fault principle constitutes one of the major social security systems. Yet, in Taiwan, this system has failed to ensure WC rights, forcing diseased workers to go through lengthy civil litigation based on the negligence principle before being recognized and compensated for as occupational diseases. Ironically, most of the occupational cancers compensated by the BLI were recognized only after long-fraught lawsuits.
Methods
For this study, eligible study participants were patients diagnosed with an ARD and who had a confirmed or highly suspected occupational history of asbestos exposure. Eligible patients were actively sought and invited to participate in this study through the assistance of physicians and case managers of the occupational medicine departments at two medical centers in Northern Taiwan. Upon agreement, researchers visited patients either at their wards, waiting rooms, or other open spaces of the hospitals. Before the interview, the purpose and contents of the interview were explained, and informed consent was obtained.
During the period from July 2014 to March 2017, 16 patients were interviewed (14 men and 2 women), including 10 patients with MM of the pleura, four patients with asbestos-related lung cancer, one patient with asbestosis, and one patient with cancers of multiple sites – the liver, lung, and breasts. All of these diagnoses were histologically confirmed. The age of disease onset ranged from 49 to 73 years old.
We used an interview outline with open-ended questions to guide the interview. The questions were grouped into four parts. In the first part, we asked participants to describe their work history, and then we asked specific questions regarding their experiences with dust exposure in the workplace. We also asked them if they were aware of the nature and health risks of dust exposure and whether they had used any personal protective equipment or other engineering measures to prevent dust exposure. In the second part, we asked the participants to describe how their symptoms appeared and progressed and how diagnoses were confirmed. In the third part, we explored how the participants explained the causalities of their diseases before being informed by their physicians; we also asked if they knew the link between asbestos and disease before the occurrence of the disease. In the fourth part, we asked the participants if they knew about the WC system; we checked their eligibility, and for those who were eligible, asked if they had or ever considered filing a claim; among those who had filed a claim, we asked about their experiences during the process. The study protocol and interview outline were approved by the research ethics committee of the National Taiwan University Hospital.
We were cautious about the limitations of patients’ self-reporting regarding asbestos exposure in the past. Because all of the study participants were referred from occupational medicine departments, before our interviews, they had gone through thorough investigation by occupational physicians or case managers in which specific questions about work-related activities were asked to improve self-reports. 54
Results
Table 4 summarizes the demographic characteristics, employment and occupational history, time of asbestos exposure, the status of labor insurance coverage, and the WC status of these patients.
Characteristics of the Study Participants (N = 16).
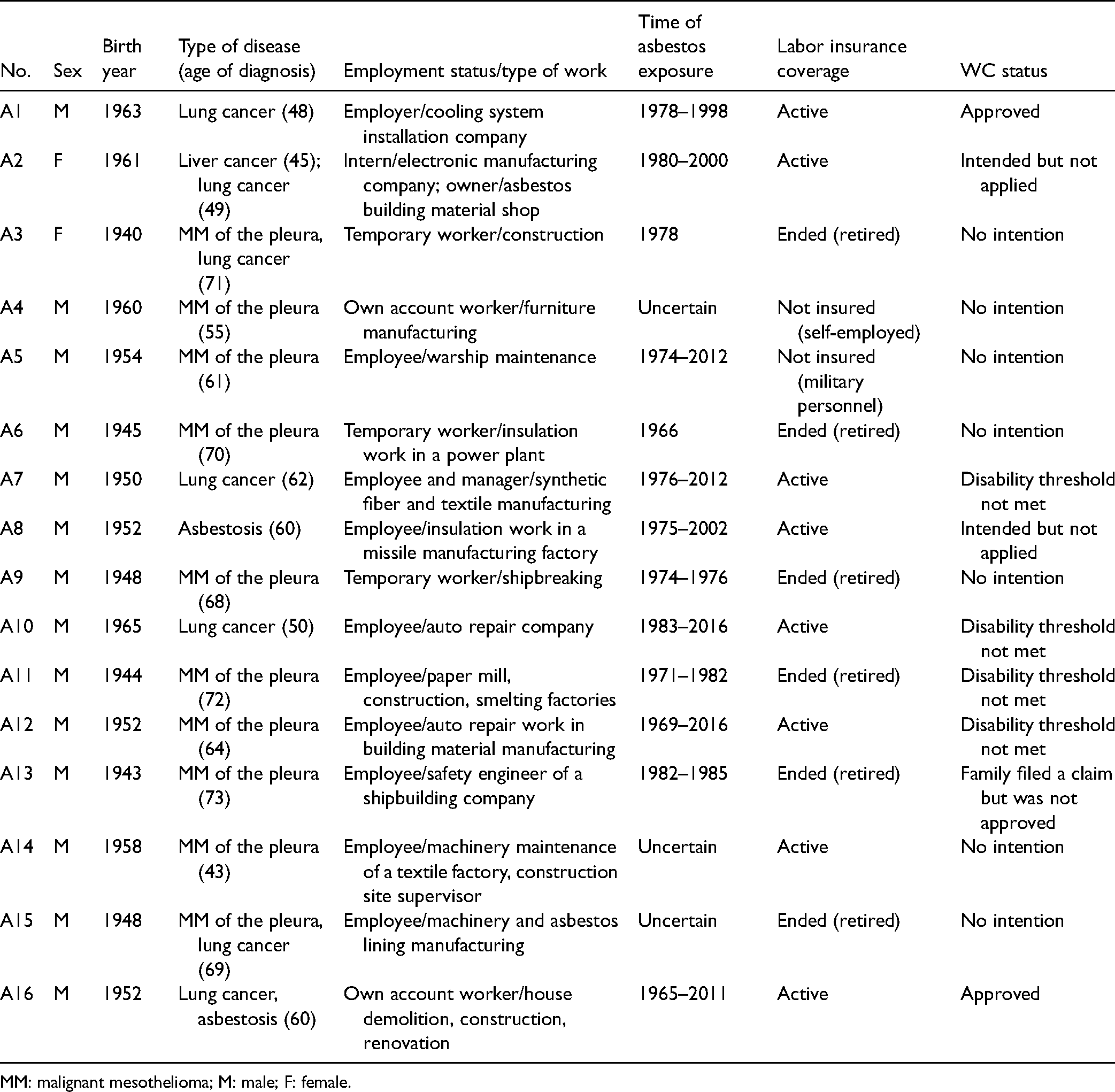
MM: malignant mesothelioma; M: male; F: female.
Work History and Past Exposure to Asbestos in the Workplace
All of these 16 patients recalled evident dust exposure in the workplace. Of them, 13 patients were certain that the dust contained asbestos. Their work types included shipbreaking, ship repairing, asbestos spraying in construction, and manufacturing and processing asbestos-containing products.
The other three patients (A4, A14, and A15), all diagnosed with MM, were not sure if the dust to which they had been exposed contained asbestos or not. These three were all self-employed workers – A4 worked in furniture manufacturing, A14 was a machinery maintenance worker of a textile factory and later became a supervisor of construction sites, and A15 worked in a manufacturing company of asbestos lining products.
Patients’ recalls may not be valid proof of past asbestos exposure, but it is evident that all these patients had worked in occupations known to have a high risk of asbestos exposure. In addition, the period of asbestos exposure for most of these patients fell in the 1970s and 1980s. The latency period from the first exposure to asbestos to the disease onset was as long as 30 to 40 years, consistent with epidemiological knowledge.
It is worth noting that some patients continued to have occupational asbestos exposure at the time of the interview. For example, A7 pointed out that thermal insulation materials in the textile factory he worked in still contained asbestos, and asbestos dust was evident during the dismantling and maintenance process. In addition, A10 mentioned that asbestos dust was still present during the auto repairing process, and asbestos-containing linings were dismantled and treated as general garbage without special care.
Discovery of Disease
Among the 16 patients, only A10 and A14 had their diseases diagnosed before symptoms appeared. A10 had a family history of lung cancer, and A14 was a hepatitis B virus carrier; both had participated in regular health check-ups on their own and had their diseases diagnosed at an early stage.
All the other participants sought medical care only after symptoms emerged. It is worth noting that A8, a worker of a missile manufacturing factory found to have asbestosis, had difficulty breathing for many years. However, he sought medical care only after two of his colleagues were diagnosed with ARDs, and one of them died of MM.
Knowledge of Carcinogenic Risk of Asbestos and Interpretation of Disease Causation
Before being diagnosed with ARDs and being informed by their physicians about the link of the disease to past asbestos exposure, all the patients except A8 (whose colleagues developed ARDs previously) were unaware of the health risk of asbestos and thus had never taken preventative measures. To our surprise, even A5, a maintenance worker of a warship, and A13, a safety engineer of a large shipbuilding company, admitted that they did not know of the carcinogenic risks of asbestos before they developed the disease.
Most patients and their families were reluctant to discuss their illnesses openly. Except for A8, these patients attributed their disease to a variety of factors, including environmental pollution (A6, A7, A10, and A14), smoking or exposure to second-hand smoking (A1, A9, and A12), poor bodily constitution (A7, A9, and A12), heredity (A10), exposure to other chemicals (A2), alcohol use (A1), and bad luck (A5 and A15). It is worth noticing that A15, a 69-year-old man, tellingly explained his illness by Buddhism concepts such as “Yeh-Zhang” (業障 or Karma) and “Inn-Guo Lun-Hui” (因果輪迴, or causal reincarnation). Such thoughts attribute misfortune experienced in current life to wrong-doing in a previous life.
Knowledge and Experiences Regarding WC
Even though all 16 patients were identified as having a highly suspected occupational ARD by occupational health physicians at the medical centers, only three patients (A1, A13, and A16) filed WC claims. Only two patients (A1 and A16) had their claims approved. These two patients shared the following features: being at work and actively insured at the time of diagnosis, engaging in the same occupation for a lifetime, having unequivocal evidence of asbestos exposure based on biological specimens, and being a non-smoker. They also had solid social support – mainly from their children – that helped them undergo lengthy compensation processes.
Patient A13 had not intended to file the claim, but his son still applied on his behalf. The BLI disapproved this claim on the ground that this patient had retired and thus had withdrawn from labor insurance at the time of disease diagnosis. The BLI decided that this case should not be compensated because the disease did not occur during the valid period of labor insurance.
The remaining 13 patients were not considered eligible by the BLI, based on the following reasons: patients were not covered by labor insurance; patients had retired and thus had withdrawn from labor insurance; patients could not provide solid evidence of past asbestos exposure; and, patients’ stage of disease did not reach the disability criteria for compensation. From our interviews, we noticed that all the patients considered the process of WC complex and difficult; none of these patients intended to fight against unreasonable restrictions imposed by the current regulations.
Discussion
We classified the reasons for the low recognition of ARDs into two categories based on qualitative analyses of interview data. One is related to the institutional barriers for recognizing occupational diseases. The other is related to non-institutional barriers, including knowledge about workplace risks and disease causation, attitudes toward the WC system, and the power relations between employers and employees in the workplace.
Since the initiation of this research project in 2014, the research team had published preliminary findings in various forms, including commentaries, reports, statements, academic publications, a documentary film in 2016, and later a whole book in 2017 (for further information in Chinese, please visit the website: https://oshlink.org.tw/about/issue/asbestos). Taiwan OSH Link also launched a series of campaign activities, demanding that the central government regulate asbestos-containing materials and reform WC systems. Through these campaign efforts and media reporting, social awareness about asbestos exposure and its health risks should have been substantially improved. For a more detailed description of these campaign activities up to 2017, please refer to a previous publication by Wu et al.. 5
Institutional Barriers to Recognizing Occupational Diseases
At the time of this writing (January 2022), regulations concerning the recognition and compensation of occupational diseases in Taiwan are stipulated in the Labor Insurance Act. Based on our findings, we summarized the institutional barriers contributing to the under-recognition of ARDs.
Insufficient coverage of the WC insurance. A sizable portion of workers is not mandatorily insured under the Labor Insurance Act. They include employees of small enterprises that hired fewer than five workers, employees of individual employers (i.e. employers without legal entities), workers without a stable employment contract, self-employed workers, and foreign domestic workers. Thus, asbestos-exposed workers belonging to these types – for instance, workers in small enterprises, temporarily hired, self-employed in the construction, demolition, decoration, and waste disposal work sites – would be excluded from the compulsory coverage of WC insurance.
Restriction on eligibility and rigid criteria for disability assessment. According to Article 20 of the Labor Insurance Act, insured workers remain entitled to all types of WC benefits within one year after the insurance contract has been ended. According to Article 20-1 of the Labor Insurance Act, workers who develop occupational diseases during the valid period of the insurance may claim WC benefits, but only permanent disability benefits. In other words, no medical benefits, sickness benefits, or death benefits are available for workers who develop occupational diseases after retirement. Furthermore, according to an administrative order issued by the BLI, permanent disability benefits can only be provided after a disease status becomes stable and a disability assessment can be performed. A waiting period of two years of medical treatment for a general disease/injury, or six months for an organ-related disease, is required before the disease status can be considered stable and permanent.
We argued that these regulations pose unreasonable restrictions to recognizing MM and other types of ARDs as occupational diseases for the following reasons. First, MM usually develops many years after retirement. Secondly, only permanent disability benefits are available, but a stable condition can hardly be achieved to evaluate disability status because MM is fatal and usually advances quickly.
After being criticized, the MOL amended the regulations on 29 July 2016, allowing workers diagnosed with MM with a stage of III or above to have their disability status evaluated right after diagnosis. However, even with this revision, in practice, the rapidly advancing disease conditions of MM still make the assessment of disability difficult.
From the experiences of the cases assisted by the Taiwan OSH Link, we found many patients died before they could complete the disability assessment. Thus these cases were not recognized, and their spouses or dependents lost the right to claim compensation benefits.
Rigid criteria of exposure evidence. For a disease to be deemed work-related, workers must provide indisputable evidence of occupational exposure, whether past or current. For ARDs, asbestos fibers detected in a sample of dust collected at the worksite or in a biological specimen constitute valid evidence, but having an occupational history itself is not sufficient proof of exposure. In addition, proof of not having other sources of exposure is considered a prerequisite. In other words, once asbestos exposure was present in the living environment, the claim would be denied on the ground that non-occupational exposure cannot be ruled out. Thus, for workers with both occupational and non-occupational exposure to asbestos, this restriction becomes an obstacle to recognizing the occupational disease.
The MOL had relaxed the restrictions on the proof of dust exposure on 16 March 2016, so miners who developed pneumoconiosis could use their occupational history as proof of exposure. However, workers in other industries still have to provide solid evidence of exposure for WC.
Perceived difficulties in the claiming process. Due to the complicated regulatory designs of WC systems, perceived difficulties in the claiming process also contributed to workers’ lack of motivation to file a compensation claim. In our study, many MM patients were too ill and too preoccupied with medical treatment and thus had no interest in seeking compensation benefits.
Moreover, in Taiwan, because of the relatively easy access to health care services and relatively low co-payments under the universal National Health Insurance, diseased workers generally have little motivation to claim medical benefits under the WC.
Dysfunction of occupational health examination. The Occupational Safety and Health Act stipulates that employers should implement special occupational health examinations for their employees in operations considered particularly hazardous to health, with asbestos operations listed as one of such types. However, occupational health examinations have not been effectively implemented. Virtually, no ARD had ever been recognized and compensated through this stipulated mechanism. Furthermore, there is no post-exposure occupational health examination for workers who retired or left hazardous employment.55,56
Non-Institutional Barriers to Recognizing Occupational Diseases
Our findings also indicated that some non-institutional barriers contribute to the low recognition of occupational diseases. We summarized these barriers as follows.
Insufficient causal knowledge regarding occupational diseases. Most interviewees did not know of the health risks of asbestos exposure. At the time of diagnosis, few had ever suspected that their diseases might link to past exposure to asbestos. Even after being informed by physicians and case managers, many patients still attribute their illnesses to non-occupational factors. Previous studies have identified cultural beliefs that impact worker attitudes toward injuries. For instance, a qualitative study of injured workers in Hong Kong 57 reported fatalistic views toward workplace injuries, with workers explaining their misfortune by supernatural forces such as fate and bad luck. In a qualitative study of Taiwanese workers, 58 some workers believed that good health was a reward for good deeds while an illness was a punishment for wrong-doing in a previous life. In our study, some patients held similar fatalist thoughts. Such thinking is likely due to insufficient knowledge on ARDs, but may also serve as a coping strategy for patients to balance themselves between the suffering of the disease and the situations they could not comprehend.
Insufficient knowledge and awareness regarding WC rights. In our study, most of the patients were not familiar with the WC system. The concept that occupational disease should be preventable and someone other than workers themselves should be held responsible for its occurrence does not seem widely held. Instead, it is still commonly perceived that occupational health risks are unavoidable costs of work. Insufficient knowledge regarding compensation rights may result from a lack of education and information regarding ARDs, occupational disease in general, and the WC system. Moreover, lack of labor rights awareness might be related to self-employment status because conventionally, self-employed workers are considered responsible for their own safety and health risks.
During the recruiting of study participants, we noticed that some patients held a negative view of WC claims. Several patients refused to participate because they did not want to be classified as “labor” – this noun has derogatory meaning in the Chinese context. In addition, some participants raised concerns about being potentially labeled as “potential profiteers” (A6 and A13), and some participants reported uneasy feelings of being rigorously scrutinized in the claiming process (A1, A2, A13, and A16).
Stigmatizing attitudes toward WC and welfare benefits have been studied elsewhere.59–63 For instance, Kirsh and colleagues documented experiences of stigmatization in injured workers in the process of WC, which was reinforced through individual-level interactions and internalized by injured workers. 61 How the concept of compensation rights for occupational injuries and diseases has formed and changed over time and how social and cultural factors might modify workers’ perception toward WC deserves further investigation.
Concerns about negative consequences after seeking compensation. Patients who were still employed or had families working in the same companies were concerned that filing a WC claim might annoy their employers and harm their employment continuity and related benefits. The fact that concerns of job loss might hinder the reporting of occupational diseases had also been reported in previous studies. 64
Advocacy for Policy Reform and the new Legislation in 2021
Since 2015, the Taiwan OSH Link has assisted several workers who had been diagnosed with MM and had a clear history of occupational asbestos exposure. These workers or their families contacted us for assistance to earn the recognition of occupational diseases. However, significant institutional barriers were noticed. For instance, workers in civil and military sectors were not covered by the Labor Insurance Act, thus were not eligible for WC benefits. In Taiwan, although civil servants and military personnel who died or were severely injured in the line of duty were entitled to solatium awards (emotional harm), there were no regulations for the recognition and compensation of occupational diseases. Furthermore, some private-sector workers were not compulsorily covered by the Labor Insurance Act, including those hired by small enterprises and individual employers and self-account workers. In our study, several workers were determined not qualified by the BLI because they developed diseases many years after retirement, and diseases advanced so fast that disability assessment was not possible.
The “Labor Occupational Accident Insurance and Protection Act,” passed on 23 April 2021 and deemed to go into enforcement on 1 May 2022, brought together compensation, prevention, and rehabilitation matters into a single law. This legislation has been a milestone in the development of occupational health systems in Taiwan. Major reforms concerning the recognition problems of occupational diseases, specifically ARDs, include the following.
Coverage of WC insurance expanded. The new legislation extends the coverage of WC insurance from employees of enterprises of five workers or more to all legally hired workers. Employers with legal entities are obliged to sign their employees up for occupational accident insurance on their first day at work, regardless of the size of the company. According to the new Act, patients A3, A6, and A9 would have been covered by WC insurance during their employment as temporary workers. However, according to Article 27 of the new Act, patients have to prove that they suffered the diseases during the existence of the insurance coverage period or within one year after the insurance contract has ended. These regulations still pose an unreasonable restriction to workers who suffer occupational diseases with a long disease latency. Furthermore, workers hired by individual workers and self-employed workers are still not mandatorily insured, and workers in the civil and military sectors are still excluded from the WC coverage.
Scope and levels of compensation benefits expanded. The new Act increased the levels and expanded the scope of compensation benefits. In addition, workers who developed occupational disease after retirement are entitled to the full range of compensation benefits, not just restricted to disability benefits. However, as mentioned previously, the one-year limit is imposed, meaning that diseased workers can only seek compensation benefits within one year after the termination of insurance coverage.
Post-exposure health examination system established. The occupational health examination is modified to include a post-exposure health examination system among those with a history of prior employment in hazardous occupations. Once occupational physicians ascertain that the disease was caused by work exposure during the period of insurance, workers are entitled to medical benefits, disability benefits, and survival benefits, regardless of their current employment or retirement status. By this reform, more cases of ARDs should be detected at an earlier stage. However, it remains controversial with regard to identifying the groups eligible for the post-exposure health examination and determining the work-relatedness of the disease.
ARDs in the Military
In early 2020, a retired Navy soldier, who was diagnosed with MM in 2016, and his family contacted the Taiwan OSH Link for help. This 69-year-old man, who died a few months later, was the first asbestos-related occupational disease from the military actively seeking compensation. This case was publicized by the Taiwan OSH Link and quickly attracted public attention. In response to an inquiry of the Legislation Yuan (the Congress), the Ministry of National Defense promised in November 2020 to initiate some measures to improve the recognition of ARDs among military personnel. These include to study the compensation policies of the U.S. military, to analyze medical records of military personnel, to examine the occurrence and trends of MM over the last three years, and to evaluate the feasibility of amending the Indemnities Act for Military Personnel and Act of Insurance for Military Personnel. However, these issues have not been a priority issue for the Ministry of National Defense.
Conclusion
Under-recognition of occupational diseases is common in many countries.9,65
The findings of this study indicated that institutional and non-institutional barriers explained the low recognition of ARDs in particular and occupational diseases in general, especially for diseases with a long latency period and multiple causalities.
In Taiwan, cancer has been the top cause of death since 1982. In 2020 alone, there were 50,161 cancer deaths, accounting for 29% of total deaths. However, except for the cancer patients of the RCA litigation, occupational cancers have rarely been recognized in the WC insurance system. Because asbestos is one of the most recognized workplace carcinogens, we argue that reform efforts on the WC system should prioritize asbestos-related cancers. However, such reforms should expand to other types of occupational cancers and occupational diseases.
The reforms in 2021 brought compensation and prevention into a single new law, expanded the compensation coverage to retired workers with occupational diseases diagnosed after retirement, and promised to set up post-exposure follow-up health examination programs. All these efforts might allow more occupational diseases to be recognized. Yet, whether or not the new Act could be effectively implemented for the recognition of ARDs, especially MM, remains questionable. It should be emphasized that since preventive efforts were not adequate in the past, special provisions should be made for the presumption of workplace exposure in the compensation of ARDs.
Nevertheless, institutional barriers only partially explain the reasons for the invisibility of ARDs. In other words, the role of non-institutional barriers should be considered, which include knowledge status, perceptions, and attitudes of both workers and the general public regarding workplace health risks and WC rights. The advocacy work promoted by the Taiwan OSH Link in the past few years has helped increase the visibility of ARDs. Yet, more efforts are needed to improve workers’ knowledge regarding the WC rights and facilitate the processes of fulfilling these rights.
Footnotes
Acknowledgments
The authors thank Ms Fan-Ju Hsiao and Dr Pei-Hua Chuang for their assistance in conducting the interviews and Prof. Jung-Der Wang for his encouragement and guidance at the initial stage of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan (grant numbers 104-2410-H-002-231-MY2 and 106-2410-H-002-171-MY3).