
Abstract
Outdoor workers are exposed to many hazards, including solar ultraviolet radiation (UVR). Identifying, reporting, analyzing and tracking the exposures or health outcomes of outdoor workers have not generally been formally considered. This article aims to summarize the best practices/strategies for creating an occupational sun exposure or skin cancer surveillance system for outdoor workers and to understand the key barriers and facilitators to the development of such a system. For the design of a successful occupational safety and health (OSH) surveillance system five occupational surveillance strategies are summarized: exposure registry, disease registry, disease screening/medical surveillance, sentinel event surveillance, and disease surveillance via data linkage. Ten key considerations are identified, including identifying a clear goal, a defined target population and stakeholder involvement, five critical barriers are highlighted including underreporting and funding, and five vital facilitators are recognized including communication/collaboration and a simple reporting process.
Introduction
Outdoor workers are exposed to numerous workplace hazards. One of the most important is solar ultraviolet radiation (UVR). It has been underestimated if not neglected as an occupational hazard. 1 In 1992, the International Agency for Research on Cancer (IARC) deemed solar radiation as carcinogenic to humans (group 1) 2 and in 2012 confirmed this classification. 3 Keratinocyte carcinoma (KC, also known as non-melanoma skin cancer) is one of the most commonly diagnosed cancers in the world, 4 especially in fair-skinned people. 5 Its primary cause is solar UVR. 6 KC includes both Basal cell carcinoma (BCC) and Squamous cell carcinoma (SCC). Typical signs and symptoms can include sores that do not heal, rough or scaly red patches, a sore that bleeds and/or a growth or area that is itchy. 7 Some studies in the last decade have provided some estimates of SCC incidences in both Canada and the United States, as well as some estimated survival data for SCC and BCC in the United States and in the state of New Hampshire. Applying statistical modeling to data obtained from epidemiologic studies published between 1960 and 2006, Abbas and Kalia estimated that in New Brunswick, SCC was responsible for 26% of KC, while in Alberta, Manitoba and British Columbia the SCC percentages were 24%, 21%, and 20%, respectively. 8
Karia and colleagues applied linear regression to published data in order to estimate the incidence of SCC and of subsequent nodal metastases and death among white people in the United States in the year 2012.a They found a statistically significant increase in SCC over time, which they attributed to an increase in cumulative exposure to UV radiation and to an aging population. They reported an average risk of nodal metastasis of 3.0% and an SCC-specific death risk of 2.1%. They estimated that the number of white people in the United States diagnosed with SCC in 2012 was between 186,157 and 419,843 and the number who died of SCC was between 3932 and 8791.9–11 A case control study, nested in a retrospective cohort study, compared residents of the U.S. state of New Hampshire, who had survived SCC or BCC and who were never previously diagnosed with non-skin cancer, with matched controls. It found that SCC survivors had a marginally higher mortality risk than matched controls (Hazard Ratio: 1.25, 95% CI: 1.01–1.54). In contrast, there was no significant difference in survival between BCC survivors and matched controls (Hazard Ratio: 0.96; 95% CI 0.77–1.19). 10 However, in rare cases, such as one reported in the Archives of Dermatology in 2003, BCC can metastasize and lead to death. 12
Due to severely limited reporting of KC to cancer registries, its exact incidence is not known, but many countries regard it as presenting a significant health burden. Rogers and colleagues estimated the incidence of KC in the U.S. population by mathematical modeling using data from Medicare claims, the National Ambulatory Medical Care Survey and the Census. They calculated the total number of KC procedures performed for Medicare fee-for-service patients over 65 in 2012 at 2.09 million. This population is approximately 63% of U.S. residents over 65. Hence, they estimated the total number of procedures performed for U.S. residents over 65 at 3.3 million. This number represents approximately 61% of all medical visits in the U.S. involving a procedure for KC. Hence they estimated the total number of KC visits in the U.S. in 2012 at approximately 5.4 million. They used the 5.4 million figure as a surrogate for incident cases of KC in the U.S. in 2012. In 2012, in the Medicare fee-for-service population, the average number of procedures per KC patient was 1.64. Applying for this number, they estimated that the total number of people in the United States treated for KC in 2012 was approximately 3.3 million. 13 Given this potentially high burden on humans and health systems, KC may be a disease of particular interest to policy makers. A surveillance system could support the development of prevention policies.
There is a large body of research linking solar UVR exposure in outdoor workers to the increasing incidence of KC.14, 15 In various countries and regions, exposure measurements (using personal dosimeters) of outdoor workers show high exposures to solar UVR compared with the general public. 14 Outdoor workers have up to 3.5 times greater risk of developing skin cancer than indoor workers. 16 For this reason, it is important to monitor UVR exposure and KC incidence in outdoor workers. Monitoring may increase the implementation of proper primary prevention strategies (e.g., engineering controls, including the provision of shade; administrative controls, including scheduling of tasks at low UV times of the day; education of workers and employers; and the provision of personal protection such as hats, long clothing, eye protection and sunscreen). These primary prevention strategies can reduce the risk of developing KC. Surveillance can increase early diagnosis and treatment. An occupational safety and health (OSH) surveillance program that focuses on outdoor workers and KC or UVR exposure could help to identify which outdoor occupations are at greatest risk, to identify which geographic areas are at greatest risk, and to obtain a better idea of how many outdoor workers are affected by KC. Ultimately the resulting information can help policymakers to determine which industries and geographic regions to focus on, identify higher risk workers, and to estimate the number of workers affected. This can lead to the development and implementation of early intervention and prevention programs.
Surveillance is defined by the Centers for Disease Control and Prevention (CDC) as “the ongoing, systematic collection, analysis, and interpretation of health data, essential to the planning, implementation and evaluation of public health practice, closely integrated with the dissemination of these data to those who need to know.” 17 The purpose of a surveillance system for OSH is to provide “the data and analyses needed to understand the relationships between work and injuries and illnesses in order to improve worker safety and health and prevent work-related injuries and illnesses.” 18 Surveillance systems are designed to be ongoing and to track changes over time. Typically surveillance includes planning and designing the system, collecting the data, organizing and managing the data, analyzing the data, interpreting the results, and communicating the information to the groups of people who need to know. 19 The final task of a surveillance system is to guide policy or to implement interventions or prevention programs. 18
A surveillance system focuses on either disease (health outcomes) or exposure. Occupational disease (OD) surveillance involves “the systematic monitoring of health events in working populations in order to prevent and control occupational hazards and their associated diseases and injuries.” 20 Occupational exposure or hazard surveillance recognizes, collects and assesses information about work processes or workers exposed to a high level of exposure or risk in particular industries or job categories. 21
In Canada, OSH is a responsibility of the provinces and territories. Hence, OSH surveillance is typically done by provinces or territories, which design their own programs to accomplish specific objectives. 22 As a result, there is no national all-encompassing OSH surveillance system or systematic process for surveillance. In North America, most surveillance focuses on disease or health outcomes rather than hazards and/or exposures. 18 Most OSH surveillance programs in Canada focus on work-related injuries rather than occupational illnesses or diseases. Recently, however, Ontario has developed an occupational disease surveillance system (ODSS) with the goal of identifying and monitoring trends in OD in Ontario. 23
Materials and Methods
Our study included a traditional literature review 24 and semi-structured key informant interviews to summarize the best practices for creating an occupational sun exposure or skin cancer surveillance system for outdoor workers, and to understand the key barriers and facilitators to the development of such systems.
Literature Review
A traditional literature review 24 of both scientific and gray literature was conducted in order to determine whether OSH surveillance has been conducted for outdoor workers previously and to identify the key planning components for structuring this type of OSH surveillance program. The review was conducted using PubMed, Web of Science, Medline, Scopus and Google Scholar between April 30 and May 7, 2019. No restrictions were placed on country or publication date. Languages were restricted to English, Dutch and German. The search strategy combined the following four concepts: OD and health surveillance and outdoor workers; OD or exposure and outdoor workers; OD and health surveillance and outdoor workers/solar UVR; best practices for OD and health surveillance. The results of the literature search were saved in an EndNote database.
After reviewing the searched literature, it became clear that no literature exists that focuses specifically on OSH surveillance systems for outdoor workers. To obtain a better understanding of OSH surveillance systems it was necessary to look beyond outdoor workers and to include surveillance systems that focus on various ODs or exposures that workers may experience. The search terms were expanded to include OD surveillance, occupational health surveillance, and exposure registry. Articles or reports that 1) describe an OSH surveillance system and include guidelines or a description of its design and/or function, 2) describe some of the strengths and limitations of the surveillance system, or 3) look at the inclusion of KC as an OD were consulted further. The included articles/reports were entered into a Table of Surveillance Practices (Appendix A).
Key Informant Interviews
Key informant interviews were conducted between August 2019 and January 2020 to gain a better understanding of best practices for the design and implementation of an OSH surveillance system and of the barriers and facilitators to creating, managing, and ensuring its ongoing success. Key informants were chosen for invitation based on the following criteria:
Canadian representation, with emphasis on jurisdictions that have experience designing or implementing occupational surveillance systems and/or expertise in skin cancer prevention International perspective, with emphasis on jurisdictions that have strong experience designing or implementing occupational surveillance systems and/or expertise in skin cancer prevention Inclusion of a broad spectrum of stakeholders (i.e., regulators, researchers, and physicians)
All of the interviewees received written information about the study objectives and a copy of the interview questionnaire. They all provided written informed consent prior to the interview. The interview component of the study received ethical approval from the Cancer Committee of the Health Research Ethics Board of Alberta (certificate #18-0615).
Interviews were semi-structured and open ended and included the following key questions (Appendix B):
What are the key considerations for developing and implementing an effective OSH surveillance program? What are the perceived barriers to developing and implementing an effective OSH surveillance program? What are the perceived facilitators to developing and implementing an effective OSH surveillance program?
The audio-recorded interviews were transcribed verbatim using Otter.ai and then double-checked for quality by listening to the audio recording and comparing it to the transcription. The transcriptions were analyzed using qualitative content analysis
25
using the software NVivo 12. We followed a conventional content analysis approach since the main aim of the interviews was to describe the informants’ views and experiences related to surveillance.
26
After familiarization with the interview content, categories or common themes were inductively identified for each topic and each interview was analyzed with these themes in mind.
Results
Literature Review
We did not locate any evidence for the existence of any OSH surveillance systems focused solely on outdoor workers. Some countries have developed OSH surveillance systems that include KC and/or skin diseases (e.g., EPIDERM, in the United Kingdom. See Table 1), but this is rare. In systems where skin diseases were included, incidence of disease or contributing exposures are not reported regularly.15, 27–31
Surveillance strategies (exposure registry, disease registry, and disease screening/medical surveillance).
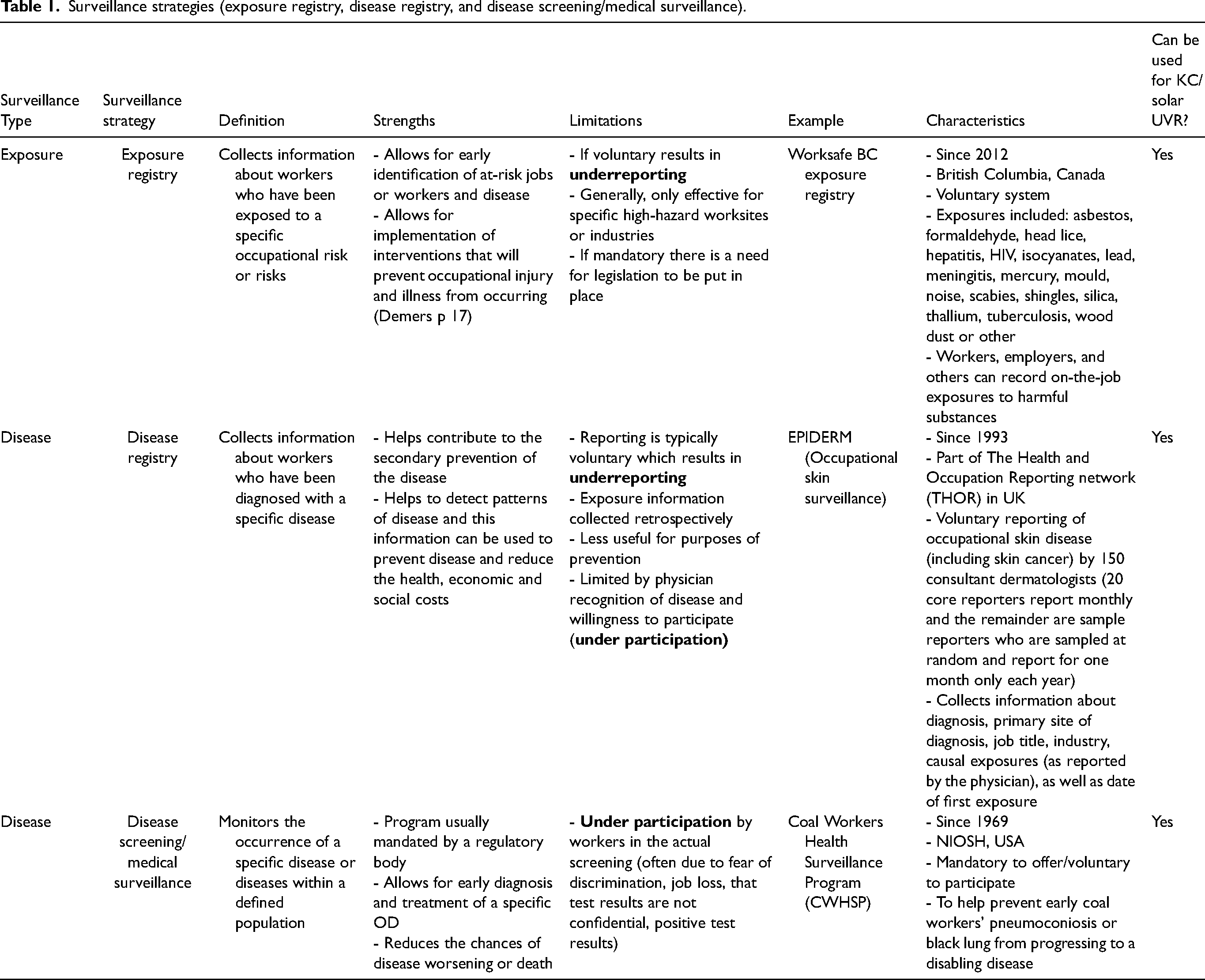
To obtain a better understanding of OSH surveillance systems, five main surveillance strategies (exposure registry, disease registry, disease screening/medical surveillance, sentinel event surveillance and disease surveillance via data linkage) were identified and summarized. These five surveillance strategies were most prevalent in the literature we reviewed and, therefore, were examined further. Most of these strategies could potentially be used for designing an OSH surveillance system for outdoor workers or more specifically for KC cases or UVR exposure.
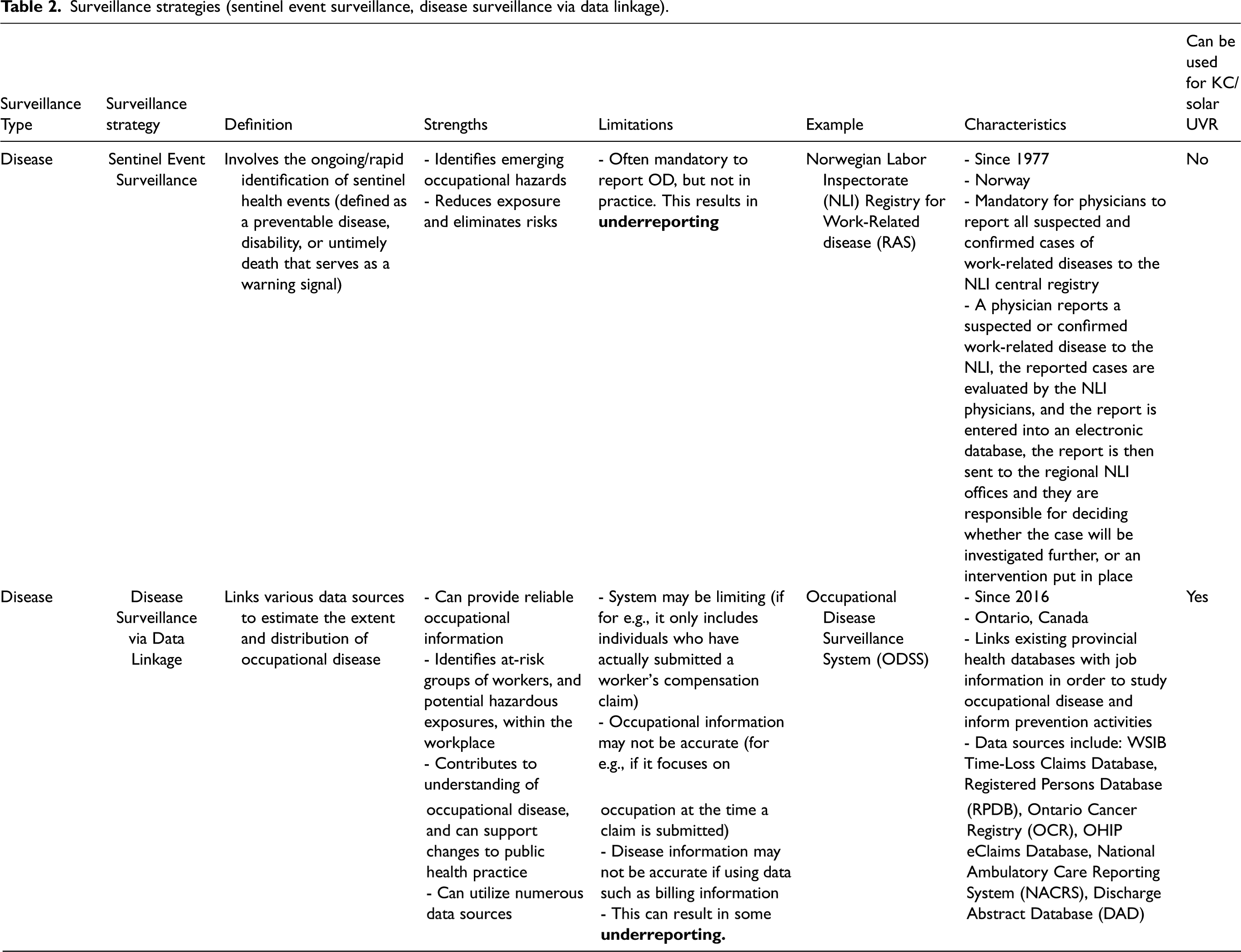
Table 1 (exposure registry,32–34 disease registry,32,35–38 disease screening39–42) and Table 2 (sentinel event surveillance,32, 43, 44 disease surveillance via data linkage22, 33, 45, 46) present the five surveillance strategies with a short definition, strengths, limitations, a current example, characteristics, and whether the strategy could be applicable to KC or solar UVR. Each strategy has strengths and limitations and cannot perfectly accomplish all surveillance goals, which is a key finding. The common limitation among the five strategies is the underreporting of OD or the under-participation of health care providers and/or workers in the surveillance program. Minimizing underreporting and under-participation to the extent possible is a factor that needs to be considered when designing an OSH surveillance program.
Surveillance strategies (sentinel event surveillance, disease surveillance via data linkage).
Key Informant Interviews
We expected to reach data saturation at approximately 20 interviews. 47 Hence, we sent email invitations to 46 potential key informants, anticipating some refusals or non-responders. We received 22 positive responses (response rate of 48%), of which 11 were from Canada and 11 were from other countries. Thirteen of the interviewees had direct experience with OSH surveillance systems and 9 had specific experience with skin cancer prevention programs or involvement with research in this area. The interviews ranged from 35 to 60 min and were conducted via telephone or video by a study team member (NS).
Key informants were from Canada (Alberta, British Columbia, Ontario, Saskatchewan, and Nova Scotia), Europe (the Netherlands, Norway, Italy, and Germany), the United Kingdom, Australia, and the United States.
Germany
During the key informant interviews, it became clear that Germany stands out when it comes to the surveillance of KC and sun exposure. The system in Germany includes a mechanism to track the cases of KC in outdoor workers. It includes a medical screening component for outdoor workers, and it integrates primary prevention strategies and education.
Themes Regarding the Design of OSH Surveillance Systems
Our qualitative content analysis of the interviews identified ten elements that should be included in the design of an OSH surveillance program for outdoor workers:
Have a clear purpose and goal(s) for any new OSH surveillance system. The questions that are to be answered or the problem that requires solving should be clear and well-articulated. For the surveillance of KC or UVR the purpose is to identify workers and/or geographic regions at greatest risk and to provide evidence for cancer prevention programs and workers compensation systems. This would be done by tracking workers either diagnosed with KC or exposed to UVR. Have a defined target population. It can be broad or narrow depending on the directly stated purpose, but inclusion in the program should be well-defined. The target population for the surveillance of KC or UVR is outdoor workers. Involve key stakeholders throughout the process. A hallmark of a successful OSH surveillance system is the identification of the correct stakeholders and their involvement at all stages of program development, implementation, and evaluation. The key informants also provided examples of the kinds of stakeholders that could be important, depending on the program: occupational health and safety professionals, labor representatives, academics and scientists, data managers, employers, and regulators. The specific stakeholders for KC or UVR surveillance can include labor unions, named below in the discussion section, and industry representatives from construction and agriculture, scientific experts on outdoor work, dermatologists, occupational hygienists, occupational physicians and workers’ compensation leaders. Distinguish between exposure and disease surveillance programs. The planning should directly address which type of surveillance is being undertaken, and if both exposure and disease will be included, then careful consideration of both should be done. To this point, there was a general consensus that a good place to start would be the surveillance of KC (non-melanoma skin cancer) as an OD. Evaluate the available resources. This will ensure that the OSH surveillance system is appropriately scaled to the resources involved. There was a strong sense that planning for a minimum of 10 years of solid funding is important to ensure the success of an OSH surveillance program. Assess the data sources that are needed and available and plan for how to analyze the data. Consideration should be given to how data will be collected, what the data capture process entails, and how it would be analyzed. For example, it would be important to develop a system for reporting KC to the various cancer registries. The next challenge would be linking these cases to occupation. Physician billing data could also be improved to include more specifics on the type of KC diagnosed and perhaps whether there is an occupational link. Include a pilot phase. This would be a useful tactic to determine how the system works, to allow the identification of any flaws, or to flag other areas of concern that could be improved before scale-up. Include an evaluation of the program. This is key in the implementation of the program. There was a concern that some OSH surveillance systems are never formally evaluated and therefore not being used to their highest potential. Disseminate results. This is also linked to the implementation of the program. Dissemination is a critical step to share learnings and can inform the development of new and improved prevention programs, interventions, or policies. Utilize the OSH surveillance system to improve the health of workers via the development of new products, programs, or policies to reduce hazardous exposures. In the case of KC, these would be interventions to protect workers from UVR targeted to workers and/or geographic regions at greatest risk as identified by the surveillance system. These are discussed in more detail below in the section entitled “policy considerations.”
Barriers and Facilitators
Table 3 indicates the top five barriers to developing and implementing an OSH surveillance system which emerged from the interviews. Thirteen of the key informants mentioned underreporting and/or under-participation as key barriers. They agreed with the findings from the literature review. The term underreporting refers to the situation in which not all cases of disease are captured or reported to the surveillance system, while under-participation pertains to employees not participating in a medical surveillance program (e.g., in the Coal Workers Health Surveillance Program, CWHSP in the USA, see Table 1). Half of the participants mentioned a lack of secure funding as an important barrier, while seven considered lack of awareness of the risk to be an important consideration for an outdoor workers’ surveillance system. Five participants stated that if an OSH surveillance system is voluntary or lacks a solid mechanism for data collection, it will be plagued by underreporting and under-participation. Other less commonly mentioned barriers included the costs of preventive measures, the lack of a mandated occupational exposure limit for sun exposure, and that KC is not universally recognized as an OD.
Top 5 barriers to developing and implementing an occupational surveillance system.
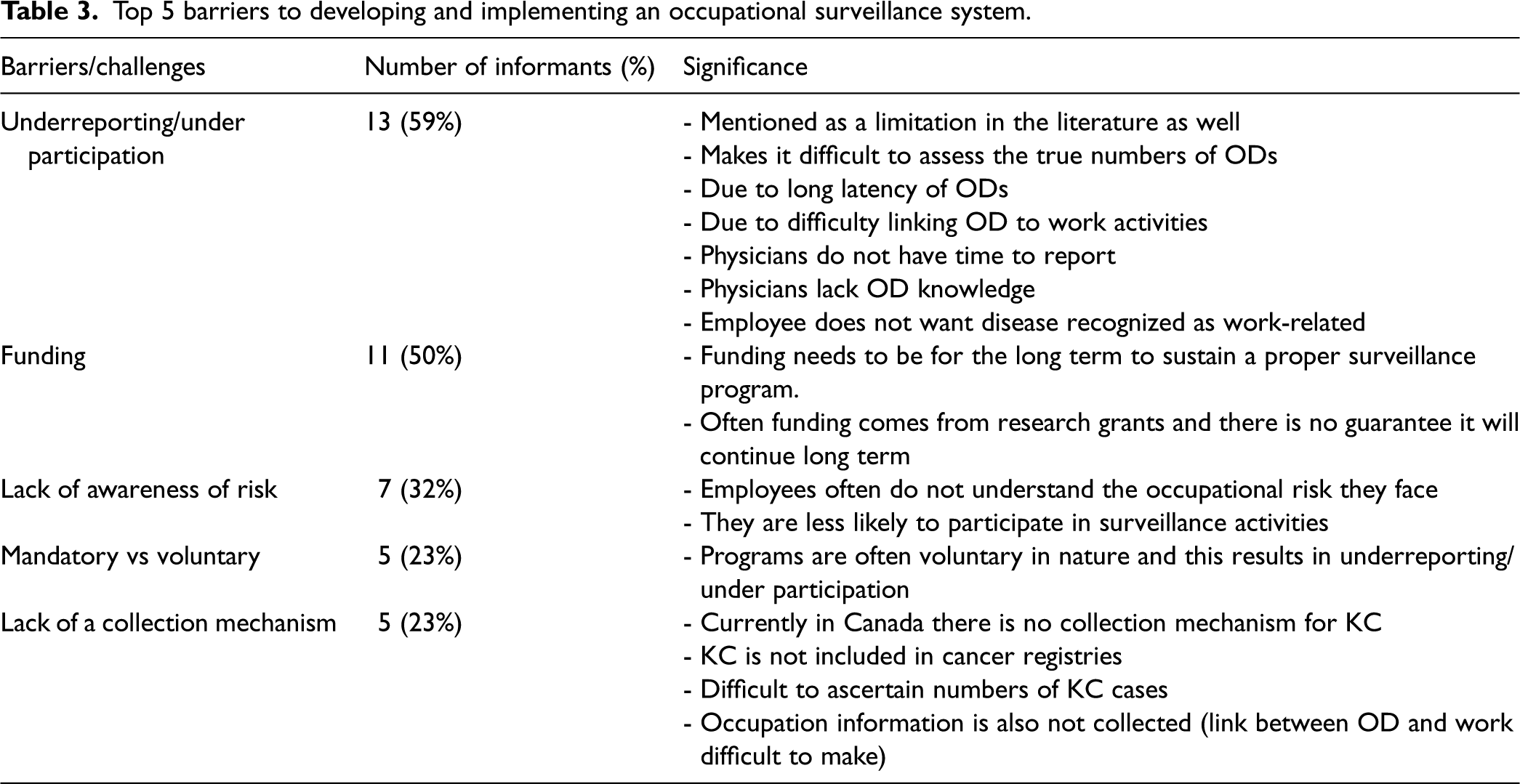
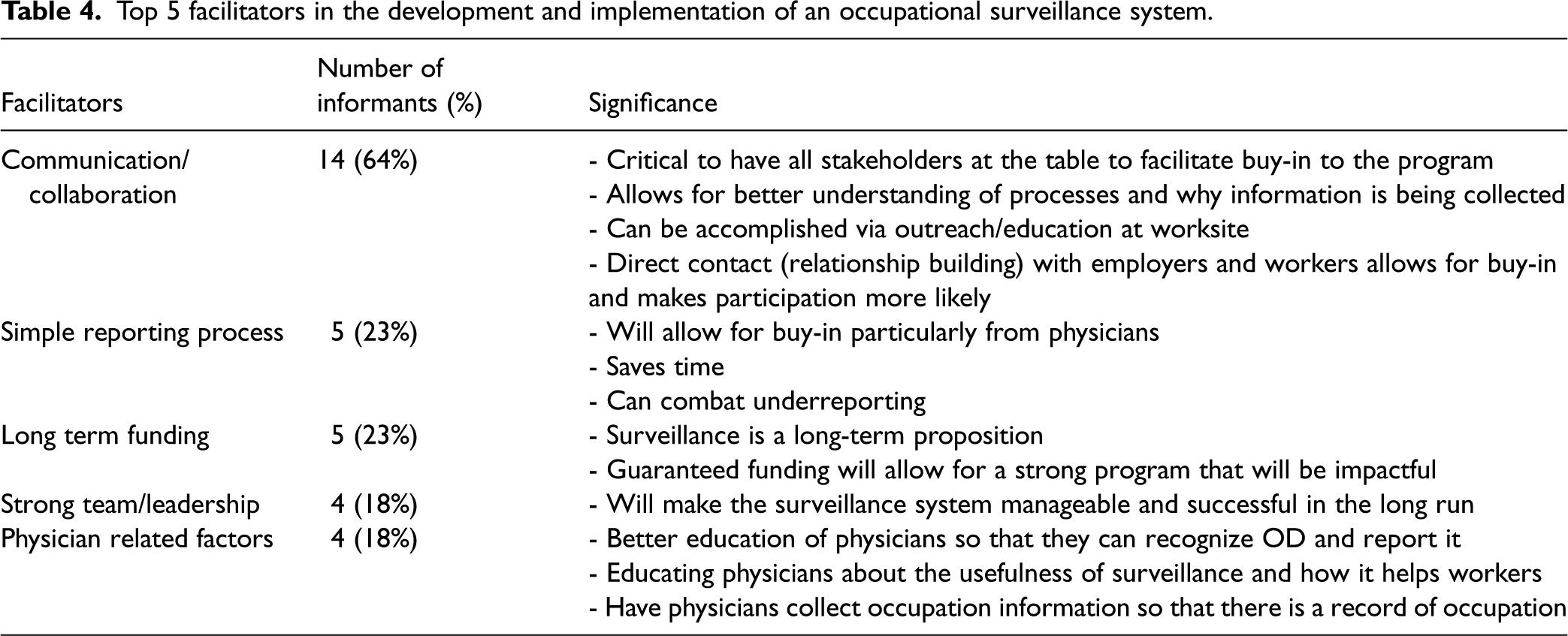
Table 4 shows the top five facilitators in the development and implementation of an OSH surveillance system. Fourteen of the key informants mentioned communication and collaboration at all levels as a key facilitator, making it the most identified facilitator. The communication/collaboration piece pertains to the key stakeholders (i.e., occupational health and safety professionals, labor representatives, academics and scientists, data managers, employers, regulators, employees, health care providers). Examples of the specific stakeholders for KC or UVR surveillance are further considered in the discussion section with a focus on the Canadian situation. Open communication and collaboration amongst these stakeholders are of utmost importance to support the successful design and implementation of an OSH surveillance system and buy into the program. It is important to note that communication and collaboration can lead to stakeholder buy-in, and that having buy-in from the outset from stakeholders can also aid in effective communication and collaboration, in a mutually reinforcing manner. Five of the key informants mentioned having a simple reporting process, and five discussed having secure and long-term funding as important to the success of an OSH surveillance program. Four key informants spoke about the importance of a strong team and good leadership, and four mentioned factors related to physician buy-in and participation. Other less commonly mentioned facilitators included legislation to support surveillance, ensuring strong scientific evidence, creating incentives for participation, and the importance of a clear goal.
Top 5 facilitators in the development and implementation of an occupational surveillance system.
Discussion
As stated in the “Results” section, while no surveillance system focuses exclusively on outdoor workers, Germany stands out when it comes to surveillance of KC and UVR exposure. It took approximately 15 years for Germany to officially recognize KC (including SCC and multiple actinic keratoses/AK) as an OD. As early as 2000, a group of researchers and dermatologists proposed that skin cancer due to UVR exposure at work should be recognized as an OD. 48 To strengthen the evidence for the connection between UVR exposure at work and the development of SCC and AK, a systematic review with meta-analysis was done.49, 50 Schmitt et al. identified 18 relevant epidemiological studies of which 16 studies found an increased risk of SCC in people who were exposed to occupational UVR, while Bauer et al. identified 24 relevant epidemiological studies that demonstrated that outdoor workers are at a significantly higher risk of developing BCC than indoor workers.49, 50 Solar UVR measurements were undertaken to quantify typical UVR exposure levels among the general population and outdoor workers. 51 Eventually due to the dedicated work of various researchers and dermatologists there was enough evidence and will to support the recognition of SCC and AK as a compensable OD.52, 53
Since 2015, KC (including SCC and multiple actinic keratoses) has been recognized as an OD and made reportable to the Deutsche Gesetzliche Unfallsversicherung (DGUV) or German Social Accident Insurance.52, 53 After the first 12 months of official recognition, more than 7,700 occupational KC cases were registered with the DGUV. 14 In 2018, the number of notifications was over 9,000 and it is expected that these numbers will continue to increase. From 2015 to 2019 approximately 44,000 OD reports for AK or SCC have been filed to the DGUV and about 60% of these have been officially recognized. 54 In Germany, physicians are offered a financial incentive to report. 14 Patients who have been diagnosed with occupational skin cancer are provided priority medical care and, in severe cases, substantial compensation. 14 Since July 2019, Germany has included medical screening in its surveillance of outdoor workers. Employers have been mandated by the government to offer skin screening every three years to workers who work outside for more than 1 h per day for 50 or more days per year. However, it is not compulsory for employees to take part in the screening.
One of our key informants, a dermatologist, told us that German employers are required to offer protective measures to workers who are exposed to solar UVR. Germany uses the “TOP Prinzip” for prevention.55–57 The “T” represents the technical measures (technische Maßnahmen) or engineering controls, which can include shade devices such as awnings or umbrellas. The “O” represents the organizational measures (organisatorische Maßnahmen) or administrative controls, which can include changing the work schedule to avoid work activities during the most sun intensive periods. The “P” represents the personal measures (persönliche Maßnahmen) or personal protective equipment, which can include wearing sun protective clothing or sunscreen. (The “TOP Prinzip” is similar to the industrial hygiene hierarchy of controls.) Unfortunately, the most recent available systematic review of whether or not skin cancer screening has a net benefit could not draw any firm conclusions. Further research is needed on whether medical screening is an effective tool for occupational skin cancer prevention and control. 58 This illustrates the fact, that screening, by itself, neither cures nor prevents disease without a defined procedure for action. The procedure would need to be accompanied by effective access to the resources (exposure prevention and/or medical care) necessary to follow the procedure.
German efforts to combat KC provided the foundation for the “Global Call to Action To End the Non-Melanoma Skin Cancer Epidemic in Outdoor Workers.”
14
This Call to Action highlighted ongoing barriers (which have been identified in our work). These barriers included the following needs:
to improve the legislative framework, to protect outdoor workers more effectively, to develop and standardize the registration process for KC cases, to improve monitoring and management by employers of outdoor worker exposure, to improve reporting of occupationally related KC cases, and to improve collaboration among stakeholders.
14
The most important barriers to an effective OSH surveillance system identified by our key informants included underreporting and under-participation, lack of funding and a lack of awareness of the risk of OD. It is not surprising that underreporting was on the list of most important barriers because surveillance systems should capture as many OD cases as possible in order to be truly representative and effective. Underreporting is a source of bias in OSH surveillance systems. Proactive and better funded employers may be more likely to participate. Funding is always a challenge in data collection and research and is a particular challenge for OSH surveillance because it is by definition ongoing; it cannot be wrapped up as a grant project in 2 or 4 years. The lack of awareness of risk can be a particular challenge for diseases with long latencies (like skin cancer). Workers who develop diseases with long latencies may not connect early symptoms of potentially severe diseases with past work exposures.
The most important facilitators for an effective OSH surveillance system identified by our key informants included communication and collaboration, having a simple reporting process and long-term funding. The purpose and importance of a proposed OSH surveillance system should be understood by all parties who are required to ensure its success. This can be achieved only by open communication and a spirit of collaboration. Obtaining buy-in from key parties as soon as possible will contribute to the long-term success of an OSH surveillance system. Having a simple reporting process is a key facilitator as it works to address some of the barriers (e.g., underreporting), and is especially important in cases where physicians or other front-line health care workers are required to be a part of reporting. Funding was identified as a facilitator as much as lack of funding was identified as a key barrier.
During the literature review and the key informant interviews, underreporting of ODs emerged as an important barrier. Kieffer and EUROGIP
38
found widespread underreporting of OD in five European countries. The main causes were:
difficulties identifying the work-related origin of certain diseases (due predominantly to the long latency between the time of exposure and the emergence of disease symptoms or because of associations with extra-occupational factors), medical personnel lacking sufficient knowledge to diagnose ODs, employees not wanting their diseases to be recognized as work-related due to fear of job loss or discrimination, employees lacking information regarding their possible exposure to relevant risk factors, and employees lacking information about the insurance system for OD available to them.
38
The report identifies best practices for addressing underreporting effectively. In Denmark, the strategy of cross-referencing or linking various databases (specifically the Cancer registry, and the National Board of Industrial Injuries) was used to determine whether cases of mesothelioma and nasal/sinus adenocarcinoma had an occupational link. Some recommendations to minimize underreporting further in Denmark included extending the obligation of reporting diseases of occupational origin from solely doctors and dentists to other practitioners in the health care sector, providing concise information about work-related disease on the Labor Market Insurance website, simple electronic reporting, and automatic reporting between the National Health Office and the Labor Market Insurance organization.
38
The cross-referencing or data linkage strategy has been used in Canada. Ontario developed the ODSS as there was no existing occupational surveillance system in Ontario that could identify high-risk populations and target prevention efforts.
45
“This system was created in 2016 by linking existing provincial health databases with job information in order to study OD and inform prevention activities. The ODSS identifies at-risk groups of workers, and potentially hazardous workplace exposures. Findings from the ODSS contribute to our understanding of OD in Ontario, and can support changes to public health practice.”
46
The ODSS links the following data sources:
Workplace Safety and Insurance Board's (WSIB) Time-Loss Claims Database, RPDB – Registered Persons Database, OCR – Ontario Cancer Registry, Ontario Health Insurance Plan (OHIP) eClaims Database, NACRS – National Ambulatory Care Reporting System, DAD – Discharge Abstract Database.
45
“The ODSS is currently being used to examine potential associations of occupation and industry with 28 cancer sites and 9 non-malignant health outcomes.”
45
A strength of this type of system is that it provides reliable occupational information. There are very few health data systems in Canada that include detailed and accurate information on occupation, but ODSS-type systems are created using accepted workers’ compensation claims (which have carefully collected occupation and industry information, assigned by occupational coding experts). A key informant told us that important limitations of this system are that it includes only individuals who have submitted workers’ compensation claims and the occupational information is available only for the time the claim is submitted. Specifically for KC, this strategy would be difficult to employ in Canada, mainly because cancer registries in Canada do not collect information about KC
59
and it is rare that a worker submits a claim to workers compensation for a KC diagnosis.
Though OSH surveillance systems for occupational exposures or diseases were not found for issues affecting outdoor workers, such as heat stress, eye conditions, or dermatitis, some countries have developed OSH surveillance systems that include KC and/or skin diseases. However, many of these systems have been hindered by underreporting. Among the reasons for underreporting of KC are:
the surveillance system is voluntary,
30
KC is rarely captured in cancer registries,
15
because KC is a disease that has a long latency, exposure and diagnosis may be far apart in time, people are exposed to the sun on and off the job, making it difficult to differentiate between occupational and non-occupational exposure,
28
as with many other diseases, health care providers do not always link the cause of KC to work,
61
and there is limited understanding of the risk that solar UVR puts on outdoor workers.1, 15
For long-latency diseases like KC, workers may have less fear of losing their current jobs because their health conditions could be linked to previous jobs. However, fear of employer retaliation and stigmatization could be a factor regardless of disease latency.
62
In addition, workers who develop diseases with long latency periods may not connect early symptoms of potentially severe diseases with past work exposures. In addition, they may not seek medical attention early enough because they don’t want to have to cover medical costs out of their own pockets.
62
Having to pay for it themselves is a very real risk in Canada, as in many of the countries we studied, because relatively few cases make it through the system and receive compensation. Moreover, independent contractors (or employees misclassified by their employers as independent contractors for the purpose of shifting workers’ compensation and other costs to the employees) would be required to pay insurance premiums to the provincial workers’ compensation system where they live and work in order to access workers’ compensation benefits. If they were not registered, workers’ compensation would be unavailable to them.
63
Unlike the workers’ compensation system, the Canadian tax-funded healthcare system would not turn away most people with skin cancer. However, some workers may have difficulty gaining access to the healthcare system or be deterred from attempting to access it, due to immigration status. It is a limitation of our inquiry that we did not seek information on access to healthcare services and compensation systems by outdoor workers who are undocumented (or otherwise unprotected by policy). There are many structural reasons that workers may not seek care or compensation for a health condition, such as KC, that can be caused by work-related exposures, non-work exposures or both.
Due to underreporting, there is a fundamental need to improve the notification of skin cancers. John 64 suggests that the updated World Health Organization (WHO) International Classification of Diseases (ICD) −11 provides some hope in this respect. According to one of our key informants, a German dermatologist, it includes separate codes for BCC and SCC and also has a 4-digit code that will allow for coding of the occupational etiology of KC. Currently in Canada occupation is rarely linked to health data and it would be beneficial to have a way to show that certain diseases have an occupational link.
Key Features of a Potential KC Surveillance Program for Outdoor Workers
To provide a working example of what an OSH surveillance program for outdoor workers could look like, we outline here the features that are important to consider for KC, which is the most common OD for outdoor workers. Four of the five considered OSH surveillance strategies (exposure registry, disease registry, disease screening/medical surveillance, sentinel event surveillance and disease surveillance via data linkage) could likely be used for the surveillance of either KC or sun exposure. There are strengths and limitations to each approach. It is difficult to assess exactly how successful each individual strategy will be for KC or sun exposure because they have been used to a limited extent for this purpose. The strategy to undertake exposure surveillance in the form of a registry for UVR exposure has not, to our knowledge, been used in practice, but there is a mounting body of data collected (mainly for research purposes) that documents the typical exposure levels experienced by workers in a variety of countries, primarily Germany, Denmark, Canada, Australia, and the United States.65–70 These studies and resulting data may include measurements taken on individual workers, or they may include some satellite and modeling techniques to estimate exposure levels over a typical working day or summed up over a year. These kinds of monitoring programs could be expanded to either measure UV exposure to individual outdoor workers, or to assign a probable exposure to each worker based on some parameters (e.g., job title, latitude of work, time spent outdoors).
The design phase of an OSH surveillance system for KC or UVR will certainly require thorough evaluation and thought prior to implementation. Of the 10 design considerations that emerged during the key informant interviews, some food for thought on how to approach four of them is provided. Of note, however, every jurisdiction may have different regulatory frameworks or systems and systems that work in one may not work in another. Of significance, however, is that all of these design considerations can be adjusted to accommodate each individual jurisdiction. The purpose of an OSH surveillance system for KC or UVR would be to identify workers and/or geographic regions at greatest risk and to provide evidence for cancer prevention programs and workers compensation systems. This would be done by tracking KC diagnoses and/or exposure to UVR over time.
The defined target population for this type of OSH surveillance system would be outdoor workers. Stakeholder involvement is of utmost importance in the design and implementation of a surveillance system and the following groups of stakeholders would be ideal for KC/UVR surveillance within the Canadian context (note that as previously mentioned, these groups may well be different in other countries or settings): labor union and industry representatives (focused on construction, agricultural, and building services workers as the largest exposed groups), scientific experts on outdoor work, occupational hygienists, dermatologists, occupational physicians, and workers’ compensation system leaders. Specifically, labor groups that represent large numbers of outdoor workers in Canada include Canada's Building Trades Unions, the Canadian Labor Congress, Canadian Union of Postal Workers, and the Canadian Union of Public Employees and their sub-affiliates, among others.
Data sources are a key component of any surveillance system. In Canada, it is difficult to ascertain the exact number of KC cases on an annual basis, mainly because most cancer registries do not collect information on KC. A first step to improve data collection could be for provincial and territorial cancer registries to include cases of KC. A system for reporting KC to the various cancer registries would need to be developed and this reporting could come from hospitals or regional cancer centers, pathology laboratories, or private practitioners. However, linking these cases to occupation would be the next challenge. This could be possible if workers compensation programs recognize KC as an OD which is entitled to compensation. The linkage of a provincial or territorial cancer registry with compensation claim data could provide important information on which occupations are at highest risk as well as an indication of how many workers are being diagnosed with KC. Physician billing data could also be improved to include more specifics on the type of KC diagnosed and perhaps whether there is an occupational link. The coding of the occupational etiology of KC in WHO ICD-11 may address this.
Policy Considerations
Some potential policy considerations to put into place in order for an OSH surveillance system for KC or UVR exposure to function in other countries would include the following:
Recognize KC as an OD which is entitled to compensation. For example, the Workers Compensation Act of the province of British Columbia, Canada, includes a ‘presumption of causation’ for primary cancer of the skin’ when there is ‘prolonged exposure to ultra-violet light’.
71
This approach presumes that the disease was caused by the related employment and expedites the compensation process. Unfortunately, no other province in Canada takes such an approach, and this approach occurs infrequently in other countries.
71
Without such an approach, compensation of work-related KC proceeds on a case-by-case basis with the majority of cases not upheld due to long latency and difficulties in linking exposure to specific employment. Establishing an OSH surveillance system for KC or UVR exposure would provide substantial evidence regarding the association of KC with specific types of work and to establish which outdoor workers have ‘prolonged exposure’ to UVR. Design and implement a notification and data collection mechanism for KC (e.g., via a registry or physician billing data) so that cases would be tabulated in a centralized repository. Such a system would most effectively be based on biopsy results or other automated forms of data collection as it has been shown that gaining clinician buy-in to investigate the occupational exposure history of patients is difficult.
72
Continue to implement primary prevention initiatives while building surveillance systems for ODs. Prevention initiatives cover a range of measures from policy, engineering (e.g., shade), administrative (e.g., task scheduling, procedures, training), and personal protection. We recommend a comprehensive and coordinated approach through the development of a sun safety program as described below.73, 74 Unfortunately, employers report that without specific OSH legislation for UVR safety there is little incentive to implement such programs.
75
Educate workers and their employers on the risk of skin cancer for outdoor workers. This education includes UVR safety training during new worker orientation, annual training updates of workers and supervisors, regular ‘tool box’/’tailgate talks’, and the use of posters and other signage to encourage specific worker behaviors (e.g., regular application and reapplication of sunscreen).73, 74
A consensus report by John and colleagues called for recognition of non-melanoma skin cancer as an OD. In addition, it called on governments and other organizations to “take steps to increase knowledge about the risk of actinic keratosis (AK) and KC among occupational workers to empower and change behavior among these groups…”.
15
In the same report, the authors call for the development of clear and accessible platforms to share educational materials to improve health literacy among outdoor workers. It is important to note, however, that education campaigns aimed at increasing knowledge of skin cancer risk factors or cancer prevention activities for workers are unlikely to be successful if they are not implemented within a comprehensive sun safety program which includes a commitment to the provision of resources and tools to act upon this knowledge, including provision of shade structures, sunscreen dispensers, and/or sun protective clothing, for example.75, 76
Safety programs for any hazard, sun included, can range from informal work practices up to formalized structures with requirements, activities, and persons responsible clearly identified, and in general, a sun safety program that considers multiple preventive considerations is likelier to be successful. Programs have been developed over the years to help support employers in controlling exposure to solar UVR among their workers.73, 74, 77, 78 For example, Sun Safety at Work Canada developed and trialed a Sun Safety Program which was designed to be embedded within an organization's OSH Management System (OSHMS). This approach applies a ‘sun safety lens’ to all elements of an OSHMS to identify sun safety aspects/initiatives for each element including workplace policy, communication, risk assessment, responsibilities and accountabilities of various roles within the organization, control measures, first aid and incident notification and reporting, preventive maintenance, procurement, workplace inspections, documentation, auditing and evaluation, management review, and ‘off the job’ sun safety.73, 74 However, evaluation of programs such as this has been limited to date.75, 79–81 This speaks very much to our finding that sustained funding, data infrastructure, and clear communication and collaboration are vital to occupational skin cancer prevention and to OSH surveillance of any kind.
This study provided a comprehensive summary of what kinds of occupational exposure or disease surveillance systems are available in current practice. We found that there are few examples anywhere in the world of jurisdictions that have OSH surveillance systems in place to support the exposure and KC risk reduction in particular for outdoor workers. However, Germany has made a great deal of progress in recognizing KC as an OD, tracking work-related KC diagnoses and providing medical surveillance to at risk workers. The German case can therefore be used as a model for other jurisdictions.
Conclusion
Solar UVR is a substantial, but often under-recognized exposure for outdoor workers. In many jurisdictions, skin cancer is not a recognized OD for outdoor workers exposed to the sun's rays, even though IARC has concluded that solar radiation is a human carcinogen. Our literature review found no OSH surveillance system that focused on outdoor workers specifically, however, the key informant interviews revealed the impressive progress Germany has made with regards to the surveillance of KC and UVR. Of the ten considerations in the design of OSH surveillance systems that were identified by key informants, the most important is having a clear purpose/goal, a defined target population, stakeholder involvement and a variety of data sources available. Further research is needed regarding the evaluation of occupational exposure and disease surveillance initiatives, including medical screening programs. However, an ideal system for the prevention and tracking of occupational KC is likely to be multi-functional, in that it would document OD occurring now from past exposure to solar UV, and document current UV exposure to create a record of such exposure occurring in the case that KC arises in a worker in the future. Further, such a surveillance system would be best suited to the primary and secondary prevention of occupational skin cancer if it tracked workers regularly over time. It should also be subject to regular evaluations to ensure it continues to evolve and respond to new challenges over time with respect to data sources and processing, infrastructure, or reporting functions, for example. This would provide a means of identifying higher-risk workers for potential intervention, as well as gaps in the system that could be addressed on an ongoing basis. A system like this would be an excellent source of evidence for cancer prevention programs and workers compensation systems and could serve as a model for other exposures and health outcomes.
Supplemental Material
sj-docx-1-new-10.1177_10482911231165975 - Supplemental material for Barriers and Facilitators in the Creation of a Surveillance System for Solar Radiation-Induced Skin Cancers
Supplemental material, sj-docx-1-new-10.1177_10482911231165975 for Barriers and Facilitators in the Creation of a Surveillance System for Solar Radiation-Induced Skin Cancers by Nicole Slot, Thomas Tenkate, Lindsay Forsman-Phillips, Victoria H Arrandale, Sunil Kalia, D Linn Holness, and Cheryl E Peters in Clinical Rehabilitation
Footnotes
Acknowledgements
We would like to acknowledge all the individuals who contributed their time to this work, including the project collaborators: Steve Quantz, Judith Purcell, Brenda Marsh, Nicole Braun, Merrill O’Donnell, Terry Parker, Brandon Leong, and Carmen Skelton. We would also like to thank the 22 key informants who participated in this study. We greatly appreciate everyone's willingness to share their time, experiences and knowledge with us. Finally, we would like to warmly acknowledge the keen editorial eye of Dr. Darius Sivin, Editor in Chief of NEW SOLUTIONS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Notes
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.