
Abstract
Purpose:
This study evaluated the benefits of a “survivor to thriver” strengths-based group intervention program to facilitate posttraumatic growth in women survivors of child sexual abuse.
Method:
A quasi-experimental, one group, pretest, posttest, time-delay design was employed using qualitative methods to evaluate the benefits of the intervention with 10 purposively selected women with a history of child sexual abuse. Six group sessions were conducted as well as a delayed follow-up session. Qualitative data were collected using drawings, narratives, and transcriptions.
Results:
Qualitative thematic content data analysis portrayed enabling processes of PTG such as emotional awareness, decisive action, posttrauma identity, and a healing group context.
Conclusion:
These themes suggest growth outcomes. However, a longitudinal study is recommended to establish efficacy and to inform practice with replicable interventions.
Worldwide, the prevalence of child sexual abuse (CSA) is high. A recent meta-analysis indicates the prevalence of CSA to be 18% for girls and 7.6% for boys (Stoltenborgh, van IJzendoorn, Euser, & Bakermans-Kranenburg, 2011). Pereda, Guilera, Forns, and Gomez-Benito (2009) reported the incidence at 19.7% for women and 7.9% for men and predict that this may be even higher in Africa. As such a study in one of the provinces of South Africa found that 39% of women and 17% of men had reported being sexually abused before the age of 18 years (Jewkes, Dunkle, Nduna, Jama, & Puren, 2010). This figure may even be greater in that most cases of sexual abuse are underreported and adult recall of CSA may not always be reliable. Establishing the true extent of CSA in South Africa is difficult as police statistics are the main source of data. The most recent South African statistics on sexual offenses against children remain alarming and indicate that 22,781 cases of alleged sexual abuse were reported to the South African Police Services between 2013 and 2014 (Lebone, 2014). CSA is thus an international crime of opportunity.
There is, however, no universal definition for CSA. In South Africa, sexual abuse in relation to a child has been defined in the
Children’s Act 38 of 2005 (RSA) as (a) sexually molesting or assaulting a child or allowing a child to be sexually molested or assaulted; (b) encouraging, inducing, or forcing a child to be used for the sexual gratification of another person; (c) using a child in or deliberately exposing a child to sexual activities or pornography; or (d) procuring or allowing a child to be procured for commercial sexual exploitation or in any way participating or assisting in the commercial sexual exploitation of a child.
Although some researchers found little evidence regarding the effectiveness of individual versus group therapy (Martsolf & Draucker, 2005), there is strong advocacy for group therapy with adult survivors of CSA, specifically given its potential to reduce stigma and its cost-effectiveness (Callahan, Price, & Hilsenroth, 2004; Lundqvist, Svedin, & Hansson, 2004). In addition, Brown, Reyes, Brown, and Gonzenbach (2013) and Callahan et al. (2004) argue that in group therapy, members might be able to better deal with issues relating to CSA such as guilt, shame, and isolation in the presence of it being shared with others. Meekums (2000, p. 114) refers to this essential component as “witnessing.” A systematic review of 13 experimental studies on the effectiveness of group treatment for adult survivors of CSA concluded that group therapy can indeed be effective in reducing symptoms and enhancing overall functioning (Kessler, White, & Nelson, 2003). In South Africa, group treatment for adult survivors of CSA is well suited as it supports the underresourced mental health services available. Furthermore, this treatment modality maintains the collectivistic South African culture of Ubuntu (Tutu, 1999). Ubuntu is an ancient African word meaning humanity to others bearing the philosophy; I am what I am because of who we all are (Tutu, 1999). Thus, group work is a culturally tailored resource (Petersen, Bhana, & McKay, 2005).
Traditional Versus Strengths-Based Approaches
A recent meta-analysis of 44 studies highlights traditional treatments for CSA, which predominantly focus on reducing symptoms and improving functioning by altering cognitive distortions and dysfunctional behavioral patterns in adulthood like substance abuse, mental health difficulties, and subsequent abuse (Taylor & Harvey, 2010). Such modalities are, for example, cognitive–behavioral therapy (CBT), which aims to alter cognitions while processing memories in order to change behavior (Wilen, Littell, & Salanti, 2012). Cognitive processing therapy (CPT) focuses on “memory activation and emotional re-processing” as well as redirecting misconceptions about the trauma (Wilen et al., 2012, p. 3). Psychodynamic therapy also focuses on reducing psychiatric symptoms and increasing social adjustment, but there is, however, also a strong focus on facilitating insight relating to the experience of trauma as well as modeling a supportive relationship (Callahan et al., 2004; Lord, 2008). In South Africa, an integrated approach exists for the traditional treatment of CSA, namely, the Wits trauma model, which combines CBT and psychodynamic therapeutic approaches in the treatment of psychological trauma (Eagle, 2000). The above approaches are limited by their lack of focus on the individuals’ strengths and strategies originating from their struggle to cope with the CSA (Calhoun & Tedeschi, 2006).
Several authors investigated strengths-based outcomes in CSA survivors and see these depicting a deeper understanding of how healing can be achieved after such a traumatic experience (Bogar & Hulse-Killacky, 2006; Ullman, 2014; Woodward & Joseph, 2003). Vilenica, Shakespeare-Finch, and Obst (2013) conclude that such studies not only focus on the traditional pathogenic outcomes and symptom reduction but also bring acknowledgment of the fact that even after enduring such a damaging trauma, the human capacity for healing, growth, and transformation can be developed. Hodges and Myers (2010) advocate for such a strengths-based paradigm when treating women survivors of CSA and state that researchers have neglected to investigate strengths-based interventions with adult female CSA survivors.
Strengths-based interventions are defined as “treatment methods or intentional activities aimed at cultivating positive feelings, behaviors, or cognitions” (Sin & Lyubomirsky, 2009, p. 467); thus, the persons strengths become the resources for change, which enable them to move toward growth, mastery, and well-being while remedying dysfunctional behaviors (Cummins, Sevel, & Pedrick, 2012). The treatment outcomes of the strengths-based approaches are not solely on the reduction of symptoms in order to return these women to their previous level of functioning, instead women are encouraged to use the traumatic recovery as “an opportunity for further individual development” (Zoellner & Maercker, 2006, p. 629). However, in strengths-based interventions, it is imperative to not focus solely on a person’s strengths and hereby create the impression that their past experiences are irrelevant. On the other hand, it may prove disempowering to only focus on the negative symptoms and stress. Hence, a balanced approach is needed (Orbke & Smith, 2013).
In South Africa, Edwards (2009) reports that the most common treatment approach to sexual abuse is from within the traditional paradigm, focusing on alleviating dysfunctional symptoms and behaviors. Recent studies illustrate that South African women can indeed demonstrate positive characteristics and changes originating from the CSA struggle such as improved relationships and increased empathy (Walker-Williams, Van Eeden, & Van Der Merwe, 2012, 2013). South Africa indeed provides a cultivating context for the strengths-based approach as the history depicts people who had overcome adversity and displayed positive transformation emerging from their past struggle with apartheid. In the opinions of Edwards (2009) and Griner and Smith (2006), it is imperative that models for treatment be adapted to the relevant country and context. As such, no evidence-based, strengths-based interventions for adult female survivors of CSA in South Africa have been reported in the literature (Walker-Williams, 2012).
Masten (2011) strongly argues that intervention methods are vital for testing theory and recommends that researchers partner in intervention trials that reflect current knowledge and focus on testing theories. LeCroy and Williams (2013) emphasize that the benefit of intervention work in the social work domain is indisputable. Furthermore, Bonanno, Westphal, and Mancini (2011) caution that such interventions may be harmful when not evaluated.
Therefore, in order to advance research-supported interventions (Thyer & Myers, 2011), the purpose of this study is to report on the benefits of a strengths-based group intervention program known as S2T, an acronym denoting survivor to thriver, that aims at facilitating posttraumatic growth (PTG) in adult South African women with a CSA history.
Posttraumatic Growth
In this study, we will work within the PTG model, which is an integrative approach building on traditional trauma interventions (Tedeschi, 2010). PTG is a strengths-based approach, which is founded on the belief that growth can follow adversity and focuses on the positive strengths, emerging as a result of the person’s struggle with the trauma (Vilenica & Shakespeare-Finch, 2012). Tedeschi and Calhoun (2004, p. 1) define it as “positive psychological change experienced as a result of the struggle with highly challenging life crises.” PTG is conceptualized as a multidimensional construct that includes changes divided into three general domains, namely, changes in the experience of relationships with others, changes in the perception of self, and changes in one’s general philosophy of life (Tedeschi & Calhoun, 1996).
Tedeschi and Calhoun (2004) have outlined a model that explains how the process of growth is conceptualized. They describe PTG as the outcome that results from a coping process (Tedeschi & Calhoun, 1996). This coping process begins with a traumatic event, for example, CSA, that internalizes a negative trauma schema or cognitive belief (Finkelhor & Browne, 1986), which severely threatens an individual’s schematic structures that have guided understanding, decision making, and meaningfulness. Higher order goals, beliefs, and the ability to manage emotional distress are challenged. The emotional distress a person experiences opens a process of recurrent rumination as well as attempts to engage in behavior aimed at reducing distress (Stockton, Hunt, & Joseph, 2011). Rumination is labeled by Tedeschi and Calhoun (2004) as cognitive processing and includes (a) analyzing the new situation, (b) finding meaning, and (c) reappraisal. Once a person experiences the first coping success, which is characterized, for example, by reduction in emotional distress, rumination is transformed into more deliberate thinking about the trauma and the impact it has on the person’s life (Zoellner & Maercker, 2006). This cognitive processing occurs until the person’s experience of the trauma becomes meaningful, comprehensible, and manageable. The individual thus has not only survived the trauma, but as a result of the successful cognitive processing, heightened emotional awareness (catharsis), and the reconstruction of a coherent life narrative (meaningful, comprehensible, and manageable) can identify transformational characteristics. These personal strengths are consequently borne from the struggle to cope with the traumatic ordeal (Tedeschi & Kilmer, 2005). PTG thus has a quality of “transformation” or a qualitative change in functioning and includes a future perspective (Tedeschi & Calhoun, 2004, p. 4). The process of PTG is dependent on the person’s characteristics such as hardiness, optimism, sense of coherence and environmental influences such as the availability of external resources (Calhoun, Cann, & Tedeschi, 2010; Oaksford & Frude, 2003; Tedeschi & Calhoun, 2004) as well as the guidance by an “expert companion.” This term is meant to convey “a sense of humility in that clinicians who are indeed well trained experts, need to have to allow for the kind of atmosphere that can lead to the personal exploration that is useful in developing a sense of posttraumatic growth” (Tedeschi & Calhoun, 2006, p. 292).
S2T Strengths-Based Group Intervention
In the S2T, we hoped that women would be able to identify strengths originating from their struggle to cope with the traumatic CSA ordeal as well as formulate a posttrauma identity encompassing a future perspective. This is founded on our beliefs as researchers and expert companions that all people have strengths and capacities, people can change, given the right conditions and internal and external resources. People are experts of their own trauma and can change and grow through their own strengths and capacities with the guidance of an expert companion. It is thus not about what is wrong but instead what is strong.
The S2T strengths-based group intervention advocates a balanced approach and draws on an eclectic mix of theories and is contextualized in existing evidence-based traditional approaches and additional strengths-based outcomes. From the outset, it serves as a supportive group intervention for women who have received initial CSA trauma counseling, and encompasses four treatment outcomes that draw on South African-based empirical research exploring the coping behaviors, PTG, and psychological well-being of a sample of women who had experienced CSA (Walker-Williams et al., 2012, 2013); a South African trauma treatment model, the Wits trauma model (Eagle, 2000), and traditional approaches and transformational strengths-based outcomes of PTG.
Outcomes and Group Sessions
The S2T comprises four treatment outcomes: (1) providing a supportive space for sharing the trauma story, experiencing heightened emotional awareness, and validating the group members’ experiences (drawing on CBT and CPT principles of cognitive processing); (2) normalizing symptoms (emerging from the psychodynamic approach) and reframing trauma messages (CBT and PTG model); (3) active adaptive coping drawing on psychological inner strengths (psychodynamic and PTG model); and (4) transforming from meaning making to personal growth by re-sharing the trauma story “for a change” from a new perspective (PTG model). Subsequently, we will briefly elucidate how these outcomes are facilitated during treatment sessions.
Sharing the trauma story
The initial session consisted of gaining informed consent, clarifying roles and expectations, setting group commitments, conducting the pretest, and then discussing the emerging themes thereof. In doing so, during the first group session, the pretest (which consisted of a draw-and-write and draw-and-talk activity) was used to initially encourage women to start sharing their traumatic sexual experience/s and to start cognitively processing and developing a coherent personal narrative of their trauma in a safe, contained, group space. This included facts, feelings, cognitions, and sensations in order to bring about intentional rumination in preparation for cognitive processing and restructuring (Stockton et al., 2011). In recounting this sequential trauma story, which is comprehensible to other group members with similar experiences, the material transforms into rational, realistic, manageable, and understandable information (Eagle, 2000; Paton, 2006). This provides further opportunities for exploring and reframing negative messages internalized during the traumatic ordeal and paves the way for the treatment outcome, which is understanding and catharsis. Emotional awareness triggered through the storytelling and catharsis in the context of group treatment for CSA survivors is highlighted by Van Loon and Kralik (2008). This ties in with what Eagle (2000) points out, namely, that remembering can be cathartic and enables the survivor to express the unexpressed feelings and experiences associated with the trauma within the safety of the group context. Therefore, in order for healing to commence, Vilenica and Shakespeare-Finch (2012) concur that increased emotional awareness of the effect of the CSA on the victim’s life is imperative.
When reflecting on the risks of facilitating the sharing of the trauma story, the facilitators took the following precautions: women were encouraged to share their stories freely without interrogation, strong emotional reactions were contained and processed by the facilitators, a “safe word” was used to indicate feelings of being unsafe, and two group facilitators were able to take turns guiding the process and being available for any individual containment needed.
Normalizing symptoms and reframing trauma messages
During the second session, participants were provided psychoeducation on the negative outcomes of CSA trauma. Literature dictates that women with a history of CSA learn to believe that they are “defective, experience shame about themselves, find it hard to trust others, feel emotionally deprived, abandoned and isolated” (Cukor & McGinn, 2006, p. 30). These symptoms appear to correspond with the four trauma-causing factors or traumagenic dynamics proposed as early as 1986, by Finkelhor and Browne (1986), namely, stigmatization, powerlessness, betrayal, and sexual traumatization. Such cognitive beliefs or internalizations become the women’s internal working model (Orbke & Smith, 2013) and may ultimately lead to numerous psychological and behavioral manifestations (Cukor & McGinn, 2006). Thus, in this session, an activity was conducted exploring the women’s individualized trauma messages or internalizations, and a significant amount of time was spent on the processing of these messages. Cognitive restructuring (meaning making and personal growth) is an important coping strategy employed in altering the survivor of CSA’s perspective on the traumatic event (Calhoun & Tedeschi, 2006).
On commencement of the third session, a cathartic healing ritual was completed and participants were equipped with skills that enabled them to challenge and process cognitive distortions emerging from these internalized trauma messages and to use their thoughts to alter their behaviors. By providing this psychoeducation and normalizing the symptoms and messages associated with the abuse, women were taught to manage the associated symptoms and reframe these internalizations and begin to actively decide to positively shift their awareness. Women were thus sensitized to the effect it may have had on their psychosocial and overall functioning. Following this, themes such as loss and forgiveness were addressed in the fourth session, during which the participants were afforded the opportunity of writing a letter to the perpetrator sharing their struggle with the adversity. It was imperative that participants also be guided toward adaptive coping strategies in each session in order to face the adversity. Hence, the treatment outcome was not only to provide psychoeducation on symptoms and internalizations but to explore the existence and manifestation of these negative cognitive beliefs in each group member and the effects of these on their overall functioning.
Active adaptive coping strategies
Active coping strategies have been associated with better adaptation to stress, and seeking social support is such a coping strategy (Olff, Langeland, & Gersons, 2005). In order to build such resilience in CSA survivors, the adult’s internal working model should include factors contributing to “hardiness,” namely, internal locus of control, sense of purpose, and seeing the potential for growth in all life experiences (Orbke & Smith, 2013, p. 49). Throughout session one to six, the group members were encouraged through skills training to explore their current coping repertoire and character strengths in order to engage in new constructive coping behaviors in order to deal actively with problems and access social support networks. The treatment outcome was thus to use existing strengths to build on a resiliently driven adaptive coping repertoire (Compton & Hoffman, 2013).
Transforming from meaning making to personal growth
The fifth and sixth sessions focused on their posttrauma identity and facilitated a re-sharing of their stories from a new perspective by focusing on their inner strengths originating from the struggle. Here, the women retold their stories with emphasis on how their struggle to survive the ordeal had elicited personal strengths and growth. The posttest and processing thereof was also dealt with in the sixth session. Activities were focused on enhancing the women’s ability to understand themselves and the world post trauma in order to move from the victim position to an altered survivor–thriver position. Women were encouraged to adjust their internal working model and philosophy of life and focus on their identity as survivors of CSA within their current life context (Calhoun & Tedeschi, 2006; Orbke & Smith, 2013). They were reminded that the impetus for growth is located in the struggle with the aftermath of the traumatic event and not with the event itself (Calhoun & Tedeschi, 2006). Discussions thus attempted to assist the women to derive some salutary meaning from the CSA experience (Draucker et al., 2011). This was, however, respectively, facilitated so as not to deny the CSA damage done as the re-sharing of traumatic experiences could open old wounds, but, most importantly, it provided an opportunity for the survivors to describe how they would like to reframe their recovery process (Hodges & Myers, 2010) and address the several losses experienced. Thus, the treatment outcome is to provide group members with an opportunity to reflect on their own positive experiences post trauma and, as a result, embrace the posttrauma survivor identity. Three months after the posttest, a refresher session was conducted, which provided an opportunity for reflection and a discussion of healing outcomes as well as a delayed posttest. This type of approach, in which qualitative methods are used to evaluate interventions, has been employed globally and in South Africa (Hill, 2012; Mitchell, Theron, Stuart, Smith, & Campbell, 2011).
Method
Design
A quasi-experimental, one group, pretest, posttest, time-delay design (Leedy & Ormrod, 2005) was employed to evaluate the benefits of the S2T strengths-based intervention for this group of women. Due to the secrecy surrounding CSA, it was impossible to randomly select women and also difficult to recruit enough women to constitute a comparison group, thus a quasi-experimental design was most suited (Yegidis, Weinbach, & Myers, 2012). The S2T program spanned 3 months, in which six group-facilitated sessions took place. These sessions typically lasted between 2 and 3 hours and were conducted at 2-week intervals. Three months after the last session, a delayed follow-up session was conducted.
Participants and Sampling
Various professionals (social workers and psychologists) from organizations in and around the Gauteng province were approached as gatekeepers. The gatekeepers screened for possible candidates according to the inclusion and exclusion assessment criteria. Inclusion criteria for the group are a minimum age of 21 years, disclosure of the CSA, the women had received some form of crisis intervention (as a child/an adult) or disclosure therapy but still had a need for further intervention, could function reasonably well in day-to-day life, could understand and respond to English/Afrikaans, and were willing to participate voluntarily and partake in the S2T intervention sessions at a central community location. Exclusion criteria included women suffering psychotic symptoms or substance dependence (this was screened by the informed gatekeepers). These issues were excluded as they were seen to have the potential of hindering the recovery experiences of other women in the group.
Once the gatekeepers had obtained informed consent from the participants to disclose their details, the researchers made telephonic contact with those who had consented. Next, researchers met up with 10 purposively selected women with a history of CSA and explained the nature and purpose of the program. Participants then completed an informed consent form stipulating their voluntary participation in the program and the researchers then provided information clarifying their expectations and dual roles as facilitators and researchers (Trondsen & Sandaunet, 2009). Ten women entered the program (four were Black and six White) and seven completed the posttest (two were Black and five White) and five the delayed posttest and follow-up (two were Black and three White). The ages of the women spanned 22–50 years. All participants were employed and nine were in a relationship. All participants had experienced contact sexual abuse and the perpetrator was known to them. Three of the participants dropped out before the posttest session (two were Black and one White). Telephonic contact was made with these participants, and attempts were made to encourage them to rejoin the group. Reasons offered by the women concurred with the study of Lundqvist et al. (2004) who found that some women may be reluctant to continue exploring their CSA experiences in a group context. These women were offered the opportunity to continue on an individual basis but declined. Two participants could not attend the delayed follow-up session due to illness and being out of the country.
Procedures
The S2T strengths-based group intervention program was developed to be implemented over a 3-month period. No consensus exists among researchers on the proposed length of group treatment (Kessler et al., 2003). Some direction is, however, given in a recent study by Kreidler and Einsporn (2012) who found that intensive shorterterm group therapy for female adult survivors of CSA may be more beneficial than less intensive longerterm group intervention. This study was conducted by a qualified registered social worker and clinical psychologist with experience in the field of CSA. Before each group session, participants received an electronic reminder and those that had failed to attend were followed up telephonically. The participants that were absent were briefed on the missed content before commencement of the next session.
Data Collection
Literature depicts that an important part of healing for women who experience CSA is to come to an understanding of these complex trauma experiences (Vilenica et al. 2013). The S2T, thus, employs a qualitative approach, which is rich in detail, sensitive to context, and capable of showing the complex processes of PTG in these survivors’ lived experiences (Neuman, 2012). This was done using the visual, participatory draw-and-talk or draw-and-write method (Mitchell et al., 2011) in collaboration with structured treatment sessions (Greeff, 2011). The combination of more than one data-gathering method enabled the researchers to gain an in-depth and holistic view of the phenomenon in question and the benefits of the S2T intervention for this group of women (Creswell, 2014). During the initial and last session, a pre and posttest was conducted, respectively, which entailed that participants partook in drawing and writing activities and then in explaining these pictures in the group setting. Mitchell et al. (2011) indicate that drawings can assist adults in capturing memories, thoughts, and feelings, which are not easily transformed into words. The following instruction was given: Draw a symbol of how you have coped with your traumatic CSA ordeal and what growth (if any) you have experienced as a victim of this childhood trauma? Then, explain in writing (e.g., write down a couple of sentences) what your drawing is saying about how you have coped and grown (if at all) from your CSA experience.
Three months after conclusion of the S2T intervention program, a delayed posttest was done. The group was exposed to a refresher session, which was facilitated by the researchers during which they received the same pretest as explained earlier. After the pre-, post-, and delayed posttest, participants were encouraged to reflect on their drawings and narratives and identify symbols and words which represented growth (if any).
Data Analysis
Data analysis was conducted in two phases: First, the transcriptions of all the treatment sessions were inductively coded using thematic content analysis (Leedy & Ormrod, 2005) by means of qualitative data analysis software, ATLAS.ti 7.0 (2012). Both researchers conducted the first round of open and axial coding independently using a coding protocol, where after they convened to discuss emerging themes and subthemes. This process resulted in some themes being combined, others eliminated or being renamed (Braun & Clarke, 2006). The broad thematic categories of the pre-, post-, and delayed posttest drawings were contrasted and inferences regarding the nature of PTG over a 6-month period were deduced. Hereafter, the refinement of themes was facilitated by independent peer reviewers and qualitative methodologists in order to answer the primary research question, namely, what are the benefits of the S2T group intervention program in facilitating PTG in these women with a history of CSA?
Second, during the post and delayed posttest, participants were invited to engage in reflections on their pictures (pre, post, and delayed), which entailed the following: participants were given their three drawings and narratives and then they were afforded the opportunity of evaluating growth (if any) as depicted in sequence. Thereafter they were encouraged to take snippets of data from the drawings and/or narratives, to formulate three phrases that described their interpretation of growth, and to juxtapose them.
Trustworthiness
Using an iterative questioning process and reflective commentary during group sessions, credibility of the data was enhanced (Shenton, 2004). For consistency and dependability, a clear audit trail was kept, which describes in detail how data were collected, how categories were derived, and how decisions were made throughout the inquiry (Creswell, 2014; Merriam, 2009). The researchers also kept a research journal as well as a detailed log of coding decisions, inclusion and exclusion criteria in relation to themes, and other memos relating to the coding (Merriam, 2009). Both researchers had undergone training in qualitative methodology, qualitative data analysis, and in the use of the software ATLAS.ti 7.0 (2012).
Ethical Considerations
Ethical clearance was obtained from the North-West University’s Ethics Committee (Institutional Review Board) prior to commencement of the intervention. The application was reviewed by external assessors and had to adhere to institutional ethical standards for behavioral research. Participants took part in the study voluntarily and could withdraw at any time without reprisal, as was explained in an introductory letter accompanied by an informed consent form which was signed by all participants as proof of voluntary participation. Confidentiality was encouraged in the group setting by means of a group commitment contract, and the voice recordings and transcriptions were labeled with codes and securely stored after completion of the data analysis (Creswell, 2014). A practice protocol (Fraser, 2004) was included, which described each session and activity in detail in order to enable researchers to replicate the intervention for future use (Hill, 2012). As suggested by Kessler et al., (2003), an ethical treatment protocol should be adhered to and includes the assessment of possible risk behaviors and referral, where necessary (two participants were referred for individual therapy and telephonic follow-up took place). Facilitators offered extra support outside the group and group members were given the telephone numbers of the facilitators in order to enable the participants to contact them if any difficulties arose that the participant could not endure until the next group session would take place.
Being a researcher and facilitator during intervention research creates a multifaceted role and several authors stipulate the inclusion of a reflexive approach when there is a dual role for the researcher (Arber, 2006; Trondsen & Sandaunet, 2009). This approach enables one to understand how the researcher who is also a facilitator has an impact on those researched (Arber, 2006) as well as on the data analysis. In order to address these challenges, researchers should interrogate their own beliefs and feelings in the same way they interrogate those of their participants. Thus, at all stages in the research, the impact of the researcher in terms of data generation and analysis, relationships in the process, and how one is addressed as a researcher and facilitator should be documented and become part of the analysis. Hence, reflexivity establishes the researchers’ integrity. In this study, we included a research journal and audit trail (Arber, 2006). However, ethical challenges also exist concerning the dual role in that the prolonged relationship between the researchers and participants in the study can produce a felt obligation to help the researchers in succeeding with the program (Trondsen & Sandaunet, 2009). Bearing these potential challenges in mind if we only had a distant relationship with this sensitive population, it would have been more challenging to gain a deep perspective on their recovery and healing experiences. Therefore, in light of the role of expert companionship (Tedeschi & Calhoun, 2006), we engaged in high-quality interactions that required skilled expert knowledge of the unique trauma and dynamics of CSA, traumatology, grief, and the enabling processes of PTG.
Findings
First, emerging themes from the transcribed data will be discussed. Thereafter, a description is given of the enabling factors emerging from the visual participatory method as seen in Table 1.
Women Who Experienced CSA: Descriptions of Drawings, Narratives, and Short Phrases.
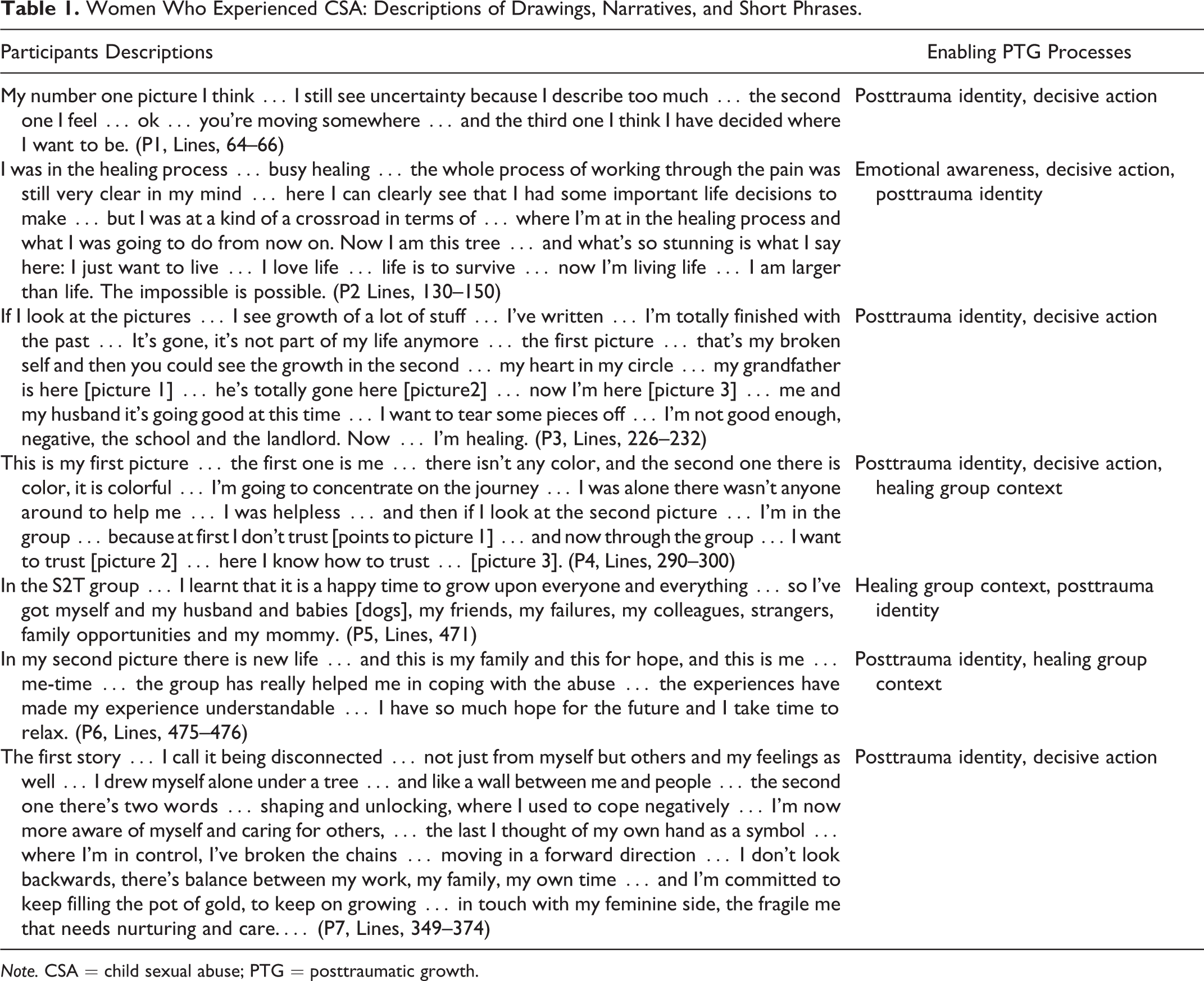
Note. CSA = child sexual abuse; PTG = posttraumatic growth.
The four key themes derived from the data analysis of session transcriptions, together with the visual participatory approach, are indicative of a variety of processes that support and facilitate PTG. The first theme suggests that intensified emotional awareness assisted the participants in initiating their process of healing through the experience of catharsis, emotional release, and deep introspection, which relates to the posttraumatic domain of a changed perception of self. Second, the participants were encouraged to identify, explore, challenge, and reframe the trauma messages relating to the CSA cognitive distortions, also indicative of a changed perception of self. Hereafter, they were steered into consciously taking decisive actions, which prompted the experimentation of new adaptive coping behavior patterns. Third, participants took ownership of their healing outcomes and it appeared that they grew into a posttrauma identity, suggesting a shift from survivor to thriver, which relates to the posttraumatic domain of a change in life philosophy. Finally, the normalizing and healing group context was reported as a vehicle for strengths-based recovery and emphasized the posttraumatic domain of a change in perceptions of relationships.
Emotional Awareness and Introspection
The S2T intervention program encouraged heightened emotional awareness that resulted in all participants displaying deep cathartic reactions, and this led to higher levels of introspection pertaining to the impact of the CSA trauma on their emotional and overall functioning. Participant 2 acknowledged that the catharsis was both painful and enjoyable, “The hurt has been pulled out with the wounds…and it was so wow… I really enjoyed that emotion coming out [in the group]” (Participant 2, line 217, 37 years). Yes, I was very emotional after the session…for about 2 days… when I got home I was very tired, and I just got into bed and the tears were flowing…I’m gonna cry now again [crying]… because you know you work through it and then you leave it…and then you start to live your life again…. (Participant 2, lines 154–164, 37 years)
Decisive Actions—Moving From Utilizing External to Internal Resources
During the S2T activities and rituals focusing on normalizing symptoms, reframing trauma messages, loss and forgiveness, and on re-sharing their CSA stories, participants reported a conscious decision to alter distorted cognitions. This resulted in the women experimenting with new adaptive coping behaviors that enabled a posttrauma identity and an internal locus of control. The following demonstrates how Participant 6 manages to challenge and reframe her negative internalized trauma message from being a sexual object to becoming a consenting adult women, When I got home the first time…I couldn’t wait to get to my husband…it was the first time we had sex in a year and a half and that was for me a highlight of this group…I am not the little bird with a broken wing…I feel I moved quite a bit…So that’s a big step for me…I can share basic feelings with my boss that is also my friend and it’s not sexual at all and that is a big step for me…so hooray to the group! (Participant 6, lines 377–378, 34 years) And that was not something that came naturally to me…it’s something that I had to decide…I am going to feel good about myself…I am going to place it into perspective…in order to get through this you have to decide everyday. (Participant 2, line 207–275, 37 years)
Participant 5 mentions the empowerment she experiences as a result of taking control over her decisions “I am better…I feel like a woman…I take my own decision and I make my own decisions…I can talk when things are bothering me” (Participant 5, line 1181, 26 years).
Posttrauma Thriver Identity
Participants reported a shift from a survivor to a thriver identity. This was reflected in their reported self-acceptance and self-efficacy during activities that dealt with adaptive coping and inner strengths in the S2T group. Participant 7 indicated that she was able to identify a specific point in time during the group treatment when growth, awareness, and self-acceptance took place, … I thought as a little girl I felt different than the other girls. But now after last night I still feel different but in a good way. It’s good to be different…I looked in the mirror, and I wanted to look away …and I looked at myself again, and I smiled at myself…now every day I think I am good enough…now I am self-worthy… I have learned so much about myself and especially that the past does not have to hold me in chains anymore, because I am worthy and so much better…I am able now to look into the mirror not in disgust, but in pride…I now reach for the stars and do not find comfort in the dark shadows anymore…I am a winner. (Participant 7, lines 623–984–1185, 39 years) … this is a positive journey…and I always say to me [myself]that this scar…it is not anymore a scar of sore, but a scar of a survivor…and now a thriver…I don’t regret anything for what I went through…I will always embrace myself…. (Participant 4, line 1085, 43 years) Wow, I didn’t know there was a thriver stage [laughs]…I was stuck in the survivor stage…and I thought it was going to be like that always and always…life is to survive…but now I’m living life. (Participant 2, line 150, 37 years)
Healing Group Context
Participants reported finding the group setting a healing space, a vehicle for recovery. After hearing the stories of the other participants throughout the group sessions (witnessing), they felt they could reveal their own pain and suffering. This could be indicative of a supportive, structured, contained, and accepting environment created by the unique common identity held in the S2T group. To come face to face with other survivors of CSA and experience people that truly understand what it really is all about is illustrated in the following statement: … You know the thing is, there’s so many things that you achieve that you cannot tell anyone else…that’s for you a real achievement…and it’s great to share that with people who have walked the same road…that know…because normal people won’t understand why this is such an achievement for me…when you go through life you hardly meet people that’s been raped or molested or anything…they don’t really talk about it…for the first time you are sharing with people who you can relate to… what you’ve been through and you can relate to what they’ve been through. (Participant 2, line 144–185, 37 years) … there is one thing about this group that I enjoy so much, it’s that here I can be absolutely me…If I want to cry I cry, nobody thinks I’m silly…If I want to laugh, I can laugh…If I want to fail, I can be a failure…I can feel, I can feel like I’m here…I’m here. (Participant 1, line 243, 50 years)
The following expressive quotes show how the group context provided an opportunity for “witnessing of experts” (survivors of CSA) to reflect on other group members’ growth: “I can see confidence and happiness, true happiness … that’s what I can see…she was beautiful at first, she has always had this presence but now it’s a confident happy presence…it really is” (Participant 1 reflects on Participant 2, line 180). I see a change in her…she is still emotional but she manages to keep it under control…she really does…at first she was just bursting out in tears and it seemed like she didn’t know how to get it under control and she was apologetic about it and now she accepts that she can be emotional and she controls it much easier. (Participant 7 reflects on Participant 1, lines 251–258) And then, I must tell you…the next session you start talking and you came across so intelligent and you started to reflect on yourself and you opened up…and that to me was stunning…and if I now look at the growth its two different people. (Participant 2 reflects on Participant 7, line 418)
Visual Participatory Data
Participants’ own analysis of their drawings, narratives, and reflective short phrases are corroborated by the emergent themes discussed earlier (no new themes emerged in the visual participatory data), describing enabling processes of PTG. Posttrauma identity and decisive action were the overarching processes depicted in these drawings and narratives of the participants. Women depicted that their struggle with CSA trauma led to the rebuilding of a shattered identity, which after taking decisive action (making a conscious decision to move past the struggle) was reintegrated into a posttrauma identity. This posttrauma identity has been reported in literature as a changed life philosophy (Calhoun & Tedeschi, 2006).
Discussion and Implications for Practice
The balanced S2T strengths-based group intervention program, developed to focus on facilitating PTG in women survivors of CSA, appears beneficial to the participants in this study. The responses and reflections of the group members as depicted over a stretch of 6 months suggest PTG-enabling processes derived from a transformational change in their view of themselves (personal narrative), others (relationships), and the world (philosophy). This suggests a realization of their personal strengths and the desire to continue on a life path of growth (thriver identity). In our study, this process entailed four distinct enabling processes: emotional awareness, decisive action, posttrauma thriver identity, and healing group context.
The heightened emotional awareness displayed by these women appears linked to a conscious cognitive process entailing decisive action through which these women could continually strive toward reconstructing a coherent posttrauma narrative. Vilenica and Shakespeare-Finch (2012) found that such increased emotional awareness is imperative when commencing a healing process. The deliberate form of cognitive processing reported is supported by Stockton et al. (2011) who suggest that this rumination is associated with growth following trauma. Orbke and Smith (2013) highlight the role of decisive action as a foremost need of survivors of CSA, as they were stripped of this sense of control as children. The healing group context provided the S2T participants with an opportunity to explore the trauma in the experience of other group members within a safe environment. This is substantiated by Meekums (2000) who declares that the experience of witnessing and being witnessed in the group contributes to a reframing of personal identity from lone victim child to collective powerful adult. After 6 months, the S2T participants appear to no longer be searching for meaning with “why” questions but instead constructing their own meaning with “how” questions (Tedeschi, 2010), relying on their personal recovery strengths. This entails continually striving toward a coherent posttrauma narrative, wherein transforming the trauma they realize that the abuse is only a segment of them and continue to build on personal characteristics and grow from the struggle to cope with the negative outcomes of the CSA trauma (Tedeschi & Calhoun, 2004).
The reported growth should, however, be reevaluated after an extended period, as at times, the negative outcomes resulting from the adversity may challenge this coherent life narrative and temporarily place the survivors back in crisis. A longitudinal study is thus recommended to establish the efficacy of this intervention and to inform practice with replicable strengths-based interventions so as to train helping professionals in South Africa. Social workers should be encouraged to incorporate strengths-based interventions into their current practices where the focus is on amplifying strengths and not only on repairing the weaknesses of clients. However, they should be cautioned about the fact that intensive therapy may often need to take place before a strengths-based approach could be incorporated and that, as social workers, they can only support the process of growth—they cannot create it for the survivor. This study highlights the worrying gap in the provision of evidence-based treatments for women survivors of CSA in South Africa. There is thus a need for greater advocacy for adult survivors of CSA through services and policy making by social workers and other helping professionals.
Limitations to this study include the small sample size; only seven women completed the posttest and five the delayed posttest, no comparison group was included, and the findings are based on a 6-month period, which is not indicative of the longer term effectiveness of the S2T intervention program. Furthermore, such interventions require professional facilitation (dual role of researchers), a possible limitation, which could be addressed with specialty training. Women participated in their second language, which may have inhibited participation. Also, during the visual participatory data collection method, participants were instructed to identify symbols and words which represented growth. This is a limitation as it may illustrate the participants’ compliance and not their growth. Lastly, we acknowledge that these women’s inherent resilient processes and supportive ecologies or other unknown factors may have contributed to this growth. However, despite these limitations, it appears that the S2T intervention is a promising practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support from the National Research Foundation (South Africa). Grant number: 94146.