
Abstract
Purpose:
To evaluate three approaches adopting collaborative depression care model in Los Angeles County safety net clinics with predominantly Latino type 2 diabetes patients.
Methods:
Pre–post differences in treatment rates and symptom reductions were compared between baseline, 6-month, and 12-month follow-ups for each approach: (a) Multifaceted Depression and Diabetes Program (MDDP) grant–hired social workers dedicated for depression care, (b) Diabetes–Depression Care-Management Adoption Trial (DCAT) supported care (SC) by clinic social workers in diabetes disease management teams, and (c) DCAT-automated care-management technology-facilitated care (TC) model. All social workers were guided by a depression care protocol.
Results:
All approaches significantly increased treatment rate, the largest improvement being MDDP (40%), followed by TC (30%) and then SC (20%). Similar patterns were found in symptom improvement (≥50% depression score reductions) and self-rated health. TC was the only approach to significantly improve patient diabetes self-care.
Discussion:
Activated social workers and technology facilitation provide promising effective adoption of collaborative depression team care in safety net.
Introduction
Patients with chronic illness are more likely to experience comorbid stress and/or depressive symptoms (Cummings et al., 2015). Latino Americans, the largest ethnic minority group in the United States (including both Mexican and Central Americans), have the highest lifetime risk of diabetes and significantly high rates of up to 33% with comorbid clinically significant depression (Li, Ford, Strine, & Mokdad, 2008; O’Brien, Alos, Davey, Bueno, & Whitaker, 2014; Schneiderman et al., 2014). Implementation of collaborative team depression care is supported by research (Katon et al., 2010). There is evidence that among Latino patients, literacy and socioculturally adapted collaborative depression team care is effective in reducing depression symptoms, while enhancing depression treatment retention among patients with concurrent diabetes, coronary heart disease, and cancer (Bauer et al., 2012; Ell et al., 2008; Ell et al., 2010, 2011; Ell, Oh, Lee, & Guterman, 2014; Wu, Ell, et al., 2014).
However, less is known about uptake and variability in the types of care provided or the outcomes achieved when different approaches are used in implementing the collaborative team depression care models in safety net community primary care settings (Bauer et al., 2011; Goodrich, Kilbourne, Nord, & Bauer, 2013). Implementation of the collaborative team care models requires organizational intervention aimed at identifying barriers and facilitators and designing training and communication between medical and psychosocial providers (Benzer et al., 2012). At the same time, rapidly growing health information technology provides both challenges and opportunities to advance integrative biopsychosocial team care practice models. Both care-management and communication technologies are increasingly relevant to medical and behavioral health clinicians’ practices, and hence, organizational leaders are calling for health information technology research (Clarke & Yarborough, 2013; Druss & Dimitropoulos, 2013; Haberer, Trabin, & Klinkman, 2013; Lyles et al., 2013; Mohr, Burns, Schueller, Clarke, & Klinkman, 2013; Schickedanz et al., 2013).
Los Angeles County Department of Health Services (LAC-DHS), the second largest safety net care system in the United States, based in part on our previous studies of social work clinical roles (Hay, Katon, Ell, Lee, & Guterman, 2012; Katon et al., 2012; Lê Cook, Doksum, Chen, Carle, & Alegria, 2013), has begun to hire licensed clinical social workers (LCSWs). Their primary roles are to engage patients and to provide counseling therapy among patients with concurrent chronic illness, such as diabetes and congestive heart failure. Its Division of Research and Innovation spearheaded a disease management program (DMP) for high-risk or high-utilization patients with a web-based disease management registry, which provided a fertile test bed for adopting collaborative team care models with technology.
In this article, we compare two clinical trials of adopting the collaborative care model in LAC-DHS ambulatory care clinics that are comparable in focusing on predominantly Latino type 2 diabetes patients suffering from depression. Both trials activated social worker roles in a collaborative team model and improved patient receipt of depression care, but three different implementation approaches were used. The first trial is a randomized clinical trial, Multifaceted Depression and Diabetes Program (MDDP; Ell et al., 2010), in which grant-hired social workers dedicated to provide problem-solving therapy in support of collaborative depression care. The second trial, Diabetes–Depression Care-Management Adoption Trial (DCAT; Wu, Ell, et al., 2014), is a comparative effectiveness research (CER) in which LAC-DHS tested two depression collaborative care adoption approaches in its diabetes DMP. While both approaches used existing clinic social workers to provide depression therapy for patients, one added the use of care-management technology to assess patients periodically and to support team collaboration. They were labeled as supported care (SC) versus technology-facilitated care (TC). All the social workers in MDDP and DCAT were guided by a depression care protocol in collaboration with physicians and nursing staff. The social workers also addressed diabetes intervention, for example, provided problem-solving therapy in which depressed patients were encouraged to keep their clinic appointments, take their prescribed medicine, and talk with their doctor. Both studies provided training to the physicians, nursing staff, and social workers about collaborative depression care management by late Dr. Wayne Katon, a psychiatrist who codeveloped the collaborative team depression care model (Katon et al., 2010).
We pooled data from these two trials and compared the pre–post differences of the three alternative collaborative care approaches—MDDP, SC, and TC—on depression treatment receipt and symptom improvement at 6 and 12 months post-enrollment. Understanding the variability and effects of the implementation approaches can support effective adoption of collaborative team care model.
Method
Comparative Study Groups
MDDP
The MDDP randomized clinical trial was conducted in two LAC-DHS public community clinics for adult patients with diabetes and depression. Trial design included enhanced usual care versus intervention (INT) social work problem-solving therapy over 12 months that included encouraging patients with severe depression to also take antidepressant medication (Ell et al., 2010). INT, the only group included in the present study, was aimed at identifying the effectiveness of team care that included bilingual master’s degree social workers, a social worker assistant patient navigator, a consulting psychiatrist, and when indicated, patient’s primary care physician-prescribed antidepressant medication. The social workers also routinely communicated with the patient’s primary care physician about patient’s need for an antidepressant and reported patient suicidal ideation.
DCAT
The DCAT clinical trial was aimed at accelerating the adoption of collaborative depression care in safety net clinics through design, development, and testing of a care-management technology to activate providers and engage patients (Di Capua & Wu, 2014; Ramirez et al., 2016; Vidyanti, Wu, & Wu, 2015; Wu, Vidyanti, et al., 2014). It used a CER design to conduct a quasiexperimental study comparing three delivery models in three groups of clinics in LAC-DHS: usual care, SC, and TC (Ell, Katon, Lee, Guterman, & Wu, 2015; Jin, Wu, & Di Capua, 2015; Jin, Wu, Vidyanti, Di Capua, & Wu, 2015; Wu, Ell, et al., 2014; Wu, Jin, et al., 2014). Only SC and TC involved social workers and were included in this study. DCAT recruited both depressed and nondepressed patients with type 2 diabetes; the present study focused on the subsample of depressed patients at baseline.
The MDDP trial was conducted within two LAC-DHS clinics and approved by the University of Southern California Health Services institutional review board (IRB). DCAT was conducted in eight LAC-DHS clinics (including those two in MDDP) and approved by the University of Southern California, Olive View UCLA Medical Center, and the Los Angeles Biomedical Research IRBs. In both studies, bilingual study recruiters used the same but two inclusion and exclusion criteria to identify adult patients 18 years or older with type 2 diabetes from medical charts. The only different eligibility criteria are that DCAT patients must have a phone (a landline or cell phone) because the DCAT interventions require telephone communication and that the SC and TC patients were enrolled in the LAC-DHS DMP. The complete set of patient data collection instruments was primarily identical for the two studies and was described in detail elsewhere (Wu, Ell, et al., 2014) except for the DCAT technology acceptance questions (Ramirez et al., 2016).
We pooled 191 depressed patients in the MDDP social workers intervention group, 113 depressed DCAT patients in the social workers SC, and 92 depressed patients in the TC. Inclusion criteria for clinically significant depression were defined as endorsing at least one cardinal symptom of depressed mood or loss of interest more than half the days over the past 2 weeks, plus having a Patient Health Questionnaire-9 (PHQ-9; Kroenke & Spitzer, 2002) total score ≥10.
MDDP, SC, and TC approaches to collaborative care model adoption
Similarities among the three approaches include using problem-solving therapy materials that were culturally adapted in eight areas: language—for example, literacy and idiomatic; persons—bilingual staff; metaphors—use of sayings or “dichos” in treatment sessions; content—cultural values recognition and knowledge; concepts—treatment concepts sensitive and consistent with culture and context; goals—for example, sensitivity to cultural values; methods—problem-solving therapy (PST)-provided homework handouts and examples in Spanish and consistent with culture; and context—consideration of patient’s health, socioeconomic, and home/family environment. All MDDP, SC, and TC patients were given English and/or Spanish patient-focused and family-focused depression educational materials, including a photo storybook fotonovela designed specifically for people with low health literacy (Unger, Cabassa, Molina, Contreras, & Baron, 2013) and a community, financial, social services, transportation, and child care resource list. All interventions provided clinic primary care physicians and nursing staff a depression treatment didactic session by the study’s consulting psychiatrist at study onset and a refresher midway.
A structured stepped care algorithm was also applied in all three approaches which was derived from evidence-based practice guidelines for primary care and was responsive to known barriers to depression treatment among Latinos with stress-related needs and cultural values (Ell et al., 2009; Fernandez y Garcia, Franks, Jerant, Bell, & Kravitz, 2011). Sociocultural enhancements included psychoeducation to dispel treatment misconceptions, reduce stigma, and enhance therapeutic alliance. However, only MDDP allowed patient choice of social worker problem-solving therapy, an antidepressant, or both. SC and TC asked patients to try an antidepressant as the first line of treatment and reserved social worker problem-solving therapy to those patients who failed to improve with antidepressant treatment due to cost and workload concerns of clinic social workers.
The MDDP intervention used grant-hired dedicated bilingual clinical social workers to provide problem-solving therapy and monitor patient depression status. The social workers routinely consulted the consulting psychiatrist and communicated with the clinic physicians about prescribed antidepressant efficacy/side effect and dosage/augmentation, provided 12-month telephone symptom monitoring, and encouraged treatment maintenance and relapse prevention patient self-care (Figure 1). The social workers were assisted by a patient navigator to address patient social–contextual barriers.
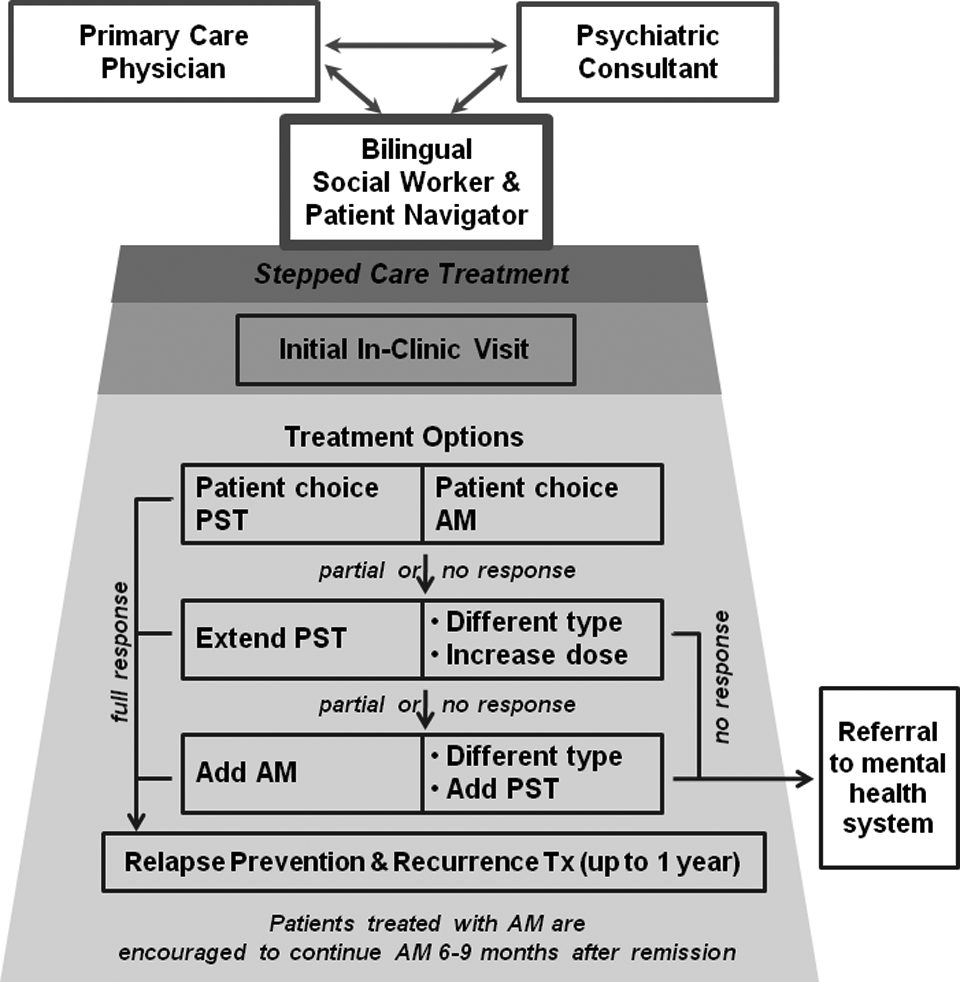
Multifaceted Depression and Diabetes Program collaborated depression care model.
The SC and TC interventions enhanced LAC-DHS outpatient DMP via addressing concurrent depression among diabetes patients to improve health-care outcomes. The disease management team included nurse care managers, nurse practitioners, social workers, and a consulting/supervising physician to provide care management designed to proactively identify, risk stratify, and treat patients using clinical protocols that emphasize patient empowerment. The program was nurse-driven and physician supervised, with nurses establishing continuity relationships with patients and using structured tools to deliver more than 80% of the care. Prior to the DCAT, PHQ-9 screening was already part of the initial evaluation that took place at the first in-person encounter, and antidepressant treatment was used.
In DCAT, the SC and TC providers received training of the stepped care algorithm and problem-solving therapy, and the clinic social workers were activated with primary role of patient depression counseling. After 6 months of disease management, patients were discharged and returned to their primary care.
TC intervention added monthly automated telephonic assessment (ATA) for depression symptom and treatment monitoring that was tailored to patient conditions and preferences over 6 months post-DCAT enrollment (Figure 2). ATA patient call results were integrated into the LAC-DHS diabetes disease management registry to deliver provider notifications; generate tasks to coordinate team care among social workers, disease management nursing staff, and physicians if patients’ PHQ scores were 8 or higher (range 0–27); and issue critical alerts of suicidal ideation for immediate response (see Wu, Vidyanti, et al., 2014, for more detail). The automated calls continued for another 6 months after patients were discharged and returned to their primary care providers, but the care-management technology limited provider notification and no more tasking due to provider workload issue. Notifications of the call results were e-mailed to patients’ primary care providers only if patients’ PHQ scores were 18 or higher.
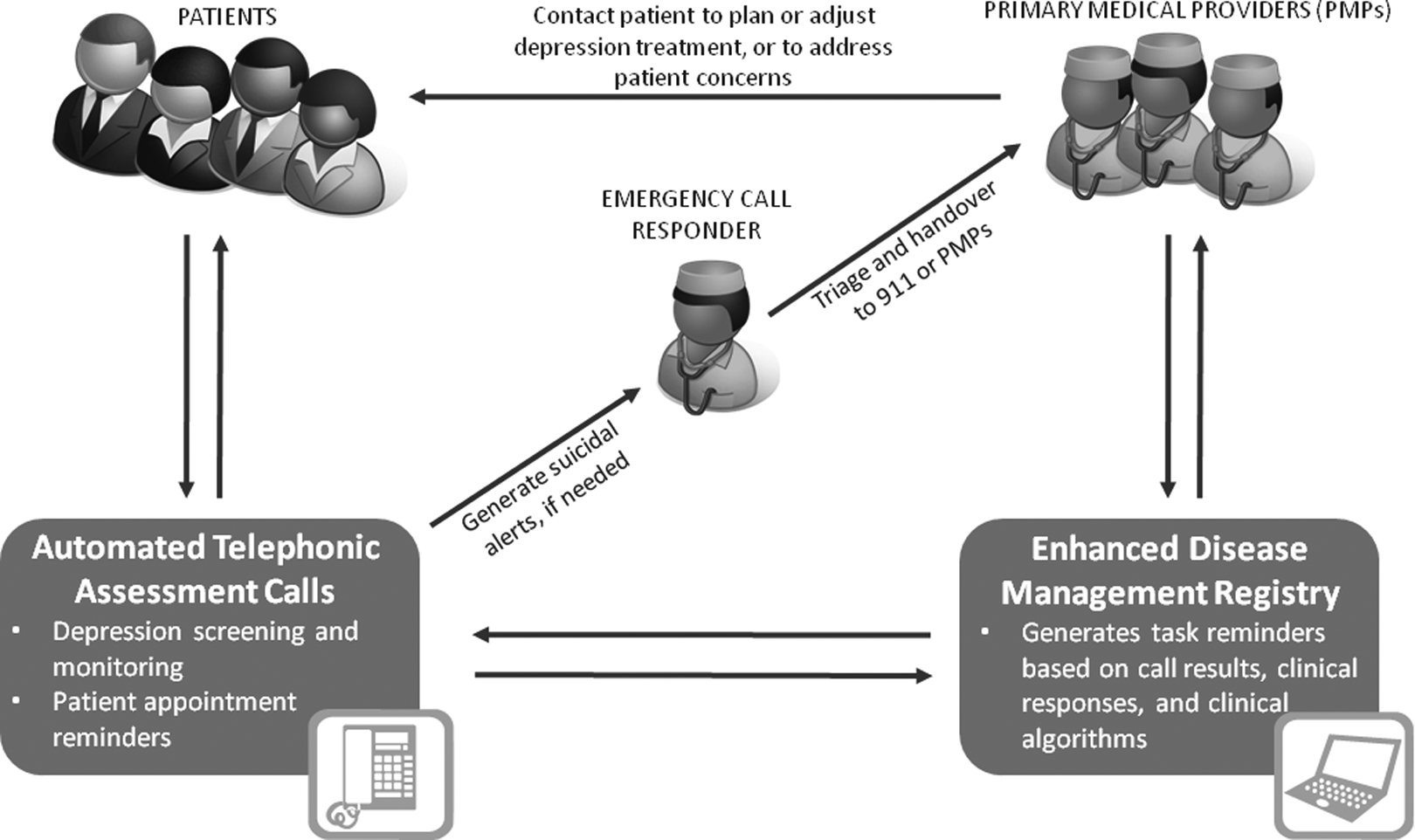
Diabetes–Depression Care-Management Adoption Trial technology-facilitated care-management model.
Data Collection
The analyzed sample is presented in Figure 3. Study participants received comprehensive assessments at baseline, 6 months, and 12 months by independent English–Spanish bilingual interviewers. Depression was assessed with PHQ-9 (Kroenke & Spitzer, 2002), which is a reliable depression screening tool with a demonstrated ability to identify clinically important depression, to monitor the severity of depression over time, and to monitor significant improvement in response to therapy. Health-related quality of life was assessed using the Medical Outcomes Study Short-Form Health Survey (SF-12; Ware, Kosinski, & Keller, 1996). Physical and Mental Component Summary norm-based scores standardized to the general U.S. population with a mean of 50 (SD = 10). The SF-12 includes 1 item for self-rated general health condition (1 = poor, 5 = excellent) and one measure of pain impact that asks respondents to rate pain interference with normal work on a 5-point scale (1 = not at all, 5 = extremely). Functional impairment was assessed by the Sheehan Disability Scale which rates impairment on a 10-point Likert-type Scale (10 indicating inability to carry out work and social roles; Sullivan, Katon, Russo, Dobie, & Sakai, 1993). Body mass index (BMI) was calculated from self-reported weight and height.
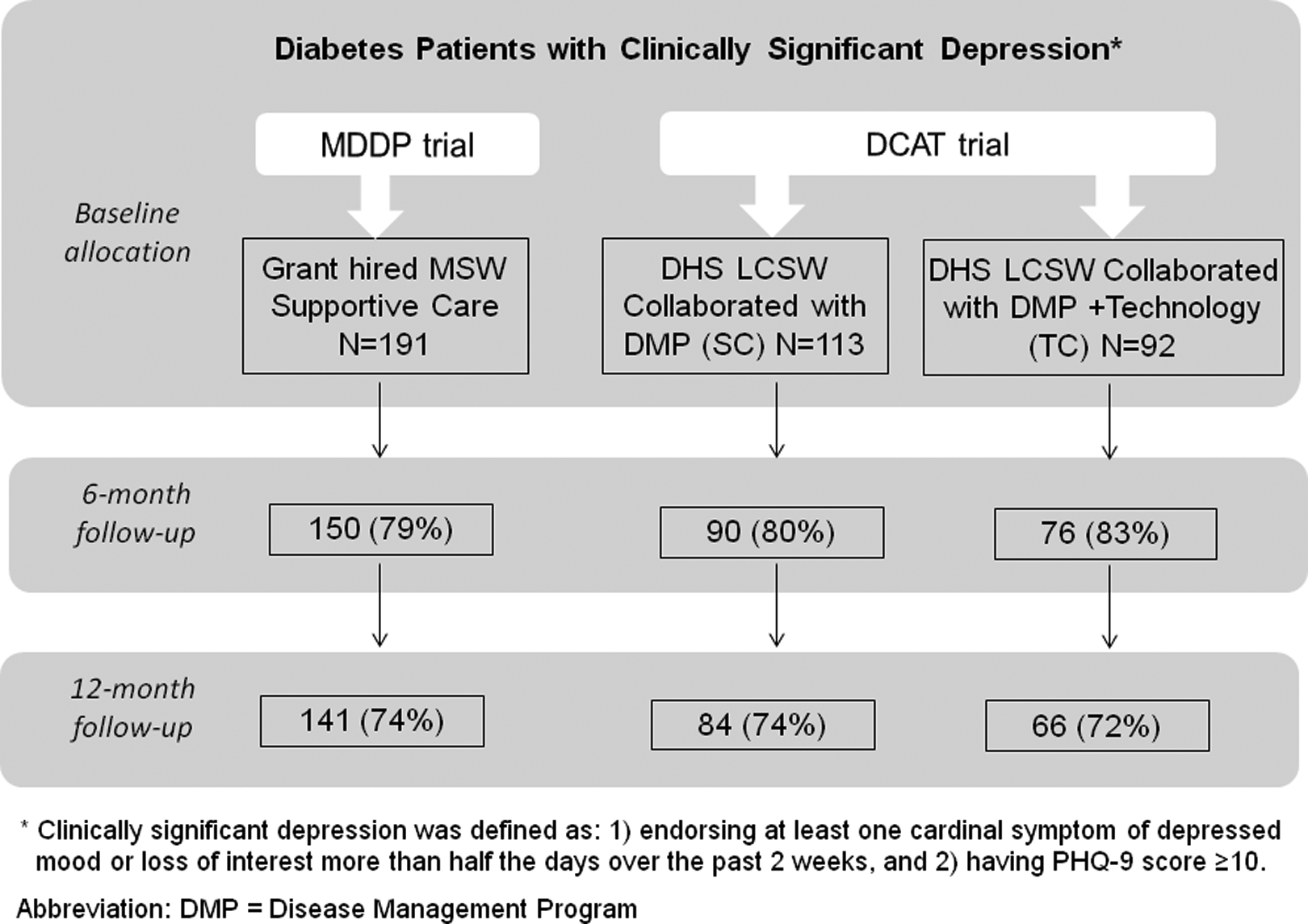
Study sample.
Diabetes symptoms were assessed using the Whitty 9-item questionnaire (Whitty et al., 1997), which has been demonstrated to change over time with effective diabetes treatment. Common diabetes complications (vision problem, kidney problem, loss or decrease of feeling in feet or legs, foot ulcer or infection, amputation, sexual impairment, and heart attack or cardiac procedure to clear up blocked vessel) were assessed by a checklist. Glycated hemoglobin A1C was obtained from medical records, reported in both National Glycohemoglobin Standardization Program A1C (%) and the International Federation of Clinical Chemistry (IFCC) Working Group developed worldwide IFCC (mmol/mol) units (Hanas, John, & International HbA1c Consensus Committee, 2010). The Summary of Diabetes Self-Care Activities measure assessed five aspects of the diabetes regimen: general diet, specific diet, exercise, blood glucose testing, and foot care. Respondents report on the frequency (number of days) with which they performed various activities over the previous 7 days (Toobert, Hampson, & Russell, 2000). Other medical comorbidity was assessed using a checklist of 10 common medical conditions (hypertension, heart disease, arthritis, retinopathy, gastrointestinal, kidney, lung disease, stroke, cancer, urinary tract, or prostate problem).
Statistical Analysis
Simple descriptive statistics (percentage, mean, and standard deviation) of demographics, baseline depression status, and clinical variables were reported by study group. To evaluate depression treatment receipt, symptom improvement, and patient quality of life effect of each collaborative care adoption approach, pre–post differences of each follow-up assessment (6 and 12 months) were compared to their baseline assessment individually. Clinically meaningful improvement of depressive symptoms was assessed as a ≥50% score reduction from baseline PHQ-9; depression remission was assessed by PHQ-9 score <5. The before and after matched pairs data testing agreement since baseline were evaluated using McNemar’s χ2 tests at each follow-up assessment for each adoption approach individually. Physical, functional, diabetes self-care quality of life measures pre–post changes were compared from baseline to each follow-up phase in paired t tests. All statistical analyses were conducted at .05 significance level (two-tailed) using SAS software, Version 9.3 (SAS Institute Inc., Cary, NC).
After pre–post differences with statistical significance for each approach were calculated, these were used in the descriptive head-to-head comparison of the three approaches. Between-group statistical pairwise comparisons were not attempted because of the significant differences of the three study samples (Table 1).
Demographics and Baseline Clinical Characteristics of Study Sample.
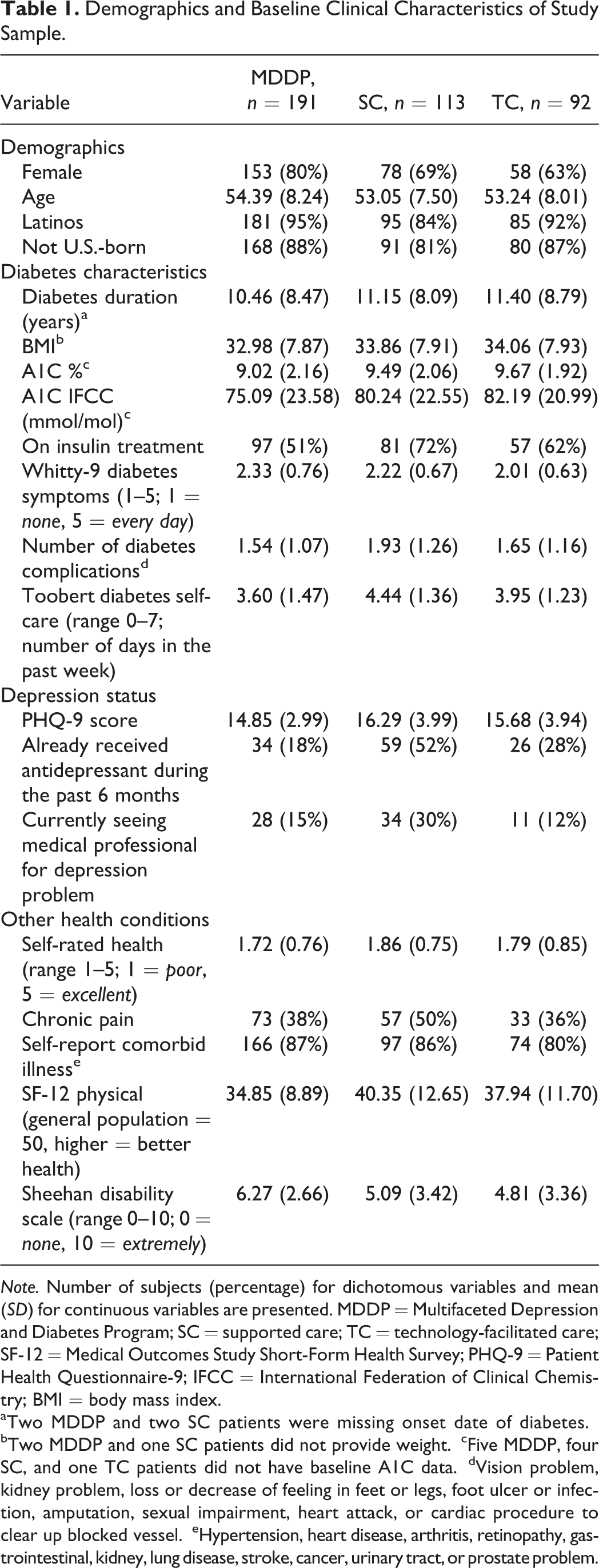
Note. Number of subjects (percentage) for dichotomous variables and mean (SD) for continuous variables are presented. MDDP = Multifaceted Depression and Diabetes Program; SC = supported care; TC = technology-facilitated care; SF-12 = Medical Outcomes Study Short-Form Health Survey; PHQ-9 = Patient Health Questionnaire-9; IFCC = International Federation of Clinical Chemistry; BMI = body mass index.
aTwo MDDP and two SC patients were missing onset date of diabetes.
bTwo MDDP and one SC patients did not provide weight.
cFive MDDP, four SC, and one TC patients did not have baseline A1C data.
dVision problem, kidney problem, loss or decrease of feeling in feet or legs, foot ulcer or infection, amputation, sexual impairment, heart attack, or cardiac procedure to clear up blocked vessel.
eHypertension, heart disease, arthritis, retinopathy, gastrointestinal, kidney, lung disease, stroke, cancer, urinary tract, or prostate problem.
Results
Table 1 provides patient baseline demographic data, depression status, diabetes, and other health conditions in each collaborative care adoption approach. Of the 396 pooled study samples, 91% patients were Latinos, foreign born (the majority from Mexico, 63%; El Salvador, 8%; and Guatemala, 7%). Although about 95% of these immigrants had lived in the United States for 10 years or longer, more than 90% were primary Spanish speaking. Over 70% of study participants had less than high school education, age ranged 22–78 with a mean of 54 years (SD = 8). These are representative characteristics of the LAC-DHS population. The average duration of diabetes was 10.9 years (SD = 8.4), and mean BMI was 33.5 Kg/m2 (SD = 7.9). TC and SC participants were enrolled from the LAC-DHS diabetes DMP specialized in the treatment of diabetes and comorbid illnesses for high-risk or high-utilization patients. Compared to MDDP group, TC and SC had more male participants (TC, 37%; SC, 31%; MDDP, 20%), more patients on insulin treatment (TC, 62%; SC, 72%; MDDP, 51%), higher A1C (TC, 9.7%; SC, 9.5%; MDDP, 9%), and self-reported more number of diabetes complications (TC, 1.65; SC, 1.93; MDDP, 1.54). These patient baseline differences were expected because SC and TC participants were enrolled from the LAC-DHS diabetes DMP for high-risk or high-utilization patients.
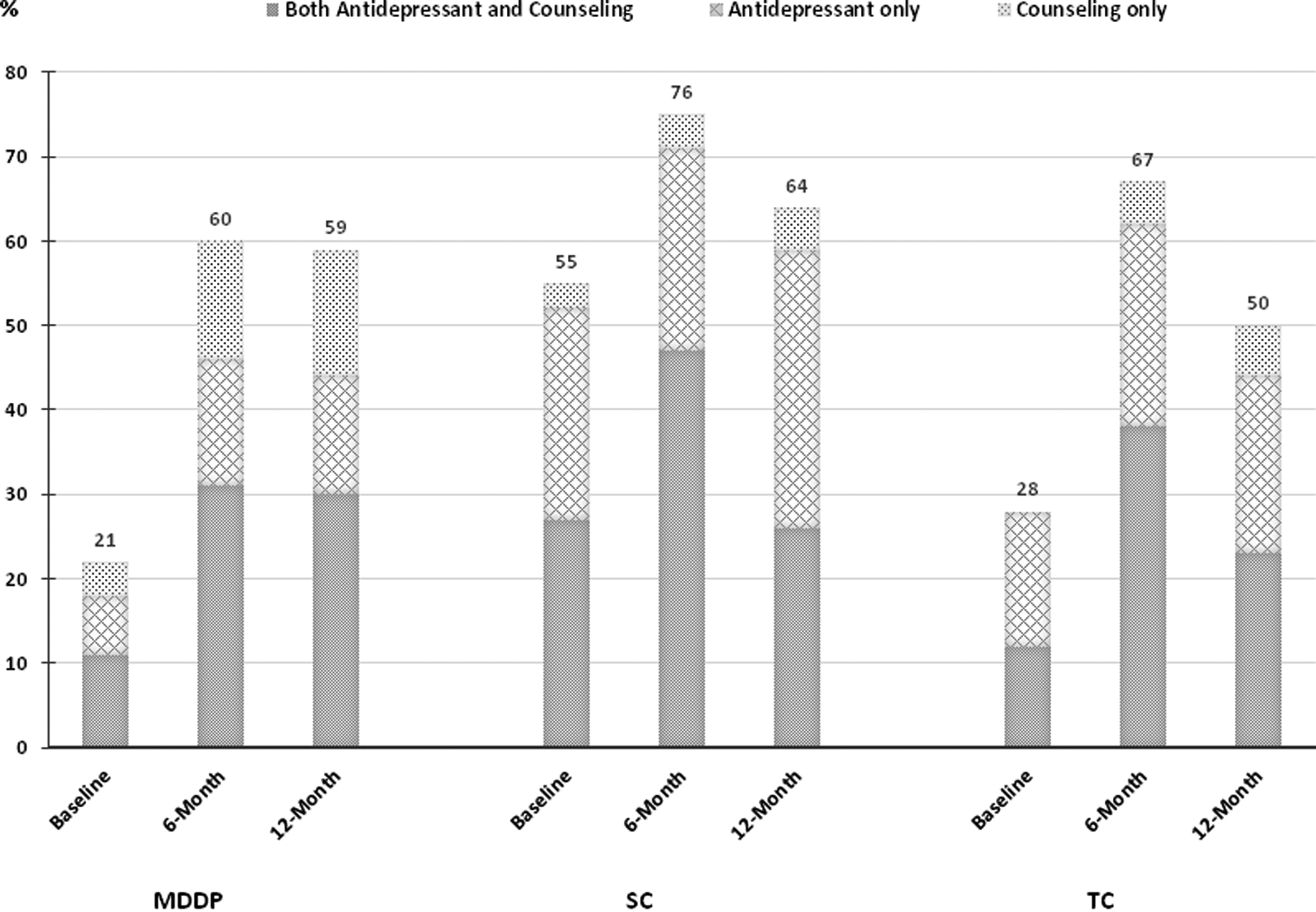
Table 2 presents depression treatment receipt at each follow-up phase and depression symptom improvement since baseline assessment for each adoption approach. SC and TC patients had more severe depression at baseline (mean PHQ-9 score: SC, 16.3; TC, 15.7; MDDP, 14.8), although 55% SC and 28% TC had already seen medical professional for depression and/or been prescribed antidepressant compared to 21% among MDDP patients. Depression treatment rate was significantly gained at 6 months for each adoption approach (treatment rate increase: SC, 20%; TC, 30%; and MDDP, 40%). With dedicated social workers still providing intervention, MDDP had a sustained treatment rate at 12 months. However, the treatment rates were reduced by more than 10% in SC and TC when patients were no longer in the DMP at 12 months (Figure 4).
Depression Treatment and Symptom Improvements.
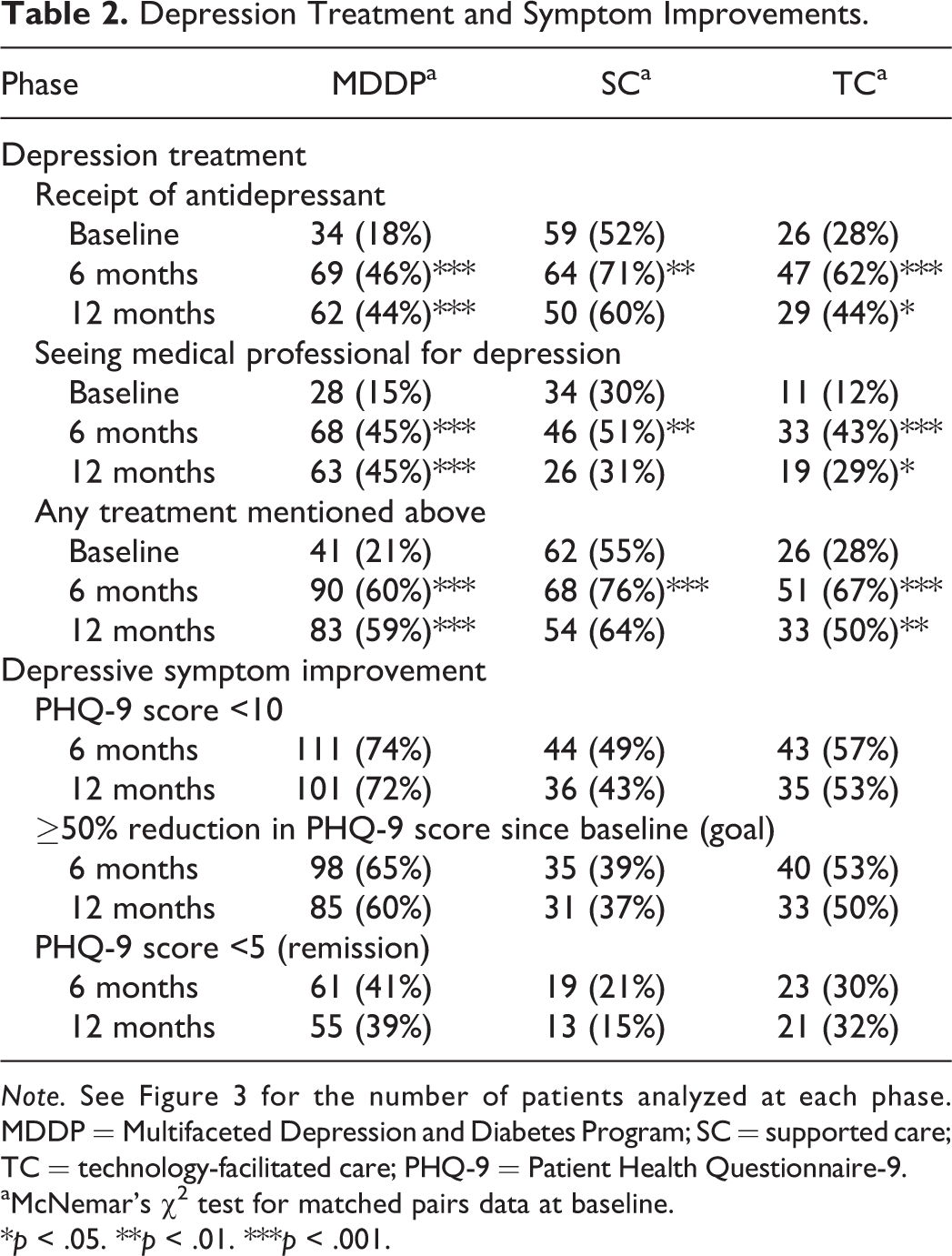
Note. See Figure 3 for the number of patients analyzed at each phase. MDDP = Multifaceted Depression and Diabetes Program; SC = supported care; TC = technology-facilitated care; PHQ-9 = Patient Health Questionnaire-9.
aMcNemar’s χ2 test for matched pairs data at baseline.
*p < .05. **p < .01. ***p < .001.
Depression treatment.
Table 2 also shows that a significant portion of patients had PHQ-9 depression score reduced under 10, a cutoff for major depression, over observed 12 months (MDDP, 74% and 72%; TC, 57% and 53%; SC, 49% and 43% at 6 and 12 months, respectively). A higher proportion of MDDP patients had clinically meaningful depression symptom improvement in ≥50% depression score reductions at follow-up assessments (65% and 60%) versus TC (53% and 50%) and SC (39% and 37%) as well as depression remission at score less than 5 (MDDP, 41% and 39%; TC, 30% and 32%; SC, 21% and 15% at 6 and 12 months, respectively).
For each adoption approach, paired t tests were performed in pre–post study outcomes of physical, functional, and diabetes self-care change scores from baseline to each follow-up time (Table 3). The MDDP model had highly significant improvements at each follow-up assessment in self-rated general health, less pain interference with work and/or housework, less disability scale, and better SF-physical summary score compared to their baseline measures (all with p < .001). TC patients had self-rated better health at each follow-up compared to that at the baseline (all with p < .05). Although SC patients had a poorer SF-physical summary score assessed at 6 months (average score change since baseline: reduced to 2.86, p < .05), the quality of life improvements were observed in self-rated general health at 12 months (mean change 0.33 in a scale of 5, p < .01). The diabetes self-care activities change scores from baseline were significantly improved only in TC at 6 months (average increase per week: 0.63 days, p < .001).
Changes in Physical, Functional, and Diabetes Self-Care Management.
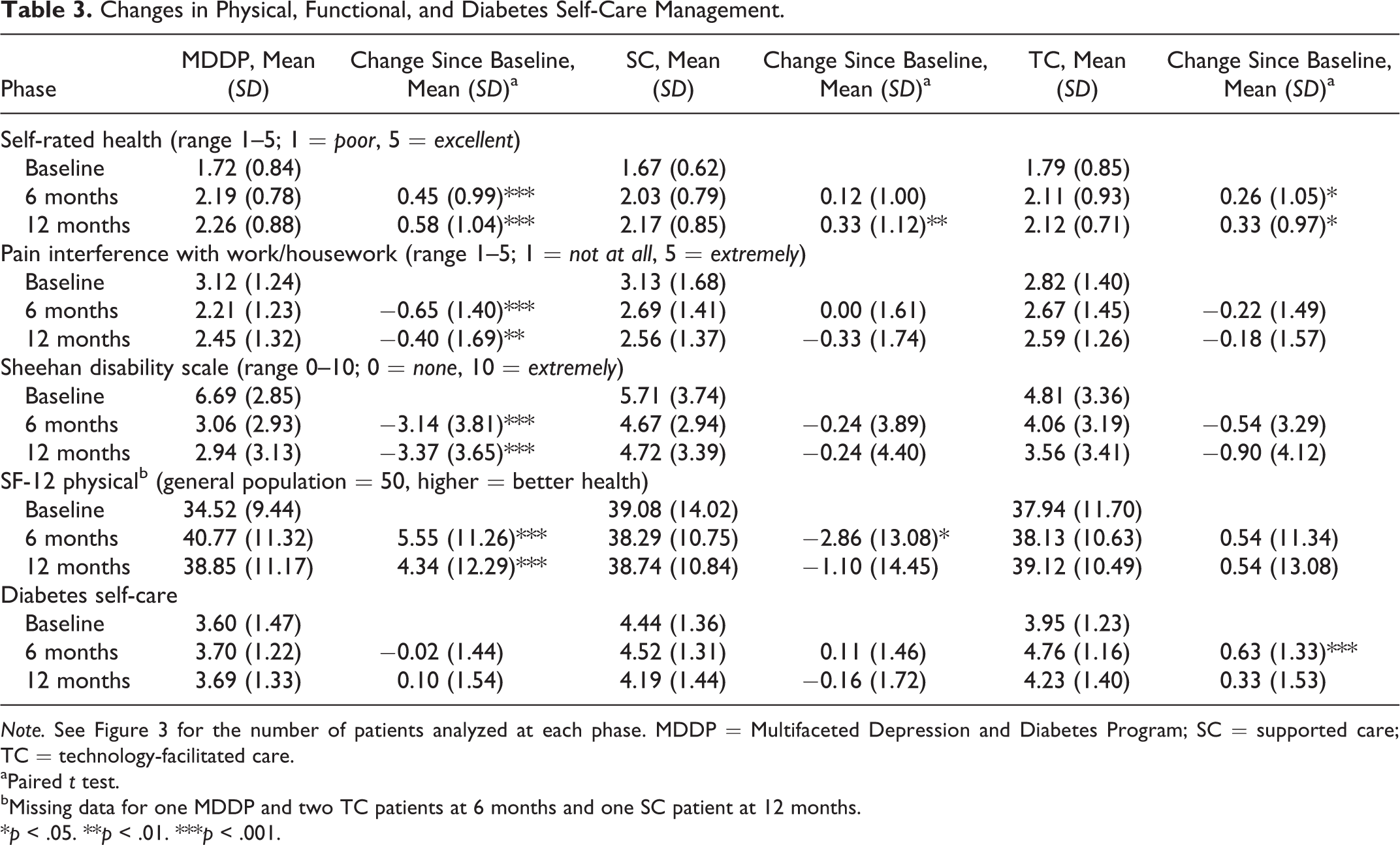
Note. See Figure 3 for the number of patients analyzed at each phase. MDDP = Multifaceted Depression and Diabetes Program; SC = supported care; TC = technology-facilitated care.
aPaired t test.
bMissing data for one MDDP and two TC patients at 6 months and one SC patient at 12 months.
*p < .05. **p < .01. ***p < .001.
Discussion and Applications to Practice
Comparison of the three approaches for adopting collaborative depression care provided practical knowledge that is highly relevant to social work practice. For example, ethnically diverse low-income patients need bilingual social workers. All three approaches activating clinical social workers in collaboration team care adoption significantly improved depression treatment receipt and symptom reduction. MDDP with dedicated bilingual social workers had the most significant effects on improving depression care receipts and patient outcomes. Compared to SC, the DCAT care-management technology facilitated greater uptake and effects of collaborative depression care and improved patient diabetes self-care when patients were in the DMP. This finding is likely attributable to the DCAT technology providing regular symptom and treatment monitoring and promoting providers to contact patients to address their depression and diabetes self-care problems.
The greater depression care improvement of MDDP in DHS was not surprising, given that it routinely implemented a standard, evidence-based stepped care algorithm (Ell et al., 2010; Katon & Guico-Pabia, 2011) by research grant–hired clinical social workers who provided undivided attention to intervention group depression care management over 12 months. Both SC and TC only had disease management team social workers for 6 months and who could only give partial attention to the study patients. Moreover, the MDDP social workers were also assisted by grant-hired bilingual patient navigators and a consulting psychiatrist. MDDP also provided patient choice of culturally adapted problem-solving therapy and community resource navigation assistance as first-line treatment option (Ell et al., 2009). Due to LAC-DHS organizational cost and social worker workload concerns, SC and TC patients received problem-solving therapy only after antidepressant treatment was used and did not work. Among Latinos, treatment is more effective if addressed with contextual stress-related needs and cultural values, that is, psychosocial therapy is frequently patient preferred over antidepressants (Ell et al., 2009; Fernandez y Garcia et al., 2011).
As the U.S. community safety care organizations move to the patient-centered medical home (PCMH) and the Affordable Care Act (ACA; Ali, Teich, Woodward, & Han, 2014), there is ongoing need to conduct further research on enhancing integrated biopsychosocial team care that includes clinical social work practitioners (Ell, Oh, & Wu, 2015). Sustainable adoption of collaborative depression care for underserved populations in safety net care systems by organizational decision makers and providers requires stable funding and qualified LCSWs. Rapidly growing health-care-management technologies can be effective in facilitating provider team access to easily applied treatment guidelines, information exchange between primary care physicians and depression care social workers, routine monitoring of patient depression symptoms and treatment adherence and satisfaction, and treatment decision consistent with patient preferences. The DCAT technology demonstrated an effective approach to enhance collaborative care model through integrating depression care within existing LAC-DHS disease management team care. It supported team care management by improving depression screening and treatment monitoring and by activating provider communication and care coordination among clinical social workers, clinic physicians, and nursing staff.
Currently, safety net care organizations, including LAC-DHS, are experiencing unprecedented organizational change driven by the ACA, increasing uptake of the PCMH models, and testing health information technology applications. The growing implementation of the ACA gives further impetus to the importance of activating health-care teams within organizational leadership-created environments that facilitate teamwork (Taplin, Foster, & Shortell, 2013). Current changing structure of delivery processes is focused on teams of clinicians working toward common patient-centered care goals, and uptake of robust health information technology (HIT) infrastructures (Blumenthal, Song, Jenna, & Ferris, 2013), aimed at achieving better interprofessional and interorganizational collaboration and continuity of care.
The present study shows activated social workers and technology facilitation provide promising effective adoption of the evidence-based collaborative team depression care in safety net clinics. However, this observational study and secondary comparison are limited in its internal validity using pre–post comparisons of each individual approach and external validity, given the primarily Latino samples. Further testing of innovative biopsychosocial team care and health technology-assisted care and building evidence on implementation and dissemination for diabetes and other chronic illness patients in safety net care are still needed (Baid et al., 2010; Pence, O’Donnell, & Gaynes, 2012; Wu, Ell, et al., 2014).
Footnotes
Authors’ Note
The opinions and conclusions expressed herein are solely those of the authors and should not be construed as representing the opinions or policy of any agency of the federal government. Trial registration: MDDP: NCT00709150 in ![]() ; DCAT: NCT01781013 in ClinicalTrials.gov
; DCAT: NCT01781013 in ClinicalTrials.gov
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MDDP RO1 MH 068468-04 randomized clinical trial was funded by the National Institute of Mental Health for which Dr. Kathleen Ell was the principal investigator. The DCAT 1R18AE000054-01 clinical trial was funded by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, for which Dr. Shinyi Wu was the principal investigator.