
Abstract
The aim of this study was to evaluate the impact of a social contact and education intervention to improve attitudes to mental illness in first-year social work students. This was a 3-month cluster randomized controlled trial with two parallel arms: intervention (87) and control group (79). The intervention was a workshop led by an OBERTAMENT activist (a person with a mental illness trained in communication skills and empowerment by a social worker). We assessed intended future behavior toward people with mental illness, personal and perceived stigma, and mental health–related attitudes (self-reported questionnaire). The intervention improved social work students’ attitudes (d ≈ 0.50, p < .05) and reduced personal stigma toward people with mental illness (d = 0.35, p = .04) as well as improving their future intended behavior 2 weeks after the intervention (d = 0.51, p = .01). The intervention impact on authoritarian attitudes toward people with schizophrenia was maintained after 3 months (d = 0.94, p = .01). Long-term impact needs to be improved.
Introduction
Prevalence of mental disorders is high among young adults and university students (Blanco et al., 2008; Chen et al., 2013; Liu, Norman, Manchanda, & De Luca, 2013; Ormel et al., 2015; Said, Kypri, & Bowman, 2013; Vázquez, Torres, Otero, & Díaz, 2011), a population that also shows high rates of mental health–related stigma (Schwenk, Davis, & Wimsatt, 2010; Yamaguchi, Mino, & Uddin, 2011). In young people and university students, stigma is a stressor that increases self-stigma (Schwenk et al., 2010), discourages help seeking (Gulliver, Griffiths, & Christensen, 2010), and triggers the development of severe mental disorders (Rüsch et al., 2015). In an effort to reduce stigma toward mental illness in a university setting, a number of interventions have been developed and tested (Yamaguchi et al., 2013). However, evidence of effective long-term interventions to reduce stigma among university students is still scarce. Most of the studies were conducted in Australia and the United States, and the vast majority of the interventions were directed to mental health professionals, especially psychiatrists, psychologists, and nurses.
Social work students are an especially relevant target group for mental health antistigma campaigns. Social workers incorporate the social component in the care of people with mental illness by guaranteeing continuity of care and providing access to the necessary resources to achieve social integration and reinsertion in the community (Towns & Schwartz, 2011). Thus, it is essential that social workers have a positive attitude toward people with mental illness. However, social work students hold stigmatizing attitudes toward people with mental illness (Covarrubias & Han, 2011).
Stigma can be explained in terms of the cognitive and behavioral constructs of stereotypes, prejudice, and discrimination (Corrigan & Shapiro, 2010). Stereotypes are beliefs about a specific social group that are learned by individuals, while prejudice is the attitude of individuals toward the specific social group. Discrimination, the behavioral construct of stigma, is the behavioral consequence of stereotypes and prejudice. In Link and Phelan’s conceptualization of stigma, stigma is explained by the convergence of several interrelated components. According to Link and Phelan (2001), stigma exists when people distinguish and label human differences and links labeled people to negative stereotypes. Labeled persons are placed in distinct categories and experience status loss and discrimination. To fight stigma, we need to change the attitudes and beliefs of powerful groups, but this changes also have to be reflected in behavior changes (Corrigan & Shapiro, 2010; Link & Phelan, 2001).
Desire for social distance and restrictions on people with a mental illness in social work students were associated with stereotypes of dangerous behavior, and it was suggested that interventions aimed at social work students may benefit from using social contact as a strategy to reduce stigma (Covarrubias & Han, 2011). Active forms of education based on a combination of formal discussions and simulations lead to greater results on mental health stigma reduction than formal lectures alone (Corrigan & O’Shaughnessy, 2007; Corrigan & Penn, 1999), and different studies support the idea of supplementing education with face-to-face contact to maximize effectiveness (Corrigan & O’Shaughnessy, 2007; Corrigan & Penn, 1999; Pinfold et al., 2003; Rickwood, Cavanagh, Curtis, & Sakrouge, 2004; Schulze, Richter-Werling, Matschinger, & Angermeyer, 2003). To maximize the performance of social contact interventions, programs should emphasize recovery and success, include live testimonies of trained people who have experienced a mental illness, refute myths about mental illness, use multiple forms of social contact, focus on behavior change by teaching skills on what to say and what to do, and include an enthusiastic instructor who uses a person-centered approach rather than a pathology-first perspective (Knaak, Modgill, & Patten, 2014).
To the best of our knowledge, only two studies have evaluated the impact of interventions to reduce mental health–related stigma in social work students (Lewis & Frey, 1988; Shera & Delva-Tauiliili, 1996). Both interventions included a contact component—with parents of chronically mentally ill adults (Lewis & Frey, 1988) and with consumers of mental health services with severe mental illness (Shera & Delva-Tauiliili, 1996)—and evaluated changes in attitudes and/or social distance immediately after the intervention. Social work students showed improvements in attitudes toward people with mental illness (Shera &Delva-Tauiliili, 1996) and parents of people with mental illness after the intervention (Lewis & Frey, 1988) but not in social distance. These studies used small sample sizes and external control groups (students on other courses) which could have introduced some bias and only evaluated the short-term impact of the intervention.
The aim of this study was to evaluate the impact of a social contact and education intervention in comparison with a waiting list approach in the improvement of stigma in the first-year social work students using a cluster randomized-controlled trial (RCT) with a 3-month follow-up.
Method
This was a prospective cluster RCT with cluster assignment by class and two parallel arms with wait-list control.
Sample Selection
A convenience sample of social work undergraduate students was used. Eligible participants were all the students enrolled in the first-year mandatory subject “Initiation to Social Work Practice and Knowledge of Social Services” of the Social Work Degree of the University of Barcelona. After the Bologna Accord in 1999, the Social Work Degree in Spain can be validated in the different European Union countries, and the degree courses are designed according to the directives set by the European Higher Education Area. Those students who attended class when the study was presented and who were willing to participate in the research were included. No other inclusion criterion was used. Taking into account the low level of risk of the study and that the questionnaires were anonymous, a passive consent was obtained: The research was explained to the students at the beginning of the session and students were told that participation was voluntary and that they only had to complete the survey if they were willing to participate. Students were considered to have agreed to participate if they completed the survey. An anonymous identifier (a combination of the last four digits of a student’s identity card number and the two first letters of their surname) was used to ensure students’ confidentiality.
Randomization
The students were divided into eight classes (four morning schedule and four evening schedule), which were randomized in a 1:1 ratio to the intervention group and control group by a member of the OBERTAMENT antistigma alliance using a manual technique without stratification. A parallel cluster randomization was used to prevent contamination between students in the same class.
The students were enrolled by a social worker from the OBERTAMENT antistigma alliance before randomization, and treatment allocation was kept by the research team until all the groups were ready to implement the intervention. All the students who fulfilled the inclusion criteria were invited to participate (complete enumeration).
Interventions
Students in the class randomized to the intervention group received the intervention during the first day of class. The intervention took place in the classrooms using the available classroom materials (computer and projector). The intervention aimed to educate and sensitize the students toward the problems faced by people diagnosed with a mental disorder. The intervention consisted of a 1-hr workshop led by an OBERTAMENT activist (“OBERTAMENT Webpage Activists”). These activists are people with a mental illness who have received nine training sessions with a social worker to improve their communication skills and empowerment.
First, the activists briefly described the OBERTAMENT project and its objectives and students were invited to participate in a dynamic group conversation to estimate and discuss the high prevalence of mental health problems. The key message was “According to the World Health Organization, one in four people will have a mental health disorder during life.” Next, the activists offered a lecture focused on mental health, diagnoses of mental health problems, stigma, discrimination, and social exclusion. The OBERTAMENT advertisements that had been used during the 2012 social-marketing campaign were used as a didactical tool. The educational component on the intervention wanted to reinforce the idea that mental illness is commonplace and was focused on breaking stereotypes and reducing prejudice. Following this, activists gave a first-person account of how they coped with mental ill-health and described how discrimination had affected them throughout their life. Students were invited to ask the activists questions and they were provided with information on family support organizations. The contact component of the intervention had a recovery emphasis and tried to refute myths about mental illness and recovery.
Finally, conclusions from students were shared, and the activists concluded the workshop with a motivational reflection, “having a positive attitude to people with mental health issues is essential in your future professional work.” The intervention tried to challenge stereotypes about mental illness, improving attitudes and reducing the desire for social distance and discrimination.
The control group was a wait-list group of students; the only difference between groups was the timing of the contact and education workshop. Students in the control group classes received the intervention after the last follow-up evaluation.
Outcomes
Students completed three evaluations: at baseline (before the intervention), postintervention (15 days later), and follow-up (3 months after the intervention; February–May 2014). The data were collected in the classrooms through a paper-and-pencil self-reported questionnaire. Data were collected on gender, age, contact with people having mental illness (family member, distant relative, friend, and acquaintance), and personal experience of mental illness.
Vignettes
Vignettes were used in order to assess the intended future behavior and personal and perceived stigma. The vignettes are hypothetical stories or situations in an everyday context and allow presentation of an elaborate stimulus in which measurements are based (Link, Yang, Phelan, & Collins, 2004). These vignettes were followed by questions that referred to the specific person who had been described. Two vignettes based on a study by Griffiths and colleagues were used: Maria, a girl with a depressive disorder; and Joan, a man with a schizophrenic disorder (Table 1; Griffiths et al., 2006). Depression and schizophrenia were selected because they are the prevalent major mental disorders and because the potential differences in beliefs associated with the two diseases could generate differences in stigma and preferred social distance. The two variants of the questionnaire (depression vignette and schizophrenia vignette) were randomly distributed among students using a series of random numbers generated by computer in blocks of six, which followed a 1:1 ratio.
Depression and Schizophrenia Vignettes.

Note. NASA = National Aeronautics and Space Administration.
Intended Behavior
Four items of the Catalan version of the Reported and Intended Behaviour Scale were used to evaluate intended behavior in future contact with people having mental illness (Evans-Lacko et al., 2011). Since assessing changes in discrimination can only be achieved through direct observation of action, behavior intention has been suggested as a proxy measure of actual behavior. The scale was combined with the vignettes to assess the intention to live with, work with, live nearby, and continue a relationship with Maria or Joan in the future. The scale shown to have adequate reliability in the general Catalan population (Rubio-Valera et al., 2015). The internal consistency of the scale in our sample study population was found to be satisfactory (Cronbach’s α = .81).
Personal and Perceived Stigma
Personal and perceived stigma were measured with the Depression Stigma Scale (DSS; Griffiths, Christensen, & Jorm, 2008), which were combined with the vignettes. The scale was originally designed to assess the stigma associated with depression, but we also used it to assess the schizophrenia vignette to allow comparisons between respondents of both vignettes and to improve the feasibility of the survey in the available time. The DSS consists of two 9-item subscales: Personal Stigma subscale which evaluated the students’ own attitudes toward depression/schizophrenia and Perceived Stigma subscale which evaluated the students’ perception about the attitudes of others toward depression/schizophrenia. The DSS was used to measure changes in stereotypes and prejudice. We conducted a cross-cultural adaptation of the scale with translation and back translation. The internal consistency of the scale in our sample was of α = .72.
Attitudes
Mental health–related attitudes were measured using a Spanish 23-item version of the Community Attitudes Towards the Mentally Ill Scale (CAMI-23) that had sound psychometric properties (Rubio-Valera et al., 2015; Taylor & Dear, 1981). The CAMI-23 is rated on a 5-point Likert-type scale from “strongly agree” to “strongly disagree”; scores of negative items were reverse coded, so that higher scores indicate more favorable attitudes. The scale has three dimensions or subscales: authoritarianism (7 items), benevolence (6 items), and support for community mental health care (10 items). The CAMI-23 was used to measure changes in stereotypes and prejudice. The internal consistency of the scale in our sample was of α = .64.
Social Desirability
Social desirability was measured with 5 items of the Spanish version of Marlowe–Crowne Social Desirability Scale (MC-SDS; Crowne & Marlowe, 1960). The original scale consists of 33 true–false items. The 5 items that showed the highest discrimination index in the Spanish validation of the scale were selected (Ferrando & Chico, 2000).
Statistical Analysis
All the analyses were conducted with STATA 13.0. The full sample of first-year social work students from the University of Barcelona was used and no sample size calculation was carried out. Baseline comparability between groups was assessed using χ2 tests or Fisher’s exact test for categorical data and Student’s t test for continuous data. There were significant differences in gender and in the CAMI-23 scores between the intervention and control group at baseline. All the analyses were adjusted for gender and baseline scores.
All the participants were included in the analysis in the group to which they were randomized irrespective of whether they had missing data. To deal with missing information due to dropouts, we used multiple imputations with chained equations. We included in the imputation model all demographic and clinical variables as well as all variables used in the final models. We generated 100 imputed data sets. All the posterior analyses were conducted in each data set, and the intervention effects and variances were combined following Rubin’s rules (1988).
To evaluate the differences between groups at postintervention and follow-up, we used multilevel mixed-effects linear models using gender and baseline outcome scores as covariates in the models. A two-level structure was used, where students were clustered within classes (random factor). The a priori α level was of .05. In some of the imputed databases, convergence problems appeared. In those cases, the imputed database was excluded from the analysis. Intracluster correlation and effect size were calculated running the models again using the data set of students who completed all three evaluations of the study. Effect size (η2) was calculated for statistically significant or marginally significant differences between groups and then converted to Cohen’s d. Then, the models were fitted again to assess differences between groups dividing students in those who had been evaluated using the “depression vignette” and the “schizophrenia vignette.” Finally, we did a sensitivity analysis to evaluate if social desirability was affecting the results of the study by adjusting the models by the aggregated scores of the social desirability scale.
Results
Figure 1 shows the flowchart of the study. Eighty-seven students from the intervention classes and 79 from the control classes attended the baseline appointment, agreed to participate and were included in the study. Fifteen days and 3 months postintervention, 22 students and 36 students, respectively, missed class and were not evaluated. Sixty-four students from the intervention group and 52 from the control group performed the three evaluations of the study. The whole sample (166) was included in the analysis.
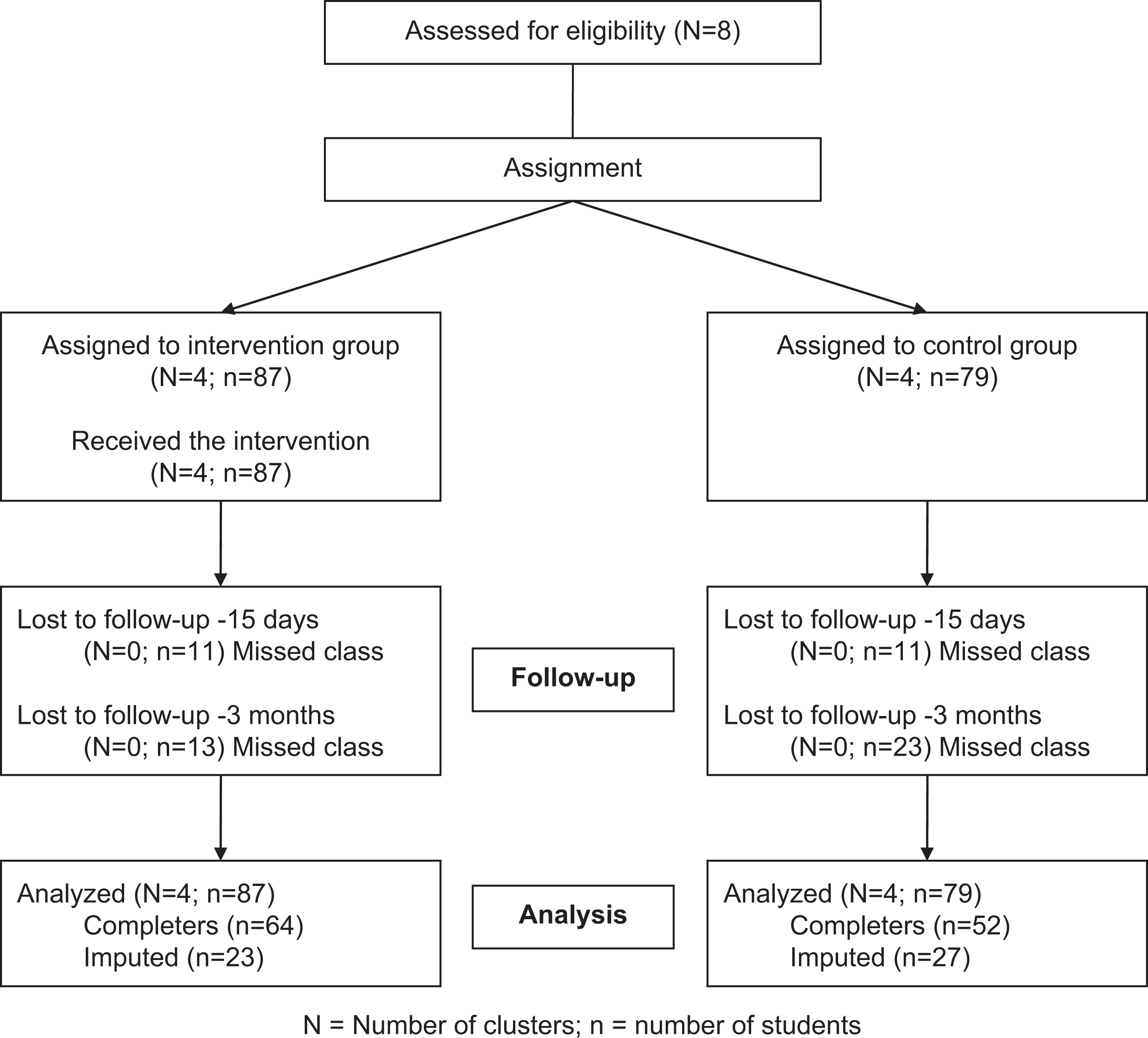
Participant flowchart.
The demographic characteristics of the sample are shown in Table 2. Almost 90% of the participants were women and the mean age was 22 years. Almost a third of the students reported having experienced a mental illness and 21% had a close relative with a mental illness. Over 80% of the students knew someone with a mental illness. Fifty-four percent of the students responded to the depression vignette. At baseline, statistically significant differences between groups in the proportion of men and women were detected (p = .022). All the subsequent analyses were adjusted for gender. There were no other statistically significant differences in demographic characteristics at baseline.
Sample Characteristics at Baseline.
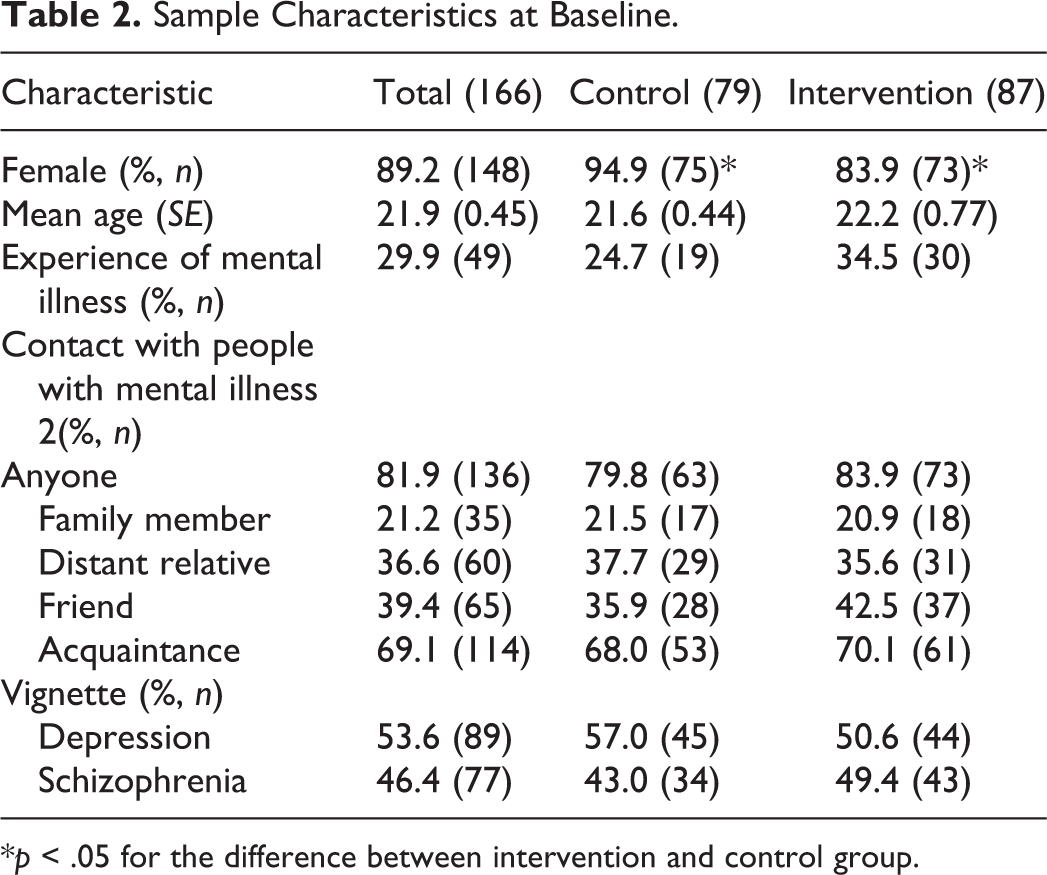
*p < .05 for the difference between intervention and control group.
Impact of the Intervention
Participants’ mean scores on attitudes, personal and perceived stigma, and intended behavior at the three assessments are shown in Table 3. At baseline, statistically significant differences between the intervention group and the control group were found in the three attitude subscales (authoritarianism, benevolence, and support for community mental health care). Students in the intervention group showed higher scores than students in the control group before receiving the intervention. No other baseline differences were found between groups. All the analyses were adjusted for baseline scores.
Means and Standard Errors for Baseline, Postintervention, and Follow-Up Test and Mean Adjusted Difference Between Groups by Outcome Measures.
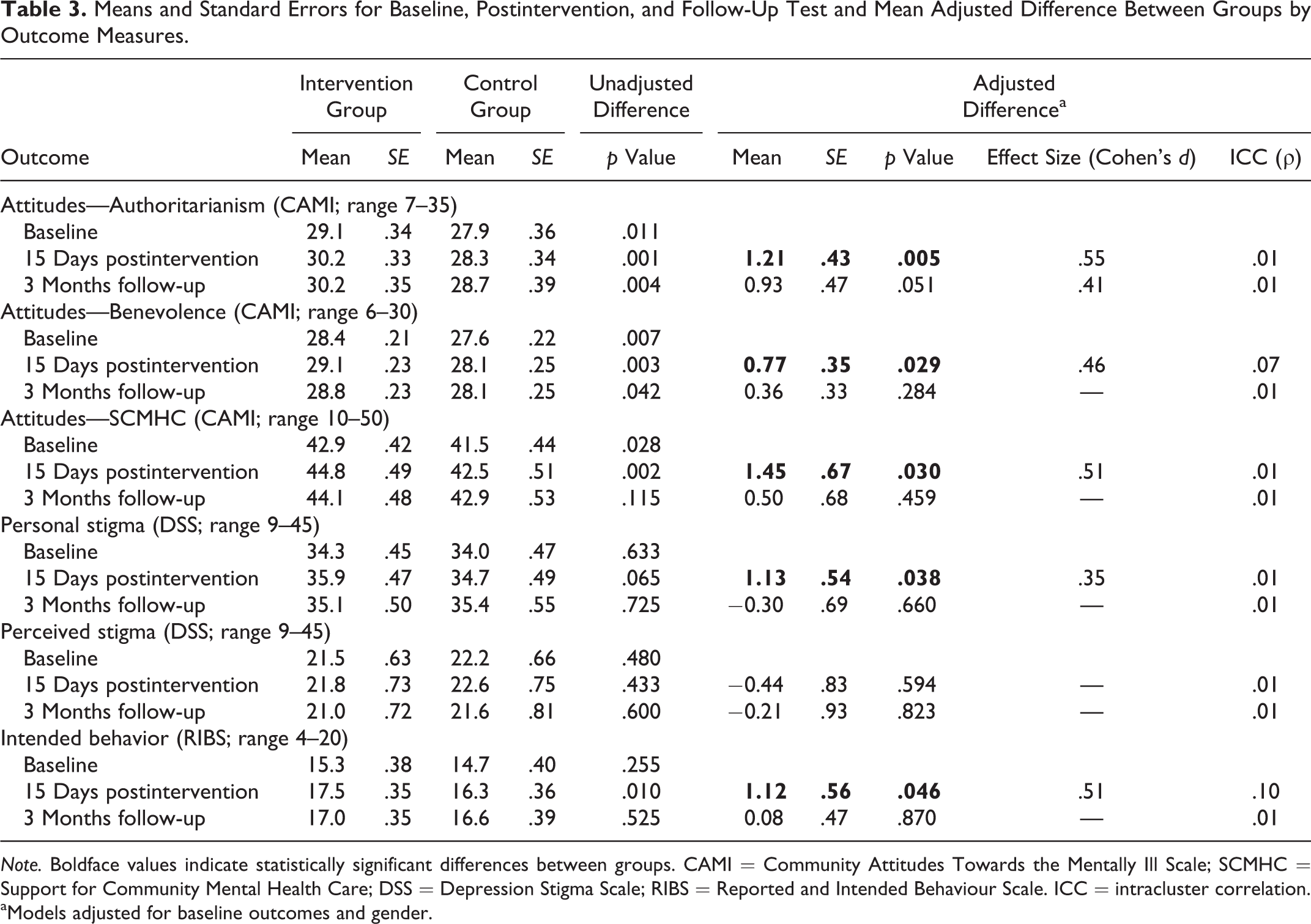
Note. Boldface values indicate statistically significant differences between groups. CAMI = Community Attitudes Towards the Mentally Ill Scale; SCMHC = Support for Community Mental Health Care; DSS = Depression Stigma Scale; RIBS = Reported and Intended Behaviour Scale. ICC = intracluster correlation.
aModels adjusted for baseline outcomes and gender.
Students in the intervention group showed better attitudes in the three subscales of the CAMI (authoritarianism, benevolence, and support for community mental health care) 15 days after the intervention (Cohen’s d = 0.55, 0.46, and 0.51, respectively), but no differences were observed between groups at 3-month follow-up.
Personal stigma was lower in the intervention group than in the control group after the intervention (Cohen’s d = 0.35) but not at the 3-month follow-up. No differences between groups were observed in perceived stigma. Similarly, the students who received the intervention showed better intended behavior than the control group only at postintervention (Cohen’s d = 0.51).
Results by Vignette
Differences in stigma between intervention and control students were assessed in the subsamples of students who had been evaluated with the depression (n = 89) and schizophrenia (n = 77) vignettes (Table 4). No differences were observed between control and intervention students responding to the questionnaire that presented the vignette of a person with depression, although the results showed a tendency toward better attitudes on benevolence and support for community mental health care 15 days postintervention.
Mean Adjusted Difference Between Groups by Outcome Measures and Vignette.a
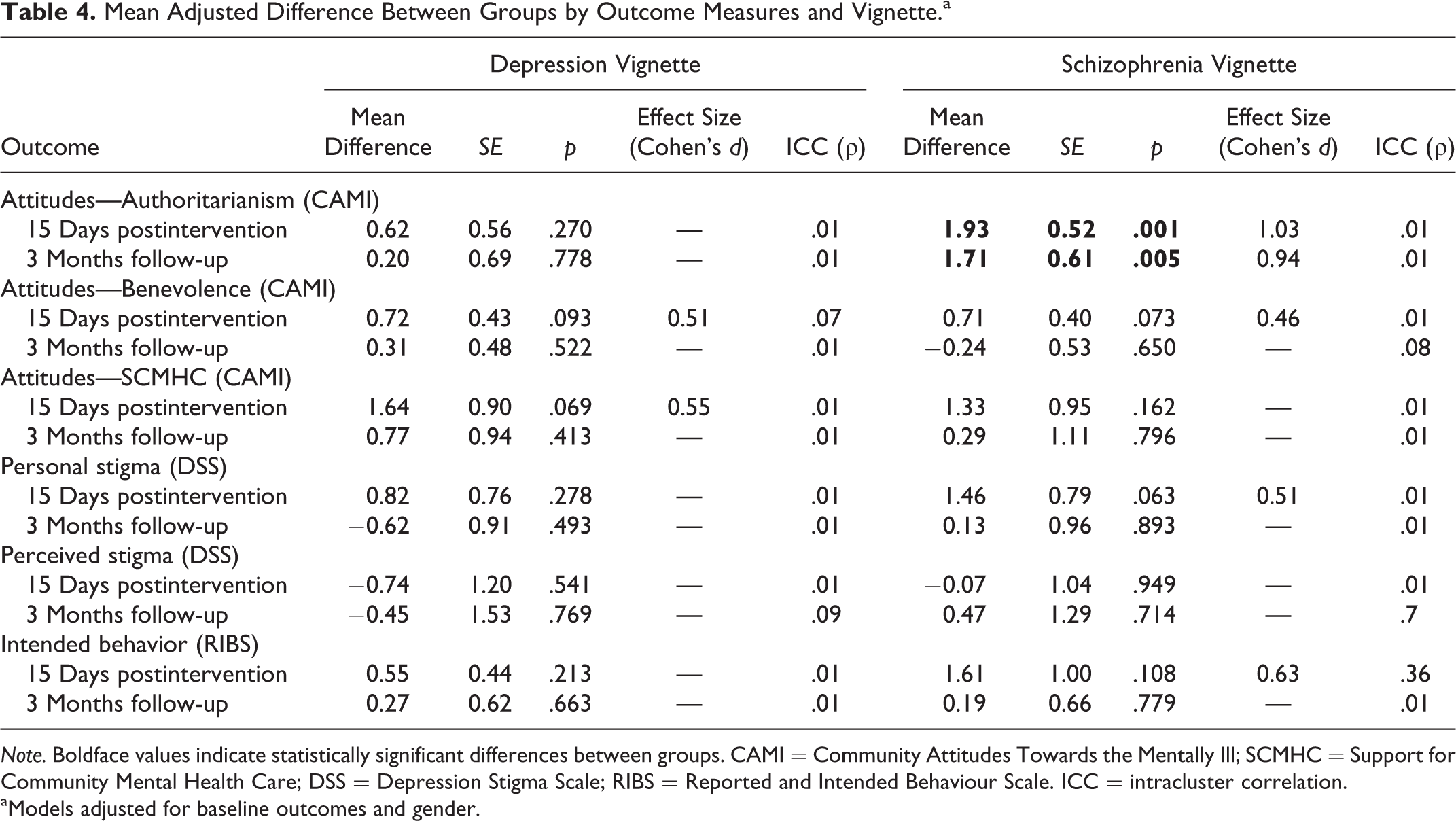
Note. Boldface values indicate statistically significant differences between groups. CAMI = Community Attitudes Towards the Mentally Ill; SCMHC = Support for Community Mental Health Care; DSS = Depression Stigma Scale; RIBS = Reported and Intended Behaviour Scale. ICC = intracluster correlation.
aModels adjusted for baseline outcomes and gender.
Within those evaluated using the schizophrenia vignette, intervention students showed better authoritarian attitudes than control students both 15 days and 3 months after the intervention. The difference was clinically relevant (Cohen’s d = 1.03 at 15 days and 0.94 at 3 months). After 15 days, better intended behavior and better attitudes toward personal stigma and benevolence were observed in the intervention class students at 15-day follow-up, but these differences did not reach statistical significance.
Impact of Social Desirability
After adjustment for social desirability, no relevant changes were observed in the results of the analyses.
Discussion and Applications to Practice
The OBERTAMENT education and contact intervention improved social work students’ attitudes and reduced personal stigma toward people with mental illness as well as their future intended behavior 2 weeks after the intervention. The intervention impact on authoritarian attitudes toward people with schizophrenia was maintained after 3 months. To the best of our knowledge, this is the first RCT that evaluates the impact of a mental health antistigma intervention on social work students, the first mental health antistigma intervention to improve intended behavior of social work students, and one of the few interventions to show impact on university students’ stigma 3 months after the intervention, although we only observed it on attitudes related to authoritarianism toward people with schizophrenia (Yamaguchi et al., 2013).
This is the first intervention to show improvements in the intended behavior of social work students (Lewis & Frey, 1988; Shera & Delva-Tauiliili, 1996). This could be explained by the content of the interventions. Social contact interventions impact stigma insofar as personal testimony effectively communicates a message of successful recovery (Knaak et al., 2014). Previous interventions promoted contact between social work students and parents of patients with severe mental illness and severely mentally ill persons who were receiving services at that time. These interventions assigned a lower status to people with mental illness and could have sent an illness-centered message. Furthermore, the OBERTAMENT intervention included some components that have been shown to improve the performance of social contact–based approaches (Knaak et al., 2014): a recovery emphasis, personal testimony from a trained speaker who has lived experience of mental illness, refuting myths about mental illness, and an enthusiastic instructor who modeled a person-centered approach.
The results of our study support results of previous studies, suggesting that educational and contact interventions are useful to reduce mental health–related stigma and improve future contact with people with mental illness (Friedrich et al., 2013; Yamaguchi et al., 2013). However, the effect was only moderate for most of the changes (Cohen’s d ≈ 0.50). Similarly to other studies, we mostly observed short-term improvements in attitudes, stigma, and intended behavior. Most short-term interventions to reduce mental health–related stigma in university students who do improve attitudes and reduce social distance achieve this immediately after the intervention and up to 1 month afterward (Friedrich et al., 2013; Yamaguchi et al., 2013). A single session could be insufficient to produce a large change in social work students’ stigma. Using booster sessions or refreshers would be necessary to increase the impact of the intervention and sustain its positive effects over time (Knaak et al., 2014). Internet programs to reduce personal stigma seem to be as effective as interventions delivered face to face (Griffiths, Carron-Arthur, Parsons, & Reid, 2014), and new technologies have been used in a university setting to deliver interventions that promote mental health in an efficient way (Braithwaite & Fincham, 2009; Griffiths, Farrer, & Christensen, 2010). New technologies could be used as a low-cost way to deliver additional contact interventions that boost the effect of a face-to-face intervention.
The 3-month impact of the intervention on authoritarian attitudes could be related to the content of the intervention: It focused on breaking stereotypes, sending a message of success and recovery, and showing that living with a mental condition is commonplace. In particular, this could have impacted the authoritarianism construct, which is represented by items stating that people with mental illness are a burden on society, should not be given any responsibility, and lack self-discipline and willpower.
A number of limitations should be considered when interpreting our results. Both intervention and control students showed improvements in attitudes, stigma, and intended behavior. We cannot be sure that there has not been contamination: Control and intervention students shared the same university and were engaged in the same course. Furthermore, OBERTAMENT was conducting a mass-media population campaign at the same time in Catalonia, and this could have reached the students. Students in the intervention group showed statistically significant better attitudes, stigma, and intended behavior than those in the control group at baseline. Adjustment was used to rectify imbalance between groups. Nonetheless, even with the possible bias introduced by contamination, other concurrent interventions, and higher baseline scores in the intervention group, we observed larger improvements in attitudes, stigma, and intended behavior in the students who received the intervention.
Time restrictions did not allow including both vignettes (depression and schizophrenia) in the questionnaire, so that we had to randomly assign one or the other to the population. Thus, we cannot be sure that differences observed between those students who responded to either the schizophrenia or the depression vignette were only due to the vignette. Also, as our sample size is limited, it is difficult to detect differences between subgroups of students responding either to the schizophrenia or to the depression questionnaire.
In spite of these limitations, this is the first RCT to evaluate the impact of a mental health antistigma intervention in social work students. Most of the literature on interventions to reduce mental health–related stigma in a university setting has quality issues mainly because of insufficient description of the randomization process, the use of nonreliable measures, and limited use of randomized controlled studies (Yamaguchi et al., 2013). The study’s intervention incorporated some of the most relevant components for social contact–based interventions (Knaak et al., 2014), used a large sample of students, and evaluated the 3-month impact of the intervention.
Future research should evaluate the impact of reminder strategies (e.g., follow-up sessions and new technologies) on the longer term impact (6 or more months) of antistigma education and contact-based interventions on social work and other university students. Although “the principles of human rights and social justice are fundamental to social work” (Workers, 2000), there is a risk that social workers’ stigma impacts negatively on people with mental illness. We need to ensure that social workers are free of stigma, and this study shows that there is scope for improvement. The university setting is ideal for working with future social workers to prevent the future negative impact of stigma on the general population. Interventions such as the OBERTAMENT intervention should be considered as crucial for the training of mental health–care providers, including social workers. The OBERTAMENT antistigma intervention had a short-term impact on social work students’ attitudes, stigma, and intended behaviors, but we should improve the intervention to achieve a higher impact and to maintain it in the long term.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The OBERTAMENT campaign was supported by the “Obra Social ‘La Caixa.’” The study was supported by the Spanish Primary Care Prevention and Health Promotion Network (redIAPP; Instituto de Salud Carlos III [ISCIII], RD12/0005/0008) and by the European Regional Development Fund (ERDF).