
Abstract
Purpose:
The objective of this article is to describe the implementation of the Skills Training in Affective and Interpersonal Regulation (STAIR), a manualized, evidence-based cognitive behavioral group treatment for childhood trauma at Cedar Centre, a community-based trauma treatment center, and describe the preliminary evaluation of the effectiveness of the treatment.
Method:
Pre- and postmeasurements of emotion regulation, interpersonal problems, and traumatic stress symptoms using psychometrically validated instruments were collected. Outcomes were assessed for 85 individuals who experienced childhood sexual abuse and participated in the first cycles of intervention at the center.
Results:
Results indicated significant reductions in difficulties in emotion regulation, interpersonal problems, and trauma symptoms among participants from pretreatment to posttreatment.
Discussion:
Overall, there was a positive response to the adoption and integration of the STAIR intervention into the program. Qualitative assessment identified the benefits perceived by both facilitators and group participants.
Keywords
In spite of the development of manualized, evidence-based treatments through clinical research, the implementation of these treatments in the “real world,” including community social work settings, has been slow (Rubin, Neal, Fenlon, Hassan, & Inouye, 2011; Thyer & Myers, 2011). The objective of this article is to recount the process through which the Cedar Centre made the shift in their adult program to include a manualized, evidence-based cognitive behavioral group treatment protocol specifically oriented toward the needs of individuals who have experienced childhood trauma, the Skills Training in Affective and Interpersonal Regulation (STAIR) treatment model (Cloitre, Cohen, & Koenen, 2006). Cedar Centre has moved toward implementing this group with an emphasis on ensuring that participants receive a treatment protocol that addresses the particular therapeutic needs of individuals who have experienced childhood sexual abuse (CSA), as well as measuring the efficacy of their services through pre- and posttreatment assessment of therapeutic outcomes.
Literature Review
Childhood Trauma
Childhood trauma has documented associations with adverse effects in adult functioning, including anxiety, depression, posttraumatic stress disorder (PTSD), and dissociative disorders, as well as behavioral difficulties such as self-harm, suicidality, substance abuse, and eating disorders (Briere, Kaltman, & Green, 2008; Browne & Finkelhor, 1986; Putnam, 2009; van der Kolk, Roth, Pelcovitz, & Mandel, 1993). CSA is one of the most well-examined areas of childhood trauma, and it has been demonstrated that the long-term negative impact of CSA appears to increase when the abuse is intrafamilial, earlier age of onset, chronic course, and more severe and penetrative abuse (Briere et al., 2008; Cloitre et al., 2009; Herman, 1992). Strong associations have been made between a history of CSA and later interpersonal difficulties including challenges in intimate relationships (Cloitre, Miranda, Stovall-McClough, & Han, 2005; Davis & Petretic-Jackson, 2000; DiLillo, 2001; Rumstein-McKean & Hunsley, 2001).
More recently, research has examined the mechanisms through which childhood trauma survivors develop these long-term difficulties in life and relationships. Challenges with emotion regulation and interpersonal skills have been identified by a number of researchers as playing an important role in the long-term functional deficits experienced by survivors. Emotion dysregulation has been generally understood as a tendency to have low-threshold, high-intensity emotional reactions followed by a slow return to baseline (Badour & Feldner, 2013; Briere, 2006; Briere, Hodges, & Godbout, 2010; Cloitre, Koenen, Cohen, & Han, 2002; Ehring & Quack, 2010). In Diagnostic and Statistical Manual of Mental Disorders-IV field trials, 77% of childhood trauma survivors evidenced substantial challenges with emotion regulation as compared to only 37% of adult onset trauma survivors (van der Kolk et al., 1993). Over 70% of childhood trauma respondents reported getting upset easily, having trouble calming down, and difficulty letting go of upsetting events (Rorty & Yager, 1996; Zlotnick et al., 1999). Without these important self-regulatory capacities, survivors may experience feeling overwhelmed by emotions, experience difficulties expressing emotions, and, as a result, experience high levels of distress. Survivors may turn to behaviors such as self-injury, dissociation, alcohol, sexual compulsivity, eating disorders, and other impulsive or self-destructive actions to distract, sooth, and numb themselves (Briere, 2006; Cloitre et al., 2006; van der Kolk et al., 1993; Zlotnick et al., 1997). Additionally, these challenges with emotion regulation have been implicated in the challenges that many survivors experience when engaging in exposure-based treatment paradigms for trauma (Cloitre, Petkova, Su, & Weiss, 2016).
While intimate relationships and social support may moderate the impact of childhood trauma on survivors (see Charuvastra & Cloitre, 2008), survivors consistently report significant difficulties in relationships, especially in couple relationships (Fredman, Monson, & Adair, 2011; Taft, Walling, Howard, & Monson, 2011; Whiffen, Judd, & Aube, 1999). Childhood trauma often occurs in the context of attachment relationships and can lead to severe challenges in interpersonal functioning. Childhood trauma survivors most frequently evidence insecure attachment styles in adulthood, with CSA survivors demonstrating predominantly fearful–avoidant styles of relating (Alexander, 2009; Cloitre, Stovall-McClough, Zorbas, & Charuvastra, 2008). The relationships of childhood trauma survivors are often characterized by higher levels of distress, dissolution and interpersonal violence, difficulties with communication, instability and chaos, and fluctuating needs for closeness alternating with avoidance, typical of fearful–avoidant attachment styles (DiLillo, 2001; Godbout, Runtz, MacIntosh, & Briere, 2013; Rumstein-McKean & Hunsley, 2001).
STAIR
STAIR is a 10-session treatment model specifically developed to assist individuals who have experienced childhood trauma in the development of emotion regulation skills and interpersonal capacities. This model is based in attachment theory and interpersonal psychology (Cloitre et al., 2006), but the intervention draws from the cognitive behavioral tradition. Each session focuses on a particular skill that may be compromised as a consequence of childhood trauma. Session topics move from a focus on emotion regulation to the use of emotion regulation in the context of relationships. The first five sessions focus on the impact of trauma on emotions and relationships, labeling and identifying feelings, emotion management, distress tolerance, acceptance of feelings, and increased capacity to experience positive emotions. The remaining five sessions include identification of trauma-generated interpersonal “schemas” or expectations that impact current relationships, formulation of alternative, more positive schemas relevant to effective living in the present, skills training in effective assertiveness, increasing flexibility regarding interpersonal expectations, and enhancing compassion for self and others. Each session follows the same format: psychoeducation about the impact of trauma on the targeted skill, demonstration of the skill, and in-session practice of the skill. Participants engage in structured activities, role plays, and homework exercises designed to apply the new skills to real-life situations.
A total of six studies have been conducted evaluating the efficacy of STAIR. Three studies were conducted in an individual format, two of which were randomized controlled trials (Cloitre et al., 2002; Cloitre, Stovall-McClough, Nooner, Zorbas, Cherry, Jackson, et al., 2010), and the other was a benchmark study evaluating the implementation of STAIR by community providers (Levitt, Malta, Martin, Davis, & Cloitre, 2007). Of relevance to our efforts, STAIR has also been tested in three studies in a group format: one a comparative study in which group STAIR was assessed compared to treatment as usual among inpatients with comorbid PTSD and schizoaffective disorder (Trappler & Newville, 2007) and two open trials with adolescents, one in a school setting (Gudiño, Leonard, & Cloitre, 2016) and the other in an inpatient unit (Gudiño, Weis, Havens, Biggs, Diamond, et al., 2014).
Cedar Centre
Founded in 1987 and incorporated in 1989, Abuse Program of York Region (operating York Region Abuse Program [YRAP]) offers publically funded, intensive trauma-specific therapeutic interventions for children, youth, and adults who have experienced childhood interpersonal trauma. The clinical director is a clinical social worker, and therapists in the program come from a number of disciplines including social work and psychology. In addition to individual therapy, YRAP offers complementary programs including support for caregivers and intimate partners, psychoeducational and therapeutic groups, prevention and education opportunities, and a group therapist training program, as well as clinical and organizational training and consultation. The organization’s primary catchment area is the nine municipalities of York Region and surrounding areas without like services. As a community service, the organization offers its programs free of charge. In the winter of 2016, YRAP rebranded and is currently operating as Cedar Centre.
Prior to 2013, the agency’s adult program offered two streams of service for people who had experienced CSA: individual and group therapy. Within this model, the organization had an unprecedented 2-year waitlist. Participants were invited to choose the modality of service (group or individual) and length of time they needed to stay in the program. In addition to referrals received from clients experiencing PTSD and complex PTSD, many community referrals came from the medical and psychiatric systems. As a result, a significant group of program participants faced complicated and compounded mental health challenges that required long-term support. From the referrers’ perspective, the agency was financially accessible (free), available long-term, and of high quality, making it an ideal resource for anyone and everyone who met the eligibility of CSA, but resulted in less than ideal conditions for trauma work. The trauma therapists on staff reported that the individual therapy program had become congested with a subpopulation of participants who appeared to be highly traumatized and were struggling with managing activities of daily living and evidencing significant conflicts in interpersonal relationships; they were simply overwhelmed by life. These clients were not moving through the program, and this resulted in long waiting lists.
Over time, it became increasingly evident to the agency administration, clinical directors, and staff therapists that this subpopulation needed something different than the existing program model, and there was great concern that people with complicated needs would fall through the cracks of any program revisions. In response, the organization made a commitment to find a way to provide effective trauma-specific services to a diversity and complexity of clientele without comprising their quality of care. Below we describe the process of adoption, implementation, and evaluation of STAIR.
Adoption
The organization used its trauma-specific expertise to identify a research-supported, time-limited model that would be appropriate for individuals with PTSD and complex PTSD while addressing the subpopulation’s special care needs. Cedar Centre began to look at the idea of a pretherapy group that could help to assess the subpopulation’s program readiness, while giving them much needed skills to manage their trauma symptoms. After consultation with the first author, the STAIR group was recommended as a potential pretherapy intervention for the subpopulation to help them prepare and become resourced enough to engage in intensive trauma-specific therapy.
When the agency was introduced to the STAIR curriculum, it became evident that STAIR groups could reach beyond the notion of pretherapy. Tools and exercises were titrated in a safe, yet powerful way that would keep group members accountable for the development of Phase I skills. Instead of the intended intervention for the subpopulation, STAIR groups became the prerequisite for all people to enter service. Once successfully completed, participants would then be invited to participate in up to 48 weeks of individual trauma-specific therapy and process-oriented group therapy, concurrently.
In an effort to demonstrate the efficacy of their services to funding agencies, as well as to provide accountability in their own clinical processes, Cedar Centre, in consultation with the first author, selected and implemented a set of standard clinical outcome measures that are administered to all participants before service commences, at the end of the STAIR group, and at the conclusion of 48 weeks of individual therapy. The first author provided support through the McGill secure online survey administration system for the administration, collection, and analysis of the pre- and posttreatment assessments. The outcomes described are the result of the clinical data collected through this newly initiated process of standard clinical measurements. We assessed the participant outcomes of the first 2 years of the implementation of the STAIR model at the Cedar Centre with individuals who have experienced CSA. It was our hypothesis that, in keeping with the literature on the STAIR model, participants in this community setting would experience decreased levels of emotion regulation difficulties, interpersonal problems, and traumatic stress symptoms. Lastly, we also collected qualitative data from the group facilitators and CSA participants regarding their experiences with the implementation of the new program and completed a thematic analysis on these data. Approval was obtained from the McGill University research ethics board for human subjects for this analysis of deidentified clinical data collected as a part of the Cedar Centre clinical assessment process.
Method
Participants
During a 24-month period, following a telephone intake, 123 individuals who had experienced CSA attended an in-person social history intake session at Cedar Centre. As indicated above, all new participants at Cedar Centre first access services through participation in the STAIR group. Approximately 31% of these individuals did not go on to participate in or complete the group after completing the intake assessment or return to complete the final posttreatment assessment. Primary reasons included scheduling and childcare conflicts. Some participants were initially apprehensive about attending a mixed-gender group but reported feeling comfortable once the format of the group was described to them. One woman decided to not participate in the group because of the presence of men. Sixteen participants withdrew before the start of the group. Eleven participants did not return for the posttreatment assessment and could not be contacted for follow-up. Five participants withdrew from the group after starting the program. Six participants were denied entry into the STAIR group due to reporting severe levels of dissociation on the measure of dissociation in the range indicative of a high likelihood of the presence of a diagnosis of dissociative identity disorder or severe levels of emotion dysregulation, as well as presenting clinically as too distressed to actively engage and participate in the structured, coeducational group, and were referred to individual treatment to encourage containment and stabilization prior to being offered an opportunity to complete the STAIR group at a later time.
Over the course of 2 years, 85 individuals who had experienced CSA (23 male, 62 female) completed the STAIR program at Cedar Centre and both pre- and posttreatment assessments. Statistical analyses revealed no significant differences between participants who completed the group and participants who did not begin or complete the group on any of the assessment measures other than a statistically higher total score on the life events checklist (LEC; completers: M = 27.37, standard deviation [SD] = 12.37; noncompleters: M = 32.93, SD = 16.48, t(121) = 2.18, p = .03).
Assessment Measures
Potential participants completed a series of assessment measurements at intake and upon completion of the STAIR program. This assessment included review of the participant’s trauma history, current traumatic symptomatology, and measures assessing the symptoms targeted by the treatment, including emotion regulation, dissociation, and interpersonal problems. Measures were chosen for their psychometric validity and utility in measuring the constructs of interest, as well as their ease of use for the ongoing clinical evaluation of treatment outcomes. We were particularly interested in assessing clinical change in emotion regulation, interpersonal problems, and trauma-related symptoms, key targets of the STAIR group intervention.
Trauma history
To assess trauma history, participants completed the Life Events Checklist (LEC) (Gray, Litz, Hsu, & Lombardo, 2004), a frequently used measure of lifetime exposure to stressful events and traumas.
Emotion regulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) is a 36-item scale assessing emotion regulation and dysregulation. It is a frequently used measure of emotion regulation representing six distinct factors that have demonstrated average-to-strong internal consistency and test–retest reliability (Gratz & Roemer, 2004). In this sample, internal consistency (Cronbach’s α) was good at .86. Dissociation, which can be understood as a defensive approach to emotion regulation in trauma survivors, was measured using the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986). The DES is a 28-item self-report measure screening for high levels of dissociation. For this sample, internal consistency (Cronbach’s α) was excellent at .93.
Interpersonal problems
The Inventory of Interpersonal Problems (IIP; Horowitz, Alden, Wiggins, & Pincus, 2000) is a 32-item self-report inventory that measures a number of frequently reported interpersonal problems that have been found to underlie psychological distress. The IIP has also been used as a measure of clinical change. For this sample, internal consistency (Cronbach’s α) was excellent at .90. The total score is the mean score of items rated on a 5-point Likert-type scale ranging from 0 to 4.
Posttraumatic stress symptoms
An overall score of posttraumatic stress symptom severity was created using the International Classification of Diseases (ICD-11) Trauma Questionnaire (ICD:PTSD; Cloitre, Roberts, Bisson, & Brewin, 2015). Scores for each item ranged from 0 (not at all) to 4 (extremely). In this sample, internal consistency (Cronbach’s α) was excellent at .95.
Training and Adherence
Therapists were trained by the first author over the course of an intensive day-long training session. The clinical director of the Cedar Centre participated in this training and provided weekly supervision and adherence checks over the course of the groups, which included a review of all materials presented in weekly sessions and a discussion of the specific therapist behaviors in the implementation of the manualized model. Over the 2 years, 16 facilitators were involved in cofacilitating STAIR groups using standardized materials developed by the originator of the STAIR model, the second author. The clinical director had direct access to both the researcher and STAIR originator (first and second authors) as needed.
Delivery of Services
The STAIR group was offered to participants on a weekly basis for 10 weeks. STAIR treatment group sessions were facilitated by two trained facilitators. Over the course of the 2 years, six groups were carried out with a range of between 4 and 10 participants in each group. Groups were coeducational. Treatment consisted of 10 sessions delivered over a 10-week period. As per the standardized model, participants were assigned homework after each session, and this homework was reviewed in subsequent sessions.
Results
Sociodemographic and Abuse Characteristics
Participants ranged in age from 18 to 66 years (M = 43, SD = 11). The sample was mixed gender, with 77% female and 23% male participants. All participants reported a history of CSA. Additionally, 60% reported a history of childhood physical abuse in childhood. Levels of trauma reported in adulthood were also high, with 63% reporting having experienced a physical assault, 32% reported having experienced physical assault with a weapon, 33% reported having experienced sexual abuse after the age of 18, and 67% reporting having experienced other unwanted sexual experiences in adulthood. Overall, these participants, while targeted for a history of CSA, represent a group of survivors who experienced multiple, early, significant traumas, and the majority experienced revictimization in adulthood.
Pre- to Posttreatment Outcomes
Comparison of preintervention to postintervention means was conducted by paired t-tests. All tests were conducted at 95% level of confidence, and the data set was built and analyzed using SPSS Version 21. To control for multiple comparisons, the Bonferroni correction was applied, and the values below represent the adjusted p values. Effect sizes (ESs) using Cohen’s d (Cohen, 1992) were calculated to assess clinical significance of change, which indicates observable clinical change; scores of .20 or less are considered to indicate small change, scores of .50 indicate moderate change, and scores of .80 or more indicate large changes. Means, SDs, significance levels of mean differences, and ESs are presented in Table 1.
Means, Standard Deviations, Mean Difference Significance Levels, and Effect Sizes for Symptom Measures.
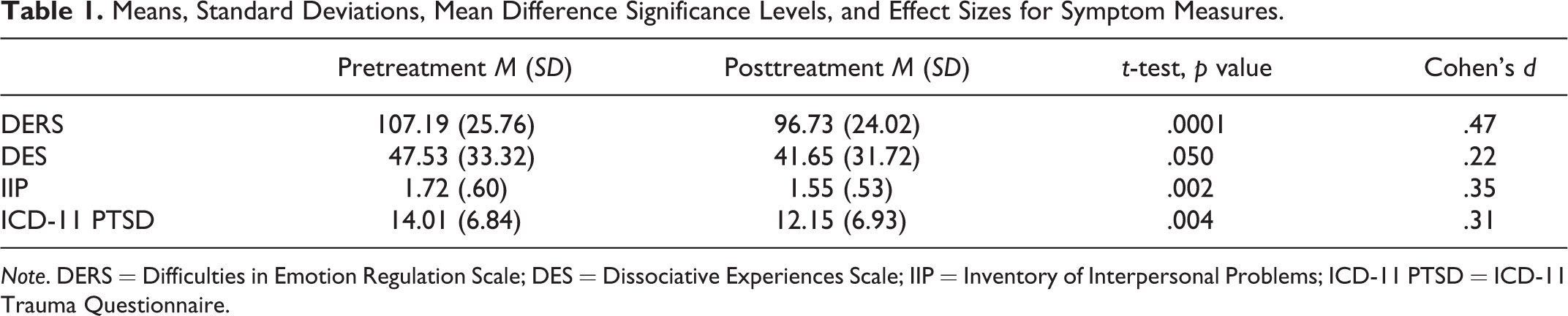
Note. DERS = Difficulties in Emotion Regulation Scale; DES = Dissociative Experiences Scale; IIP = Inventory of Interpersonal Problems; ICD-11 PTSD = ICD-11 Trauma Questionnaire.
Emotion regulation
Pre-to-post treatment scores on the DERS indicated a significant decrease in scores where lower DERS scores suggesting lower levels of emotion dysregulation—therefore, higher emotion regulation, t(84) = 4.31, p < .001. The ES was moderate. Pre-to-post treatment scores on the DES indicated a significant decrease in scores where lower scores indicate less dissociation, t(84) = 1.98, p = .050. The ES was small.
Interpersonal problems
There was a significant reduction in IIP scores from pretreatment to posttreatment with lower IIP scores suggesting lower levels of interpersonal problems, t(84) = 3.18, p =.002. The ES was small to medium.
Posttraumatic stress symptoms
There was a significant reduction in the mean levels of trauma symptoms reported by participants from pretreatment to posttreatment, with lower ICD:PTSD summary trauma scores reflecting lower levels of trauma symptoms, t(84) = 2.99, p =.004. The ES indicated a small-to-medium effect.
Qualitative Feedback
As a part of the implementation evaluation, the executive director carried out random, unstructured interviews with therapists and participants in the first two STAIR groups to assess their perceptions and experience of the new program. Certain themes emerged in both groups. For the therapists, these themes included a feeling that clients received the model positively, that initial misgivings about shifting to a manualized program were unfounded, and that they, as therapists, felt that they were providing clear and concrete resources and skills to clients that addressed their very real day-to-day challenges in living. For participants, these themes included feelings of hope, greater understanding, and a sense of confidence in the development of usable skills. Some quotes from therapists and participants include:
Therapists: As a frontline worker, the program change provided clear and meaningful program offerings that are easy to communicate to service users, community partners, and other agencies. The new model was well received by those accessing our program. I continue to hear how impressed folks are with the practical and comprehensive nature of the service. Additionally, the new model filled a gap and provided a real resource to quickly connect those with trauma-related high-priority needs (i.e., mental health, housing, primary health care, addictions, etc.) with service. The positive feedback I get from clients who have gone through the STAIR program is a testament to how well this program works. When I meet with clients for their initial introduction to the program they often show up with uncertainty, fear, and emotional pain. After graduating from the STAIR program, they honestly appear and interact differently with me. They seem more dynamic and alive and comfortable—they smile more, speak more confidently, and have a desire for more programming/knowledge. Clients have reported that the STAIR material has been very helpful to them in terms of how they manage their feelings and thoughts. In therapy, people consistently report how useful the skills they learned in STAIR are and often refer back to STAIR material and apply it to their current situations. In terms of how STAIR has impacted clients compared to our previous model, I think that clients are coming into individual therapy generally more regulated in terms of emotional and verbal expression in the therapy room. Clients also have more awareness of the connection between their feelings and thoughts, and so when they begin individual therapy, they are generally able to identify their stuck points and areas of challenge. Clients are coming in now with a vocabulary around their current emotional and cognitive state, something that sometimes took weeks to establish under our previous model. I feel that this greater awareness helps clients develop a more clear form of self-assessment, and as such, clients are able to identify goals more clearly and specifically.
Participants: [My group experience] has validated all my behaviors, my choices, and also how the trauma played such a huge role in my life decisions. I felt hopeful and strong about the future. Great theories and tools for everyday life. I feel as if I'm myself again.
Discussion
The goals of this report were to describe the adoption and implementation of the STAIR model at the publically funded, community-based Cedar Centre as well as to conduct a preliminary evaluation of the effectiveness of treatment with individuals who have experienced CSA. The adoption and implementation involved multiple stakeholders and successfully engaged experts in the provision of research-supported treatments of individuals with symptoms and problems related to childhood abuse. The intervention participants showed significant improvement in three specifically targeted problem areas: emotion regulation difficulties, interpersonal problems, and trauma symptoms. In addition, the STAIR group was well liked by both the facilitators and group participants.
The participants treated in this community treatment program evidenced high levels of CSA and other childhood traumas, as well as subsequent revictimization. Given the high levels of trauma in this sample, the treatment outcomes can be considered quite positive. Additionally, there was a very low level of dropout in the program, less than 5% of the total number of less than 5% of the total number of participants who started the program. Negative outcomes were limited but included initial participant concerns about being in a mixed-gender group and, for some, the view that the curriculum would be too overwhelming or, in cases where participants had a history of therapeutic intervention, underwhelming. Results from annual client engagement interviews with the executive director, the fourth author, showed that these initial perceived barriers were, in fact, not identified by participants following completion of the STAIR group, but rather, participants felt that the program had been profoundly helpful and, in many cases, described as a participant’s greatest achievement.
Limitations
The data on which the analyses were conducted were collected for the purposes of ongoing clinical program evaluation and not for academic research. As such, certain data that might have proven elucidating, such as particular demographic variables (education, race, income), were not collected. Co-facilitators did not need to reach a specific identified level of competency (e.g., observed and rated on tapes by experts regarding quality of delivery) before participating in the groups that were part of the implementation evaluation. Once the training was completed, co-facilitators began facilitating the intervention. Similarly, there was no quantitative assessment of adherence to the protocol. The sessions were not taped for independent raters to assess how closely the interventions adhered to the protocol, nor were weekly adherence rating collected by either the supervisor or the facilitator (self-rated adherence). It is unknown whether the impact of the program would be enhanced with more individualized training and attention to adherence.
Implementation scientists suggest that for evidence-based programs to be implemented and evaluated within the context of real-world settings, it will be essential to be adaptive and flexible in developing evaluation protocols that are manageable within the daily operations of a clinical setting (Tseng & Nazmi, 2015). Additionally, a balance must be found between methodological rigor and the value of research results arising from real-world clinical settings to ensure that the transition from academic research to clinical practice can occur (Larner, 2004; Soldz & McCullough, 2000). As stated by Youkey (2013), Scientific rigor must be balanced with a need to conduct research that applies to real world settings. In this context, research rigor should not be confused with the quality of research. Rather, this form of research may not produce results with the same precision than other forms of research.
Future Challenges
Cedar Centre has taken on the challenge of implementing a research-supported treatment as the first stage of intervention within their publically funded trauma-specific therapy program and has shown dedication and commitment to providing individuals who have experienced CSA with the most effective and suitable interventions for their specific challenges. Over the next few years, it will be important to find ways to continue the important work of ongoing clinical outcome evaluation that is integrated into the daily functioning of the organization. At this point, we are looking to find ways to transfer back the data collection and analysis to Cedar Centre so that they are more in possession and control of their own clinical data. This will require some technical adjustments and education in terms of psychometrics and evaluation of clinical measurement tools.
Conclusions
This article represents a foray into an important and underexplored area: the implementation of research-supported treatments and evaluation of outcomes in publically funded clinical social work settings. The importance of researchers and academic clinicians making themselves available to share their expertise with community partners is essential for these processes to take place.
It is a tremendous shift to move from a process-oriented, unstructured group and individual therapy intervention model to a manualized, structured, cognitive behaviorally oriented treatment protocol, and this was accomplished with a lot of strong leadership and determination. While there was some initial resistance from participants, the overall feedback coming from participants who were provided the opportunity to talk about their impressions of the new program was positive and reflective of feelings of hope for the future and a sense of confidence in their newly acquired skills.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.