
Abstract
Objective:
This article describes the validation of the Religious/Spiritually Integrated Process Assessment Scale (RSIPAS) across five helping professions. The RSIPAS was originally developed to measure clinical social workers’ self-efficacy, attitudes, perceived feasibility, behaviors, and overall orientation toward integrating clients’ religion and spirituality in practice.
Method:
The current study examines the internal consistency and criterion, discriminant, convergent, and factorial validity of this instrument with a sample of clinical social workers, psychologists, nurses, counselors, and marriage and family therapists in Texas (N = 550).
Results:
Findings support the reliability (α = .95) and various forms of validity, with an improved fit in the factor structure among this more diverse sample.
Conclusions:
The RSIPAS may be used among these five helping professions to identify training needs or evaluate training efforts related to the integration of clients’ religious or spiritual beliefs in mental and behavioral health treatment.
Keywords
Over the past few decades, research has indicated that religion and spirituality are two important components in clients’ lives worth considering in clinical practice, as they relate to various health and mental health issues (Koenig, King, & Carson, 2012; Koenig, McCullough, & Larson, 2001). These issues cut across a number of clinically trained helping professions, such as social work, nursing, psychology, marriage and family therapy, and counseling. With a majority of Americans identifying themselves as religious (Pew Research Center, 2015) and clients expressing a preference for their religion/spirituality (RS) to be understood and considered in the treatment of various clinical issues (Leitz & Hodge, 2013; Post & Wade, 2014; Post, Wade, & Cornish, 2014; Stanley et al., 2011; Tepper, Rogers, Coleman, & Maloney, 2001; Taylor & Mamier, 2005; Weld & Eriksen, 2007), it is important for helping professionals to be aware of how and the degree to which practitioners are ethically and effectively incorporating clients’ RS into practice.
Religion and Spirituality in Clinical Practice
When conceptualizing these two terms, religion may be defined as “a system of beliefs and practices observed by a community, supported by rituals that acknowledge, worship, communicate with, or approach the Sacred, the Divine, God (in Western cultures), or Ultimate Truth, Reality, or nirvana (in Eastern cultures),” and it relies on scriptures, teachings, and offers a moral code of conduct (Koenig, 2008, p. 11). Likewise, spirituality may be defined as the personal quest for understanding answers to ultimate questions about life, about meaning, and about relationship to the sacred or transcendent, which may (or may not) lead to or arise from the development of religious rituals and formation of community. (Koenig et al., 2001, p. 18)
A large majority (77%) of Americans actually consider religion to be at least somewhat important in their lives (Pew Research Center, 2015). Although this number has fallen slightly in the past decade, there has been a simultaneous increase in feelings of spiritual well-being, indicating a shift from religiosity to spirituality. An overwhelming 88% believe in a “God or Universal Spirit” and over half pray daily (Pew Research Center, 2015), often times praying for one’s own or others’ healing (Levin, 2016). Further, some racial and ethnic cultures in the United States (e.g., Hispanic or African American communities) have higher rates of considering religion to be important (84% and 91%, respectively), pray daily (58% and 73%, respectively), read scripture weekly (38% and 54%, respectively), and rely heavily on their RS traditions in their daily lives (Pew Research Center, 2015). Given the importance of religion and/or spirituality in many Americans’ lives, these beliefs are likely to intersect with one’s mental and behavioral health and be intricately woven into presenting clinical issues. In fact, recent research suggests that clients prefer their RS beliefs to be explored by the helping professional and integrated in their treatment planning and interventions (Post & Wade, 2014; Stanley et al., 2011). This integration may have the potential to improve a number of clinical issues ranging from anxiety and stress (Rosmarin, Pargament, Pirutinski, & Mahoney, 2010) depression among those with chronic illness (Koenig et al., 2015), eating disorders (Richards, Berrett, Hardman, & Eggett, 2006), migraines (Wachholtz & Pargament, 2008), and even overall mortality (Shanshan, Stampfer, Williams, & VanderWeele, 2016).
Although the potential exists for clients’ RS beliefs and behaviors to be the sources of support or comfort during seasons of struggle, there is also the possibility for their RS beliefs to be a source of angst and difficulty within the presenting issue. In both situations, clients’ use of religious coping (e.g., meditation, prayer, religious service attendance, being in conflict or collaboration with a higher power, receiving support—or not—from one’s RS community, or engaging in various RS rituals) is important for the helping professional to be aware of, just as any other coping mechanism would be (Pargament, 1997). For example, while an adolescent suffering from depression may be wondering whether his higher power has abandoned him, a veteran might practice meditation to relieve trauma symptoms, and an older woman may struggle with obsessive–compulsive disorder, utilizing religious rituals to the degree of impairment.
RS Integration Across Multiple Helping Professions
These various issues around considering clients’ RS cut across multiple helping professions, and are not siloed within one particular profession. Many helping professions currently have standing expectations surrounding their ethical codes related to clients’ and practitioners’ RS, often focusing on not discriminating based on religion (American Psychological Association [APA], 2010; American Association for Marriage and Family Therapy [AAMFT], 2012, American Counseling Association [ACA], 2014; American Nurses Association [ANA], 2015; National Association of Social Workers [NASW], 2008). Aside from the expectation to not discriminate clients based on their religion, these five professions vary with regard to their ethical standards surrounding integrating clients’ RS in practice. For example, the ANA includes considering RS under treatment planning (ANA, 2015), while the ACA attends to RS during assessment, recognizing clients’ social support, and even points it out as a valuable component of counselors’ self-care (ACA, 2014). While the AAMFT (2012) only mentions religion within the context of not discriminating, the APA (2010) encourages training on RS when it impacts delivery of services, to respect religious diversity, and extends discouragement of discrimination based on religion to include not harassing or demeaning based on one’s religion. The NASW’s (2008) Code of Ethics includes religion under five standards, as it relates to cultural diversity and competency, respecting diversity among clients and colleagues and avoiding conflicts of interest. Therefore, it is enough of an important area of clients’ lives to consider as it relates to ethical practice; however, the degree to which it’s being integrated in practice may vary.
A review of the available literature found few studies have been conducted within each helping profession to describe their views or behaviors with integrating RS in practice, and even fewer have surveyed multiple professions simultaneously. Although mental and behavioral health professions appear to have identified this area of clients’ lives as worthy of consideration in practice, each struggles to actually integrate it. For example, a recent, national survey of clinical social workers found they have positive views toward integrating clients’ RS in practice but have received little training on this area and are not engaging in this practice behavior often (Oxhandler, Parrish, Torres, & Achenbaum, 2015). In psychology, although four of the five psychologists feel as though there’s a positive relationship between religion and mental health, only half ask clients about their RS during assessment (Delaney, Miller, & Bisono, 2007; Shafranske & Cummings, 2013). Nurses often conduct spiritual histories on clients due to the Joint Commission’s standing expectations (Koenig, 2008) and have participated in various RS practices with clients as they request it (Grant, 2004). In marriage and family therapy, an awareness of one’s own RS beliefs is valued (McNeil, Pavkov, Hecker, & Killmer, 2012), and therapists report being up front that discussing clients’ RS is appropriate and they are willing to engage in this topic with clients (Carlson, Kirkpatrick, Hecker, & Killmer, 2002). With each of these studies, the method of measurement and background variables vary greatly, making it difficult to compare these various professions.
Although studies of individual professions have been much more common, few attempts have been made to conduct a cross-sectional study of multiple helping professions’ integration of clients’ RS in practice. In 1992, Sheridan, Bullis, Adcock, Berlin, and Miller surveyed licensed professional counselors (LPCs), licensed clinical social workers (LCSWs), and psychologists in Virginia and found that LPCs had the most positive attitudes toward utilizing RS-related interventions in practice, followed by LCSWs and then psychologists. Similarly, Bergin and Jensen (1990) surveyed MFTs, psychiatrists, social workers, and psychologists and found that MFTs were the most religious and had the highest degree of intrinsic religiosity. They also found, unexpectedly, there were more therapists across professions involved in personal RS behaviors, but far fewer considered RS matters to be important in treatment efforts with all or most clients.
Further, although many helping professions are participating in discourse around the integration of clients’ RS in practice, they equally struggle with training on this topic and practice behaviors. Specifically, practitioners across each of these professions have expressed a desire for an increase in training, stating they did not receive enough training on attending to this area of clients’ lives (Brawer, Handal, Fabricatore, Roberts, & Wajda-Johnston, 2002; Crook-Lyon et al., 2012; McNeil et al., 2012; Oxhandler et al., 2015; Prest, Russel, & D’Sousa, 1999; Schulte, Skinner, & Claiborn, 2002; Shafer, Handal, Brawer, & Ubinger, 2011). One method to bridge this gap in training includes the evidence-based practice (EBP) process model (Oxhandler & Pargament, 2014). This model includes a five-step process that integrates “best research evidence with clinical expertise and [client]
Since practitioners have clearly not received adequate training on this important, sensitive practice area, it is critical to better understand various helping professionals’ current attitudes and behaviors related to clients’ RS. Further, having received little to no training on this area of practice, perceived feasibility and self-efficacy are two constructs worth exploring, which have only been assessed in social work (Oxhandler et al., 2015). Although some efforts have assisted helping professions in understanding their individual profession views or behaviors related to this area of practice, there have been glaring inconsistencies in measurement with varying degrees of reliability and validity, and none have assessed this area within the context of providing EBP (Oxhandler & Parrish, 2016). Given the growth in inter- and transdisciplinary practice, it is important to understand the degree to which practitioners across disciplines consider clients’ RS in treatment to ensure that there is continuity of care. Further, given the inclusion of RS across each helping profession’s code of ethics, especially as they relate to respecting this area of clients’ culture and avoiding RS discrimination (AAMFT, 2012; ACA, 2014; ANA, 2015; APA, 2010; NASW, 2008), such professions may want to assess current practitioners’ orientation toward integrating clients’ RS in practice and evaluate any changes over time. The implications of these findings may be important for graduate training efforts, evaluating continuing education (CE), treatment planning, and adequate sensitivity to clients’ diverse RS beliefs. There is a need for an instrument that is validated across professions—clinical social workers, psychologists, counselors, marriage and family therapists, and nurses—to assess the attitudes, self-efficacy, perceived feasibility, behaviors, and overall orientation toward integrating clients’ RS in practice to guide interprofessional practice and training efforts on this important topic.
In 2014, the Religious/Spiritually Integrated Practice Assessment Scale (RSIPAS) was developed to assess a national sample of clinical social workers’ attitudes, self-efficacy, perceived feasibility, behaviors, and overall orientation toward integrating clients’ RS in clinical social work practice (Oxhandler & Parrish, 2016). The overall 40-item RSIPAS had an excellent Cronbach’s α of .95, with the subscales’ reliability ranging from .84 to .91. The RSIPAS had established face, content, criterion, discriminant, convergent, construct, and factorial validity, with a majority of items having an excellent factor loading. The clinical social workers’ responses and predictors of their RSIPAS scores can be found in Oxhandler, Parrish, Torres, and Achenbaum (2015).
Purpose of the Current Study
The purpose of this current study was to reassess the internal consistency, criterion validity, and factorial validity of the RSIPAS (Oxhandler & Parrish, 2016) with a larger, interdisciplinary sample. The instrument was originally developed and deemed reliable and valid using a national sample of LCSWs. Given that the role of clients’ RS may be an important consideration among other, related helping professions, the current study extends beyond a clinical social work sample to include clinical psychologists, marriage and family therapists, advanced practice nurses (APNs), and professional counselors to assess whether the RSIPAS would be reliable and valid with such a diverse group of helping professions.
Therefore, the guiding research questions for this study were as follows: (1) To what degree is the RSIPAS reliable across these five helping professions? (2) Does the RSIPAS have content and criterion validity across these five professions? (3) Can these five professions’ responses to the RSIPAS be explained by four factors (self-efficacy, attitudes, behaviors, and perceived feasibility)? and (4) Can these five professions’ responses to the RSIPAS be explained by four first-order factors (self-efficacy, attitudes, behaviors, and perceived feasibility) and one second-order factor (orientation toward integrating clients’ RS into practice)? At the time of the first study, this instrument was the first to assess social workers’ overall orientation toward integrating clients’ RS in practice, including self-efficacy and perceived feasibility. Should the current study’s findings further support the RSIPAS’s reliability and validity, it would be the first instrument with factorial validity to assess nurses, psychologists, counselors, marriage and family therapists, and social workers’ overall orientation toward integrating clients’ RS in practice as well as their attitudes, self-efficacy, perceived feasibility, and behaviors.
Method
Sample
Baylor University’s Committee for the Protection of Human subjects approved this study. The study population consisted of all licensed psychologists in independent practice (4,614), APNs (21,036), clinical social workers (7,826), marriage and family therapists (2,917), and professional counselors (18,090) registered with the Texas State Board in July 2015. These publicly available licensing lists were used to identify the sampling frame and consisted of 3,500 licensed helping professionals. Specifically, 700 LCSWs, 700 psychologists, 700 APNs, 700 MFTs, and 700 professional counselors (LPCs) with Texas mailing addresses were systematically randomly selected from their appropriate Texas licensing list. This sampling method was selected for its ability to have a consistent form of contact across the five professions, specifically via mail, and because only licensed individuals were included. One limitation of using the state’s licensing list is the typically lower response rate that’s often obtained from mail-based contacts; therefore, a larger sampling frame was utilized in order to obtain at least 400 responses needed for the proposed analyses with the 40-item RSIPAS.
Data Collection
A slightly modified version of Dillman, Smyth, and Christian’s (2015) survey method was utilized for recruitment in this anonymous, online survey. Potential participants received a preinvitation postcard, an initial invitation letter with a SurveyMonkey link, a follow-up postcard with the survey link, and a follow-up letter with a link to the survey as well as a link to assess reasons for nonresponse. Each method of contact briefly described the study, invitations included the link to participate, ensured anonymity, and provided the principal investigator’s and institutional review board’s contact information. To maximize the response rate, participants were given the opportunity to enter to win one of the five, US$50 target gift cards upon completing the survey. Of the 3,500 included in the initial sampling frame, 3,347 were included in the final list due to the mailing company removing outdated or bad addresses. Three potential participants’ letters bounced back, resulting in a final sample frame of 3,344. A total of 550 responded to the survey, resulting in a 16.45% response rate.
Upon entering the online survey link into their browser, participants were directed to the front page of the survey that contained the purpose of the study, consent process, and guiding definitions for religion and spirituality. The questionnaire contained a slightly modified version of the RSIPAS, which was tailored to resonate with all five professions (e.g., instructing participants to interpret “client” to include patients, and “treatment” to include care or therapy, depending on their profession), 26 background items, and 3 open-ended items. The RSIPAS is a 40-item instrument with four subscales that was originally designed to assess social workers’ (1) Self-Efficacy with Regard to Integrating Clients’ RS in Practice (α = .91), (2) Attitudes Toward Integrating Clients’ RS in Practice (α = .88), (3) Perceived Feasibility to Engage in RS Integrated Practice (α = .84), and (4) Behaviors Related to Integrating Clients’ RS in Practice (α = .87). The RSIPAS has excellent reliability (α = .95) and established content, criterion, construct, discriminant, and factorial validity (Oxhandler & Parrish, 2016). The background section included practitioner-related items that have been used in previous, related studies of helping professionals (Oxhandler et al., 2015; Parrish & Rubin, 2011); the Duke University Religion Index (DUREL), a 5-item scale designed to measure intrinsic and extrinsic religiosity (Koenig & Bussing, 2010); 1 item to assess burnout that has been tested among physicians (Rohland, Kruse, & Rohrer, 2004); 2 items from the General Social Survey that measure the extent to which the respondent considers himself or herself religious or spiritual (Smith, Hout, & Marsden, 2013); and 3 open-ended items assessing what has helped or prevented the helping professional from integrating clients’ RS and their educational experiences with this topic. Many of these items were included for future, secondary analyses of these data and are outside the scope of this current article.
Data Analysis
SPSS 23 (IBM Corp., 2015) was used to check assumptions, assess missing data, and run descriptive analyses. Cronbach’s α was used to assess internal consistency reliability of the overall scale and each subscale. Consistent with the original study, criterion validity was determined based on examining the point-biserial correlations between scale and subscale scores with whether or not the participant took a course on integrating clients’ RS in practice (yes/no), continuing education (CE) on this topic (yes/no), or were aware of empirically supported interventions that integrate clients’ RS in practice (yes/no). Given that intrinsic religiosity has been shown to be a significant predictor of considering this area in clients’ lives in previous studies (Kvarfordt & Sheridan, 2009; Larsen, 2010; Murdock, 2005; Oxhandler et al., 2015), Pearson’s r correlation was run between the Intrinsic Religiosity subscale of the DUREL(Koenig & Bussing, 2010) and the overall scale and subscale scores. Additionally, Spearman’s ρ was used to assess the relationship between overall and subscale scores and participants’ nonorganized religious activity (NORA) and organized religious activity (ORA) as measured by the DUREL.
Mplus 7.0 (Muthen & Muthen, 1998–2015) was used to assess the factor structure of the RSIPAS, examining the first- and second-order confirmatory factor analyses (CFAs). Kline’s (2016) goodness-of-fit indices were used: χ2, comparative fit index and Tucker–Lewis index (TLI) values over .90, and root mean square error of approximation (RMSEA) with a 90% confidence interval (CI) with acceptable values between .05 and .08. Additionally, the weighted root mean square residual was examined to be as close to 1 as possible; however, Muthen (2010) suggests that this value is of less concern when the other methods of assessing fit look good.
Results
Sample Characteristics
Background characteristics for the final sample are reported in Table 1. Of the 534 who responded and had complete data, 139 (26%) were from the clinical social worker list, 96 (18%) from psychology, 96 (18%) from marriage and family therapy, 119 (22.3%) from professional counseling, and 70 (13.1%) from nursing and 14 (2.6%) did not specify from which list their letter or postcard indicated they were drawn. Although an equal number of practitioners were sampled from each helping profession (N = 700 from each of the five professions), the response rate varied from each profession. A majority of the overall sample was female (73.5%) and Caucasian (78.8%) with an average age of 52 (SD = 13.01) and 17.52 years (SD = 11.17) in practice.
Sample Characteristics and Background Variables for Sample.
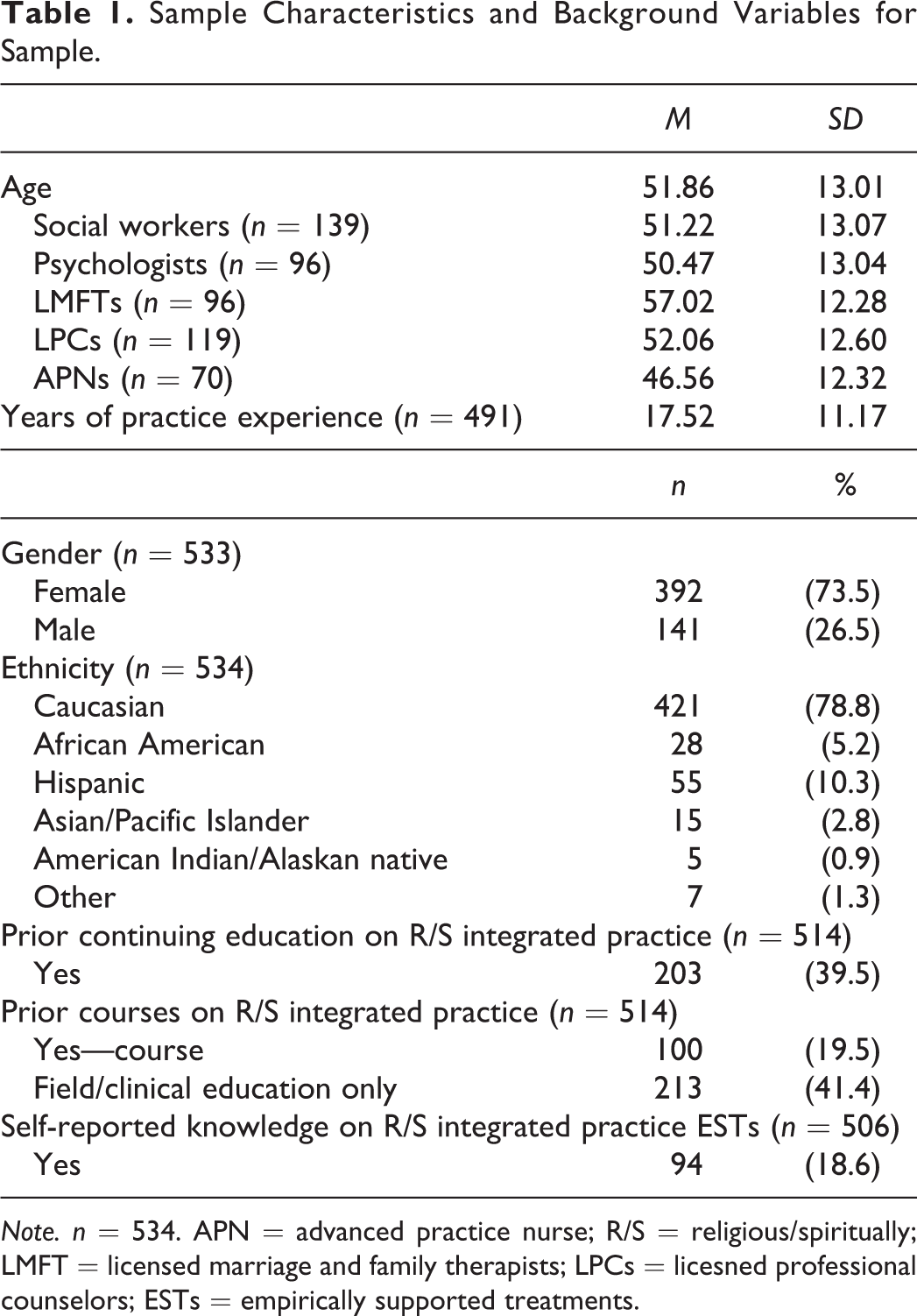
Note. n = 534. APN = advanced practice nurse; R/S = religious/spiritually; LMFT = licensed marriage and family therapists; LPCs = licesned professional counselors; ESTs = empirically supported treatments.
Twelve cases were removed from the final sample for not having any RSIPAS data, and four had acquiescent response set (described under Missing Data and Assumptions), resulting in a sample size of 534. A majority of the entire sample was female (73.5%) and Caucasian (78.8%) with an average age of 51.86 years (SD = 13.01) and 17.52 years (SD = 11.17) of practice experience. Participants reportedly had little training on this topic, with 19.5% having taken a course on integrating clients’ RS in practice, and twice the respondents (39.5%) having received CE on this topic.
Missing Data and Assumptions
Data were assessed for missing values among the 538 cases with at least one subscale complete using SPSS and were found to be well within acceptable range, under 5% (Tabachnick & Fidell, 2013), with 0.2–3% of data missing per item. The Behavior subscale had missing data from 2.2 to 3.0, which is to be expected given its placement at the end of the instrument. Little’s missing completely at random (MCAR) test was used to assess whether data were missing at random (MAR) or MCAR. The results indicated data were not MCAR (χ2 = 212.81, df = 1885, p < .001); therefore, χ2 tests of independence and independent samples t-tests were used to compare various background characteristics to assess if the data were MAR. χ2 tests of independence showed no difference between those with and without missing data regarding gender, race/ethnicity, the licensing list from which they drawn, master’s/doctorate, whether or not the respondent had taken a course on RS in practice, whether the respondent was a field instructor for his or her profession, self-identifying as a religious or spiritual person, or religious affiliation. Independent samples t-tests showed no significant difference between those with and without missing data with regard to age or years in practice. Therefore, in addition to the extremely low percentage of missing data, the data were considered MAR. Given Mplus’s ability to generate modification indices for models with incomplete data, Mplus’s weighted least squares with robust estimates approach was used to handle the missing data (Asparouhov & Muthen, 2007).
To check for respondent fatigue or acquiescent response bias, Attitude Items 5 and 12 (2 items that are the opposite of one another) were checked, along with the direction of their responses to the other Attitude subscale items, Feasibility 3 and 4 (2 other reverse coded items), and their overall RSIPAS responses. Four cases appeared to be truly acquiescent and were removed from subsequent analyses. Seventeen cases appeared to have conflicting responses between ATT5 and ATT12 by having responses within 1 point on both items. However, after examining FEAS3 and FEAS4, as well as the remaining Attitude subscale and overall RSIPAS items, the 17 cases were not considered acquiescent. Three of these cases had a response of three (neutral) on both and were left alone. The responses to item ATT12 of the remaining 14 cases were then adjusted to reflect the direction consistent with their response to ATT5.
After reverse scoring Attitude Item 12 and Feasibility Items 3 and 4, item and subscale scores, the data normality were assessed using frequency distribution, skewness, and kurtosis indices (Abu-Bader, 2010; Tabachnick & Fidell, 2013). Items in the first three subscales and their overall scores were negatively skewed. The Behaviors subscale items and total scores reflected normal distributions. Given these issues, Mplus’s weighted least squares means and variance-adjusted approach was used, as it is robust in handling issues with data that are not normally distributed. Finally, the assumption of linearity was assessed and was met.
Reliability
To assess the internal consistency using Cronbach’s α, participants without any RSIPAS data (n = 12) were removed as were those with acquiescent response bias (n = 4), leaving a sample size of 534. Internal consistency reliability was assessed in SPSS 23 using Cronbach’s α on each of the subscales and the overall RSIPAS Scale. Missing data were removed by listwise deletion. The reliability for the overall, 40-item scale was .95, which Kline (2016) considers excellent, and the four subscales’ reliability ranged from .87 to .91, which is very good to excellent. These results can be found in Table 2 along with the average scores in each of the subscales and overall scale.
Coefficient α, Mean Score, and Standard Deviation (SD) for Entire Scale and Each Subscale (Based on Final 40-Item RSIPAS).
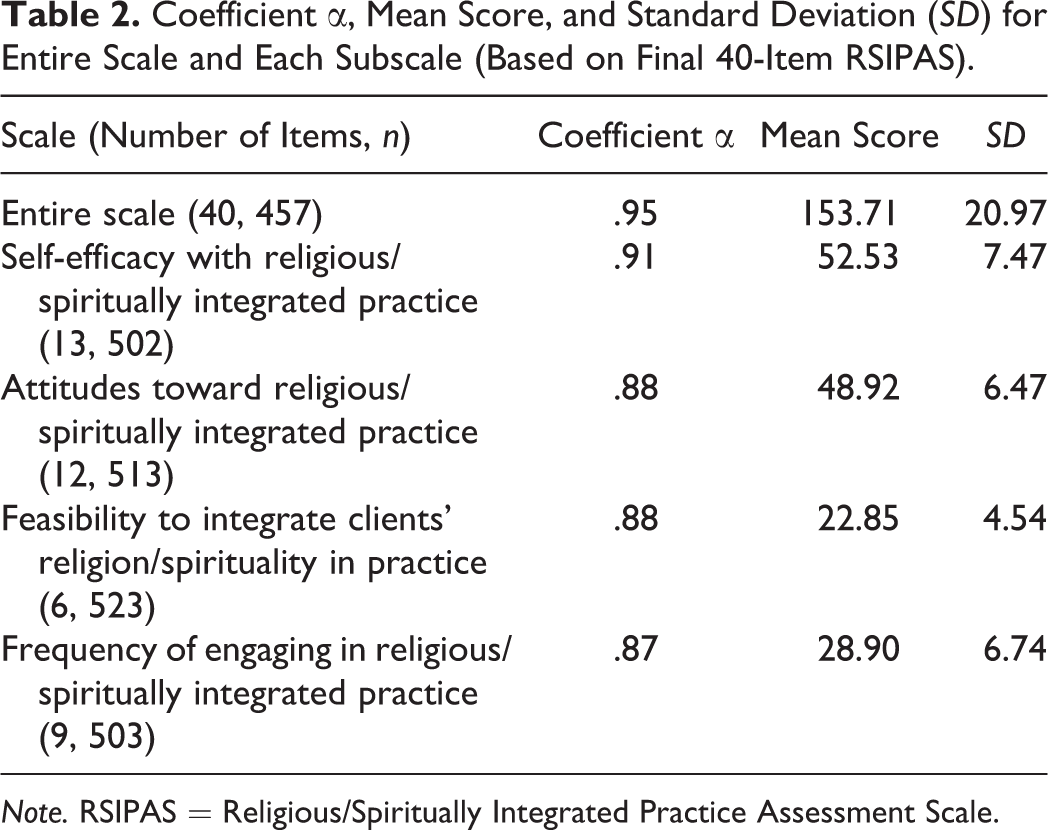
Note. RSIPAS = Religious/Spiritually Integrated Practice Assessment Scale.
Criterion Validity
In the original development of the RSIPAS (Oxhandler & Parrish, 2016), criterion validity was established by assessing bivariate correlation coefficients between scale and subscale scores with the DUREL’s ORA item, NORA item, and Intrinsic Religiosity subscale; prior coursework and CE on integrating clients’ RS in practice; and knowledge of empirically supported treatments that integrate clients’ RS in practice. As shown in Table 3, all 30 correlations were statistically significant. Most indicators had a moderately strong relationship with the overall scale and subscale scores, with intrinsic religiosity having the strongest relationship with the overall scale score.
Relationships Between Amount of Prior Training or Education in R/S Integrated Practice, Practitioner Religiosity, and Summated Scores on the Final CFA Model of the RSIPAS and Its Subscales.
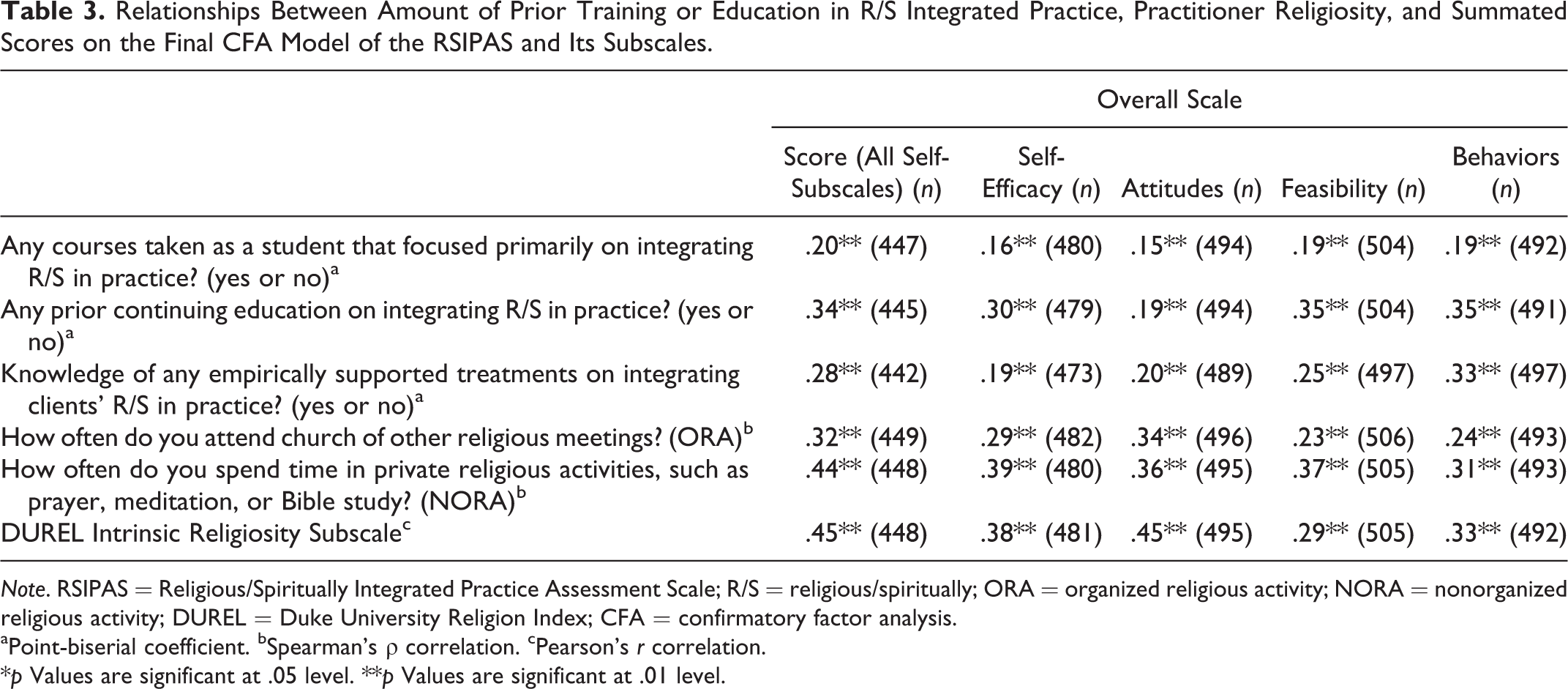
Note. RSIPAS = Religious/Spiritually Integrated Practice Assessment Scale; R/S = religious/spiritually; ORA = organized religious activity; NORA = nonorganized religious activity; DUREL = Duke University Religion Index; CFA = confirmatory factor analysis.
aPoint-biserial coefficient. bSpearman’s ρ correlation. cPearson’s r correlation.
*p Values are significant at .05 level. **p Values are significant at .01 level.
CFAs
A CFA was conducted in Mplus to test whether the fit identified in the first-order and second-order models in the original study was consistent with the diverse sample.
First hypothesized model: Can the RSIPAS be explained by four factors (self-efficacy, attitudes, perceived feasibility, and behaviors)?
The baseline, first-order model is displayed in Figure 1. This model tested whether four factors that measured self-efficacy, attitudes, perceived feasibility, and behaviors emerged from the responses to the RSIPAS and contained the 10 correlated error terms identified in the original study for similarly worded items (Oxhandler & Parrish, 2016). These correlated error terms included FEAS1 with FEAS2, FEAS1 with FEAS4, ATT2 with ATT4, ATT3 with ATT4, ATT5 with ATT12, ATT6 with ATT9, BEH1 with BEH2, BEH2 with BEH3, BEH3 with BEH5, and SE7 with SE10.
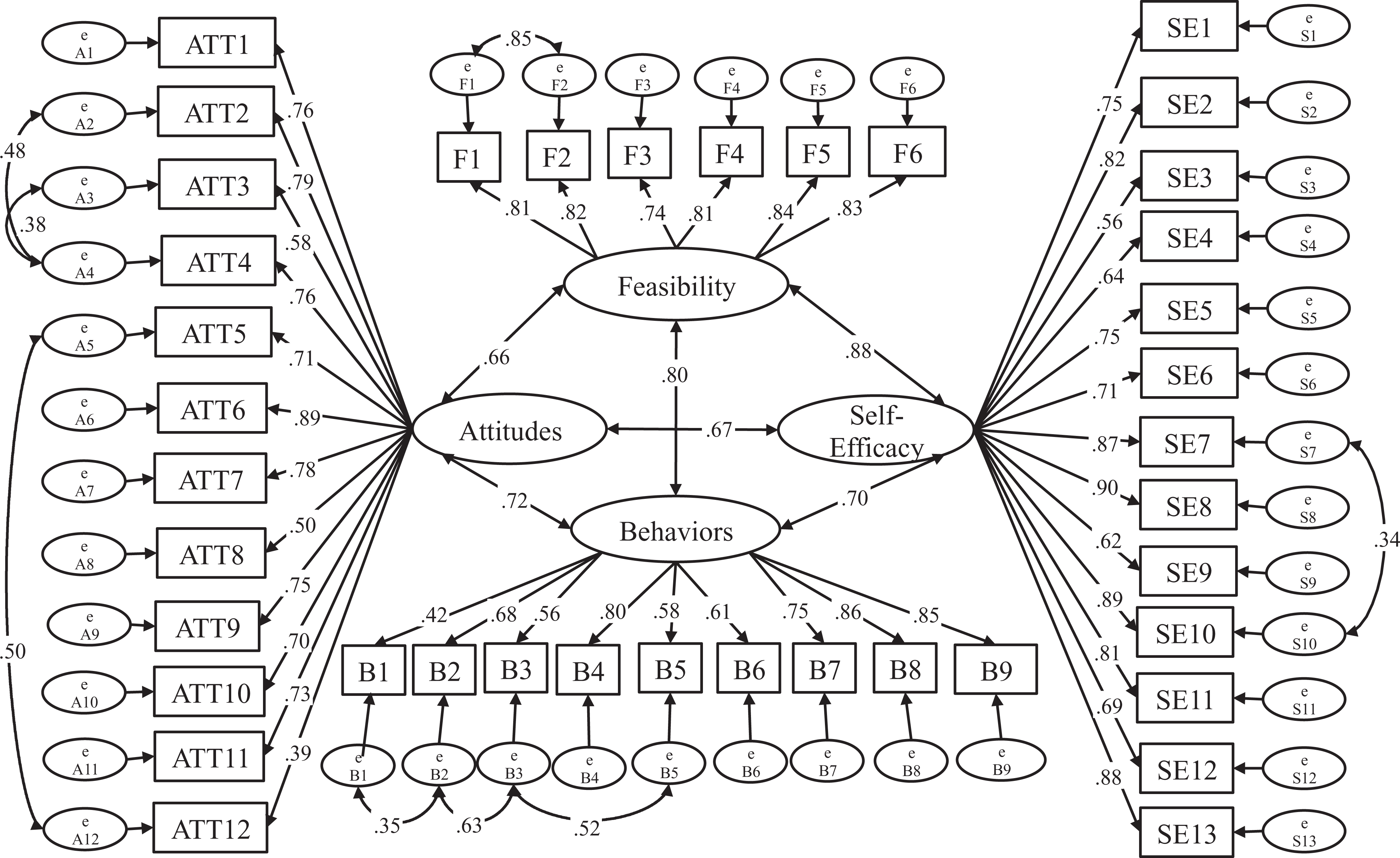
Religious/Spiritually Integrated Practice Assessment Scale revalidation first-order model (includes standardized loadings).
Tabachnick and Fidell’s (2013) rule of thumb for determining item loading cutoff (above .32), based on Comrey and Lee’s (1992) factor loading criteria, was used when assessing item loadings. All items were above the .32 cutoff and the model had adequate fit, as indicated in Figure 1. However, two correlations between error terms that were included in the original study were dropped from this first hypothesized model due to not being significant and/or below .32 (ATT6 and ATT9: .018, p = .816; FEAS1 and FEAS4: .10, p < .01).
Second hypothesized model: Can the RSIPAS be explained by four first-order factors and one second-order factor (orientation toward integrating clients’ RS in practice)?
After confirming the first-order factor structure, the second-order, overarching factor was tested. The same model in the original study was used (Figure 2) to test this hypothesis, with the removal of the two correlated error terms mentioned above that were not significant and/or below .32 when testing the first hypothesized model (ATT6 and ATT9 as well as FEAS1 and FEAS4). This second hypothesized model was deemed to have adequate fit, with improvement from the first-order model (described in Table 4): χ2 diff (2, n = 534) = 129.23, p <.001.
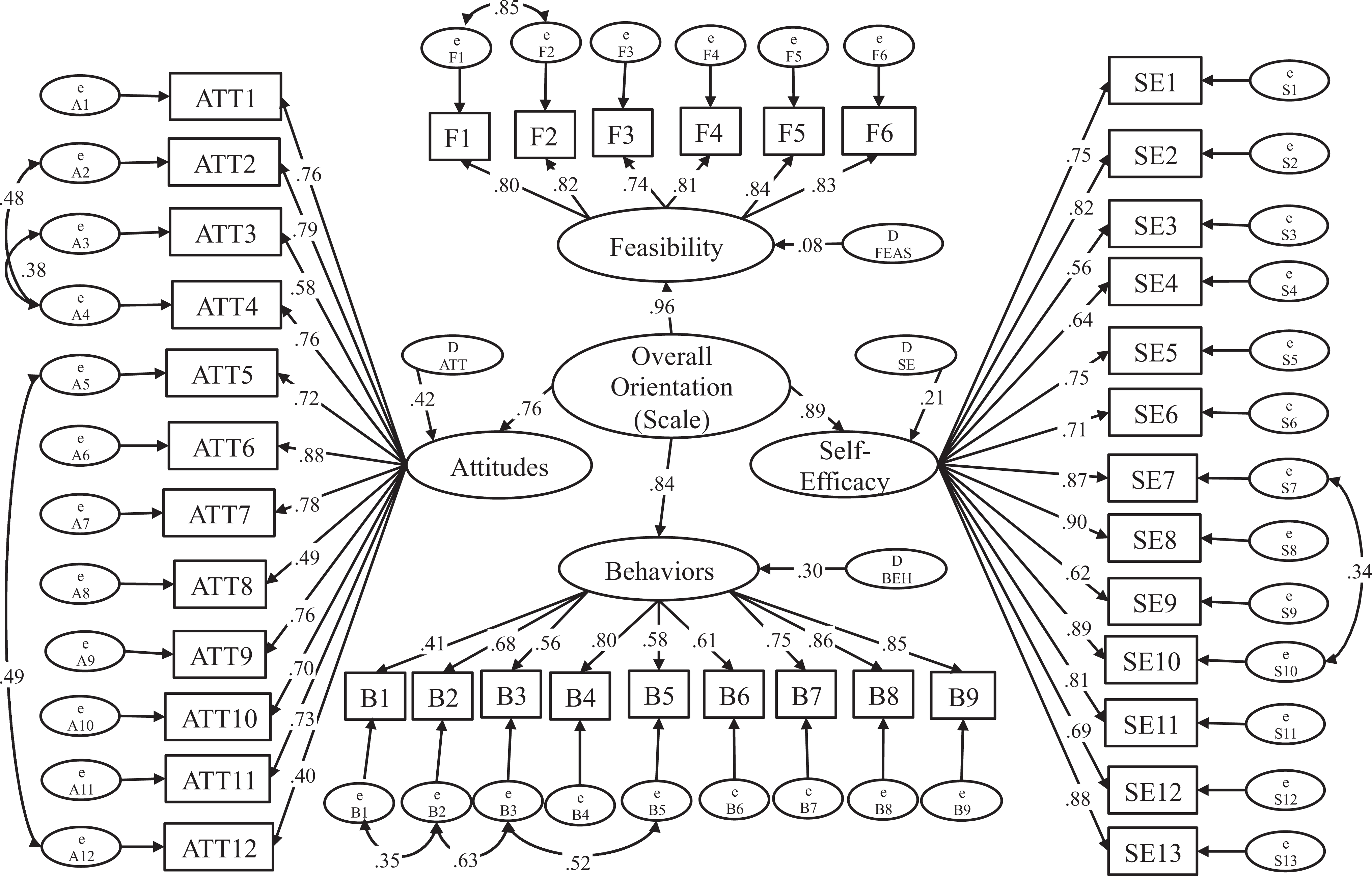
Second-order model (includes standardized loadings).
Summary of CFA Fit Results.
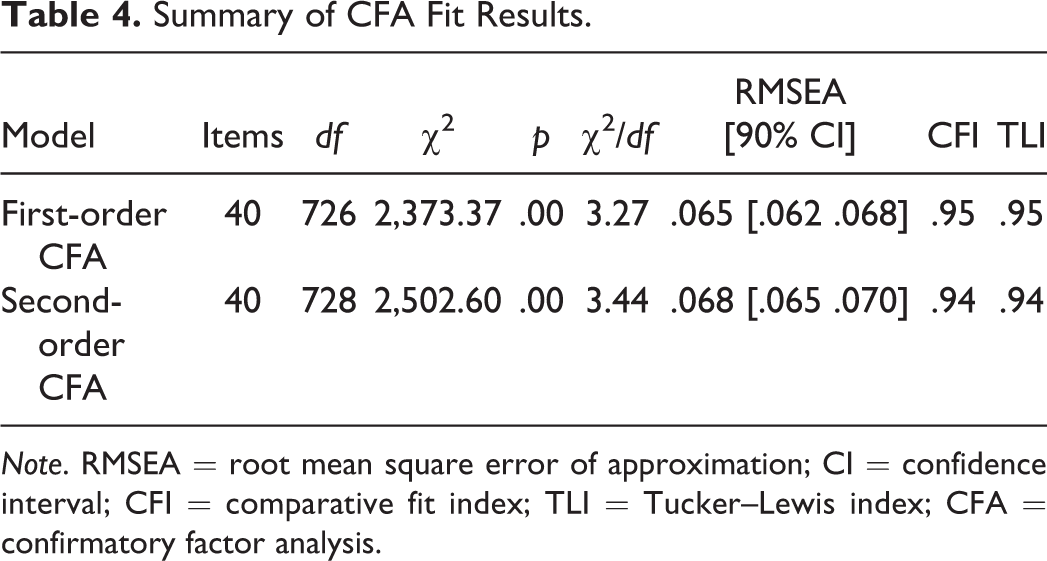
Note. RMSEA = root mean square error of approximation; CI = confidence interval; CFI = comparative fit index; TLI = Tucker–Lewis index; CFA = confirmatory factor analysis.
Factor loadings and correlations
With a more diverse sample, Comrey and Lee’s (1992) suggested cutoff of .32 was used for standardized factor loadings. Three scale items were less than fair (below .54) but were retained in the instrument. Twenty-seven of the 40 items were considered excellent, loading above .71, 4 were considered very good (.63 to .70), and 6 were considered good (.55 to .62) (Comrey & Lee, 1992). The scale’s convergent validity was established by assessing the subscales’ standardized factor loadings, which were excellent, ranging from .76 to .96 (Kline, 2016). Subscale correlations were examined to assess for discriminant validity, ensuring none of the subscales were highly correlated with one another (>.85, or 28% unique variance; Kline, 2016). Like the original study, self-efficacy and perceived feasibility had a slightly higher correlation (.89); however, with a correlation of .89, 21% of the variance remains unique to each of the two theoretically different constructs, which were maintained.
Discussion and Applications
The purpose of this study was to test the reliability and validity of the RSIPAS with a larger, more diverse sample of helping professionals, including clinical social workers, clinical psychologists, marriage and family therapists, APNs, and professional counselors. The findings from this study support the reliability, criterion validity, discriminant and convergent validity, as well as the factorial/construct validity of the RSIPAS, with this diverse pool of helping professionals. The factor analyses for both the first- and second-order analyses had adequate fit, indicating factorial validity for the four subscales and overall scale, measuring practitioners’ orientation toward integrating clients’ RS in practice.
Interestingly, as compared with the original study, which was purely a clinical social work sample, the RSIPAS’s model had a better fit with the current data, with its diverse sample of five helping professions. Specifically, looking at the second-order model, the RMSEA dropped from .077 (90% CI: [.074, .080]) to .068 (90% CI: [.065, .070]), the TLI and CFI both increased from .92 to .94, all indicating an improved fit. Further, although the reliability for the overall instrument, the Self-Efficacy, Attitudes, and Behaviors subscales remained the same as compared with the original study, Cronbach’s α increased slightly (.04) for the Perceived Feasibility subscale.
These results suggest the instrument may now be used with other helping professions besides social workers, including psychologists, marriage and family therapists, counselors, and nurses. With the widening and diversifying of the current sample, it may be of interest to interdisciplinary agencies, settings, or practice teams to assess various professions’ areas of strength for including this portion of clients’ lives in treatment or identify opportunities for growth. Especially considering many helping professionals have not received training on this area of practice, this instrument could serve as a baseline to assess new hires’ views and behaviors regarding this area of practice, or even practitioners who have been with the agency or setting for years, and monitor change over time. It also may serve as a tool by which more discussion can be facilitated on how, when, and in what ways clients’ RS beliefs are being considered in practice or methods to improve this process through inter- and transdisciplinary training. Should one profession be much stronger in this practice area—for example, marriage and family therapists, as found in Oxhandler and Parrish (Under review)—this could create an opportunity for professions to learn from one another around this practice area. Similarly, areas in which various professions struggle, or items in which respondents typically score lower on, could serve as topics of discussion among these helping professions. This would be especially true in settings such as hospitals, mental or physical health clinics, private practice, or social service agencies where interdisciplinary and transdisciplinary collaboration often occurs. Finally, agencies may also consider surveying clients and patients regarding their preferences surrounding integrating their RS beliefs and practices and pair the results with how the helping professionals respond to the RSIPAS, ensuring clients’ RS needs are being attended to and identifying opportunities for improvement.
Considering that many of these professions have communicated a desire for increased training on integrating clients’ RS in practice, this instrument may also serve as a method for implementing and evaluating such training efforts in graduate education and CE. Particularly given the lack of standardization in many postgraduate CE trainings (Thyer & Pignotti, 2016), this reliable and valid instrument may help guide and ensure CE content is the most relevant and empirically supported. Additionally, graduate programs from these five professions may consider using this instrument to guide the delivery of content related to RS in practice and evaluate the degree to which students’ self-efficacy, attitudes, perceived feasibility, and behaviors change throughout their education. Similarly, graduate programs among these professions may want to assess the degree to which their alumni are attending to this area of clients’ lives as a way to evaluate their graduate program, identifying gaps in which the graduate program may fill via CE efforts. Finally, given that internship opportunities are often a critical component of training across helping professions, graduate programs may wish to assess their clinical faculty or internship/field instructors’ orientation toward this area of practice to ensure students are receiving proper training and consultation in the field.
Although this study has a number of strengths, it is certainly not without limitations. Although the sample size was adequate to combine the five professions’ responses, the overall response rate was lower than anticipated. Along the same vein of the issue with response rate, one unforeseen limitation to this study was the number of participants who struggled with accessing the SurveyMonkey link. A total of 20 participants e-mailed the author, stating that upon entering the website link, their browser tried searching for the link (e.g., Google search), resulting in a page that said “Your search did not match any documents” rather than connecting them directly to the link. Although the investigator replied with the direct link for each of these individuals, of which six were reportedly able to connect to the survey, it is unknown how many others tried connecting to the link, were unable to, and did not attempt to contact the investigator. Additionally, although the sample largely reflects these licensed professionals in the United States who are mostly White, older women (Center for Health Workforce Studies, 2006; Center for Workforce Studies & APA Center for Workforce Studies, 2015; Northey, 2002; U.S. Department of Health and Human Resources and Services Administration, 2010), the psychometric properties of the RSIPAS might vary among those who are not. It is encouraging, however, that a sufficient number from each of the targeted disciplines participated in this study with an overall sample that was fairly large.
In conclusion, this study provides the evidence to support the use of the RSIPAS with clinical psychologists, social workers, marriage and family therapists, professional counselors, and nurses. Specifically, the RSIPAS may be used to assess these various helping professionals’ overall orientation toward integrating clients’ RS in practice as well as their self-efficacy, attitudes, perceived feasibility, and behaviors with regard to this area of practice. With further support of this instrument’s reliability and validity, it is the author’s hope that the RSIPAS may be used to continue supporting and evaluating training and education in this area of practice across disciplines and that the results of future studies which use this instrument will be shared.
Footnotes
Acknowledgment
The author would like to thank Baylor University’s Research Committee for their generous support of this project. The author would also like to thank Danielle E. Parrish, PhD, for her feedback during this follow-up study.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.