
Abstract
Purpose:
Virtual reality exposure therapy (VRET) is an intervention used to treat alcohol and nicotine dependence that delivers cue exposure therapy using a virtual reality environment; however, little is known about the effects of these interventions.
Method:
We used systematic review methods to examine the effects of VRET on alcohol or nicotine dependence, craving, and substance use with persons with current nicotine or alcohol dependence. We conducted a comprehensive search to retrieve published and unpublished intervention studies in 18 databases and other gray literature sources. Studies were screened, and data were extracted by two independent reviewers.
Results:
Five studies including 212 participants were included. Effects were found for alcohol and nicotine dependence and craving; however, significant methodological issues and high risk of bias were present across studies.
Conclusion:
Evidence of effects of VRET is sparse, and methodological flaws and gaps in reporting were identified. Implications for practice and research are discussed.
With more than 80 million adults abusing drugs or alcohol and 40 million meeting diagnostic criteria for addiction, the use and misuse of substances is one of the greatest and costliest public health problems in the United States (The National Center on Addiction and Substance Abuse at Columbia University [NCASA], 2012). The two most prevalent abused substances, nicotine and alcohol, account for a significant portion of these public health costs. Nicotine dependence results in a staggering US$170 billion per year in annual health costs (Xu, Bishop, Kennedy, Simpson, & Pechacek, 2015). While use has been on decline since the 1980s, nearly 42 million adults and 3.5 million adolescents consume cigarettes, and nicotine remains the second leading cause of U.S. deaths (U.S. Department of Health and Human Services, 2012). Prevalence of alcohol abuse also remains significant, with 15.1 million U.S. adults 18 and older meeting criteria for a substance use disorder (Substance Abuse and Mental Health Services Administration, 2015). Furthermore, alcohol-related public health costs due to consequences of drinking result in approximately US$250 billion dollar spent per year (Sacks, Gonzalez, Bouchery, Tomedi, & Brewer, 2015). With 88,000 annual deaths related to alcohol abuse and consequences, alcohol consumption is the second leading cause of preventable death (Centers for Disease Control, 2010), with nicotine dependence the first. Combining these two, alcohol- and nicotine-related use is the leading cause of preventable death in the United States.
The use of alcohol and nicotine is often correlated; alcohol consumers are 3 times more likely to smoke and nicotine consumers are 4 times more likely to consume alcohol (Grant, Hasin, Chou, Stinson, & Dawson, 2004) than those who do not consume alcohol or nicotine, respectively. It has been suggested (McKee & Weinberger, 2013; Verplaetse & McKee, 2017) that a similar path for alcohol and nicotine cue exposure reactivity and resulting craving may be due to activation of the mesolimbic reward pathway, with a release of dopamine within the nucleus accumbens and ventral tegmental area (VTA; Gonzales & Weiss, 1998; Nestler, 2005). Nicotinic acetylcholine receptors (nAChRs) are activated using nicotine, potentially enabling the release of neurotransmitters such as acetylcholine, dopamine, glutamate, and others into the presynaptic cleft (Dani & Harris, 2005; Giorguieff-Chesselet, Kemel, Wandscheer, & Glowisnki, 1979). Once released, these neurotransmitters are mediated by dopamine release within the NA and VTA. While alcohol reinforcement may not be based solely on the same neurotransmitters (i.e., serotonin is released during alcohol consumption, but not activated by nAChRs), the mesolimbic reward pathway (NA, VTA) is involved in producing dopamine similarly for both substances (Gonzales & Weiss, 1998; Nestler, 2005). Furthermore, alcohol consumption may activate nAChRs and increasing dopamine production in the VTA and NA while interacting with the nAChR system to produce reward (Blomqvist, Engel, Nissbrandt, & Söderpalm, 1993; Söderpalm, Löf, & Ericson, 2009; Tizabi, Copeland, Louis, & Taylor, 2002). As the systems of reward are activated through the same mesolimbic reward pathway, it appears that they may work in unison to provide a combined effect, acting similarly in the way that they produce dopamine to provide a reinforcement for use (McKee & Weinberger, 2013; Verplaetse & McKee, 2017).
The use of alcohol or nicotine may be conditioned by craving for dual use (Drobes, 2002). Craving for alcohol is often stimulated by nicotine-related cues and vice versa, indicating cross-referencing of cues related to alcohol and nicotine dependence. This cross conditioning may result in the nicotine-dependent individuals increased likelihood to use alcohol (S.-W. Choi et al., 2014). It appears that cue conditioning often induces craving between the two substances, contributing to dual and cross addiction and comorbid effects of consumption (S.-W. Choi et al., 2014). Due to the prevalence of dual use, as well as the similar pathways and cross conditioning of craving, it is appropriate to simultaneously evaluate virtual reality (VR) cue exposure therapy (CET) intervention outcomes for both alcohol and nicotine dependence.
Effectiveness of Substance Use Treatment Efforts
While US$28 billion a year is spent to treat addiction, 95% of that funding pays for the consequences of addiction while only 2% goes toward prevention or treatment (NCASA, 2012). Due to addiction stigma, federal funding of the costs of substance abuse primarily pay for consequences (law enforcement, judicial, etc.). Within an environment of limited public funding, treatment expectations are considered ideal when the treatment is brief and cost-effective (Babor, Del Boca, & Bray, 2017). Additionally, within the private sector, insurance companies have influenced treatment length and duration, retiring long-term treatment modalities and replacing them with short-term brief therapy (Maclean, Popovici, & Stern, 2018) . As intervention episodes continue to decrease in length and duration, outcome expectations have increased. Due to costs associated with alcohol and drug addiction, third-party reimbursement rates, and the need for efficient use of money for the treatment of addiction, National Institute of Drug Abuse (NIDA, 2016) has focused further efforts to support evidence-supported interventions for addiction treatment.
Efficacy of CET
CET aims to reduce cue reactivity through extinction by exposing the individual to the drug-related cue repeatedly leading to habituation and reduction of cue reaction (J.-H. Lee et al., 2004). The method is based on classical conditioning; as the cue is reinforced with a different outcome, the individual begins to loosen associations between the cue and the previously experienced outcome. CET first saw success in treating individuals struggling with phobic anxiety disorders and obsessive-compulsive disorders (Marissen, Franken, Blanken, Brink, & Hendriks, 2007).
The concept of craving when referring to substance abuse is defined as an intense desire to use substances (Pericot-Valverde, García-Rodríguez, Gutiérrez-Maldonado, & Secades-Villa, 2015; Sayette et al., 2000; Tiffany, 1990). Various studies have captured the effects of cue exposure on self-reports of craving (Carter & Tiffany, 1999). Specifically, in addiction research, cue exposure to drug-related stimuli has been shown to elicit craving in individuals struggling with addiction (Carter & Tiffany, 1999). It is generally accepted that drug use and relapse can be brought on by cue-induced cravings, making CET a potentially viable option for the treatment of substance abuse disorders (J.-H. Lee et al., 2004). Despite the potential for using CET for treating alcohol use disorders, surprisingly, CET has demonstrated limited effects on reducing alcohol use disorders (Mellentin et al., 2017). CET has not consistently been shown to be more effective than other treatments like cognitive behavioral therapy (CBT), and it is believed that there are certain factors limiting the effectiveness of CET (Kavanagh et al., 2006). One of those factors is the ecological validity of cues (Kavanagh et al., 2006). Realistic cue exposure experiences are often costly and hard to replicate as they typically require a real bar/environment and paid actors (Bordnick et al., 2008); thus, many CET sessions occur at inpatient treatment centers and do not adequately mimic a realistic exposure environment (Kavanagh et al., 2006).
VR CET
One potential solution to mitigate many of the current limiting factors for delivering CET is VR. VR is a computer-generated simulation, often using a head mounted display (HMD), to experience a virtual environment (Hale & Stanney, 2015). Fox, Arena, and Bailenson (2009) offer that a “virtual environment (VE) is a digital space in which a user’s movements are tracked and his or her surroundings rendered, or digitally composed and displayed to the senses, in accordance with those movements” (p. 95). Within the HMD, an individual will experience what is known as immersion which occurs when one loses oneself in the digital environment and shuts out cues from the physical world (Fox, Arena, & Bailenson, 2009). Because the environments are created and edited digitally, there are more options for tailoring them to the client and sharing them across time and space. VR is increasingly being used across the health-care field from rehabilitation after strokes to understanding the effects of hearing loss on multitasking (Lau, Pichora-Fuller, Li, Singh, & Campos, 2016). VR is also being used in the mental health profession for treating social anxiety and post-traumatic stress disorder (Reger et al., 2016).
VR cue reactivity has been tested for both nicotine (Bordnick, Graap, Copp, Brooks, & Ferrer, 2005) and alcohol (Kwon, Choi, Roh, Yang, & Lee, 2006) with positive results. Participants exposure to addiction-related cues in a virtual environment experience significant increases in subjective craving following exposure (Bordnick et al., 2005). Three-dimensional representations of cues have also been shown to elicit a higher level of craving than static images (J.-H. Lee et al., 2004). The ability of VR environments to elicit cravings through cue exposure is important to the potential efficacy of VR exposure therapy (VRET) because extinguishing craving seems to hinge on the ability to elicit it first (Hone-Blanchet, Wensing, & Fecteau, 2014). While much research exists indicating the ability of addiction cues in VR environments to induce craving, there has yet to be a consensus around the efficacy of VRET with multiple exposures for the purpose of extinction as an intervention to increase positive outcomes in substance use disorder treatment (Hone-Blanchet et al., 2014).
Objectives
The purpose of the present study is to systematically and quantitatively measure the effect of VRET on alcohol or nicotine craving, dependence, and usage with adults who are alcohol or nicotine dependent. Specific questions guiding the review are as follows: (1) What is the state of evidence regarding the use of VRET for the treatment of alcohol or nicotine dependence and (2) What are the effects of VRET on alcohol or nicotine craving, dependence, and usage with adults identified as nicotine or alcohol dependent?
Method
The conduct of this review, including search, selection, and coding of studies, followed systematic review procedures (Methods Group of the Campbell Collaboration, 2017). Meta-analytic methods were planned to synthesize outcomes reported from studies meeting inclusion criteria; however, there was an insufficient number of studies reporting data needed to calculate effect sizes on any of the outcomes, thus meta-analysis was not possible. The protocol for the review, developed a priori, is registered with PROSPERO (Registration #CRD42018087663; Trahan, Smith, & Maynard, 2018). Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA; Moher, Liberati, Tetzlaff, & Altman, 2009) guidelines were followed for reporting of this review.
Eligibility Criteria
Study design
Published and unpublished studies were included in this review if they employed a randomized controlled trial (RCT) or quasi-experimental design (QED) with a comparison group that received treatment as usual, no treatment or were wait-listed, or an alternative treatment. Due to the nascent nature of VRET interventions and sparse RCT and QED studies in this area, we chose to modify the protocol to include single-group pre–posttest studies to obtain a more complete assessment of the VRET intervention research being conducted to treat nicotine and alcohol dependence.
Participants and settings
To be included in this review, participants must have been adults (age 18 and older) identified as nicotine dependent or alcohol dependent using the DSM criteria of the version applied by study authors at the time of the study. Procedures for diagnosis must have included a general and structured clinical interview (based on DSM criteria applied by the study authors dependent upon the version current at the time), written history and sociodemographic questionnaires, either/both over the telephone and in person, or validated/reliable scales for the condition. We included studies from any setting. Studies including children or adolescents (17 or younger), dependence/abuse of chemicals other than nicotine or alcohol, and cue exposure studies that only measure cue reactivity with singular exposure were excluded.
Interventions
Interventions using VRET were included in this review. VRET is a combination of exposure therapy and virtual simulations to provide the participant with a greater sense of presence for habituation (for more information, see Hone-Blanchet et al., 2014). VRET for addiction consists of exposure to virtual scenarios that contain images related to substance use or cues including scenarios in the presence of nicotine or alcohol or scenarios of places where nicotine or alcohol is normally consumed. The purpose of exposure to these scenarios is to habituate to cue reactivity by consistent exposure to cue-related situations. VRET requires computer hardware and software that can deliver virtual simulations, providing the viewer with a sense of presence, or feeling as if one is experiencing the VR scenario (Lombard & Ditton, 1997). Computer programs like Second Life which are experienced on a two-dimensional (2-D) computer monitor and do not use VR headsets and three-dimensional computer graphics were excluded from this review. Studies that include other interventions with VRET, such as CBT and coping skills, were included.
Outcome measures
To be included in this review, study authors must have measured outcomes related to dependence, craving, or use using standardized measures. Instruments for alcohol craving may include the Penn Alcohol Craving Scale (Flannery, Volpicelli, & Pettinati, 1999), the Alcohol Urge Questionnaire (Bohn, Krahn, & Staehler, 1995), and Obsessive-Compulsive Drinking Scale (Anton, Raymond, Moak, & Latham, 1995). Instruments for nicotine craving may include the Urge to Smoke Scale (Jarvik et al., 2000) and both brief and long version Questionnaire of Smoking Urges (QSU; Cox, Tiffany, & Christensen, 2001; Tiffany & Drobes, 1991). Alcohol dependence may include instruments such as the Michigan Alcohol Screening Test (Selzer, 1971), The Alcohol Use Disorders Test (Babor, de la Fuente, Saunders, & Grant, 1992), and/or other standardized measures. Nicotine dependence may include instruments such as Nicotine Dependence and Use Structured Clinical Interview (SCID I/P; First, Spitzer, Gibbon, & Williams, 1996), the Fagerstrom Test for Nicotine Dependence (FTND; Heatherton, Kozlowski, Frecker, & Fagerstrom, 1991), and the Nicotine Dependence Syndrome Scale (Becoña, Fernández Del Río, Durán, & Míguez, 2009).
Time frame and geographical context
Studies must have been conducted between 2000 and the time of our search, which occurred in November 2017. Due to resource constraints, studies must have been published in English but could have been conducted in any country; studies were not excluded due to geographical location.
Search Procedures
A comprehensive and systematic search procedure was conducted in November 2017 to identify all relevant published and unpublished research that met inclusion criteria. Electronic databases for this search included Academic Search Complete, Academic Search Ultimate, Applied Science & Technology Source Ultimate, Business Source Ultimate, CINAHL Complete, Complementary Index, Directory of Open Access Journals, Education Source, Food Science Source, MEDLINE Complete, PsycARTICLES, PsychINFO, Science Citation Index, ScienceDirect, Scopus, Social Sciences Citation Index, Sociology Source Ultimate, and SPORTDiscus. Additionally, we searched Google Scholar. Combinations of the following search terms were used: “virtual reality” OR “virtual environment” OR “augmented reality” AND “substance abuse” OR “addiction” OR “craving.” We also reviewed reference lists of included studies and contacted authors with multiple published articles related to addiction interventions using VR to find unpublished studies or studies currently in progress.
Study Selection, Data Extraction, and Analysis
Titles and abstracts of studies identified through the search procedures were initially screened for relevance by one of the review authors. Those that were obviously ineligible were screened out. For example, studies deemed ineligible at this stage were those that did not involve the target population (e.g., adolescents), did not involve an intervention, or were descriptive or theoretical in nature. The full text of all articles that were not obviously ineligible was retrieved for further review and screened using a study screening instrument that included all eligibility criteria. Two reviewers then independently screened the full text of each potentially eligible article to determine inclusion. Discrepancies regarding inclusion decisions were reviewed and discussed between the two reviewers. If agreement regarding eligibility could not be reached by consensus, the reviewers consulted with two additional reviewers who provided input and made the final decision by consensus.
After agreement was reached on inclusion of eligible studies, two reviewers then independently extracted data from all studies using a data extraction tool developed by the review team (the data extraction tool is available from the authors by request). Prior to data extraction, the reviewers pilot tested the coding instrument, adjusting if necessary, to clarify items. Coding categories included the following: (1) source descriptors and study context, (2) sample descriptors, (3) intervention descriptors, (4) research methods and quality descriptors, and (5) effect size data. Risk of bias was also assessed by two independent reviewers using the Cochrane Risk of Bias tool (Higgins & Altman, 2008) for the following domains: selection bias, performance bias, detection bias, attrition bias, and reporting bias. All studies were rated on each domain as low, high, or unclear risk of bias. Data were extracted and input into an Excel spreadsheet by each coder. After independent extraction, the codes were reviewed, and discrepancies were resolved by discussion and consensus. If questions about coding could not be resolved, two additional reviewers were consulted, and final decisions were made by consensus. If data were missing from the reports, attempts were made to contact authors to request missing data.
Analyses were designed to produce descriptive information on the characteristics of all included studies, interventions, and outcomes across all included studies, with additional detail narratively reported for each included study. We planned to conduct a meta-analysis of outcomes reported in randomized and quasi-experimental studies to examine mean effects across studies; however, there was not an adequate number of studies reporting on any of the outcomes. Effect sizes were calculated, using the standardized mean difference effect size statistic, for outcomes when authors reported enough information to calculate an effect size. If sufficient information was not reported by study authors, and authors did not respond to requests for that data, we reported effect sizes as reported by primary study authors when available. If effect sizes could not be calculated by review authors and were not reported by study authors, we reported outcomes as described by the study authors. Due to the number of studies included in this review, it was not possible to assess publication bias.
Results
Study Search and Selection
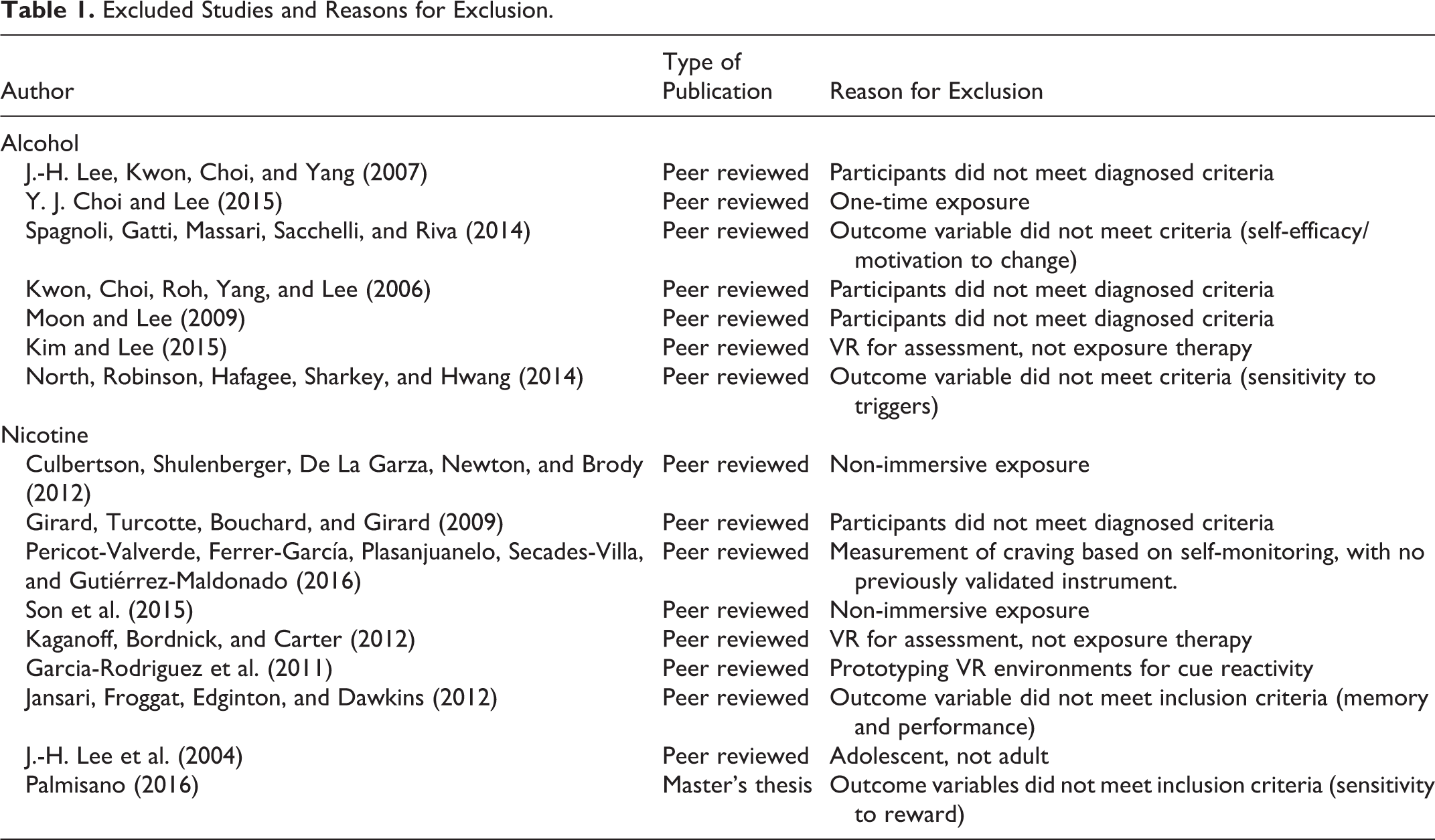
The search procedures yielded 1,267 citations. After duplicates and obvious ineligible studies were removed, 54 studies were identified and screened for eligibility by two reviewers for inclusion. Initial full-text screening of articles by reviewers identified cue reactivity studies (n = 32) that did not include multiple session exposure therapy and thus were excluded. After full-text screening of remaining studies, 16 studies were excluded due to not meeting the following eligibility criteria (see Table 1): participant inclusion criteria of addiction diagnosis not met (n = 4), outcome variable did not meet inclusion criteria (n = 4), single VRET exposure (n = 1), assessment not treatment (n = 2), non-immersive or 2-D virtual exposure (n = 2), nonvalidated scale of craving measurement (n = 1), prototyping study (n = 1), and adolescent participants (n = 1). The remaining six articles met criteria for inclusion in the review; however, one article appeared to replicate results but focused on moderator analysis. Thus, this article was included as secondary to a publication in the analysis. The final sample included five studies. See Figure 1 for flowchart outlining the search and selection process.
Excluded Studies and Reasons for Exclusion.
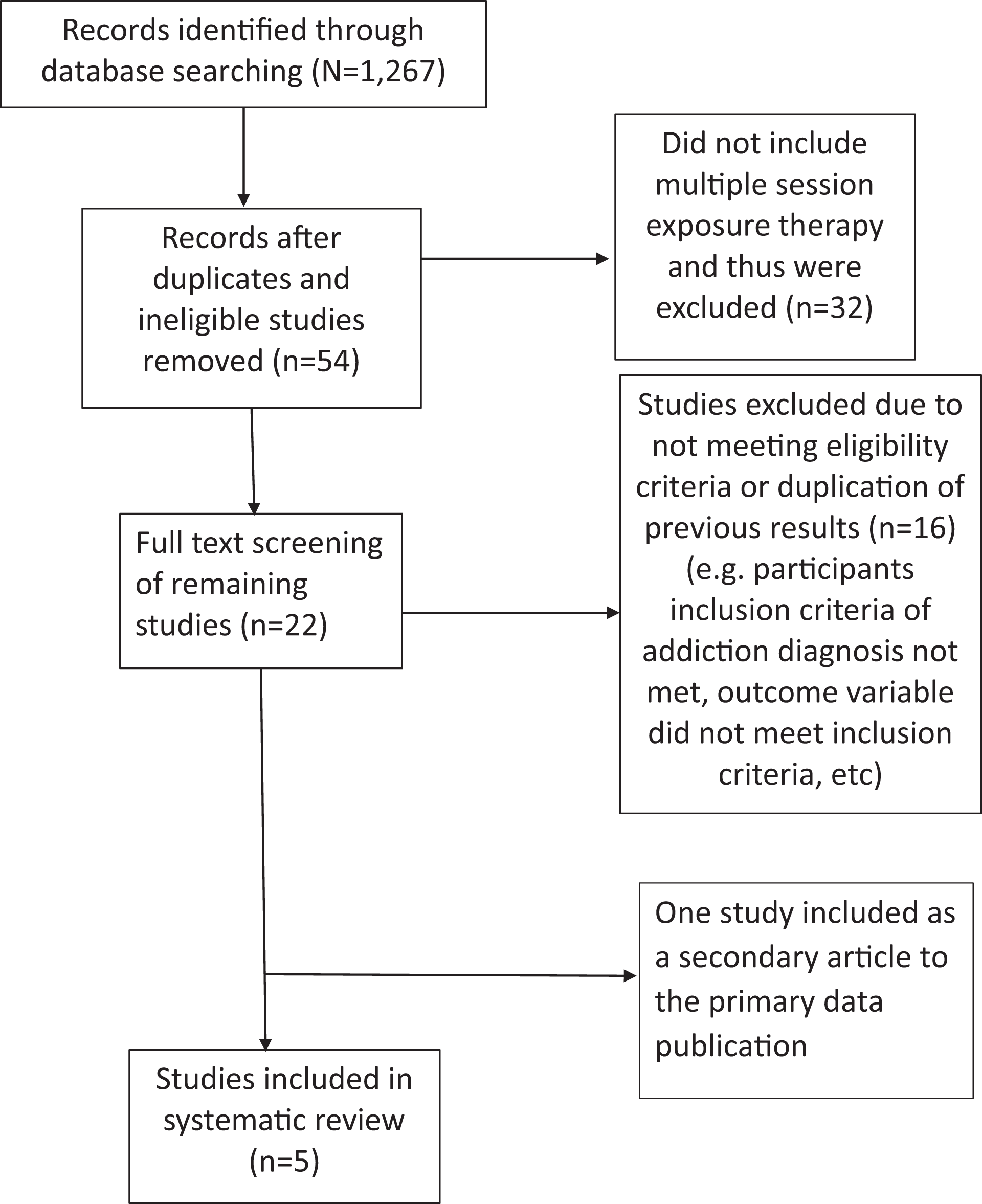
Study selection flowchart.
Study Characteristics
Table 2 summarizes the five included studies. All studies were published in peer-reviewed journals. The country of origin of the studies included the United States (n = 1), Spain (n = 1), and South Korea (n = 3). Forty percent of the included studies employed a single-group pre–posttest design (n = 2), 40% employed a QED (n = 2), and only one employed an RCT design (20%). Most of these studies were published after 2011 (n = 4, 80%), while one study was published in 2009. Sample sizes were relatively small, with all but one having under 50 participants (n = 4, 80%). Most of the studies focused on VRET treatment for nicotine/cigarette dependence (n = 4, 80%), including 174 participants in those studies, while one study focused on alcohol dependence with 38 participants. For the three studies that used a comparison group design, a total of 75 nontreatment sample participants received either an alternative treatment (n = 2) or treatment as usual (n = 1). The alternative treatment with which VRET was compared included cognitive behavioral therapy (Park et al., 2014) and education with cognitive therapy (S.-H. Lee et al., 2009). Treatment as usual used in the Bordnick, Traylor, Carter, and Grapp’s (2012) study was nicotine replacement therapy (NRT).
Characteristics of Included Studies.
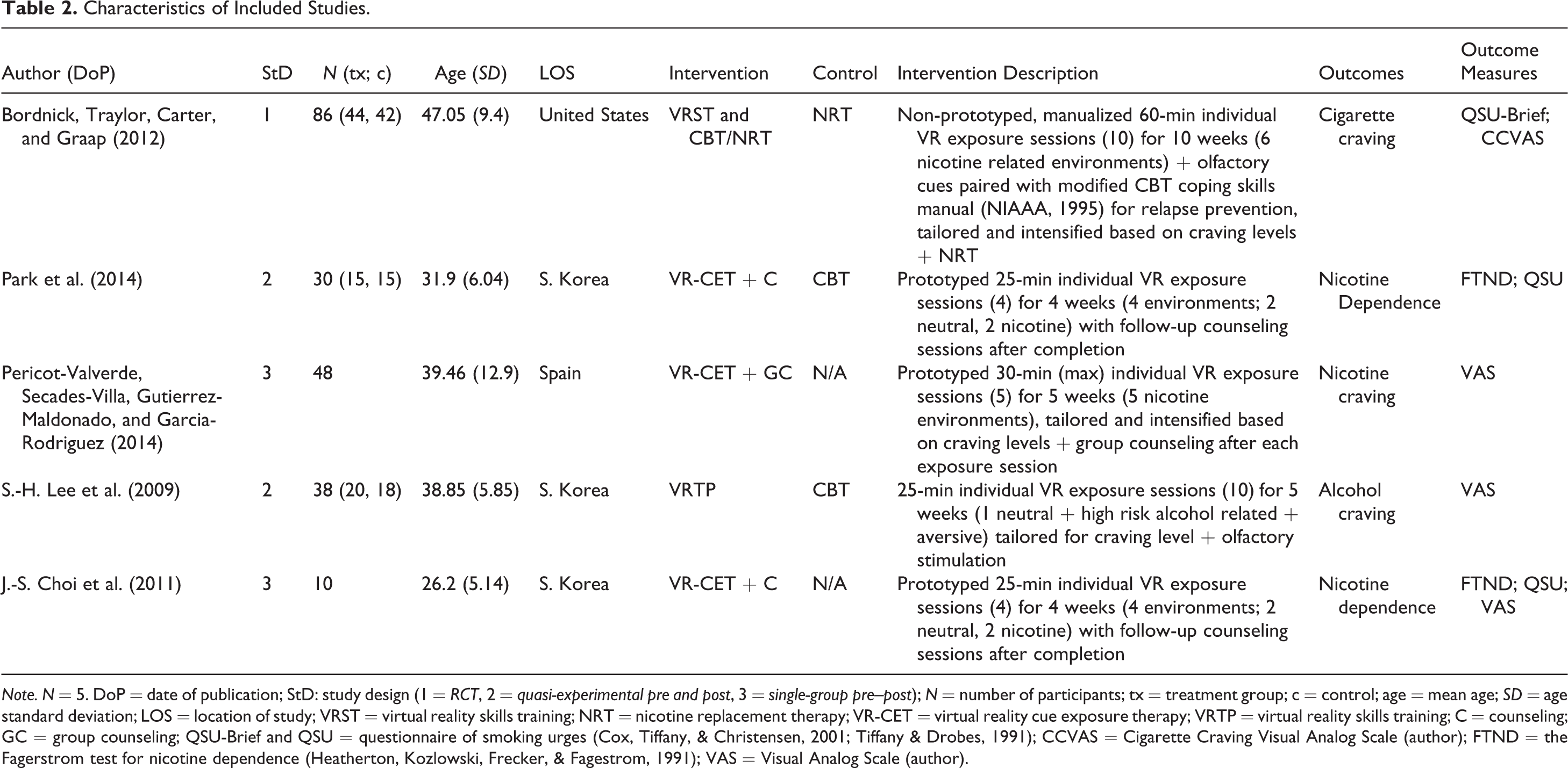
Note. N = 5. DoP = date of publication; StD: study design (1 = RCT, 2 = quasi-experimental pre and post, 3 = single-group pre–post); N = number of participants; tx = treatment group; c = control; age = mean age; SD = age standard deviation; LOS = location of study; VRST = virtual reality skills training; NRT = nicotine replacement therapy; VR-CET = virtual reality cue exposure therapy; VRTP = virtual reality skills training; C = counseling; GC = group counseling; QSU-Brief and QSU = questionnaire of smoking urges (Cox, Tiffany, & Christensen, 2001; Tiffany & Drobes, 1991); CCVAS = Cigarette Craving Visual Analog Scale (author); FTND = the Fagerstrom test for nicotine dependence (Heatherton, Kozlowski, Frecker, & Fagestrom, 1991); VAS = Visual Analog Scale (author).
Participant Characteristics
A total of 212 adults participated in the studies included in this review. All studies had participants who met criteria for nicotine (n = 4) or alcohol dependence (n = 1), based on DSM-IV-TR (n = 1, 20%), DSM-IV (n = 2, 40%), or a standardized scale for measuring dependence (n = 2, 40%). The mean age of participants overall was 37 years of age (SD = 7.8). One study did not report race/ethnicity of participants, and one study reported all African American participants (n = 86, 40%). As more than half of the studies were conducted in South Korea, Korean participant race was strongly represented (n = 78, 36%). Including treatment and control, most participants were male (n = 146, 68%). All studies used severe mental illness as exclusionary criteria.
Intervention Characteristics
The format for VRET interventions was delivered on an individual basis in all studies. Sessions were generally administered once per week (n = 4) for 4–10 weeks (m = 5.6), for 24–60 min (m = 32.8). Total dose of VRET was 1.6–10 hr (m = 3.98). Qualifications of exposure provider were often not reported (n = 3).
VRET environments were commonly designed to stimulate craving cues; thus, often environments where alcohol or nicotine is consumed. Common environments included a virtual bar or pub (n = 3), restaurant (n = 3), or other venues for consuming nicotine or alcohol such as a whiskey house (n = 1) or beer garden (n = 1). Other environments included a convenience store, watching TV, a home environment, a street scene, and an airport lounge. VRET environments were prototyped in two of the studies prior to treatment and often tailored during treatment to the individual (n = 3). Only one of the studies used a manualized intervention, and only two studies reported that their protocol was tested for reliability (n = 2, 40%). No study reported how their environments were designed.
In addition to multiple exposures within environments, most studies (n = 4, 80%) paired a secondary intervention with exposure. These interventions included cognitive behavioral therapy and NRT (n = 1), individual counseling unspecified (n = 2), and group counseling unspecified (n = 1). All studies with secondary interventions did not include whether the research team delivered the paired intervention. Secondary intervention dosage was not reported in any of the studies. Only one study utilized a manualized protocol for the secondary intervention.
Most studies did not include information pertaining to the setting of the study (n = 4, 80%), with one study reported to be conducted at an outpatient facility. Furthermore, more than half of the studies did not indicate whether the researcher also provided the intervention (n = 3, 60%). In two of the studies, the researcher was active in planning, designing, supervising, or managing the treatment. Only one study reported that fidelity was monitored but not measured, while the other studies did not report any fidelity information. No study reported the computer platform on which the VR intervention was delivered.
Outcome Measures
Outcomes of interest for this study were nicotine or alcohol craving and dependence. All studies measured substance craving and two measured substance dependence (both nicotine). The studies employed commonly used measures for nicotine and alcohol dependence. For nicotine, outcomes were measured by a visual analog scale of 0–100 by self-report, the brief and long version of the QSU (Cox et al., 2001; Tiffany & Drobes, 1991), and the FTND (Heatherton et al., 1991). For alcohol, outcomes were measured using a visual analog scale of 0–100 for alcohol craving.
Study Design, Intervention, and Outcomes by Study
Studies examining effects on nicotine
A feasibility study of VR-based coping skills training for nicotine dependence
Bordnick et al. (2012) conducted a randomized control trial with a 10-week feasibility study of a VRET skills training with NRT to treat nicotine dependence. Eighty-six participants were randomly assigned to two groups, both groups receiving NRT. The treatment group received an individualized integrated treatment of both VRET and cognitive behavioral smoking cessation therapy with NRT, while the comparison group received NRT only. VRET sessions were 60 min in length, one session per week, provided by a master’s-level mental health clinician. VRET exposure environments included a party, driving with cigarettes on the dashboard, a restaurant with other smoking, an office building and courtyard with smokers present, a convenience store, and an airport smoking lounge. Fidelity was monitored, but measurement of fidelity was not reported. Measures included a nicotine dependence based on a structured clinical interview for DSM-IV (SCID 1/P), smoking history, the FTND (Heatherton et al., 1991), a time line of daily use, Smoking Confidence Questionnaire (SCQ; Condiotte & Lichtenstein, 1981), Smoking Abstinence Self-Efficacy Scale (SASE; DiClemente, Prochaska, & Gibertini, 1985), the Brief QSU (Cox et al., 2001), and a Cigarette Craving Visual Analogue Scale (CCVAS; Wewers, Rachfal, & Ahijevych, 1990).
Outcomes
The authors measured outcomes pre- and postintervention based on cigarettes smoked and craving measurement on the QSU. The authors reported a decrease in cigarettes smoked, confirmed using expired CO levels. The authors observed a statistically significant difference in cravings between groups at posttest, F(1, 39) = 6.6, p < .05, partial η2 = .37; 2 months posttreatment, F(1, 34) = 5.2, p < .05; and 6 months, F(1, 20) = 9.9, p < .01. Effect size calculation indicates a large effect of treatment (d = −.91; CI [−1.52, −.30]; Cohen, 1988). Furthermore, authors reported a significant difference between groups on the SASE and SCQ. The CCVAS was collected at baseline; however, outcomes were not provided by authors. The authors inferred from these results that VRET with CBT appears to be effective for smoking cessation. They further cautioned that results may be due to traditional skills training, not the virtual exposure, recommending further research comparing straight exposure session and traditional skills training for clarifying evidence.
Comparison of virtual CET and CBT for nicotine dependence
Park et al. (2014) conducted a quasi-experimental pre–post design study comparing VRET with CBT for smoking cessation. Each group consisted of 15 participants, receiving four sessions of either VRET or CBT once per week for 25 min in a medical outpatient setting. VRET participants received exposure therapy with one scenario of a VR bar, with neutral cues pre- and postexposure. The CBT group received individual counseling on smoking cessation and withdrawal education, coping skills, cognitive restructuring, and stress management from a psychiatrist.
Outcomes
Measures included expiratory CO concentration levels, the FTND (Heatherton et al., 1991), the Minnesota Nicotine Withdrawal Scale (Hughes, Gust, Skoog, Keenan, & Fenwick, 1991), and the QSU (Tiffany & Drobes, 1991). Baseline comparison of measurement indicated that there were differences between groups on the FTND (p = .03). Authors reported reduced levels of daily smoking count, expiratory CO levels, and nicotine dependence (FTND: F = 84.39, p < .01) for both groups, but no significant differences were found between groups on outcome measures. The authors concluded that both treatments may be effective for smoking cessation as treatment effects were roughly equal. Authors did not report enough data for our review team to calculate effect sizes and authors did not report effect sizes. The authors also noted that no subjective changes were found related to cravings, which they suggest was potentially due to the short-term nature of the intervention and lack of randomized assignment. They further acknowledge the need for a control group not receiving either intervention, larger sample sizes, and homogeneous groups for future research, particularly in the dimension of gender and current medication use.
Systematic cue exposure through VR on cigarette craving and individual variables related to craving reduction in cue exposure treatment
Pericot-Valverde, Secades-Villa, Gutiérrez-Maldonado, and García-Rodríguez (2014) conducted a single-group pre–post study evaluating the use of a hierarchical VRET on cue-induced cravings and smoking behavior. Participants (n = 48) who meet criteria for nicotine dependence (SCID; DSM-IV-TR) completed five sessions in 5 weeks of VR scenarios. Maximum exposure was 30 min in length. Scenarios for exposure were individually tailored to induce increasing levels of craving and included a pub, lunch in a home, breakfast in a home, coffee at a cafe, lunch at a restaurant, a street scene, and watching TV at night. The scenarios were previously prototyped and validated for inducing craving. After participant finished each exposure, they participated in a support/advice group with four to five other participants.
Outcomes
Measures included a clinical history form, the FTND (Heatherton et al., 1991), CO concentrations, a VR Presence Questionnaire (Slater, Steed, McCarthy, & Maringelli, 1998), and a craving VAS measured every 2 min during exposure. Outcomes were analyzed using the highest and last craving level during exposure. Authors reported that the highest value of cue-induced craving declined during sessions, F(44, 160) = 7.935, p < .001. Authors reported an effect size, using partial η2, of .68. Additionally, the authors reported the final value of cue-induced craving decreased over sessions, F(44, 160) = 7.188, p < .001, and reported a partial η effect size of .66. The authors also reported a significant decrease in cigarettes smoked per day and CO in expired air. They stated that cue-induced therapy sessions reduced craving, while noting that length of session, 8–20 min, may have been conditional and critical. The authors also acknowledged limited change between background craving and cue-induced cravings, indicating a lack of influence over craving from VR-specific exposure. The authors acknowledged limitations and threats to generalizability in the study, including small sample size, lack of a control group, lack of follow-up to determine long-term gains, lack of control for physiological changes using bio measures, and inability to control outside influences over smoking behavior.
Pericot-Valverde, García-Rodríguez, Gutiérrez-Maldonado, and Secades-Villa (2015) published another study similar to Pericot-Valverde et al. (2014), with a slightly different sample size and study purpose and outcomes, although it wasn’t clear to the review team whether there was overlap in the samples between the two studies and attempts to contact the author to clarify were unsuccessful; thus, we are reporting this study as a secondary report of the primary study described above. The purpose of this secondary study was to identify factors that may predict craving cues, including sociodemographic (age, gender, marriage status, and years of education), tobacco-related, and psychological characteristics, rather than outcomes of the intervention. Pericot-Valverde et al. (2015) used a single-group pre–post study using VRET on cigarette craving to determine whether individual variables were associated with outcomes. Like Pericot-Valverde et al. (2014), participants (n = 41) meeting criteria for nicotine dependence (SCID; DSM-IV-TR) completed five sessions in 5 weeks of VR scenarios. Scenarios were consistent with the previous study. Results of the multivariate analysis indicate that a decrease in craving was predicted by younger age, greater cigarettes smoked per day, higher values on delay discounting, and higher BDI-II scores, F(4, 35) = 4.38, p = .006.
Effect of repeated virtual nicotine CET on psychophysiological responses: A preliminary study
J.-S. Choi et al. (2011) conducted a single-group pre–post study to evaluate the effect of VRET on the psychophysiological responses in nicotine dependence. Participants (n = 10) assessed as moderately nicotine dependent on the FTND received four 1-hr VRET sessions over 4 weeks. A secondary intervention identified by authors as “simple counseling” was paired with VRET sessions. Further information about the secondary intervention was not reported. For VRET, participants were immersed in a virtual bar with multiple cues related to cigarette smoking. Participants were presented with a neutral cue at the beginning and end of the session, a park or an aquarium, and then two smoking cues, an object then a social situation. Craving was measured between each exposure and after all exposures were completed.
Outcomes
The authors administered a smoking history, FTND, and QSU. During exposures, participants rated their craving levels using a self-rated VAS from 0 to 100. CO expiration levels were also measured to verify follow-up abstinence report at Weeks 4 and 12. Authors report reduced daily smoking count, FTND, QSU, and expiratory CO level after 4 weeks of exposure therapy. Significant main effects were found on types of cue in session, F(3, 24) = 22.03, p < .01, and session number, F(1, 8) = 8.62, p = .01, utilizing the VAS. Effect size was not reported or calculated based on presented data. Authors note threats to validity and generalizability including small sample size, limited VRET sessions, and lack of a control group. Also, only one female participated in the study, indicating a gender-based homogeneous group.
Studies examining effects on alcohol
Quantitative electroencephalographic correlates of craving during VR therapy in alcohol-dependent patients
S.-H. Lee et al. (2009) conducted a two group quasi-experimental pre–post study to evaluate the effects of VR therapy in reducing cravings and increasing alpha wave activity in the frontal cortex in alcohol-dependent males. Twenty participants were treated using VRET, while 18 participants in the control received education and cognitive treatment. All participants were diagnosed using the DSM-IV and recently had completed detoxification in an inpatient program. All participants were medication free. A psychiatrist conducted the VRET groups, delivering 10 sessions, 2 per week for 5 weeks. Treatment sessions consisted of a 5-min relaxation exposure, 10-min high-risk situation exposure, and 5-min aversive simulation exposure. Relaxation scenarios included five relaxing landscapes. High-risk scenarios included four different environments (beer garden, whiskey house, restaurant, and pub), with exposure to four kinds of alcoholic beverages for olfactory stimulation (beer, soju, whiskey, and wine) tailored to individual preference. The aversive scenario was a video of an alcohol-dependent patient vomiting. The control group received six sessions of cognitive behavioral therapy and two sessions of education, 45 min in length per session.
Outcomes
Alcohol craving was assessed both during and after sessions using a 10-point VAS. EEG was also administered for examining changes in alpha wave activity. The authors reported that the VRET group exhibited greater decrease in cravings after the 10th session compared to the group that received education and cognitive treatment (F = 8.73, p = .01). Authors concluded that VRET was more effective than CBT, with greater reduction in craving. They hypothesized that tailored high-risk situations may have contributed to these findings. They acknowledged potential threats to generalizability and validity such as small sample size with large number of variables monitored over time and a short follow-up period.
Risk of Bias and Study Quality Across Studies
When conducting a review of intervention studies, it is important to assess the risk of bias, the extent to which the results of the study are valid, and from which one can infer a causal relationship between the intervention and the outcome. A synthesis of weak studies fraught with threats to internal validity will limit the extent to which one can use the findings to draw conclusions related to the effects of an intervention (Higgins & Altman, 2008). Due to the lack of experimental studies in this area, we chose to include weaker study designs, including preexperimental designs, to provide a more complete picture of the state of evidence, but it is important that we consider the bias that is present in these included studies and use caution in the inferences we make based on these studies.
We used the Cochrane Risk of Bias tool (Higgins & Altman, 2008) that is commonly used to assess risk of bias in experimental studies of intervention effects. Because three of the six studies used a preexperimental study design without essential experimental design features to guard against threats to internal validity (namely, a control group, but other features are also missing), those three studies were assessed to be at high risk of bias. Two of the five studies used a QED, with nonrandomized control groups, thus, demonstrate high risk of selection bias. The study by Bordnick et al. (2012) is the only study that was assessed to be low risk of selection bias. None of the included studies employed blinding of participants or personnel, thus all were rated high risk of performance and detection bias. Most of the studies were rated as low risk of attrition bias. Bordnick et al. had high attrition (n = 25, 30%), with exiting in both the treatment and control. Because the included studies did not have preregistered protocols, it is difficult to assess reporting bias; however, most of the studies did not report adequate data for review authors to calculate effect sizes. Overall, studies included in this review were assessed as moderate to high risk of bias.
Generally, all studies were conducted with convenience samples and smaller sample sizes (largest study was N = 86), limiting generalizability of results. Several studies neglected to publish important details such as credentials of the intervention provider and the setting of the experiment, thus limiting reproducibility and relevance for practice. Three of the five studies did report prototyping environments prior to the experiment, which validates that the exposure has some evidence to induce cues. Furthermore, all studies neglected to report information related to fidelity, either due to lack of measurement (n = 4) or absence of reporting (n = 1). An absence of information related to the publication authors’ role in the experiment is also suspect, thus we could not assess potential bias related to researcher allegiance. All but one study (Bordnick, Traylor, Carter, & Grapp, 2012) did not report or did not use a manualized approach to the exposure process. All authors of the included studies recognized study limitations and recommended that research on intervention effectiveness continue and that more rigorous research be conducted.
Discussion
As individuals continue to struggle to have access to quality care, treatment, and maintenance efforts for addiction (Wells, Klap, Koike, & Sherbourne, 2001), the issue of nicotine and alcohol dependence remains a significant health concern. The use of VR in the treatment of substance use could expand access and improve affordability of substance use treatment, particularly with increased accessibility through smartphone technology. The purpose of this review was to determine the state of research and examine effects of VR to treat alcohol and nicotine addiction and to establish a direction for future research in this area. This review included a total of five studies of which four assessed effects on nicotine dependence and one assessed effect on alcohol dependence. Overall, the evidence of the effects of VRET interventions on nicotine and alcohol addiction is sparse, and the studies that are available have important flaws and limitations. All included studies were at moderate to high risk of bias, and only one study used a randomized study design, thus confidence in the validity of the findings reported in the included studies is low. While the number and quality of studies included in this review precludes providing a clear answer on the effects of VRET interventions, this review provides a good indicator of the state of the evidence for VRET for alcohol and nicotine dependence and identified several important gaps to inform future research.
Although the quality of evidence in this review is low, evidence from the included studies points to potential promise of VRET interventions, particularly when combined with CBT (Bordnick et al., 2012). Included studies indicate positive results, with those studies reporting effect size data indicating moderate to large effect sizes in reducing craving, dependence, and cigarettes smoked. However, comparison to other evidence-based interventions not requiring technology such as CBT (Park et al., 2014) indicate that VR intervention may not be necessary to provide treatment, and further evidence is necessary to support VR as an additive effect. Because it does appear that this intervention shows promise, we recommend further evaluation that addresses many of the limitations of the studies included in this review including larger samples, randomized control design, and more care into measuring fidelity in the intervention.
Evidence from this analysis demonstrates several factors future researchers should consider when evaluating the implications of VR in substance abuse treatment. First, there is a significant variation between number of sessions, duration of session, and length or dose of exposure of stimuli. Thus, it is not clear what threshold an individual requires to obtain clinical results. Two studies determined that the number of sessions was an influential variable with one study reporting a greater decrease in cravings after the 10th VR treatment. Studies should focus on identifying key aspects of treatment, such as dosage requirements, so we can begin identifying standards of treatment when using VR with other treatments. Pericot-Valverde et al. (2015), a supplemental study not included in our sample set, identified several variables that may affect treatment outcomes such as age, number of cigarettes smoked per day, impulsivity, and depression levels. Further evaluation of moderators and mediators contributing to effects is important to determine key factors specific to certain contexts or populations (MacKinnon, 2011)and control for these factors in future research experiments. These outcomes allow us to understand what components of treatment are more influential thus informing practice.
Additionally, there was significant variance in the type of environments used in VRET. Fewer than half of the studies reviewed did not prototype the environments prior to implementation to validate cue reactivity or identify what matters in these spaces to impact the individual. Park et al. (2014) and Pericot-Valverde et al. (2014) reported a prior prototyping process of identifying and confirming that virtual environments produced cue reactivity, confirming that the environment is effective for virtual exposure therapy. The other included studies did not include this information; thus, it is not clear whether this was done across all studies. While many studies have evaluated VR environments for cue reactivity for both nicotine (Pericot-Valverde, Germeroth, & Tiffany, 2016) and alcohol (Bordnick et al., 2008), it remains necessary for researchers to report the process of evaluating how they developed the environments used in their experiments. Further research and reporting of specific elements of environments that stimulate craving would be helpful for future study and replication.
The included studies lacked important information about intervention fidelity, thus limiting validity and contributions to informing clinical practice. Only one study measured treatment fidelity, although the authors did not report the degree to which the intervention was delivered with reliable consistency. Only one study reported using a treatment manual, although did not monitor, measure, or report fidelity to the manualized intervention. Intervention fidelity is important, as it has implications for internal and external validity, statistical power, and magnitude of effect (Chen & Rossi, 1983; Durlak & DuPre, 2008; Moncher & Prinz, 1991; Resnick et al., 2005; Summerfelt, 2003). If interventions are not implemented as intended, internal validity is compromised, and it is unclear whether outcomes were related to the independent variable, other unknown influences, or the failure to implement the intervention as designed (Dumas, Lynch, Laughlin, Smith, & Prinz, 2001; Waltz, Addis, Koerner, & Jacobson, 1993). Moreover, for an intervention to be replicable and adoptable by clinicians, adequate information about the intervention is necessary. Similarly, without adequate detail in the reporting of the intervention, replication and comparison of studies is compromised (Smith, Daunic, & Taylor, 2007). Given that VRET interventions are relatively new and the combination of VRET and traditional methods is not well understood, it is critical that interventions be well described and fidelity measured. Future research examining effects of VRET should clearly describe and measure fidelity of the VRET intervention as well as any paired interventions provided with VRET.
VRET could benefit from more rigorous and sophisticated designed experiments. Only one study, Park et al. (2014), compared VR to an evidence-based intervention for reducing nicotine dependence. Initial evidence from this study demonstrated that standard face-to-face evidence-based interventions resulted in similar treatment effects to VR exposure. The similar effect observed from VRET and CBT in this study is promising in that results indicate that VRET may be an alternative intervention to face-to-face treatment, providing a potentially less expensive (ultimately), more accessible or preferred format by some people and thus allowing for more people to receive treatment. Unfortunately, cost-benefit, accessibility, and preference are not being measured or reported in current VRET studies. Furthermore, it might be best to isolate and evaluate the effect of VRET with and without a paired intervention, such as CBT, to understand the additive effect of VRET. Researchers may also consider multiple arms to compare VRET to a no-treatment control, an established evidence-informed intervention, such as CBT, alone, and VRET paired with a secondary intervention. Moreover, as research moves from a more exploratory focus to identifying key components of VRET treatment, it will be important for researchers to employ rigorous study designs, such as RCT, mitigating potential risks of bias and using larger samples. RCTs can be challenging when evaluating underdeveloped interventions; however, the use of rigorous study designs is critical towards building evidence of efficacy and effectiveness. There are several strategies to improve rigor and causal inference which VRET researchers could employ to improve the rigor, validity, and relevance of studies (Sanson-Fisher, D’Este, Carey, Noble, & Paul, 2014; Shadish, Cook, & Campbell, 2002).
In terms of measurement, most studies employed self-report measures. The use of self-report measures is common in substance use intervention research; however, self-report suffers from potential bias due to social desirability, with potential for greater positive presentation (Crowne & Marlowe, 1964). Particularly with smaller samples, VR research needs to employ additional metrics to ensure treatment outcomes. Biometrics, eye and position tracking, and neuroimaging can be used in VR environments to triangulate outcomes (J.-H. Lee, Lim, Wiederhold, & Graham, 2005). This information can be matched with self-report data to confirm outcomes. Social desirability scales may also be used to determine validity of self-report (Perinelli & Gremigni, 2016).
As technology continues to remain a significant factor within our social fabric, and as people continue to rely more heavily on technology to address issues in everyday life, research should continue to evaluate its applicability and impact on various health-related issues. With the VR market continuing to grow, allowing more and more users to gain access to the technology, research is critical toward developing a repository of evidence-based practice and identifying standards in both research and practice.
Implications for Social Work Practice
While VR technology for treatment is in the early stages of development and implementation, development of VR for treatment of addictions as well as other behavioral health problems for which social workers provide treatment is increasing rapidly and may soon be available on a much wider scale. Costs of commercial mainstream applications of virtual technology have plunged over the past decade. From 2000 to 2018, VR equipment dropped considerably in price, from US$20,000 to $30,000 to a current range of US$200–$500. While many of the more sophisticated systems use an expensive computer platform, smart phone applications are now accessible to most populations. Recent versions of iOS and Android mobile devices offer VR capability. For less than US$20, individuals can access Google Cardboard, while the Samsung Gear VR (US$99) is adaptable to any Samsung smart phone. Cost and availability position VR to become the next generation of public technology, thus increasing the potential for accessibility of applications and use of VR for a range of treatment options.
With costs of VR technology becoming increasingly affordable and access being more widely available, social workers may soon be in the position to adopt VR technologies in their practices and agencies; thus, it is important that social work practitioners be knowledgeable of technological advancements in treatment delivery and the state of the evidence of the effects of technology delivered treatment on outcomes. While there are few studies and the state of evidence is currently relatively weak, the research in the area of substance dependence points to some promise in use of VR for treatment. We anticipate with the growing interest, development and use of VR technology in general, and for use as a treatment modality, that research in this area will increase and we will have more evidence soon that can better guide the adoption of VR by social work practitioners.
While the evidence is still new and needs to be improved, there is some evidence that VR may offer an alternative exposure therapy technique, perhaps as effective as in vivo or imaginal exposure. As VR becomes more accessible via mobile phones, it may provide a complimentary or additive effect to traditional treatment methods. Studies of application based non-VR mobile technology delivered in addiction-based treatment in primary care settings demonstrate growing interest (Quanbeck et al., 2014) and positive effects (Quanbeck et al., 2018; Tofighi, Nicholson, McNeely, Muench, & Lee, 2017). Thus, it appears that mobile phone technology provides a promising platform for changing addiction behavior and may be the future for VR interventions. This technology-driven approach to treatment may be especially relevant to young adult populations, who are more likely to use their phones than older adults and may be more likely to maximize usability and effectiveness of a mobile application (Bae, Chung, Ferriera, Dey, & Suffoletto, 2018). Populations that feel more intimidated by technology, or do not recognize technology as an efficacious tool, may be less likely to access or utilize these interventions. Unfortunately, as the mean age of participants in studies identified through this review (m = 37) are primarily middle-aged adults, there is no evidence that this technology has more utility with a young adult population, thus more research on age differences and history of technological experience on VR intervention outcomes appears relevant.
Limitations
While this study made every attempt to rigorously review all research literature available, following PRISMA and Campbell Collaboration guidelines, there are limitations that must be considered. The authors chose not to include studies that relate to VR interventions for relapse prevention with an intention of focusing on populations exhibiting active addiction. Studies included in this review indicate current or recent active nicotine or alcohol addiction. The rationale for this decision includes concern that relapse prevention VR interventions may exhibit different effect sizes and results due to the participant stage of change (Prochaska & DiClemente, 1983; Prochaska, DiClemente, & Norcross, 1992). This study limited search to studies in the English language, due to the lack of translational resources for studies in other languages. From our current review, several of the studies were conducted in non-U.S. countries, indicating that international research of VRET is being conducted and published in English; however, there may be additional studies conducted in non-English-speaking countries that were published in other languages that are not included in this review. Second, VR is a growing technology and the use of VR for social interventions is growing; thus, it is possible that there are studies currently in process that are not included in this review. We made attempts to contact authors in this area of research to inquire about studies that we may have missed in our search process, but this line of inquiry did not produce any additional studies. This review is also limited by the quality of studies included. As previously stated, several of the studies did not use a control group and were assessed to have a high degree of risk of bias. Only one study included in our review contained a randomized control experiment, indicating that evidence supporting a causal relationship between VRET and reduced craving and dependence cannot be inferred. Additionally, due to the small number of studies and lack of reporting of data for the review team to calculate effect sizes, we could not conduct a meta-analysis. Furthermore, a lack of diversity among participants limits any generalizations about the effectiveness of the treatment.
Conclusions
This review provides the first synthesis of VRET for nicotine and alcohol dependence. Although only five studies met the inclusion criteria, the review provides an appropriate and worthwhile review of the state of evidence for VRET for alcohol and nicotine dependence. This review can serve as a call to researchers to improve the quality and reporting standards of VRET research. Furthermore, it suggests that standards be applied within the field to the process of prototyping, manualizing, and randomizing experiments, thus decreasing potential study bias and increasing causal evidence of VRET interventions. There is a need for further evidence of whether VRET is more effective than, or enhance effects of, other evidence-informed interventions, such as CBT. Additional data such as cost-benefit, accessibility, and preference should also be measured in VRET studies, as this information can be valuable to practitioners and consumers when deciding between interventions that have been demonstrated to have similar effects on the primary outcomes. This will require the use of larger samples and more complex study designs. Given that alcohol and nicotine dependence are significant public health issues, further research to inform practice to improve outcomes is important. VRET could be a more effective practice, provide an alternative to or enhance current practice, or provide greater access to care, but more and better research is needed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.