
Abstract
Purpose:
Recently, public health networks in Australia have introduced clinical research specialists to drive research in the allied health professions by helping clinical social workers engage in research. This study examines the benefits of a flexible research program for busy social work novice and experienced clinicians.
Methods:
Thirty hospital-based social workers were allocated a total of 12 research projects. Participants were given a mixed-methods survey both pre and post an education program with 17 responses for the presurvey and 12 responses postsurvey. The responses were coded via thematic analysis.
Results:
Despite initial clinician apprehension, the majority of participants found it beneficial. In the busy hospital context, support that was valued included simplified information and regular mentorship and training.
Discussion:
The role of a research lead with management support is pivotal in promoting a positive research culture and active research. However, clinical demand still reduces capacity to engage in research.
Keywords
Purpose
Research is the foundation of evidence and knowledge in the health sciences (Padgett, 2016). It continually advances clinical practice standards and ensures that these standards are effective and evidence-based (Slade et al., 2018). Research has long been an important part of health and allied health (Richardson-Tench et al., 2018). In social work, there is no single understanding of what constitutes social work research. It has been argued that social work research involves empirical inquiry such as research, evaluation, or analysis to develop knowledge related to service users, clinical practice, and education (Shaw & Norton, 2008). Similarly, Rubin and Ballie (2016) noted that social work research is like other professions and is a form of scientific enquiry that provides knowledge about the effectiveness of social work interventions.
As a profession, social work has experienced an uneasy history with research. In 1994, Lorenz noted that there were tensions and negative attitudes about the function research has in the social work profession. These setbacks were again highlighted by Orme and Powell (2007) who noted that qualifying social work students required little grounding in research methods. These setbacks continued outside of educational settings, with social workers having a history of failing to appropriately incorporate research into clinical practice when compared with other professions (Grady & Keenan, 2014).
Indeed, at various points in the history of social work research, there have been debates as to whether the social work profession is science-driven in an evidence-based research (EBR) culture (Rosen, 2003), more of an art using the principles of self (Graybeal, 2014) or a combination of the two (Hoffman & Weinberger, 2007). Social work students continue to struggle with research topics at university (Grady & Keenan, 2014) and may express negative reactions when research methods are discussed at the start of their studies (Bellamy et al., 2008).
There has been a steady progress, however. Social work is moving away from being an emergent research discipline (Sharland, 2011) in demonstrating advances in clinical and health settings (Rubin & Babbie, 2016).The Australian Association of Social Work (AASW, 2010) code of ethics strongly advocates for practice-led research that underpins values such as social justice. Terms of social work employment now have conditions where research and evidence-informed practices are a part of the job’s expectations (Finch et al., 2013). More recently, the number of social workers expressing an interest in doing research or gaining experience has been equal to that of other allied health professions (Taylor et al., 2019).
Barriers to Research Culture in Social Work
There are a number of barriers that can hamper research endeavors within health organization contexts (Luckson et al., 2018). For example, research and researchers can be seen as distant, mechanized, hard to understand, and driven by governmental forces (Grady & Keenan, 2014). Academic researchers have a history of being disconnected from social work clinicians, meaning research can be easily dismissed and considered irrelevant to clinical practice. This has led to many social workers having limited research exposure and experience (Goel et al., 2018). Other barriers are more operational, with many studies stating that there is not enough time for social workers to engage in practice-led research (Grady & Keenan, 2014; Pager et al., 2012) due to a high proportion of part-time staff, workforce shortages, and high staff turnover (Pager et al., 2012).
Other reasons appear clearer and include infrastructure problems such as access to working computers (K. E. Harding et al., 2014). In a health system with high caseloads and urgent priorities, social workers (and other allied health workers) find it difficult to justify doing research or attend research skills development training when there are patients who need urgent assessment and treatment (Pager et al., 2012; Proctor et al., 2007). The reactive perception that research is expensive (rather than the reality that good research leads to efficiency) means that cost is also a barrier to practitioner-led research (Nelson et al., 2006). Furthermore, there are systemic issues of scale, whereby social workers are often in smaller teams within agencies (Shaw & Norton, 2008). It should be noted, however, that within hospital settings, this issue is not exclusive to social work. Many social workers feel they are not equipped with the academic skills to conduct research (Harvey et al., 2013) or are disadvantaged by living in a rural region (Murphy & McDonald, 2004).
Social work research is not as bleak as this initial picture suggests, however. Social work practitioners hold positive beliefs toward the importance of research (Jaynes, 2014) and are keen to conduct research and complete research training (Goel et al., 2018). Social workers report that research is an opportunity to develop their own skill set, achieve career advancement, improve clinical services (R. J. Wenke et al., 2018) and that it increases job satisfaction (Pager et al., 2012). There has been a positive shift in management support to promote a research culture, especially in hospital and health settings (Ekeland et al., 2018). There is growing support within social work to develop research skills as it is a collaborative method of research (Drisko & Grady, 2015) that is amenable to social work values. As Orme and Powell (2007) noted, social work practitioners are in the unique position of being well placed to challenge existing practices and promote change. These values, beliefs, and ambitions are the building blocks needed to develop a strong research capacity.
Research Capacity Building (RCB)
The term “research capacity building” is used to describe circumstances where strategies are implemented to promote enhanced and sustainable practices (Hulcombe et al., 2014). Strong research capacity has positive outcomes such as reduced patient mortality, staff and patient satisfaction improvement, journal publications, conference presentations, and the securing of grant funding (K. Harding et al., 2017). In social work, research capacity is necessary to enable rigorous evidence and practice by development and evaluation of best practice and high-quality service provision (Orme & Powell, 2007). If there is a lack of research capacity in an organization, it can take many years for it to develop (Crisp et al., 2000).
The robust development of clinician research capacity has been associated with an overall positive work culture by social workers. The opportunity to research allows the development of many skill sets, increases job satisfaction, and helps address parts of the social work role perceived as problematic (Pager et al., 2012). Good clinician research capacity in health has been attributed to efficiency, better coherence with social work practice to the betterment of service users (Orme & Powell, 2007), and higher education opportunities (Cooke, 2005).
In this space, there are essentially three main types of research activities within hospital settings: original research, quality assurance, and continuous improvement. For the purposes of this study, original research essentially involves an investigation beyond standard care to test a hypothesis or theory. In comparison, quality assurance investigates or evaluates if these processes are working as they should be (National Health Service, 2016), and continuous improvement targets safety improvements and waste minimization (McFadden et al., 2015). Completing smaller projects such as continuous improvement or quality assurance with the support of an experienced researcher has been shown to increase practitioner confidence and improve the research culture in organizations (Beddoe, 2011).
In recent years, health settings (such as hospitals) have been employing dedicated research positions as a means of building research capacity and influencing research skills more broadly (R. Wenke & Mickan, 2016). Also termed a research lead (Whitworth et al., 2012), it is hoped that these positions become embedded in social work departments and have a positive influence on the research culture and existing practices at all levels (Orme & Powell, 2007). While this is a positive step forward, the research lead needs to be able to engage social workers to establish a link between practice and research (Epstein, 2009; Heinsch et al., 2015). Having a research lead can also help build an evidence base to improve clinical practice and research capacity (Williams et al., 2015).
Herein lies the importance of the research lead position in hospital settings. On one level, the position drives social work research and capacity (Misso et al., 2016), while at the same time contributing to the research capacity and culture for busy social work clinicians who have high caseloads, may work part-time, and who have varying degrees of research ability. The research lead has a small window with competing interests to educate and inspire staff while contributing to the research output. This must be achieved while the research leads integrate themselves into the health setting, ensure they are accessible, and provide support and guidance to clinicians’ individual levels of knowledge, skills, and abilities (R. J. Wenke et al., 2017).
Social Work at St. Vincent’s Hospital
St. Vincent’s Hospital in Melbourne (SVHM) is a large inner-city public hospital providing care for people from a wide range of cultures and backgrounds. Each social work practitioner has a research portfolio complementing their clinical commitments, and during the past few years, there has been a range of supports available. Research in the social work department is modeled through leadership at a management level and with the guidance of a social work research lead.
The aim of this study was to ascertain how effective the research lead role has been in helping hospital social work practitioners participate in research and quality studies given their busy workloads. The study asks the following questions: Has the introduction of a research program via the research lead increased practitioners’ confidence in doing research in the SVHM social work department? Which aspects of the research program were perceived as helpful or otherwise by the participants? What influences practitioners’ ability to engage in research/EBR in a public hospital social work department?
Method
The study was divided into three phases: an educational component, the development of quality and research projects, and online questionnaires.
Finch et al. (2013) noted the importance of a preintervention measure prior to implementing any research strategies to assist with the quantifying of the results. Therefore, a preintervention questionnaire was sent to staff via Survey Monkey to measure their confidence concerning core research skills prior to any educational sessions. The questionnaire asked about their ability to complete a literature review, formulate a research question, liaise with ethic committees, develop a methodology, write up a conclusion, and present findings or write-up for journal publication. The same questionnaire was completed as a postintervention measure at the completion of the brief educational program and after the mentoring.
Phase 1 of the study included an educational package designed to assist social work practitioners with the foundations of research. This included a monthly email (“The Research Blurb”) and a monthly oral presentation at each team meeting (e.g., the family violence team, the acute medical ward team) called “Ten Minute Tips.” The topics covered in both of these educational packages included how to formulate a research question, the foundations of a literature review, ethics applications, methodology and analysis, how to formulate relevant conclusions, and presentation skills.
Phase 2 of the study was the development of a quality assurance or research project with management support. Each social work clinician identified any gaps in their service provision and formulated a research question individually or as part of a small team. This led to the development of 12 individual or group research projects conducted by 30 social workers. Only one social worker was unable to participate due to the nature of their part-time employment and high clinical demand.
Finally, each social worker was invited via letter to complete two anonymous online questionnaires. The first questionnaire (pretraining) measured their perceived confidence and was completed in the second week of the research lead’s tenure and prior to the research training. The second questionnaire (posttraining) was completed toward the end of the calendar year and at the end of the educational intervention. The first questionnaire included six questions designed to measure the participants’ confidence in a range of research-related topics, while the second questionnaire included the same six questions as well as four qualitative questions regarding the barriers to and enablers of research, recommendations for future research support, and any further comments.
In between these two surveys, the participants were provided with a range of research training support, including regular mentoring, brief but structured education (Ten Minute Tips), and involvement in a research or quality assurance project. Participants were invited to rate the value of the Ten Minute Tips after each session.
It is important to note that this program was initially designed for a 10-month period; however, this was reduced to 7 months for two reasons. First, the increase in clinical demand meant that research/quality projects were delayed. Second, the research lead left the organization at the 8-month mark.
Results
A total of 30 participants were invited to complete the questionnaires and were assigned an anonymous name. Seventeen responded to the first questionnaire, while 12 responded to the second. This decrease was probably due to a loss of staff (four staff members resigned and two went on maternity leave) and an increase in clinical demand during the research period. Before they received any research training support, the participants’ mean overall confidence in doing research was 5.02 (range = 2–7.5) out of a possible 10. After receiving 7 months of support, this increased to 7.4 (range = 5–9). Confidence levels increased in all research areas, and there was an average increase in confidence of 19.5%. Figure 1 highlights improvements for confidence in research in general, formulating a research question, completing a literature review, developing a methodology, formulating a conclusion, and making a professional poster.
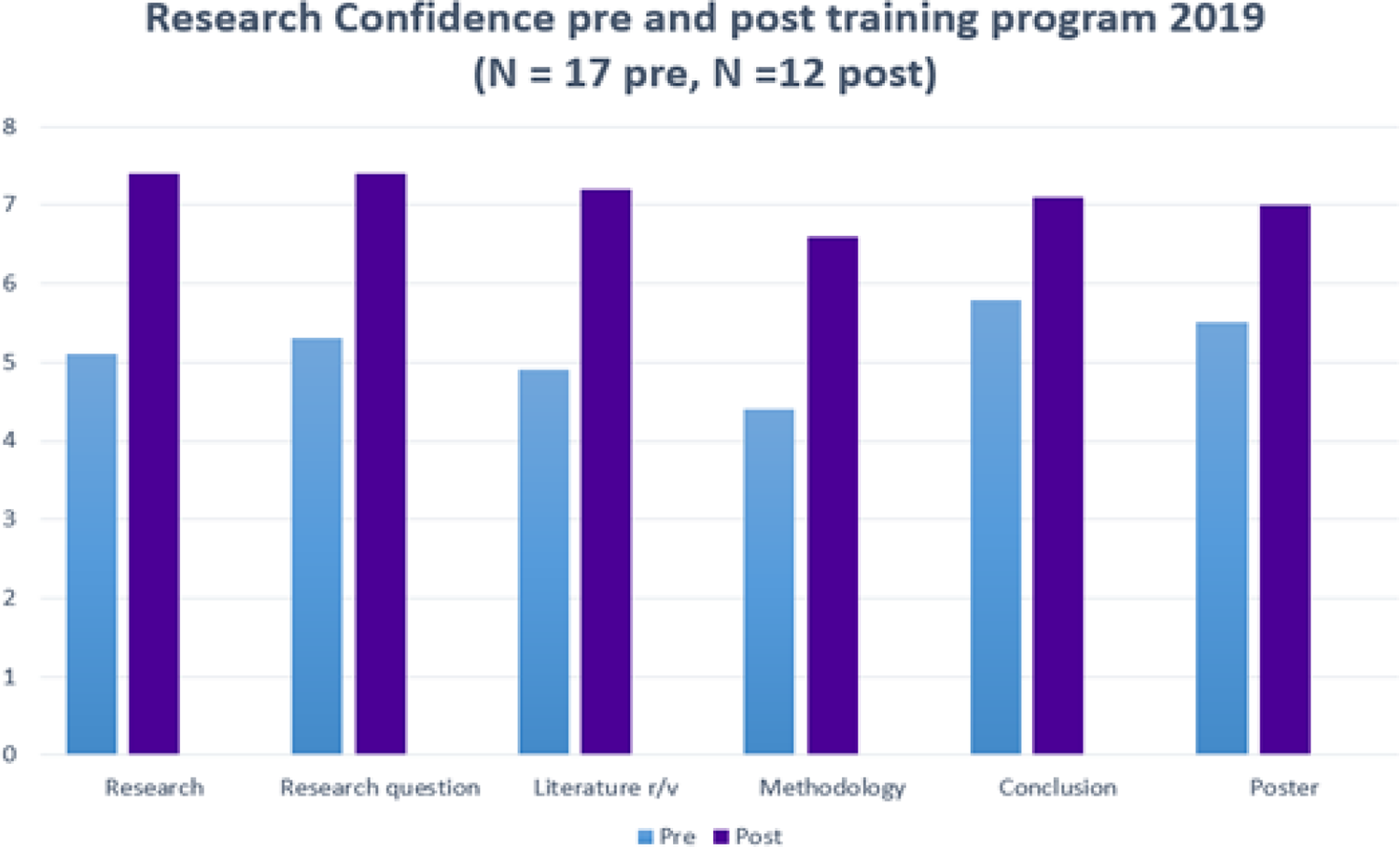
Pre- and postscores out of 10 for research confidence before and after training program.
The answers to the open questions in the second questionnaire were coded via thematic analysis. A total of seven participants responded to these questions, with four participants commenting on the training they hoped would be covered. Two participants reported that they were feeling nervous about doing research and felt inexperienced; however, one of these participants also added that they were excited. Another participant stated that they needed general research support, and two participants requested guidance and mentoring. Participant Suneet noted that: “Overall I am nervous about research due to limited experience. However, I am excited about (the) prospect of starting (a) project and exploring an area of interest. Will need guidance and support ++.” Twenty-two staff members were asked how helpful the training program presentations were and all of them reported that they were either “very helpful” (n = 17) or “helpful” (n = 5).
The posttraining survey included four open-ended questions. The first question examined the challenges participants had experienced while doing research. Respondents answered this question and their responses were coded into themes. Most of the respondents stated that they had experienced more than one challenge. Research had less priority than meeting clinical demand (8), and social workers were often too exhausted to focus on project work (1). Departmental and organization barriers included a lack of protected time where they were supported to complete research (3), lack of resources (2), and reduced staffing (6).
Amy summed up a number of themes: Significant short staffing resulting in clinical work taking priority and leaving no time for research. High levels of stress due to chronic short staffing resulting in burnout and a lack of passion about engaging in non-clinical tasks such as research.
Finally, respondents also emphasized the importance of being involved in research (n = 2), having some form of leadership (n = 2), being encouraged to do research (n = 2), and doing research with a partner (n = 1). A regular theme regarding what was helpful within all of these resources was mentoring (n = 9). Many different terms were used for this type of support, such as “check-ins” (Charlie), “helpful hints” (Olivia), and “discussions” (Cameron).
The third question examined any recommendations the participants had for facilitating research, and eight participants responded. All the respondents reported the idea of protected time (n = 8), but there was also a range of responses, for example, “Research is valued but a poor second when patients need discharging” (Taylor) and “Potentially introducing ‘protected’ QA time…where your pager buddy takes your pager and you have uninterrupted QA time” (Zoe).
Other themes again reiterated the shortage of staff (n = 2), that some quality assurance projects were assigned to them and they had little interest in them (n = 2), that there was little access to professional development to inspire research (n = 1), and that the process was made too complicated (n = 2). One respondent on this topic stated a number of barriers: “There is not enough time. You lose staff, you lose co-researchers, but the patients keep coming. Try not to over complicate the process either. There is a lot of confusing paperwork along the way” (Cameron).
As in the pretraining survey, participants were again offered the opportunity to add any extra comments. Two participants took this opportunity, with one reporting that it was exciting to see new research emanating from the department, and the other stating that the guidance of the research lead had been very helpful in increasing their low confidence.
The respondents consistently reported challenges such as having limited time due to clinical demands and having limited research experience, poor resources, and low levels of staff. If they had appropriate mentoring and education for their skill level, allocated time, and a relevant research topic, they would be likely to participant in research.
Discussion
It is interesting to note that this study experienced the same barriers many staff experience when participating in research and evidence-based practice (EBP). Although it was initially intended to take place over 10 months, with each staff member contributing to some form of research or EBP activity, a significant staff turnover and the loss of staff combined with high clinical demand meant that the participants (and at times the research lead) had to delay the research. This outcome mirrors the observations of Grady and Keenan (2014) and Pager et al. (2012), who noted that time and staff retention were continuous barriers to research in hospital settings.
This study did have some positive findings, however. By being flexible and innovative in the training process, the research lead can develop the skills of clinicians to help them engage more often in research and EBP. A number of research projects were started but not completed during the study period due to clinical demand and the research lead leaving the position. If research continues to have manager support, clinicians are more likely to engage in research and EBP in the future. Furthermore, this study provides a good basis for how research leads should operate in a busy hospital environment. Many staff expressed that they had engaged well with the research lead in a program that was perceived as helpful and that had been designed to be flexible and not overly complex. Having regular access to a research lead or a senior clinician helped drive their interest, motivation, and confidence in research, while the attempts of senior management to create a research culture were also initially beneficial.
Despite the well-received intervention and management support, the research lead is still vulnerable to competing demands and is particularly vulnerable to staff retention. In the future, it is worth considering how this may fit within organizations or practice settings that demonstrated similar characteristics to acute hospitals, namely, clinical areas involving high daily rate of clinical demands, potential for staff turnover, and variation and diversity in clinician knowledge and skill. Hospital social work is typically solution- or task-oriented, regarding psychosocial issues that social workers are driven to understand and resolve. Approaching research with a simplified task mindset focused on an issue or problem that will sustain interest and passion as a core need. The support that participants cited as most helpful was often simple and immediately available, such as 10-min tips and a weekly newsletter that could be read at leisure. Adapting academic research knowledge into easily digestible units that have relevance and applicability with the service context would enhance research program design.
A limitation is that this article was unable to use outcomes as an indicator of quality. Several projects were initiated but subsequently fell by the wayside. This is again a reflection of fluctuations in staffing and clinical demands. One solution may be to integrate key performance indicators (KPI) for individuals or departments regarding research outputs such as conference attendance, oral and poster presentations, publications in scholarly journals, and grant funding applications. KPI should carry incentives that are attractive for clinicians, managers, and the organization as a whole, hopefully facilitating support for increased resources and protected time. Furthermore, it would be interesting to track research outputs in relation to core themes and topics prevalent in the hospital context to identify saturation of inquiry, and the potential for missed populations or interventions that would benefit from research activity.
In summary, the respondents noted ongoing challenges that have been noted elsewhere, such as having limited time due to clinical demands, limited research experience, poor resources, and low levels of staff. However, the results from this study highlight how a hospital research lead translated and integrated the research processes into the clinical setting. Ensuring that education is focused, harnesses clinical passion and relevance to practice, and involves minimal procedural burden eases clinician anxiety regarding research involvement. The presence of research leads has the potential to augment research culture and capability with the support of culture set by leadership.
Footnotes
Acknowledgments
The author would like to thank the St. Vincent’s Hospital Melbourne, Social Work Department leadership team (Lisa Braddy and Penny Lording) and clinicians, and Eastern Health Melbourne for their assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.