
Abstract
Purpose:
A meta-analysis of group interventions to reduce post-traumatic stress symptoms (PTSS) and/or depression among refugee and immigrant children and adolescents.
Methods:
A systematic search was followed by independent reviews of each study for risk of bias. The meta-analysis pooled between- and within-condition effect sizes on PTSS and depression across studies using a random effects model.
Results:
The search yielded 16 studies utilizing eight interventions involving 976 participants. For all studies, within conditions, there were good effects on PTSS (d = −0.66, 95% CI [−0.86, −0.46]) and depression (d = −0.51, 95% CI [−0.79, −0.23]) with substantial heterogeneity. For studies with control groups, the between-group effect sizes yielded a small effect on PTSS (d = −0.31, 95% CI [−0.65, 0.03]) with no significant effect on depression.
Conclusions:
The interventions helped to reduce PTSS and depression. Most studies lacked rigorous designs and provided little information on group variables needed for replication.
Every day, 37,000 people leave their home countries in search of security and stability (United Nations High Commissioner for Refugees [UNHCR], 2019). The number of forced displacements across the world is at its highest rate (nearly 71 million) and children below the age of 18 make up more than half of this population, a rate that has been rising (UNHCR, 2019).
Forced migration has a profound impact on the health and well-being of families (Naseh, Macgowan, et al., 2019; Naseh, Wagner, et al., 2019). Displaced children face unique challenges that intensify the negative impacts of the trauma experienced before and after migration (Nocon et al., 2017; Potocky & Naseh, 2019; Yakushko et al., 2008). The immigration process disconnects parents and children from their usual support system of friends and family who are not available to help with childcare and support while having to manage issues related to migration (Bryant et al., 2018; Stewart et al., 2015). Forced migration brings higher mental health challenges among refugee and immigrant children when compared with children in host populations (Barghadouch et al., 2018; Close et al., 2016; Fazel et al., 2005; Jakobsen et al., 2014).
The rates of challenges are affected by factors that include the type of trauma experienced, family income, the migration experience from the country of the origin to the host country, and the reception in the host country (Fazel, 2018). Huemer et al. (2009) found that unaccompanied refugee minors have a significantly higher prevalence of depressive disorder (47% vs. 27%), borderline disorder (22% vs. 9%), and psychosis (15% vs. 1%), when compared with refugee minors with families. Fazel et al. (2015) reported that PTSD rates among refugee children resettled in high-income countries were between 10% and 25% but up to 75% among minors in low- and middle-income countries (Fazel et al., 2015).
The heterogeneity of the population and range of mental health issues have resulted in the design and development of a variety of interventions. These interventions differ in their target populations (i.e., refugees with families, unaccompanied minor refugees, immigrants, and undocumented immigrants), setting (urban areas or refugee settlements), primary outcomes, intensity of the mental health problems, level of exposure to trauma, and intensity, level, and comprehensiveness of provided services. These issues make it difficult to review and classify the psychological and psychosocial interventions for children affected by forced displacement. Several systematic reviews have focused on either one subgroup of refugee and immigrant children or one setting of service provision (Demazure et al., 2018; Nocon et al., 2017; Pfefferbaum et al., 2019). For example, Demazure et al. (2018) completed a scoping review of 17 psychosocial interventions with unaccompanied minor refugees but could not reach a conclusion on the efficacy of the reviewed intervention due to methodological flaws and the heterogeneity of the interventions. In a meta-analysis, Nocon et al. (2017) reviewed 23 studies that evaluated the effectiveness of psychosocial interventions on war-traumatized children and reported that cognitive behavioral–based interventions were promising. Pfefferbaum and colleagues’ (2019) meta-analysis of 21 studies investigated the effectiveness of interventions on depression and anxiety in youth exposed to political violence or natural disasters but did not find significant combined effect on any of the outcomes.
Group work is an effective modality with adolescents and young adults (Burlingame & Jensen, 2017; Rosner et al., 2010; Ssegonja et al., 2019; Wethington et al., 2008), including immigrant and refugee adult populations (Sakamoto & Couto, 2017). The most common group works with refugee and immigrant adults include education and psychoeducational groups, support groups, and trauma-informed groups (Sakamoto & Couto, 2017). Empirically tested effective group interventions include eye movement desensitization and reprocessing therapy (Lehnung et al., 2017; Yurtsever et al., 2018), group cognitive behavioral therapy (Hinton et al., 2012; Kananian et al., 2020; Shaw et al., 2019), trauma-focused group therapy (Drožđek & Bolwerk, 2010), and group art therapy (Dieterich-Hartwell & Koch, 2017). A meta-analysis found that both individual and group interventions on PTSD, depression, and anxiety among immigrant and refugee populations were efficacious with no significant difference between the modalities (Turrini et al., 2019). Group interventions, especially school-based, are increasingly being used with immigrant and refugee adolescents. However, there is no systematic review that critically examines the effectiveness of group interventions among refugee and immigrant children and adolescents. This study is a systematic review and meta-analysis of the efficacy of psychosocial group interventions to reduce psychological harm for refugee and immigrant children.
Method
Inclusion and Exclusion Criteria
To identify psychosocial group interventions for the affected population, a broad set of inclusion criteria was chosen. The population includes individuals who experienced international migration under the age of 18, which include refugees, asylum seekers, and undocumented and documented immigrants. Studies needed to include psychosocial group-based interventions without accompanying pharmacological interventions. Any randomized or nonrandomized quantitative design was included. The primary outcome was post-traumatic stress symptoms (PTSS) and the secondary outcome was depression. Although studies could be in any country, the study had to be in English and published in a peer-reviewed journal. Excluded from the search were children who did not move across borders (i.e., internally displaced children) and qualitative studies. The review followed the 2020 preferred reporting items for systematic reviews and meta-analyses statement (Page et al., 2021), although the review protocol was not registered.
Literature Search
A search of PsycINFO, Applied Social Sciences Index and Abstracts, Published International Literature on Traumatic Stress, Medline, Social Service Abstracts, and Social Work Abstracts was conducted by both authors in April 2020. Keywords were chosen relevant to population (refugee, immigrant, undocumented children), problem (PTSS and depression), and intervention (to exclude nonintervention studies). The main keywords searched separately and in various combinations included migrant, refugee, DACA, dreamer, alien, displaced, undocumented, illegal, unauthorized, asylum, foreign-born, irregular, child, youth, adolescent, teen, minor, intervention, treatment, therapy, practice, program, strategy, trauma, and post-traumatic stress. Additionally, bibliographies of other systematic reviews and meta-analyses were reviewed (i.e., Demazure et al., 2018; Nocon et al., 2017; Sullivan & Simonson, 2016). All identified studies were examined by title and abstract using Covidence (2019) online software program based on the inclusion criteria to eliminate irrelevant studies. Full-text versions of relevant articles were examined by both authors to determine final inclusion for data extraction.
Analytic Strategy
The authors used a systematic process to determine risk of bias and to extract data for the meta-analysis. For the risk of bias, the authors independently assessed each article and then met to compare results to resolve discrepancies through discussion. For the data extraction, the authors used the population, intervention, control, outcome framework (Schardt et al., 2007). One author extracted the sample characteristics, intervention variables, methodological variables, and outcome variables from each article, which the second author verified. The reviewers contacted study authors for additional data where necessary. In a few cases, where the publication was missing summary statistics (e.g., standard deviations), the authors used other information in the study to calculate the needed variable for the meta-analysis. For example, a standard deviation was calculated based on provided standard error and sample size.
Risk of bias
As both randomized controlled trials (RCTs) and nonrandomized studies were eligible, two different tools were used to check the quality of studies, appropriate for the respective design. RCTs were assessed using the Cochrane Risk of Bias Assessment Tool (Sterne et al., 2019), assigning “low,” “some concerns,” or “high” bias risk. The Risk of Bias in Nonrandomized Studies—of Interventions (ROBINS-I) tool (Sterne et al., 2016) assessed the bias risk for nonrandomized trials, assigning “no information,” “low,” “moderate,” “serious,” or “critical” risk of bias. A limitation of the ROBINS-I tool is that it is designed for studies with multiple groups (conditions) and not for assessing the risk of bias in single-condition designs. For example, one of the domains (“classification of interventions”) assumes multiple conditions in the study being reviewed, which is not useful for single-condition designs. Given it is the recommended tool for nonrandomized studies (Sterne et al., 2016), the authors used and adapted it for single-condition studies, as other researchers have done (Dhiman et al., 2020; Goldstein et al., 2019). Specifically, the authors refrained from making a judgement on the “classification of interventions” when the study used a single-condition design. In addition, the bias of “confounding” was interpreted as referring to factors that may confound the findings in a single-condition study.
Two independent reviewers conducted the assessment and compared results to resolve discrepancies through discussion. To interpret the level of interrater reliability, Cohen’s κ statistic, the following guideline was used: none (0 to .2), minimal (.21 to .39), weak (.40 to .59), moderate (.60 to .79), strong (.80 to .90) and almost perfect (.91 to 1) (McHugh, 2012).
Statistical methods
For controlled trials, between-group Cohen’s d (1988) effect sizes (standardized mean differences) were calculated using pooled standard deviations (Faraone, 2008). As few of the studies included follow-ups, combined effect sizes were calculated using pre- and post-test data. Pre–post (within-group) effect sizes for outcomes were computed for all studies, and raw scores were used to calculate standardized mean changes (Morris & DeShon, 2002). Data were extracted from the studies, and the effect sizes were calculated using the Psychometrica online calculator (Lenhard & Lenhard, 2016).
Meta-essentials (Suurmond et al., 2017) was used to conduct the meta-analysis for examining overall effect sizes of the group interventions on PTSS and depression, both for between-group effect sizes and within-group effect sizes. To account for pretreatment differences between groups across studies, the meta-analysis was based on change from baseline scores. For within-group effect sizes, imputed correlation coefficients of .50 were used (Diehle et al., 2014).
A random effects model was used for data synthesis because of the expected diversity among the studies in sample size, population, age range, intervention, and settings (Borenstein, 2009). Several statistics were used to assess observed heterogeneity across the studies, including I2, Q, and tau (τ) (Borenstein, 2009; Borenstein et al., 2017). In particular, the variation in effect sizes across the studies was assessed using the I2 statistic that measures the extent of heterogeneity. When observed I2 was larger than 50%, the heterogeneity was interpreted as substantial (Higgins et al., 2019) and subgroup analyses were performed. In addition, τ and prediction intervals are reported, which are measures of dispersion of true effect sizes between studies in terms of the scale of the effect size (Borenstein et al., 2017).
Subgroup analyses were completed for within-condition effect sizes based on a priori factors from the literature that could potentially moderate the intervention effect (Bonanno et al., 2010; Brown et al., 2017; Fazel, 2018; Newman et al., 2014; Pfefferbaum et al., 2014, 2019), and if data were available across all studies. The factors can be grouped into three major categories: population, intervention context, and intervention. The factors under population include residence (i.e., group living facilities, settlement camps, and residential settings), children accompanied or unaccompanied by their families, migration classification (i.e., refugee and immigrant), and age (i.e., 6–10, 11–14, and 15–18). Intervention context includes setting (i.e., school-based, and nonschool-based) and host country economic classification (i.e., high income and not high income; The World Bank, 2019). The intervention category includes type of intervention (i.e., cognitive behavioral therapy [CBT] and non-CBT), number of sessions (i.e., less than five sessions, five to seven sessions, eight to 10 sessions, and more than 10 sessions), length of intervention (i.e., less than 5 weeks, 5–7 weeks, 8–10 weeks, and more than 10 weeks), and interventionist’s qualification (i.e., mental health professionals and trained lay persons). For within-group effect sizes, publication bias was assessed by examining the funnel plot with a trim-and-fill analysis (Shi & Lin, 2019) and the Egger’s regression test (Egger et al., 1997). For between-group effect sizes and subgroup analyses, conducting a publication bias test was not possible due to small number of studies (<10; Higgins et al., 2019). In all analyses, p values less than .05 were considered significant.
Results
As indicated in Figure 1, the search yielded 1,513 articles with 505 excluded as duplications. In the title and abstract review stage, an additional 834 studies were excluded as not relevant. Out of 174 articles remained for full-text screening, 156 studies were excluded for not being an empirical intervention study (n = 82), wrong target population (n = 32), not written in English (n = 11), wrong outcomes (n = 11), wrong study design (n = 8), or not including group work (n = 14). At this stage, one additional study was excluded for duplication. In the end, 16 studies remained for review and data extraction.
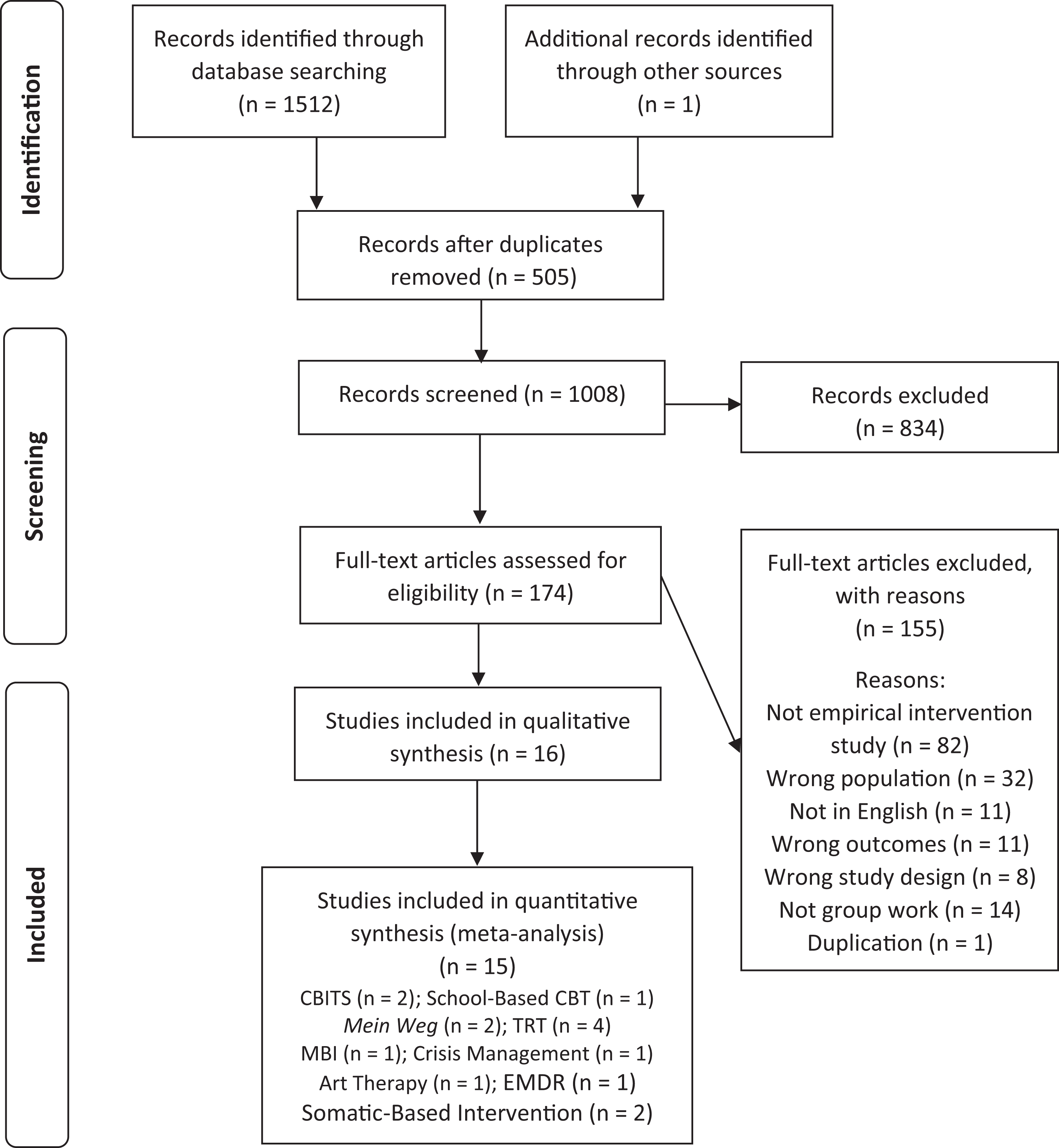
Preferred reporting items for systematic reviews and meta-analyses flow chart of the study selection process. Note. CBITS = cognitive behavioral intervention for trauma in schools; CBT = cognitive behavioral therapy; EMDR = eye movement desensitization and reprocessing; MBI = mindfulness-based intervention; TRT = teaching recovery technique.
The 16 studies were published from 2003 to 2019. As indicated in Table 1, participants included refugee, immigrant, and asylum-seeking children between the ages of 6 and 18 with diverse psychopathological concerns, including PTSS and depression. Overall, 976 participated (316 females, 644 males) with sample sizes ranging from 13 (Van der Gucht et al., 2019) to 229 (Kataoka et al., 2003).
Characteristics of the Samples Across Studies.
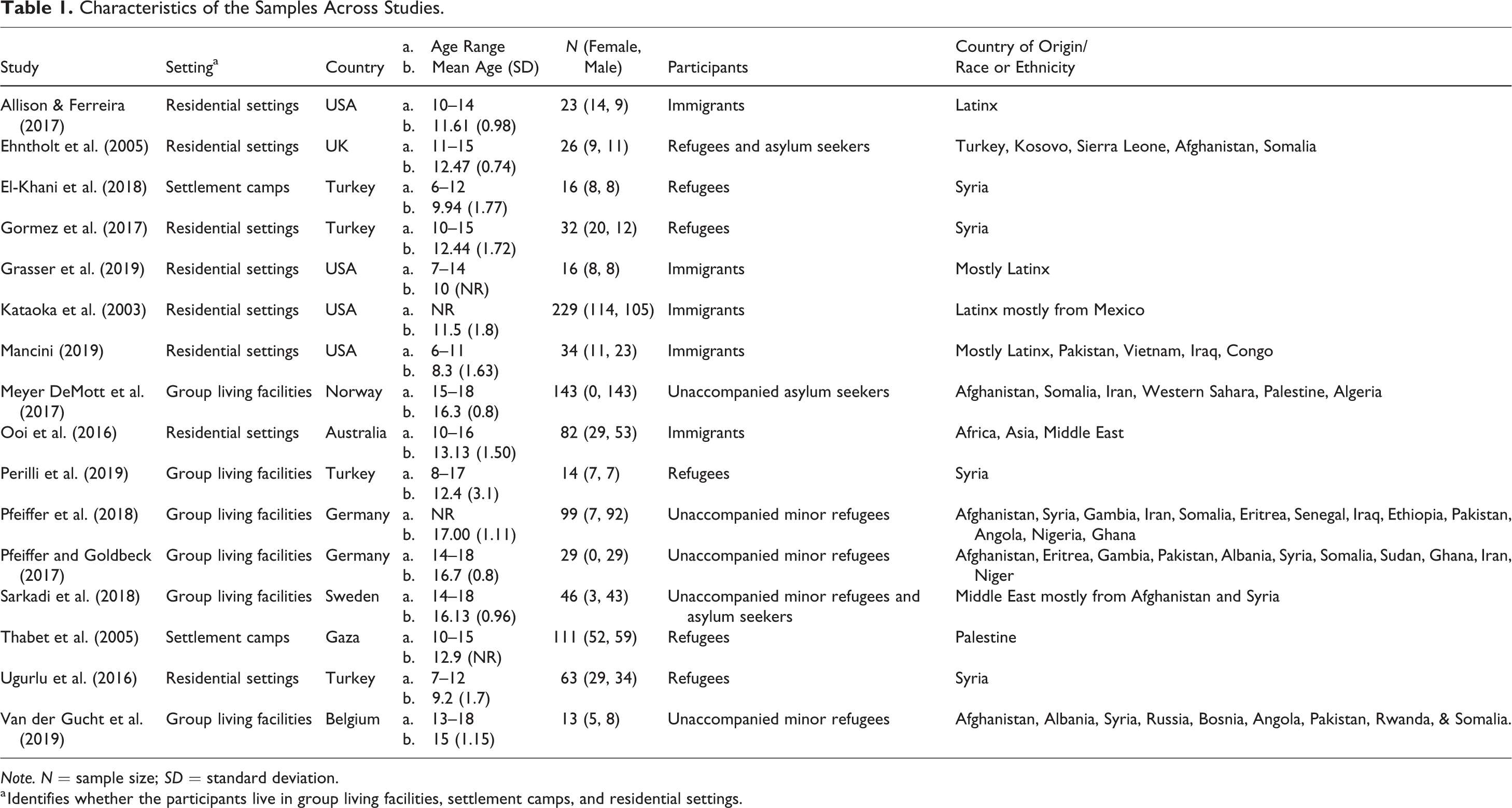
Note. N = sample size; SD = standard deviation.
a Identifies whether the participants live in group living facilities, settlement camps, and residential settings.
Six hundred and forty-six lived with their families and three hundred and thirty were unaccompanied (Table 1). All participants resettled in the host countries within 5 years of their arrival. With respect to setting, 127 children were in settlement camps, 344 in group living facilities, and 505 were in other residential settings. Participants were from all over the world with the majority from Latin America, Syria, Afghanistan, and Africa. The host countries were equally diverse (Table 1).
Characteristics of the interventions and methodological variables are in Table 2. Most (n = 9) interventions were delivered in school settings. Interventions ranged from three to 15 sessions that were from 35 to 90 min in duration. In most (n = 9) studies, interventions were provided by mental health professionals. For studies that reported information about leadership and group composition, most groups were facilitated by a single leader in groups sizes that ranged from 2 to 31.
Methodological and Intervention Characteristics of the Studies.
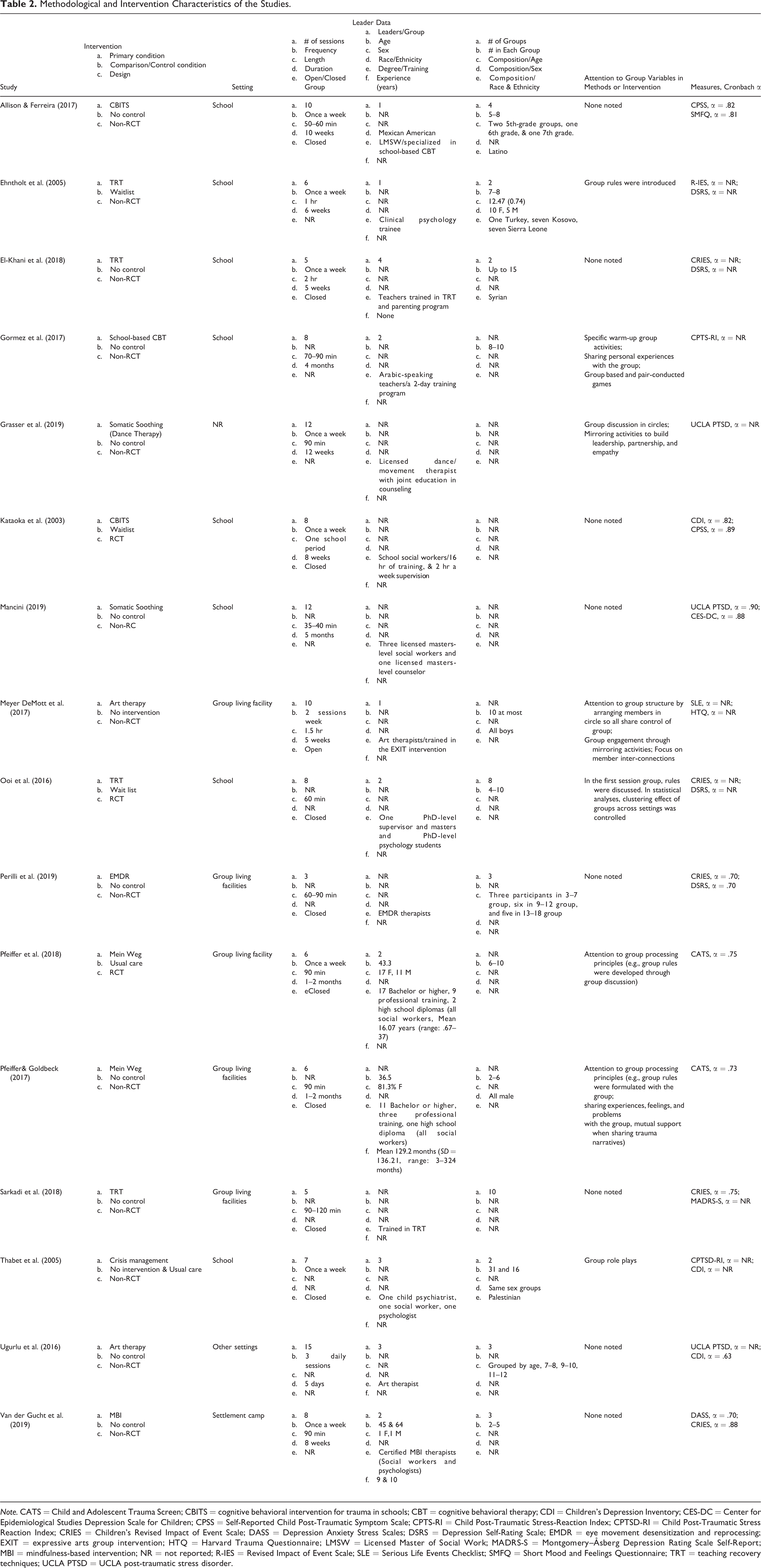
Note. CATS = Child and Adolescent Trauma Screen; CBITS = cognitive behavioral intervention for trauma in schools; CBT = cognitive behavioral therapy; CDI = Children’s Depression Inventory; CES-DC = Center for Epidemiological Studies Depression Scale for Children; CPSS = Self-Reported Child Post-Traumatic Symptom Scale; CPTS-RI = Child Post-Traumatic Stress-Reaction Index; CPTSD-RI = Child Post-Traumatic Stress Reaction Index; CRIES = Children’s Revised Impact of Event Scale; DASS = Depression Anxiety Stress Scales; DSRS = Depression Self-Rating Scale; EMDR = eye movement desensitization and reprocessing; EXIT = expressive arts group intervention; HTQ = Harvard Trauma Questionnaire; LMSW = Licensed Master of Social Work; MADRS-S = Montgomery–Åsberg Depression Rating Scale Self-Report; MBI = mindfulness-based intervention; NR = not reported; R-IES = Revised Impact of Event Scale; SLE = Serious Life Events Checklist; SMFQ = Short Mood and Feelings Questionnaire; TRT = teaching recovery techniques; UCLA PTSD = UCLA post-traumatic stress disorder.
With respect to study design, all but three studies were nonrandomized. Specifically, 11 studies were single-condition pre–post studies (Allison & Ferreira, 2017; El-Khani et al., 2018; Gormez et al., 2017; Grasser et al., 2019; Mancini, 2019; Perilli et al., 2019; Pfeiffer & Goldbeck, 2017; Sarkadi et al., 2018; Ugurlu et al., 2016; Van der Gucht et al., 2019), three used nonrandomized comparison conditions (Ehntholt et al., 2005; Meyer DeMott et al., 2017; Thabet et al., 2005), and three used a randomized controlled design (Kataoka et al., 2003; Ooi et al., 2016; Pfeiffer et al., 2018). All studies used valid and reliable measures to assess the intervention effect on the outcomes. As seen in Table 2, the most widely used PTSS measure was Children’s Revised Impact of Event Scale (CRIES; Perrin et al., 2005) used by five studies and the most widely used depression measure was Depression Self-Rating Scale (DSRS; Birleson, 1981) used by four studies.
Overview of Interventions
Just over half (n = 9) of the studies included interventions based on cognitive behavior therapy, with the others based on art therapy, mindfulness, crisis management, eye movement desensitization and reprocessing (EMDR), and two types of somatic soothing and emotional regulation. The overview of the included interventions is as follows. More details are included in Table 2.
Cognitive behavioral intervention for trauma in schools (CBITS)
Two studies (Allison & Ferreira, 2017; Kataoka et al., 2003) used CBITS which is a school-based, group intervention, designed to reduce symptoms of behavioral problems including PTSD and depression. The program (Kataoka et al., 2003) included cognitive-behavioral techniques, such as education about reactions to trauma, relaxation training, cognitive restructuring, social problem solving, and exposure. Allison and Ferreira (2017) later utilized the same CBITS model in their study.
School-based CBT
Gormez et al. (2017) developed an eight-session CBT-based group program specifically designed to be delivered by teachers in schools (Gormez et al., 2017). The intervention focused on trauma- and grief-related experiences. Relaxation techniques, psychoeducation, problem-solving strategies, creating alternative explanation, for relapse management, and constructing a trauma narrative were also embedded in the program.
Mein Weg (My way)
Two studies (Pfeiffer et al., 2018; Pfeiffer & Goldbeck, 2017) tested the impact of Mein Weg, a trauma-focused CBT intervention for unaccompanied minor refugees in Germany. The group intervention included psychoeducation and relaxation, trauma narrative, and cognitive restructuring, enhancing safety and future development. The intervention integrated trauma-focused CBT into group-processing principles, such as sharing experiences, feelings, and problems with the group and showing mutual support for one another when sharing the trauma narratives.
Teaching recovery techniques (TRT)
Four studies (Ehntholt et al., 2005; El-Khani et al., 2018; Ooi et al., 2016; Sarkadi et al., 2018) tested the effects of a manualized CBT-based group program, Children and War: Teaching Recovery Techniques, to “educate children about the symptoms of PTSD and to teach them appropriate coping strategies” (Ehntholt et al., 2005, p. 237). TRT included dual-attention techniques, breathing exercises, progressive muscle relaxation, coping self-statements, graded exposure, processing of wartime experiences, and attention to sleep hygiene and pleasurable activities.
Mindfulness-based intervention (MBI)
MBI involves extensive training in mindfulness meditation skills, and mindfulness meditation practice is employed as a central foundational methodology. Van der Gucht et al. (2019) conducted an eight-session MBI group intervention for children aged 13–18 in Belgium. The intervention includes breathing, eating, pause, and grounding exercise, monkey
Crisis management
Thabet et al. (2005) developed a crisis management group model for children exposed to political conflict trauma, which was based on critical incident stress management (Everly et al., 2002). The intervention included free drawing, talking about their traumatic experiences and feelings, writing about traumatic events, storytelling, games, and role-play related to the conflict.
Art therapy
Two studies (Meyer DeMott et al., 2017; Ugurlu et al., 2016) provided art therapy. Ugurlu et al. (2016) adapted elements of skills for psychological recovery (Berkowitz et al., 2010) that was designed for populations experiencing disaster. The program included building problem-solving skills, promoting positive activities, identifying feelings, handing difficult feelings and managing reactions, promoting helpful thinking, and rebuilding healthy social connections.
Meyer Demott et al. (2017) studied the effectiveness of an expressive arts group intervention (EXIT) on unaccompanied minor asylum-seeking adolescents in Norway. The main elements of EXIT include connecting and engagement, calming and imagining a “safe place,” efficacy, identity, and hope, and finding inner “resource animal,” its movements and sounds.
EMDR
Perilli et al. (2019) used the EMDR Integrative Group Treatment Protocol (EMDR-IGTP; Jarero et al., 2006), which combined the eight phases of EMDR with a group art therapy model that used “butterfly hug” self-administered bilateral stimulation (Artigas & Jarero, 2014).
Somatic-based interventions
Two studies used somatic-based interventions. Grasser et al. (2019, p. 1124) provided a manualized, multimodal, somatic-based intervention called dance/movement therapy, aimed at “strengthening emotional, cognitive, physical, and social integration.” They used different techniques including breathing, stretching, tension release exercises, mirroring, group discussion, movement-based coping mechanisms, and movement games.
Mancini (2019) assessed effectiveness of the other somatic-based intervention, Somatic Soothing and Emotional Regulation Skill Development (SSERSD) intervention. SSERSD is a school-based, trauma-informed group intervention, rooted in mindfulness and yoga. The intervention included relaxation and movement strategies, creating space and boundaries, body and somatic resources, grounding resources, releasing activities, and somatic resource movements.
Group-Related Factors
A concern about group-based intervention research is the underreporting of group variables and inattention to examine how such variables affect processes and outcomes. These problems affect the ability to replicate the interventions and to understand the effects of the variables that research has shown to affect group processes and outcomes (Burlingame et al., 2004, 2013; Miles & Paquin, 2014). Given the effects of group processes on outcomes, researchers have utilized reliable and valid measures of group structures and processes (e.g., cohesion), which can inform how such groups should be constructed and maintained advancing an understanding of group-level mechanisms of change (Burlingame et al., 2013). The concerns about the lack of documentation of the nature of the groups is important as more details allow for accurate replication, validity, and illumination of putative-mediating factors related to outcomes.
A few studies provided information about the groups and attended to group-relevant factors, either in the intervention delivery or in statistical methods. As seen in Table 2, some authors included descriptive information about group sizes, composition, and leader variables, which help for replication. Most (n = 8) provided no information about how group factors were brought into the groups, so the nature of the groups was unclear. The studies about Mein Weg (Pfeiffer & Goldbeck, 2017; Pfeiffer et al., 2018) provided the most information. The authors shared information suggesting explicit attention to group processing principles. For example, group rules were introduced and written for the whole intervention group discussion. Group processing principles included sharing experiences, feelings, and problems with the group during psychoeducation, relaxation, cognitive restructuring, and mutual support for one another when sharing trauma narratives. None of the studies used measures of group process, such as cohesion, which could help interpret findings.
Risk of Bias
The authors assessed the studies’ risk of bias using the Cochrane Risk of Bias Assessment Tool (RoB2; Sterne et al., 2019) for RCTs and the ROBINS-I (Sterne et al., 2016) for non-RCTs and single-condition studies. The Cohen’s κ interrater reliability of the ratings was 0.81 (p < .05), indicating strong interrater agreement (McHugh, 2012).
As seen in Table 3, all but one RCT had an overall high risk of bias. Pfeiffer et al. (2018) had an overall rating of “some concerns” due to the rating in one domain (Selection of the reported result), but otherwise had low risk of bias. Missing outcome data had a low risk of bias and selection of the reported results showed concerns. As for deviation from intended intervention, only one study (Pfeiffer et al., 2018) showed minimal risk and the other two (Kataoka et al., 2003; Ooi et al., 2016) showed some concerns. Measurement of outcome was rated as high risk of bias for two (Kataoka et al., 2003; Ooi et al., 2016) and low for one (Pfeiffer et al., 2018). Kataoka et al. (2003) did not describe the method of random sequence generation and was considered as showing high risk of bias.
Risk of Bias for Randomized Controlled Trials.
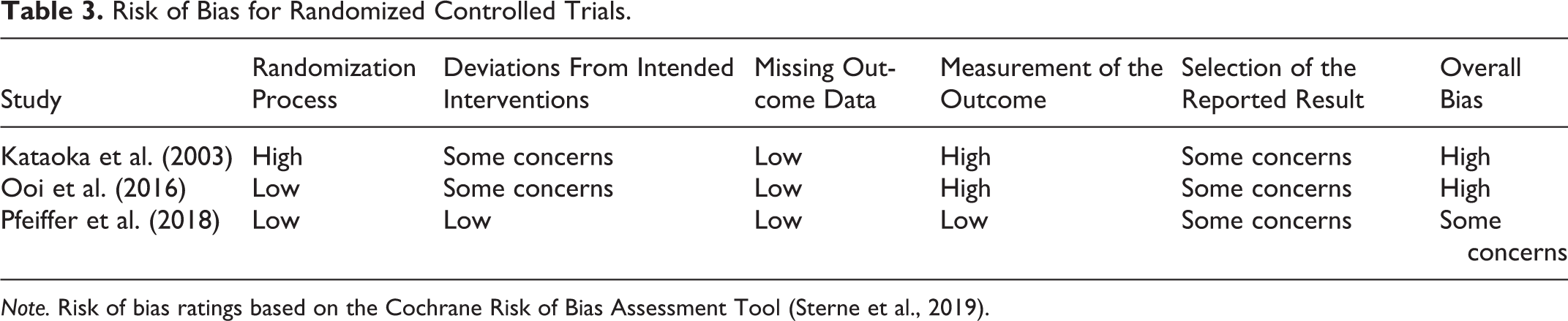
Note. Risk of bias ratings based on the Cochrane Risk of Bias Assessment Tool (Sterne et al., 2019).
For nonrandomized studies (Table 4), the studies were divided based on design (i.e., non-RCTs and single-condition pre- to post-test studies). All non-RCTs were classified as having a serious to critical risk of bias. In general, the most problematic domains were bias due to confounding variables and bias in measurement of the outcomes. Three studies had better ratings but still had serious overall risk of bias (Gormez et al., 2017; Meyer DeMott et al., 2017; Pfeiffer & Goldbeck, 2017).
Risk of Bias in Non-Randomized Studies of Intervention.
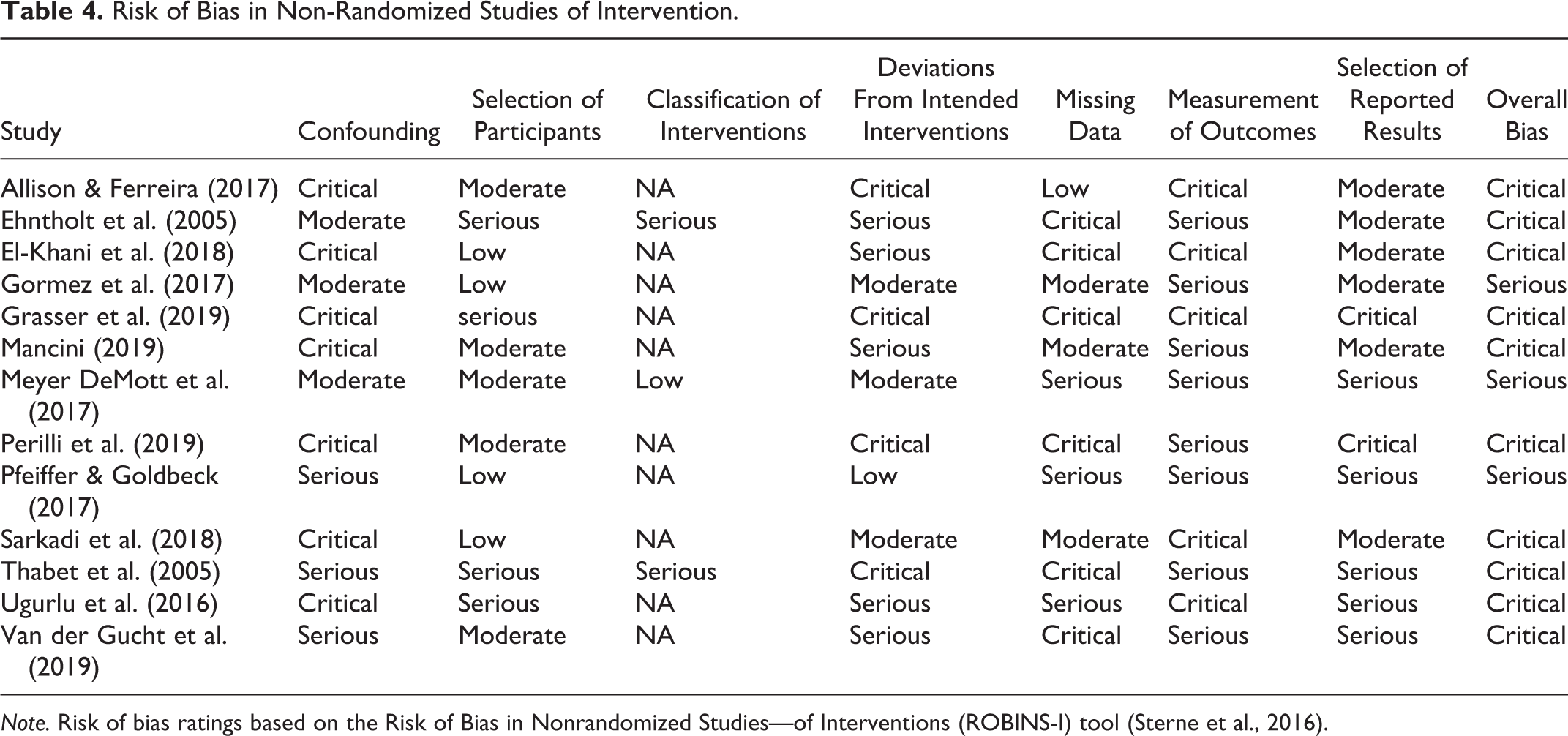
Note. Risk of bias ratings based on the Risk of Bias in Nonrandomized Studies—of Interventions (ROBINS-I) tool (Sterne et al., 2016).
Within-Condition Effects
PTSS
One study (Meyer DeMott et al., 2017) did not provide the required data for a meta-analysis and thus 15 studies were included in the meta-analysis of PTSS. The combined pre–post effect size for PTSS was statistically significant in the random effects model, d = −0.66, 95% CI [−0.86, −0.46], p < .001 (Figure 2). The heterogeneity among effect sizes was substantial and statistically significant (I2 = 65.11%, τ = .26, Q = 40.13, p < .001), suggesting that the variability across studies was due to heterogeneity rather than chance.To explore this further, subgroup analyses were completed on variables related to context of the intervention, intervention characteristics, and population, which the literature suggested may moderate the intervention effects.
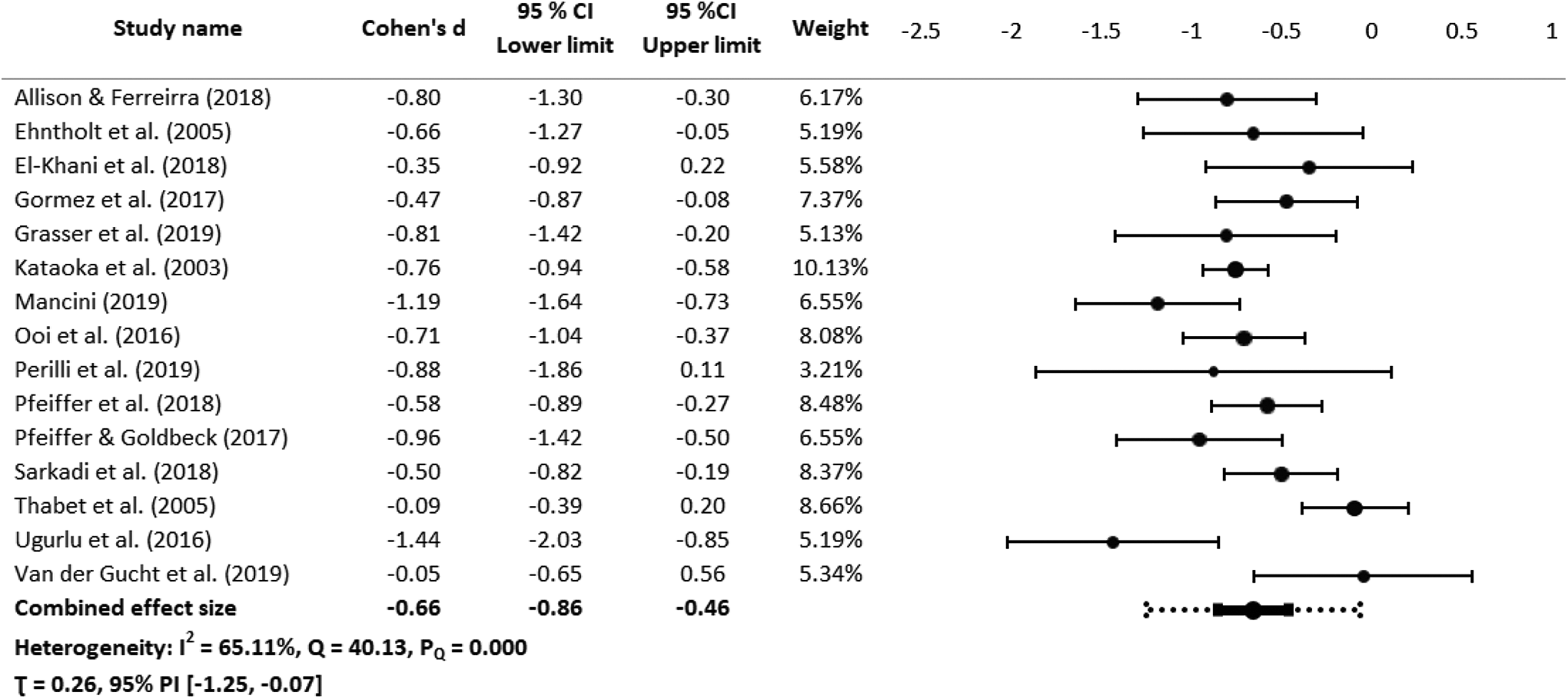
Forest plot of within-conditions effect sizes for post-traumatic stress symptoms. Note. CI = confidence interval; PI = prediction interval. Random effects model was used. The Forest plot for the combined effect size shows both confidence interval (solid black) and prediction interval (dash black).
The first test was to examine each subgroup to determine if there were significant differences between the variables within each subgroup. As seen in Table 5, the intervention effect was statistically significant based on number of sessions and residence setting. There were larger effects for PTSS with interventions delivered for children living in residential settings (d = −0.81, 95% CI [−1.10, −0.62]), those delivered in more than 10 sessions (d = −1.15, 95% CI [−1.49, −0.82]). There was no significant difference among other subgroups. A funnel plot using trim-and-fill analysis and Egger’s regression test (t = −0.46, p =.651) did not provide evidence of a publication bias.
Subgroup Pre-Test to Post-Test Effect Sizes and Heterogeneity.
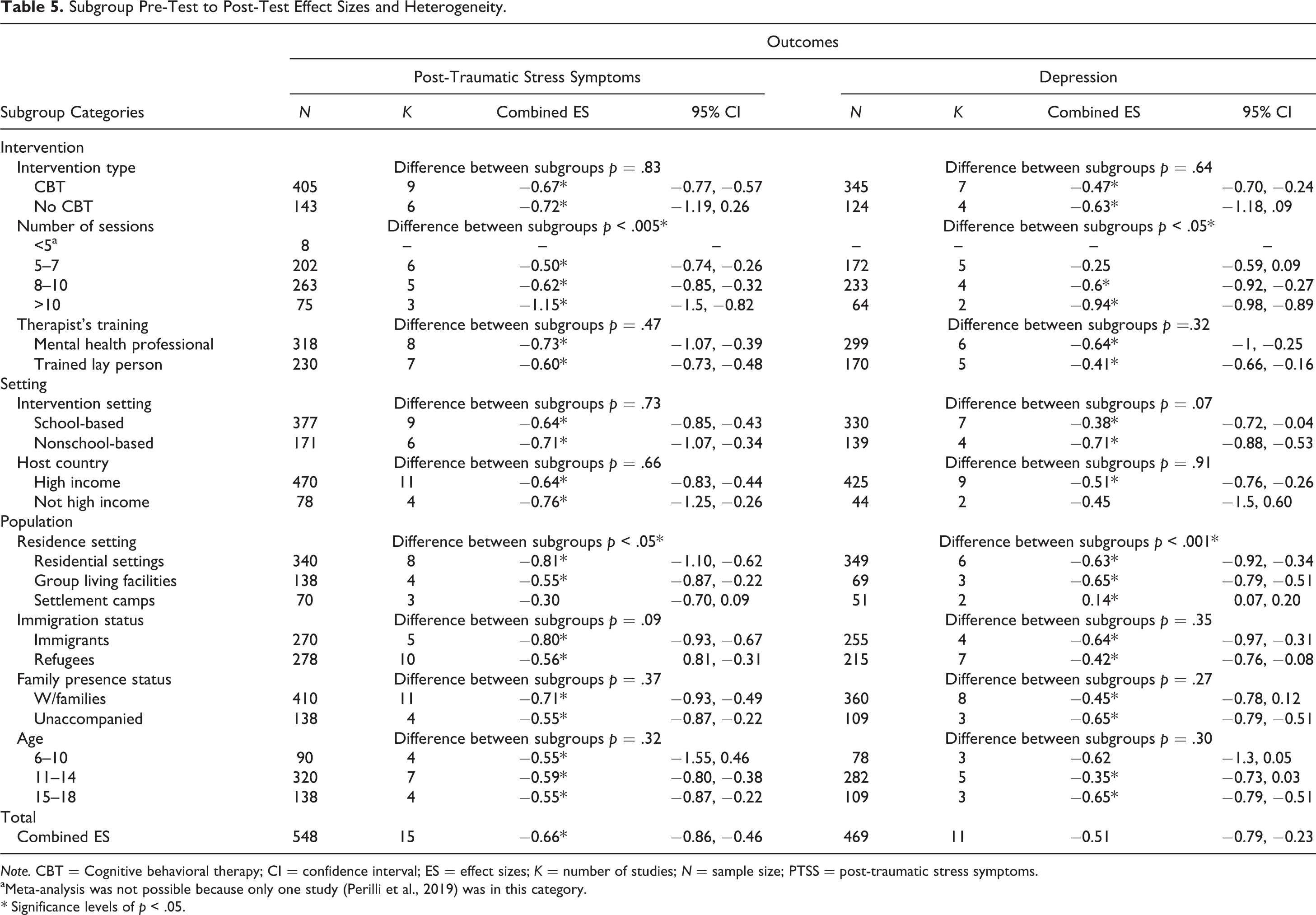
Note. CBT = Cognitive behavioral therapy; CI = confidence interval; ES = effect sizes; K = number of studies; N = sample size; PTSS = post-traumatic stress symptoms.
aMeta-analysis was not possible because only one study (Perilli et al., 2019) was in this category.
* Significance levels of p < .05.
The meta-analysis was repeated for the subgroup of CBT-based interventions, as the group was expected to be homogeneous. PTSS outcomes were reported for nine CBT treatment groups (Allison & Ferreira, 2017; Ehntholt et al., 2005; El-Khani et al., 2018; Gormez et al., 2017; Kataoka et al., 2003; Ooi et al., 2016; Pfeiffer et al., 2018; Pfeiffer & Goldbeck, 2017; Sarkadi et al., 2018). The combined pre–post effect size for PTSS among CBT-based interventions was statistically significant in a random effects model, d = −0.67, 95% CI [−0.79, −0.55], p < .001. No heterogeneity among effect sizes was observed (I2 = 0%, τ = 0, Q = 6.49, ns), indicating a meaningful combined effect size.
Depression
Of 12 studies that reported depression, 11 provided data adequate to be included in a meta-analysis (Allison & Ferreira, 2017; Ehntholt et al., 2005; El-Khani et al., 2018; Kataoka et al., 2003; Mancini, 2019; Ooi et al., 2016; Pfeiffer et al., 2018; Sarkadi et al., 2018; Thabet et al., 2005; Ugurlu et al., 2016; Van der Gucht et al., 2019). The combined pre–post effect size for depression was statistically significant in a random effects model, d = −0.51, 95% CI [−0.79, −0.23], p < .001. The heterogeneity among effect sizes was statistically significant and the proportion of that heterogeneity due to between-studies variation rather than sampling error was high (I2 = 77.01%, τ = .32, Q = 43.50, p < .001; Figure 3).
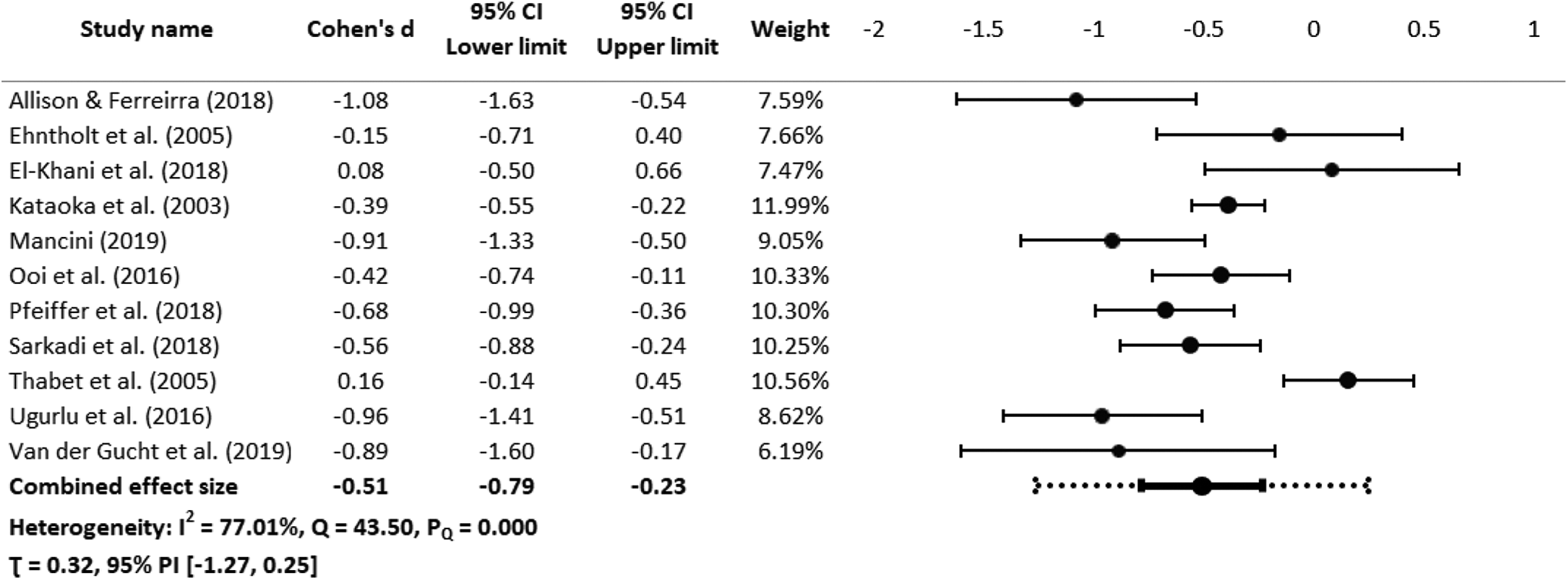
Forest plot of within-conditions effect sizes for depression. Note. CI = confidence interval; PI = prediction interval. Random effects model was used. The Forest plot for the combined effect size shows both confidence interval (solid black) and prediction interval (dash black).
The subgroup analyses across the subgroups selected a priori found the intervention effect to be statistically significant based on number of sessions and residence setting. Subgroup analyses showed significant differences based on residence setting and number of sessions. There were larger effects for depression with interventions delivered for children living in group living facilities (d = −0.65, 95% CI [−0.79, −0.51]), those delivered in more than 10 sessions (d = −0.94, 95% CI [−0.98, −0.89]). Other variables did not demonstrate a statistically significant effect (Table 5). The funnel plot using trim-and-fill analysis and Egger’s regression test (t = −0.80, p = .445) did not provide evidence for a publication bias.
The combined effect size on depression among the subgroup of seven CBT-based interventions (Allison & Ferreira, 2017; Ehntholt et al., 2005; El-Khani et al., 2018; Kataoka et al., 2003; Ooi et al., 2016; Pfeiffer et al., 2018; Sarkadi et al., 2018) was statistically significant in a random effects model, d = −0.47, 95% CI [−0.70, −0.24], p < .001 with substantial heterogeneity (I2 = 57.60%, τ = .2, Q = 14.15, p < .001).
Between-Condition Effects
PTSS
For studies with a comparison condition (n = 5), a between-group meta-analysis was performed. Although having a comparison or control condition, the study by Meyer DeMott et al. (2017) lacked data to be included in the analysis. The combined between-group effect size for PTSS was small and statistically significant in a random effects model, d = −0.31, 95% CI [−0.65, 0.03], p < .001. The heterogeneity among effect sizes was low (I2 = 29.42%, τ = .14, Q = 5.67, p = .225), indicating a meaningful combined effect size in a homogeneous population (Figure 4).
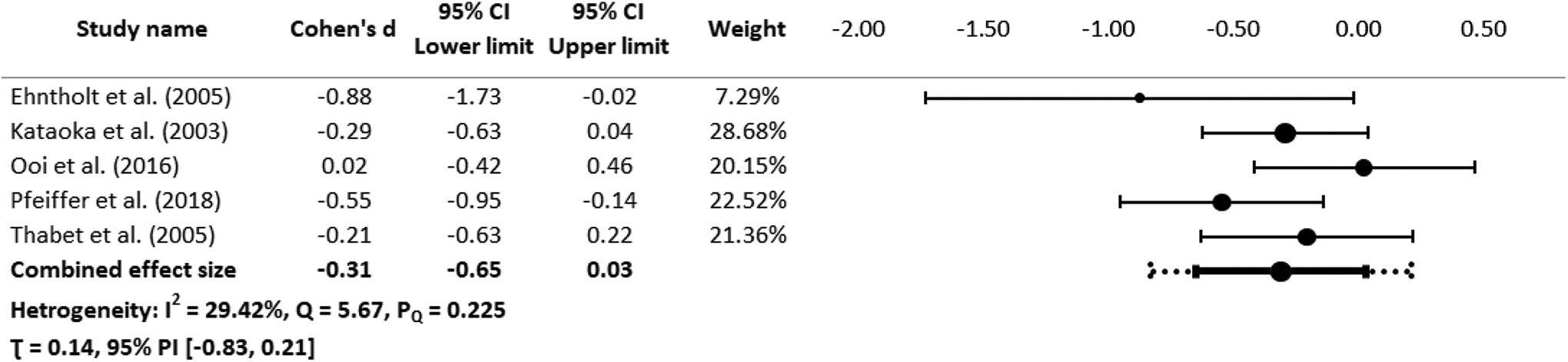
Forest plot of between-conditions effect sizes for post-traumatic stress symptoms. Note. CI = confidence interval; PI = prediction interval. Random effects model was used. The Forest plot for the combined effect size shows both confidence interval (solid black) and prediction interval (dash black).
Depression
The combined between-condition effect size for depression among the studies with a comparison or control group was small but not significant in a random effects model, d = −0.23, 95% CI [−0.63, 0.17], p = .055. The heterogeneity among effect sizes was substantial (I2 = 54.26%, τ = .24, Q = 8.75, p = .068), indicating that the combined effect size was not meaningful (Figure 5). The subgroup analyses were not conducted as the combined effect was not statistically significant (Figure 5).
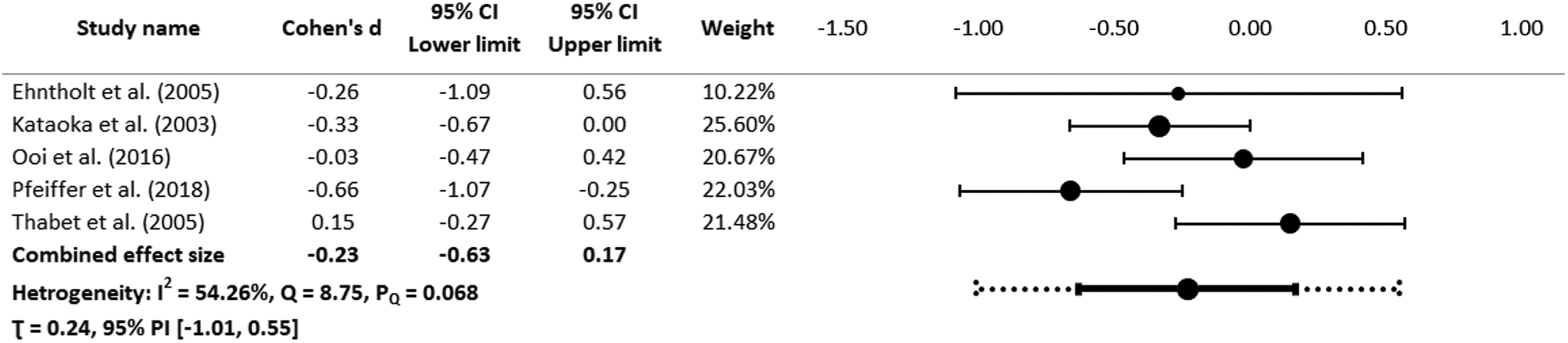
Forest plot of between-conditions effect sizes for depression. Note. CI = confidence interval; PI = prediction interval. Random effects model was used. The Forest plot for the combined effect size shows both confidence interval (solid black) and prediction interval (dash black).
Discussion and Applications to Practice
Overall, the analyses indicated that group interventions were generally effective in reducing psychological harm for refugee and immigrant children. The interventions had the largest effects in reducing PTSS rather than depression, and there were differences in effects across all interventions (Figures 2–5). For the meta-analysis, the differences became apparent when the studies were categorized into CBT and non-CBT interventions. CBT interventions were the most rigorous and effective for reducing PTSS and depression (Kataoka et al., 2003; Pfeiffer et al., 2018). Most studies (particularly non-RCTs) had high risk of bias, reducing confidence that the interventions were largely responsible for observed changes. The intervention in an RCT that had a combination of lowest risk of bias with significant positive effects was Mein Weg (Pfeiffer et al., 2018).
Interventions in non-RCT studies that reported good intervention effects but had the highest levels of risk of bias, such as somatic soothing (Mancini, 2019) and art therapy (Ugurlu et al., 2016), should be interpreted with caution. That said, the intervention effects suggest that these interventions show promise but need replication in more rigorous research. Indeed, most studies lacked rigorous designs with many methodological flaws and few studies used randomized controlled designs. More RCTs are needed to demonstrate the efficacy and effectiveness of group interventions in reducing PTSS and depression.
When examining each outcome within and across conditions, there are further insights. For within-condition for PTSS, there was a combined Cohen’s d effect size of −0.66. The analyses suggested heterogeneity was significant, and when further analyzed, significant differences were detected based on number of sessions and participants’ residence setting. Larger intervention effect sizes were found as the number of sessions increased. The studies with over 10 sessions showed the largest combined effect size on PTSS. There was also a significant difference based on residence setting. While studies with participants who lived in residential settings show a large effect on PTSS, studies with participants who lived in group living facilities showed a medium effect and studies with participants in settlement camps showed a small intervention effect.
For depression within conditions, there were significant differences in residence setting and number of sessions. There were larger effect sizes on depression for studies that provided interventions over more than 10 sessions. Indeed, the effect size increased as the number of sessions increased. There was also a meaningful difference based on participants’ residence setting. Specifically, there was a small negative intervention effect for those who lived in settlement camps. This might be because of the temporary nature of these residential settings. Those who lived in group living facilities and other residential settings in urban areas showed a medium intervention effect.
The between-condition effect size for depression was not meaningful and thus could not be interpreted. However, the combined effect size for PTSS was meaningful (d = −0.31, 95% CI [−0.65, .03], p < .001) and homogenous (I2 = 29.42%, Q = 5.67, p = .23). This is notable given that the studies included in this analysis had relatively rigorous designs, giving more confidence in the efficacy of the interventions in reducing PTSS.
Group variables (e.g., structures, processes) were either not reported or analyzed in many studies. The lack of adequate discussion about the nature of the groups was a missed opportunity to advance the science of group work. As discussed by Burlingame et al. (2013), group theory, group structures, processes, leadership variables, and membership combine to bring strength to group-based interventions. Measurement of key group variables such as cohesion (Burlingame et al., 2018) or engagement (Macgowan & Newman, 2005) and including basic information about the groups such as composition and leadership will help advance the practice and science of these interventions. That said, it may be that some interventionists deliberately use groups for economy or efficiency without interest in member interactions or other benefits of groups; essentially, group work is used to deliver individual therapy to multiple individuals rapidly, in a crisis perhaps. However, this purpose was not explicit in the studies reviewed in this paper. With respect to attention to group variables, the study involving Mein Weg was the standout (Pfeiffer et al., 2018). The study integrated trauma-focused CBT into group processing principles, which included sharing experiences, feelings, and problems with group members, and showing mutual support for one another when sharing the trauma narratives. Future group intervention studies should include both description and analysis of group factors so that they could be better understood.
Practitioners working with young refugee and immigrant children can utilize any of the group-based interventions (except for crisis management), given they were effective. Specifically, the CBT-based Mein Weg is recommended. Mein Weg provided the best guidance for practitioners on how the groups should be constructed.
This study was limited by including published studies that had undergone peer-review, which excluded unpublished research reports. Although the inclusion criterion would have drawn in mixed method studies (none were found), qualitative studies were excluded. Additionally, only studies written in English were included in this review. Many refugees and immigrants live in non-English-speaking countries and there may be studies written in the languages of those countries. As few studies included follow-ups, the meta-analysis focused on pre- to post-test only, so the longer term effects of the interventions could not be determined. More studies are needed with follow-ups. Moreover, the findings from the subgroup analyses should be viewed with caution. The high heterogeneity observed in the meta-analyses of both outcomes could not be fully explained from the factors derived from the literature.
In conclusion, all interventions reduced PTSS and depression in immigrant and refugee children to some degree. However, Mein Weg (Pfeiffer et al., 2018) was the most reliable, rigorous, and effective intervention, specifically designed for adolescent refugees. It has not been widely used or tested and should therefore be replicated. Future group intervention studies should include more rigorous designs and a description and analysis of group factors so that within-group factors could be better understood.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported in part by a graduate assistantship from Robert Stempel College of Public Health and Social Work, Florida International University.