
Abstract
Purpose
This pilot study evaluates the acceptability and preliminary efficacy of solution-focused brief therapy (SFBT) for depression, anxiety, and hope among adolescent and young adult (AYA) diagnosed with cancer. Method: 10 AYAs with a primary sarcoma diagnosis participated in an open pilot of SFBT for their depression between January and June 2019 delivered by trained social work interns.
Results
All participants completed four planned sessions and reported strong acceptability of SFBT. Statistically significant improvements were observed for pre- and post-treatment scores for depression, anxiety, and levels of hope. These improvements were maintained at 1-month follow up, with significant patterns of difference in study participants’ depression, anxiety, and levels of hope over time.
Conclusions
SFBT is an acceptable intervention approach for depression (and anxiety) among AYAs diagnosed with cancer. SFBT offers a brief, strength-based, and hope-engendering approach to address mental health concerns among young adult diagnosed with cancer.
Keywords
Adolescents and young adults (AYAs) diagnosed with cancer is an age-defined cancer population between 15 and 39 years old (Siegel, Miller, & Jemal, 2020). Population-based cancer incidence data in the United States estimated 90,000 AYAs are newly diagnosed with cancer every year, and there are over 650,000 AYA cancer survivors in 2020—a statistic expects to rise rapidly in the next decade (Miller et al., 2020). Unlike their pediatric or adult counterparts diagnosed with cancer, AYA cancer survivors experience unique biopsychosocial challenges due to their distinct developmental needs and, consequently, are disproportionately impacted by the side- and late-effects of their cancer diagnoses and treatments (Patterson, McDonald, Zebrack, & Medlow, 2015). Common challenges distinct to AYA cancer survivors include but are not limited to premature confrontation of death, grief due to loss of reproductivity, financial toxicity caused by academic and occupational disruptions, and compromised sexual health due to cancer treatment (Kaddas et al., 2020; K. Young et al., 2019; Zebrack & Isaacson, 2012). As a result, AYA cancer survivors are at significantly greater risk of psychological distress than their pediatric or adult counterparts, including depression (Jones et al., 2020; Kaul et al., 2017).
Clinical and population-based studies reported over 30% of AYAs diagnosed with cancer meet criteria for clinical depression, a rate significantly higher than cancer survivors of other age groups (Prasad et al., 2015; Zhang, Hu, Wang, & Antalis, 2020). Notably, the rate of depression among AYA cancer survivors is three to four times higher than that of the general population without cancer (Brody, Pratt, & Hughes, 2013). If not properly treated, depression among AYA cancer survivors is likely to cause poor treatment adherence, increased social isolation, reduced self-efficacy, compromised life quality, and alleviated suicide risk (Geue et al., 2018; Lauer, 2015; Park & Rosenstein, 2015). Therefore, it is essential to effectively address depression among AYAs diagnosed with cancer.
Although research-supported psychotherapeutic depression interventions are available, such as cognitive behavioral therapy (CBT), there exists several gaps in the literature targeting clients with comorbid depression and cancer. First, diagnostically oriented psychotherapies that target irrational or unrealistic thoughts and negative emotions among clients with depression may not be sufficient for individuals with cancer (Dekker et al., 2017). For example, Greer and colleague (2010) argued that traditional CBT techniques may not effectively address negative thought patterns and emotions that are rational/normal but nonetheless intrusive and distressing for cancer survivors, such as death related fear and sadness, or low mood triggered by cancer treatment related fatigue.
Second, few strength-based psychotherapeutic intervention has been empirically evaluated targeting depression among cancer survivors (Casellas–Grau, Font, & Vives, 2014; Yan, Chan, Chow, Zheng, & Sun, 2020). This represents a major gap in the literature given a wealth body of evidence supporting the therapeutic value of strengths and positive emotions for individuals diagnosed with cancer (Baczewska et al., 2019; Casellas–Grau et al., 2014; Seiler & Jenewein, 2019). For example, studies have found that hope among cancer patients is inversely associated with major cancer-related symptoms including pain, fatigue, and psychological distress, and the relationship persists even after accounting for important demographic and medical variables like cancer stage (Berendes et al., 2010). Therefore, it is essential to empirically evaluate strength-based psychotherapeutic intervention targeting depression among individuals diagnosed with cancer.
Finally, many well-validated depression treatment options are structured/manualized and often require a minimal of eight sessions. Such requirement, however, discourages cancer survivors from seeking depression treatment because many of them are already overwhelmed with busy medical appointments and personal schedule addressing life disruptions caused by cancer and its treatment (Zhang et al., 2021b). Tighe and colleagues (Tighe, Molassiotis, Morris, & Richardson, 2011) offered insights into the post-treatment life of 39 breast cancer survivors, with many of them reporting a sense of being overwhelmed, stressed out, and do not have time to properly attend to their mental health needs. As a result, AYA cancer survivors are more likely to engage in brief depression treatment approaches than those that are longer and require more time commitment. In summary, when treating depression among AYAs diagnosed with cancer, it is essential to consider non-diagnostic, strength-based, and brief psychotherapeutic approaches. One approach that meets all these criteria is solution-focused brief therapy.
Solution-focused brief therapy (SFBT) is a strength-based, solution-focused, and research-supported brief psychotherapy (Franklin, 2015). SFBT is a popular clinical approach among social workers, especially those working in school and hospital settings (Bond, Woods, Humphrey, Symes, & Green, 2013). For example, SFBT has been reported as a top school-based clinical intervention delivered by school social workers in the United States and internationally (Franklin & Belciug, 2015). Similarly, numerous clinical trials have supported the use SFBT in healthcare settings as administered by health social workers (J. S. Kim, Brook, & Akin, 2016; Li et al., 2018). SFBT’s non-diagnostic orientation and its focus on individual strength are consistent with social work values, making it well accepted among social work practitioners (Franklin, 2015).
SFBT overcomes various gaps in the psychotherapy literature alleviating depression among AYA cancer survivors. First, grounded in social constructivism, SFBT practitioners pay little attention to what have caused the problem (the diagnostic model) but focus on co-constructing solutions with the clients by identifying their previous success and/or inner strengths (the strength-based model) (J. S. Kim, Jordan, Franklin, & Froerer, 2019). As a result, SFBT practitioners do not focus on identifying AYA cancer survivors’ “irrational” thoughts and correcting them, such as “I have to be fearful of cancer returning for the rest of my life.” Instead, SFBT practitioners may ask the clients to think about a previous experience when they had no control over something but were able to maintain their fear at a manageable level.
Second, SFBT explicitly uses positive emotions, such as hope and resilience, as its core change mechanism. Kim and Franklin (2015) reviewed a robust body of literature and found that solution-focused techniques, for example, miracle question or exception question, invoke clients’ positive emotions, which further elicit their thought-action repertoires that are broad, flexible, and receptive to new thoughts and actions. In addition to broadening clients’ though-action repertoires, positive emotions also help build durable resources that can be utilized for future use. This is especially relevant to AYA cancer survivors given few existing psychotherapeutic approaches utilizes positive emotions when being delivered to individuals diagnosed with cancer.
Third, SFBT is a brief intervention approach requiring an average of three to four sessions to show therapeutic progress, including for clients in medical settings (Zhang, Franklin, Currin–McCulloch, Park, & Kim, 2017). In comparison to other structured and longer treatment approaches, a brief option, like SFBT, is ideal for AYAs diagnosed with cancer to accommodate for their busy life schedule. Besides, younger clients are more likely to accept brief psychotherapies than longer options due to their natural tendency to disengage from authoritative figures (Tanner–Smith & Lipsey, 2015).
Finally, SFBT has been empirically validated as an effective depression treatment approach in medical setting, including for those diagnosed with cancer. Zhang et al (2017) conducted a meta-analysis of SFBT in medical settings, and results of the study revealed an overall statistically significant treatment effect of SFBT for psychological distress among individuals with chronic health conditions, d = 0.34, p < 0.05. In addition, studies have reported SFBT as a viable approach working with cancer patients and their family members in the United States (Neilson–Clayton & Brownlee, 2008). Finally, studies have reported that SFBT is effective in reducing psychological distress, including depression, among caregivers of cancer patients (Zhang et al., 2018) and for Chinese AYAs diagnosed with cancer (Zhang et al., 2021a), further supporting SFBT’s potentials in alleviating depression among AYAs diagnosed with cancer.
Despite a robust body of theoretical and empirical literature indicating SFBT’s potential in alleviating depression among AYA cancer survivors, to our knowledge, no existing study has evaluated SFBT for depression among AYA cancer survivors in the United States. This represents a critical gap for social work practitioners as oncology social workers are the largest mental health workforce for cancer patients in America (Zebrack et al., 2016). Therefore, this pilot study aims to examine the acceptability and (preliminary) efficacy of SFBT for depression among AYAs diagnosed with cancer when being delivered by social workers. Specifically, we hold the follow study hypotheses: 1. SFBT is acceptable among AYAs diagnosed with cancer as measured by AYA reported Acceptability of Intervention Measure (AIM) score; 2. SFBT is efficacious in reducing depression for AYAs diagnosed with cancer as measured by the Patient Health Questionnaire, 9 items (PHQ-9); 3. SFBT improves the level of hope among AYAs diagnosed with cancer as measured by the Herth Hope Index (HHI); and 4. SFBT is efficacious in reducing anxiety for AYAs diagnosed with cancer as measured by the Generalized Anxiety Disorder, 7-item (GAD-7).
Method
Participants and Recruitment
Participants were referred to the study from the Michigan Medicine Sarcoma Clinic between January and June 2019. The sarcoma clinic provides comprehensive cancer care to patients diagnosed with sarcoma, ranging from medical cancer treatment to psychosocial support. This study was designed to evaluate SFBT as an embedded depression treatment for AYAs diagnosed with sarcoma. The clinic manager introduced the study to all patients who expressed an alleviated level of distress and connected them with the investigative team. Interested patients reached out to the study coordinator and scheduled a screening session. To be eligible for participation, a patient had to (1) be between the age of 15–39 years old—an age range corresponds to AYA as defined by the National Cancer Institute (2011); (2) have a sarcoma diagnosis; (3) screen positive for moderate or greater depression (PHQ-9 ≥ 10); and (4) willing to provide informed consent (and assent if applicable). Individuals were not eligible if they (1) did not speak English; (2) were receiving other forms of mental health treatment at the time; (3) had clear signs of active psychosis; (4) had cognitive impairment (based on a patient’s electronic health record, EHR); (5) reported prominent suicidal/homicidal ideation with imminent risk; or (6) were receiving end-of-life care. Participants on psychotropic medication were eligible to participate.
Design Overview and Study Procedure
This study was approved by the University of Michigan medical Institutional Review Board (IRBMED). A single group pre-test and post-test design was utilized to compare outcomes over time across pre-treatment, immediate post-treatment, and 1-month follow up. Figure 1 presents the study participant flowchart. Interested participants met with a research staff for an initial in-person screening meeting to determine their eligibility in an office that is in walking distance to the sarcoma clinic. The screening interview assessed individuals’ depression using PHQ-9, and those who reported a score of 10 or higher were invited to provide informed consent (and assent) as well as to conduct pre-treatment assessment, including Generalized Anxiety Disorder, 7-item (GAD-7), and the Herth Hope Index (HHI). Participant Flowchart.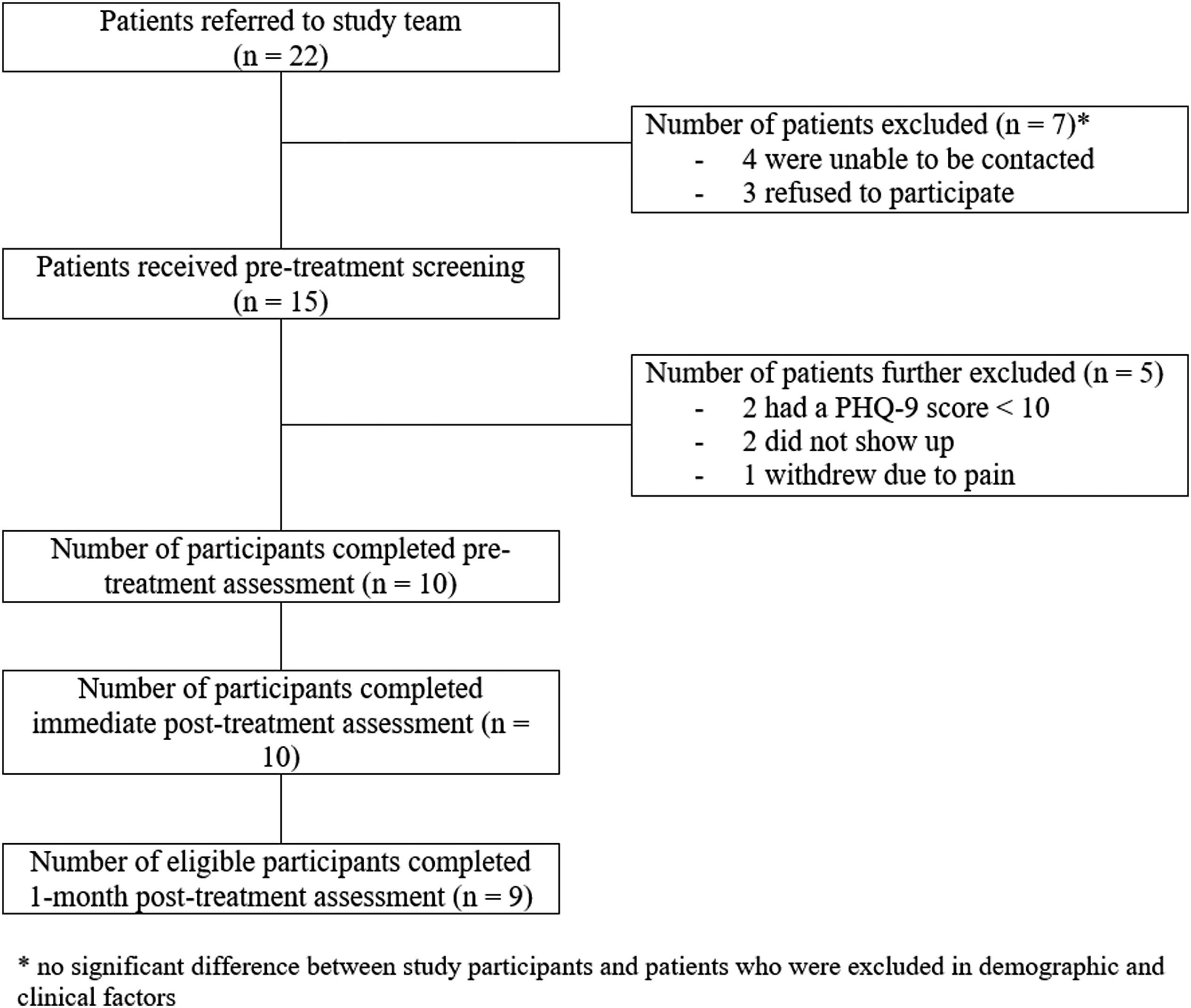
Eligible participants were then invited to meet with a study clinician to receive SFBT over a 4-week period (described later). The research assistant who administered pre-treatment evaluation also conducted immediate post-treatment (by the end of session 4) and 1-month post-treatment assessment to evaluate participants’ progress. Pre- and post-treatment assessments were completed in-person in a room without the study clinician, and the 1-month follow up assessment was conducted over the phone. Participants received free therapy as reimbursement and did not receive other incentives for participation except for parking ticket.
SFBT Intervention Protocol
Modified Content for Solution-Focused Brief Therapy with AYAs Diagnosed with Cancer.
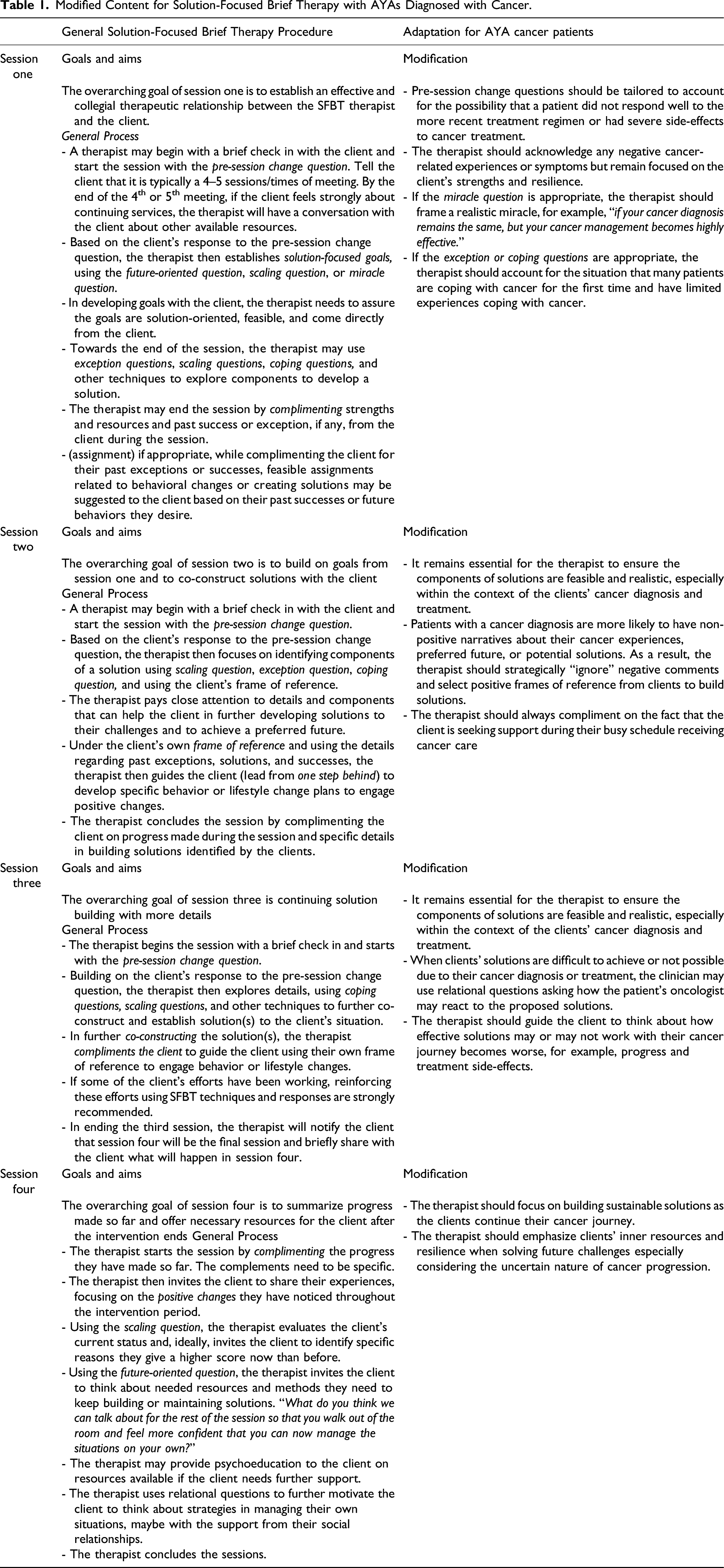
Session 1: Building rapport and setting client-generated goals with solution-focused languages and techniques. Key techniques include: solution-talk, pre-session change questions, future-oriented questions, formula first session questions, and, if appropriate, miracle question. Pay attention to the feasibility of client-generated goals, especially as contextualized in their cancer diagnoses.
Session 2 and 3: the SFBT clinician begins the session with a brief check-in and focuses on any positive changes, for example, progress, since last meeting. Through the client’s own frame of reference, the SFBT clinician attends to co-construct solutions to solve clients’ on-going challenges related to depression. Key SFBT techniques include: coping questions, exception questions, miracle questions, relational questions, and scaling questions.
Session 4: the SFBT clinician checks in with the client, informs participant that this is the last session for the study, and offers follow-up resources if the client wishes to continue receiving mental health support. The SFBT clinician focuses on reviewing client’s progress and discusses with participants about plans to continue using SFBT strategies.
An important principle when delivering SFBT to AYAs diagnosed with cancer is the adjusted use of SFBT techniques to invoke clients’ positive emotion, for example, asking about their preferred future or what would be different if a miracle happens. Most, if not all, cancer survivors would want to be cancer free when being given the chance to envision a preferred future, which is neither realistic nor constructive to the therapeutic encounter. Therefore, it is essential for SFBT clinicians to ensure SFBT techniques are asked in ways that the client’s preferred future is realistic and possible.
Training, Supervision, and Fidelity Assessment of Study Clinicians
Two master’s level social work students in their advanced year served as study clinicians. The study clinicians were trained by a PhD-level licensed clinical social worker with 5 years of clinical experiences delivering SFBT to young patients in hospital settings, including AYAs diagnosed with cancer. Study clinicians spent 4 hours reading the original SFBT manual and attended an all-day long training using the modified study specific SFBT manual for AYAs diagnosed with cancer. Each study clinician also attended a 2-hour role play session with the trainer and was evaluated using 10 criteria from the original SFBT treatment manual. Both study clinicians achieved an average score of 90 out of 100 before initiating clinical contact. The same trainer provided on-going weekly supervision throughout the duration of the study. Random (audio) recording of sessions as additional fidelity checks was not feasible in this study.
Outcome Measures
Intervention acceptability
SFBT acceptability was measured by the Acceptability of Intervention Measure (AIM), which is a psychometrically validated scale evaluating participants’ perceived acceptability of an intervention (Weiner et al., 2017). Participants responded to a 5-point Likert scale ranging from 1 = completely disagree to 5 = completely agree to the following four questions: 1. The intervention meets my approval; 2. The intervention is appealing to me; 3. I like the intervention; and 4. I welcome the intervention. The AIM has a theoretical range from 4 to 20, with a higher AIM score indicating higher acceptability of SFBT.
Depression
Depression was evaluated using the Patient Health Questionnaire, 9-item (PHQ-9) (Kroenke et al., 2001). PHQ-9 has been psychometrically validated and is one of the most widely used depression scale internationally. For cancer patients, a large sample study reported PHQ-9’s Cronbach’s alpha of .84 or higher, suggesting strong internal reliability (Hinz et al., 2016). Participants responded to a list of nine questions inquiring how often they have been bothered by these problems over the last 2 weeks using a 4-point Likert scale: from 0 = not at all to 3 = nearly every day. PHQ-9 has a theoretical range from 0 to 27, which a higher score indicating greater severity of depression. A PHQ-9 score below 10 indicates minimal or mild depression, a PHQ-9 score between 10 and 19 indicates moderate or moderately severe depression, and a PHQ-9 score of 20 or higher indicates severe depression (Manea et al., 2012).
Anxiety
The Generalized Anxiety Disorder, 7-item (GAD-7) (Spitzer, Roenke, Williams, & Löwe, 2006) was used to measure anxiety. GAD-7 is psychometrically validated anxiety measure among cancer patients, with studies reporting strong internal consistency, for example, Cronbach’s alpha ≥ .88 (Esser et al., 2018). Participants responded to how often over the last 2 week have they been bothered by a list of seven problems. Participants responded to a 4-point Likert scale (from 0 = not at all to 3 = nearly every day) with higher score indicating greater severity of anxiety. A GAD-7 score of 0–9, 10–14, and 15–21 represents minimal or mild, moderate, and severe anxiety, respectively.
Hope
Participants’ hope level was measured by the Herth Hope Index (HHI) (Nayeri et al., 2020). HHI is a psychometrically validated scale for hope with satisfactory performance among AYAs diagnosed with cancer (Phillips–Salimi, Haase, Kintner, Monahan, & Azzouz, 2007). A systematic review of HHI revealed its consistency being .88 or higher (Redlich–Amirav et al., 2018). Participants responded to 12 questions using a 4-point Likert scale (1 = strongly disagree–4 = strongly agree), with a theoretical score range from 12 to 48 and higher score indicating higher level of hope.
Data Analysis
Descriptive statistics were used to characterize participants’ demographic and pre-treatment clinical characteristics, as well as their treatment attendance. SFBT acceptability was quantified using descriptive statistic of participants’ reported AIM score.
Within-group difference between pre- and immediate post-treatment outcome scores were evaluated using two-tailed, paired samples t-test with a critical alpha level of .05. Within-group effect sizes were calculated using small sample size corrected Hedges’ g (Cooper, Hedges, & Valentine, 2019). Repeated Measures Analysis of Variance (ANOVA) was used to identify the pattern of difference on outcomes across the three timepoints, that is, pre-treatment, immediate post-treatment, and 1-month follow up. Partial eta square was used to calculate effect sizes for the repeated measures ANOVA. All enrolled participants completed all four sessions and provided pre- and immediate post-treatment scores.
We lost contact with one participant during 1-month post-treatment follow-up and used that participant’s immediate post-treatment score for imputation. Other imputation methods, such as using group average mean scores 1-month post-treatment or using the participant’s pre-treatment scores, were conducted for sensitivity analysis and all results remained the same. Distributional assumptions and outliers were evaluated for all statistical analyses and no concern was revealed. All data analyses were conducted using R Software version 4.1.1 (R Core Team, 2021).
Results
Sample Characteristics
Demographic and Pre-Treatment Clinical Characteristics (N = 10).
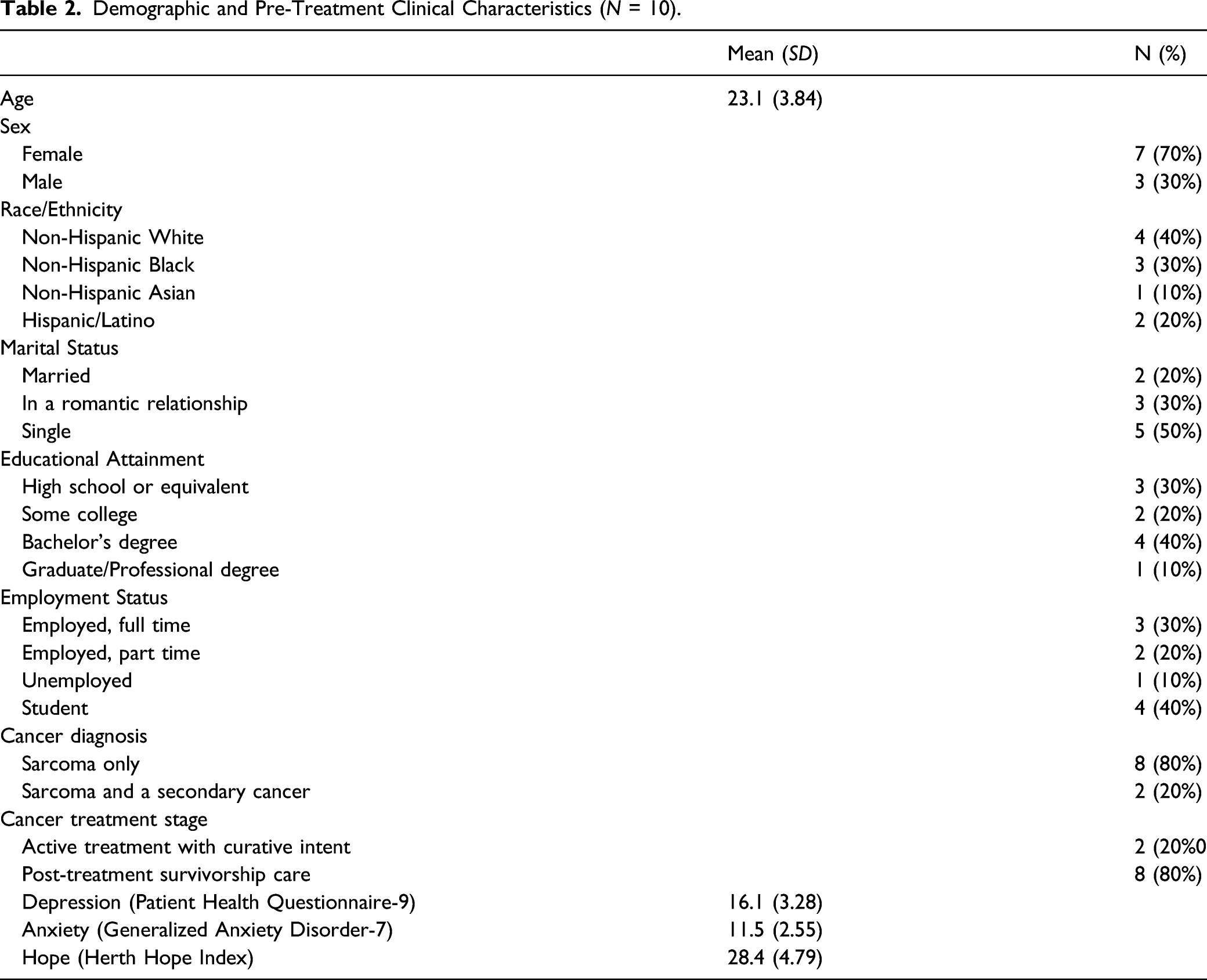
Regarding pre-treatment clinical characteristics, all study participants reported a sarcoma diagnosis, including two participants reported an additional secondary cancer (one with bone cancer and another with acute myeloid leukemia). The majority of the participants (n = 8, 80%) had completed their cancer treatment, that is, in the survivorship care stage, leaving 2 (20%) participants receiving on-going cancer treatment with curative intent. On average, participants reported a pre-treatment PHQ-9 score of 16.1 (SD = 3.28), suggesting moderately severe depression. Participants reported a pre-treatment GAD-7 mean score of 11.5 (SD = 2.55), indicating moderate anxiety. The average score of pre-treatment level of hope among study participants was 28.4 (SD = 4.79), suggesting relatively low level of hope among study participants pre-treatments.
Treatment Adherence and Acceptability
Ten study participants (100%) completed all four SFBT sessions, with an average session length of 40 minutes (SD = 9.18) per session. Participants reported an average of 18.6 (SD = 1.58) AIM score out of 20, which suggested very strong acceptability of SFBT among AYAs diagnosed with cancer. Specifically, participants reported an average of 4.8 (SD = .42) out of 5 for “SFBT meets my approval”; 4.5 (SD = .53) out of 5 for “SFBT is appealing to me”; 4.8 (SD = .53) out of 5 for “I like SFBT”; and 4.8 (SD = .42) out of 5 for “I welcome SFBT.”
SFBT’s Treatment Effect for Adolescent and Young Adults Diagnosed with Cancer
Treatment effect for depression
Within-group pre- and post-treatment change in depression, anxiety, and hope (n = 10) a

aM (SD) = Mean (SD); g = small sample size corrected Hedges’ g
*p < .05, ** p < .01, *** p < .01
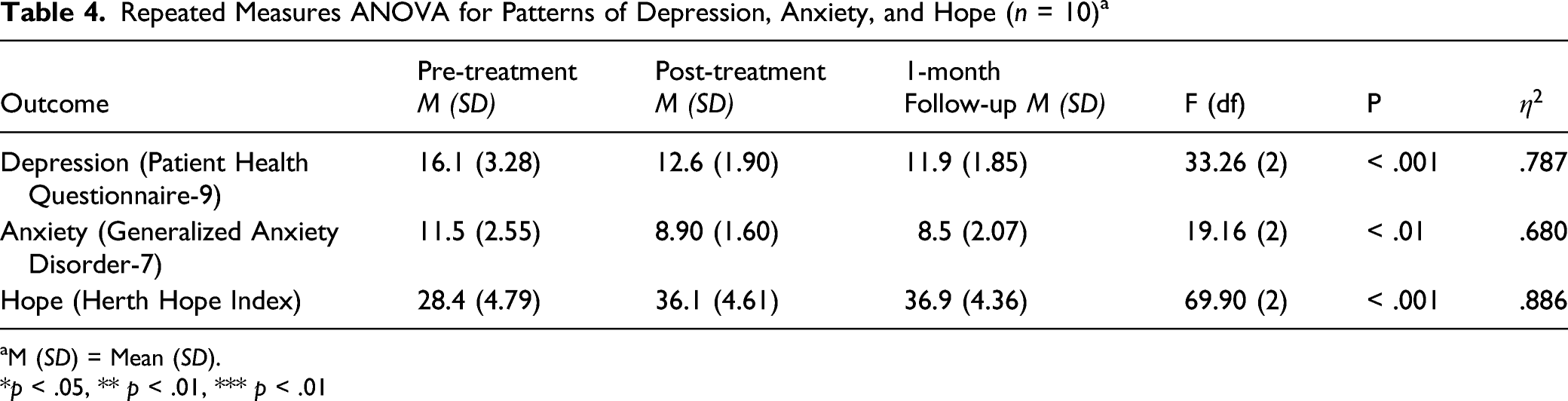
Repeated Measures ANOVA for Patterns of Depression, Anxiety, and Hope (n = 10) a
aM (SD) = Mean (SD).
*p < .05, ** p < .01, *** p < .01
Treatment effect for anxiety
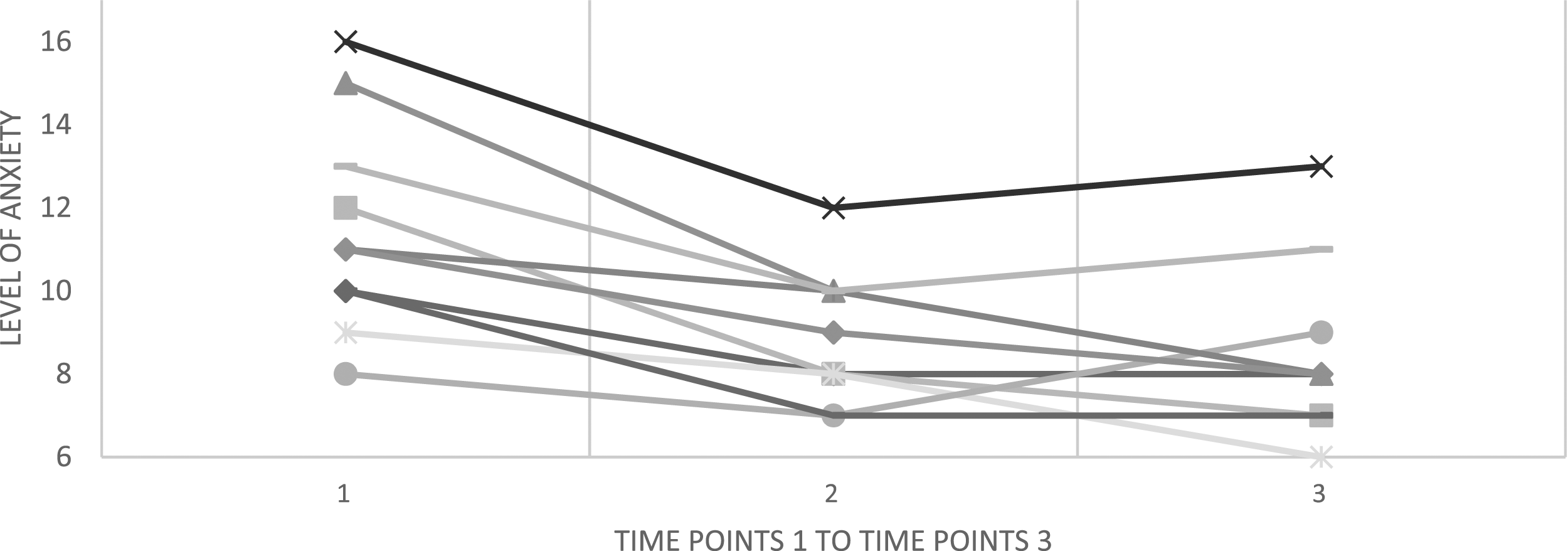
Paired sample’s t-test (in Table 3) revealed an overall statistically significant reduction in AYA cancer survivors’ anxiety from pre-treatment (mean = 11.5, SD = 2.55) to immediate post-treatment (meant = 8.90, SD = 1.60), t(9) = 5.75, p < .001. Such reduction represented a statistically significant and large treatment effect size for anxiety among AYAs diagnosed with cancer, g = .92, p < .05. Repeated measures ANOVA (Table 4) revealed a statistically significant pattern of difference on AYA cancer survivors’ GAD-7 score overtime, F(2) = 19.16, p < .01. The partial eta-squared demonstrated a within-group effect size of .680.
Treatment effect for hope
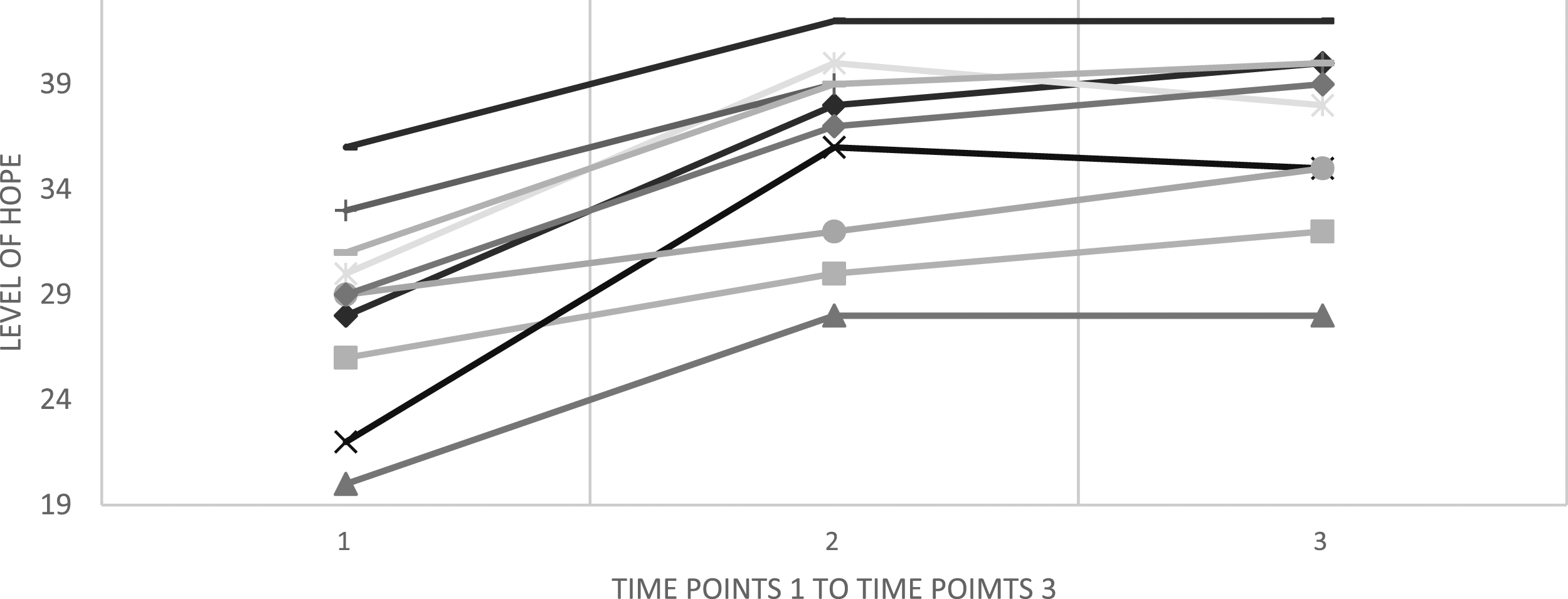
Paired sample’s t-test (in Table 3) revealed an overall statistically significant improvement in AYA cancer survivors’ anxiety from pre-treatment (mean = 28.4, SD = 4.79) to immediate post-treatment (mean t = 36.1, SD = 4.61), t(9) = 7.61, p < .001. Such increase represented a statistically significant and large treatment effect size to improve hope among AYAs diagnosed with cancer, g = 1.57, p < .001. Repeated measures ANOVA (Table 4) revealed a statistically significant pattern of difference on AYA cancer survivors’ HHI score overtime, F(2) = 69.90, p < 0.01. The partial eta-squared demonstrated a within-group effect size of .886. Figures 2–4 present the trajectory of each participant’s depression, anxiety, and hope over three timepoints, that is, pre-treatment, immediate post-treatment, and 1-month follow up. Participants' PHQ-9 Scores Across Three Timepoints. Participants' GAD-7 Scores Across Three Timepoints. Participants' HHI Scores Across Three Timepoints.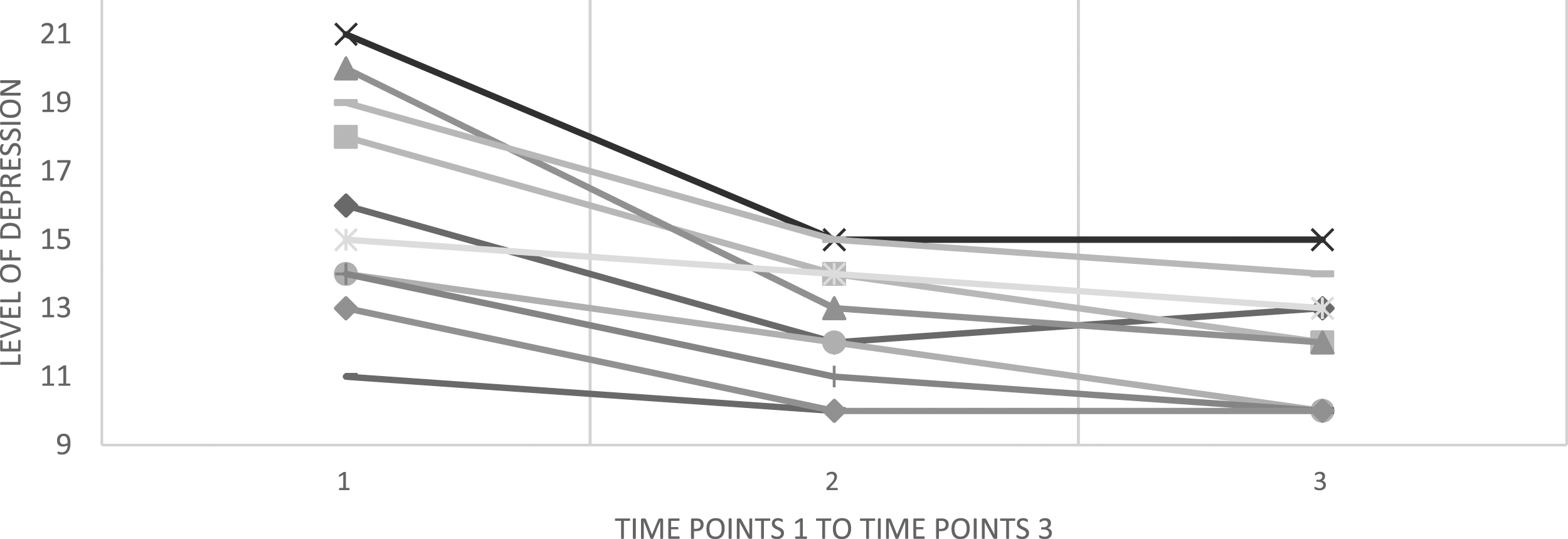
Discussion
Depression is highly prevalent and debilitating, especially for AYAs diagnosed with cancer. To address the gap that diagnostically oriented psychotherapies that require eight or more sessions often do not fit well with the unique needs of AYAs with comorbid cancer and depression, this pilot study evaluated a brief, strength-based, hope-engendering psychotherapy for depression among AYA cancer survivors. Overall, results of this pilot trial were highly promising in that SFBT was well accepted by AYAs diagnosed with cancer, and was efficacious in reducing depression, anxiety, and in promoting hope.
Treatment adherence in this study was excellent, evidenced by all study participants (100%) completed four planned sessions of SFBT. Participants’ strong adherence to SFBT identified in this study was similar to published studies of SFBT when being delivered to patients in medical settings (Li et al., 2018; Zhang et al., 2021a). As a strength-based and client-centered approach, SFBT’s collaborative nature has been repeatedly documented for its high level of acceptability among clients who may otherwise be resistant to other diagnostically oriented psychotherapies (Matanov, McNamee, Akther, Barber, & Bird, 2021; McPherson et al., 2017). This is especially important for social work practitioners because the profession’s unique emphasis on strength-based practices when serving vulnerable populations. Besides, the brief format of SFBT had likely contributed to participants’ treatment adherence, especially given the hectic life schedule of many AYAs diagnosed with cancer. Another possible factor contributing to the high adherence rate among AYAs diagnosed with cancer was the high proportion of post-treatment cancer survivors versus those who were undergoing active cancer therapy. Studies have found that cancer patients receiving active treatment are at significantly greater risk of pain, nausea, and sleep disturbances than their peers in the post-treatment survivorship phase (Cillessen, Johannsen, Speckens, & Zachariae, 2019; Zhang et al., 2020). Therefore, adherence to psychotherapies is less likely to be disrupted by side-effects of cancer treatment, for example, pain or fatigue, among post-treatment survivors than their peers receiving active cancer treatment.
Findings of this pilot study also suggested that SFBT has promise for alleviating depression among AYA cancer survivors, with statistically and clinically significant reduction in post-treatment depression. Besides, the pattern of depression across three time points (pre-treatment, immediate post-treatment, and 1-month follow up) was statistically significant, and with a partial eta-squared of .787. Such finding was consistent with existing studies evaluating SFBT for internalizing disorders in healthcare settings (Schmit, Schmit, & Lenz, 2016; Zhang et al., 2017) as well as a study evaluating SFBT for AYA cancer survivors in China (Zhang et al., 2021a). Findings of this study further extend the literature by demonstrating promising evidence of SFBT for depression among AYA cancer survivors in the United States. Oncology social workers are the largest workforce in supporting the psychosocial needs among individuals diagnosed with cancer, including AYA cancer survivors. In light of the promising finding, oncology social workers are encouraged to consider SFBT as a promising intervention with preliminary research support to alleviate depression among U.S. AYA cancer survivors.
Additionally, results of this study revealed that SFBT significantly reduced AYA cancer survivors’ anxiety, with a statistically significant and large treatment effect size. Anxiety is common among AYA cancer survivors as many of them experiencing fear of cancer recurrence and death anxiety (Gonen et al., 2012). Although having anxiety was not an inclusion criterion for this study, all enrolled participants reported a mild or greater level of anxiety pre-treatment, confirming the high prevalence of anxiety (comorbid with depression) among AYAs diagnosed with cancer. There exists substantial overlap in both the symptoms and etiologic factors of comorbid depression and anxiety (Garber & Weersing, 2010). Therefore, we were not surprised to see a reduction in anxiety among AYAs diagnosed with cancer, especially given SFBT’s treatment effect for depression (Jeannet, Conijn, Oijevaar, & Riper, 2014). It is also worth noting that SFBT by nature is transdiagnostic due to its focus on strengths rather than diagnoses/problems (H. S. Kim & Hogins, 2018). Therefore, it is most likely that SFBT techniques and skills were effective for general psychological distress, which includes both depression and anxiety. Understanding the clinical burden of comorbid depression and anxiety, oncology social work practitioners may consider SFBT as a potentially efficacious treatment that simultaneously addresses AYA cancer survivors’ depression and anxiety.
Finally, coherent with the SFBT change mechanism literature (Franklin, Zhang, Froerer, & Johnson, 2017; J. S. Kim & Franklin, 2015), this study identified a statistically significant improvement in AYA cancer survivors’ positive emotion, hope, before and after treatment. Besides SFBT’s change mechanism literature, numerous empirical studies have linked positive emotions, especially hope, with lower risk of depression and anxiety among individuals diagnosed with cancer (Jimenez–Fonseca et al., 2018; Yang, Liu, Wang, Wang, & Wang, 2014). Although this study was not sufficiently powered to formally evaluate hope as a mediator, based on existing literature and findings of this study, it is reasonable to infer that participants’ positive emotions, enhanced by SFBT, contributed to the reduction in AYA cancer survivors’ depression and anxiety.
The proposed SFBT change mechanism, however, needs to be further considered across subgroups of AYAs with different cancer diagnoses and treatment stages. Certain cancer diagnosis may pose unique challenges that have long-term impact on patients’ hope about their future. For example, prostate cancer—a drastically increasing diagnosis among AYAs—poses significant risk of infertility and family making to young adults (Bleyer, Spreafico, & Barr, 2020). Without proper oncofertility support, AYAs may have to give up the hope of having biological child, which calls for further tailoring of hope-engendering strategies of SFBT when working with subgroups of AYAs diagnosed with cancer.
It is important to note several limitations of this study. First, although results have suggested that SFBT significantly reduce depression, anxiety, and increase hope, these findings must be interpreted with caution due to the small sample size. It is important to further evaluate SFBT for AYA cancer survivors in a larger sample. Second, this study used a single-arm pre-/post-test design, which did not compare SFBT with a control condition or an active comparison. As a results, findings of the study remain preliminary, and a randomized controlled trial design should be utilized in future studies. Finally, due to the referral source for the study, all AYA cancer survivors had a sarcoma diagnosis, which limited the findings generalizability to other cancer diagnoses.
These limitations notwithstanding, results from this pilot study demonstrate the significance of offering a brief, strength-based, and hope-engendering psychotherapeutic approach for depression among AYAs diagnosed with cancer. Due to various disparity related factors, AYAs is an age-specific cancer population that is least likely to seek for mental health treatment. It is critical for social work researchers and practitioners to incorporate a research-supported and clinically meaningful intervention for this vulnerable cancer population. Results from this pilot study extend beyond existing SFBT literature and provide promising empirical evidence supporting the delivery of SFBT to AYAs diagnosed with cancer in the United States. Future research testing SFBT with larger samples and using a randomized controlled trial design is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.