
Abstract
Keywords
During the global COVID-19 pandemic, approximately two-thirds of people with mental illness felt increasingly overwhelmed by additional emotional distress while managing their preexisting mental health conditions (Gobbi et al., 2020). The pandemic has further burdened the already pressurized mental health care services (Food and Health Bureau, 2018). Despite these challenges, this might be a pivotal moment for the transformation of the way of living and attitudes by cultivating a lifestyle with self-compassion and mindfulness to face the ever-changing world, especially for people recovering from mental illness.
Beyond symptom and functional remissions, personal recovery is a unique, continuous process of reconnecting with self and others, taking responsibilities, regaining optimism, hopes, and goals, and living a satisfying and meaningful life with the potential of personal growth to face inevitable challenges in life, even with the persistence of mental illness (Leamy et al., 2011; O’Keeffe et al., 2022). Both religious and secular mindfulness-based interventions (MBIs) incorporate the ancient wisdom of mindfulness and compassion practices to enlighten and liberate all sentient beings from sufferings (Davis, 2022). People with mental illness can benefit from these MBIs to transform their way of living to manage their illness and everyday life issues and thus improve well-being through mindful compassionate self-care strategies (Villaggi et al., 2015).
MBIs generally involve practices to cultivate the mindful “being” mode, which are to be aware of the experiences at the present moment with an accepting and curious attitude, without judgment (Kabat-Zinn, 2013). A further step from the “being” mode, compassion practices are bringing the “being” mode into the human instinctive “doing” mode, considering and motivating the actions for how one can do to provide love, kindness, and better self-care after being aware of the experiences at the present moment (Neff, 2003b). By adopting the mindful compassionate mode, the person in recovery may be mindful of their present experiences with loving-kindness, nonjudgmental, open, and accepting attitudes with an understanding of common humanity to self-care when facing inevitable challenges in managing their conditions and everyday life (Muris & Petrocchi, 2017; Van den Brink & Koster, 2015). Therefore, developing innovative, effective MBIs for intervention and prevention in the mental health recovery population is an urgent research priority.
An MBI (Remind1.0) was constructed by adapting and attuning contemporary mindfulness and self-compassion practices, from the established mindfulness and self-compassion training programs such as the mindfulness-based cognitive therapy (MBCT) and the mindful self-compassion (MSC) to facilitate personal recovery among people with mental illness in community settings. Due to the exploratory nature of this pre-pilot study, hypotheses were not postulated. Information about the feasibility, acceptability, and potential effectiveness of the MBI (Remind1.0) was collected for further development of tailored MBIs in exploratory and definitive trials to target at facilitating personal recovery among people with mental illness.
Method
Study Design
A mixed-methods exploratory, single-center, two-armed, parallel-group, pre-pilot randomized controlled trial (RCT) of MBI for personal recovery was adopted in the current study. The recruitment, intervention, and data collection period was from February 2020 to September 2020 in Hong Kong at an Integrated Community Centre for Mental Wellness (ICCMW). The CONSORT extension to randomized pilot and feasibility trials (Eldridge et al., 2016) and the COREQ checklist (Tong et al., 2007) were adhered. The flowchart of the current pre-pilot RCT is shown in Figure 1. Eligible participants were randomized to either the MBI or treatment-as-usual (TAU) inactive control group. The registration number of the current pre-pilot trial is ISRCTN90791918 (https://doi.org/10.1186/ISRCTN90791918).

The CONSORT flow diagram of a randomized controlled trial (RCT) of mindfulness-based intervention (MBI, REMIND1.0) for people in mental health recovery in Hong Kong.
Participants
Potential participants were recruited by referral and advertisement at the ICCMW, and were screened for eligibility according to the following inclusion and exclusion criteria:
Inclusion criteria were aged 18 or above; permanent Hong Kong residents (i.e., period of stay greater than or equal to 7 years); diagnosed with mental illness with standardized diagnostic criteria such as the International Classification of Diseases (11th ed.; ICD-11; World Health Organization, 2019) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), for any length of illness; capable of providing informed consent to participate in the trial; able to understand Chinese languages to engage in the intervention or to complete written assessment in Chinese; and current service user from the community-based mental health service such as ICCMW, halfway houses, or integrated vocational training center.
Exclusion criteria were with diagnosis of learning disability or major cognitive impairment arising from any underlying medical condition resulting in significant functional impairment; primary diagnosis of substance abuse, as substance use may increase and/or trigger symptoms of mental illnesses as it has different trajectories from other mental illnesses; mental state that precludes the possibility of engaging in the intervention (e.g., significant thought disorder); engagement in concurrent mindfulness intervention; did not provide informed consent; or refused to be randomized.
A total of 20 participants (18 females, 2 males; age, M = 46.75 years, SD = 12.82, range: 21–62 years) were enrolled in the current RCT, given the size of the mindfulness group tended to be small to optimize delivery quality (Goldberg et al., 2017), and the sample size could provide precision about the mean and variance as it is divisible by block sizes of 2 and 4 (Julious, 2005; Whitehead et al., 2016). The sample size of the current trial was not determined from a formal power analysis, as this study aimed to examine the acceptability, feasibility, and collect information on MBI rather than its effectiveness per se.
Procedures
All procedures were approved by the Research Ethics Committee of Hong Kong Baptist University. Eligible participants were given an information sheet about the trial and sufficient time to discuss their questions and concerns. After giving the written informed consent, participants were instructed to complete a self-report questionnaire that included demographic questions and quantitative measures. Besides the baseline assessment (T0), all participants were assessed immediately after the intervention (T1) and 1 month after the intervention (T2). Each assessment included a self-report questionnaire, which took up to 30 min to complete. Participants in the MBI were also required to attend a 30-min face-to-face semi-structured intake interview at T0 with the MBI facilitator and two 45 to 60 min semi-structured interviews at T1 and T2 with the principal investigator, who has regular personal practice of mindfulness and Vipassana meditation and experience in the mental health field. In cases of dropout, the ICCMW or research staff attempted to contact the participant at least 3 times to complete the assessments and to identify the reason for dropout. As incentives to complete the assessments and intervention, participants had to complete the baseline and post-intervention assessments and attend at least 70% of the MBI to receive a HK$50 cash coupon and another HK$100 cash coupon after completing the 1-month follow-up assessment. Dropout participants still received the respective amount of cash coupons according to the number of assessments and intervention sessions they completed to thank for their contributions.
Randomization and Blinding
Participants were randomly allocated (1:1) into either the MBI or the TAU control group. The stratified randomization by age and gender was employed using SPSS syntax to reduce potential selection bias and promote similarity between groups, which was conducted by an independent third-party statistician who was not involved in any other parts of the research. Participants were inevitably aware of their group allocation. Nevertheless, quantitative outcomes were assessed via self-administered questionnaires, which were then collected by the research team, and were analyzed by a researcher blinded to the participant's group allocation as MBI and TAU groups were only represented by an alphabet (A, B, C, or D) that was assigned by the third party.
TAU Inactive Control Group
TAU consisted of any routine, typical, and normative treatment considered necessary by the participants or health professionals such as medical and ICCMW case manager follow-up. Participants were encouraged to continue with the treatment they followed before enrolling in the study. Nevertheless, due to the COVID-19 pandemic, none of the participant received other interventions but only received follow-up calls from their case managers during the current trial. Control participants received a mindfulness and self-compassion information booklet after the 1-month follow-up.
MBI Group (Remind1.0)
The current MBI was postulated by adopting existing practices from contemporary mindfulness and self-compassion training programs, including MBCT (Segal et al., 2012) and MSC (Germer & Neff, 2019). The concept of personal recovery was emphasized. Psychoeducation about the mental illnesses and relapse prevention was included. The current MBI was culturally attuned to Chinese mental health service users. Previous research suggested that Hong Kong people in recovery emphasize the outcomes and neglect the process (Law, 2017), the importance of seeing recovery as a process was highlighted in the current MBI, in which mindfulness and self-compassion skills could empower them to support the process. In addition, Chinese people were more reserved and cautious about sharing and discussing personal or emotional topics in group settings (Shen et al., 2006). Hence, the facilitator reminded participants that they could be listeners with self-reflections and that all sharing and discussion should be respected and remain confidential. Further, Chinese people often consider social context and support are prominent in recovery (Yip, 2005). However, contemporary MBIs focus on the personal motivation. The current MBI participants were encouraged to explore social and community support, responsibilities, and resources to facilitate change. Finally, culturally rooted core values and beliefs might not be appropriate to challenge as they are in the Chinese people's identity as community members (Shen et al., 2006). Thus, the facilitator encouraged participants to be mindful of those values and beliefs with compassion. Overall, the MBI content had been reviewed and refined by experts in mental health and contemplative practices.
The current MBI consisted of 8 weekly 2.5 h of experiential learning sessions delivered by a mental health professional with teacher training and personal practice of mindfulness and Vipassana meditation. The MBI facilitator also provided between-session follow-up calls to each participant to follow-up on their practice and address any questions and concerns. Alternatively, participants could contact the facilitator directly and other MBI participants if they had any inquiries through the individual or group chat on the online messaging service. The topics, content, practices, and home assignments of the MBI are summarized in Table 1.
A Summary of the Mindfulness-Based Intervention (MBI) (Remind1.0) in the Current pre-Pilot Randomized Controlled Trial (RCT).
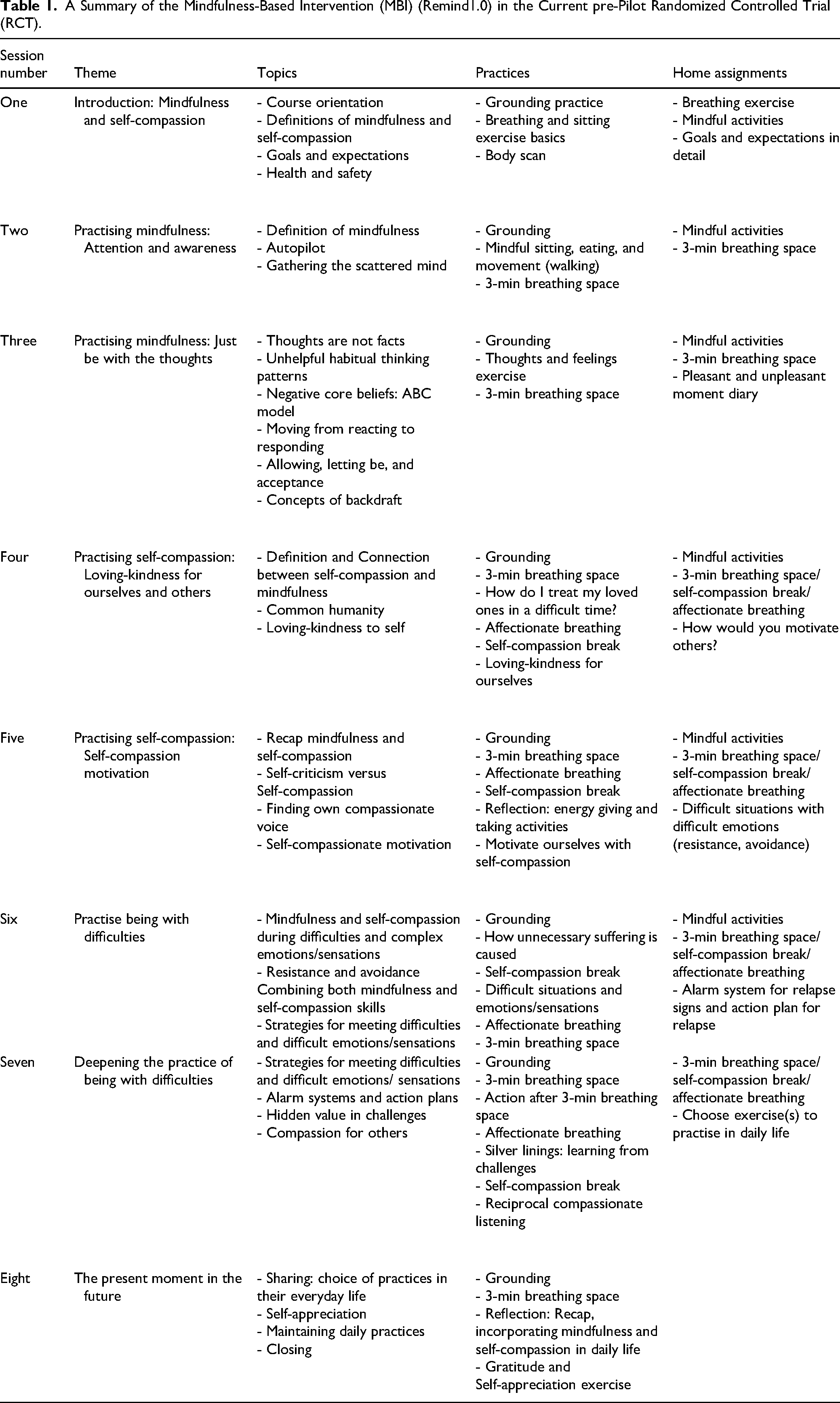
MBI participants were also encouraged to continue with their usual treatments during the study period. Due to the COVID-19 pandemic restrictions, the MBI was delivered in mixed mode: the first two MBI sessions were delivered face to face, and the rest were delivered through online Zoom video conferencing.
Primary Outcome Quantitative Measures
Personal Recovery
Personal recovery was assessed with the 24-item Recovery Assessment Scale (RAS-C), with five subscales: (1) personal confidence and hope, (2) willingness to ask for help, (3) goal and success orientation, (4) reliance on others, and (5) no domination by symptoms (Giffort et al., 1995). Higher scores indicate higher levels of perceived recovery. The RAS-C demonstrated good internal consistency (Cronbach's α = 0.92) among a Hong Kong mental health sample (Young et al., 2017).
Trait Mindfulness
Trait (or dispositional) mindfulness was assessed with the 15-item Mindful Attention Awareness Scale (MAAS) (Brown & Ryan, 2003), with a core structure focusing on the awareness or attention of the present moment. Higher scores indicate higher levels of trait mindfulness. The MAAS demonstrated good convergent and divergent validity and internal consistency (Cronbach's α = 0.82 to 0.87) across seven separate samples.
Self-Compassion
Self-compassion was assessed with the 26-item Self-Compassion Scale (SCS), with six dimensions: (1) self-kindness, (2) self-judgment, (3) common humanity, (4) isolation, (5) mindfulness, and (6) overidentified (Neff, 2003a). Higher scores indicate higher levels of self-compassion. The Chinese version of the SCS demonstrated good internal consistency (Cronbach's α = 0.84), test–retest reliability (Cronbach's α = 0.89), and validity (Chen et al., 2011; Neff et al., 2008).
Resilience
Psychological resilience was assessed with the 25-item Connor-Davidson Resilience Scale (CD-RISC), with five dimensions: (1) personal competence, high standards, and tenacity, (2) trust or tolerance of negative affect and stress, (3) acceptance of change and secure relationships, (4) control, and (5) spiritual influence (Connor & Davidson, 2003). Higher scores indicate higher levels of resilience. The Chinese version of CD-RISC demonstrated satisfactory internal consistency reliability (Cronbach's α = 0.91 to 0.97) (Ni et al., 2016; Yu & Zhang 2007).
Secondary Outcome Quantitative Measures
Positive and Negative Moods
Positive and negative moods were assessed with the Positive and Negative Affect Schedule (PANAS), with two subscales measuring the positive and negative affect (Watson et al., 1988). Higher scores indicate higher levels of affects. The Chinese version of the PANAS demonstrated good internal consistency of both the positive affect subscale (Cronbach's α = 0.85) and negative affect subscale (Cronbach's α = 0.83) (Huang et al., 2003).
Quality of Life and General Health
The overall quality of life and general health were assessed by two global items from the World Health Organization Quality of Life – BREF (WHOQOL-BREF) (World Health Organization, 1996). Higher scores indicate higher quality of life or general health. The Chinese version of WHOQOL-BREF (HK) demonstrated good reliability (intraclass correlation coefficient (ICC), ranged from 0.73 to 0.84) across all domains (Leung et al., 2005).
Acceptability and Feasibility
Feasibility
Feasibility was assessed through accrual, attrition, and compliance of the participants. Specifically, the accrual refers to the recruitment rate, which was the total number of participants screened for eligibility, informed consent to enroll, and eventually randomized to a group. Attrition and compliance refer to the number of dropouts and the attendance rate of the MBI sessions and assessments.
Acceptability
Acceptability was assessed through semi-structured qualitative interviews on participants’ experiences and perceptions toward the MBI. Responses were considered “acceptable” if most participants gave positive responses to the interview questions related to the arrangement, content, and the modes of delivery of the MBI and the perceived influence on personal recovery during and after the MBI.
Qualitative Semi-Structured Interviews
The qualitative approach assessed the feasibility by exploring the participants’ perspectives toward MBI. All MBI participants were invited to two individual, face-to-face, semi-structured interviews to discuss their experiences and perspectives of the MBI immediately and 1 month after the intervention. The interview protocol consisted of open-ended questions developed to guide the interview process. Interviews were conducted by a principal investigator who was not involved in facilitating the MBI to minimize the potential of demand characteristics. All interviews were audiotaped.
Data Analyses
Quantitative data was organized and analyzed using SPSS 25.0. Missing data were treated on an intention-to-treat (ITT) basis and replaced using the expectation–maximization (EM) algorithm. Descriptive statistics of baseline demographic characteristics and total scores across time points were presented. Continuous variables were summarized using mean, standard deviation, frequency, and percentage for categorical variables. The trends of potential interaction effects across time-points on all outcomes between MBI and TAU groups and effects within participants were estimated with ANOVAs. If the assumption of sphericity was violated, the Greenhouse–Geisser correction was applied. Post hoc analyses with the Tukey and Games-Howell were conducted. As an a priori sample size calculation was not conducted in this small pre-pilot study, the quantitative data should be interpreted cautiously.
Qualitative data collected from semi-structured interviews were transcribed and analyzed using thematic analysis (TA) to inductively identify patterns and emerging themes, following Braun and Clarke’s (2019, 2022) guide for reflexive TA. NVIVO 12.0 software package was used to assist the organization and coding process. After data familiarization with the transcripts, data were coded using open codes to identify concepts and features, categorized and clustered to themes. The process was conducted through repeated revision, refinement, and comparison to ensure coherence, exhaustive, and mutual exclusivity. Interrelationships among themes and subthemes were examined. Reflection was undertaken throughout the process to avoid potential bias. Analytic narrations were included to provide data descriptions. Quotations were selected from raw data to contextualize and support the credibility of the narrations. Quotations were edited for clarity and protection of participants’ confidentiality, in which the ellipsis (…) indicated omission and materials in square brackets ([ ]) indicated inserted materials. The first author (DC) completed the initial TA, and co-author (DY) reviewed and discussed the initial results. Before finalizing the themes and subthemes, data triangulation was performed between quantitative outcomes and qualitative interviews to enhance the confidence and reduce the uncertainty of the interpretation.
Results
Demographic Characteristics
Baseline demographic characteristics were comparable between the MBI and TAU groups, as shown in Table 2. In both groups, almost all were female (90%), with age ranging from 21 to 62 years (MBI: M = 46.30, SD = 13.17; TAU: M = 47.20, SD = 13.16), and completed at least senior secondary education (MBI: 90%; control: 90%). Most were diagnosed with depression (MBI: 60%; TAU: 70%), of which four had comorbidity of depression with anxiety disorders (MBI: n = 2; TAU: n = 2), the onset of mental illness was greater than 10 years (MBI: 60%; TAU: 70%), and had never been hospitalized (MBI: 80%; TAU: 70%). Around half had experience in contemplative practice (MBI: 50%; TAU: 40%), but the majority did not have the habit of contemplative practice (MBI: 80%; TAU: 70%), and four rarely practised (MBI: 20%; TAU: 20%), and one from TAU sometimes practised.
Demographic Characteristics of Participants by Intervention Group at Baseline.
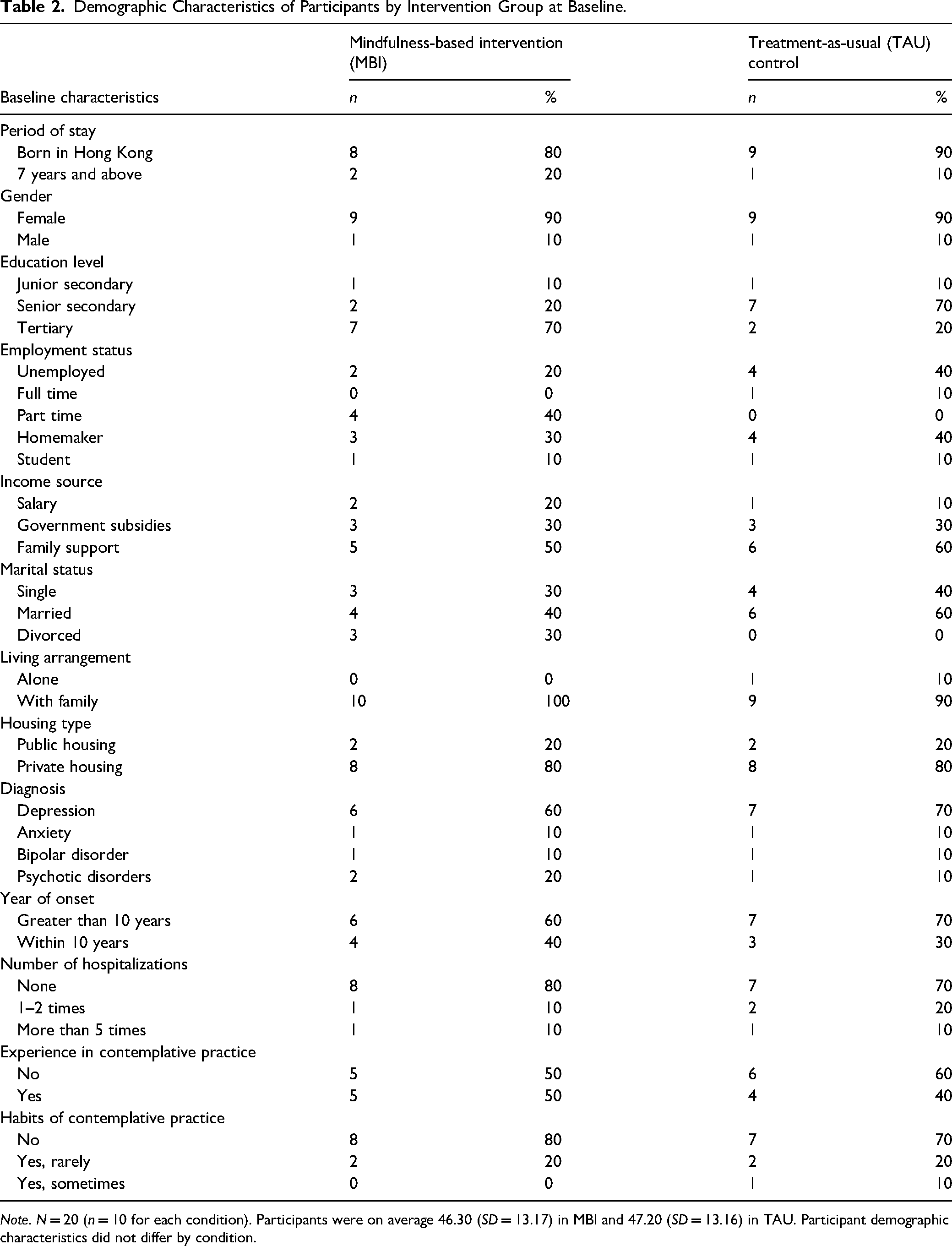
Note. N = 20 (n = 10 for each condition). Participants were on average 46.30 (SD = 13.17) in MBI and 47.20 (SD = 13.16) in TAU. Participant demographic characteristics did not differ by condition.
Primary Quantitative Outcomes
The descriptive and between and within subject ANOVA statistics on all primary and secondary outcomes are presented in Table 3. For personal recovery, the main effect of group was not significant [F(1, 18) = 1.23, p = .28, ηP2 = .064]. However, there were significant main effect of time [F(2, 36) = 12.69, p < .001, ηP2 = .41] and time by group interaction [F(2, 36) = 37.83, p < .001, ηP2 = .68]. Among the MBI group, the personal recovery scores changed significantly between time points [F(2, 18) = 42.47, p < .001, ηP2 = .83]. The personal recovery scores increased by 20.60 (p < .001) at T1 but decreased by 7.90 at T2 (p < .01) and overall increased by 12.70 (p < .001) from T0 to T2. Among the control group, the personal recovery scores changed significantly between time points [F(1.28, 11.49) = 5.01, p < .05, ηP2 = .36]. The personal recovery scores decreased by 5.20 (p < .01) at T1 and 0.90 at T2 (p = .70) and overall decreased by 6.10 (p < .05) from T0 to T2.
Means, SD, and ANOVA Statistics for the Primary and Secondary Outcomes at Baseline (T0), Post-Intervention (T1), and 1-Month Follow-up (T2).
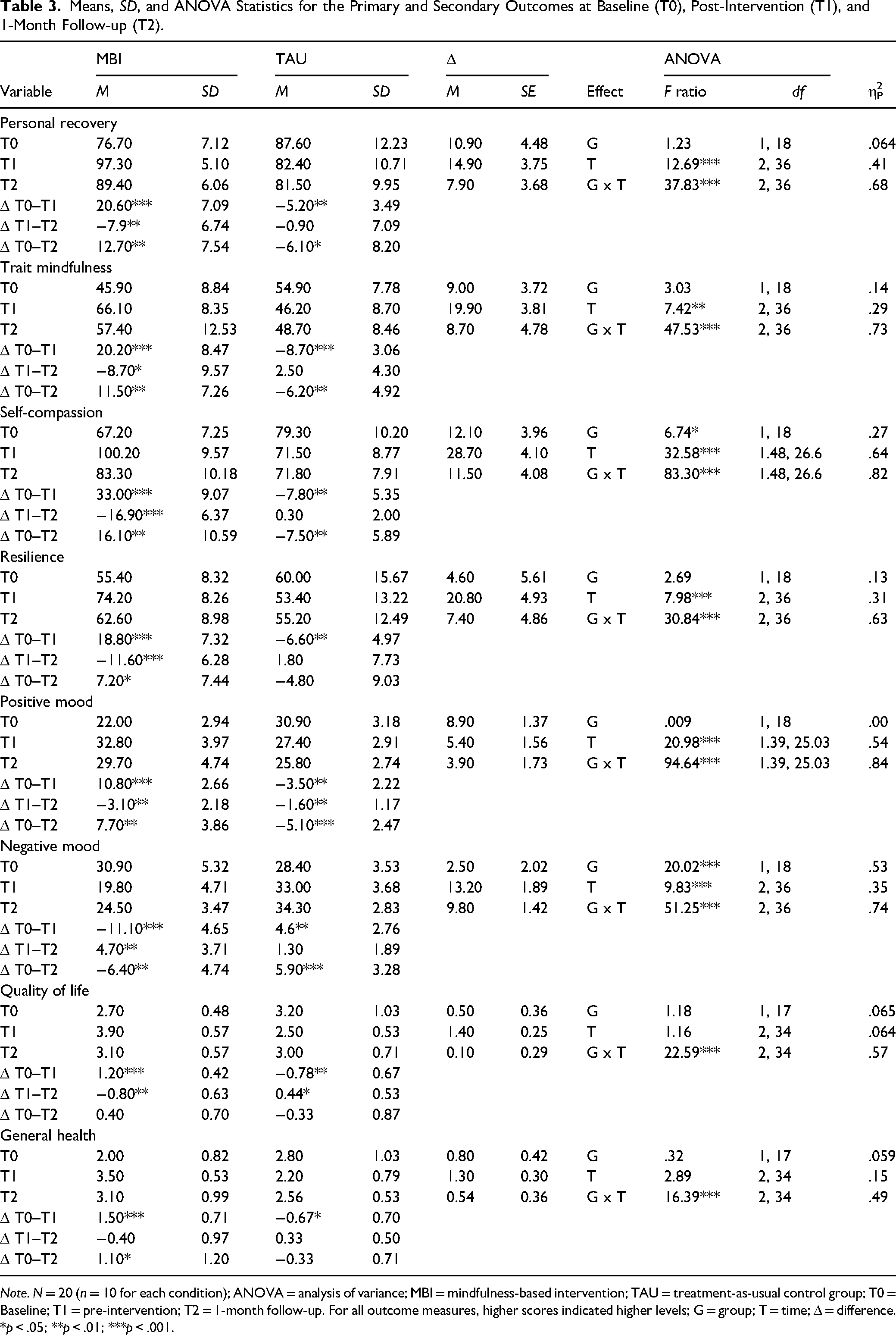
Note. N = 20 (n = 10 for each condition); ANOVA = analysis of variance; MBI = mindfulness-based intervention; TAU = treatment-as-usual control group; T0 = Baseline; T1 = pre-intervention; T2 = 1-month follow-up. For all outcome measures, higher scores indicated higher levels; G = group; T = time; Δ = difference.
*p < .05; **p < .01; ***p < .001.
For trait mindfulness, the main effect of group was not significant [F(1, 18) = 3.03, p = .099 , ηP2 = .14]. However, the main effect of time [F(2, 36) = 7.42, p < .01, ηP2 = .29] and time by group interaction were significant [F(2, 36) = 47.53, p < .001, ηP2 = .73]. Among the MBI group, the trait mindfulness scores changed significantly between time points [F(2, 18) = 28.52, p < .001, ηP2 = .76]. The trait mindfulness scores increased by 20.20 (p < .001) at T1 but decreased by 8.70 at T2 (p < .05) and overall increased by 11.50 (p < .01) from T0 to T2. Among the control group, the trait mindfulness scores changed significantly between time points [F(2, 18) = 23.14, p < .001, ηP2 = .72]. The trait mindfulness scores decreased by 8.70 (p < .001) at T1 and 2.50 at T2 (p = .099) and overall decreased by 6.20 (p < .01) from T0 to T2.
For self-compassion, there were significant main effects of time [F(1.48, 26.6) = 32.58, p < .001, ηP2 = .64], group [F(1,18) = 6.74, p < .05, ηP2 = .27] and time by group interaction [F(2, 26.60) = 83.30, p < .001, ηP2 = .82]. Among the MBI group, the self-compassion scores changed significantly between time points [F(2, 18) = 69.56, p < .001, ηP2 = .89]. The self-compassion scores increased by 33 (p < .001) at T1 but decreased by 16.9 at T2 (p < .001) and overall increased by 16.10 (p < .01) from T0 to T2. Among the control participants, the self-compassion scores changed significantly between time points [F(1.18, 10.59) = 17.40, p < .01, ηP2 = .66]. The self-compassion scores decreased by 7.80 (p < .01) at T1 but increased by 0.30 at T2 (p = .65) and overall decreased by 7.50 (p < .01) from T0 to T2.
For resilience, there was no significant main effect of group [F(1, 18) = 2.69, p = .12, ηP2 = .13]. However, the main effect of time [F(2, 36) = 7.98, p < .001, ηP2 = .31] and time by group interaction [F(2, 36) = 30.84, p < .001, ηP2 = .63] were significant. Among the MBI group, the resilience scores changed significantly between time points [F(2, 18) = 36.43, p < .001, ηP2 = .80]. The resilience scores increased by 18.80 (p < .001) at T1 but decreased by 11.60 at T2 (p < .001) and overall increased by 7.20 (p < .05) from T0 to T2. Among the control group, the resilience scores changed significantly between time points [F(2, 18) = 4.21, p < .05, ηP2 = .32]. The resilience scores decreased by 6.60 (p < .01) at T1 but increased by 1.08 at T2 (p = .48) and overall decreased by 4.80 (p = .13) from T0 to T2.
Secondary Quantitative Outcomes
For positive mood, there were significant main effect of time [F(1.39, 25.03) = 20.98, p < .001, ηP2 = .54] and time by group interaction [F(1.39, 25.03) = 94.64, p < .001, ηP2 = .84], but not the main effect of group [F(1, 18) = .009, p = .93, ηP2 = .00]. Among the MBI group, the positive mood scores changed significantly between time points [F(2, 18) = 69.40, p < .001, ηP2 = .89]. The positive mood scores increased by 10.80 (p < .001) at T1 but decreased by 3.10 at T2 (p < .01) and overall increased by 7.70 (p < .01) from T0 to T2. Among the control group, the positive mood scores changed significantly between time points [F (2, 18) = 32.86, p < .001, ηP2 = .79]. The positive mood scores decreased by 3.50 (p < .01) at T1 and 1.60 at T2 (p < .01) and overall decreased by 5.10 (p < .001) from T0 to T2.
For negative mood, there were significant main effect of time [ F(2, 36) = 9.83, p < .001, ηP2 = .35], time by group interaction [F(2, 36) = 51.25, p < .001, ηP2 = .74], and the main effect of group [F(1, 18) = 20.02, p < .001, ηP2 = .53]. Among the MBI group, the negative mood scores changed significantly between time points [F(2, 18) = 32.15, p < .001, ηP2 = .78]. The negative mood scores decreased by 11.10 (p < .001) at T1, but increased by 4.70 at T2 (p < .01) and overall decreased by 6.40 (p < .01) from T0 to T2. Among the control group, the negative mood scores changed significantly between time points [F(2, 18) = 26.29, p < .001, ηP2 = .75]. The negative mood scores increased by 4.60 (p < .01) at T1, further increased by 1.30 at T2 (p = .06) and overall increased by 5.90 (p < .001) from T0 to T2.
For quality of life, there were no significant main effects of time [F(2, 34) = 1.16, p = .32, ηP2 = .064] (but significant time by group interaction [F (2, 34) = 22.59, p < .001, ηP2 = .57] and group [F(1, 17) = 1.18, p = .29, ηP2 = .065]). Among the MBI group, the quality of life scores changed significantly between time points [F(2, 18) = 21, p < .001, ηP2 = .70]. The quality of life scores increased by 1.20 (p < .001) at T1 but decreased by 0.80 at T2 (p < .01) and overall increased by 0.40 (p = .10) from T0 to T2. Among the control group, the quality of life scores changed significantly between time points [F(2, 18) = 5.59, p < .05, ηP2 = .41]. The quality of life scores decreased by 0.78 (p < .01) at T1 but increased by 0.44 at T2 (p < .05) and overall decreased by 0.33 (p = .28) from T0 to T2.
For perceived health, the main effect of time [F(2, 34) = 2.89, p = .069, ηP2 = .15] and group were not significant [F(1, 17) = .32, p = .32, ηP2 = .059]. However, the time by group interaction was significant [F(2, 34) = 16.39, p < .001, ηP2 = .49]. Among the MBI group, the perceived health scores changed significantly between time points [F(2, 16) = 12.63, p < .001, ηP2 = .58]. The perceived health scores increased by 1.50 (p < .001) at T1 but then decreased by 0.40 at T2 (p = .22) and overall increased by 1.10 (p < .05) from T0 to T2. Among the control group, the perceived health scores changed significantly between time points [F(2, 18) = 4.80, p < .05, ηP2 = .38]. The perceived health scores decreased by 0.67 (p < .05) at T1 but increased by 0.33 at T2 (p = .20) and overall decreased by 0.33 (p = .08) from T0 to T2.
Acceptability and Feasibility of the Trial Procedures and MBI
Feasibility
Accrual and Attrition: Thirty-two potential participants were approached to achieve the target sample size of 20 eligible participants; hence, the recruitment rate was 62.5%. Those who declined participation did not meet inclusion criteria, refused to participate due to physical illnesses and relapsed, as shown in Figure 1.
All participants completed the follow-up assessments, except one from the TAU group who declined due to physical illness at post-intervention (T1) but completed the assessment at 1-month follow-up (T2). Another participant moved aboard due to the COVID-19 pandemic and thus did not complete the assessments at T1 and T2. Among 60 assessments, three assessments were incomplete. The retention rate was 95% (MBI: 100%, TAU: 90%).
Compliance: MBI session attendance was 90%. One participant discontinued after the first three sessions due to physical illness but completed all assessments. Attendance and adherence of the participants were motivated by factors related to personally relevant MBI content, the facilitator, and positive group dynamics. All participants believed the topics discussed in the MBI were pertinent to their needs. One highlighted that MBI was necessary to support them during the COVID-19 pandemic. Most mentioned the facilitator was effective, compassionate, caring, and patient with them. The weekly follow-up call with the facilitator assisted them in further exploring their experiences, witnessing their transformation, and following through with the course of the MBI. Additionally, positive group dynamics among participants, who all shared similar goals, motivated and supported one another, were considered helpful for learning, maintaining attendance, and adhering to daily practice.
Most participants only adhered to the practice part of the home assignments. They reported their experience verbally to the facilitator during the calls, but only two completed the written part. All participants gave feedback about the home assignments and their perspectives on MBI in the semi-structured interviews.
Acceptability
Logistical Arrangements: Length, Duration, and Handouts: Participants generally believe the length of the MBI (i.e., 8 weeks) and duration of each session (i.e., 2.5 hours) were reasonable. A few highlighted that it would be difficult for them to concentrate for a longer duration or to learn more materials in each session, as they tended to be affected by psychotropic medications and needed the time to digest and review the content. An additional optional 20 to 30 min at the end of each session was advisable for participants to an extent slightly of their sharing and discussion of the content. Continued weekly practice sessions after the 8 weekly sessions were considered desirable, enabling them to practise together and keep one another motivated to continue with the practice and support. Handouts were deemed essential to facilitate their learning, which helped them catch up and review, as medications and mental conditions affected their concentration and memory.
Delivery Mode: In-person Versus Online: After two face-to-face in-person MBI sessions, the remaining sessions were delivered via online videoconferencing to comply with the COVID-19 restrictions. All participants perceived similar advantages and disadvantages of the virtual sessions. Participants believed videoconferencing sessions enabled them to learn and receive mutual support safely during the pandemic, after two in-person sessions as a warm-up, with greater flexibility such as they could choose to stay behind for further sharing, switch off the camera when they felt emotional and switch it on again when ready, attend sessions at places of their choice, and could still attend the sessions even when they were slightly physically unwell. Some felt the connections among group members when everyone switched on their cameras, and one preferred live videoconferencing sessions over individual self-paced online courses. In contrast, some still preferred human interactions as the ones via videoconferencing were slightly surreal, but one felt easier to express oneself. Despite one was able to concentrate during videoconferencing sessions with family support, others mentioned that total concentration was difficult with the distractions from their family and phone. Despite the advantages of online videoconferencing sessions, all participants preferred in-person group sessions that enabled direct human interactions with eye contact, total concentration, and engagement in the present moment synchronously at the same physical location.
Content and Perceived influence on Personal Recovery: Participants responded positively to the content of the MBI. Majority of the participants perceived there were generally positive influence on personal recovery during and after the MBI. These are supported by the qualitative findings from the following thematic analyses.
Perspectives on the MBI: At Post-Intervention (T1)
Three main themes and related subthemes emerged across T1 interviews with the MBI participants, as presented in Table 4 along with quotations from interviews.
Quotes of the Themes and Subthemes Emerged From Semi-Structured Interviews at Post-Intervention (T1).
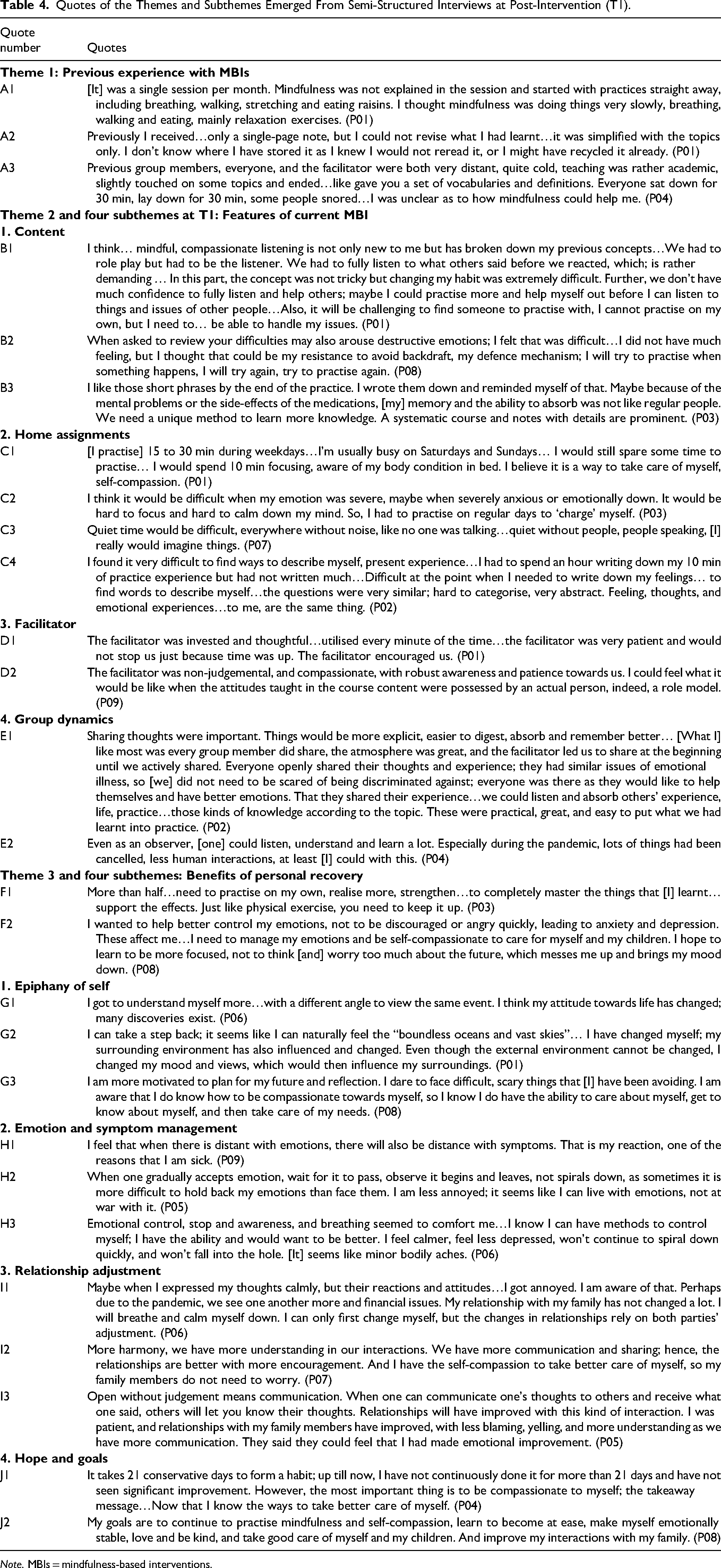
Note. MBIs = mindfulness-based interventions.
Theme 1: Previous Experience With MBIs
Participants only previously engaged in MBIs that solely focused on mindfulness without mentioning self-compassion. The length of the MBIs ranged from a single session to eight sessions. The single-session MBI involved mindfulness practices, including body scans, breathing, walking, stretching, and eating, but without explaining the concepts of mindfulness and the practices. The 8 weekly structured MBIs were MBCT, mindfulness-based stress reduction (MBSR), and mindful yoga. These MBIs generally gave an initial impression of mindfulness as doing things slowly and were referred to as relaxation, distraction, or attention training (A1). Detailed handouts were rarely provided in those MBIs, which led to difficulties revisiting and recalling the details during and after the MBI (A2). Some considered the MBIs monotonous, not personified, with vague handouts and descriptions of the topics. The interactions among learners and between learners and the MBI facilitator were considered somewhat distant (A3).
Theme 2: Features of Current MBI
Four subthemes emerged from this main theme, which included: (i) content, (ii) home assignments, (iii) facilitator, and (iv) group dynamics.
i. Content: Participants pointed out that some MBI practices were quite challenging. Almost all emphasised that the 3-min breathing space practice was too rapid, and they were pressured and discouraged when they could not shift their attention flexibly within 3 min. Most considered the mindful compassionate listening practice was challenging to practise individually, as they felt unprepared and needed to tackle their issues first (B1). One considered it was difficult to recall past struggles’ feelings (B2). Some considered self-compassion unfamiliar, and the practice was challenging, yet they grasped the theoretical concept as it was highly relevant to their issues. They generally appreciate concept illustrations through examples, especially in the local context, to stimulate how they could realise all the concepts in their daily lives. Despite some challenging practices, all perceived the use of short phrases, handouts, and the structure assisted them in learning progressively, and the content was relevant to their daily lives (B3). Some believed the content was easy to understand and practically interrelated, such as the links between cognition, mindfulness, and self-compassion that enabled them to comprehend these concepts further. Interestingly, some also considered self-compassion motivated them to maintain their practices as self-care after the MBI. Participants generally agreed regular continued content review and practices were required to fully benefit from and incorporate what they had learnt in daily life. ii. Home Assignments: Participants generally stated they completed the practical part of the home assignment daily for 15 to 40 min, and a few sustained their practice for at least 10 min on busy days as self-care (C1). Almost all found it was easier to practise alone and in a comfortable and quiet place or in nature that enabled them to fully use their five senses to be aware of their experiences. At the same time, some also preferred practising in daily activities such as walking, exercising, on transportation, before, during and after meals or bedtime to incorporate practices into their busy daily life, without the need to find extra time to practise. Participants identified practice distractions such as fatigue, busy lifestyles, or emotionally overwhelmed and unstable (C2), and when it was quiet, no one was around due to the delusional symptoms of one participant (C3). Most participants admitted having vaguely completed half of the written assignments but verbally reported their experiences in their ways (e.g., in colors) under the facilitator's guidance during weekly follow-up calls. However, a few viewed home assignments as beneficial for self-reflection. Still, some were discouraged as they had spent almost triple of the practice time writing down their experiences and criticized the assignments were monotonous. The questions were ambiguous as they found it difficult to categorize their experiences into the overall experience, emotions, feelings, thoughts, and bodily sensations. Training in writing skills and vocabularies was needed to describe their experiences in detail, besides training in attention (C4). iii. Facilitator: The facilitator played a crucial positive role in mediating the current MBI. Participants generally considered the facilitator's personal qualities of mindfulness and self-compassion relevant to their learning of these qualities. They also described the facilitator as supportive, patient, considerate, sincere, affectionate, and responsible, making learning enjoyable. Notably, one considered the facilitator the role model of mindfulness and self-compassion (D1–D2). All participants believed the weekly follow-up call was constructive for personalized guidance and addressing general and personal issues after each session. iv. Group Dynamics: All stressed that the group dynamic enabled a supportive learning environment. Participants’ sharing encouraged self-reflection and integration of mindfulness and self-compassion practices in daily life. Discussing the concepts and content could foster clarification, learning, and memory, even as observers. The majority described a sense of inclusion and belonging to the group. They warmed up quickly and started sharing under the facilitator's lead in the secure and nonjudgmental environment provided by the MBI to express their thoughts and ideas. Also, there was mutual respect and support among participants, which stemmed from their shared group-based learning and practice experience, sharing experiences of similar diagnoses and goals of self-help and emotional management (E1). Further, a few elaborated that they felt less isolated when almost all their activities were canceled during the COVID-19 pandemic (E2). A few mentioned that the group size was suitable for sharing as each participant could have their turns to express themselves.
Theme 3: Benefits of Personal Recovery
Participants generally believed they had achieved more than half of their initial expectations. All mentioned the MBI provided ways to help themselves but were not quite there yet, as the concepts were still slightly abstract and continued self-practice was required (F1). Participants’ expectations were similarly about learning ways to manage their emotions to live a serene life and become more self-compassionate. Specifically, some believed that treating themselves harshly accelerated their mental health conditions and relapses. They would also like to learn to take good care of themselves and not make others worry about them (F2). Few also expected to receive systematic guidance on mindfulness and self-compassion to gain in-depth knowledge. Four subthemes emerged from this theme, which included: (i) epiphany of self, (ii) emotion and symptom management, (iii) relationship adjustment, and (iv) hope and goals.
i. Epiphany of Self: Participants commonly reported positive changes related to the epiphany of self. The majority recognized they had become increasingly capable and motivated to self-care and, most importantly, better understand themselves through mindful awareness and reflection (G1). Some were particularly motivated to self-care due to self-compassion. Some also became more open to their experiences, shifting their habitual perceptions and accepting themselves, others, and things around them as they were (G2). They started developing the courage to conquer changes and challenges and avoid issues (G3). ii. Emotion and Symptom Management: Relating to the epiphany of self, participants believed the current MBI offered alternative methods to exert emotion management, in turn, helped manage their symptoms as emotions and symptoms as interrelated (H1). Some described emotional management involved a cascade of tasks: first by understanding their cognition, then being aware and practising to mindfully meet what was in their experiences that they could pause, notice, let go of negative feelings and thoughts, and finally bring themselves back to the present by focusing on their breathing. Without spiraling down negative emotions and responding rather than reacting to their emotions, most considered the MBI provided new insights and methods for managing their emotions, yet to improve how they handle their crisis. The majority felt more relaxed, calmer, less angry, and reduced symptoms, including somatization, stress, anxiety, and depression, and one described feeling less “at war” with emotions. They also felt less resistance and were more compassionate and in charge of themselves (H2–H3). A few also mentioned they recognized they had developed a greater acceptance of their emotions and symptoms. iii. Relationship Adjustment: Building on improvements in self, emotion, and symptom reduction, participants perceived positive adjustments in their relationships, mainly with their family. Only a few mentioned there was little to no influence as the relationships had been good or experiencing an extreme family crisis and still unable to communicate. Most adopted open and accepting without judgmental attitudes toward their family and took the first step to be more aware of and understanding themselves and others through communication. The majority considered joint efforts were necessary for relationship improvement but agreed that changes among themselves were possible such as adjusting their attitudes and practising mindfulness and self-compassion. A few mentioned receiving compliments, support, and encouragement from their family (I1–I3). Due to the COVID-19 pandemic, most did not meet up with people other than their family, but connected with others through phone calls, being more caring, patient, and understanding with colleagues and friends. Interestingly, participants observed others on autopilot mode and had compassion for those wishing that they would also have the opportunity to learn mindfulness and self-compassion. iv. Hope and Goals: All participants planned to carry on with the mindfulness and self-compassion practices and hoped to turn them into a daily habit eventually and incorporate mindfulness training with enjoyable activities in everyday life. They hoped to improve their self-care ability by maintaining practices to care for their family and others, such as those facing similar issues. The ultimate goals of some participants were to have better relationships with themselves, emotions, and others (J1). A few mentioned that they hoped to take responsibility for fulfilling their social roles and realise their potential and personal growth, and with the hope to generate new self-improvement targets through self-compassionate motivations (J2).
Perspectives on the MBI: At 1-Month Follow-up (T2)
Three main themes and related subthemes emerged across T2 interviews with the MBI participants, as presented in Table 5 along with quotations from interviews.
Quotes of the Themes and Subthemes Emerged From Semi-Structured Interviews at 1-Month Follow-up (T2).
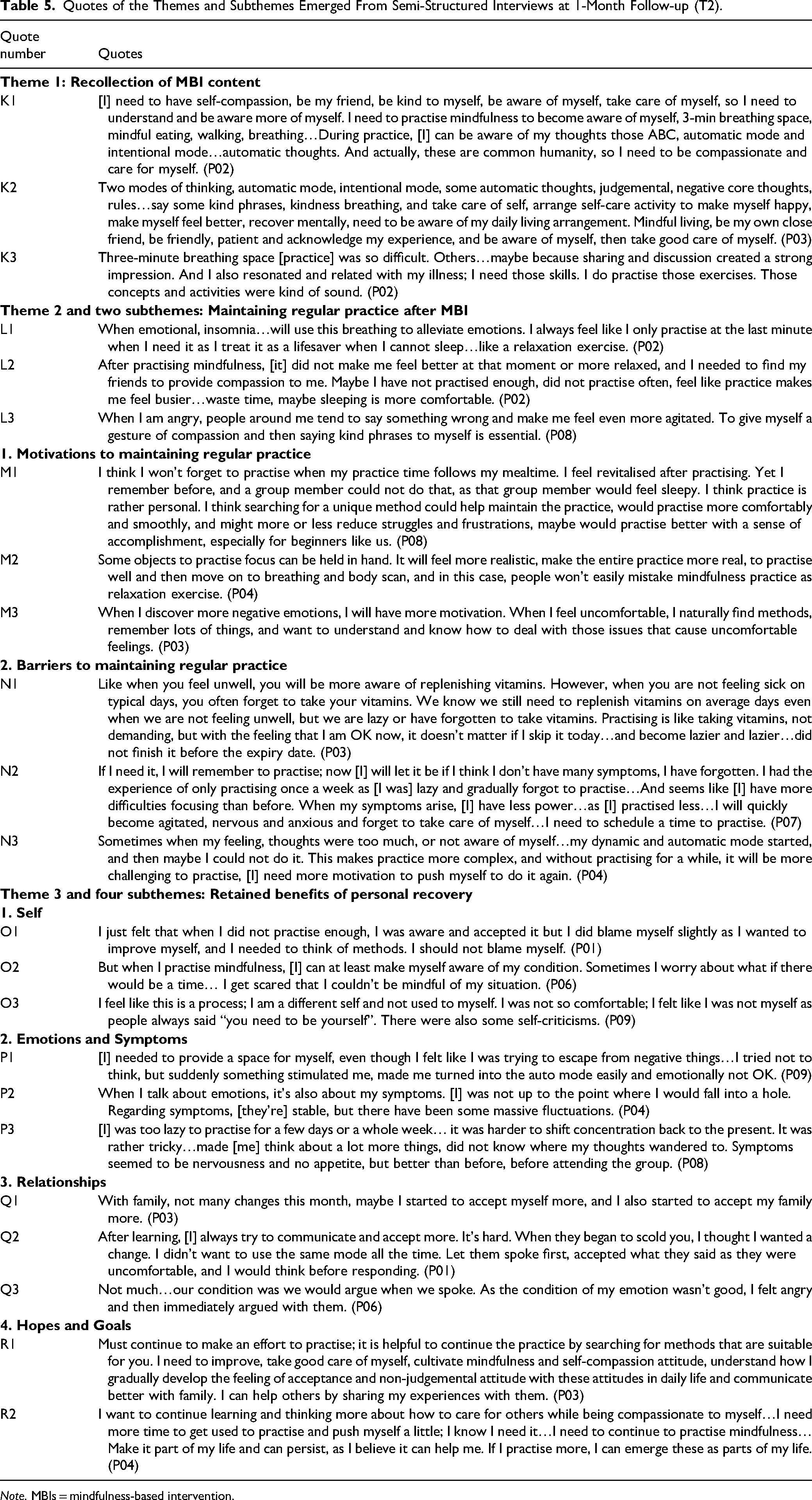
Note. MBIs = mindfulness-based intervention.
Theme 1: Recollection of MBI Content
All participants recalled more than three topics, subtopics, exercises, or practices from the MBI. Interestingly, two logical sequences were identified based on the participants’ recollections. Some first recalled the concept of self-compassion, then mindful awareness of internal and external events, and ended with self-care with compassion (K1). Some first recalled the understanding of cognition, then self-compassion, and ended with mindfulness practice as a way of self-care (K2). Either way, self-compassion was remembered in an associated manner with mindfulness. The well-remember content was related to them, either needed or suitable for them, helpful or having applied those concepts or practices in their daily lives, and had relatively more sharing among group members in the sessions. A few mentioned that challenging practices, such as the 3-min breathing space (K3), were unforgettable.
Theme 2: Maintaining Regular Practice After MBI
All participants generally expressed that they understood the importance of maintaining practice in daily life. However, almost all confessed that they practised more spontaneously for shorter periods and less frequent than during the MBI. A few were inclined to practise before sleep and when encountering issues such as insomnia or emotional disturbances (L1). A few considered the practice had made them busier, unhelpful for relaxation and alleviation, and preferred receiving compassion from others. Nevertheless, these participants considered it could be due to their lack of regular and proper practice, and admittedly they might have misused the practices as relaxation exercises (L2). Though most believed that recalling the concepts of mindfulness and self-compassion in daily lives or during adverse events provided alternative insights and relief (L3). Two subthemes emerged from this theme: (i) motivations and (ii) barriers to maintaining regular practice, predominantly individual factors.
i. Motivations to Maintaining Regular Practice: Most were motivated to maintain the mindfulness and self-compassion practices as all practices were straightforward, convenient, and can be incorporated into daily activities. Most also considered that having the ways and conditions to suit personal preferences would help maintain the practice (M1). Participants were novices and amateurs, and they believed external objects could aid them to mindfully anchor themselves to be present with nonjudgmental acceptance and remind them not to mistake mindfulness practices for relaxation exercises (M2). One further suggested that personalized practices could also reduce the struggles and frustrations while providing a sense of accomplishment for novices. Although participants admitted having practised less than during the MBI, they were still motivated to maintain practice by the experienced benefit of practice. They considered themselves less skillful when responding to their emotions than when they had more practice before, and they believed the practice was crucial to maintain and attain beneficial effects. They also wanted to facilitate compassionate self-care by maintaining the practice to sustain beneficial effects. Noteworthy, some considered the MBI handouts acted as a means to recall the MBI's knowledge and memories that would reignite their motivation to maintain their practice again. It also provided information for them to recap and revisit the concepts and practices for maintaining the practices. A few used reinforcement techniques to motivate themselves to practise. For example, a participant described having favourite snacks or compassionate hugs after practising as incentives or encouragements. Finally, two were motivated to practise partially by their negative emotions. The uncomfortableness generated by the negative emotions or fear partially acted as motivation to maintain practice to attain the power to handle emotions and situations (M3). ii. Barriers to Maintaining Regular Practice: Participants equally considered the barriers to maintaining the practice in their discussions. The most focused obstacle was the deprivation of ongoing MBI, the weekly follow-up call from the facilitator and group meetings. Some were not being reinforced to practise frequently and properly as they no longer needed to share and receive responses from the follow-up calls or session discussions. Another focus was on the lack of motivation and energy to maintain the practice in their hectic life. For the majority was laziness, while for some, it was combined with fatigue and bodily pain. One described feeling sleepy when required to concentrate for practice, such as meditating and reading. Some considered practice had a lower priority, as one felt stressed and guilty for prioritizng practice over taking care of others on busy days. Nevertheless, some added time management could overcome these obstacles. Some thought irregular practices would be acceptable as they felt fine, so the vicious cycle began. Interestingly, a participant metaphorically described the practice situation as taking vitamins: people tend to take vitamins when they feel unwell and skip taking them on good days (N1). Nevertheless, participants became less skillful, more challenging to concentrate, declined in awareness that they often found themselves on autopilot mode of thinking before they recognized, and became less emotionally stable (N2). These made practising even more challenging, so they struggled to start practising again after stopped practising for a short while. Such difficulties made them felt frustrated and less motivated to continue to practise for a while, so they continued the vicious cycle (N3).
Theme 3: Retained Benefits of Personal Recovery
Participants described aspects of themselves, relationships, hopes, and goals that remained unchanged but slightly declined in their emotion and symptom management since the T1 interview. They suspected that was due to less frequent proper practice.
i. Self: In general, participants considered their self has remained relatively unchanged. However, most had more acceptance of themselves and their internal and external experiences, such as past painful or uncontrollable events (O1). A few also highlighted they were able to be mindfully aware of their experience, but one worried about losing such ability (O2). Notably, another one described the change process as slightly uneasy and frustrating as there were struggles between changing or just being oneself (O3). ii. Emotions and Symptoms: Since the T1 interview, most participants experienced a slight decline in their emotion and symptom management. Although emotions and symptoms were interconnected, the negative decline in emotion was slightly more evident than the change in symptoms. The change of emotion was mainly concerned with emotional control. A few were less aware of their emotional experiences, more reactive, and less responsive in autopilot mode (P1). In comparison, slight negative shifts in symptoms were reported among the majority, as some considered the change was mainly due to the occasional uncontrollable emotional outbursts (P2). Some added that it was due to the decline in mindful awareness. Nevertheless, most considered they had improved since attending the MBI (P3). iii. Relationships: The majority mentioned that their relationships with family were somewhat similar to the previous interview. A few emphasized that they continued to be more accepting of their family (Q1). Some also tried facilitating communication with their family to enhance their understanding and rebuild their relationships (Q2). However, one mentioned that emotional reactivity still negatively affected family relationships (Q3). All participants considered that their relationships with colleagues and friends remained unchanged from the T1 interview. iv. Hopes and Goals: Hopes and goals were similar among participants and remained similar to the T1 interviews but with different emphases. Since almost all mentioned being less skillful and emotionally stable due to infrequent practice, they all highlighted that they would try maintaining practice. They would continue searching for suitable ways to help them persist and integrate practices into their daily lives. Some hoped these could foster mindfulness and self-compassion to facilitate emotion management and self-care, and hence better care for others. A few also hoped to improve their communication with family members by cultivating mindfulness and self-compassion. Further, some emphasized the goal of continue developing nonjudgmental and accepting attitudes toward self and others (R1–R2).
Discussion
The current pre-pilot RCT indicated that MBI (Remind 1.0) is acceptable, feasible, and potentially beneficial among people with mental illness. Although the current study was not statistically powered to assess changes, statistical analyses have shown promising trends along with the qualitative findings of participants’ experiences and perceptions. The current MBI was potentially effective in enhancing personal recovery, trait mindfulness, self-compassion, resilience, positive mood, quality of life, general health, and reducing negative mood, despite only general health maintained at the 1-month follow-up. The current study aimed to explore the acceptability, feasibility, and potential effects and provide in-depth information for the subsequent development of MBI and RCT. Therefore, the key findings are discussed, along with eight corresponding implications for intervention and methodological modifications in subsequent MBI and RCT.
First, adaptation considering specific interrelated factors of the population's needs, characteristics, and culture is needed. Although participants were readily engaged in the present moment, they were unfamiliar with focusing and expressing internal experiences, including thoughts, emotions, and bodily sensations. They had difficulties describing their experiences of mindfulness practice. Training on emotional expressions and describing and differentiating thoughts and emotions from feelings and body sensations, as such abilities are relatively less accustomed to Asian cultures (Hall et al., 2011). Guidance for the description processes is needed such as providing vocabularies, as writing narratives were associated to improve mindfulness and mental health, and reduce experiential avoidance (Moore et al., 2009). This may reduce barriers and increase incentive for participants to complete the write-ups of the assignments.
Further, participants highlighted that they tended to place their needs after the needs of others around them. Self tends to be conceived with the needs and emotions more closely of others and perceives the self as an extension of significance to others in the Asian family and community (Kastanakis & Voyer, 2014; Shen et al., 2006; Sun, 2017). Such habitual practice made it difficult to adopt self-compassion in their daily lives, despite having a clear understanding of self-compassion. The myths regarding self-compassion were emphasized to motivate participants to practise. The interconnections of common humanity could also be further explained to highlight the prominence of self-compassion practice to care for others. Thus, it would be easier for them to accept and be motivated to practise self-compassion for self-care with a greater intention to take better care of others simultaneously.
The current study also reflected the need for strategies to enhance learning among participants with mental illness. Participants stated that symptoms of the mental illness and psychotropic medications affected their learning and memory. Hence, they repeatedly considered learning strategies were prominent, such as the organized handouts provided in the current MBI had facilitated their learning and revision processes during and after the MBI to recall knowledge and reignite motivations from memories of the MBI to adhere and maintain practice. Further, health communication strategies, including social cognitive and communication theories and models to craft the messages strategically (Malikhao, 2020), can also help educate and influence the behaviors of a target population so that they can benefit and maintain the practice in their daily lives.
Second, rationale and culturally relevant examples, sharing and discussions are prominent to accompany the existing MBIs’ experiential learning approach. Explaining the intentions, aspirations, and theoretical backups of the concepts of mindfulness and self-compassion and practices along with real-life related examples, such as stories and parables, can facilitate learning and real-life application (Wasserman & Wasserman, 2017). The discussion and sharing based on the concepts, practices and exercises were found to facilitate the understanding, especially in the real-life context of the practices that followed the conceptual learning and exercises among participants. Group chats on instant online messaging platforms (e.g., WhatsApp) allowed participants to continue the peer support, sharing, and discussing the concepts and practices during and after the MBI. Nevertheless, extra effort was required from the facilitator to monitor or modulate to make sure the group sharing, discussion, and polarization were in an appropriate direction.
Third, the current study findings implied that the understanding of the concepts of mindfulness, self-compassion, and cognitive theories are interconnected and prominent to facilitate the participants’ learning processes and practices. Participants recalled concepts to view their experiences and integrated knowledge and practices into their self-care routines in their everyday lives. Cognitive theories were introduced to participants at the beginning of the MBI, made them aware of their habitual, automatic thought processes, internal, external, and mindful self-compassionate experiences, as both physical and cognitive facets played prominent roles in their experiences (De Silva, 2005). Novices in the current study made sense of mindfulness as the foundation for self-compassion and became more aware of their moment-by-moment experiences with self-care as a form of self-compassion. The balanced combination of “being” and “doing” mode allows novices to gradually build up their ability to engage in the “being” mode rather than radically eradicate the “doing” mode (Germer & Neff, 2019). Participants were more readily deploy mindful, compassionate practices when prompted by bodily sensations, thoughts, or feelings typically associated with physical or psychological health threats and followed with self-care or asked for help from others.
Fourth, consistent with other MBI studies (Keyworth et al., 2014; Parsons et al., 2017; Quach et al., 2017), participants’ home assignment compliance was less than ideal. Most reported having difficulties completing the write-ups due to monotonous and abstract questions. As suggested by the participant, modifications, including improving the clarity and adding additional probes and examples, are needed to assist their learning through relating and reflecting on mindfulness and self-compassion in the context of their daily life through the MBI materials. Specifically, participants believed that home assignments might assist them in gradually adopting the practice in their daily lives, which was essential for adherence and maintenance.
Fifth, participants in the current MBI highly valued group inclusion and cohesion as these motivated their learning process and maintained attendance. The senses of group inclusion and cohesion in the MBI were provided through a safe, nonjudgmental, and supportive learning environment with mutual respect for participants to share their thoughts and experiences. Most importantly, sharing experiences encouraged them to explore and integrate what they had learnt from the MBI into daily life. These were consistent with existing studies that the peer support in the MBI was considered prominent and predicted the effects (Canby et al., 2021; Van Aalderen et al., 2014; Wyatt et al., 2014). Specifically, the peer social support process enabled positive bonding, mutual recognition, and understanding, normalizing and de-stigmatizing, expressing feelings, enhancing reflection from recognizing the process of others, instilling hope and as a motivating factor to stay in the MBI, and helped sustain practice after the MBI.
Sixth, the facilitator was considered by the current MBI participants to have played an integral role in mediating the learning process in two main ways throughout the MBI. First, participants described the facilitator as possessing positive personal qualities embodying mindfulness and self-compassion and as a “role model” to learn from, which were considered relevant to learning and made learning enjoyable. The embodiment of mindfulness and self-compassion by the facilitator has been considered as a crucial MBI element for the group environment and attending to the group dynamics in the learning process (Banerjee et al., 2017; Crane et al., 2017).
Additionally, participants appreciated the weekly follow-up calls from the facilitator that provided personalized guidance, addressed personal questions, and that they each also had an independent relationship with the facilitator. Existing studies implied the facilitator's role included support, care, empowerment, and non-reactivity in participant interactions (Brandsma, 2017; Crane & Griffith, 2021). The MBI facilitator was also to mediate the unique learning process of each participant, as the recovery process is also personal and unique to each participant.
Seventh, the misconceptions about mindfulness had emerged from their previous experience with other MBIs among the participants. Around half of the participants had previously engaged in group-based mindfulness practices. They had initially mistaken mindfulness as doing everything slowly and as ad hoc relaxation exercises. Therefore, some suggested physical objects can help them anchor themselves to the present moment and as a reminder to avoid mistaking practices such as relaxation exercises. Mindfulness and relaxation are similar yet meaningfully distinct approaches with unique benefits. However, the two have been discussed interchangeably as researchers and clinicians applied mindfulness practices to elicit calm or relaxation, such that the differences between them become obscured (Luberto et al., 2020). Highlighting the rationale of concepts and practices to the MBI participants may address the common misconceptions.
Eighth, as the current findings and literature suggested that mindfulness practices were mistaken as relaxation practices (Luberto et al., 2020), relaxation training can serve as a comparative active control condition with similar but without the main active ingredients of the MBI provides a structurally equivalent foundation that is necessary for rigorous investigations of the relative efficacy of the MBI to identify the main ingredients such as mindfulness and self-compassion (Goldberg et al., 2017). With the relaxation control group, it may be possible to rule out the potential effects of relaxation, received attention, interpersonal and demand characteristics, and to further clarify the differential effects between mindfulness and relaxation. It can also reduce the attrition rate by avoiding the disappointment of participants for not being randomized into any activities (Kinser & Robins, 2013). Thus, a structurally equivalent relaxation control group may benefit MBI research.
The current pre-pilot study has several limitations that can be addressed in future research. The first limitation was inherent to most psychological intervention studies as double-blinding was not feasible. It was impossible to conceal the group allocation from participants. Nevertheless, precautionary procedures were carried out to blind the researcher to the MBI and TAU control group allocations until the completion of the analysis.
Another limitation concerning the change of the study protocol by adopting the mixed mode delivery of the MBI to accommodate the COVID-19 restrictions, in which the first two sessions were delivered in person, and the rest were delivered online. The delivery modes might influence the intervention effects. However, such mixed-mode allowed the current study participants to compare the two delivery modes and paved the way for further explorations of the efficacy and cost-benefits of mixed-mode MBI in future research.
Further, as in other small-scale mindfulness studies, a small sample of participants in the current pre-pilot study had specific demographic characteristics from a single center. Nevertheless, the current study was set out to estimate potential effects and collect information for subsequent trials without intending to be fully powered to detect significant effects. Moreover, participants were mainly females living in private housing and had received at least senior secondary education, possibly raising concerns about the generalizability of the results. Studies revealed that females were more likely than males to engage in mindfulness or meditation interventions (Bodenlos et al., 2017; Upchurch & Johnson, 2019). Further, participants in MBIs studies conducted in the Hong Kong community mental health settings were predominately female (Lam et al., 2020; Ting et al., 2020). Further research can explore such gender disparity among MBIs. Despite the small sample size of the current study, data saturation was reached after the semi-structured interviews, aligning with the trends suggested in quantitative results, have provided in-depth information for the further development of MBI and RCT.
Conclusions
Overall, the results of the current mixed-methods pre-pilot RCT support the feasibility and acceptability of the MBI. Although the current study was not fully statistically powered, the quantitative findings suggest the MBI conferred potential effects among mental health service users compared to the age and gender-stratified TAU inactive controls. These effects facilitated personal recovery, improved trait mindfulness, self-compassion, resilience, mood, quality of life, and general health. The qualitative findings provide in-depth information on MBI participants’ previous and current experiences in MBIs, possible mechanisms of changes in personal recovery related to the MBI, and the motivation and obstacles to adhere to and maintain practices in everyday life during and after the MBI. The results together provide practical implications for informing researchers and practitioners when delivering and developing MBI for people in recovery and refining research methodology when evaluating MBI in RCT.
Footnotes
Author’s Contribution
DC conceived and designed the study, conducted data collection, analysis, and interpretation, and prepared the manuscript. All co-authors (DY, PC, PN, and SH) contributed to subsequent manuscript revisions and approved the final version of the manuscript.
Availability of Data and Materials
Due to this study's sensitive and personal nature, participants were assured that any raw data would remain confidential and would not be accessed openly. Consent was not sought from the participants for data sharing.
Consent for Publication
Consent for publication is not applicable, as information from the individual's data was aggregated and compiled into data summaries. Individual person's data and identifiers are not presented in the current manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Research Ethics Committee (REC) of Hong Kong Baptist University (December 24, 2019). All procedures performed in the study followed the REC guidelines. Informed consent was obtained from all participants in the current study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.