
Abstract
Internet addiction (IA) is typically characterized as the loss of control over one's Internet usage, leading individuals to engage in excessive Internet activities (Young, 2009; Young & De Abreu, 2011), and it has emerged as a pervasive issue of great concern within the global community (Laconi et al., 2014). Specifically, adolescents are more likely to develop IA, due to their proficiency with digital technologies, innate curiosity about the Internet, and a penchant for poor self-control (Al-Kandari & Al-Sejari, 2021; Lei et al., 2018; Zhitomirsky-Geffet & Blau, 2016). However, with the development of digital society, some scholars have found IA also exists among older people who have early access to the internet (Jia et al., 2022; Ozbek & Karas, 2022; Yang et al., 2022). And excessive internet use among older adults was found to have adverse consequences on their physical well-being and overall daily functioning, such as impairing sleep quality (Karaş et al., 2023), leading to high-level social isolation (Meshi et al., 2020).
Based on official statistics, by the end of 2022, the number of Internet users aged 60 and above in China is around 153 million, accounting for 14.3% of the overall number of Internet users (CINIC, 2023); meanwhile, in a survey from China, when smartphones cannot be connected to the network, almost half of the elderly reported to have negative psychological states such as anxiety or uneasiness, which are typical IA withdrawal reactions (Zhu et al., 2018). Considering the magnitude of elder Internet users in China and the proportion of them to have IA symptoms, it is meaningful to explore the problem of IA among the elderly in China.
Several strategies and interventions have been proposed by researchers, healthcare professionals, and social workers to address the issue of IA among the elderly. These include the provision of social support (Jia et al., 2022), enhancement of self-control (Busch et al., 2021; Özdemir et al., 2014), involvement in leisurely pursuits (Jun, 2022), and the reinforcement of digital literacy (Jeong & Bae, 2022). However, we should notice that accurate assessment and screening for IA is the prerequisite of IA prevention and intervention.
The Chen Internet Addiction Scale (CIAS) is a popular and widely used tool for the assessment of IA among the Chinese population (Ko et al., 2019; Nie et al., 2017; Wu et al., 2015). Based on the constructs of impulse control disorder and substance use disorder, Chen et al. (2003) developed the CIAS to assess pathological and addictive Internet use on the basis of this conceptual framework. The revised version, the revised CIAS (CIAS-R) follows the traditional conceptual model of diagnosing addiction disorders, focusing on the psychological and behavioral aspects of addicted college students in Taiwan. CIAS-R can be characterized by IA Core Symptoms (IA-Sym) and Related Problems of IA (IA-RP). IA-Sym comprises Compulsive Use of the Internet (Sym-C), Withdrawal Symptoms of IA (Sym-W), and Tolerance Symptoms of IA (Sym-T). IA-RP consists of Interpersonal and Health-Related (RP-IH) and Time Management Problems (RP-TM). Totally, CIAS-R is composed of five factors and 26-item with good reliability and validity (Mak et al., 2014).
The CIAS-R is the only instrument that is designed for the Chinese population specifically, amidst a multitude of other similar scales. This distinct measurement tool has garnered considerable attention from scholars who have undertaken the task of revising and modifying it to further enhance its efficacy. For example, Bai and Fan (2005) revised this CIAS-R scale in Mainland China, and after modification, 19 items were retained, yielding four factors, namely compulsive use and withdrawal, tolerance, interpersonal and health-related problems, and time management problems. Their results suggested that this scale is an effective approach to evaluating the internet dependence of Mainland Chinese college students, and compared with the original CIAS-R scale, Bai's version combines Sym-C and Sym-W factor into one dimension. Moreover, Ko et al. (2005) determine the ideal cut-off points of the CIAS-R to detect and diagnose IA in community-dwelling teenagers using accepted diagnostic criteria for the disorder. They found that a of 57/58 and 63/64 for the 26-item CIAS-R was used for the two-stage diagnostic and one-stage epidemiological screenings in adolescents (Ko et al., 2005). Additionally, Mak et al. (2014) expanded the application of the CIAS-R in Hong Kong Chinese adolescents and examined whether the CIAS-R's criterion-related validity might be used to explain adolescents’ general health and social functioning. Both Chen's five-factor model and Bai's four-factor model were tested, and the four-factor model was found to have better internal consistency, concurrent validity, and incremental validity in Hong Kong adolescents, suggesting that this scale conformed well to the available data in Hong Kong Chinese adolescents (Mak et al., 2014).
Overall, based on the results of studies on college students in Taiwan and mainland China and adolescents in Hong Kong, the CIAS-R is a reliable measurement tool with a four- or five-factor structure to reflect the core symptoms and related problems of IA in college students and adolescents. Compared to other scales that are dichotomous (i.e., yes or no internet addict), the CIAS-R is more expansive as it can identify the degree of Internet dependence by an individual's performance in interpersonal, health, and time management aspects (Ko et al., 2005; Mak et al., 2014). However, it is yet unknown whether CIAS-R is useful and effective among China's older population, as generations may vary in behaviors regarding Internet use and addictive behaviors (Zhitomirsky-Geffet & Blau, 2016). For example, IA among younger adults is influenced by the fear of missing out, while this is not the case for older adults (Busch et al., 2021). Meanwhile, Karaş et al. (2023) discovered that there is a significant positive relationship between sleep quality and IA among elderly individuals, whilst the impact of this factor on younger individuals remains uncertain. Therefore, the elderly may, therefore, have different patterns and levels of IA than young people (Alhassan et al., 2018). Consequently, it may not be appropriate to use the current CIAS-R scale designed for adolescents to assess IA among the elderly, so modifications of the CIAS-R scale are needed.
The present research aims to adapt the CIAS-R among Chinese older adults and examine its psychometric characteristics, including the factorial structure, internal consistency reliability, measurement invariance (MI), structural invariance (SI) across genders, and criterion validity. Moreover, this research also hopes to investigate whether the modified CIAS-R could distinguish individual's IA severity.
Method
Participants
Participants aged 55 years were recruited via online survey with the help of a Chinese professional market research organization which has built a massive database encompassing a significant portion of the elderly. The elderly individuals were recruited from various provinces and cities within China, encompassing the eastern, central, and western areas. The survey was distributed to the members of the data company by random sampling. Considering the elderly might be incapable of autonomously accomplishing this questionnaire, it is permissible for their offspring to undertake the task on their behalf. Ultimately, 1,117 old people participated in this research, among them, 53.3% were male, and the average age of the sample was 66.39 years (range from 55 to 90 years, SD = 7.1). Seventy-one participants were excluded because they failed the attention test or the cognitive test. A total of 1046 responses were retained for the following analysis, and they were separated into two sets for the following analyses. Sample 1 comprised 647 individuals who only finished the CIAS-R scale, among them 57% were male (Mage = 65.17 years, SD = 7.2). The respondent-to-item ratio was 23.96, which was greatly larger than the traditional criterion (10:1) (Sitgreaves, 1979), so, this sample size was enough to conduct confirmatory factor analysis (CFA). Sample 2 consisted of 399 people (48.9% were male, Mage = 68.26 years, SD = 5.86) who were asked to fill in a package of questionnaires, including the CIAS-R and its relevant constructs which can be used to examine the criterion validity of CIAS-R.
Procedure
Before conducting the formal study, items were revised to suit the condition of the elderly, for example, the item from the initial version was stated as negatively affected work or study (Duan et al., 2013), whilst in our research, this item was revised as “I have been stuck doing other stuff because of IA, such as picking up my grandchildren from school or doing housework”. Both sample 1 and sample 2 were recruited through a survey company, and all of them were elder than 55 years old. Consent was obtained from the participants, and those who finished the survey would be given 5 RMB as a reward. Participants should complete each question before submitting the questionnaire, therefore no missing values were reported.
Measures
The CIAS-R Scale
The CIAS-R was adapted to assess the IA of older adults. The scale consists of 26 items, which are divided into two factors “core symptoms of Internet addiction” and “Internet addiction-related problems” (Chen et al., 2003). The Core Symptoms of the IA subscale include the Compulsive Use of the Internet (Sym-C), Withdrawal Symptoms of IA (Sym-W), and IA Tolerance (Sym-T). The IA-Related Problems subscale includes interpersonal and health-related problems of IA (RP-IH) and Time Management Problems (RP-TM). Respondents completed CIAS-R on a 5-point scale from 1 (did not match my situation at all) to 5 (totally match my situation). Both Chen's five-factor model and Bai's four-factor model were examined in this research (Bai & Fan, 2005; Chen et al., 2003).
Time Spent Online
Time spent online was assessed by the following question “How many hours a day do you spend online or on your smartphone?” (Pawlikowski et al., 2013). We provided horizontal lines for participants to fill in their own answers. The values ranged from 1 to 12.
Loneliness
The ULS-8 Loneliness Scale was adopted to measure the loneliness perceived by the participants (Hays & DiMatteo, 1987). This scale is a simplified version of the UCLA Loneliness Scale (ULS-20). Zhou et al. (2012) tested the reliability of the ULS-8 Loneliness Scale within China with a sample of 839 elderly people from rural communities, and the Cronbach's alpha of the total scale was 0. 741. The ULS-8 Loneliness Scale includes 8 items, and each item represents the frequency of feelings of loneliness. Sample item includes statements like “There is no one I can turn to.” Each item was measured on a five-point scale (1 = never, 5 = daily). The higher the score was, the greater the loneliness people feel. The Cronbach's alpha estimate was acceptable, with a value of 0.84 for the entire scale.
Depression
This study applied the Depression subscale of the Depression Anxiety Stress Scale (DASS-21) to assess depressive symptoms. The Depression subscale includes 7 items (e.g., I felt sad and depressed). Respondents rated on a scale ranging from 1 (did not apply to me at all) to 5 (applied to me very much). Higher mean scores for the Depression subscale indicates higher degrees of perceived depression. The Depression subscale has been widely used in Chinese (Duan et al., 2020). The Depression subscale of DASS revealed good internal consistency with Cronbach's alpha being 0.887.
Data Analysis Strategy
Four models were tested to investigate the factorial structure of CIAS-R, with data from sample 1. Specifically, Model 1 specified five correlated factors according to Chen et al. (2003), of which 26 items were used, and Model 2 was a four-factor model proposed by Bai and Fan (2005), which adopted 19 items. Due to the high inter-factor correlations, the corresponding second-order models were then analyzed. After identifying the best-fitting model of CIAS-R, we evaluated MI across gender by sample 1. Specifically, to investigate the invariance at the item level, MI was examined in four levels from the weaker to the strongest: Configural, metric, scalar, and strict invariance. And when the MI was satisfied, further investigation on whether the invariance could be established at the factor level (e.g., SI) should be conducted (Vandenberg & Lance, 2000). Following previous studies (Mu et al., 2021; Xie et al., 2022), we conducted latent variance-covariance invariance to examine whether variance and covariance of the CIAS-R were invariable across gender. And then, latent mean invariance was analyzed to compare the means of CIAS-R spanning gender. All models were estimated by Mplus 7.4 (Muthén & Muthén, 2017), using robust maximum likelihood (MLR) estimator.
Multiple fit indices were used to evaluate the goodness-of-fit of each model (Jia et al., 2019): Comparative Fit Index (CFI) and Tucker-Lewis index (TLI) with value ≥ 0.90 indicating an appropriate fit; and root mean square error of approximation (RMSEA) with values ≤ 0.08 suggesting an accepted fit of the model to the data (Byrne, 2006; Wang et al., 2022). Moreover, changes in CFI, TLI, and RMSEA (Δ) were also employed to compare the nested models, with the values of ΔCFI and ΔTLI ≤ 0.01, and ΔRMSEA ≤ 0.015 indicating the difference is not significant (Cheung & Rensvold, 2002). In addition, differences between sample-size-adjusted Bayesian Information Criteria (ΔABIC) were also computed, with a value larger than 10 suggest that lower ABIC model could better fit the data (Kuha, 2004). The chi-square test of the model fit was also reported, however, we did not refer these results as it relied heavily on sample size (Cheung & Rensvold, 2002).
As for the reliability of the scale, omega (ω), omega subscale (ωS) and Cronbach's alpha were computed by SPSS 26 (IBM Corp, 2019). To examine the criterion validity of CIAS-R, Pearson correlations between IA (both general and specific factors) and the covariates (i.e., loneliness, depression, and time spent online) were computed. Sample 2 was employed to conduct the aforementioned reliability and criterion validity analyses.
After that, latent profile analysis (LPA) was employed to further examine whether this new CIAS-R could be used to differentiate the severity of IA among the elderly. The whole 1,046 samples were used for this analysis. The MLR estimator was used, and the classifications from two to five profiles were explored. The number of initial stage random starts was set at 200 with the 50 best solutions retained for the final stage of the optimizations. To achieve the best solution for the LPA, several criteria were reviewed: Akaike's Information Criterion (AIC), the Bayesian Information Criterion (BIC), the sample-size adjusted BIC (a-BIC), and the adjusted Lo-Mendell-Rubin likelihood ratio test (aLMR) (Marsh et al., 2009), bootstrap likelihood ration test (BLRT), and the entropy. Meanwhile, sample size of the smallest group was also taken into consideration, which suggests that the smallest group should contain 5% of the sample at least (Ntoumanis & Myers, 2016). Using LPA, different profiles could be distinguished, which would provide a better understanding of the discriminant validity of this scale. Models with lower BIC were regarded to better fit the data. As for LMR and BLRT, when the comparison between models with K profiles and K−1 profiles yielded a p-value greater than 0.05, it suggested the model with K−1 profiles should be selected as the final model. Apart from the LMR and BLRT, entropy was also chosen as a criterion to evaluate the quality of profile membership classification, relating to the accuracy of the model to distribute students into s specific profiles. The entropy value ranges from 0 to 1, with a value closer to 1 indicating better classification (Araújo et al., 2018). However, we should note that no single statistic has been demonstrated to be preferable across every condition (Tein et al., 2013), profile interpretability and uniqueness were also taken into account when deciding the final model (Olivera-Aguilar et al., 2016).
Results
Factor Structure of the CIAS-R
Model 1 and Model 3 were constructed based on Chen et al.'s (Chen et al., 2003) five-factor structure, while Model 2 and Model 4 were based on Bai and Fan's (Bai & Fan, 2005) four-factor structure. Goodness-of-fit indices of the four models were presented in Table 1. No non-significant chi-square test results were found from the proposed models, but for model comparison, we did not rely on this result as the Chi-square test was overly sensitive to sample size. Referring to the values of CFI, TLI, and RMSEA, both Model 1 and Model 3 provided acceptable fit indices. The chi-square test suggested a significant difference between Model 1 and Model 3, Δχ2 = 210.434, Δdf = 5, p < .001. Meanwhile, the values of the AIC and ABIC of Model 1 were lower than Model 3 (ΔAIC = 200.434, ΔABIC = 193.947), indicating Model 1 fit the data better. Thus, the first-order five-factor structure following Chen et al.'s (Chen et al., 2003) research obtained best-fit indices and was used for the following analysis. The standardized factor loadings of Model 1 were shown in Table 2.
Goodness of fit Indices of the Hypothesized CFA Models.
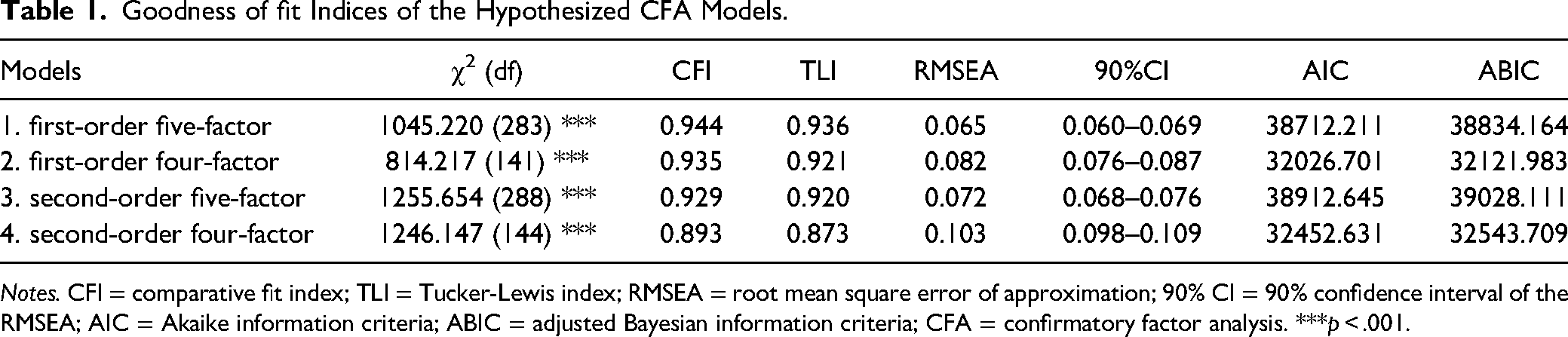
Notes. CFI = comparative fit index; TLI = Tucker-Lewis index; RMSEA = root mean square error of approximation; 90% CI = 90% confidence interval of the RMSEA; AIC = Akaike information criteria; ABIC = adjusted Bayesian information criteria; CFA = confirmatory factor analysis. ***p < .001.
Factor Loadings of Model 1.
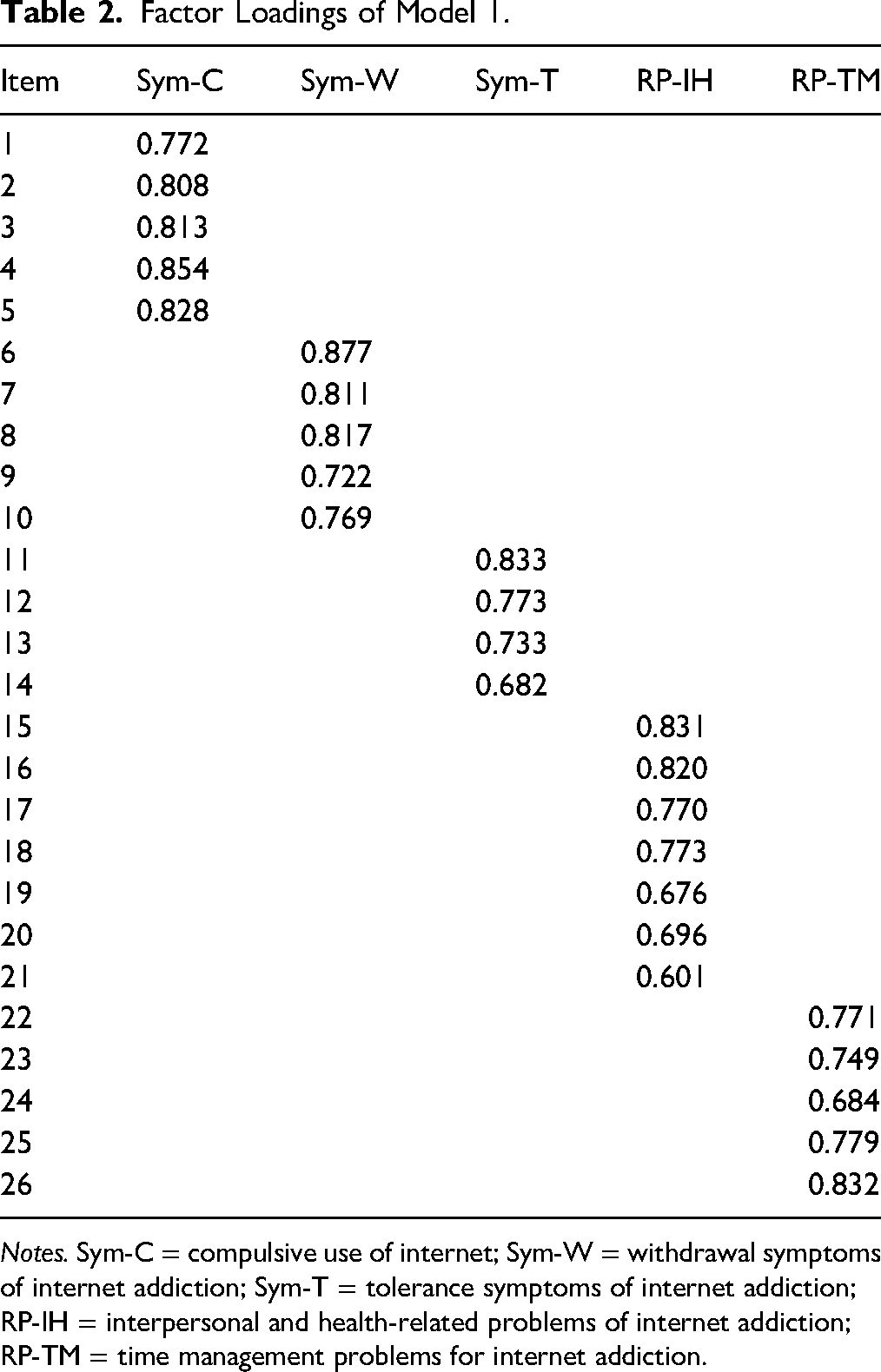
Notes. Sym-C = compulsive use of internet; Sym-W = withdrawal symptoms of internet addiction; Sym-T = tolerance symptoms of internet addiction; RP-IH = interpersonal and health-related problems of internet addiction; RP-TM = time management problems for internet addiction.
Measurement and SI
Multigroup CFA was adopted to examine MI and SI across gender. Following the procedures put forward by previous research (Duan et al., 2012; Jia et al., 2020; Tang et al., 2016), six levels of invariance were tested, from the least strict to the strictest, and male group was set as the reference group. All fit indices are presented in Table 3. At the first four models, the changes in CFI (|ΔCFI| ≤ 0.001), TLI (|ΔTLI| ≤ 0.004), and RMSEA (|ΔRMSEA| ≤ 0.002) were all insignificant, therefore MI was supported. For the latent variance-covariance invariance model test, the changes were also insignificant, with the values of |ΔCFI|, |ΔTLI| and |ΔRMSEA| that were all less than 0.003. When we exerted equity constraint on latent means between male and female group, the results suggested negligible changes in CFI (|ΔCFI| = 0.001), TLI (|ΔTLI| = 0.004), and RMSEA (|ΔRMSEA| = 0.001). Thus, SI was demonstrated.
Measurement and Structural Invariance
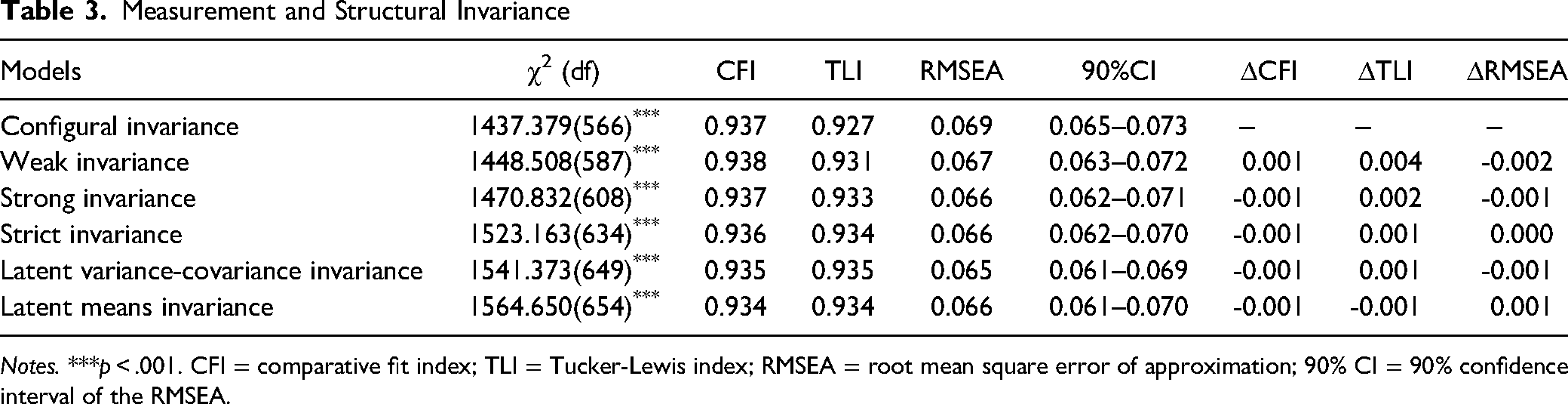
Notes. ***p < .001. CFI = comparative fit index; TLI = Tucker-Lewis index; RMSEA = root mean square error of approximation; 90% CI = 90% confidence interval of the RMSEA.
Reliability Tests
Sample 1 was employed to calculate reliability indices. As shown in Table 4, the total CIAS-R and its five subscales performed excellent on Cronbach's alpha, ranging from 0.87 to 0.97. A lot of researchers criticized that Cronbach's alpha is less reliable, so model-based omega coefficients are needed for further reliability investigation (Dunn et al., 2014). The omega for the total scale was 0.97, which indicates that 97% of the variance in item responding could be ascribed to the factors, and only 3% of the variance was because of errors. Omegas for each dimension were also calculated: omega for Compulsive Use of the Internet (Sym-C) was 0.94, omega for Withdrawal Symptoms of IA (Sym-W) was 0.93, omega for Tolerance Symptoms of IA was 0.91 (Sym-T), omega for Interpersonal and Health-Related Problems of IA (RP-IH) was 0.92, and Time Management Problems for IA (RP-TM) was 0.91.
Reliability Indices of the CIAS-R.
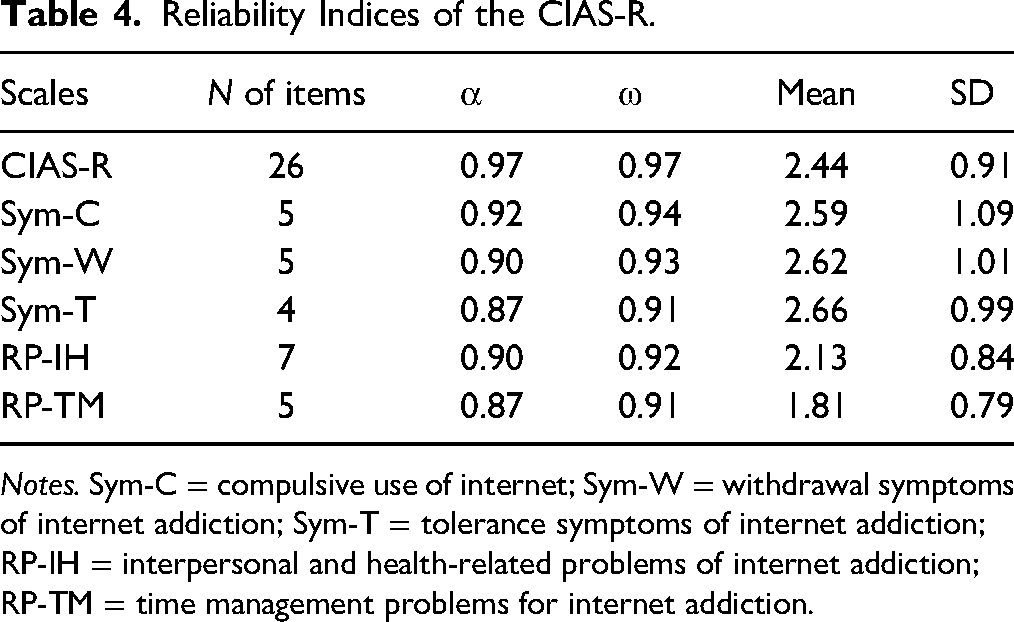
Notes. Sym-C = compulsive use of internet; Sym-W = withdrawal symptoms of internet addiction; Sym-T = tolerance symptoms of internet addiction; RP-IH = interpersonal and health-related problems of internet addiction; RP-TM = time management problems for internet addiction.
Criterion Validity
Criterion validity was examined through the correlations between CIAS-R factors and three relevant constructs (see Table 5). During this process, sample 2 was used for analysis. Correlation matrix showed that the associations between total scores of CIAS, its five sub-dimensions, and the three selected constructs (e.g., time spent online, sense of loneliness, and depression) were significantly positive. Consequently, the CIAS-R had good criterion validity.
Criterion Validity Tests.
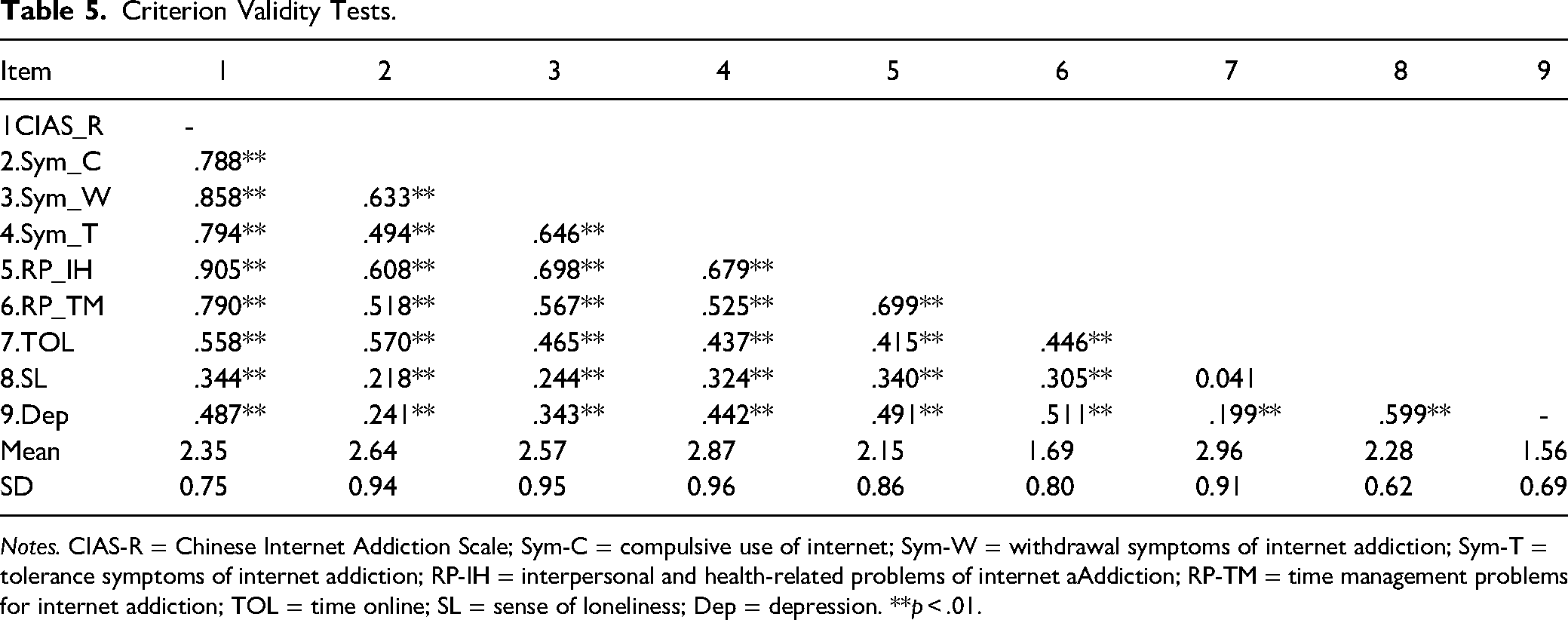
Notes. CIAS-R = Chinese Internet Addiction Scale; Sym-C = compulsive use of internet; Sym-W = withdrawal symptoms of internet addiction; Sym-T = tolerance symptoms of internet addiction; RP-IH = interpersonal and health-related problems of internet aAddiction; RP-TM = time management problems for internet addiction; TOL = time online; SL = sense of loneliness; Dep = depression. **p < .01.
Latent Profile Analysis
Table 6 presents the results of LPA. The value of AIC, BIC, and ABIC tends to decrease as the number of profiles increases. Among the six solutions, all the models have an entropy value greater than 0.8; and the five to seven profile's p value of the LMR for K compared with K-1 group was not significant, suggesting a K-1 profile might be more suitable to describe the data; moreover, the p value of the BLRT was statistically significant in all the models tested. Based on the entropy, LMR value, and taking the cases of the smallest group into consideration, a four-group solution was considered the most reasonable.
Latent Profile fit Statistics for Models Based on Five Dimensions of CIAS-R.
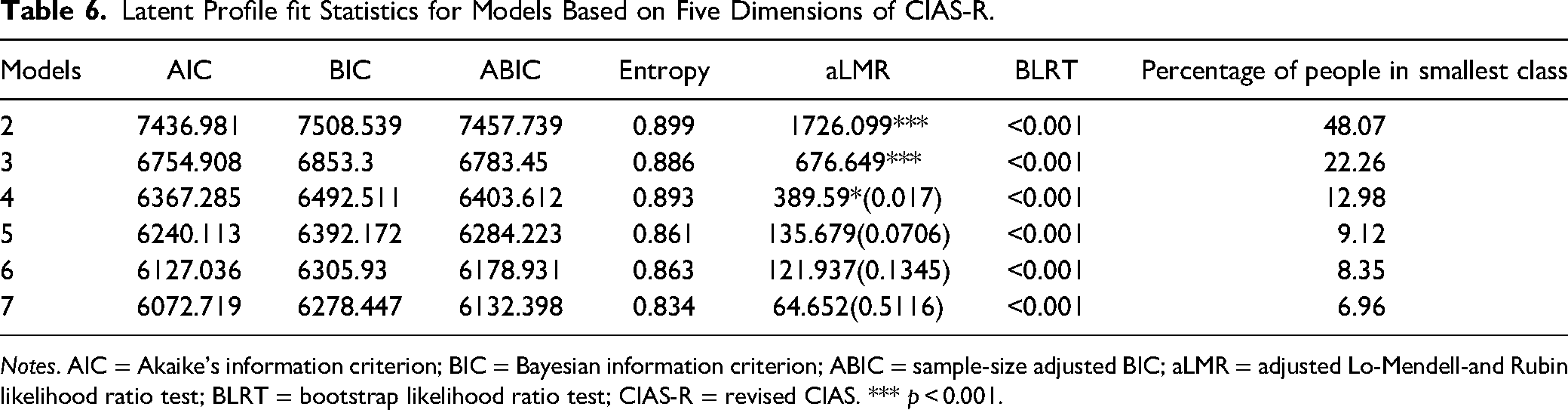
Notes. AIC = Akaike's information criterion; BIC = Bayesian information criterion; ABIC = sample-size adjusted BIC; aLMR = adjusted Lo-Mendell-and Rubin likelihood ratio test; BLRT = bootstrap likelihood ratio test; CIAS-R = revised CIAS. *** p < 0.001.
The patterns of the four profiles are shown in Figure 1. Profile 1 makes up 35.86% of the sample and is described as (the less IA). Profile 2 is consisted of 31.69% of the sample, and is characterized as (the more internet addicted). For profile 3, this type is named as (the least IA), which occupies 19.47% of the total sample. With regard to profile 4, 12.98% of the sample belongs to this type, which is regarded as (the most internet addicted).
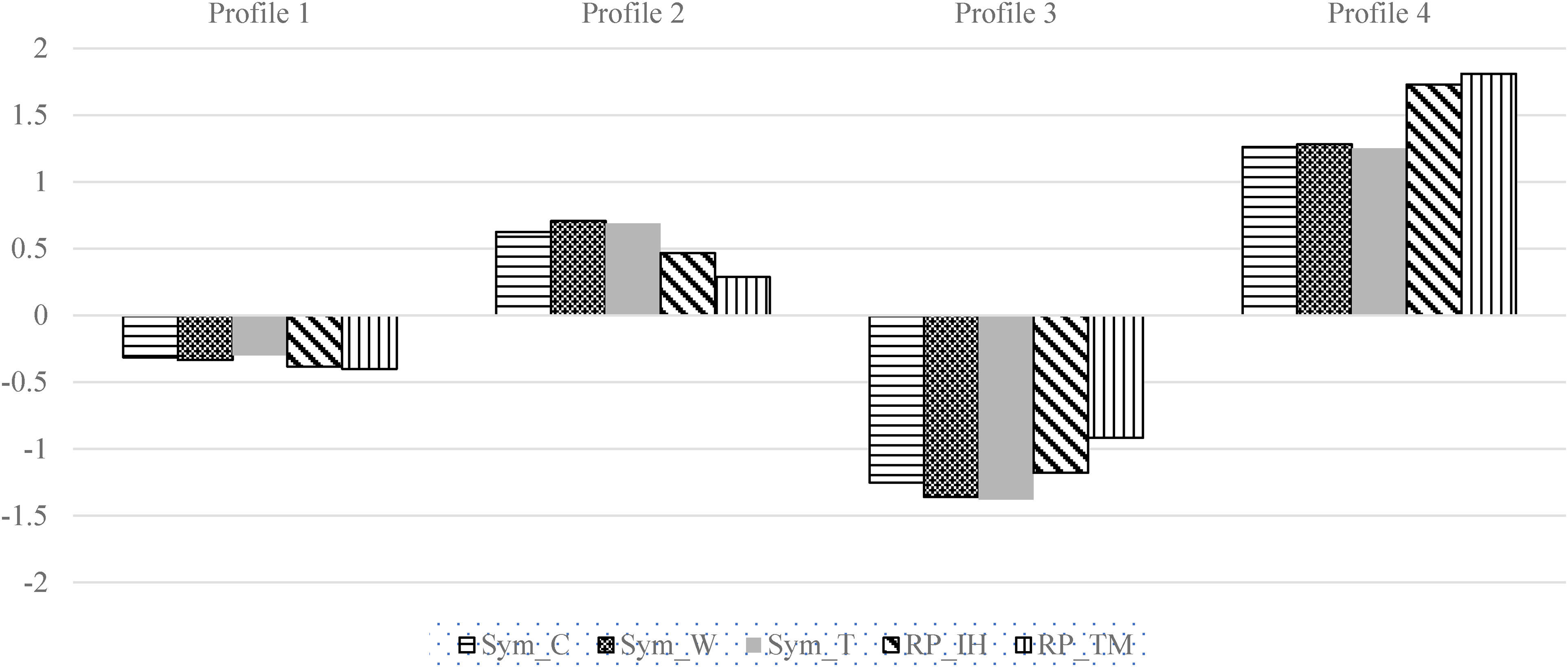
Characteristics of the latent profiles. Notes
The descriptive statistics of the four profiles are shown in Table 7. Profiles 1 and 3 are two groups that reported less IA behaviors, with negative mean scores on the five dimensions of CIAS-R. To be more specific, elders in profile 3 have the least IA symptoms and caused problems, suggesting the healthiest internet usage behavior. Elder people in profile 1 marks the second least in IA behaviors, with scores on all five dimensions below average. Elder people in profile 2 and profile 4 are regarded as IA users, with all scores higher than 0. Compared with profile 2, people in profile 4 are the most addicted internet users, who have the highest scores on all five dimensions. Post hoc analyses suggest that score differences between those four profiles are all significant, with p values all significantly different from zero.
Cluster Means of the Four Profiles Solution of the LPA.
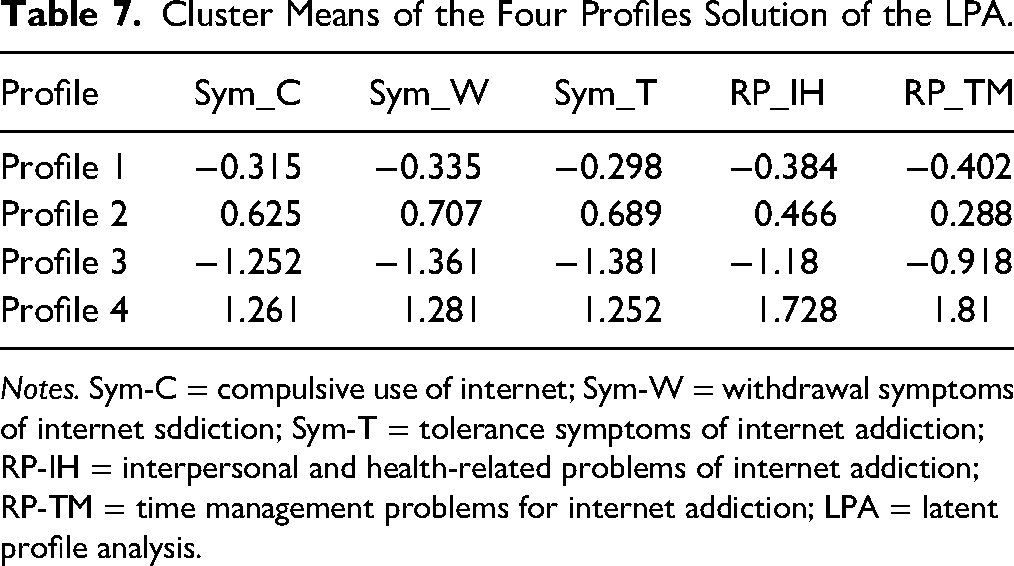
Notes. Sym-C = compulsive use of internet; Sym-W = withdrawal symptoms of internet sddiction; Sym-T = tolerance symptoms of internet addiction; RP-IH = interpersonal and health-related problems of internet addiction; RP-TM = time management problems for internet addiction; LPA = latent profile analysis.
Discussion
A myriad of researchers have developed their own instruments or revised the existing scales to assess IA behaviors deriving from various conceptual frameworks. However, all of them are either Western culture-based scales or examined among college students in China. In light of the increasing prevalence of Internet usage among the Chinese elderly, it is imperative to develop an effective assessment to identify individuals who are susceptible to or already experiencing problematic behaviors. Though there is no available IA scale for older people in China, Chen et al. (2003) designed a scale that can both reflect the core addiction symptoms and health-related problems for internet users, and this scale had been examined widely in Chinese culture, spanning various locations in China (e.g., Hongkong and Mainland China) and population (e.g., college students and adolescents). Given this is the first Chinese culture-based IA scale and its good reliability and validity records, our research revised this CIAS-R scale, so that the items were modified more in accordance with the real situation of the elderly, and then analyzed the psychometric characteristics of CIAS-R in the elderly group.
First, we examined the factorial structure of CIAS-R by setting four alternative models according to Chen et al.'s and Bai and Fan's research (Bai & Fan, 2005; Chen et al., 2003), of which two were first-order models and the others were their corresponding second-order models. By comparing the values of CFI, TLI, RMSEA, AIC, ABIC, and the changes of these indices between models, Model 1 was found to obtain best-fit indices, suggesting the five correlated first-order factors can reflect IA conditions among the elderly effectively, specifically, IA of elder people can be assessed through their Compulsive Use of Internet, Withdrawal Symptoms, Tolerance Symptoms, Interpersonal and Health-Related Problems, and Time Management Problems for IA. The omega values and Cronbach's alpha of the whole scale and its subscales showed excellent internal consistency reliability.
Second, after identifying the best-fit model, we furthered the analysis of the chosen model for MI and SI tests. Our results confirmed full MI of the CIAS-R across genders, implying that the constructs of CIAS-R work similarly in male and female groups, so males and females can both understand the items of CIAS-R effectively, and the obvious disparities in CIAS-R scores across genders can be attributed to the real situation of people's IA, not because they are males or females. The results of SI analysis also suggested that the CIAS-R factors do not have significant gender differences.
Third, correlation analysis between CIAS-R, time spent online (Ko et al., 2009), sense of loneliness, and depression provided evidence for the criterion validity of this scale. The results showed that the total score of CIAS-R was significantly related to the three selected criteria, and the direction was positive as expected. Similar results were discovered on the associations between the five specific factors of CIAS-R (e.g., Compulsive Use of the Internet, Withdrawal Symptoms, Tolerance Symptoms, Interpersonal and Health-Related Problems, and Time Management Problems for IA) and the three selected covariates. The magnitude of the correlation coefficients indicated that IA behaviors may lead to psychological problems, alerting us to pay attention to the mental health of the elderly.
Implications for Social Work Practice
Given the constant evolution of IA among senior adults, the choice of the assessment tool has important implications in both clinical and research settings (Laconi et al., 2014). Diagnosing the symptoms and knowing the extent of IA in older adults are the basis for clinicians and social workers to adopt suitable therapies, which could in turn promoting the elderly's well-being and reducing psychological distress, such as depression and anxiety. Young (1999) suggested that setting goals, abstinence, reminder cards, personal inventory, support groups, and family therapy are effective interventions for treating IA behaviors. The aforementioned intervention programs could be selected and implemented based on symptoms and extent of IA. For example, the elderly who have left their hometown and followed their children to settle in an unfamiliar city, are usually struggling with social integration due to the disruption of original social ties. And for them, the Internet has become a key leisure activity, making up for the lack of offline social support, while excessive Internet usage is more likely to cause Internet dependence and addiction (Kanat, 2019; Khalaila & Vitman-Schorr, 2018; Wegmann et al., 2015). For such type of IA users, community and social workers could adopt interventions like establishing support groups and family therapy to limit their time on Internet use.
At the community and society level, IA should be considered in policy discussions because it is more relevant to the core orientation of digital society and production aging. Encouraging and facilitating older people to actively participate in digital life is of utmost importance for the development of a digital society and an actively aging society. However, we should also anticipate the issue of IA among the elderly due to insufficient digital literacy. As a result, programs and measures for the prevention, measurement, and intervention of IA among the elderly should be incorporated into the digital society development planning as early as possible. Our scale provides a useful approach to the assessment of IA among the older population, and the dissemination of effective treatment and prevention interventions that are lacking to date. This is a benefit for the community and social workers to be able to carry out prevention and intervention work on the elderly's IA scientifically.
IA may lead to many psychological and physical issues (Alhassan et al., 2018; Bertocchi et al., 2022; Karaş et al., 2023). No mental illness does not mean mental health, and achieving mental health should simultaneously seek to prevent IA and strive to enhance self-control on Internet use. Therefore, in practice, this study will help social workers shape the new perception of Internet access among the elderly, and incorporate the instrument into evaluating the effectiveness of social work programs in the intervention of IA, which is the evidence-based practice needed in Chinese social work practice (Tang et al., 2016).
In addition, this study found that individuals of advanced age, who spent more time with the Internet, are likely to experience a decline in offline social interactions and social support from their offline community. Consequently, this may result in a reduced inclination to engage in face-to-face interactions and an elevated interest in engaging with the Internet, which finally leads to IA issues (Jia et al., 2022). An increasing number of elderly individuals experience feelings of loneliness and depression as a result of not having the companionship of children, a prevalent negative emotion in their later years. To alleviate their psychological stress, surfing the Internet has emerged as a vital means for them. However, it is important to note that the more time they spend engaged in online activities, the higher possibility of developing addiction to the Internet (Kim, 2018; Mahapatra, 2019). Therefore, it is imperative for clinicians and social workers to be attentive to the adverse emotional experiences encountered by older individuals, including feelings of loneliness and depression. This attentiveness is crucial in facilitating their access to offline support systems, thereby mitigating the risk of prolonged reliance on the Internet for emotional solace.
Limitations and Future Research
The present research also has some limitations that need to be addressed. First, though our findings provided evidence to support the use of this scale in elder people, the samples were chosen from urban areas, which may decrease the representativeness of the sample, and the MI and structure invariance across area distribution (e.g., rural and urban) should also be examined. Second, this research did not examine the test-retest reliability, which is essential for obtaining a stable construct of the scale. Third, measures for criterion validity tests were procured by self-report, which may bring about common method variance. To avoid this bias, more sources or methods should be adopted to collect data.
Conclusion
In conclusion, our findings suggested that the five correlated first-order factors model could best explain the underlying structure of the CIAS-R among the elderly. The results of MI analyses indicated that males and females can share a common understanding of this scale, and the differences in the CIAS-R scale can be attributed to the severity of an individual's real internet use behaviors, instead of the influence of gender. The correlations with the covariates supported the criterion validity of this scale. Consequently, our findings demonstrated that the CIAS-R is a reliable IA measurement that can be applied to Chinese elder people. Furthermore, this scale can provide an evaluation for the elderly's IA behaviors and be a solid foundation for future elderly-internet-addiction-related research.
Footnotes
Acknowledgments
The authors are grateful to all the participants who participated in the questionnaires.
Author contributions
The first author designed and conducted the research, analyzed the data, and contributed to writing the manuscript. The second author and the third author contributed to conducting the research, analyzing the data, and writing and revising the manuscript. The fourth author and the fifth author contributed to data curation, methodology, review, and editing.
Author Note
Tianyuan Liu is now at the School of Sociology, Wuhan University. Yu Jia and Wenlong Mu are now at the School of Journalism and Communication, Wuhan University. Yang Yang is now at the School of Marxism, Wuhan University. Jinglu Yan is now at the Institute for Social Science Research, The University of Queensland.
Data Availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
This study was approved by the School of Sociology, Wuhan University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. This work is supported by the National Natural Science Foundation of China [72102170;72172107], the National Social Science Found of China [22CSH035] and Independent Research Project of Wuhan University [2021XWZY009].
Informed Consent
Informed consent was obtained from all individual participants included in the study.