
Abstract
Keywords
Since its inception in 2014, the behavioral health workforce education and training (BHWET) program has provided specialized training and stipend support to nearly 40,000 mental health professionals, including more than 10,000 Master of Social Work (MSW) students in the United States (National Center for Health Workforce Analysis, 2023). Given that each trainee received a $10,000 stipend, this translates to more than $100 million in support for social work students nationwide. BHWET-funded programs are mandated to collect and report performance data, including a one-year postgraduation follow-up requirement. The current study sought to understand long-term workforce outcomes for social workers as the BHWET program ended its first decade to get a sense of whether social work programs meet the goals of the professional training program. This is relevant for two reasons. First, it is valuable to understand how tailored training and student funding shape professional trajectories among social workers after graduation. Second, it is important for social work educators to gather evidence of program outcomes and inform future opportunities to support social work training in behavioral health.
The Behavioral Health Workforce Crisis
Over the past 25 years, a growing number of practitioners, policy makers, and researchers have identified an emerging behavioral health workforce crisis (Hoge & Paris, 2018; Hoge et al., 2013, 2019; Hyde, 2013; Interlandi, 2023; Lin et al., 2016; National Academies of Sciences, 2025; Olfson, 2016; Ward, 2022). Problems within the behavioral health workforce encompass four main elements. There are not enough providers to meet the demand for services (National Center for Workforce Analysis, 2024). There is a geographic misalignment with too many providers in some areas and not enough in other communities, especially rural communities (National Center for Workforce Analysis, 2024). The workforce also has a quality problem, with too few providers prepared to implement evidence-based practices with fidelity and respond to changes in the context of practice (e.g., telehealth) (National Academies of Sciences, 2025) as well as changing demographics (e.g., population aging) of those served (Hoge et al., 2013). The demographic makeup of the behavioral health field, being overwhelmingly White, also fails to match the diversity of individuals who seek help, which may contribute to behavioral health inequities (Fischer et al., 2024; Shim & Alegría, 2025). In 2021, the Health Resources Services Administration (HRSA) identified increasing the “diversity, inclusion, and representation in the health professions” as an objective in their health workforce strategic plan (U.S. Department of Health and Human Services, 2021).
BHWET: A National Workforce Initiative
BHWET is a decade-long federal grant program designed to address the behavioral health workforce crisis. Its expressed goal is developing and expanding the workforce, and it has a special emphasis on working in underserved communities (Kepley & Streeter, 2018; National Center for Health Workforce Analysis, 2019, 2023). The BHWET initiative was launched in the aftermath of the Sandy Hook tragedy, when the Obama administration made the commitment to train 5,000 mental health providers to practice with youth and emerging age adults (The White House, January 16, 2013).
BHWET was developed and is administered by HRSA through the Bureau of Health Workforce. BHWET includes two complementary support mechanisms, one for health professionals (BHWET Pro), which has included a range of professional degrees, and one for paraprofessionals (Afayee, 2023). BHWET Pro has funded professional disciplines including psychology, nursing, marital and family counseling, and psychiatry, but social work students have received more than 60% of the traineeships from 2014 to 2022 (National Center for Health Workforce Analysis, 2023). Since an initial grant cycle from 2014 to 2017, the BHWET mechanism was reissued from 2017 to 2021, expanding to prepare social workers to serve populations across the lifespan, and again from 2021 to 2025, retaining a focus on children, adolescents, and transition-age youth at risk for behavioral health disorders.
The core elements of the BHWET Pro program were $10,000 in stipend support during the advanced year of social work education, a requirement of a signed commitment letter agreeing to work in behavioral health within “high need and high demand areas” (e.g., medically underserved communities), and a practicum placement in the advanced year in behavioral health. These programs have had a broad emphasis on training in (or preparing students for) behavioral health integration, interprofessional team-based care, youth and young adults, and work in underserved settings. The content and structure of specialized training for BHWET vary by grantee, program discipline(s), and other program-specific factors (e.g., online vs. in-person) as grantees have adapted their programs to operate within their own educational and geographic context.
Evaluating Social Work BHWET Programs: Three Grantees
The three specific programs evaluated in this study include one in a Mid-Atlantic state, one in the Midwest shared between two social work programs, and one in a Plains state. These programs operated independently but have coordinated data collection and program planning efforts as part of a consortium of social work grantees. As noted, all three programs adhered to the core elements noted above and developed a specialized curriculum for trainees that varied by site. Students at the Mid-Atlantic site were required to take two clinical methods courses (e.g., cognitive behavioral therapy), attend six monthly seminars focused on specialized topics in behavioral health (e.g., health integration), participate in an interprofessional education experience, and take a telebehavioral health course. At the Midwest site, two universities collaborated to create a single fellowship program. Students’ practicum placements included health care sites that collaborated with the higher education institutions. They were required to take part in two integrated health seminars at one institution, and at the other institution, a conference and a webinar were held annually. At the Plains site, students completed a capstone project and took part in monthly value-added training in integrated care; their practicums had an interprofessional emphasis as well.
While including multiple sites in differing geographic contexts, the current study focuses on three BHWET programs but does not capture the workforce needs and demographically diverse regions the national BHWET program serves. For example, regions of the US with a high proportion of designated mental health-health professional shortage areas (MH-HPSAs) and medically underserved areas (MUAs) have higher unemployment and lower educational attainment compared with regions with fewer designated MH-HPSAs and MUAs (Holden et al., 2026). The programs under study did not operate in southern or western states, where the employment (U.S. Bureau of Labor Statistics, 2025) and education attainment (McElrath, 2025) differ from the study sites, which can impact the opportunities and likelihood of students graduating from these programs to be employed in underserved areas. Similarly, any exploration of the diversity of the workforce is influenced by regional differences (U.S. Census Bureau, 2026) that the current study is unable to account for fully.
In early 2024, the programs agreed to collaborate on a shared evaluation with the following aims: (1) assessing the persistence of BHWET program alumni in the field of social work including a focus on successful licensure, (2) assessing the extent to which graduates practice in areas of highest need, (3) understanding the practice context of BHWET graduates’ work with a broad goal of understanding the outcomes of BHWET in social work education and practice.
Method
Sample
To explore long-term BHWET employment outcomes, each of the three grantees (Mid-Atlantic, Midwest, and Plains) utilized a shared online (i.e., Qualtrics) survey. The survey was sent electronically to all BHWET program graduates via the most recent contact information collected by each program prior to graduation and as part of the one-year outcome reporting required by HRSA. Additionally, extensive efforts were made via social media and internet searches to obtain active email addresses for each graduate. The survey was active for 60 days, with a dedicated link for each respondent. Those who filled out the survey could choose to receive a $10 gift card. Each of the three programs received Institutional Review Board approval locally, and data were anonymized and then pooled for analysis.
The overall response rate was 62%, with 863 invitations sent and a total of 537 responses; the response rate varied somewhat, with a 45% rate for the Midwest site and 71% for the other two sites. Survey respondents were overwhelmingly female (88.2%) and approximately two-thirds self-identified as White (see Table 1). The average age of alumni was 35 (SD = 8.1). By site, respondents were roughly divided into thirds, with slightly larger percentages in the Mid-Atlantic (40.6%) and Plains (35.0%), and slightly lower (24.4%) at the Midwest site. Cohort/year of graduation was well distributed across academic years, except for the 2014–2015 year, when grantees were first developing their programs. A large majority of alumni were practicing social workers (94%) and licensed (90%). Among graduates who provided a work address, 40.6% practiced in an MUA, 52.8% in a geographically defined MH-HPSA, 57.9% in a geographically defined primary care-health professions shortage area (PC-HPSA), and 19.2% in a rural area. Combining MUA, MH-HPSA, and PC-HPSA, 74% of graduates practiced in high-need areas.
Sample Description (N = 537).
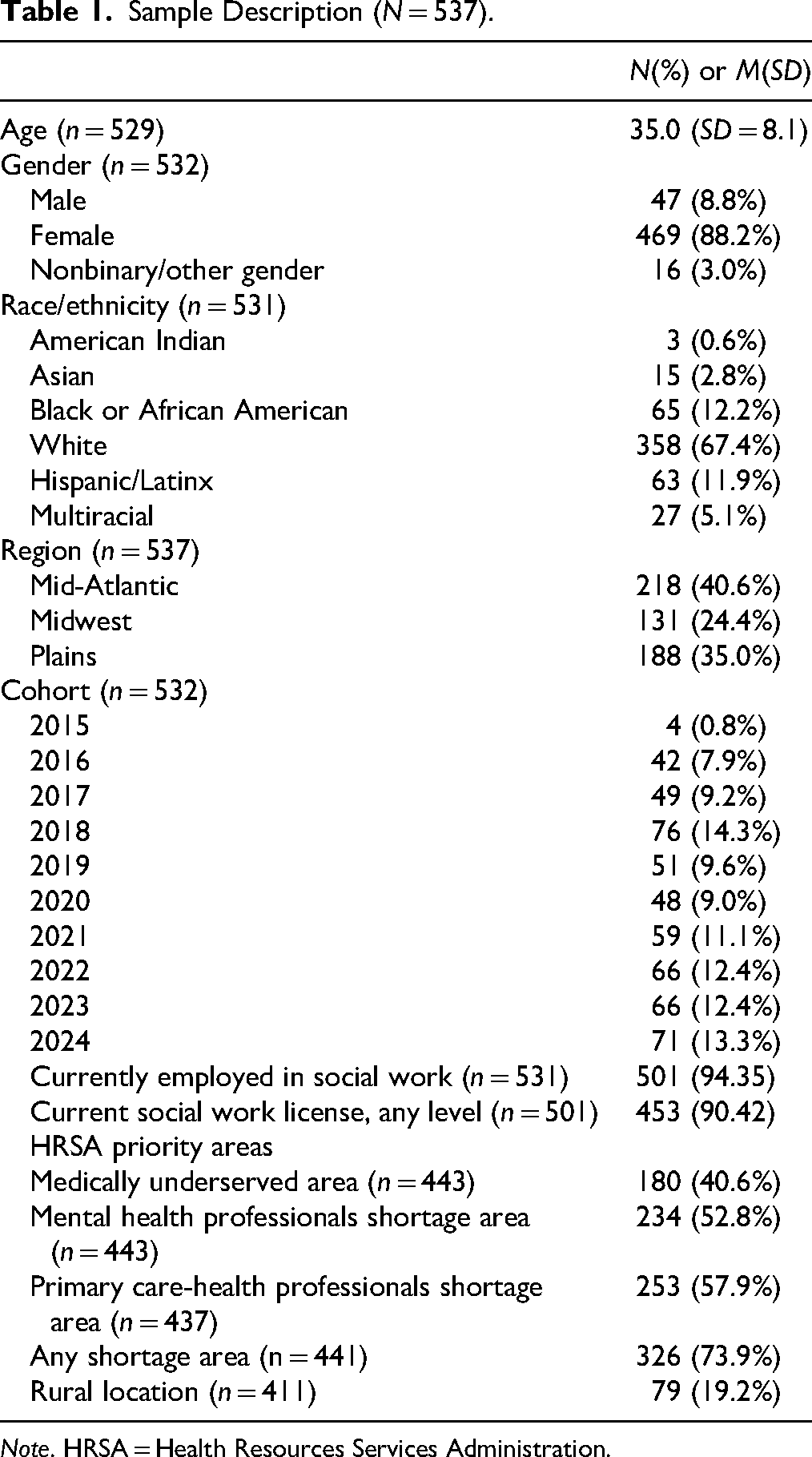
Note. HRSA = Health Resources Services Administration.
Measures
The survey collected sociodemographic information, including age, gender, and race/ethnicity. Alumni provided their traineeship year (equivalent to year of graduation) and were asked a range of questions about postgraduation employment, including: whether they were currently employed in the social work profession; whether they were seeking work in the field; how long they had been in their current position; and their work address. Work addresses of those currently employed in social work were entered into HRSA's Shortage Area Batch Processing tool (Health Resources and Services Administration, n.d.) to determine whether former students were employed within an MUA, MH-HPSA, PC-HPSA, and rural locality (Health Resources and Services Administration, n.d.–a). An omnibus variable of “shortage area” was created if an alum worked in an MUA, MH-HPSA, or PC-HPSA. Work addresses were also entered into HRSA's Rural Health Grants Eligibility Analyzer tool to identify rural employment (Health Resources and Services Administration, n.d.–b).
Alumni also provided information about whether they possessed a social work license at the clinical level, MSW level, or Bachelor of Social Work (BSW) level, and were asked about their annual income from their job in 2023, with options in $20,000 increments from $0 to $200,000+ (11 categories). To assess the utilization of teletherapy in practice, respondents reported the percentage of time they provided services electronically (never, 1%–25%, 26%–50%, 51%–75%, 76%–99%, 100%, and not applicable).
Using categories developed by the Social Work Census (Kim, 2025), respondents reported on the type of setting where they practiced (e.g., “elementary or secondary school” and “home health care agency”) and the population groups (among 17 options) mainly served by their current job. Respondents were allowed to choose as many as applied to their service setting. Similarly, they reported on the functions of their agency, such as “substance use/addiction services” and “mental/behavioral health” (among 24 options).
Analyses
For Aims 1 and 2 (persistence and high-need practice), chi-square analysis assessed differences in social work career status, licensure, and practice in a geographic shortage area based on race/ethnicity, gender, and age. Given the need to diversify the behavioral health workforce (Fischer et al., 2024; Shim & Alegría, 2025) and considering ongoing concerns about differential licensure pass rates (Kim, 2022; Kim & Joo, 2025; Senreich & Dale, 2021), this study sought to assess disparities in professional outcomes. Two multivariable logistic regressions were conducted to further assess demographic correlates of social work professional status (i.e., working as a social worker) and practicing in a geographic shortage area. To address missing data on independent and dependent variables, multiple imputation with chained equations was used to create 20 imputed datasets using Stata (Royston & White, 2011).
For the third aim of the study, latent class analysis (LCA) was used to derive distinct subpopulations or classes of social work practice. LCA is a form of so-called “person-centered” analysis that clusters cases, in this case, individual BHWET alumni, into relatively homogeneous groups from a heterogeneous sample (Rosato & Baer, 2012). The classes themselves are latent or unobserved but are drawn from a series of dichotomous manifest variables (Lanza & Rhoades, 2013). This approach has been used in other studies to understand the diversity in practice roles (Lombardi et al., 2021) and educational pathways in social work (Jensen et al., 2025).
Eighteen latent class indicators were used in the analysis. They included the following: working in a (1) MUA, (2) MH-HPSA, (3) PC-HPSA, (4) rural locality, working with (5) low-income persons, (6) non-English speaking persons, (7) youth, (8) adults, (9) older adults, practicing in (10) mental health settings, (11) health, (12) homelessness, (13) family and child, (14) addictions, and (15) working 50% or more in telehealth capacity, (16) government sector employment, (17) for-profit employment, and (18) self-employed. We used nested model testing (i.e., 1-class, 2-class, etc.) to determine the optimal number of classes by evaluating the lowest values on information criteria, the Vuong–Lo–Mendell–Rubin (VLMR) test (Lo et al., 2001) and Bootstrapped Likelihood Ratio Test (McLachlan & Peel, 2000), and model entropy (Celeux & Soromenho, 1996; Nylund et al., 2007). After the classification model was determined, covariates were added to the model to explore correlates of latent class using a three-step approach, as this technique preserves class assignment (Vermunt, 2010). Covariates included African American/Black race, Latinx ethnicity, age, program site, number of years postgraduation, and income. Full information maximum likelihood addressed missingness in the classification model with listwise deletion for model covariates. Mplus (Muthén & Muthén, 1998–2024) was used for latent class models.
Results
Aim 1 and Aim 2 Results
In Table 2, bivariate results for working in the social work profession were nonsignificant for race, gender, and age, and there were no significant differences in licensure rates by race, gender, and age. There were significant differences in the percentage of alumni practicing in high-need areas by racial group, with slightly lower percentages of Asian (57%) and African American (55%) practicing in high-need areas compared with other racial groups (∼75%–80%).
Social Work Career Outcomes by Sociodemographic Characteristics.
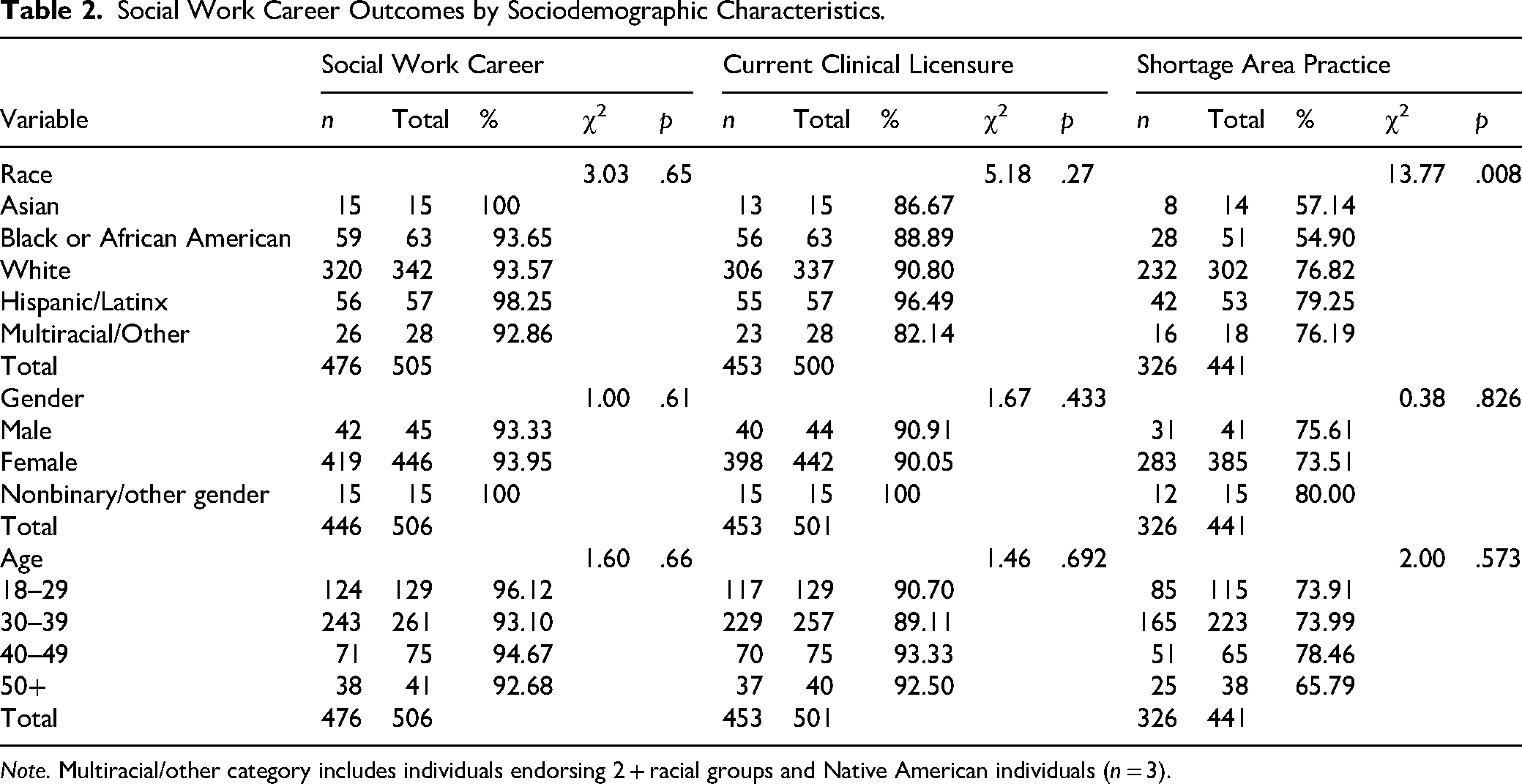
Note. Multiracial/other category includes individuals endorsing 2 + racial groups and Native American individuals (n = 3).
Multivariable models were estimated, adjusting for potential confounders. A logistic regression predicting social work practice (not shown) was nonsignificant for race, gender, age, region (site), and years since graduation. A second logistic regression model (Table 3) was estimated, including race, gender, age, region (site), years since graduation, tenure in current position, income, employer type, and licensure status. Significant differences were identified by race, region (site), and employer type. African American graduates were less likely to work in geographically defined shortage areas (ORadj = 0.44; p = .01). Midwest (ORadj = 2.51; p = .005), and Plains graduates (ORadj = 2.61; p = .01) had more than twice the odds of being employed in a high-need area compared with Mid-Atlantic graduates. Individuals employed at private, for-profit organizations had lower odds of being employed in a high-need area (ORadj = 0.37; p = .001) compared with alumni working in private nonprofit organizations.
Logistic Regression Predicting the Likelihood of Working in a Shortage Area (n = 497).
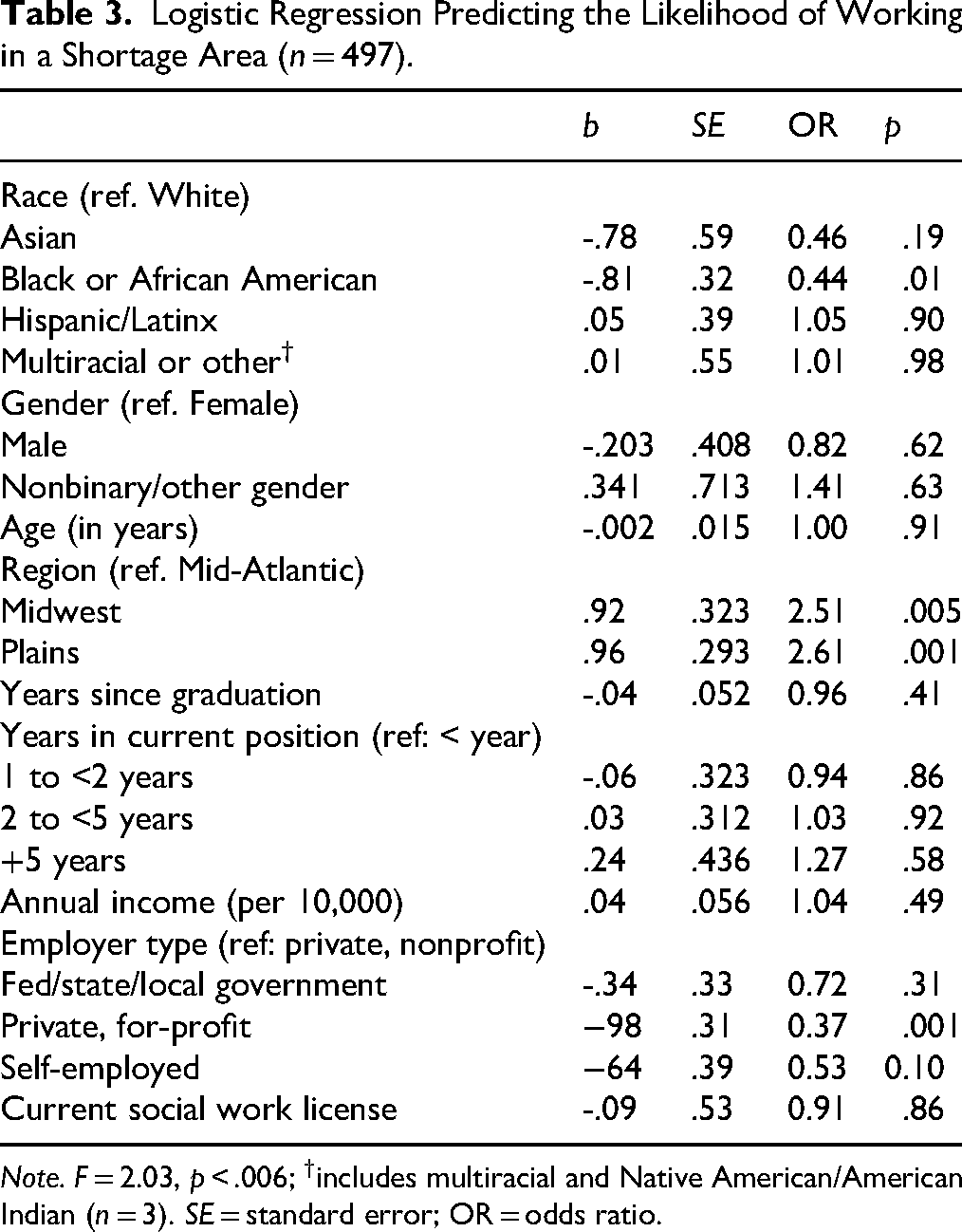
Note. F = 2.03, p < .006; †includes multiracial and Native American/American Indian (n = 3). SE = standard error; OR = odds ratio.
Aim 3 Results
Latent class analyses estimated models between one- and eight-class models. Based on VLMR tests, a four-class model was optimal, as a five-class model was not significantly improved in fit over the four-class model. Model entropy was marginally acceptable at 0.80 (Celeux & Soromenho, 1996). Notably, some logit thresholds were fixed for stable model estimation, suggesting probabilities approaching zero or one. The four classes (see Figure 1) were named as follows, with sample percentages: Class 1: Private Practice (14%), Class 2: Low Need/For Profit (20%), Class 3: High Need/Rural (41%), and Class 4: Youth Serving (26%).
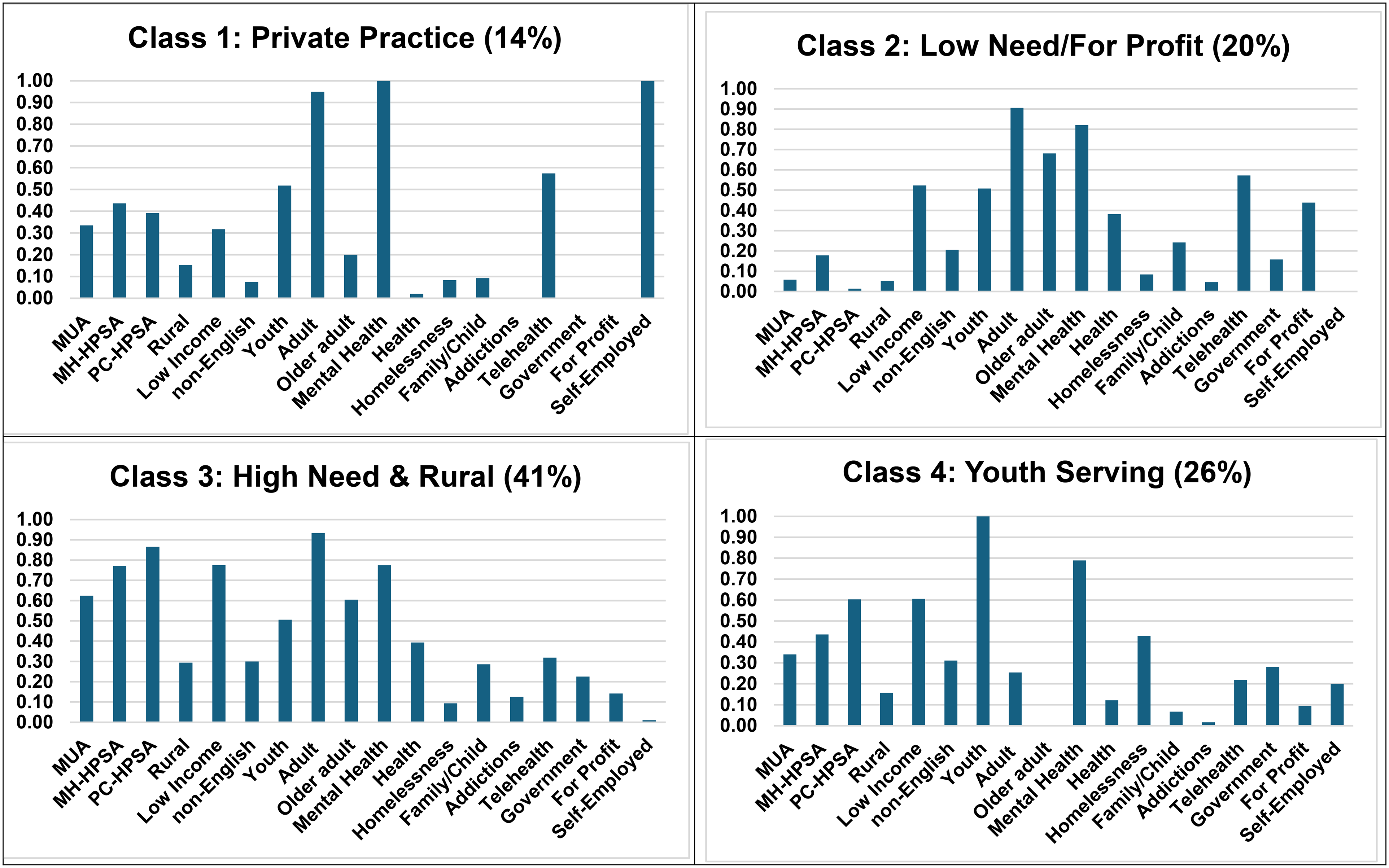
Classes of social work practice (n = 501). Note. Entropy = 0.80; percentages based on most likely class status; Y-axis denotes item probability.
Class 1, named “Private Practice” (14%) was distinct for extremely high probabilities of self-employment (∼1), working in mental health (∼1), and working with adults (.95). The second class, Class 2, which we titled, “Low Need/For Profit” had the highest probability of for-profit employment (.44) and the lowest probabilities of working in HRSA-designated high-need areas including MUA (.06), MH-HPSA (.18), and PC-HPSA (.01). Conversely, Class 3 (41%) had among the highest probabilities of working in high-need areas (MUA: .62; MH-HPSA: .77; PC-HPSA: .87) as the highest probability of working in rural communities (.29). The final class [Class 4: Youth Serving (26%)] was distinctive for nearly a 100% probability of working with youth and in mental health settings.
When covariates were added to the model (see Table 4), a multinomial model identified class differences by region, post-MSW experience, and income. For every year of experience post-MSW of a BHWET alum, the odds of being in Class 1 (Private Practice) were 47% greater than being in the reference class (Class 3: High Need & Rural). Alumni of the Midwest region had 87% lower odds of being in Class 1 than individuals in the Mid-Atlantic region. Similarly, Midwest region graduates also showed lower odds (OR = 0.23) of being in Class 2 (Low Need/For Profit) and Class 4 (Youth Serving: OR = 0.31) compared with Mid-Atlantic graduates. Post-MSW experience was also associated with membership in Class 4. Each year of post-MSW experience was associated with 15% greater odds of being in Class 4 compared with the reference category (Class 3).
Correlates of Social Work Practitioner Latent Class Membership (n = 501).
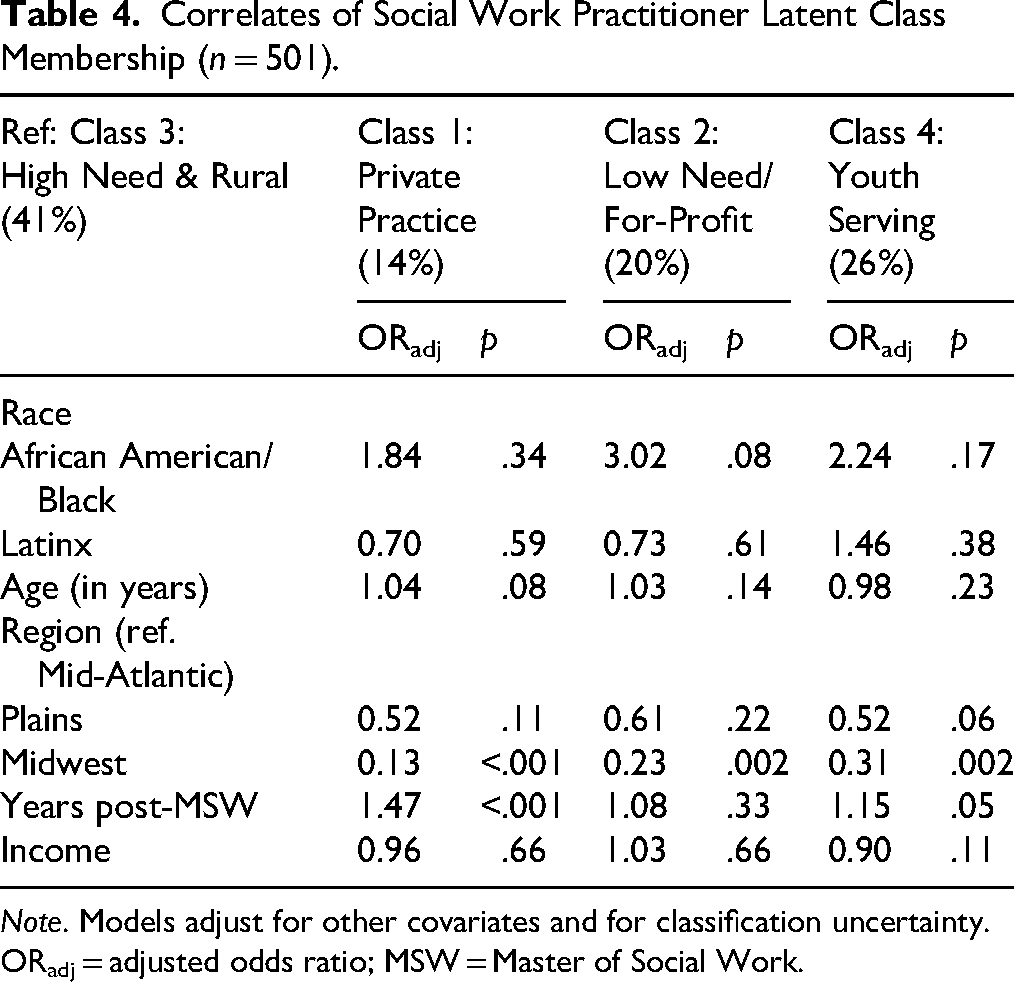
Note. Models adjust for other covariates and for classification uncertainty. ORadj = adjusted odds ratio; MSW = Master of Social Work.
Discussion
Study findings suggest that graduates of BHWET programs go on to practice in target communities, with nearly three-quarters of graduates working in geographically defined shortage areas (73.9%). While the demographics of the alumni from these three programs continue to reflect the predominantly White workforce (Fischer et al., 2024; Shim & Alegría, 2025), our analysis suggests there is no evidence of racial, gender, or age-related disparities in post-MSW milestones of social work licensure and practice. This is an encouraging finding in light of identified racial and ethnic disparities in licensing exam pass rates (Kim & Joo, 2025). Recent research by Jensen et al. (2026) found that increases in loan amount decreased the probability of MSW completion (following a BSW) among non-Hispanic Black individuals but increased the probability of graduation among non-Hispanic White students. It is possible that BHWET financial support has value for individuals from racial and ethnic minority groups who may not possess a reservoir of personal or family wealth (Dwyer & DeMarco, 2024).
This study, however, identified race-related differences in practice in geographically defined shortage areas (i.e., MUAs, MH-HPSAs, and PC-HPSAs). LCA findings highlight the diversity of practice outcomes among BHWET graduates. A majority of graduates have gone on to practice in settings that are responsive to BHWET priorities, including rural practice, work with children and youth, and health settings. Approximately 34% of graduates (Classes 1 and 2) transition to practice in relatively low need communities, typically working in private practice or for-profit settings, with greater odds in the Mid-Atlantic region and among alumni with more post-MSW experience.
Racial Differences in Geographically Defined Shortage Area Practice
Bivariate and multivariate models identified racial differences in alumni practicing in HRSA geographically defined shortage areas, as African American graduates were less likely to practice in MUAs or geographic HPSAs. Seemingly, this finding appears to be in tension with a recent report finding that 80.8% of Black/African American recent graduates worked with a majority (>50%) of clients who have incomes below the federal poverty level (Salsberg et al., 2020) compared with 64.7% of White graduates. However, low-income clients are present in all areas, and the presence of providers does not necessarily reflect the income of the clients they serve. Consequently, racial differences in geographic shortage area practice may not be a reliable proxy for measuring the economic status of the clients served by former trainees.
The differences found by race may be a function of the sites included in the study. The Midwest and Plains sites contained a greater number of MH-HPSAs and PC-HPSAs (Bureau of Health Workforce, 2024) and ranked much lower in the number of mental health providers per 100,000 people (United Health Foundation, 2024). The Mid-Atlantic site had the highest percentage of African American alumni (16%) compared with approximately 10% for the other two sites. It is possible that in the broader population of BHWET alumni and programs in varied locations, these differences may diminish or change.
The Role of Site in Geographic Shortage Area Practice
Graduates in the Midwest and Plains regions had twice the odds of practicing in a high-need area compared to the Mid-Atlantic region. This may reflect higher levels of rurality in those localities. In 2025, 63% of geographic PC-HPSAs and 62% of geographic MH-HPSAs were in rural areas (Bureau of Health Workforce, 2025), so graduates entering practice in a rural context may have a higher likelihood of practicing in a high-need area, as based on our criteria. In the current study, 70% of graduates in nonrural areas were in a geographic shortage area, but 92% of graduates in rural areas were in a geographic shortage area. This is relevant as only 6% of Mid-Atlantic graduates were in a rural area. Although formal research on this is limited, some evidence suggests that most graduates of MSW programs remain in the region where they are trained (Skinner et al., 2022), so urban programs may show lower rates of geographic shortage area practice. Moreover, rural shortage areas may cover larger geographic areas, meaning social workers residing in rural areas would be more likely to practice in high-need areas.
The practice contexts that emerged from the LCA can shed light on the potential influence of BHWET on the long-term practice outcomes of program graduates and offer suggestions for preparing students for this type of work. The probability of practicing in mental health, regardless of whether in a high-need or in a rural location, was high in all four classes (>.70), aligning well with an overall goal of BHWET “to increase the supply of behavioral health professionals” (Health Resources and Services Administration, 2020).
Class 3 (High Need/Rural: 41%) had the highest probabilities of working in a low-income area (.78), working in a rural setting (.29), and provision of addiction treatment services (.13). That all three of these indicators grouped together in the LCA likely reflects the increasing burden of poverty (Farrigan, 2021), substance use, and overdose (Centers for Disease Control and Prevention, 2024) in rural America. Class 3, in which the probabilities for practice in underserved areas were highest, also tended to include a high probability of practicing in a low-income area. This is not surprising as MH-HPSAs and MUAs should overlap with indicators of community-level poverty (Holden et al., 2026) and, therefore, alumni report of the clientele with whom they work. In our study, shortage area address and self-reported low-income practice were moderately positively correlated (ρtetra = 0.26, n = 433, p = .002). This co-occurrence has important implications for BHWET programs that seek to prepare students for practice within these communities. While training in mental health, health, and interdisciplinary practice is a hallmark of these training programs, additional training that incorporates preparation for work in low-income communities may further advance the aims of BHWET by “improving distribution [and retention] of a quality behavioral health workforce and thereby increasing access to behavioral health services” (Health Resources and Services Administration, 2020).
Alumni in Low-Need Areas
LCA findings suggest that the practice profiles (i.e., latent class) of approximately 35% [Class 1: Private Practice (14%) and Class 2: Low Need/For Profit (20%)] of alumni are inconsistent with the HRSA-designated shortage areas. Our findings suggest that individuals may move away from practice in a geographic shortage area as they get more experience. As this study utilized cross-sectional data, we could not assess whether the earlier cohorts pursued careers in low-need areas or whether this is a process that unfolds over the course of years of practice. Specific market factors (e.g., wages, demand, and reimbursement) may also influence who pursues work in private practice or in the for-profit sector, which is reflected in our finding that Mid-Atlantic alumni displayed greater odds of these private and for-profit practice profiles. Still, the Private Practice Class prevalence (Class 1: 14%) was lower than a recent estimate of private practice (26%) from the Social Work Census (Kim, 2025)
It is possible that the provision of a mandated period of work requirement (akin to the Title IV-E program) would address this issue, but may also make BHWET less attractive to prospective BHWET participants. Alternatively, programs such as the National Health Corps Scholars or NHCS Program, which provides loan relief to health professionals working in shortage areas, could be altered so that they support students making the transition from MSW graduation to the first job. At the time of this writing, NHCS programs require clinical licensure, so BHWET alumni cannot take advantage of loan repayment for at least two years post-MSW.
Strengths and Limitations
The current study has several strengths that support the validity of the findings. The use of address data to determine shortage areas where there is a high need for practitioners avoids socially desirable reporting about practice. The overall response rate for the study was relatively high (62%), suggesting with some confidence that the estimates are reliable. A long-term follow-up has the strength of a larger window into career outcomes for BHWET alumni and addresses the weakness of shorter follow-up studies that cannot detect attrition from the social work profession.
Still, the study has limitations that should be considered in interpreting results. The absence of a comparison group of alumni makes it impossible to assert that BHWET programs alter practice trajectories. We do not know whether these same social workers, in the absence of BHWET support, would have gone on to similar careers. This includes the possibility that BHWET student outcomes are no different than those of other graduates and/or that BHWET graduates represent a particular type of student (i.e., selection effects) that would seek employment in underserved communities even in the absence of BHWET support.
The sample consisted of graduates from three programs only, limiting the generalizability of the findings to the population of BHWET trainees and the overall field of social work. Findings, as noted in the discussion, may reflect the characteristics of these programs as well as the employment markets surrounding them, since most social work graduates stayed in their region postgraduation. Although there are important shared elements (e.g., stipend and commitment letter) in the three BHWET-funded programs, the design of each program was distinct. The use of address data may also undercount alumni whose practice focuses on those with high need, but who practice outside a geographically defined shortage area, including via telehealth. It is also possible that social desirability biases impacted survey responses (e.g., reported licensure when having not attained licensure because it is expected of graduates of social work programs). Our latent class model also showed marginal classification quality, suggesting that classes are an imperfect approximation of patterns of postgraduation practice.
Implications
While it is impossible to determine whether the graduates from these three programs would practice in high-need areas in the absence of the support and training provided through BHWET, our findings suggest that federally funded programs aimed at preparing and increasing the number of social workers who practice in these areas are successful in doing so. Postgraduate funding support designed to incentivize retention in shortage areas could be effective in promoting social work in those areas. Pairing BHWET traineeships with ongoing support (enhanced salary, benefits, and/or continuing education) could be more effective at increasing the workforce in high-need areas than BHWET alone. Encouragingly, the most recent round of BHWET funding (awarded in 2025), HRSA significantly increased the BHWET stipend amount to $25,000, which may reduce future graduates’ financial pressures and increase opportunities for them to accept positions that fulfill the intent of the program.
Our findings suggest that concerted efforts to diversify the behavioral health workforce are a crucial element of workforce development in behavioral health. However, the current federal funding environment – mirrored in many statehouses – diminishes public funding opportunities to support reducing these disparities. Structured evaluations, such as the current study, offer data to illustrate the value of programs such as BHWET to make the case for philanthropic support for these programs in an uncertain funding environment.
We would advocate for a longitudinal study of postgraduate outcomes among social work BHWET trainees from a plurality of grantees across the country. Future research should incorporate some form of comparison group with non-BHWET fellows, through some form of matching or a comparison with national data (e.g., the Social Work Census) or surveys to collect information from matched graduates from the same social work programs in which BHWET programs operate, for a more rigorous test of the causal effects of the BHWET program. This research would help to clarify findings from this study in terms of replicability, especially our idiosyncratic finding regarding racial differences in shortage area practice. Conducting a longitudinal evaluation over a period of postgraduation years, looking at the trajectory of graduates’ careers, could provide additional important insights related to recruitment, selection, training/preparation, and retention of the behavioral health workforce preparing to serve high-need communities. We would also welcome greater study into exit from the profession, to help promote retention in the field.
Studies that collect qualitative data could also provide insights into career decision-making among BHWET alumni, insights that would provide valuable context about why BHWET trainees choose specific career trajectories. An informal analysis of an open-ended question in this survey revealed that trainees valued exposure to these work opportunities and that this exposure informed their career choice. An in-depth qualitative study could reveal more about the important aspects of training for preparing students to fulfill the purpose of BHWET.
Footnotes
Acknowledgements
This information, content, and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received programmatic support for Behavioral Health Workforce Education and Training, funded through the Bureau of Health Workforce of the HRSA of the U.S. Department of Health and Human Services (M01HP31364, M01HP31466, and M01HP31360). The University of Maryland School of Social Work Investigators received $3,000 internal funding support. The University of Kansas School of Social Welfare investigators received $2,000 internal funding support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.