
Abstract
Purpose
Experience of out-of-home care (OHC) is associated with long-term adverse outcomes, partly due to insufficient preparation for independent living. This study examined the preliminary effectiveness of My Choice–My Way! (MCMW), a transition support service.
Methods
A 2 × 2 mixed design with natural allocation compared MCMW (n = 55) to service as usual (SAU; n = 77). Youth (n = 132), aged 15 + and currently in or recently leaving OHC, were recruited from 21 sites. Outcomes were assessed at baseline and posttest (∼8 months).
Results
Perceived competence improved over time in both groups. Social support increased significantly in MCMW compared to SAU. No group differences were found for preparedness or intervention satisfaction. Five moderating effects were identified, and provider attitudes were associated with outcomes.
Discussion
MCMW shows promise in enhancing perceived social support, though broader effects were limited. Findings highlight the importance of implementation context.
Keywords
Out-of-home care (OHC) placement (e.g., foster care placement, group home placement) during childhood is linked to several serious and long-term consequences for the individual across the lifespan. Young adults with experience of OHC have lower graduation rates from high school and struggle with post-secondary educational achievement, have lower employment rates, are more likely to experience unstable housing, have higher rates of mental health problems, including substance abuse, and are more often involved in criminal behaviors (Gypen et al., 2017). These challenges are similar regardless of whether care services are provided within a child protection system or a family service system (Gypen et al., 2017). As such, an important question for practice, policy, and research is how youth might be effectively supported in their transition from OHC to independent living in ways that prevent these later challenges (Bergström et al., 2020; OECD, 2022; Olsson et al., 2020; SBU, 2020; Statens offentliga utredningar (SOU), 2023; Strahl et al., 2021). The purpose of this study is to advance our understanding of how to support youth in their transition from OHC to independent living by investigating the preliminary effectiveness of services for youth transitioning from OHC.
Poorer outcomes for people with experience of OHC may be linked to several factors. For instance, pre-existing mental health or behavioral problems may stem from traumatic experiences encountered either before or during an OHC placement episode (Bailey et al., 2019), or they may result from shortcomings within the care environment itself, which can negatively impact the individual placed in OHC as well as subsequent generations (Straatmann et al., 2021). Another explanation is that the termination process itself is such that it does not fully prepare the young person for their transition from OHC to independent living (Becevic & Höjer, 2025), indicating a need for targeted transition interventions for this population (Heerde et al., 2018). Internationally, supportive interventions are provided in the form of transition support programs or extended care policies (Taylor et al., 2024). These may include such things as independent living programs, coaching or peer support programs, intensive individualized support services, transitional housing, or supports to young people that extend past the age of maturity. Although these types of programs have been implemented in a range of settings (Taylor et al., 2024), a recent systematic review of the effectiveness of policies and interventions to improve outcomes for young people leaving OHC concluded that the evidence supporting any one policy or intervention is insufficient and that current policy and practice does not provide care leavers with the foundations and resources they need to thrive (Taylor et al., 2024).
Approximately 1% of Sweden's 2.5 million children and youth aged 0–20 were placed in OHC at some point in 2023 (National Board of Health and Welfare, 2024; Statistics Sweden, 2024). The majority of child welfare services provided in Sweden are not evidence-based (Bergström et al., 2022). In addition, Sweden lacks formal legislation governing the provision of transition services for young people leaving the care system, which sets it apart from other Nordic countries (e.g., Denmark and Finland) as well as other countries globally (e.g., India, the United States of America, Australia, and Romania; Strahl et al., 2021). Further, there are no widespread state or municipally run programs designed specifically to support young people in their transition from OHC to independent living, and no known systematic routines for managing care exits among older adolescents. Due to this shortcoming in youth service provision (Heerde et al., 2018), a new intervention, My Choice–My Way! (MCMW; Swedish: Mitt Val-Min Väg!) was developed to provide support to young people in their transition from OHC to independent living.
The development and content of MCMW has been described in detail elsewhere (Karlsson et al., 2025; Olsson et al., 2020, 2022a, 2022b, 2024; Skoog et al., 2024; Turner et al., 2023). MCMW is a voluntary intervention for young people aged 15 years and older who are (1) currently living in OHC, or (2) have recently transitioned from OHC. As such, the population targeted by MCMW is similar to that of other independent living programs (ILPs) such as those supported by the Chafee Program in the United States (Landers, 2024). The current study is the ninth in a series of studies that together aim to increase our understanding of how to develop and deliver effective interventions for this extremely vulnerable population, and is the first investigation of the preliminary effectiveness of MCMW.
Study Aims and Questions
As MCMW is a newly developed intervention, the aim of this study is to explore its preliminary effectiveness for young people transitioning from out-of-home care to independent living after eight months. The following primary research question is asked:
RQ1: What are the short-term outcomes for young people participating in MCMW compared to Services as Usual (SAU)? Hypothesis1 (H1): Youth participating in My Choice–My Way! will exhibit gains in perceived general health relative to youth participating in Usual Services.
Hypothesis2 (H2): Youth participating in My Choice–My Way! will exhibit gains in perceived general self-efficacy relative to youth participating in Usual Services.
Hypothesis3 (H3): Youth participating in My Choice–My Way! will exhibit gains in perceived autonomy relative to youth participating in Usual Services.
Hypothesis4 (H4): Youth participating in My Choice–My Way! will exhibit gains in perceived competence relative to youth participating in Usual Services.
Hypothesis5 (H5): Youth participating in My Choice–My Way! will exhibit gains in perceived relatedness relative to youth participating in Usual Services.
Hypothesis6 (H6): Youth participating in My Choice–My Way! will exhibit gains in perceived resilience relative to youth participating in Usual Services.
Hypothesis7 (H7): Youth participating in My Choice–My Way! will exhibit gains in perceived social support relative to youth participating in Usual Services.
Hypothesis8 (H8): Youth participating in My Choice–My Way! will exhibit gains in perceived social support satisfaction relative to youth participating in Usual Services.
Hypothesis9 (H9): Youth participating in My Choice–My Way! will exhibit gains in daily routines relative to youth participating in Usual Services.
Hypothesis10 (H10): Youth participating in My Choice–My Way! will exhibit gains in help-seeking intentions relative to youth participating in Usual Services.
In addition, the following secondary research questions are asked:
RQ2: What are participants’ perceptions of the programs with which they participated? RQ3: What are MCMW providers’ perceptions of the program they delivered and of estimated program delivery? RQ4: How do subgroup characteristics moderate outcomes?
Methods
We follow CONSORT guidelines (Hopewell et al., 2025) in the reporting of this study.
Participant and Public Involvement
There was no additional participant or public involvement other than that described in the following recruitment and data collection sections of this article.
Design
A 2 (intervention: MCMW, SAU) × 2 (time: pretest, posttest) mixed design with natural allocation between MCMW and SAU groups was used. Data were collected prior to starting the intervention and approximately 8 months following the pretest.
Changes to Study Protocol
The study protocol was followed as published (Skoog et al., 2024). Deviations from a priori projections regarding intervention group equivalence in sample size may have impacted statistical power negatively.
Setting and Recruitment
This study was conducted as a multicenter research project across organizations (n = 21) providing support to young people transitioning from OHC to independent living and included municipal social service agencies, non-profit organizations, group homes, or transitional housing units across Sweden. Participating organizations self-selected to provide either MCMW or SAU (MCMW = 12; SAU = 9). Participants were referred to the study via these organizations, where they were assessed for eligibility and informed about the study during a rolling inclusion period starting October 2, 2022 and ending March 1, 2024. Youth who expressed an interest in additional information about the study were referred to the research team. No information is available regarding the number of youth initially screened and subsequently informed about the research project, but not interested in being contacted by the research team, as the collection of this data was not approved by the Swedish Ethical Review Board upon ethical review. A total of 141 youth were contacted by the research team, and 132 (94%) gave informed consent. All participating youth were provided with remuneration for their time in their choice of cash or gift certificates worth 500 Swedish Crowns (∼$50.00).
Participants and Eligibility
Young people were eligible to participate in the research if they were (1) at least 15 years of age, and (2) were living in OHC, or (3) had recently transitioned from OHC, and (4) were not undergoing any treatment (e.g., substance abuse treatment) that participation in transition services were deemed by the responsible social worker to complicate. Additionally, the youth was in contact with one of the participating referring organizations.
Data was collected electronically via personal invitation. Participants were given the option of completing the survey in person with or without help. Of participants (n = 132; MCMW = 55; SAU = 77), 23 (17.4%) requested help filling in the survey at T1 (MCMW = 5, 9.1%; SAU = 18, 23.4%, p = .03). Eight participants (6.1%) filled out the survey in English (MCMW = 3, 5.5%; SAU = 5, 6.5%; p = .79). One participant asked to fill out the survey with an interpreter, and an independent authorized interpreter was provided by the research project. At pretest, participants were living in transitional housing provided by the municipality (n = 70, 53%), independently (n = 27, 20.5%), in group homes provided by the municipality (n = 19, 14.4%), or had other living arrangements (including foster home care, n = 15, 11.3%). One participant reported being homeless at pretest. Participants were born in 26 different countries, including Sweden (n = 78, 59.5%), Syria (n = 7, 5%), Iraq (n = 5, 3.7%), Somalia (n = 5, 3.6%), and Afghanistan (n = 4, 3%). One participant reported not knowing where they were born.
Interventions
My Choice–My Way!
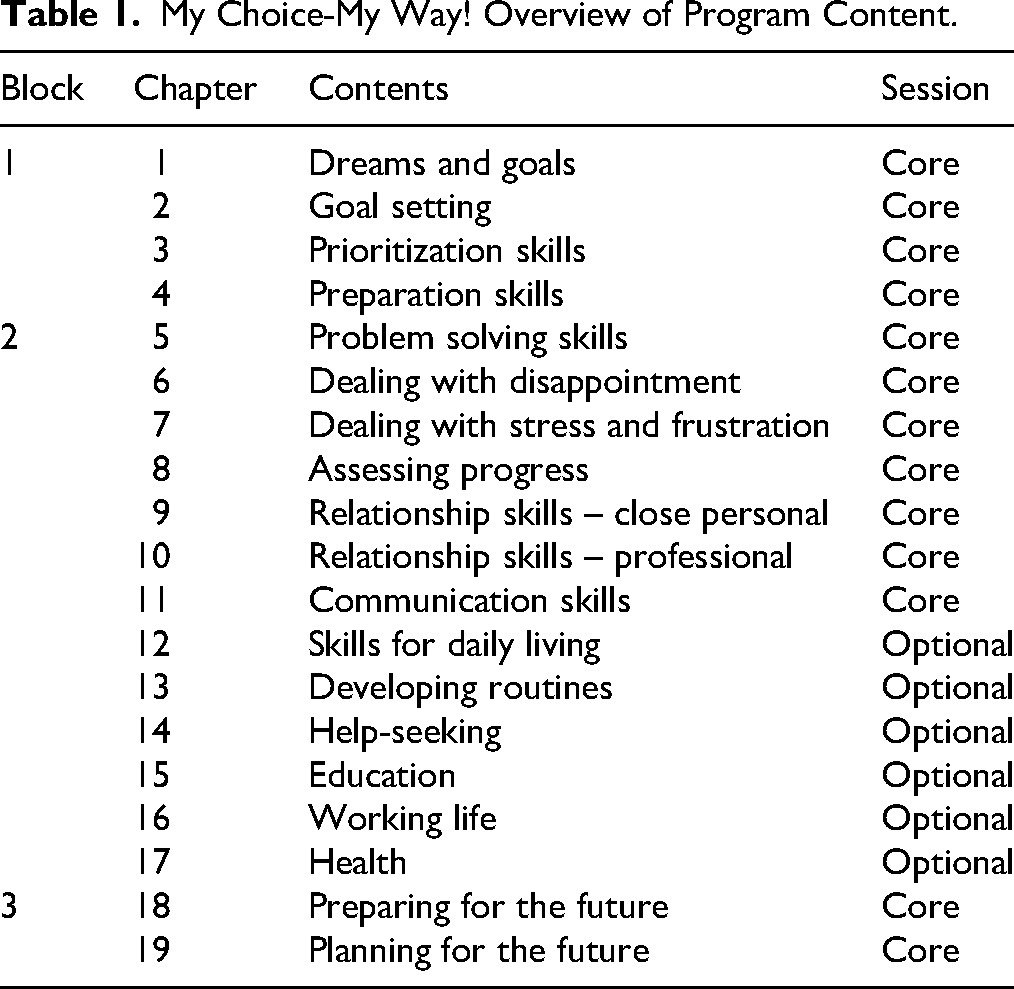
MCMW is an individually delivered intervention designed to support young people aged 15 and older in their transition from OHC to independent living. Developed through co-production with both youth and professionals (Olsson et al., 2024), the program is theoretically grounded in Self-Determination Theory (Ryan & Deci, 2017), Social Cognitive Theory (Bandura, 1986), and the COM-B Model of Behavior Change (Michie et al., 2014), as well as prior research on the effects of interventions designed to support youth in their transition from OHC to independent living (Bergström et al., 2020; Greeson et al., 2020; SBU, 2020; Yelick, 2017). MCMW aims to achieve the following long-term goals: (1) that youth be prepared to continue or complete their education, (2) gain or maintain employment, (3) develop positive help-seeking behavior, and (4) develop healthy routines, all of which are protective of later negative outcomes. Achievement of MCMW intervention goals is theorized to work by providing support in line with the principles of youth-centered practice (Olsson et al., 2022a), with emphasis on (1) youth-directed skill building (e.g., identifying and selecting goals, problem solving) and (2) consistency in promoting positive youth attitudes and beliefs around self-determination capacity. MCMW is documented in two manuals. One for the deliverer of MCMW and one for the youth participant. MCMW is based on the principle of youth-directed practice and, as such, the use of the youth materials is voluntary. Both MCMW manuals are structured around 19 chapters (13 core and six optional), organized into three thematic blocks: (1) orienting towards the future, (2) developing knowledge and skills, and (3) applying these in practice (Olsson et al., 2022a, 2022b). The information contained in the manuals serves as the foundation for the intervention which aims at consisting of a minimum of 16 sessions (13 core and three optional) delivered over 4–8 months, which are collaboratively tailored by the professional based on the identified youth-directed goals. Program sessions may be delivered in the young person's home, at the social services’ office, or in another setting, according to the nature of the providing organization and the preferences of the youth. No incentives to encourage adherence or compliance with program participation were given. MCMW is described in an explicit program theory (Olsson et al., 2023) that can be found in Figure 1. An overview of program content can be found in Table 1. Social workers responsible for delivering MCMW received training through a four-day, in-person training conducted by two trainers based on principles from Adult Learning Theory (Knowles, 1978; Knowles et al., 2005), Kolb's Experiential Learning Model (Cheung & Delavega, 2014; Kolb et al., 2001), and employed a skills-based approach. Deliverers also participate in a half-day follow-up digital booster session approximately 6 months following initial training. Both training components were developed in parallel with the intervention to ensure alignment with its theoretical foundations and practical implementation.
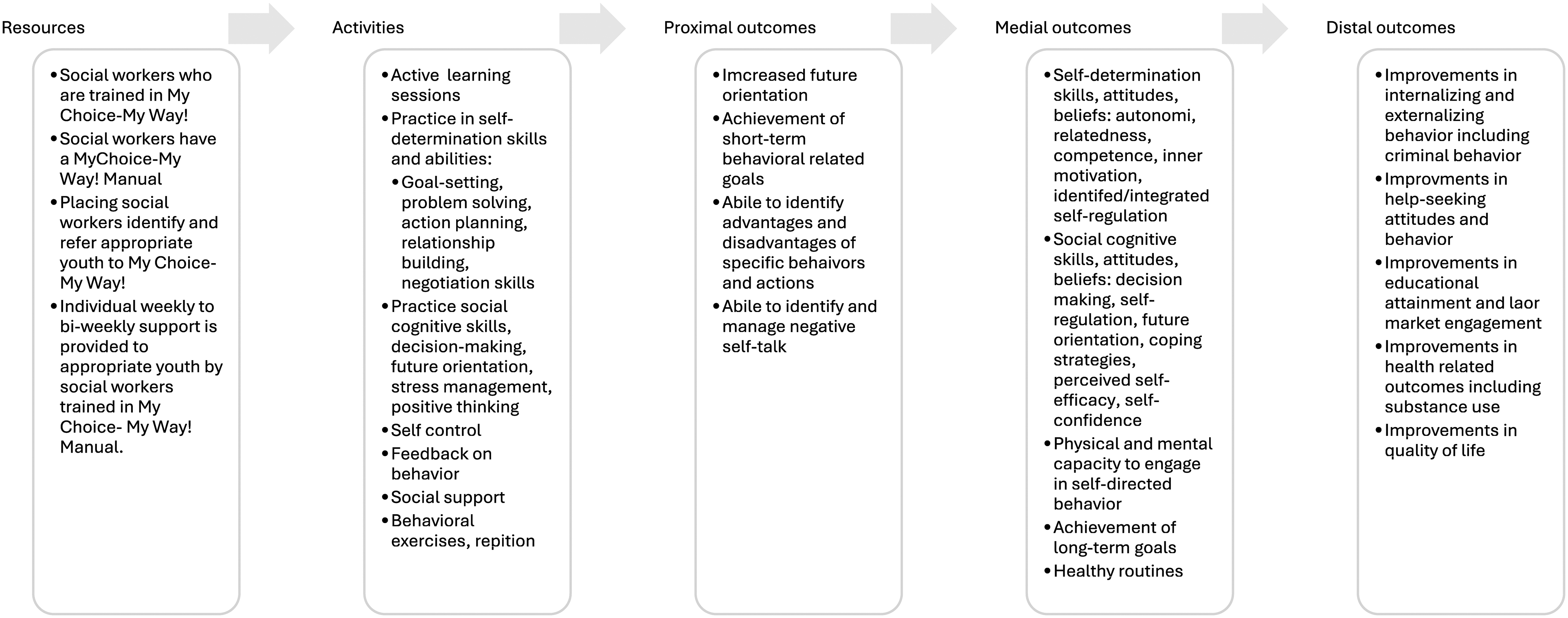
My Choice–My Way! program theory.
My Choice-My Way! Overview of Program Content.
Services as Usual
SAU consisted of individual support services ranging from daily support with routine-building and management of daily tasks to regular visits from a social worker for youth living independently. Service providers (sometimes in collaboration with the individual youth) determine the amount and type of support through individual needs assessments, often followed by the development of an individualized case plan. Regardless of service provider and support intensity, youth taking part in SAU were commonly assigned a social worker by the municipality, with whom they met regularly to discuss progress and difficulties. The support provided generally included components of information, in writing and/or in dialogue with staff; skill building in areas such as personal economics, social skills, and housework; and practical support in areas such as searching for housing or developing/maintaining routines. In some instances, staff were trained in using certain methods such as motivational interviewing (MI; Miller & Rollnick, 2013), feedback-informed treatment (FIT; Miller et al., 2015), or rePULSE.
Attrition
Participant flow through the study can be found in Figure 2. A total of 141 youth were referred to the study. Nine youth (MCMW n = 2; SAU n = 7) did not provide informed consent. Two of the youth (both referred from SAU) declined participation. We were unable to reach the remaining seven after the initial referral. Twenty-seven (20.5%) participants did not complete the follow-up measure at T2. More youth in the MCMW group were lost to follow-up compared to youth in the SAU group (MCMW = 16, 29.1%; SAU = 11, 14.3%; p = .04). There were no differences in sex, place of birth, mother tongue, whether at least one parent was living or in Sweden, if the youth was employed, type of living arrangement, citizenship status, or age between those that completed T2 follow-up and those that did not. Those youth not in school at T1 dropped out of the study to a larger extent (n = 9, 45%) than youth in school at T1 (n = 18, 16.1%; p ≤ .01).
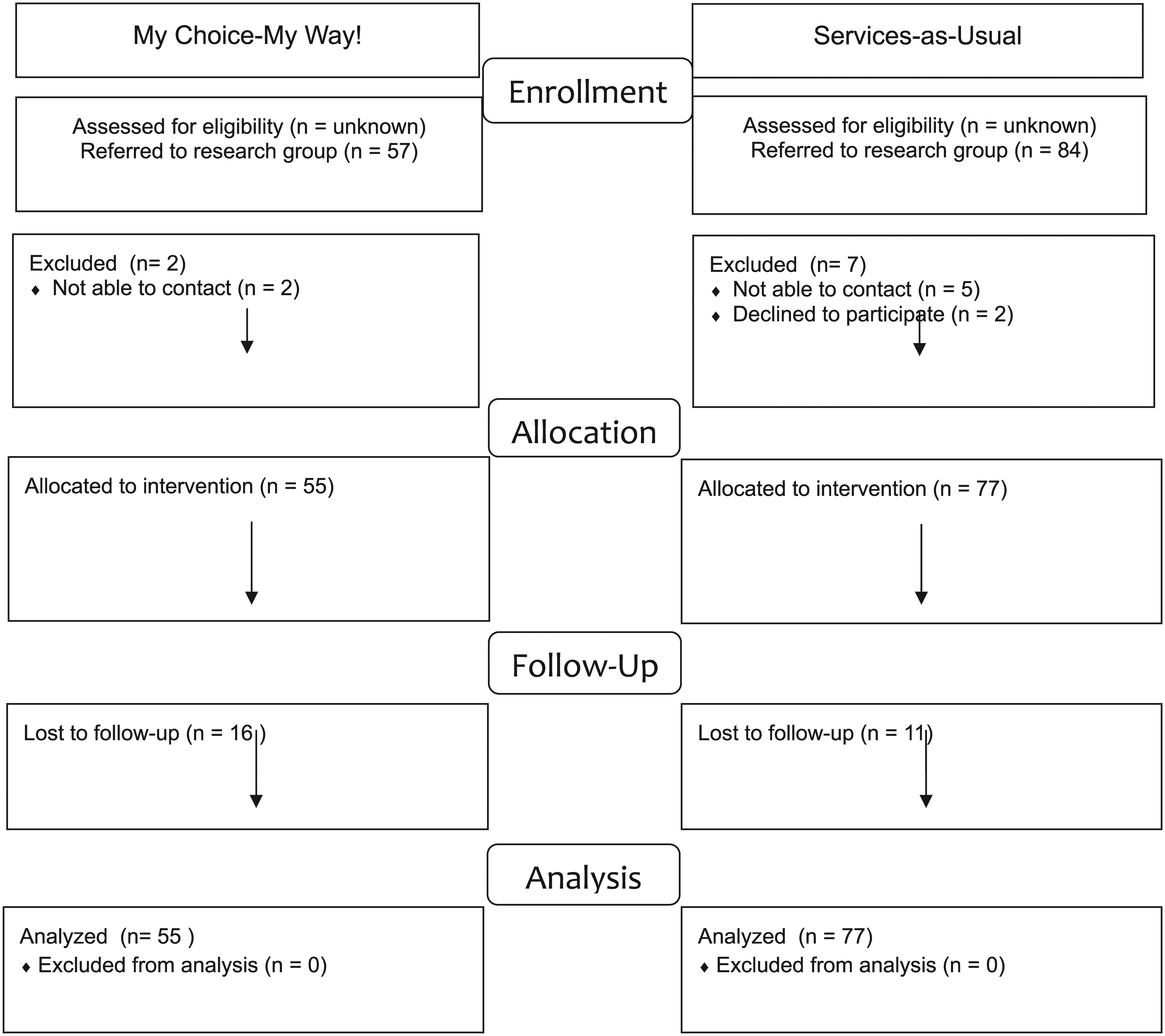
Participant flow through the study.
In the MCMW group, more youth who were not attending school at T1 dropped out of the study (n = 8, 61.5%) compared to youth who were attending school at T1 (n = 8, 19%; p ≤ .01). There were no other differences in background characteristics for those youth who completed and did not complete T2 follow-up within the MCMW group. There were no differences in background characteristics for those youth who completed and did not complete T2 follow-up in the SAU group.
Measures
Participant Characteristics
Participant characteristics included respondents’ sex (male and female), age, birthplace (Sweden and other), living situation at intake (OHC and other), mother tongue (Swedish and other), whether at least one parent was living (yes and no), whether at least one parent was living in Sweden (yes and no), whether the respondent had Swedish citizenship (yes and no), whether the respondent was attending school (yes and no), and whether the respondent had a job (yes and no).
Primary Outcomes
General Health
The General Health Questionnaire (GHQ-12) is a screening instrument that detects psychosomatic symptoms and conditions (Goldberg et al., 1997). The scale consists of 12 items phrased as statements about symptoms with four semantic response options on a 4-point scale. Six of the items are positively phrased, and six are negatively phrased but worded so there is no need to reverse scores. A high score indicates more psychosomatic symptoms. The GHQ-12 has demonstrated good to excellent psychometric properties in Swedish populations, including acceptable to high internal consistency and strong criterion validity against diagnostic interviews, with area under the curve values ranging from ∼0.73 to 0.90 (Lundin & Dalman, 2020; Lundin et al., 2016a, 2016b). It is therefore considered a valid and reliable screening instrument for psychological distress in both the general population and clinical contexts in Sweden. The license to use the Swedish version for this study was granted on December 1, 2022 and February 24, 2023 by Mapi Research Trust (https://mapi-trust.org). Internal consistency on this measure was adequate (α = .858).
General Self-Efficacy
Self-efficacy reflects an optimistic self-belief that one can perform a novel or difficult task or cope with adversity, and is measured with the General Self-Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995). Perceived self-efficacy eases goal setting, effort investment, robustness in the face of barriers, and recovery from setbacks. The scale consists of 10 items rated on a 4-point semantic scale (“not at all true” to “exactly true”). A high score indicates high self-efficacy. The Swedish version was translated by Koskinen-Hagman et al. (1999) and validated by Löve et al. (2012). The Swedish version of the General Self-Efficacy Scale has demonstrated good psychometric properties, including high internal consistency (α ≈ .89–.90), a unidimensional factor structure, and evidence of convergent validity across population and clinical samples (Lönnfjord & Hagquist, 2017; Löve et al., 2012). Internal consistency in the current sample was adequate (α = .895).
Autonomy, Competence, and Relatedness
The Need Satisfaction and Frustration Scale (NSFS-18) measures external motivation within three subscales: autonomy (the need that your own actions are self-initiated and self-regulated), social relatedness (the need in your own social environment to develop secure and satisfying connections), and competence (the need that one can perform necessary actions with efficiency; Longo et al., 2016). The scale consists of 18 items rated on a 5-point likert scale (“agree” to “disagree”). Psychometric studies support the validity and reliability of Need Satisfaction and Frustration Scale measures in both adolescent and Swedish samples, demonstrating stable factor structures, measurement invariance, and expected associations with well-being and distress (e.g., Chávez-Ventura et al., 2026; Holmquist et al., 2024a, 2024b; Janić et al., 2025). However, this evidence primarily concerns full versions of the scale (e.g., BPNSFS/NSFS), and specific psychometric validation of abbreviated forms such as the NSFS-18 remains limited. A high score on each subscale indicates high autonomy, social relatedness, or competence. Each of the three subscales is used in this study. Internal consistency in the current sample was adequate (α = .876).
Resilience
The Resilience Scale (RS-14) was used to measure the degree of individual resilience (Wagnild, 2016; Wagnild & Young, 1993). The scale consists of 14 items rated on a 7-point likert scale (“disagree” to “agree”). A high score indicates high resilience. The Swedish version was translated by Lundman et al. (2007). The Resilience Scale (RS-14) has demonstrated good psychometric properties in adolescent samples internationally, including high internal consistency, a stable structure, and evidence of convergent validity. Although a Swedish version of the original Resilience Scale (RS-25) has shown acceptable reliability and validity in adult populations, specific validation of the RS-14 in Swedish adolescents remains limited (Nygren et al., 2004; Pritzker & Minter, 2014; Zelviené et al., 2021). License to use the Swedish version of the RS-14 was granted by The Resilience Center (https://www.resiliencecenter.com) on October 27, 2021 and May 8, 2024. Internal consistency was adequate (α = .885).
Social Support and Social Support Satisfaction
The Social Support Questionnaire (SSQ-6) assesses the number of available others the respondent feels they can turn to when in need for each of six situations (Sarason et al., 1987). The total score is used in this study. A high score indicates more perceived available support. The SSQ-6 also measures the extent to which the respondent is satisfied with their perceived support in each of six given situations. The SSQ-6 has demonstrated good psychometric properties, including high internal consistency and evidence of construct validity, with studies showing strong correspondence with the original full-scale measure and associations with related psychological constructs. Subsequent validation studies have supported its reliability and factorial structure across diverse populations, although evidence in Swedish adolescent samples remains limited (Friedman et al., 2018; Sarason et al., 1987). The total score is used in this study. A higher score indicates higher satisfaction with their perceived social support. Internal consistency on the satisfaction of social support scale was adequate (α = .824).
Daily Routines
Daily routines were measured by a shortened instrument inspired by the Sustainability of Living Inventory (Hou et al., 2019) and adjusted to fit youths’ everyday life. The 18 items are measured on a 5-point semantic scale (“very unusual” to “very common”) and span Personal Hygiene, Eating Habits, Sleeping Habits, Household Chores, Physical Activities, and Social Activities. The internal consistency was adequate (α = .858).
Help-Seeking Intentions
The General Help Seeking Questionnaire (GHSQ) was used to assess intentions to seek help from different sources, including both formal and informal help source options (Wilson et al., 2005). The GHSQ uses a matrix format that can be modified according to purpose and needs to meet sample characteristics and study requirements. The GHSQ has demonstrated satisfactory psychometric properties, including acceptable internal consistency and evidence of construct validity, in both initial validation and subsequent studies. Research in adolescent samples further supports its reliability and factorial structure, typically distinguishing between formal and informal help sources, although its flexible format means that psychometric properties may vary depending on the specific adaptation and context of use (Deane & Wilson, 2007; Olivari & Guzmán, 2017; Wilson et al., 2005). A high score indicates high intentions to seek help. The questionnaire was translated from English to Swedish using the consensus method (Douglas & Craig, 2007) for this study.
Secondary Outcomes, Participant Perceptions of MCMV and SAU
Participant Perceived Preparedness for Transition
We assessed participants’ perceived preparedness for transition with a single item, “How well prepared do you feel you are for life as an adult (e.g., to live on your own, take care of daily responsibilities, etc.)?” Youth were asked to answer on a 4-point scale ranging from “definitely not prepared” to “definitely prepared.”
Participant Perceived Satisfaction
We measured youth's perceived satisfaction with the intervention with which they participated, with six of the eight items in the Client Satisfaction Questionnaire (CSQ-8; Attkisson & Greenfield, 1996). A high score indicates high satisfaction. Internal consistency was satisfactory in both the intervention (α = .899) and control group (α = .946). The Swedish version was purchased from https://csqscales.com
Participant Estimated Number of Sessions
We asked youth participants in the MCMW group to estimate their level of participation with the following question: “Approximately how many times would you say you met the person who helped you with the intervention?” Participants could provide their estimated number of meetings within the intervention with which they participated.
MCMW Providers’ Perceptions
Provider Estimated Number of Sessions
We asked providers to estimate the number of sessions with which they met participating youth with the following question: “Approximately how many times have you met with (the participant) to provide My Choice-My Way! Over the last eight months?” Respondents could answer with the estimated number of sessions.
MCMW Provider Estimated Proportion of Intervention Delivered
Providers of MCMW answered two questions to capture the estimated amount of intervention delivered. The first question was “How long did the youth participate in My Choice-My Way!?” Four response options were possible: “The youth did not participate,” “The youth started but then quit or the intervention was discontinued,” The youth started and participated in the entire the program,” and “The youth is still participating.” The second question was, “How much of My Choice-My Way! Do you estimate that the youth participated in over the past eight months?” Response options were “∼25%,” “∼50%,” “∼75%,” “∼100%,” or “other.”
MCMW Provider Perceived Acceptability, Appropriateness, and Feasibility
We used the 4-item Acceptability of Intervention measure (AIM), the 4-item Appropriateness of Intervention Measure (IAM), and the 4-item Feasibility of Intervention Measure (FIM; Weiner et al., 2017). To assess providers’ perceptions of implementing MCMW to participating youth. Internal consistency was satisfactory for the AIM (α = .872), IAM (α = .892), and FIM (α = .750)
Harms
Harms in this study are defined as statistically significant group by time effects in favor of SAU.
Sample Size
Following Cohen's proposed interpretation of f, a priori power calculations (Faul et al., 2007, 2009) determined that this study would need a minimum of 124 youth to fully participate in the trial in order to obtain 85% statistical power to detect a medium (f ≤ .25) effect with alpha set at .05 for repeated measures ANOVA with within and between interactions.
Blinding
Service providers and participants were not blinded to the services being provided nor the group in which they were participating. SAU providers were unaware of which youth were participating in the study. MCMW was made available only to research participants during the study period. All data were collected via an online platform and, therefore, were blinded from both researchers and service providers.
Statistical Analysis
All analyses were conducted with SPSS v. 29.02. Participant characteristics are reported with descriptive statistics (e.g., percent and mean) depending on variable measurement characteristics. Differences between MCMW and SAU groups on participant characteristics were tested with X2 or the independent means t-test, depending on variable characteristics. When cell counts were low, Fisher's exact test was used as an alternative to X2. Main and interaction effects are initially assessed with the repeated measures ANOVA, and where appropriate, the independent t-test and/or paired samples t-test are used as post-hoc tests to further investigate significant time and/or interaction effects. Diagnostic tests for the repeated measures ANOVA revealed that all variables fulfilled the assumptions of homogeneity of variance and homogeneity of intercorrelations. There were, however, some deviations from normality in the data (i.e., competence, relatedness, social support, social support satisfaction, and daily routines). The repeated measures ANOVA has been found to be robust to deviations from normality (Blanca-Mena et al., 2022).
Multiple regression analysis was used to explore the moderating effect of participant characteristics (i.e., sex, age, living situation at intake, place of birth, and citizenship status) and transition service delivery context (i.e., whether the MCMW and SAU were provided within the out-of-home care setting or within a community-based setting) on outcome across outcomes. The moderation analyses were conducted in two steps. First, pretest score, group, and background characteristics (e.g., age) were entered into the model using stepwise multiple linear regression. Second, the interaction term (e.g., age × group) was added to assess the impact of the interaction term on change in R2 as well as whether this addition resulted in a significant improvement in outcome prediction. Due to the exploratory nature of these moderation analyses, the probability level is set to .10. Due to the high number of moderation analyses, only significant moderation effects are reported.
Intent to Treat
We conducted intent-to-treat (ITT) analyses on all outcomes using full data for all participants who provided informed consent.
Imputation
We imputed missing values for participants and scales using multiple imputation. Values at pretest were predicted based on background variables and scores of available scale items. Values at posttest were predicted based on background variables, available item scores, and total scale scores at pretest. The number of imputations was set to 5, and pooled scores at the item level were used in the analyses.
Post-Hoc Tests
We conducted several post-hoc tests to explore the relationship between MCMW provider-reported implementation measures (i.e., provider-estimated number of sessions, provider-perceived acceptance, appropriateness, and feasibility) and outcome. In total, 40 tests were conducted, and the resulting Bonferroni correction, for the interested reader, is p ≤ .001.
Results
Participant Characteristics at Pretest
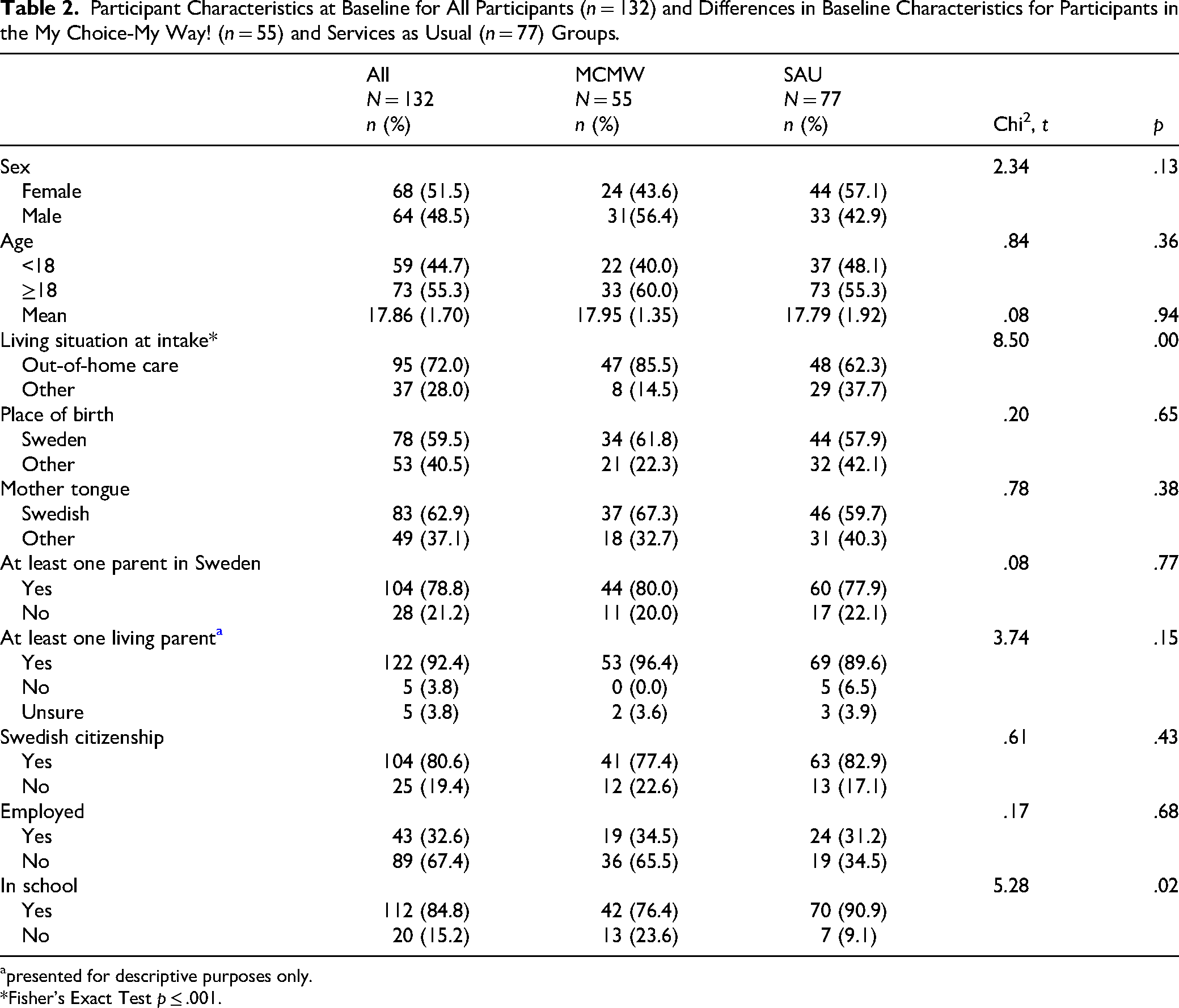
Participant characteristics can be found in Table 2. A higher percentage of youth in the MCMW group were living in OHC compared to SAU group youth (MCMW = 85.5%; SAU = 62.3%, p < .001) at pretest. Additionally, more youth in the MCMW group reported not attending school compared to SAU youth (MCMW = 23.6%; SAU = 9.1%; p = .02) at pretest. At pretest, participants in MCMW reported better general health (M = 1.12, SD = .52), higher perceived self-efficacy (M = 3.02, SD = .58), higher perceived competence (M = 3.44, SD = .68), and higher levels of perceived resilience (M = 5.34, SD = .98) compared to participants in the SAU group (general health M = 1.35, SD = .58; perceived self-efficacy M = 2.77, SD = .53, perceived competence M = 3.20, SD = .66; perceived resilience M = 4.91, SD = .89, all ps < .05; Table 3).
Participant Characteristics at Baseline for All Participants (n = 132) and Differences in Baseline Characteristics for Participants in the My Choice-My Way! (n = 55) and Services as Usual (n = 77) Groups.
presented for descriptive purposes only.
*Fisher's Exact Test p ≤ .001.
Means, Standard Deviations at Pretest (Time 1) and 8-Month Follow-Up (Time 2) for Both Intervention Groups, Interaction Effects, Time Effects, and Effect Sizes From 2 × 2 Mixed ANOVA.
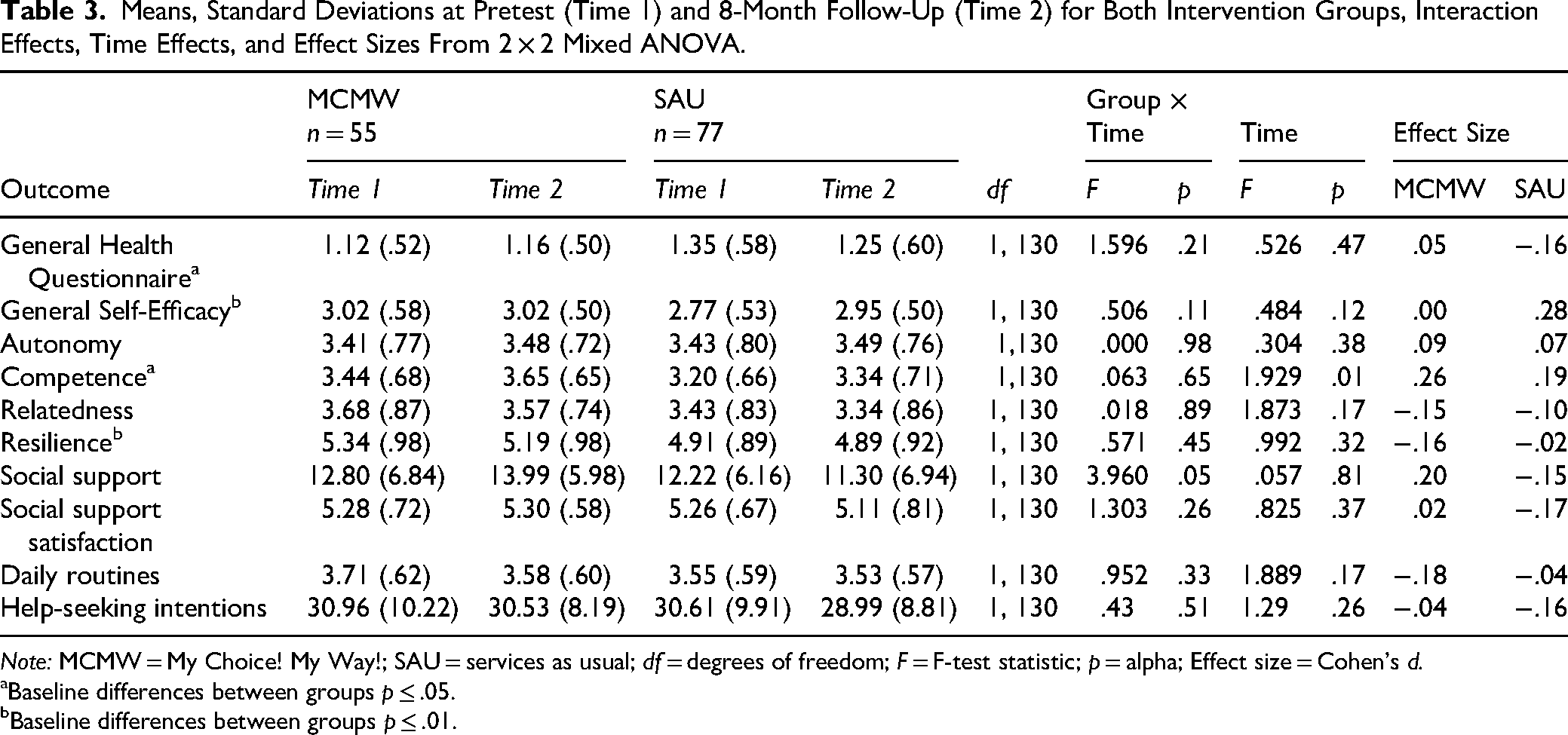
Note: MCMW = My Choice! My Way!; SAU = services as usual; df = degrees of freedom; F = F-test statistic; p = alpha; Effect size = Cohen's d.
Baseline differences between groups p ≤ .05.
Baseline differences between groups p ≤ .01.
Short-Term Outcomes of MCMW Compared to SAU
Results of the repeated measures ANOVA can be found in Table 3. H1 posited that youth participating in MCMW would exhibit gains in perceived general health as measured with the GHQ-12 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 1.13, SET1 = .075, 95% CIT1 = 0.98–1.28; MCMW MT2 = 1.18, SET2 = .075, 95% CIT2 = 1.01–1.31) and SAU groups (SAU MT2 = 1.35, SET2 = .063, 95% CIT2 = 1.23–1.48; SAU MT2 = 1.25, SET2 = .063, 95% CIT2 = 1.12–1.37) did not exhibit significant improvements in perceived general health over time, F(1, 130) = .53, p = .47, η p 2 = .004. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = 1.596, p = .21, η p 2 = .012.
H2 posited that youth participating in MCMW would exhibit gains in perceived general self-efficacy as measured by the GSE relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 3.02, SET1 = .07, 95% CIT1 = 2.88–3.17; MCMW MT2 = 3.02, SET2 = .07, 95% CIT2 = 2.89–3.15) and SAU groups (SAU MT1 = 2.77, SET1 = .06, 95% CIT1 = 2.65–2.90; SAU MT2 = 2.95, SET2 = .06, 95% CIT2 = 2.84–3.06) did not exhibit significant improvements in perceived general self-efficacy over time, F(1, 130) = 2.41, p = .12, η p 2 = .018. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .506, p = .11, η p 2 = .019.
H3 posited that youth participating in MCMW would exhibit gains in perceived autonomy as measured by the NSFS-18 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 3.41, SET1 = .11, 95% CIT1 = 3.20–3.62; MCMW MT2 = 3.48, SET2 = .10, 95% CIT2 = 3.28–3.68) and SAU groups (SAU MT1 = 3.43, SET1 = .09, 95% CIT1 = 3.25–3.60; SAU MT2 = 3.49, SET2 = .09, 95% CIT2 = 3.33–3.66) did not exhibit significant improvements in perceived autonomy over time, F(1, 130) = .79, p = .38, η p 2 = .006. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .000, p = .98, η p 2 = .000.
H4 posited that youth participating in MCMW would exhibit gains in perceived competence as measured by the NSFS-18 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 3.44, SET1 = .09, 95% CIT1 = 3.26–3.62; MCMW MT2 = 3.65, SET2 = .09, 95% CIT2 = 3.47–3.83) and SAU groups (SAU MT1 = 3.20, SET1 = .08, 95% CIT1 = 3.05–3.35; SAU MT2 = 3.34, SET2 = .08, 95% CIT2 = 3.19–3.50) exhibited significant improvements in perceived competence over time, F(1, 130) = 6.444, p = .01, η p 2 = .047. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .063, p = .65, η p 2 = .002.
H5 posited that youth participating in MCMW would exhibit gains in perceived relatedness as measured by the NSFS-18 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 3.68, SET1 = .11, 95% CIT1 = 3.46–3.91; MCMW MT2 = 3.57, SET2 = .11, 95% CIT2 = 3.36–3.79) and SAU groups (SAU MT1 = 3.43, SET1 = .10, 95% CIT1 = 3.24–3.62; SAU MT2 = 3.34, SET2 = .09, 95% CIT2 = 3.15–3.52) did not exhibit significant improvements in perceived relatedness over time, F(1, 130) = 1.87, p = .87, η p 2 = .014. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .018, p = .89, η p 2 = .000.
H6 posited that youth participating in MCMW would exhibit gains in perceived resilience as measured by the RS14 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 5.35, SET1 = .13, 95% CIT1 = 5.10–5.60; MCMW MT2 = 5.19, SET2 = .13, 95% CIT2 = 4.93–5.44) and SAU groups (SAU MT1 = 4.91, SET1 = .11, 95% CIT1 = 4.70–5.12; SAU MT2 = 4.89, SET2 = .11, 95% CIT2 = 4.68–5.10) did not exhibit significant improvements in perceived resilience over time, F(1, 130) = .99, p = .32, η p 2 = .008. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .571, p = .45, η p 2 = .004.
H7 posited that youth participating in MCMW would exhibit gains in perceived social support as measured by the SSQ-6 relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA supported this hypothesis. Participants in the MCMW group (MCMW MT1 = 12.80, SET1 = .87, 95% CIT1 = 11.08–14.53; MCMW MT2 = 13.99, SET2 = .88, 95% CIT2 = 12.24–15.74) made significant improvements, F(1, 130) = .06, p = .81, η p 2 = .000, in perceived social support between pretest and posttest relative participants in the SAU group (SAU MT1 = 12.23, SET1 = .74, 95% CIT1 = 10.77–13.68; SAU MT2 = 11.30, SET2 = .75, 95% CIT2 = 9.82–12.78). There was a significant time × group interaction, indicating that the pattern of change differed between the groups, F(1, 130) = 3.96, p = .05, η p 2 = .030.
H8 posited that youth participating in MCMW would exhibit gains in perceived social support satisfaction as measured by the SSQ-6 relative to participants in the SAU group. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 5.28, SET1 = .09, 95% CIT1 = 5.09–5.46; MCMW MT2 = 5.30, SET2 = .10, 95% CIT2 = 5.10–5.49) and SAU groups (SAU MT1 = 5.27, SET1 = .80, 95% CIT1 = 5.11–5.42; SAU MT2 = 5.11, SET2 = .08, 95% CIT2 = 4.94–5.27) did not exhibit significant improvements in perceived social support satisfaction over time, F(1, 130) = .83, p = .37, η p 2 = .006. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = 1.303, p = .25, η p 2 = .010.
H9 posited that youth participating in MCMW would exhibit improvements in daily routines relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 3.71, SET1 = .08, 95% CIT1 = 3.55–3.87; MCMW MT2 = 3.58, SET2 = .08, 95% CIT2 = 3.43–3.74) and SAU groups (SAU MT1 = 3.55, SET1 = .07, 95% CIT1 = 3.42–3.69; SAU MT2 = 3.53, SET2 = .07, 95% CIT2 = 3.40–3.66) did not exhibit significant improvements in daily routines over time, F(1, 130) = 1.89, p = .17, η p 2 = .014. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .952, p = .33, η p 2 = .007.
H10 posited that youth participating in MCMW would exhibit gains in help-seeking intentions relative to youth participating in SAU. Results from the 2 × 2 mixed ANOVA did not support this hypothesis. Participants in the MCMW (MCMW MT1 = 30.96, SET1 = 1.35, 95% CIT1 = 28.29–33.64; MCMW MT2 = 30.53, SET2 = 1.15, 95% CIT2 = 28.25–32.81) and SAU groups (SAU MT1 = 30.61, SET1 = 1.14, 95% CIT1 = 28.34–32.87; SAU MT2 = 28.99, SET2 = .98, 95% CIT2 = 27.06–30.92) did not exhibit significant improvements in help-seeking intentions over time, F(1, 130) = 1.29, p = .26, η p 2 = .010. There was no significant time × group interaction, indicating that the pattern of change did not differ between the groups, F(1, 130) = .431, p = .51, η p 2 = .003.
Participant Perceptions
There were no differences in participants’ perceived preparedness following participation in either MCMW (Mean Rank=50.96) or SAU (Mean Rank=50.24; p = .89). There were no differences in participants’ perceived satisfaction with the intervention they received (MCMW = 18.81, SD = 3.63; SAU =17.94, SD = 4.64; p = .34).
MCMW Provider Perceptions
Providers reported data on 39 youth participants (71%). MCMW providers estimated that they met with youth an average of 7.6 times (SD = 5.1) over the eight-month study period. This varied from a minimum of 1 session to a maximum of 17 sessions (Median = 6.5). Providers of MCMW estimated that ∼10.3% (n = 4) of youth did not start the program, ∼43.6% (n = 17) started but quit or discontinued participation, ∼12.8% (n = 5) participated in the entire program, and ∼33.3% (n = 13) of participants were still participating at eight-month follow-up. MCMW providers estimated that 41% (n = 16) of youth participants received 0%–25% of the program, 12.8% (n = 5) of participants received 26%–50% of the program, 12.8% (n = 5) perceived 51%–75% of the program, and 17.9% (n = 7) of participants received ∼76%–100% of the program. MCMW providers perceived MCMW as acceptable (AIM = 3.99, SD = .57), appropriate (IAM = 3.60, SD = .83), and feasible (FIM = 3.61, SD = .67).
Outcome Moderation
We found five significant (p ≤ .10) moderating relationships. First, whether the youth had reached the age of maturity (i.e., 18) moderated the relationship between group and perceived self-efficacy, R2Δ = .026, F(1, 127) = 3.718, p = .056; <18 years MCMW Mdiff = −.27, SAU Mdiff = .16, p = .04;
Post Hoc Tests
There was a significant and positive correlation between youth and provider-estimated number of sessions (rho = .53, p = .04). The estimated number of sessions was not significantly related to any outcome. MCMW participant satisfaction was moderately and positively correlated with relatedness (rhodiff = .36, p = .03) and self-efficacy (rhodiff = .33, p = .05). Provider perceived acceptability was significantly and negatively correlated with social support (rhodiff = −.40, p = .05). Provider perceived appropriateness was significantly and negatively correlated with autonomy (rhodiff = −.48, p = .02). Provider perceived feasibility was significantly and negatively correlated with autonomy (rhodiff = −.45, p = .03).
Discussion and Applications to Practice
MCMW is a newly developed intervention that aims to support young people in their transition from out-of-home care to independent living (Olsson et al., 2022a, 2022b). The aim of this study was to explore the preliminary effectiveness of MCMW after 8 months, and it is the first experimental test of the MCMW program theory. Importantly, this is one of a paucity of primary studies aimed at evaluating the effectiveness of transition support services for young people transitioning from OHC and one of only two studies of its kind conducted outside of the United States (Taylor et al., 2024). As young people in OHC in the United States and Sweden (and likely other contexts) differ in several areas central to the provision of transition support services (Olsson et al., 2020), this study provides important insights into how transition services can be developed, refined, and delivered in order to best serve this highly vulnerable population.
We aimed to answer four questions in order to gain a preliminary understanding of how MCMW achieves its goals when implemented in normal practice settings. First, we were interested in the short-term outcomes associated with participation in MCMW compared to participation in SAU. We found that young people participating in MCMW improved over time in their perceived competence. There was, however, no group effect and, as such, we are unable to determine if this change is a result of participation in a transition support intervention specifically or indicates a more general maturity effect. In addition, we found that participants in MCMW reported significant improvements in perceived social support compared to participants in the SAU group. These results are highly promising as they are in line with the MCMW theory of change (Figure 1) and its focus on supporting competence development through youth-centered practices. In addition, early changes in intervention mechanisms, such as perceived competence and social support, are in line with what could reasonably be expected in a short-term effectiveness study. We are aware of only two prior effectiveness studies that have measured social support in the context of supportive interventions for young people transitioning from OHC (Courtney et al., 2019; Jacobs et al., 2015; Leip, 2020; Skemer & Jacobs, 2016; Taylor et al., 2024). These studies reported no effect on measures of social support. Importantly, social support for this population may be an important correlate for wellbeing (Karlsson et al., 2026; Olsson & Skoog, 2026) and act as a buffer for later wellbeing (Corwin et al., 2020) and is a component of other transition support services (Courtney et al., 2019; Greeson et al., 2014; Leip, 2020) that have either not measured or have failed to find an effect on this mechanism. Given that young people in transition from the OHC system have a history of instability in social support and smaller social networks compared to their peers (Horan & Widom, 2015; Negriff et al., 2020; Olsson & Skoog, 2025, 2026), interventions that can improve perceived social support among this population may promote positive well-being and successful transitions into adulthood (Bennett et al., 2024; Cederbaum et al., 2023), both of which are long-term goals for MCMW.
Second, we were interested in understanding participants’ perceptions of the interventions within which they participated. We found no differences in participant-reported satisfaction with services for those participating in MCMW or SAU. Although overall measures of youth reported satisfaction with MCMW was high and similar to that reported by children receiving community based mental health services in the United States (Copeland et al., 2004) and foster children receiving outpatient psychiatric services in Switzerland (Urben et al., 2015), satisfaction was substantially lower (SD > 2) than that reported in other studies involving a diverse range of youth populations participating in a range of programs (Babiano-Espinosa et al., 2021; Kennard et al., 2024). Understanding youth satisfaction in services is paramount in the development of new interventions, as dissatisfaction is related to poor outcomes and premature dropout (Garnick et al., 2006). We, however, found no clear relationship between youth-rated satisfaction and youth-estimated participation in MCMW. As such, our findings indicate that the introduction of MCMW did not negatively impact participant satisfaction with services. Additionally, participant satisfaction was moderately and significantly correlated with participant perceived relatedness and self-efficacy, two important medial outcomes of MCMW. As these were results from post hoc tests, future studies should be designed to investigate this relationship further.
Third, we were interested in understanding MCMW provider estimates of the amount of program delivered as well as their perceptions of the program they delivered. The accuracy of the provider, as well as the participant, reported program participation as measured in this study is questionable due to potential recall bias. However, in this study, provider-reported and participant-reported participation was rather strongly related (Schober et al., 2018), given the time-period within which they were asked to recall and the two very different groups of stakeholders. In a study of self-reported health service utilization recall from between 7 and 12 months, found underreporting of 36% (Brusco & Watts, 2015), leading investigators to suggest inflating self-reported participation over a one-year period by 16%. Additional attempts to study MCMW should incorporate more objective measures of program participation and fidelity.
Provider-perceived acceptability, appropriateness, and feasibility are important early outcomes for attaining desired service delivery and program outcomes (Proctor et al., 2011). Providers participating in this study found MCMW acceptable, appropriate, and feasible. Curiously, provider perspectives were found in post hoc tests to be related to changes in social support and autonomy. These associations were, however, not in the expected direction. Within the implementation literature, provider perspectives are seen as precursors to intervention effects and ultimate participant satisfaction (e.g., Proctor et al., 2011), while participant satisfaction has long been conceptualized as a precursor to service outcomes within the program evaluation literature (e.g., Godley et al., 1998). We found no clear relationship in our analyses between provider perspectives and participant satisfaction in post hoc tests, but we did find that provider and participant perspectives were uniquely and differentially related to early (provider) and medial (participant) outcomes in our program theory. These findings raise important questions regarding the complexity of the relationship between participant and provider perspectives and intervention outcome in the development of transition (and likely other) services for youth in out-of-home care. To our knowledge, a potential interaction or other association between provider and participant perspectives has not been investigated previously in clinical, psychological, or social intervention research (e.g., Ryan-Bengtsson et al., 2025; Sundell & Olsson, 2021), but instead, participant perspectives and provider perspectives have been considered in isolation from each other. Both being found, individually, to be important for ultimate, more distal, intervention outcomes.
Fourth, we were interested in exploring the extent to which subgroup characteristics moderate outcomes. We found several associations that are candidates for consideration in developing MCMW further. First, participants who were 18 years or older fared better in relation to perceived self-efficacy in the MCMW group than younger participants. This was the only moderating effect found for age, but it may be an indication that the age range for inclusion in MCMW is too broad. Prior studies of interventions to improve outcomes for young people leaving the OHC system (Taylor et al., 2024) have typically identified outcomes in the 18–21 age range and services earlier. Our findings raise questions as to whether transition services should be provided later to avoid potential negative effects. Second, MCMW was not as successful with participants who do not have Swedish citizenship in terms of developing daily routines as SAU. This result is difficult to interpret and, as such, deserves further investigation, which can more qualitatively explore non-citizen youth's use of time. A gap between immigrant and non-immigrant use of time has been investigated in previous research (Chen, 2022; Kuhlemann, 2022); however, this literature has not typically included adolescent populations. Our findings may be due to the types of routines investigated in this study, which may not fully capture activities typically engaged in by young people who lack citizenship. Third, MCMW tended to fare better with participants who had already moved out of OHC. As the move from OHC is a time of great instability coupled with comparatively less social support (Arnett, 2007; Sulimani-Aidan, 2017a, 2017b), the provision of MCMW at this time point specifically may be especially important. All of these factors are important for the further development and study of MCMW.
This study offers several important strengths. First, the research aims, questions, and methods were presented in a study protocol prior to gathering data and conducting the analyses (Skoog et al., 2024). This arguably increases transparency, credibility, and methodological rigor. Second, the study was implemented under naturalistic conditions, increasing its external validity and generalizability to real-world practice settings. Third, the study used validated and psychometrically sound measures across a wide range of domains relevant to youth transitioning from OHC. Additionally, the diverse sample improves the generalizability of findings to various care-leaving contexts.
At the same time, the study also has limitations that need to be acknowledged when interpreting the results. First, although a priori power analyses were conducted, inequalities in group size, attrition, and subgroup variation may have limited our ability to detect significant effects, especially in the moderation analyses. Relatedly, the study did not have the power to examine potential nested structures (e.g., clustering by site or provider). Second, although implementation measures were included, the study lacked a robust fidelity assessment, making it difficult to draw firm conclusions about intervention delivery quality. Development of fidelity measures for use with MCMW is planned in relation to ongoing work with the intervention's development. Third, the MCMW group had higher baseline scores on some outcomes, and, although these were controlled in the analyses conducted, this complicates causal attribution. Fourth, the moderation analyses were exploratory in nature and should be interpreted with caution given the use of a more liberal significance threshold. It should be noted, however, that most of the significant findings were found at the p ≤ .05 probability level. Finally, the use of self-reports increases the risk of validity threats such as social desirability bias or biases due to limitations in participant self-insight.
This study offers several implications for policy, practice, and research focused on supporting young people transitioning from OHC to independent living. The observed improvement in perceived social support among participants in MCMW, alongside positive trends in competence, provides promising evidence for the value, and therefore implementation, of structured, youth-centered interventions—especially in contexts like Sweden, where formal transition support is often lacking. Our findings call attention to the need to develop national frameworks and policies that address the gap in care-leaving services. Enhanced social support, in particular, may serve as a protective factor during this vulnerable transition (Bennett et al., 2024), making it a strategic target for investment.
In relation to practical implementation, MCMW demonstrates feasibility and acceptability among providers, but variability in delivery and outcomes points to a potential need for better implementation support and monitoring. Similarly, an increased understanding of how training (in the case of MCMW, 4 ½ days) impacts professional practice as relates to youth-centered practice is warranted as our investigation showed improvements in the MCMW group above those in the SAU group despite a seemingly low delivery rate. Results also suggest that timing of the support matters—older youth and those who had already exited OHC appeared to benefit more, while noncitizen youth may require more tailored support. Finally, the current findings underscore the importance of exploring long-term effects, improving fidelity measures, and examining the complex associations between provider and participant perspectives in future research. It is also important to carefully consider and select intermediate and outcome measures that align with the intervention's theory and components, and that demonstrate strong psychometric properties. A final recommendation for future studies is to more closely examine and describe SAU. This is important for many reasons, including that the control condition could include elements that overlap with the intervention and thus mask (some of) the intervention effects.
Footnotes
Author Contributions
The trial was registered with ClinicalTrials.gov (Identifier: NCT05813197). The authors contributed to the study as follows: conceptualization (TMO, MB, and TS); methodology (TMO, MB, and TS); formal analysis (TMO); investigation (TMO and MK); resources (TMO, MB, and TS), data curation (MK); writing–original draft preparation (TO, MK, MB, DK, and TS); writing–review and editing (TMO, MK, MB, DK, and TS); supervision (TMO); project administration (TMO, MK, and DK); funding acquisition (TMO, MB, and TS). The trial sponsor is the Department of Social Work, School of Health and Welfare, Jönköping University, P.O. Box 1026, 551 11 Jönköping, Sweden.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Swedish Research Council for Health, Working Life and Welfare grant #2021-01352.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.