
Abstract
Purpose
This study examined the effectiveness of Strengths-Based Cognitive Behavioral Therapy (SBCBT) in reducing psychological distress and enhancing resilience among university students.
Methods
A longitudinal randomized controlled trial was conducted with 60 students experiencing mild-to-moderate depression, anxiety, and stress and low resilience. Participants were randomly assigned to either an 8-week SBCBT intervention or a Cognitive Behavioral Therapy-based self-help control condition. Outcomes were assessed at baseline, postintervention, and one-month follow-up using the depression, anxiety, and stress and Brief Resilience Scale.
Results
Generalized Estimating Equations revealed significant Time × Group interactions across all outcomes. In the SBCBT group, depression decreased from 14.62 to 9.19, anxiety from 11.08 to 8.01, and stress from 20.45 to 13.45. Resilience increased from 2.41 to 3.48. Between-group analyses indicated large effect sizes, particularly for stress reduction (d = −1.08) and resilience improvement (d = 1.65).
Discussion
Findings support SBCBT as an effective, resilience-focused intervention for improving student mental health and well-being in university settings.
Mental health challenges have emerged as a critical public health issue worldwide, with increasing prevalence across diverse populations (Wainberg et al., 2017). University students represent one of the most vulnerable groups, as they often face multiple, intersecting stressors that negatively influence their well-being (Barbayannis et al., 2022; Gao et al., 2025). These include demanding academic workloads, financial strain, difficulties in building and maintaining social networks, and the challenges of adapting to new living environments (Beiter et al., 2015; Kirkbride et al., 2024; Stallman, 2010). Research has consistently shown that university students report significantly higher levels of depression, anxiety, and stress (DASS-21) compared to their nonstudent peers (Eisenberg et al., 2007; Larcombe et al., 2016; Mofatteh, 2021). The onset of these mental health problems during early adulthood is particularly concerning, as it can disrupt developmental milestones such as identity formation, career planning, and the establishment of long-term relationships (Schlack et al., 2021; Duffy et al., 2020). Furthermore, untreated psychological distress in students has been linked to academic underperformance, dropout, impaired social functioning, and long-term adverse health outcomes (Hunt & Eisenberg, 2010). Thus, the mental health of university students is not only a matter of individual well-being (Gao et al., 2025) but also a broader societal concern with implications for educational systems, healthcare services, and workforce development (Hyseni Duraku, Davis & Hamiti, 2023; Li et al., 2025).
Within this context, resilience has gained prominence as a central construct in understanding adaptive responses to adversity (Infurna et al., 2024). Resilience is generally defined as the capacity to withstand, adapt to, and recover from significant stress or trauma, while maintaining or regaining psychological well-being (Masten, 2014). Importantly, resilience is now widely conceptualized as a dynamic process that develops through the interaction of individual, relational, and contextual factors, rather than as an immutable personal trait (Ungar, 2011). The ecological model of resilience emphasizes that protective processes operate across multiple domains, including cognitive (e.g., problem-solving, flexible thinking), emotional (e.g., regulation of negative affect, positive appraisal), behavioral (e.g., persistence, goal-directed actions), interpersonal (e.g., supportive relationships, social competence), and physical (e.g., adequate sleep, physical activity) (Troy et al., 2023; Fergus & Zimmerman, 2005). These multidimensional resources act as buffers that can reduce the negative impact of challenging life situations, such as poverty, discrimination, chronic illness, or social exclusion. By doing so, they promote positive developmental outcomes, even in the face of significant challenges. During adolescence and emerging adulthood periods marked by exploration, identity formation, and increased sensitivity to stress, the development of resilience is especially vital (Xing, Xu, Li & Luo, 2023; Taylor et al., 2017). Interventions that enhance resilience have been shown to reduce psychological distress, enhance academic performance, and strengthen social-emotional competencies (Durlak et al., 2011; Hartley, 2011; Pan & Zhuang, 2024). Resilience was selected as the central intervention target because it is a key protective factor against psychological distress in university students. Given the high levels of academic stress and emotional difficulties in this population, strengthening resilience is expected to enhance adaptive coping, reduce symptoms of DASS-21, and support longer-term psychological well-being, making it a theoretically and practically justified focus of intervention.
Cognitive Behavioral Therapy (CBT) is one of the most extensively researched and empirically validated interventions for mental health problems, with demonstrated efficacy in reducing DASS-21 across diverse populations (Hofmann et al., 2012). The foundational principle of CBT is that maladaptive thoughts and behaviors contribute to emotional distress, and that modifying these cognitions and behaviors can promote more adaptive functioning. Traditional CBT interventions focus on identifying and restructuring dysfunctional beliefs, practicing adaptive coping skills, and engaging in behavioral activation to improve emotional well-being. Contemporary developments in psychotherapy highlight the limitations of a solely deficit-based approach and emphasize the importance of integrating recovery-oriented and strengths-based perspectives (Rashid, 2015; Slade, 2010). Recovery-oriented approaches prioritize personal growth, meaning, and empowerment, shifting the therapeutic focus from symptom reduction to the cultivation of personal strengths and long-term well-being.
Although CBT is well-established in reducing psychological distress across populations (Hofmann et al., 2012), recent developments in psychotherapy have increasingly emphasized the integration of strengths-based and resilience-oriented approaches to enhance treatment outcomes. Strengths-based CBT (SBCBT) extends traditional CBT by shifting the therapeutic focus from symptom reduction toward the identification and systematic utilization of personal strengths as central mechanisms of change (Padesky & Mooney, 2012). This strengths-oriented perspective aligns with recovery-focused and positive psychology approaches that emphasize psychological growth, meaning, and empowerment alongside symptom alleviation (Rashid, 2015; Slade, 2010). Strengths-based and recovery-oriented interventions have been shown to improve psychological functioning by enhancing individuals’ perceived resources, self-efficacy, and adaptive coping capacities rather than focusing solely on psychopathology (Slade, 2010; Yuen et al., 2020). Empirical studies directly examining fully integrated SBCBT remain limited, particularly among university students. Most existing research has examined CBT or strengths-based approaches separately rather than in a unified framework, highlighting the need for further randomized controlled trials testing the combined effect of SBCBT on both psychological distress and resilience in the student population.
Strengths-based CBT represents one such adaptation, blending the core methods of CBT with strategies explicitly designed to build resilience and psychological strengths. The SBCBT encourages individuals to recognize and enhance their self-efficacy, cultivate positive emotions, foster a sense of meaning and purpose in life, and leverage personal and social resources to navigate adversity (Yuen et al., 2020; Padesky & Mooney, 2012). Empirical studies suggest that integrating strengths-based or spiritual elements into CBT can yield additional benefits. Spiritually adapted CBT has been shown to improve hope, peace, and spiritual health in individuals recovering from opioid use disorder (Sonbol et al., 2025). Acceptance-and strengths-focused interventions such as the “EmpowerU” program have demonstrated success in enhancing resilience, promoting self-discovery, and improving overall well-being among adolescents and university students (Arslan, Aydoğdu & Uzun, 2025). These findings align with the behavioral activation model, which emphasizes that consistent engagement in meaningful, goal-directed activities can alleviate depressive symptoms and reinforce adaptive patterns of behavior (Martell et al., 2010). Collectively, such approaches highlight the therapeutic value of interventions that go beyond correcting deficits to actively build enduring psychological resources (Wang & Feng, 2022).
Despite these encouraging findings, the evidence for SBCBT is still limited, especially among university students. Although resilience training, CBT, and strengths-based approaches have each been shown to be effective on their own, only a small number of experimental studies have tested the combined use of strengths-based strategies within a CBT framework to improve resilience and mental health in student populations (Xiang, Wan & Zhu, 2025). This gap is important to address, as university students are a vulnerable group who face a range of academic, developmental, and psychosocial stressors. Improving resilience in this population is important not only for mental health but also for academic functioning and longer-term well-being. This intervention was guided by a clear logic model linking student needs, intervention mechanisms, and expected outcomes. University students often experience elevated psychological distress due to academic demands and limited coping resources, which are typically maintained by maladaptive cognitions and reduced self-efficacy. Accordingly, SBCBT was selected because it integrates cognitive restructuring with strengths identification and resilience-building strategies. The intervention components (e.g., strengths identification and application, and Personal Model of Resilience [PMR] development) are designed to enhance adaptive thinking and coping, leading to reduced DASS-21, and improved resilience. Therefore, this study aims to examine the effectiveness of a SBCBT intervention among university students. The main aim is to assess whether SBCBT reduces symptoms of DASS-21, and the secondary aim is to examine whether it improves resilience (Brief Resilience Scale, BRS). By combining standard CBT techniques with strengths-based strategies, this study seeks to provide evidence for a more integrated approach to intervention and contribute to research on resilience and mental health in university students.
Method
Research Design
This study employed a repeated-measures, randomized controlled experimental design with two parallel groups (intervention and control). Assessments were conducted at three time points: baseline (pretest), immediately after the intervention (posttest), and at follow-up (4 weeks after posttest).
Participants and Sampling
The target population of this study comprised undergraduate university students. Recruitment was conducted through the distribution of brochures across various campus platforms, utilizing convenience sampling. Students were eligible to participate if they (a) provided informed consent, (b) scored within the mild-to-moderate range on the DASS-21 (Lovibond & Lovibond, 1995), and (c) obtained a low score on the BRS (Smith et al., 2008). Sample size estimation was conducted using G*Power version 3.1.9.7 (Faul et al., 2007). With parameters set at a medium effect size (f = 0.25), an alpha level of .05, and a power of .95, the required sample size was determined to be 60. Accordingly, 60 eligible students were recruited and randomly allocated into two equal groups of 30 participants each (intervention and control) using computer-generated random numbers. To ensure allocation concealment, the computer-generated random allocation sequence was held by an independent researcher who was not involved in the recruitment or assessment processes. The primary investigator was only informed of a participant's group assignment after the participant had formally provided informed consent and completed all baseline assessments.
Procedure
Participants were recruited between June and October 2025 following ethical approval through recruitment brochures disseminated on student platforms. Following approval, recruitment brochures were disseminated on various student platforms. After screening the responses, 70 participants who met the inclusion criteria were contacted and enrolled, with 35 participants randomly allocated to each group. During the intervention and follow-up phases, 10 participants discontinued their participation due to scheduling difficulties, including competing personal and family commitments, time constraints, and travel-related challenges, as well as nonresponsiveness to repeated scheduling attempts) (see Figure 1). Consequently, the final analytic sample comprised 60 participants, with 30 participants in each group.
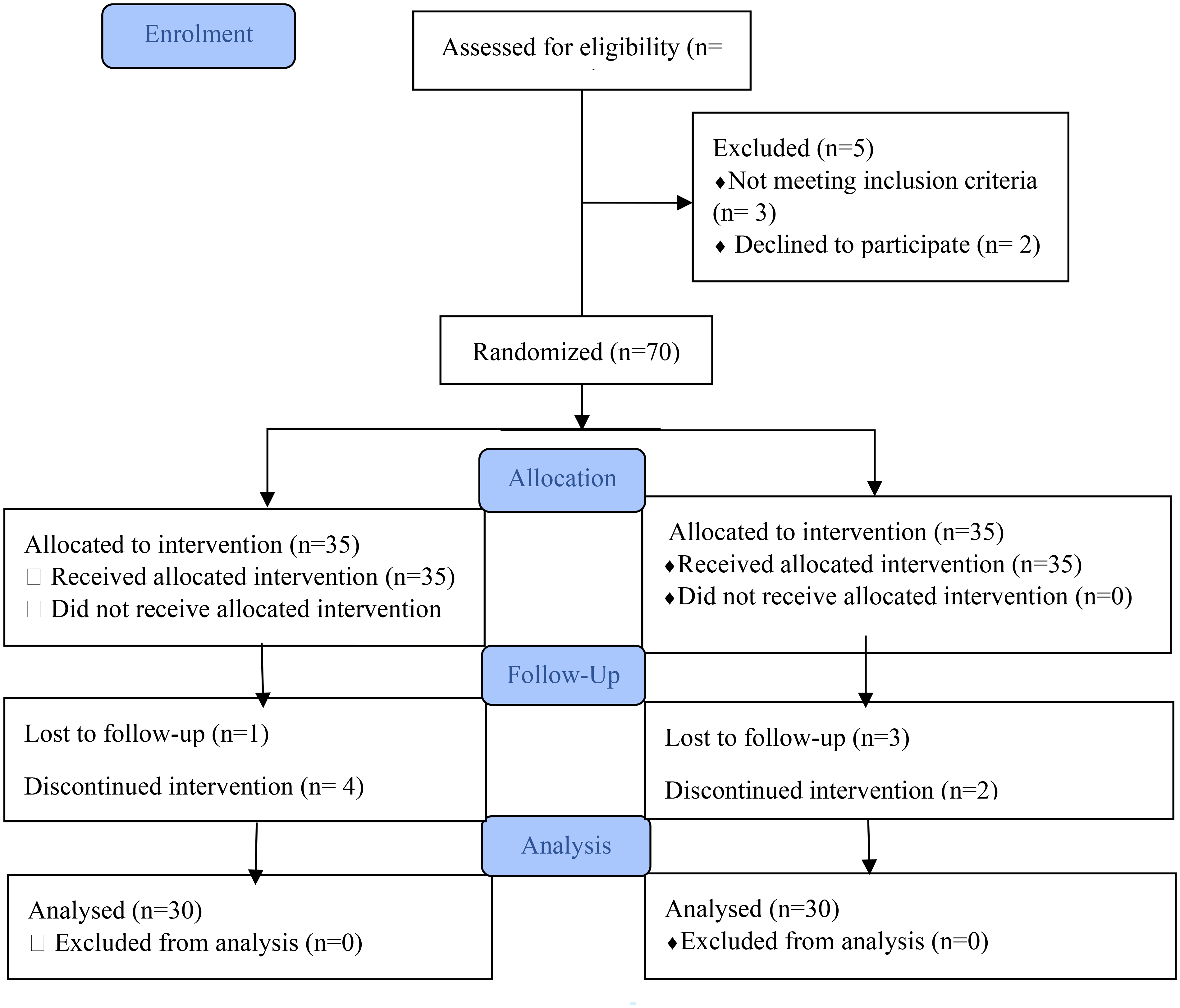
CONSORT diagram for enrollment of the participants.
Assessments were conducted at baseline (pretest), immediately after the 8-week intervention (posttest), and 4 weeks later (follow-up). The intervention followed Padesky and Mooney's (2012) four-step SBCBT model. The process began with searching for strengths, where participants were guided to identify and acknowledge their personal assets and positive qualities. Building on this foundation, they were encouraged to construct a PMR by developing an individualized framework that highlighted how these strengths could be organized and mobilized to foster resilience. Once the PMR was established, participants learned to apply it to areas of difficulty, using their resilience strategies to address and manage real-life challenges. Finally, participants engaged in practicing resilience, which involved reinforcing and consolidating these skills through repeated application across various contexts, thereby promoting long-term adaptability and psychological well-being.
Intervention Group
Participants in the intervention group engaged in an 8-week SBCBT program grounded in the model proposed by Padesky and Mooney (2012). The sessions were conducted face-to-face in small group settings, once per week, with each session lasting approximately 60 min. Each intervention activity was selected based on cognitive-behavioral and strengths-based theoretical principles to ensure alignment between therapeutic mechanisms (e.g., cognitive restructuring, self-efficacy enhancement, and adaptive coping) and targeted outcomes of reduced psychological distress and improved resilience. The SBCBT framework is specifically designed to enhance resilience through a structured four-step process. The first step, searching for strengths, involved guiding participants to identify and acknowledge their personal strengths and positive qualities.
The second step involved the development of a PMR, in which participants integrated identified strengths into coherent adaptive strategies. The third step focused on applying the PMR to personally relevant difficulties, enabling participants to translate strengths into adaptive responses to real-life challenges. The final step emphasized repeated practice of resilience strategies across contexts to facilitate skill consolidation and long-term adaptation. Collectively, this process reflects a shift from a deficit-oriented approach toward strength development and psychological growth.
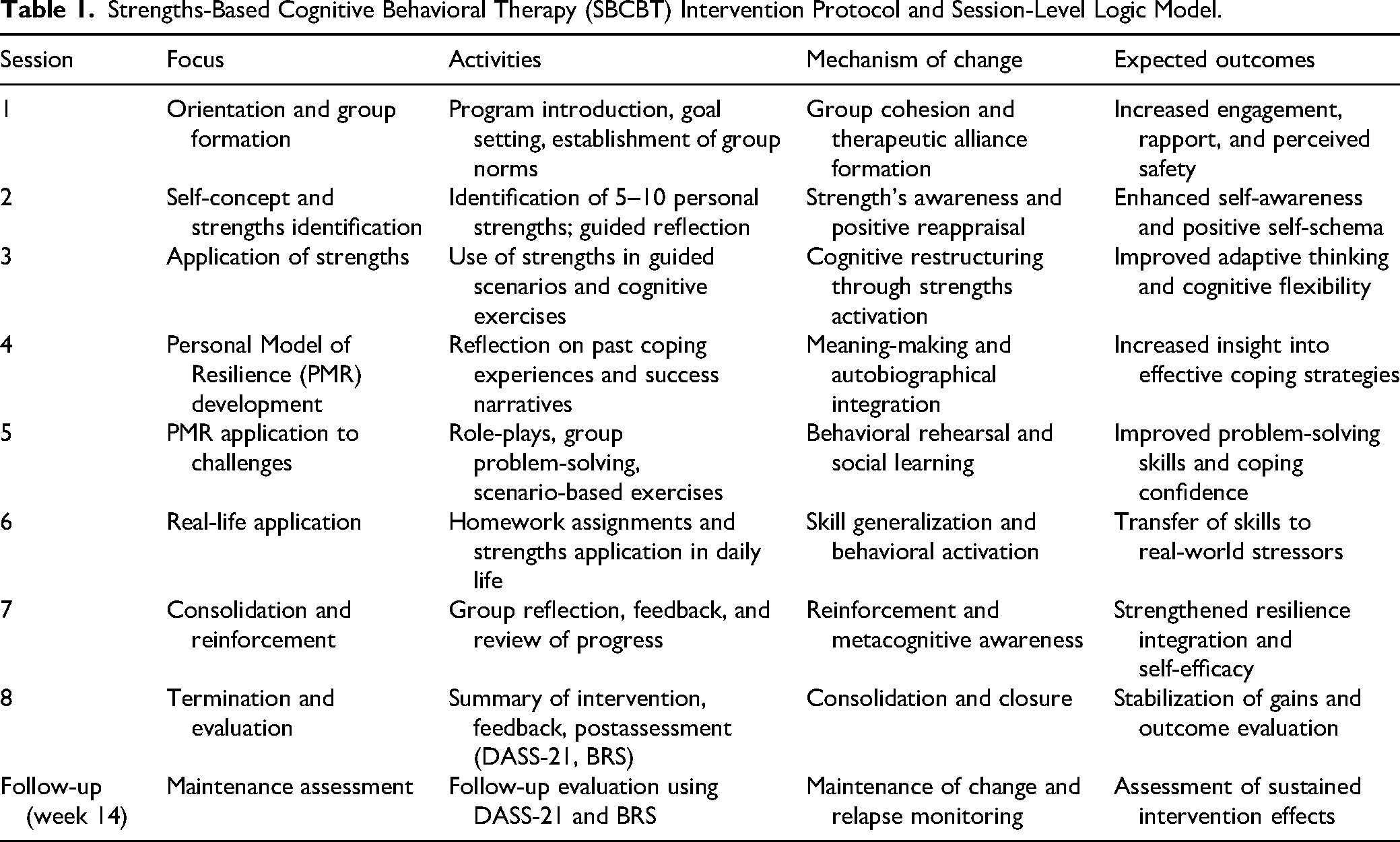
The SBCBT was delivered in a group format due to its alignment with social learning and cognitive-behavioral principles. Group-based delivery facilitates peer learning, normalization of shared experiences, and social reinforcement of adaptive cognitions and behaviors. It also enables participants to benefit from both therapist-guided strengths identification and peer modeling, which may enhance the internalization of resilience-related skills. Previous research supports the effectiveness of group CBT in reducing psychological distress and improving accessibility and efficiency in university settings (Hofmann et al., 2012). Accordingly, the group format was considered both theoretically consistent and practically suitable for the present student sample. Table 1 presents the weekly intervention structure, including session objectives, core components, mechanisms of change, and expected outcomes.
Strengths-Based Cognitive Behavioral Therapy (SBCBT) Intervention Protocol and Session-Level Logic Model.
Control Group
Participants in the control group did not receive structured therapy. Instead, they were provided with written self-help materials derived from CBT principles, including worksheets and activities designed to promote reflective practice and basic coping strategies.
Treatment Fidelity
Treatment fidelity and intervention integrity were ensured through a fully manualized SBCBT protocol designed to maximize standardization and replicability. The manual specified detailed session-by-session objectives, structured therapeutic procedures, in-session activities, therapist prompts, and standardized homework assignments, thereby reducing variability in intervention delivery. Implementation fidelity was further strengthened through consistent adherence to the protocol across all sessions, supported by a structured adherence checklist completed by the therapist after each session to monitor compliance with prescribed procedures and session content. In addition, periodic clinical supervision was conducted throughout the intervention to review session delivery, address potential deviations from the protocol, and minimize therapist drift. Although independent fidelity coding or formal interrater reliability assessment was not conducted, the combination of manualization, structured adherence monitoring, and ongoing supervision provided a robust framework for maintaining high levels of treatment integrity, implementation consistency, and methodological rigor across the trial.
Instruments
Depression, Anxiety, and Stress Scale-21 Items
The DASS-21, developed by Peter F. Lovibond and Sydney H. Lovibond at the University of New South Wales in 1995, is a widely used self-report instrument designed to assess emotional distress across three domains: DASS-21. Each domain contains seven items rated on a 4-point scale from 0 (“did not apply at all”) to 3 (“applied very much or most of the time”). To calculate scores, responses for each subscale are summed and then multiplied by two to correspond with the norms of the original 42-item version. Recommended severity cutoffs classify scores into normal, mild, moderate, severe, or extremely severe ranges: for depression (0–9 normal; 28 + extremely severe), anxiety (0–7 normal; 20 + extremely severe), and stress (0–14 normal; 34 + extremely severe). The DASS-21 is based on a dimensional model of psychological distress, distinguishing differences in severity rather than assigning categorical diagnoses. It has demonstrated high reliability and validity across diverse populations, with strong internal consistency for all subscales. While it offers a valuable snapshot of emotional states over the past week and is particularly useful for screening and monitoring changes over time
Brief Resilience Scale
The BRS, developed by Smith et al. (2008), is a concise tool designed to assess an individual's ability to bounce back or recover from stress. Unlike many other resilience measures that incorporate protective factors, such as coping strategies or social support, the BRS focuses specifically on resilience as a recovery process following adversity. It consists of six self-report items rated on a 5-point Likert scale ranging from 1 = Strongly Disagree to 5 = Strongly Agree. Three items (2, 4, and 6) are reverse-scored before calculating the total score, which ranges from 6 to 30. The mean score is then derived by dividing the total by 6. The interpretation of scores suggests that a mean between 1.00 and 2.99 indicates low resilience, 3.00 to 4.30 reflects normal resilience, and a mean of 4.31 to 5.00 indicates high resilience. Psychometric evaluations demonstrate strong reliability with Cronbach's alpha ranging from 0.80 to 0.91, along with evidence of validity as indicated by positive correlations with optimism, purpose in life, and social support, and negative correlations with anxiety, depression, negative affect, and perceived stress. The BRS has a one-factor structure representing “resilience as recovery” and is advantageous due to its brevity, direct measurement of the capacity to recover from stress, and applicability across clinical, educational, and research contexts.
Data Analysis
Prior to analysis, data were screened for missing values, normality, and outliers; no serious violations were detected. Descriptive statistics were first computed to examine group trajectories across DASS-21, and resilience at three assessment points (pretest, posttest, and follow-up). Generalized Estimating Equation (GEE) analyses were then conducted to evaluate group differences over time. Pairwise comparisons with mean differences (MDs) and 95% confidence intervals were used to identify within-group changes across time points. The GEE was specified with an appropriate working correlation structure, and baseline values were included as covariates where applicable. Effect sizes (Cohen's d) were calculated for both within-group and between-group comparisons. Within-group effect sizes were computed using the mean change divided by the pooled standard deviation of the respective time points. Between-group effect sizes were calculated using the difference between group means divided by the pooled standard deviation. All analyses revealed significant group × time interactions, indicating that the intervention group showed substantial reductions in DASS-21, as well as significant increases in resilience, compared to the control group, which remained largely stable.
Posttreatment, the SBCBT group will display statistically significantly lower Depression scores, compared to the control group, as assessed by the Depression subscale of the DASS-21.
Posttreatment, the SBCBT group will display statistically significantly lower Anxiety scores, compared to the control group, as assessed by the Anxiety subscale of the DASS-21.
Posttreatment, the SBCBT group will display statistically significantly lower Stress scores, compared to the control group, as assessed by the Stress subscale of the DASS-21.
Posttreatment, the SBCBT group will display statistically significantly higher Resilience scores, compared to the control group, as assessed by the BRS.
Results
Demographics
A total of 60 undergraduate students participated in the study, with 30 allocated to the intervention group and 30 to the control group. Participants were aged between 19 and 23 years (M = 20.78, SD = 0.86). The overall sample included 38 females (63.3%) and 22 males (36.7%). In the intervention group, 20 participants (66.7%) were female and 10 (33.3%) were male, whereas the control group comprised 18 females (60.0%) and 12 males (40.0%). The groups were comparable in terms of gender distribution, indicating successful randomization.
Baseline Equivalence
All participants were enrolled in the Psychology and Counselling program. Independent samples t-tests and chi-square analyses confirmed baseline equivalence across all primary variables. No statistically significant differences were observed between the intervention and control groups in age (p = .658), depression (p = .818), anxiety (p = .779), stress (p = .378), or resilience (p = .486) at baseline (see Table 2). The participants reported moderate psychological distress at baseline, with a combined mean DASS-21 score of approximately 47.33, consistent with the study's inclusion criteria.
Baseline Demographic and Clinical Characteristics of the Study Participants.
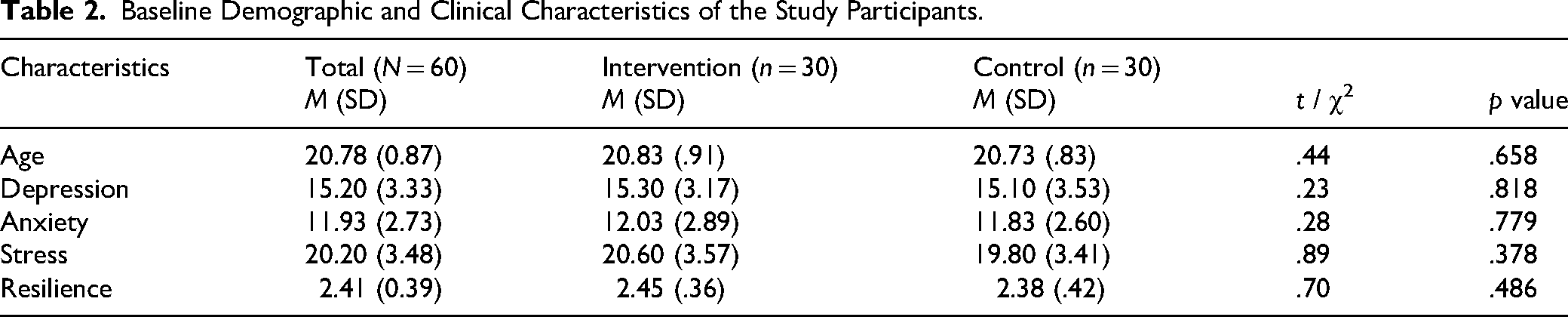
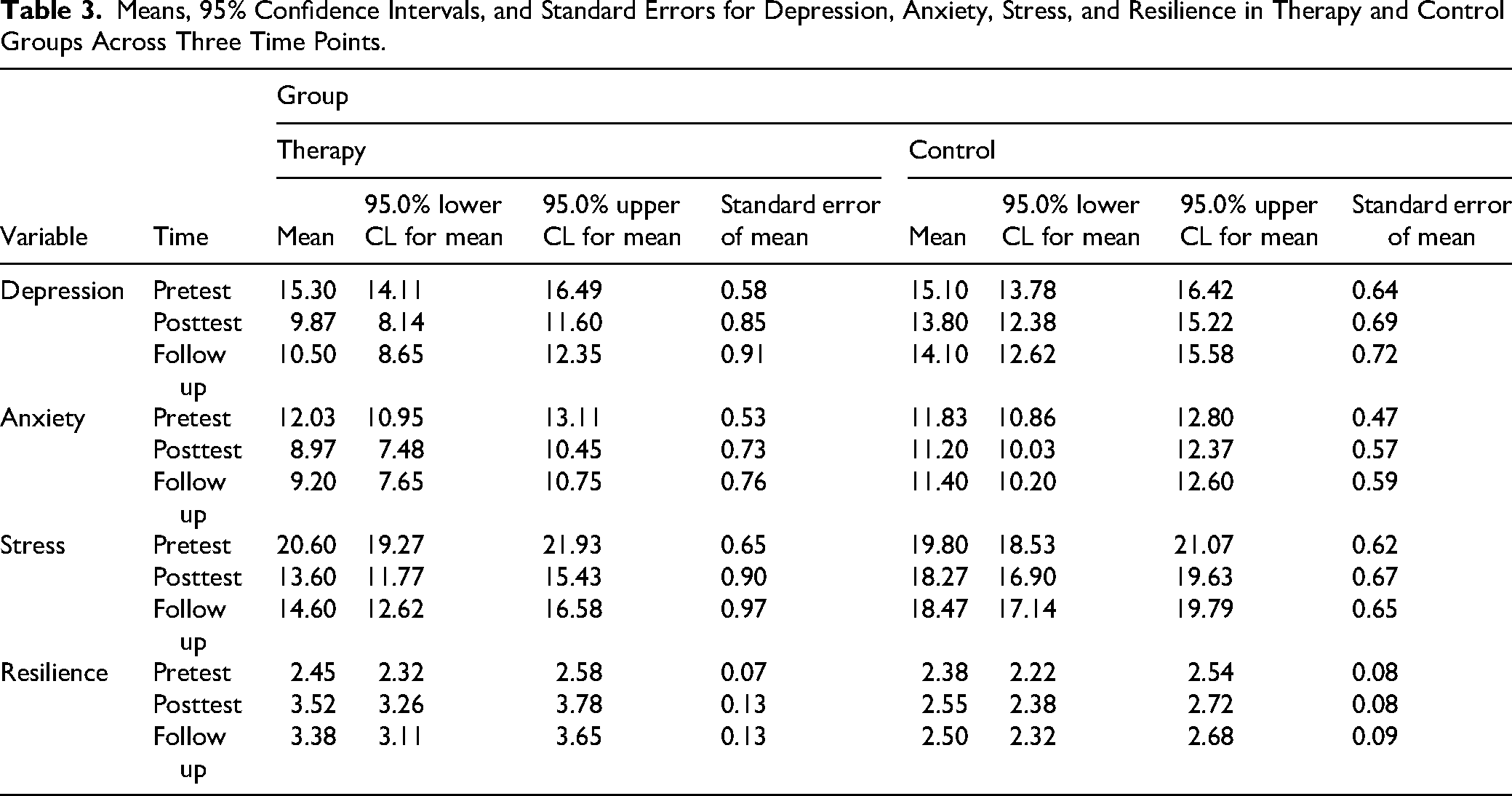
Table 3 illustrates distinct trajectories of psychological adjustment in the therapy and control groups across three assessment points.
Means, 95% Confidence Intervals, and Standard Errors for Depression, Anxiety, Stress, and Resilience in Therapy and Control Groups Across Three Time Points.
Hypothesis 1: Depression
Hypothesis 1 predicted that, posttreatment, participants in the SBCBT group would report significantly lower depression scores than participants in the control group, as measured by the Depression subscale of the DASS-21. Descriptive findings indicated a marked reduction in depression among participants receiving SBCBT. Mean depression scores decreased from 15.30 (95% CI [14.11, 16.49]) at pretest to 9.87 (95% CI [8.14, 11.60]) at posttest and remained substantially below baseline at follow-up (M = 10.50, 95% CI [8.65, 12.35]). In contrast, participants in the control group demonstrated only minor fluctuations across the three assessment points (pretest M = 15.10, posttest M = 13.80, follow-up M = 14.10; see Figure 2). The GEE analysis further confirmed that depression scores were significantly lower in the SBCBT group than in the control group at both posttest (MD = −3.93, p = .001) and follow-up (MD = −3.60, p = .003). These findings indicate that SBCBT produced meaningful and sustained reductions in depressive symptoms. Therefore, Hypothesis 1 was supported.
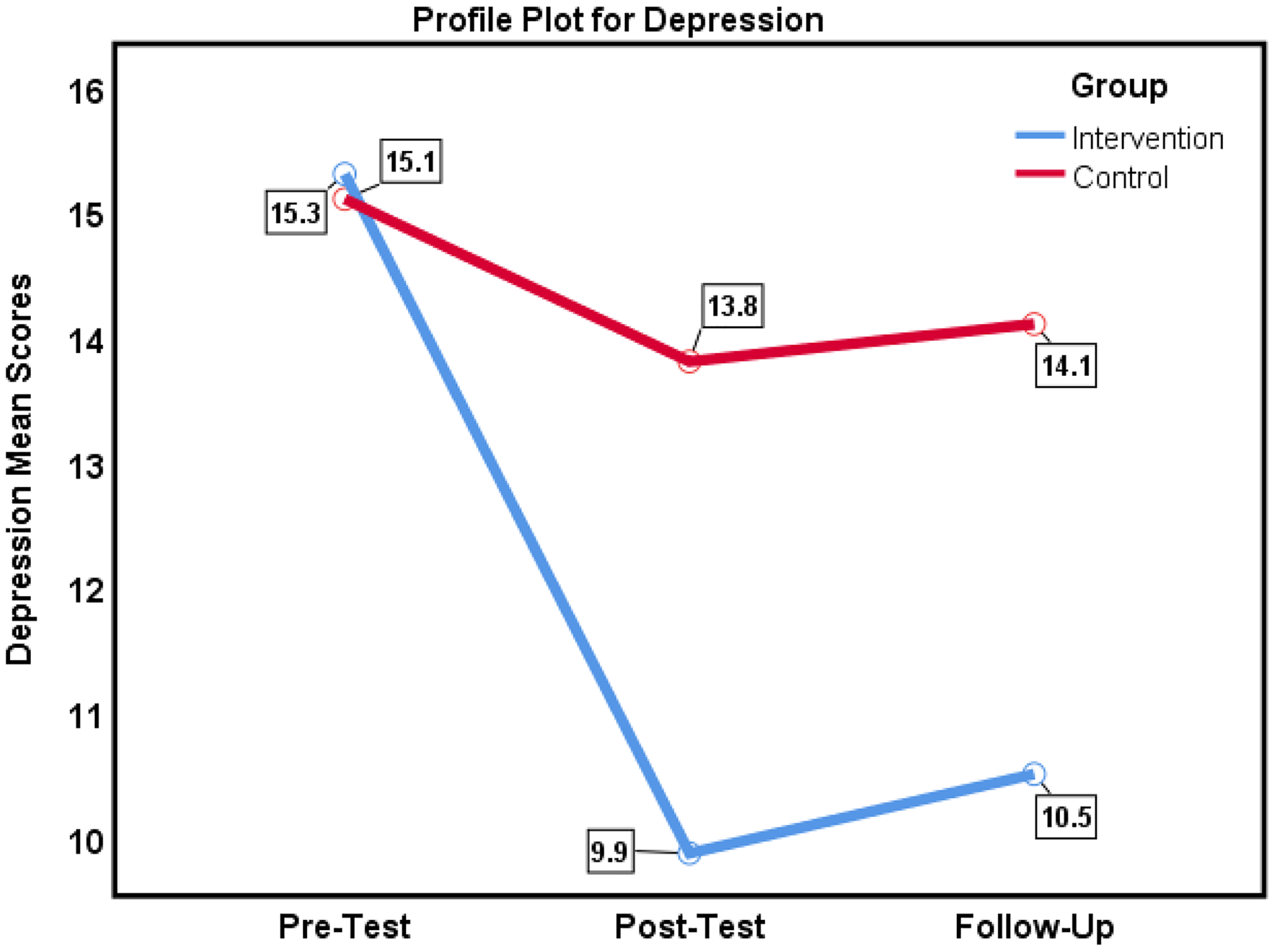
The depression scores for intervention and control groups across baseline, posttest, and one-month follow-up.
Hypothesis 2: Anxiety
Descriptive findings indicated a substantial reduction in anxiety among participants receiving SBCBT. Mean anxiety scores decreased from 12.03 (95% CI [10.95, 13.11]) at pretest to 8.97 (95% CI [7.48, 10.45]) at posttest and remained relatively stable at follow-up (M = 9.20, 95% CI [7.65, 10.75]). In contrast, anxiety scores in the control group showed minimal variation across the three assessment points (M range = 11.20–11.83; see Figure 3). Descriptive results suggest that participants who received SBCBT experienced meaningful reductions in anxiety symptoms, whereas little change was observed in the control group.
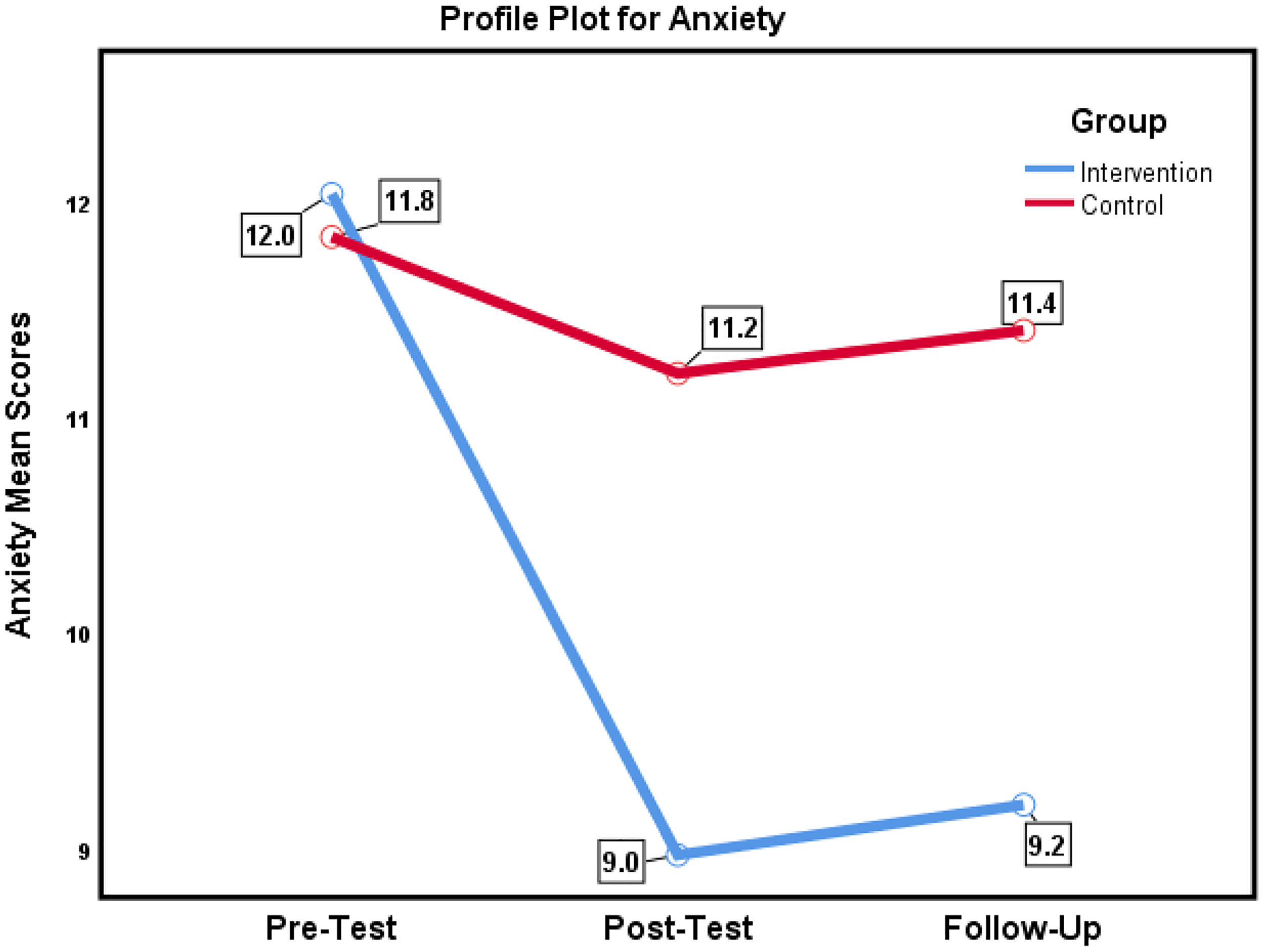
The anxiety scores for intervention and control groups across baseline, posttest, and one-month follow-up.
Hypothesis 3: Stress
Descriptive findings indicated a marked reduction in stress among participants receiving SBCBT. Mean stress scores decreased from 20.60 (95% CI [19.27, 21.93]) at pretest to 13.60 (95% CI [11.77, 15.43]) at posttest, with scores remaining relatively stable at follow-up (M = 14.60, 95% CI [12.62, 16.58]). In contrast, the control group demonstrated only minor fluctuations across the three assessment points (pretest M = 19.80; posttest M = 18.27; follow-up M = 18.47; see Figure 4).
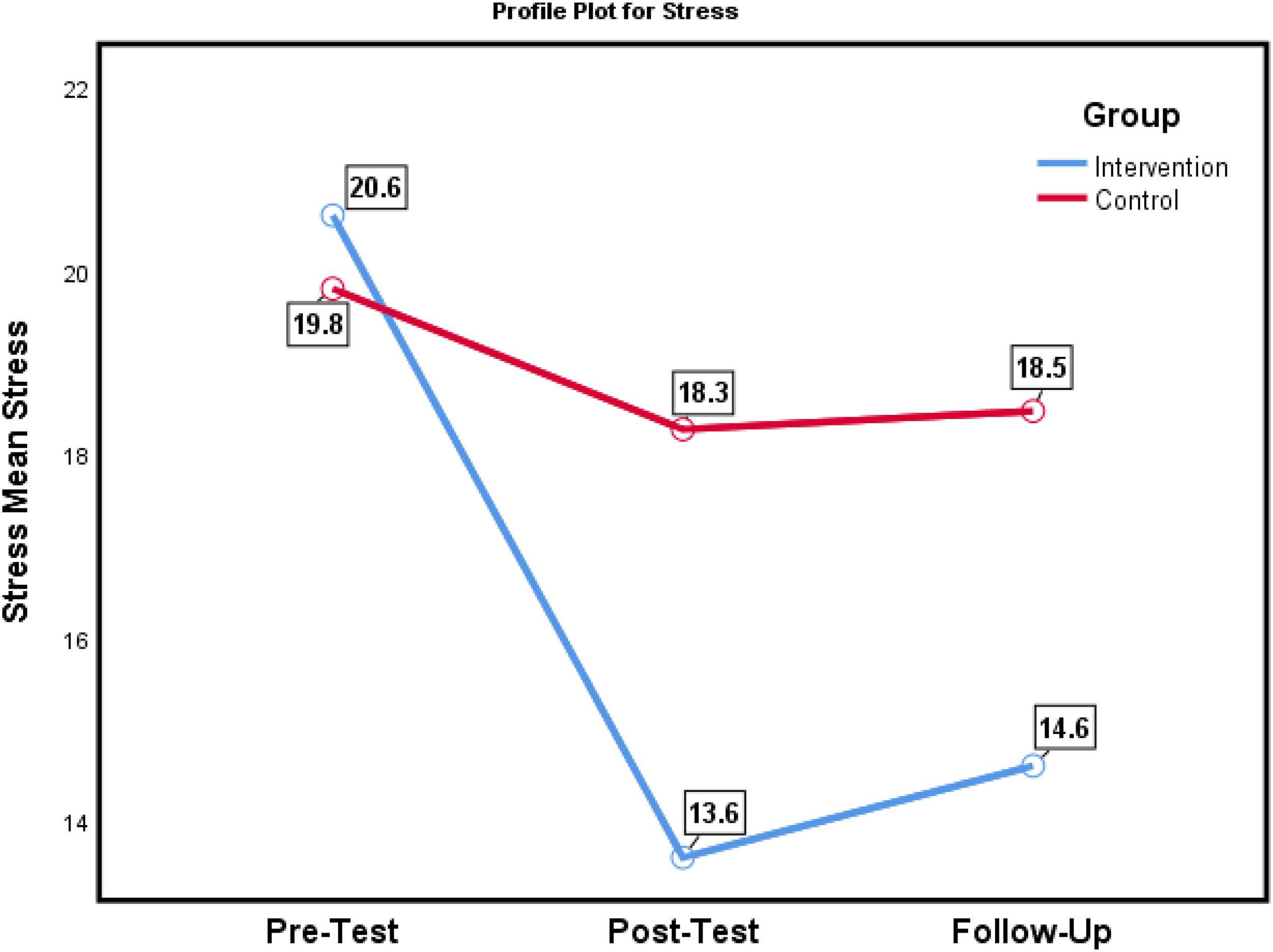
The stress scores for intervention and control groups across baseline, posttest, and one-month follow-up.
Hypothesis 4: Resilience
In contrast, resilience showed an increasing trend in the intervention group, rising from pretest (M = 2.45, 95% CI [2.32, 2.58]) to posttest (M = 3.52, 95% CI [3.26, 3.78]), with a small decline at follow-up (M = 3.38, 95% CI [3.11, 3.65]) while remaining above baseline levels. The control group demonstrated only negligible changes across assessments (M range = 2.38–2.55) (see Figure 5). These descriptive findings indicate that the intervention was associated with substantial reductions in DASS-21, alongside meaningful improvements in resilience, with effects largely maintained at follow-up. In contrast, the control group exhibited minimal changes across all outcomes.
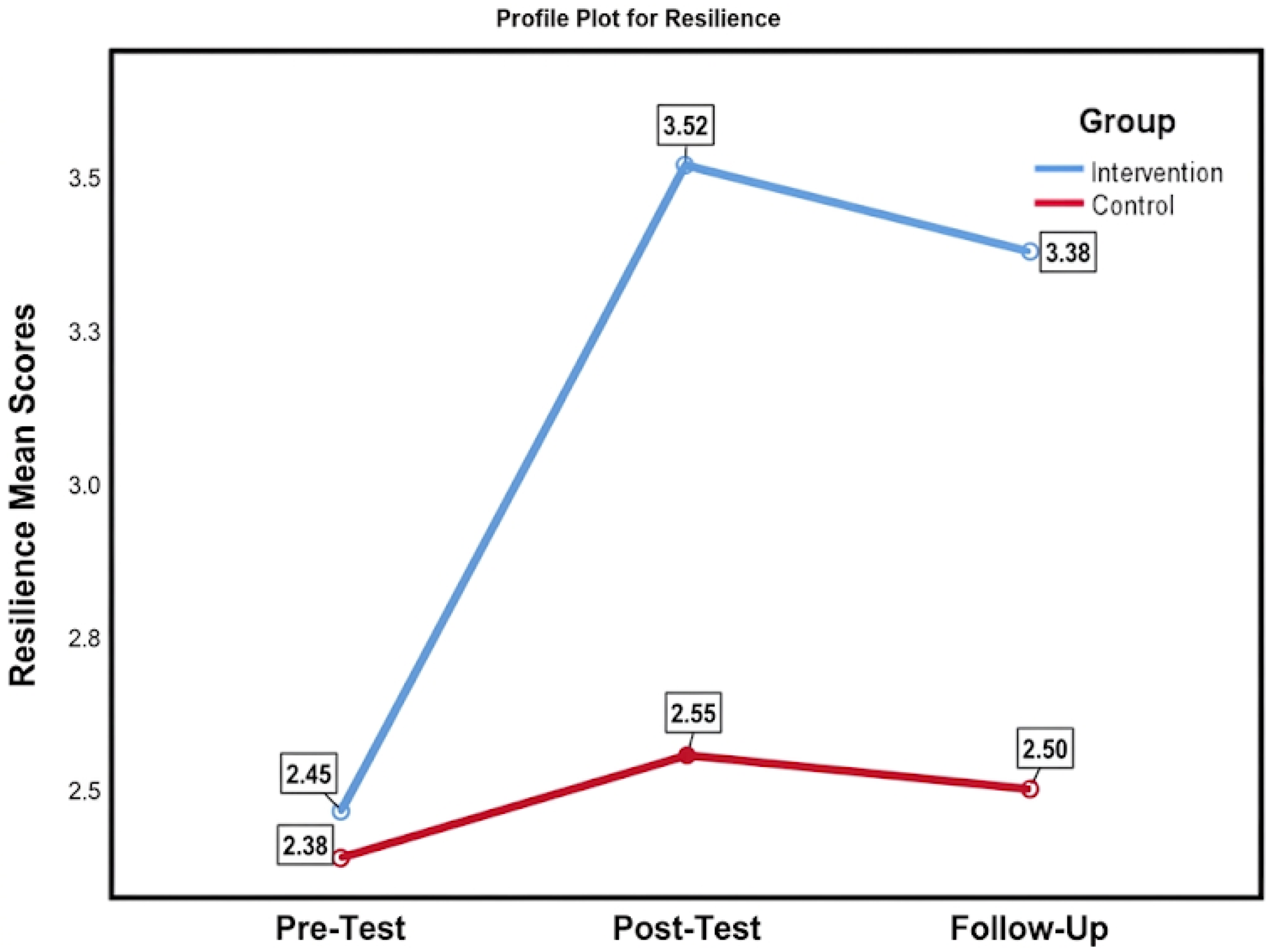
The resilience scale scores for intervention and control groups across baseline, posttest, and one-month follow-up.
Generalized Estimating Equations Analysis
The GEE analysis was employed to examine the longitudinal effects of the intervention across the four outcome variables (see Table 4). Baseline comparisons indicated no significant differences between the intervention and control groups across all measures (p > .05), confirming group equivalence prior to the intervention. The intervention group demonstrated significantly lower depression scores compared to the control group at posttest (MD = −3.93, 95% CI [−6.12, −1.74], p = .001) and follow-up (MD = −3.60, 95% CI [−5.92, −1.28], p = .003). Similarly, anxiety scores were reduced at posttest (MD = −2.23, 95% CI [−4.09, −0.38], p = .019) and follow-up (MD = −2.20, 95% CI [−4.12, −0.28], p = .026). Stress levels also showed significant reductions at posttest (MD = −4.67, 95% CI [−6.90, −2.43], p < .001) and follow-up (MD = −3.87, 95% CI [−6.20, −1.53], p = .002). Regarding resilience, the intervention group showed significantly higher scores than the control group at posttest (MD = 0.97, 95% CI [0.67, 1.27], p < .001) and follow-up (MD = 0.88, 95% CI [0.56, 1.20], p < .001). Effect sizes ranged from moderate to large, with d = 1.65 at posttest and d = 1.41 at follow-up, indicating robust improvements in adaptive functioning alongside reductions in psychological distress.
Results of Generalized Estimating Equations (GEE) in Total Professional Depression, Anxiety, Stress, and Resilience Score.
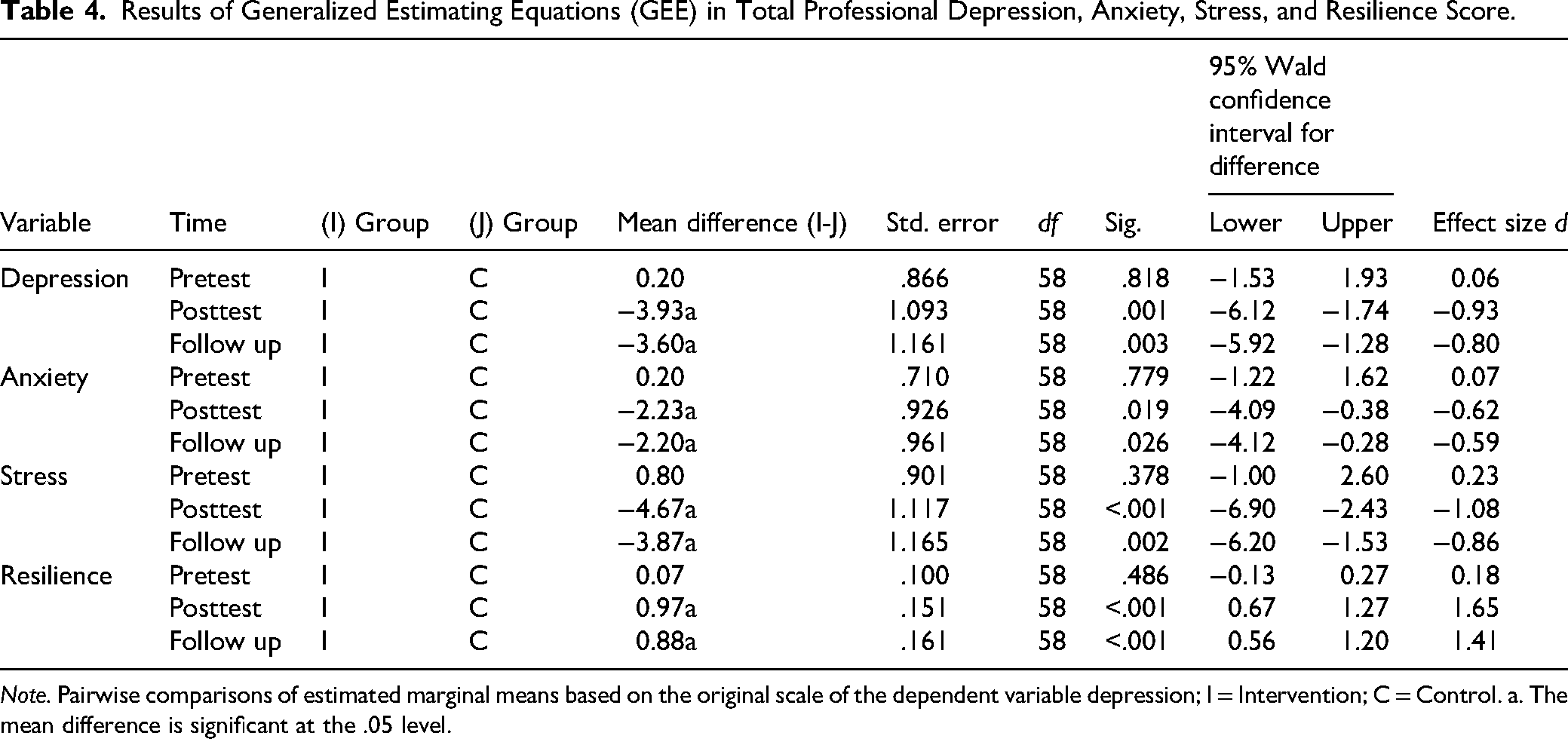
Note. Pairwise comparisons of estimated marginal means based on the original scale of the dependent variable depression; I = Intervention; C = Control. a. The mean difference is significant at the .05 level.
The pairwise comparisons revealed clear temporal changes in the intervention group relative to the control condition (see Table 5). A significant reduction in depression was observed in the intervention group from pretest to posttest (M_diff = 5.43, SE = 1.06, p < .001, 95% CI [3.25, 7.62], d = .93), which remained significant at follow-up (M_diff = 4.80, SE = 1.14, p < .001, 95% CI [2.46, 7.14], d = .76). The difference between posttest and follow-up was not statistically significant (M_diff = −0.63, SE = 1.24, p = .616, 95% CI [−3.19, 1.92]), suggesting that treatment gains were maintained over time. In contrast, no significant changes were detected in the control group across any time points (all p > .05). A similar pattern emerged for anxiety. The intervention group demonstrated a significant decrease from pretest to posttest (M_diff = 3.07, SE = .77, p < .001, 95% CI [1.50, 4.64], d = .73), as well as from pretest to follow-up (M_diff = 2.83, SE = .96, p = .006, 95% CI [0.87, 4.79], d = .54), whereas the posttest to follow-up comparison was not significant (M_diff = −0.23, SE = .90, p = .796, 95% CI [−2.06, 1.60]). Meanwhile, anxiety levels in the control group remained stable, with no statistically significant differences observed over time (all p > .05).
Pairwise Comparison of Professional Depression, Anxiety, Stress, and Resilience Scores Across Time.
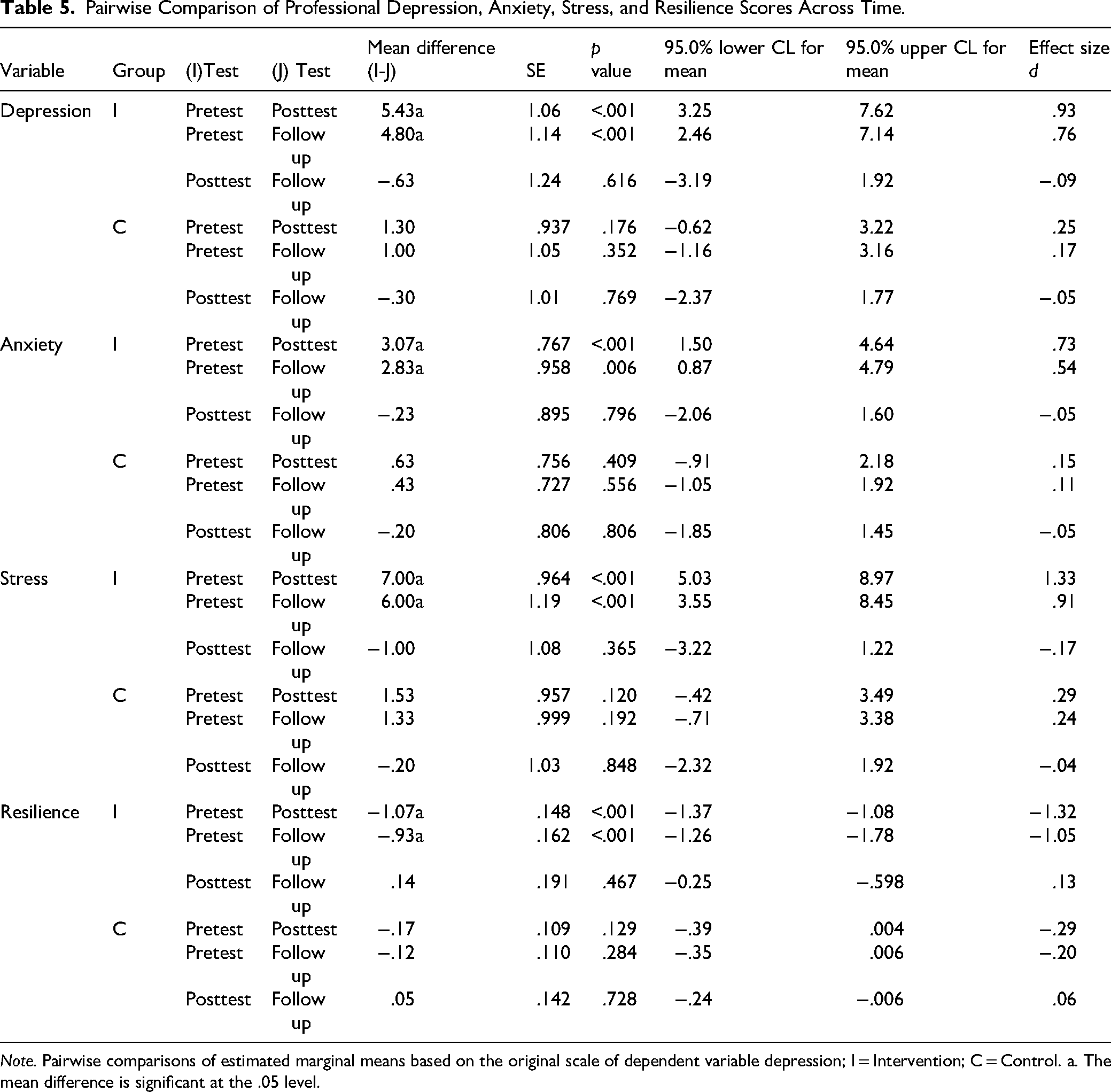
Note. Pairwise comparisons of estimated marginal means based on the original scale of dependent variable depression; I = Intervention; C = Control. a. The mean difference is significant at the .05 level.
With respect to stress, substantial reductions were evident in the intervention group. Scores decreased significantly from pretest to posttest (M_diff = 7.00, SE = .96, p < .001, 95% CI [5.03, 8.97], d = 1.33) and from pretest to follow-up (M_diff = 6.00, SE = 1.19, p < .001, 95% CI [3.55, 8.45], d = .91). However, the change between posttest and follow-up did not reach statistical significance (M_diff = −1.00, SE = 1.08, p = .365, 95% CI [−3.22, 1.22]), indicating stability of improvement. The control group, by comparison, did not show significant changes across any measurement points (all p > .05). Improvements in resilience further supported the effectiveness of the intervention. The intervention group showed a significant increase from pretest to posttest (M_diff = −1.07, SE = .15, p < .001, 95% CI [−1.37, −0.77], d = −1.32) and from pretest to follow-up (M_diff = −0.93, SE = .16, p < .001, 95% CI [−1.26, −0.60], d = −1.05). The posttest to follow-up change was not significant (M_diff = 0.14, SE = .19, p = .467, 95% CI [−0.25, 0.53]), indicating that gains were sustained rather than further increased. In contrast, resilience scores in the control group remained largely unchanged over time (all p > .05). The pairwise comparisons across time points were conducted to further examine within- and between-group changes. These analyses supported the primary GEE results.
Discussion
This randomized controlled trial evaluated the efficacy of SBCBT in improving psychological well-being among university students. Consistent with our hypotheses, participation in SBCBT produced substantial reductions in DASS-21, alongside significant improvements in resilience. Baseline equivalence across all measures confirmed the rigor of our randomization, allowing us to confidently attribute the observed changes to the intervention. These positive effects were evident immediately following the intervention and were largely maintained at the one-month follow-up, whereas the control group, which received only self-help materials, showed no meaningful change. Collectively, these findings provide strong evidence that SBCBT addresses both the reduction of psychological distress and the cultivation of adaptive psychological resources in vulnerable student populations.
The current findings both align with and extend the existing literature on mental health interventions for students. Recent meta-analyses of digital and in-person CBT programs for university students have traditionally shown small to moderate improvements in depression and anxiety (Li et al., 2025; Kambeitz-Ilankovic et al., 2022). In contrast, the effect sizes observed in this trial were exceptionally large (e.g., Cohen's d > 1.0 for stress reduction and resilience enhancement). This magnitude of change indicates that explicitly incorporating strengths-based strategies within a traditional CBT framework may synergistically enhance therapeutic effectiveness. This support calls for “next-generation” process-based CBT approaches that focus on resilience, coping self-efficacy, and positive adaptation, in addition to merely reducing symptoms (Çalışkan & Gökkaya, 2025).
The findings on resilience further contextualize these results. Systematic reviews indicate that resilience-focused interventions in higher education can enhance coping confidence and well-being, although effects often attenuate after a few weeks (Abulfaraj et al., 2024). For instance, O’Connor and colleagues’ RISE program improved coping confidence but produced only modest reductions in psychological distress. In contrast, SBCBT in the present trial simultaneously yielded clinically meaningful improvements in resilience and robust reductions in DASS-21. This suggests that weaving resilience-building strategies into the CBT framework produces broader and more durable benefits than resilience-only programs. Evidence from strengths-oriented approaches also corroborates our results. Smith et al. (2025) found that strengths-based group interventions improved students’ resilience and self-discovery, while Murphy (2023) demonstrated that spiritually adapted CBT enhanced hope and psychological well-being in clinical populations. By extending such approaches to a nonclinical academic setting, our findings highlight the versatility of SBCBT adaptations across populations and contexts.
The observed concurrent decline in distress and rise in resilience aligns with theoretical models such as broaden-and-build theory, which proposes that cultivating positive psychological resources widens coping repertoires and fosters long-term well-being. Process-based CBT and foundational SBCBT models (e.g., Padesky & Mooney, 2012) similarly emphasize tailoring interventions to mechanisms such as self-efficacy and strengths use, providing a conceptual framework for understanding SBCBT's dual effects. Psychometrically, the increases in resilience measured by the BRS are consistent with recent multicountry studies, which demonstrate the scale's sensitivity to change and measurement invariance across cultures (Zhou & Ma, 2026). Likewise, the reductions observed on the DASS-21 subscales align with recent cross-cultural validation studies, which confirm its reliability in diverse student populations (Bonifacci et al., 2024).
Theoretical and Practical Implications
The findings are theoretically significant as they support the broaden-and-build model, which posits that positive emotions and strengths expand cognitive and behavioral repertoires, thereby facilitating resilience. By guiding students to identify personal strengths, construct personal models of resilience, and apply them to real-life challenges, SBCBT enhances coping self-efficacy and fosters adaptive behavioral flexibility, key transdiagnostic mechanisms in process-based CBT. Practically, the results have direct implications for campus mental health services. These findings have important implications for university counseling services and social work practitioners working with student populations. The SBCBT can be delivered efficiently in group formats, making it a scalable and resource-sensitive intervention for universities facing an increasing demand for psychological support. Importantly, the intervention's dual effect, which reduces distress and strengthens resilience, suggests it could serve both preventive and therapeutic functions. The attenuation of gains at follow-up underscores the need for booster sessions or integration with digital maintenance tools to ensure long-term sustainability.
Strengths and Limitations
This study possesses several notable strengths, including its randomized controlled design, the use of validated outcome measures, and the simultaneous assessment of both distress and resilience trajectories. By integrating resilience-enhancing components within a CBT framework, the intervention extends beyond a narrow focus on symptom reduction and instead demonstrates a dual-action model that targets both psychological vulnerability and protective factors. The theoretically grounded nature of the intervention, combined with a rigorous analytic approach using GEE that appropriately account for missing data, further strengthens the robustness of the findings. Moreover, the inclusion of both negative emotional outcomes and resilience indicators offers a more comprehensive evaluation compared to symptom-focused investigations alone.
Despite these strengths, several limitations warrant consideration. First, the relatively homogeneous sample, drawn from a single academic setting, may have contributed to the high treatment fidelity and substantial effect sizes observed, thereby limiting the generalizability of the findings to more diverse populations and individuals with more severe psychological difficulties. Second, the follow-up period was limited to one month, restricting conclusions regarding the long-term maintenance of treatment gains. Third, the study did not employ an active comparison condition. Consequently, the observed benefits of SBCBT may have been influenced, at least in part, by nonspecific therapeutic factors, such as therapist attention, treatment expectancy, group interaction, and participant engagement. Future trials should incorporate a more rigorous comparison condition that is perceived as equally credible by participants and requires a comparable level of time, effort, and therapeutic contact as the SBCBT intervention. Such an approach would provide a more stringent test of the specific efficacy of SBCBT and strengthen causal inferences regarding treatment effects. In addition, treatment fidelity and therapist competence were not formally evaluated, which may limit confidence in the consistency and replicability of intervention delivery. Future research should extend follow-up assessments to at least 3–6 months to evaluate the durability of treatment outcomes. Mechanistic investigations are also warranted to examine whether improvements in resilience and coping self-efficacy mediate reductions in psychological distress. Finally, evaluating SBCBT across culturally diverse populations and exploring hybrid or fully digital delivery formats would help establish its scalability, adaptability, and broader external validity.
Conclusion
This trial provides compelling evidence that SBCBT is an effective, mechanism-aligned intervention for enhancing the psychological well-being of university students. The intervention produced large and clinically meaningful reductions in DASS-21, accompanied by substantial gains in resilience that persisted at one-month follow-up. This dual action alleviating psychopathology while simultaneously fostering adaptive psychological resources addresses both vulnerability and protection, thereby advancing current models of student mental-health intervention.
Importantly, the findings highlight that integrating strengths-based strategies into conventional CBT frameworks may enhance therapeutic potency beyond the effects typically observed in standard or digital-only CBT programs. The observed concurrent improvement in resilience and reduction in distress is consistent with broaden-and-build theory and process-based CBT models, which emphasize the centrality of self-efficacy and resource activation as drivers of enduring change. From a practical perspective, these results underscore the potential of SBCBT to be implemented within university counseling services and preventive mental-health programs as a scalable, low-stigma, and high-impact intervention. Embedding resilience-oriented CBT modules into student support systems could provide a first-line or stepped-care option, particularly during periods of heightened academic stress.
Future research should extend these findings by examining longer-term trajectories, testing active comparators, and exploring hybrid delivery formats (e.g., digital boosters or group-based modules) to optimize scalability and sustainability. Taken together, the evidence positions SBCBT as a next-generation intervention that not only mitigates psychological distress but also equips young adults with the enduring psychological strengths required to thrive in challenging academic and life contexts.
Footnotes
Ethical Approval
This study involving human participants was conducted in accordance with all applicable institutional guidelines and received approval from the Institutional Review Board of Universiti Pendidikan Sultan Idris (UPSI; No: RIMC/2024-0415-01). Documentation of the ethical approval can be obtained from the corresponding and primary authors [AP] upon reasonable request.
Consent to Participate
Informed consent was obtained from all participants prior to their involvement in the study. Participation was voluntary, and individuals were clearly informed that they could withdraw at any stage without any consequences. Copies of the signed consent forms are available from the corresponding author upon reasonable request.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding and primary authors [AP] upon reasonable request.