
Abstract
In this study, we explored the lived experience of Japanese mothers who have delivered multiple children with intellectual disabilities (ID), using interpretative phenomenological analysis. We identified three superordinate themes and seven subordinate themes from the narrative data collected from 10 participants. The superordinate themes were: abandoned hope for having an ordinary family, accumulating physical and mental fatigue, and searching for positive experiences in parenting multiple children with disabilities. How they perceived the birth of children with disabilities for the second time differed depending on the disability types; specifically, whether they detected the disabilities early or not. Encountering the disability in another child overwhelmed mothers, especially when the disabilities were diagnosed after several years with or without suspicion; they struggled to accept the fact. Despite mothers facing extreme difficulties in parenting multiple children with disabilities, they tried to alter the negative perceptions and find an optimistic way of living.
Keywords
In Japan, there were 117,300 children under the age of 18 and 289,600 adults over 18 with intellectual disabilities (ID) living with their families in 2005: an increase from 93,600 children and 221,200 adults in 2000 (Ministry of Health, Labor, and Welfare, 2001, 2007). According to the American Association on Intellectual and Developmental Disabilities (n.d.), “Intellectual disability is a disability characterized by significant limitations both in intellectual functioning (reasoning, learning, problem solving) and in adaptive behavior, which covers a range of everyday social and practical skills. This disability originates before the age of 18” (para. 1)
A plethora of research which shows the negative impacts on families of children with ID has been reported (Neece & Baker, 2008). For example, parents of children with ID have higher levels of stress and morbidity of depression and/or anxiety than parents of children without disabilities (Baker et al., 2003; Emerson, 2003; Gallagher, Phillips, Oliver, & Carroll, 2008), and the stress is related to the child’s temperament and problem behavior, caregiver burden, parents’ sleeping conditions, and poor social support (Boström, Broberg, & Bodin, 2011; Dunn, Burbine, Bowers, & Tantleff-Dunn, 2001; Gallagher et al.; Hassall, Rose, & McDonald, 2005; Norizan & Shamsuddin, 2010; White & Hastings, 2004). Different aspects including children’s disabilities and social conditions are intertwined to affect the life of parents of children with disabilities.
The difficulties of parenting are different depending on the type of disabilities, which contributes to children’s emotional and behavioral states. In particular, parents of children with autism/pervasive developmental disorder (PDD)—invisible disabilities—undergo a long and difficult period of time before they receive the initial diagnosis, and require a lengthy time to accept the impairment (Nakata, 2002). Comparatively, parents of children with autism/PDD who exhibit problem behaviors experience higher levels of stress than parents of children with Down syndrome (Dabrowska & Pisula, 2010). In addition, because of persisting traditional gender roles, mothers experience higher levels of stress and poorer health conditions than fathers (Boström et al., 2011; Gray, 2003). These mothers of children with ID are less likely to be employed, and are more likely to experience social isolation and stress and develop depression (Shearn & Todd, 2000; Singer, 2006). Therefore, mothers of children with ID seem to be significantly affected by their parenting.
Recently, researchers have increasingly focused on parents’ stress-coping resources, such as positive perceptions, hope, optimism, self-esteem, self-efficacy, and a sense of coherence (Baker, Blacher, & Olsson, 2005; Hassall et al., 2005; Hastings, Allen, McDermott, & Still, 2002; Hastings & Brown, 2002; Hyman & Oliver, 2001; Olsson & Hwang, 2002; Padencheri & Russell, 2002; Trute, Hiebert-Murphy, & Levine, 2007). Researchers have found that parents of children with ID who have more stress-coping resources are more likely to avoid stress, maintain better health, and show lower risks of depression than those with few stress-coping resources facing similar difficulties (Hassall et al.; Hastings & Brown; Hedov, Anneren, & Wikblad, 2002; King et al., 2006; Mak, Ho, & Law, 2007; Oelofsen & Richardson, 2006; Olsson & Hwang; Trute et al.).
There has been little research in Japan on the relationship between parents of children with ID and their stress coping; instead, there is some evidence to suggest that the environment surrounding people with ID in Japan is harsher than that in other developed countries. In a survey comparing the opinions of people with disabilities in Japan, Germany, and the United States, researchers asked people with ID whether their country had seen an improvement in six areas over the previous decade, including accessibility to welfare services and understanding of people with disabilities (Cabinet Office, 2006). The result showed that Japan had seen the lowest rate of improvement. The percentages of respondents recognizing improvement in the six areas were as follows: United States, 61.8%; Germany, 51.6%; Japan, 14.8% (Cabinet Office).
In Japan, most individuals with disabilities are taken care of by their family in the family home. In a recent article, it was reported that approximately 90% of individuals with disabilities were dependent on their parents, and more than half of the caregivers were over 60 years of age (Kyosaren, 2011). In addition, traditional Japanese social norms place significant cultural burdens on mothers. For example, data collected from a general survey showed that the ratio of women who continued working after their first birth was 25.3%, whereas the ratio of women who retired after their first birth was 41.3% (Ministry of Health, Labor, and Welfare, 2010b). The percentage of women who had children with disabilities was not considered in this survey, although how responsibilities of parenting were weighted more on mothers was indicated. Despite such social norms, mothers of children with disabilities have very limited social support, and sufficient attention has not been paid to the health of these mothers.
The concept of women’s health was included in a recent Japanese policy (Ministry of Health, Labor, and Welfare, 2010a), yet the policy does not include any approaches to the health promotion of mothers who have children with disabilities. Moreover, the policy is focused on individuals’ life stages, and lacks a perspective on family health promotion. Youda (1999) claimed that children with disabilities were considered an “unacceptable presence” in Japanese society, and that mothers of children with disabilities tended to be blamed and accused by family members and relatives, especially by the parents and siblings of their husbands.
In this context, there is a notable concern for mothers of multiple children with ID as one of the most vulnerable populations in Japanese society. What do mothers of multiple children with ID experience? How does raising multiple children with ID impact mothers? Several quantitative studies revealed negative impacts on parents of multiple children with disabilities in both mental and social aspects, compared with those with a single child with a disability (Lawton, 1998; Orsmond, Lin, & Seltzer, 2007). Few researchers used qualitative research methods based on parental narratives to specifically explore what sort of experience those parents had.
Wakiguchi, Arikawa, Hayashi, and Abe (2000) investigated the experience of a mother who had two children consecutively with infantile early epileptic encephalopathy, but they focused on a single case, examining only her experience during a short period of time immediately after the birth of the second child. Additionally, although Kimura, Yamazaki, Mochizuki, and Omiya (2009) showed that the birth of a sibling with PDD following a child with the same disability led to a mother’s recognition of impairment, little is known about other cases of siblings with different disabilities. Such research topics seem to be extremely sensitive, but proper understanding of a mother’s experience of repeatedly having to handle children with disabilities is necessary for providing an appropriate environment for them. Thus, we designed our study to explore the lived experience of mothers of multiple children with ID in Japan.
Methods
Design
We used interpretative phenomenological analysis (IPA; Smith, Flowers, & Larkin, 2009) as the method of analysis. The aims of IPA are to grasp and seek the meanings of participants’ experiences by hearing the voices of participants from across the sociocultural spectrum. It is adaptable when exploring uninvestigated areas in which theoretical pretexts are absent (Reid, Flowers, & Larkin, 2005). In other words, IPA helps to understand “what the experience for this person is like, what sense this particular person is making of what is happening to them” (Smith et al, 2009, p. 3). It includes a case-by-case analysis that examines in detail the perceptions of a specific group, and has especially been used to explore difficult reproductive decisions that individuals have to face, as well as the ethical issues faced by society (Chapman & Smith, 2002).
In this study, we were concerned about not only common experiences among mothers of multiple children with ID, but also how the children’s disability type and the situation surrounding each participant reflect their perception. Researchers using IPA have been interested in the nature of gaps that exist between a situation/state and an individual’s perception (Chapman & Smith, 2002). Moreover, whereas analyses of IPA highlight differences, attempts are made to balance this against an account of commonalities (Reid et al., 2005). These aspects also suited to our purpose; thus, we regarded IPA as the most adaptable approach for this study.
Participants
The potential participants for this study were Japanese mothers living within the greater Tokyo metropolitan area who had given birth to multiple children with ID within the previous 18 years. We obtained data from 10 participants within a homogeneous sample whose children’s disabilities were diverse. IPA has a focus on analysis of language used by a small and homogenous sample (up to 10 participants according to Smith et al., 2009), and it is for us to challenge the traditional linear relationship between the number of participants and the value of the research (Reid et al., 2005). If the participants had more than two children with ID, the number of children with/without disabilities and their birth order were not restricted.
Ages of the 10 participants ranged between 35 and 50 years, with a mean of 41.7 years, and all participants were married. Eight participants were full-time homemakers, whereas two worked part time. Ages of the older children with ID ranged between 3 and 18 years, with a mean of 11.5 years; six were boys and four were girls. Disability types included autism/PDD (six children), Down syndrome (three), and other chromosome anomaly (one). Their 10 younger siblings with ID, eight boys and two girls, were aged between 0 and 13 years, with a mean of 7.4 years. Their disability types were autism/PDD (three), Down syndrome (two), craniostenosis/ID (one), developmental delay (one), attention-deficit/hyperactivity disorder (two), and intellectual disability with autistic tendency (one). There were two other undiagnosed children who were born after a younger child with ID, and had some developmental delay and problem behavior.
Procedure
The proposal for this study was approved by the Department of Medicine’s Institutional Review Board at the University of Tokyo. We used purposeful sampling to recruit participants through a parents’ group and a day service center, where they provided educational services for a number of school-age children with intellectual/developmental disabilities. The parents’ group had a membership of parents of children with a wide array of ID, and we asked the leaders of the group and staff members of the day service center to introduce the overview of our study and discuss the interview process with mothers who met the criteria. Following the discussion, our contact details were provided to the mothers. Participation was voluntary; those who expressed an interest in participating contacted Kimura, the first author, to learn more about the study, and if they were still interested in taking part, a time and place for the interview was arranged.
Prior to and on the day of the interview, privacy assurances were given to the participants, both through verbal explanations and in written documentation. Before the interviews began, participants signed a consent form that included permission to record interviews. In addition to the first group of mothers, we recruited more participants through word of mouth in the community. When someone who met the criteria expressed an interest in participation, they contacted Kimura and followed the same procedure.
Data were collected in one-on-one semistructured interviews conducted by Kimura between November 2007 and April 2010. Interviews lasted between 80 and 165 minutes, with a mean of 140 minutes. The interview questions included the following: For the second time, how did you notice the disability of your child? How did you feel about that fact? Please tell me about your experiences taking care of multiple children with intellectual disabilities. During the interview we also obtained demographic information, such as ages and types of disability of the children, whether there was a sibling without a disability, the standard of living, employment status, and marital status.
Analysis
Throughout the interviews, Kimura followed IPA guidelines (Smith et al., 2009) and took careful note of participants’ emphasized points, repeated words and expressions, pauses, laughter, verbal tones, and degree of fluency. IPA guidelines were also followed with respect to how to create and analyze verbatim transcripts from interview recordings. Searching for metaphors in such a study is particularly important because they are useful for understanding participants’ shared experiences (Shinebourne & Smith, 2010). In this study, metaphors were selected from participants’ actual words, which seemed to be most adaptable to imply their experiences, situations, emotions, and perceptions. In addition, we used the metaphors to cluster subordinate themes, which categorized specific experiences of the participants. These processes were also helpful to grasp superordinate themes, which indicated more consistent experiences among the participants.
Similar to the procedure used in a previous study (Kimura, Yamazaki, Mochizuki, & Omiya, 2010), Kimura took responsibility for the following: (a) reading the transcripts multiple times, making initial comments on the text, searching for metaphors and their meanings, and transforming these into themes that captured the essential qualities of the text; (b) analyzing the relationships among the themes until they formed a consistent whole and creating a rank-ordered list of themes that allowed us to identify the superordinate and subordinate themes for each participant; (c) identifying shared superordinate themes for the group as a whole, confirming by checking relevance to subordinate themes, metaphors and their implications, original comments, and actual language used in the interviews; and (d) adding descriptive commentary.
Yamazaki, the second author, confirmed the adequacy of coding, themes, metaphors, and interpretations at each stage, and provided alternatives to those suggested by Kimura. Also, to avoid a prejudiced viewpoint and reflect multiple perspectives, we presented our work to a group of researchers who were familiar with health sociology, disabilities, nursing, and qualitative research. Their feedback was taking into consideration in finalizing the themes, commentary, and analyses.
Findings
Three superordinate themes emerged from descriptions by Japanese mothers who gave birth to multiple children with ID (see Table 1). The first was “abandoned hope for having an ordinary family,” which described how participants faced the fact that they had become the mother of multiple children with ID, and what this meant to them. The second was “accumulating physical and mental fatigue,” which referred to the difficulties of parenting multiple children with ID, the undesirable circumstances in which they lived, and how these were intertwined and affected the participants. The third was “searching for positive experiences in parenting multiple children with disabilities,” which explained the ways participants altered their perceptions based on their own experiences, their relationships with others, and their children with ID. After each citation, the children’s information (the birth order and the type of disability) is described. In the text below, disability types are noted using the following abbreviations: attention-deficit/hyperactivity disorder (AD/HD), chromosome anomaly (CA), Down syndrome (DS), and pervasive developmental disorder (PDD). Children without disability are noted with “WD.”
Themes, Main Metaphors, Their Implications, and Similar/Related Expressions.
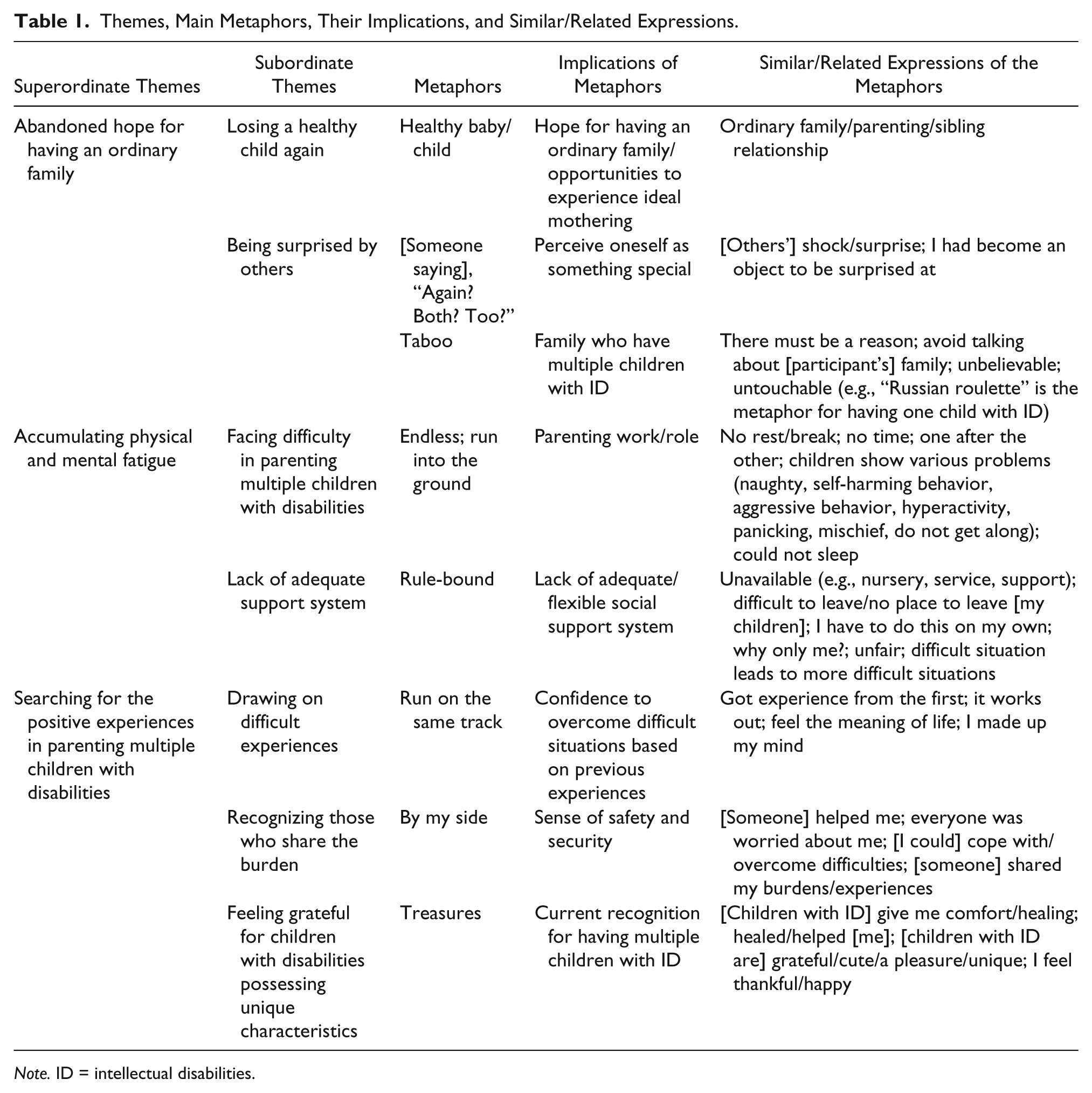
Note. ID = intellectual disabilities.
Abandoned Hope for Having an Ordinary Family
When they first realized their children had ID, the majority of the participants felt that their dreams and life plans were completely destroyed. What had been giving the participants hope was the birth of the next child. Six participants whose first child had ID decided to have their second child specifically to raise a healthy child and to reconstruct what they thought of as an “ordinary” family. The three participants who had older children without a disability before having children with ID had wished for someone who would support their healthy children, with a hope of having an ordinary sibling relationship. In one case, after the second child was born, the first child was diagnosed with PDD. Although the participant in this case became depressed at the time, she still hoped to experience ordinary parenting with her second child. Thus, facing disability for the second time meant losing hope. The shock the participants were suffering from was from two sources: the disability itself and the negative impact on their own status in society.
Losing a healthy child again
One of the devastating things among the participants was facing disability for the second time. This was overwhelming for most of them, because they once again lost the chance to have a healthy child and failed to reconstruct an “ordinary” family. The disability of the next child manifested itself at various points, depending on the disabilities. In one case, a woman who had experienced abnormal labor faced the possibility of the next child’s disability immediately following its birth. The doctor was an advocate of natural childbirth, and did not give the participant the option of delivery by cesarean section. The baby was born with the umbilical cord wound around her neck:
The doctor explained that he wasn’t sure what the baby’s development was going to be like, and that’s all. I just cried, cried, and cried. I don’t know how many times I have wished I could reset my life. I definitely wanted to have healthy baby, like an ordinary family, but I’ve lost it again. (1st: CA; 2nd: craniostenosis)
The use of the phrase “lost it again” implies that the woman thought she had lost a healthy baby that was needed for the reconstruction of an ordinary family. Most participants used the metaphor “healthy baby/child,” which implied “hope for having an ordinary family/opportunities to experience ideal mothering.” There were also mothers of multiple children with Down syndrome, which they detected immediately after birth:
My third one was obviously different [from a healthy baby]. It was even more obvious than my second one, and I thought, “Again?” I didn’t say that aloud, but it was clear to me. I was feeling like at the bottom of everything. (1st: WD; 2nd & 3rd: DS)
In our study, there were two mothers of multiple children with Down syndrome, and neither of them had an amniotic fluid test before delivery because they did not expect to have a child with Down syndrome. Both participants were feeling an extreme level of shock, but one felt completely devastated, whereas the other was not so overwhelmed. These mothers’ acceptance was different, although because the disability was visible and it was “obvious” that they had to work hard to cope with it, both of them quickly began the task of caring for their multiple children. In contrast, when subsequent children were born with “invisible” disabilities such as autism/PDD, participants struggled to detect the disabilities at an early stage, which made them even more difficult to accept:
I wasn’t aware of his disability until he entered elementary school.
Did you have any suspicion?
Not at all. I was like, “What is pervasive developmental disorder?” I had had an amniotic fluid test, thinking that it might have Down syndrome too [like her first child], but the result came out clean, and the delivery was normal, so I didn’t even imagine he might have a disability. (1st: DS; 2nd: PDD; 3rd: undiagnosed)
Only one mother in our study had a first child with Down syndrome and a second child with PDD. In this case, obtaining negative results from an amniotic fluid test underpinned the participant’s positive expectation for her next child, and being mainly concerned about Down syndrome had resulted in a late detection of the disability. However, even for mothers who already had children with autism/PDD, it was not easy to detect the same type of disabilities in their next child:
Because the second child was totally different from the first, I had confidence that the second one didn’t have any disability. I was very happy to raise a healthy child [pause] and I thought that I was experiencing ordinary parenting. So when the teacher of my first child pointed out the disability of my second child, I ignored her advice. I thought it shouldn’t be. After a while, we received a diagnosis for the second one, and at that time I was completely overwhelmed by the fact and couldn’t cope with it for several years. This shocked me more than before. (1st: AUT; 2nd: autistic tendency)
For mothers who had been raising their children under the assumption that they did not have disabilities, diagnosis of a disability was not easy to deal with and took considerable time to accept. During this process, they were experiencing differences between the siblings as well as the feeling of loss of “ordinary parenting.”
There was an exception. A participant had experienced devastating sorrow at the death of her first child with cerebral palsy, and when she faced the disability of her third child (PDD), she felt that, “Okay, here it comes again.” In this case, “again” did not imply the devastation of her hope, but rather it referred to the challenging second opportunity of raising a child with ID. Thus, mothers’ reactions and the magnitude of those reactions varied depending on their background and their previous life experiences.
Being surprised by others
Not only the mothers’ own shock of repeated encounters with disabilities, but also other’s reactions had a negative impact on mothers of multiple children with disabilities. Often others reacted with surprise when they found that more than one child in a family had disabilities. This also overwhelmed the mothers because being surprised by others made them realize that they had acquired a special status in society, which also implied that their hope of becoming an ordinary family was to be abandoned. The participants had common experiences in which others were surprised and tossed short but unpleasant questioning words such as, “Again?” “Both?” and “Too?”:
It is hard when I imagine how people may say, “What? Both kids [have disabilities]?” If I had one child with a disability, I can have an excuse by saying, “It’s like Russian roulette, and I got bad luck.” But when you have two, they would say, “There must be a reason,” and that’s awkward. In fact, I used to see mothers who had multiple children with disabilities with a prejudiced attitude. I have to resist that now [that] I am on the other side, but that was hard to get over.
Did somebody say such a thing?
No, no. Other mothers with healthy children avoid talking about my family as a taboo. But I can see their reaction. It was extremely disturbing to see the look of shock on people’s faces; the magnitude of my shock would have been three times greater than theirs. (1st: WD; 2nd: AUT; 3rd: AD/HD)
Notice how the differences in perception about having one child with ID and multiple children with ID were described by this participant. In particular, she used two metaphors, “Russian roulette” and “taboo.” The former referred to having one child with ID, and other participants used similar expressions such as “bad luck,” “accident,” “chance,” and “rare possibility.” The latter metaphor referred to having multiple children with ID, and it had an opposite meaning to the former, such as “there must be a reason,” “avoid talking about [participant’s] family,” and “unbelievable.” Therefore, the participants cognitively understood others’ surprise, but in reality, it was difficult to accept that they had become something special, as an “untouchable” in society.
Accumulating Physical and Mental Fatigue
Taking care of multiple children with disabilities involves a considerable amount of work and effort, which could contribute to mothers’ experience of extreme physical and mental fatigue. Mothers had to meet a range of different needs for the children with various types of disabilities and characteristics. Undesirable circumstances such as lack of adequate support also heightened the burdens on the participants, and led to perceptions of unfairness. These circumstances were intertwined and added to the fatigue they felt.
Facing difficulty in parenting multiple children with disabilities
Parenting multiple children with ID constantly burdened the mothers both physically and mentally. The everyday work of parenting was endless, and children’s behaviors altered constantly. The words most repeated by the participants were “no rest/break,” “no time,” and “one after the other”:
I haven’t taken the two kids out by myself before.
What? Never? Your children are both in elementary school, right?
Yes, but when they both get hyperactive, and they run off in different directions, I can’t chase them around. I can’t shop either.
I see. It must be hard. And how about at home, do they always need attention?
Of course, I can’t rest at all, because a mother’s work is endless. Both kids alternately show aggressive behaviors, which causes many problems, one after the other. [pause] I have run into the ground. (1st & 2nd: PDD)
This is a typical example of mothers of multiple children with ID who had behavior problems. Most participants reported that their children had behavior problems, and these resulted in perceptions that their parenting work seemed to be “endless,” and that they were being “run into the ground.” They also had to worry about others around them, including neighbors and siblings without disabilities:
My oldest son is really naughty, and often clogs the toilet. I always go around and apologize to my neighbors. The middle kid acts violently and the youngest refuses to go to school. I somehow manage to take her to school, but it’s almost lunch time when we arrive, and then soon afterward I have to go to pick her up. They push me around all day long. No matter how old they get, there is no time for myself at all. (1st: DS; 2nd: PDD; 3rd: undiagnosed) The third cries loudly, and the second gets panics. They don’t get along. The first talks loudly to his brothers, and the second panics again. His self-harming behavior became worse, and he started taking medication. The first is slack and it is terrible. (1st: WD; 2nd: AUT; 3rd: AD/HD)
These cases show how children affect each other, and how difficult it can be to manage them when they “don’t get along.” Especially when the children with ID were young or if they had a sleep disorder, mothers did not get enough sleep. The participant who had multiple children with Down syndrome reported that she was only able to sleep for 3 hours at a time since her second child was born. Although there was a change in rhythm in conjunction with the children’s growth, participants had lived without breaks, regardless of whether they had infants or children of high-school age.
Lack of an adequate support system
Most participants claimed that they had no adequate support system, and such circumstances added to the difficulty of parenting and the fatigue of mothers, which sometimes provoked their feelings of unfairness toward society. Generally, participants’ husbands did not have time to care for children during weekdays, and grandparents were often too old to take care of hyperactive children. Therefore, the mothers required flexible social support, especially in emergencies such as hospitalization, and during hospital visits, family illnesses, and school events. The challenge was that, even when there were various services and systems available, these tended to be “rule-bound” and were not easily accessible:
My third child had intestinal stenosis and had to have surgery immediately. I was in the hospital with her for a few days. It was most difficult to leave my second child [with Down syndrome] during that period.
Was it difficult for you to stay in the hospital with other children?
Oh no, it was impossible. The hospital was rule-bound, which prohibited any children to visit or stay in the room, even if he or she was a sibling and had a disability. (1st: WD; 2nd & 3rd: DS)
The phases “difficult to leave” and “no place to leave [my children]” were repeated by all the participants. This made them think, “I have to do this on my own.” No matter how hard participants tried to do everything by themselves, there were limitations. One participant observed, “When someone in the family gets sick, I can’t take the kids to school. So they don’t go to school.” This showed that lack of support in emergencies resulted in negative impacts not only for mothers but also for children. In addition, mothers of children with ID were often required to attend education/care centers with their children, despite this being another burden:
Mothers of healthy children are able to work and are eligible to use nurseries. But I can’t work because of caring for my kids. That’s why I can’t use nurseries and have to do everything by myself. I find it very difficult to take two children with Down syndrome to an education/care center by bus. To do so every single day is such a struggle, and I do not have an alternative. One difficult situation leads to another. It is so unfair, isn’t it? (1st & 2nd: DS)
In Japan, nursery and after-school services are provided, in principle, only for mothers who are employed. This provoked feelings of unfairness in mothers who had multiple children with ID: most wanted to work, but there were significant obstacles. These circumstances increased the physical and mental fatigue of the mothers.
Searching for the Positive Experiences in Parenting Multiple Children With Disabilities
The majority of mothers expressed their willingness to accept their life of caring for their children with ID. Although there were enormous difficulties in parenting, most said things like, “I had to survive for my children.” To achieve this, participants needed to alter their perceptions about life by searching for the positive aspects of parenting. These came from three sources: themselves, others, and their children with ID.
Drawing on difficult experiences
One positive experience was that the participants felt some confidence to overcome difficult situations based on their previous experiences. When they first began raising a child with disabilities, not only did they lack information about the disabilities but also about the support and education that was available. They worked hard to find information, until finally they were able to reach out and connect with others, confronting each challenge. That experience was beneficial when they learned of their next child’s disabilities, and one mother described this as being able to “run on the same track”:
It’s an advantage that the younger child could run on the same track that the older child has laid. The teachers of the special support school who worked with the first child know me well, even though there were times when we differed. So if the second child doesn’t have a disability, then it’s a good thing, but even if the second has a disability, it works out because you have experience from the first [laughs]. (1st: AUT; 2nd: autistic tendency)
This description also indicates that tackling difficult experiences had led some to develop the confidence and optimism to say that “it works out”:
There was no other way to live other than as a mother of children with disabilities. I made up my mind about every aspect.
How about now?
Now I know what I want to do and what I should do. I think I’m happier now than before. Life is harder, and my health is a lot worse than before, but yet, I think I am happier. I like where I am positioned, and I have a meaning in life. I feel like I rely on myself for my life, probably more than for a life in which I only had a child without disability. (1st: WD; 2nd: AUT; 3rd: AD/HD)
The phrase “made up my mind” is an indication the that participants’ sense of purpose had become clear based on repeated experiences. Also, they had begun to believe that life had meaning, as their interests shifted from becoming a mother of children without disabilities to building a society in which children with disabilities could live well. Half of the participants told similar stories.
Recognizing those who share the burden
In addition to confidence to handle difficult situations by themselves, the participants were able to reach someone who tried to understand and share their burden. The realization that someone was available to share their burden put the participants in a positive frame of mind. The majority of mothers felt better when they had found someone whom they considered to be “by my side,” and it provided them with a sense of safety and security to have “[someone who] helped me.” These feelings also related to phrases such as “[I could] cope with” and “overcome difficulties.” Those closest to the participants were often their husbands and parents. In our study, 6 participants were able to receive support from their parents, their husbands, and/or their husbands’ parents, and they realized that they also had been cared for:
When I was in trouble, my parents helped me immensely. There have been times when I felt like I might not be able to cope with the fact of two kids with Down syndrome, but when I looked at my parents, I felt like it was not that bad. (1st & 2nd: DS) My husband protected me from his mother and brother, who accused me of having multiple children with aggressive behavior. But one day, my husband said to them, “Both kids have disabilities, even you don’t want to accept the fact. Because my wife and I have to raise our children together, don’t interrupt us.” Wow, that’s what I wanted to hear [laughs]. Then I thought that I could raise these children and cope with difficult parenting because he is by my side. (1st: AUT; 2nd: autistic tendency)
Such feelings were not common to all participants. Some became isolated even within their families or felt helpless because the situation was not understood by other members of their family. These women had to rely on others. For example, being able to share difficulties with the leader of a nonprofit organization was an important support for one participant, who otherwise faced raising three children with very little support:
Even when the child broke the milk bottle and got all bloody, my husband didn’t do anything. He has never gone to school events. Although he said, “Let’s work together to raise our kids,” I am the only one who does everything.
How about your parents?
Not at all. My mother always scolded me because she thought that having multiple children with disabilities was my fault. But instead of my husband and my mother, the staff of the NPO [nonprofit organization] for disabled have always helped me. The leader of the NPO is a mother of a child with a disability, and is always willing to hear my complaints. Without her, I wouldn’t have been able to raise my children. (1st: DS; 2nd: PDD; 3rd: undiagnosed)
Similarly, meeting someone who would understand the circumstances of mothers of multiple children with ID eased the participants’ fears of being somehow special or marginalized. One participant stated,
The parents’ association for children with disabilities has helped me learn a great deal, and I have come to think that it can work out. Usually, if you tell someone that both your children have disabilities, the person gets shocked. But in the parents’ association, no one is shocked no matter how many of your kids have disabilities. It’s like, “Her kids too, so are hers. So what?” (1st: WD; 2nd: AUT; 3rd: AD/HD)
This mother had no family support, and was afraid of facing discrimination. Nevertheless, she finally found a place where she could feel safe and secure. Even though the circumstances were not exactly the same, all participants had someone who filled the role of sharing the burden.
Feeling grateful for children with disabilities possessing unique characteristics
Although having multiple children with ID had deprived participants of hope and made them exhausted, every participant found the value of each child and recognized their own affection for the unique characteristics in their children:
Everyone says, “It must be hard on you to have two children with disabilities,” but I think it is good that I have two because I don’t have to face just one. It is a lot of work, but there are differences in their disabilities. In my case, my older child has a severe disability, while my younger has intermediate, and the younger one often gives me some comfort or healing. (1st: AUT; 2nd: autistic tendency)
Surprisingly, no one in our study referred to similarities in their children with ID. Instead, the participants mainly described the differences between the children, and they stated that when they faced particular difficulties with one child, the other child “healed” or “helped” them. In the interviews, participants reported finding positive features in their children and recognizing them as “treasures.” This metaphor was expressed with feelings such as “grateful,” “cute,” “pleasure,” and “unique,” and participants looked back at their own lives and felt “thankful” and “happy”:
It’s quite a lot that I get from my two kids. They are cute. Well, any child must be cute for his or her parents, but there are parts that are difficult and that are dear and lovable because of the disability. Smiles, gestures, silliness . . . everything is cute [laughs].
You mean, it is good that you have two children?
Yes, I have no regrets that I had them. Kids are treasures. There are hard times. There are times when I feel like hitting them [laughs], but children without disabilities also have various difficult things, so disability has nothing to do with that. (1st: CA; 2nd: craniostenosis)
As this example illustrates, the majority of the participants were trying to find a positive and optimistic way to live their life, although the mother quoted had described the previous year as being “rock bottom” because of the children’s problem behaviors and her own health issues. Moreover, all participants spoke about how optimistic feelings could be drained away when they faced chronic fatigue and unceasing worries of raising multiple children with ID. Thus, these mothers were often desperate to find an optimistic perspective in life while experiencing extreme conditions. In other words, without finding positive experiences in parenting, everyday life might have been extremely difficult.
Discussion
We explored the lived experience of Japanese mothers who had multiple children with ID. The majority of the participants had placed their hopes of the reconstruction of their lives and families on their unborn children, and having to face disabilities in these children had been a significant shock to them. In addition, they experienced extreme physical and mental fatigue from the everyday work of dealing with the disabilities. Nonetheless, by realizing that there were family members and others who would share their burden, the majority of participants collected themselves and continued their positive efforts in trying to find the positive aspects of the challenges they faced.
How the mothers perceived the birth of a second or subsequent child with ID differed depending on the disability type of that child, and more specifically, whether or not the disability could be detected early. In another study, in which pregnancy after a woman had had a child with Down syndrome was considered, it was noted that the women perceived a subsequent pregnancy as a chance to regain their self-worth, experience ordinary parenting, and provide a sibling for the child with Down syndrome (Tsuji, 2003). In the article about our previous research (Kimura et al., 2010, Findings, “The potential joy,” para. 1) we reported that pregnancy following the birth of a child with PDD was “a fervent hope for an opportunity to improve their current situation, alter their lives, and reclaim lost dreams.” These findings were echoed in this study, in that the child following a child with ID was perceived to offer a promise of a reconstructed life and family, and acknowledging his or her disability meant seeing that dream shatter.
In the cases in which two children had Down syndrome, the participants had noticed the disability of the next child even before a physician told them because physical characteristics were visible, and there was no alternative for them but to accept the reality that was presented to them. By contrast, with regard to next children diagnosed with the so-called invisible disabilities, such as autism/PDD (Nakata, 2002), the participants raised the next children for some years on the assumption that they had no disability, which later brought them much intense conflict and ambivalence between understanding and accepting the disabilities. Nakata stated that invisible disabilities were considered more difficult to accept, and the same conclusion was found in our study for the cases in which mothers encountered a child with disabilities for the second time. Therefore, medical care providers should consider psychological support for parents being notified of a disability for the second time.
The effect on mothers’ health from the lack of rest and the need for lessening the physical and mental fatigue associated with parenting should be highlighted. The participants did not have time to sleep, and it was not easy to take more than one child out of the house by themselves because of their hyperactivity and problem behaviors. They often felt extremely ashamed, and lived a life of constant dread within their neighborhood. Because parents’ poor sleep conditions, caregiver burden, and children’s problem behaviors have a negative impact on parental mental health (Gallagher et al., 2008; Neece & Baker, 2008), the current situation—in which the mother spends the majority of her time with multiple children with ID—needs to be changed by providing respite care that is more readily available and accessible.
Lack of adequate support has left mothers of children with ID largely to do everything by themselves, despite their body and mind being exhausted. Considering not only the mothers’ health but also the children’s health, it is clear that more flexible social support systems, such as nursery and after-school services, helpers, and places to leave children in emergencies, are much in need. Also, support from husbands is important to ensure that mothers’ burdens are shared, though caring for children during the work week is not an easy task in Japanese society. Therefore, it is necessary to introduce flexible working hours for men and to increase social awareness about their right to take leave for looking after their children. More comprehensive approaches to facilitate these, such as shifting the target of health promotion from unit of generation to unit of family and involving mothers of children with disabilities in strategies to promote women’s health, should be helpful.
What was most notable in this study were the frequently observed positive aspects in the mothers’ narratives, although they had been notified of disability multiple times and were at times overwhelmed by caring for their children with ID. For mothers who were faced with the unbearable reality of disability in their next children, support from family and others were perceived as sharing the burden, and had a significant influence in altering their outlook to a positive one. According to Hastings et al. (2002), positive perceptions in mothers of children with ID were positively associated with reframing coping strategies (positively reframing events to make them more manageable), the helpfulness and usefulness of support from family and friends, and caregiving demands. We found in this study as well that having someone who would share the burden was essential for increasing mothers’ sense of safety and security, and underpinned the confidence to manage difficult situations.
Also highlighted by a number of participants was that they drew on past experiences that had been difficult and challenging for them. When they faced disability for the first time, they had no information about the disability itself nor the surrounding environment and issues such as support, educational system, or parents’ networks, and it took them a great deal of time and effort to collect the information. In contrast, when they faced disability for the second time, they found it to be an advantage that they had previously faced a challenging experience, as exemplified in the remark, “run on the same track.” This reflects an attitude of living in a way that draws on difficult experiences, including both stress-related growth and positive change (Siegel, Schrimshaw, & Pretter, 2005) that emerged as they faced disability multiple times.
Another aspect, seeking a purpose in life as a mother of multiple children with ID, could offer a renewed meaning of life with broader perspectives. After having multiple children with ID, the interests of mothers shifted from being focused on becoming mothers of children without disability to building a society where children with disabilities are able to live well, indicating a strengthened resolve to live a life as a mother of children with ID. In several studies, it has been observed that a sense of purpose is developed in the process of parenting children with disabilities, leading to positive changes (Stainton & Besser, 1998). In this study too, it appeared that the participants had achieved a positive change by thinking about their roles and purpose and affirming themselves as mothers of multiple children with ID.
Additional new findings from the present study included the observation that mothers found comfort and pleasure in the unique characteristics, attitudes, and roles of children with ID, and the differences between their children even when they had the same type of disability. Researchers have reported that a parent who raises multiple children with disabilities experiences greater negative impacts than those who have a single child with a disability (Lawton, 1998; Orsmond et al., 2007). Similar to this, our study participants suffered severe distress and fatigue, and they felt that they could easily fall into an abyss. Nonetheless, most recognized the worth of their children and their own life, and had the strength to live optimistically. Optimism provided buffering effects relating to children’s problem behaviors and increased mothers’ well-being (Baker et al., 2005). It seemed to be one of the strong stress-coping resources to overcome difficulties among the mothers.
The ability to describe complex feelings and attitudes was an advantage of the IPA methodology we applied in this study. Considering the types of disabilities and situations surrounding each participant allowed us to understand their differences. Seeking metaphors was also an effective way to grasp common experiences among the participants. By using IPA methodology, significantly new detailed insights were revealed regarding mothers’ experiences of giving a birth to another child with ID, as well as their challenges of raising those children.
This study had several limitations. Because we relied on a parents’ group and a day service center for children with disabilities, the sample was necessarily limited to those participants who availed themselves of these networks. This leaves important questions about the experiences of mothers without such support networks unanswered. Also, all participants lived in Tokyo and most lived with their nuclear family. Hence, in our research, the experiences of participants living in more rural regions, many of whom typically share dwellings with their husband’s families, were not included. Furthermore, because in this study we focused only on mothers, the experiences of fathers were not explored. Finally, ethical considerations limited our study to those mothers with an active interest in discussing these issues.
Future issues to be addressed include examining the experiences of fathers and siblings without disabilities who live with multiple children with ID, and the type of support needed by families. There has been little research to date illuminating these issues, and we believe that in this study, valuable descriptions to help our understanding of women who have multiple children with ID have been revealed. Further investigations into the mechanisms of coping resources of parents of multiple children with disabilities, and the expansion of research on disability acceptance that addresses the lives of parents holistically, are required to further our understanding.
Footnotes
Acknowledgements
We thank all participants and members of the Department of Health Sociology, and Department of Epidemiology and Preventive Health Sciences, Graduate School of Medicine, at the University of Tokyo.
Authors’ Note
Portions of this article were presented at the 77th Annual Research Conference of The Japanese Society of Health and Human Ecology in Tokyo, Japan, November, 2012.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A grant was received from Grants-in-Aid for Scientific Research (Basic Research A, 21243033).
Author Biographies