
Abstract
We compared face-to-face focus groups and an online forum in qualitative research with people with multiple sclerosis (MS) and family members. Although the merits and challenges of online qualitative research have been considered by others, there is limited literature directly comparing these two data collection methods for people with disability or chronic illness. Twenty-seven people participated in one of four focus groups and 33 people took part in an online forum. Demographic and MS-related characteristics were similar between the two groups, with a slight nonsignificant trend toward nonmetropolitan residence in online forum participants. There was a high level of overlap in the themes generated between groups. Participant responses in the online forum were more succinct and on-topic, yet in the focus groups interaction was greater. Online qualitative research methods can facilitate research participation for people with chronic illness or disability, yielding generally comparable information to that gathered via face-to-face methods.
Keywords
Qualitative research is conducted to gain insights into people’s experiences and the meanings they place on their actions and the world around them (Carter & Henderson, 2005). One of the key methods in qualitative health research, focus groups play an important role in understanding the experience of health and illness. Central to their use is the role of interaction in stimulating talk, as people remember and describe views, behavior, and experiences. As Carter and Henderson noted, they are a “collective activity” (p. 221) organized to explore a set of issues. When conducting research with people with chronic illness or disability, or their carers, researchers need to consider how to involve people who can find it difficult to physically attend a focus group location. Being at work, having small children or being a carer, impairment, pain, fatigue, cost, and distance can act as barriers to participation. An online forum or focus group provides an opportunity to overcome some of these barriers (Mann & Stewart, 2000).
Because more people are online, qualitative researchers are increasingly exploring the use of online research tools as a way of researching the experiences of people with chronic illness or disability. These tools include email interviewing, synchronous online focus groups, or asynchronous online forums. Various forms of email interviewing have been used to research the experiences of people with autism (Benford & Standen, 2011), traumatic brain injury (Egan, Chenoweth, & McAuliffe, 2006), physical and sensory disabilities (Bowker & Tuffin, 2004; Seymour, 2001), and cerebral palsy (Ison, 2009). Uptake of online focus groups and forums has been slower (Turney & Pocknee, 2005), but such studies have been conducted with people with cerebral palsy (Dattilo et al., 2008) and chronic fatigue syndrome (Guise, Widdicombe, & McKinlay, 2007).
Conducting online forums and focus groups in preference to face-to-face focus groups presents a number of advantages and disadvantages for both participants with chronic illness or disability and researchers. The use of online methods requires participants to have access to the Internet and adequate computer literacy (Egan et al., 2006). People with chronic illness or disability, and older people might face significant difficulties because their Internet access is typically lower than that of the general population (Fox & Purcell, 2010), although this “digital divide” is reducing over time (Australian Bureau of Statistics, 2009, 2011). Some people with disability might also need training or practice in how to use online research platforms (Dattilo et al., 2008; Turney & Pocknee, 2005). Others might simply prefer a face-to-face approach or have physical or other limitations precluding their use of a computer.
An advantage of asynchronous online methods (such as email interviewing and online forums) is that they offer participants greater convenience: they can engage with researchers in their own time, at their own pace, and in their own location (Bowker & Tuffin, 2004; Seymour, 2001). A staggered contribution is particularly helpful for those who experience symptoms such as fatigue (Guise et al., 2007). Because participants can access the Internet at any time, they can revisit their ideas and potentially edit or extend them (Egan et al., 2006; Seymour). The ability to take part in their own home can help people to feel safe sharing what might be quite personal stories and experiences (Bowker & Tuffin; Egan et al.). It also translates into savings in travel costs and time (Egan et al.).
An anonymous online environment might reduce the social barrier to being rude that exists when meeting in person, raising the possibility of some voices being silenced by rude or disparaging comments. Yet face-to-face focus groups can also be dominated by one “louder” person without skillful moderation (Mann and Stewart, 2000). Others have found that the anonymity of the online environment can encourage greater disclosure (Campbell et al., 2001; Turney & Pocknee, 2005).
For researchers, data collected online present a number of differences, particularly in the analysis. Although the paralinguistic cues that are a foundation of face-to-face qualitative research are not typically captured, textual cues are often used. The use of capital letters, emoticons, and abbreviations (such as LOL for laugh out loud) can infer body language, emphasis, and voice inflection (Kenny, 2005; Seymour, 2001), but it is unclear if these textual cues would be used by older participants. Typing a response might encourage participants to engage in a more expansive discussion and might reduce verbal communication barriers for some (Benford & Standen, 2011; Seymour). In fact, researchers have commented on the richness and eloquence of participants’ written responses (Benford & Standen; Egan et al., 2006).
Asynchronous online data collection typically runs for several weeks (Williams, Giatsi Clausen, Robertson, Peacock, & McPherson, 2012). There can be time and costs savings in not having to transcribe data (Bowker & Tuffin, 2004; Seymour, 2001), but lengthy data collection periods or the degree of interaction required by a researcher could still mean face-to-face methods are more efficient (Egan et al., 2006). Conducting qualitative research online can also make it more difficult to build rapport with participants, with some authors suggesting that a face-to-face meeting with participants with disability prior to data collection is required (Bowker & Tuffin; Egan et al.; Ison, 2009). Early ethical concerns with online qualitative research centered on accessing and analyzing publically accessible forums without participants’ knowledge (Eysenbach & Till, 2001); however, for participants who actively volunteer to take part in online research projects, it is argued that the ethical considerations are no more sensitive than for face-to-face qualitative research (Williams et al.).
Numerous authors have reflected on the relative merits and challenges of online qualitative research compared with face-to-face methods (Egan et al., 2006; Stancanelli, 2010; Williams et al., 2012), but there has been limited consideration of the implications of the different methods for participation by people with disability or chronic illness, or for the collection and intepretation of data. The opportunity arose in a larger study to conduct an online forum in addition to face-to-face focus groups. The objective of this article is to compare the aspects of research planning and conduct, access and participation, and data and analysis for two methods of qualitative research with identical aims.
Methods
In the first stage of the IN-DEEP study (
To encourage greater participation in this study, we used an online forum in addition to four face-to-face focus groups. Incorporating an online data collection method was particularly appropriate given our focus on Internet use in health information seeking (Egan et al., 2006; Seymour, 2001). Contrary to the general trend for lower Internet access for people with a disability, people with MS (and presumably their family members) are high users of the Internet (Bishop, Frain, Espinosa, & Stenhoff, 2009; Lejbkowicz, Paperna, Stein, Dishon, & Miller, 2010), and it was likely that having an online forum would lead to increased participation, especially for those unable to attend a face-to-face focus group.
Participants included people with MS and family members of people with MS in the Australian states of Victoria and Tasmania. We included family members because they might seek health information in addition to or on behalf of the family member with MS. Demographic and disease-related data collected from participants included gender, age, time since diagnosis with MS, education, self-reported disability level, postal code, and whether or not participants used the Internet to seek health information. We conducted the focus groups first and promoted them via email and mailouts through the networks of MS Australia, the peak body providing support and advocacy for Australians with MS. Across the four focus groups, a total of 27 people participated (21 women, 6 men; 20 people with MS, 7 family members). The La Trobe University Faculty of Health Sciences Human Ethics Committee granted approval for the project.
The focus groups, lasting 1 hour, were conducted in a standard way, with two researchers present, audio recording, and full transcription. For each focus group, we had one moderator and the second person took notes and made sure all the questions were addressed. We asked participants about their health information seeking, using the following four questions to guide the discussion: Where do you get reliable information on the evidence of treatments for MS? What kinds of information do you need, and how do these needs change over time? How do you use the Internet to access information about treatments for MS? How do you assess the quality and usefulness of this information?
Participants were initially asked to describe what kind of information seeker they were (i.e., “likes to know everything” or “operates on a need-to-know basis”). Few prompts were required because participants were keen to share their experiences and provided rich stories and descriptions that answered our questions. Prompts included asking participants to describe their experiences with information provision through doctors and other health professionals, whether they used social networking Web sites, what kind of information was preferred from different sources, and the information that they had difficulty finding.
Participants who responded to the focus group flyer but were unable to attend were invited to take part in the online forum, with additional recruitment through the email networks of MS Australia. The month-long online forum was held 2 months after the last focus group. Thirty-three people participated (26 women, 7 men; 25 people with MS, 2 family members). The online forum was created specifically for this study, with MS Australia information technology staff ensuring that it was easy to navigate and accessible to those with vision impairments (a common issue for people with MS). The forum was conducted on a password-protected discussion board on the MS Australia Web site.
We sent online forum participants hard copies of the information and consent forms and demographic forms in reply-paid envelopes. On receipt of their completed paperwork, participants were emailed their individual username and password. We invited participants to log in any number of times and post responses to 10 questions about their MS information seeking and to the comments posted by other forum participants. The 10 questions we used were based on the focus group questions and included: Tell us about your experiences finding information about treatments and therapies to manage MS on the Internet. How do you decide which information about MS treatments and therapies you’ll trust?
We checked all comments for appropriateness, but the moderator did not engage in discussion on the forum itself. We sent a weekly email to all participants encouraging them to take part and advising them when two new questions were added partway through. Two participants expressed an interest in taking part in the online forum but were unable to participate because of physical limitations; they received additional assistance to participate offline and we manually added their comments to the online forum questions.
Thematic analysis was underpinned by an interpretivist framework (Allsop, 2013), wherein we sought to explore and understand the subjective experiences of participants (Green, 2013). Initially, we analyzed qualitative material from the focus groups and online forum transcripts separately. Two researchers read the transcripts several times to familiarize themselves with the key issues and identify emerging themes and categories. In consultation with a third researcher, we developed and applied a coding frame to compare and organize the data into categories, themes, and relationships (Krueger & Casey, 2009). Because of the overlapping nature of the themes that emerged from the two data sets, we applied the same basic codes to each set of data and then analyzed them together. In addition, we analyzed the data from the people with MS and family members together because we felt there were too few family members to be able to reliably draw conclusions about similarities and differences. We used NVivo qualitative data analysis software (QSR International, 2008).
For the demographic data, we classified each participant’s location as metropolitan or nonmetropolitan based on the Australian Bureau of Statistics’ Accessibility/Remoteness Index of Australia (Commonwealth Department of Health and Aged Care, 2001) for postal codes. Self-reported disability levels were measured using a modified version of Hohol, Orav, and Weiner’s (1995) Disease Steps Scale used in the Australian MS Longitudinal Study, which can be collapsed into three categories (Wollin et al., 2010). We compared quantitative demographic and MS-related data using SPSS (Version 18). We analyzed continuous variables (age and years with MS) by independent t test and the remaining demographic and MS-related variables by chi-squared test.
Results
Access and Participation
Overall, the demographic and MS-related characteristics of focus group and online forum participants were similar, with no statistically significant differences between groups (see Table 1). Both groups had a gender ratio reflective of the broader MS population (3 to 1 in favor of women; Compston & Coles, 2002)). Mean age of focus group and online forum participants was similar (48.6 ± 11.6 years vs. 51.1 ± 12.3 years), with both including a wide range of ages (22 to 76 years and 22 to 73 years, respectively). Mean length of time since diagnosis with MS was 11 years; both groups included people newly diagnosed with MS (within the previous year) and those living with MS for more than 30 years. Participants in both groups were high online health information seekers (89% and 91%, respectively), reflecting our e-recruitment strategy.
Demographic and Multiple Sclerosis–Related Characteristics of Participants.
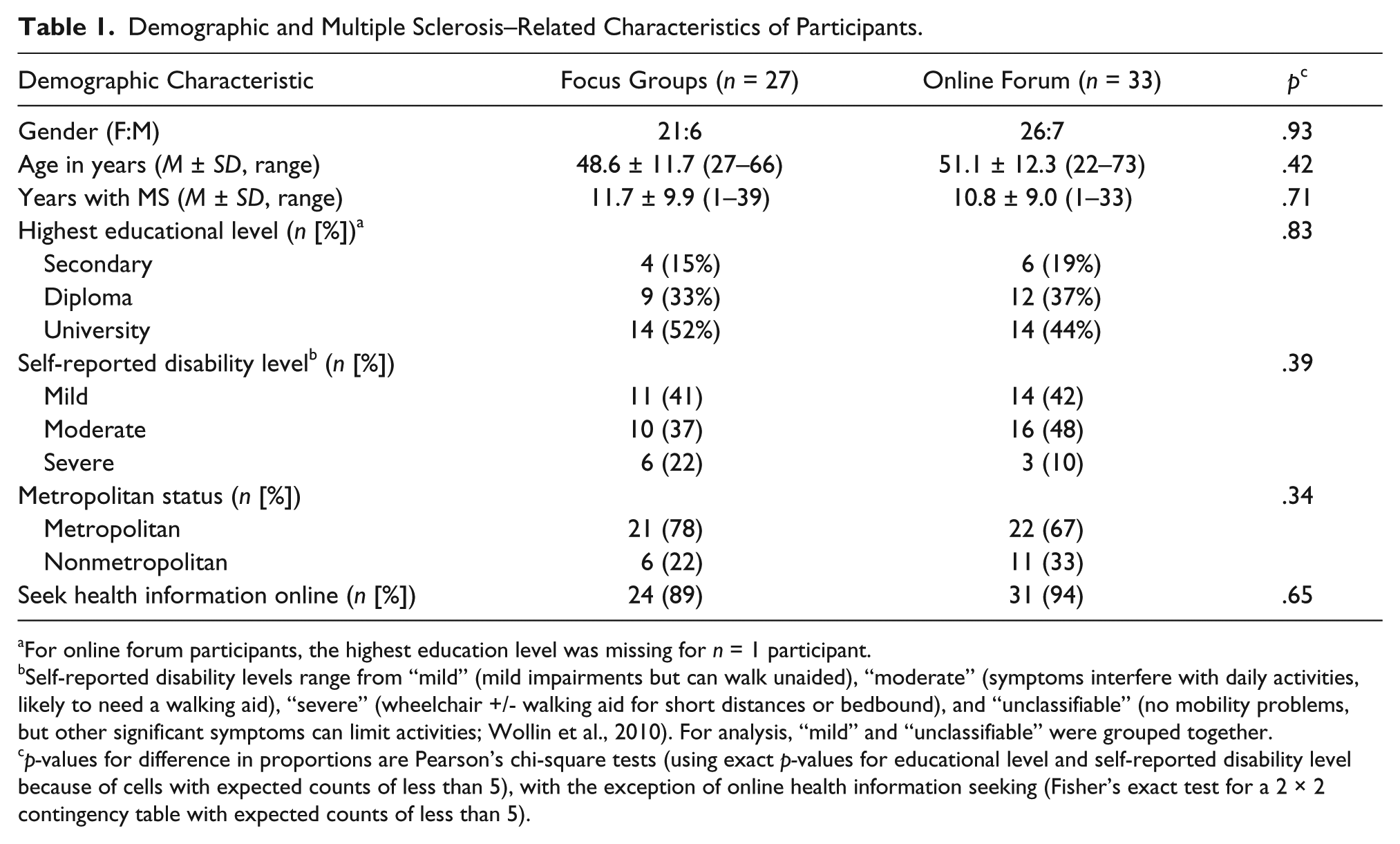
For online forum participants, the highest education level was missing for n = 1 participant.
Self-reported disability levels range from “mild” (mild impairments but can walk unaided), “moderate” (symptoms interfere with daily activities, likely to need a walking aid), “severe” (wheelchair +/- walking aid for short distances or bedbound), and “unclassifiable” (no mobility problems, but other significant symptoms can limit activities; Wollin et al., 2010). For analysis, “mild” and “unclassifiable” were grouped together.
p-values for difference in proportions are Pearson’s chi-square tests (using exact p-values for educational level and self-reported disability level because of cells with expected counts of less than 5), with the exception of online health information seeking (Fisher’s exact test for a 2 × 2 contingency table with expected counts of less than 5).
With regard to self-reported disability level, more than half (59%) of the focus group participants reported their disability level as “moderate” or “severe,” as did most (58%) online forum participants. Approximately 22% of focus group participants lived in nonmetropolitan areas compared with 33% of online forum participants. This indicates a slight (albeit statistically nonsignificant) trend toward greater online participation by people with MS in nonmetropolitan areas. The small number of participants in each research group might have limited the ability to distinguish statistical similarities or differences.
Data and Analysis
The online forum transcripts contained less “noise”: participants were more succinct in their responses and less likely to stray from the topic. Focus group participants tended to think while talking and were subject to interruption; as such, their comments made less sense when read in the transcript. They also tended to share more stories, potentially providing richer data, but some of these stories were not always relevant to the research questions. In contrast, the online forum respondents tended to be more articulate, providing more concrete examples of where and how they searched for information. Their responses were often both eloquent and emotionally powerful:
I have gradually come to accept that my condition is individual to myself, and that MS differs in different people. I am like [another participant], very lucky that I have minimal symptoms, and think that the actual psychological impact of MS on me was almost greater than its physical impact. So far, for me, MS’ bark has been worse than its bite. For this reason I don’t feel the need to really immerse myself in MS information, and to some extent it is depressing for me to do so. (Person with MS [PMS], online forum [OF])
The focus group data were easier to analyze than the online forum data in some respects, because of the advantages of having paralinguistic cues and revisiting the audio recordings. Recall of the demographics and contextual information about each participant (i.e., gender, age, length of time since diagnosis, and other information gleaned on meeting them) assisted with reading and coding participant comments. Because we had not met the online forum participants in person, it was not possible to put a “face to the name” when reading, so we had to cross-check their demographic and MS-related details with our records.
As the analysis progressed, it became apparent that the ideas expressed by participants and the themes generated overlapped. Although we do not intend to dwell on the thematic results in this methodological article, we include a selection of the themes. For example, in relation to changes in information seeking over time, many participants described a period of high information seeking soon after diagnosis before reaching “information overload.” Participants moved from searching various sources for a range of things to using a refined or restricted number of trusted sources:
I see my neurologist once a year and I know he’ll tell me anything I need to know. And if something comes up I’ll hear it because I watch the news and I read the papers. So I don’t actively seek out anything on MS anymore. (PMS, focus group [FG]) At first I read everything and took everything on board. Now I am selective and really just do what is working for me. (PMS, OF) I look for anything medical that I can see that it’s actually come from like an MS-based society or a medical or something like that. I don’t ever go to just any . . . I don’t go to forums and things like that, I try and stick with medical based. (Family member [FM], FG)
Participants in both groups expressed a desire to engage with health professionals in a research partnership. Many were uncertain about how to judge the quality of the information they found online and highly valued health professionals who could help them interpret and appraise the information they had found:
If I read something on the Internet and I sort of think, “Mmm sounds okay,” then I’ll ask the MS Society or the neurologist have they heard anything about it, what’s their opinion, because you can read all sorts of things on the net [Internet] and you don’t really know whether it’s truth or not. (PMS, FG) I listen to my neurologist. Other friends with MS often have found a “possible” helping aid for heat, cramping, etc., but I don’t trust the Internet unless the information is coming from a reliable, well-known source. (PMS, OF)
Though the ideas expressed and themes generated overlapped, differences emerged in how participants expressed themselves and described their experiences. Focus group participants shared more stories and tended to introduce their examples of information seeking with stories to contextualize this information. Many of these stories centered on their experiences of being diagnosed with MS. Online forum participants tended to provide more examples of their information-seeking behaviors. These differences often complemented each other, allowing greater differentiation between themes and hastening data saturation:
After going to all and sundry, an ear, nose, and throat guy told me over the phone, “You have MS,” and I shat my pants. . . . So anyway, I had a preconception that, holy shit, you’re gonna be in a wheelchair and you’ll be a vegetable in six months, etc., etc. So I put that energy of fear into going, all right, well, what is the story with it, and just got on the Internet and looked up MS. . . . [I] just tried to hunt down any information I could find about it, more so to understand what I was in for . . . just so that I could formulate a battle plan. (PMS, FG) I use the [MS-specific] Web site from time to time, which is great to ask questions of people registered with MS. It is really informative if asking about specific things, e.g., catheter use or side effects of treatment, and how they impact certain people. Also it can be a reassurance for newly diagnosed MS people. There is always someone who has experienced something and everyone is kind enough to share their experiences. I find this very supportive. (PMS, OF)
Observations on the Research Method
In both the focus groups and the online forum, participants engaged in some sharing of information resources and the provision of informal support. Such activities were more prominent in the focus groups; some participants (particularly those who were newly diagnosed) commented at the end of the session how useful it was to pick up some more tips about good sources of health information (names are changed):
I’d be really interested to know Sue’s opinion on how she decides on what’s sensible or not because being of a science background. (PMS, FG) I’m a bit like John. I would really see where the funding [has come from and] where the research has been done, and whether or not it’s in peer-reviewed articles. (Sue; PMS, FG)
After one focus group, participants who were previously unfamiliar with each other stayed behind and talked among themselves for 30 minutes; one participant said that he would look into becoming more involved with the support services of MS Australia after learning about them in the focus group. Some online forum participants did read and respond to the comments of others, but much less interaction occurred between them. Although taking part in a focus group facilitated greater sharing of information between participants, there were inevitably those who spoke more than others. The online forum provided a more “equal social environment” because everyone who logged on could post a comment without being drowned out by louder voices. However, one online forum participant responded to another person’s comment by telling them to “get a grip” and to stop “blaming and complaining.” The moderator deleted this post. Similar negative interactions were not observed in the focus groups.
We did not record researcher time to enable us to compare the cost of one method with another, but the online forum appeared to be a time- and cost-efficient way of including an extra 33 participants in the project. Because the ideal number for focus groups is six to eight people (Carter & Henderson, 2005), an additional five focus groups (with two researchers, in varying locations) would have been required to obtain the same number and geographical spread of participants. The transcripts were readily downloadable at the conclusion of the online forum, saving on transcription costs. We benefited from an existing secure online platform established by MS Australia, but the cost of establishing an equivalent platform would need to be considered in an overall assessment of costs.
Discussion
Participants in the online forum were demographically similar to those taking part in a face-to-face focus group, with a slight (but nonsignificant) trend toward higher participation by people living in nonmetropolitan areas. Despite the small sample, this trend supports the assertion that online methods can facilitate participation in research for people who are otherwise unable to participate for reasons of geographical distance (Egan et al., 2006; Guise et al., 2007). Two other studies that have directly compared demographic characteristics in people with disability or chronic illness using the two methods reported conflicting results: Campbell et al. (2001) found that online forum participants were younger, more educated, and wealthier, whereas Nicholas et al. (2010) found that participant characteristics were similar.
We found that online methods did not compromise the data generated. Similar themes were evident in the transcripts, although the focus groups generated discussion and the online forum generated thoughtful reflection and description. The fact that very similar themes emerged strengthened our view that the data sets were equally valid and could be reliably analyzed together. The thematic overlap we identified is consistent with the findings of Guise et al. (2007) and Campbell et al. (2001); however, by commencing our research with face-to-face methods, we gained familiarity with the community and the issues and “tested” our questions and prompts. This means that we cannot exclude the suggestion that our interpretation of the online data was informed by the face-to-face experiences.
Our results echo those of previous research, finding that online forum participant responses were more succinct, articulate, and remained directly on topic (Benford & Standen, 2011; Campbell et al., 2001; Egan et al., 2006; Nicholas et al., 2010). Similarly, face-to-face focus group participants tended to be more expansive in their descriptions and stories, adding richness to the data, though the details were at times peripheral to the research question (Campbell et al.; Nicholas et al.). Like previous researchers, we found that focus group participants engaged in more interaction and gained more informal support from others, yet the discussion was more likely to be dominated by the views of a single person (Campbell et al.; Nicholas et al.). These differences need to be considered when weighing up research options.
Our findings reflect the fact that our research topic, online health information seeking, lends itself to an online research approach. The data we sought were reasonably concrete, and the addition of participant interaction/support, plus the paralinguistic cues in interpretation, were not considered essential to the project. Using this approach to research other topics with other participant groups and contexts might not be as practical or appropriate, nor generate such similarities in participant characteristics and themes (Nicholas et al., 2010). Consistent with others, our view is that the addition of an online forum allowed us to involve considerably more people than we could have achieved in conventional focus groups, given the funding available (Bowker & Tuffin, 2004; Seymour, 2001). Flexibility of attendance in an online forum also appeared to be more convenient for participants. However, we engaged in online forum monitoring, rather than moderating. More active moderation and engagement with participants would increase the costs associated with an online forum.
We are reluctant to conclude that online methods can replace focus groups (in certain situations) for people with chronic illness or disability, but they are undeniably feasible, potentially cost-saving, yield generally comparable information, and enable participation by many people who would not otherwise be able to attend. Researchers need to balance some of the issues raised in the context of reaching a wider group of people.
Footnotes
Authors’ Note
This article is based on a presentation given at the Social Participation: Knowledge, Policy and Practice Conference, November 28, 2011, in Melbourne, Australia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MS Research Australia (Synnot, Hill), MS Australia—ACT/NSW/VIC (Synnot, Hill).