
Abstract
In this study, we aimed to explore the process of recovery over time from the perspective of those who had fully recovered from chronic anorexia nervosa (AN), using stringent recovery criteria. Eight women, assessed as fully recovered from chronic AN, told their story of the process of recovery. Data were analyzed using the qualitative method, narrative inquiry. Recovery was identified as a long and complex process that spanned four phases: from being unable or unready to change, to experiencing a tipping point where motivation increased and changed in quality, allowing the women to take action against the AN and finally allowing them to reflect and rehabilitate. Results provide a framework for understanding this complex process. Findings suggest that full recovery from chronic AN is possible and emphasize the importance of hope, motivation, self-efficacy, and support from others in the recovery process.
Anorexia nervosa (AN) is a serious mental illness associated with numerous physical and psychological concerns. AN has no single etiology or pathway, but rather appears to be influenced by multiple risk factors, such as genetic predisposition, family disturbance, social and cultural pressures, low self-esteem, and high anxiety (Steinhausen, 2002). The effects of AN can be devastating for the sufferer. AN has the highest mortality rate of any mental illness (Beumont & Touyz, 2003), and research suggests that fewer than half of survivors do well over time (Steinhausen).
Recovery from AN is a complex phenomenon that has been explored from a variety of approaches. Most research in this area has been conducted from the fields of psychology and medicine, which largely adopt a medical-model approach to recovery. The majority of research within these fields has been undertaken from the perspective of quantitative outcome studies that focus on the probability of recovery and relapse over time. A handful of researchers have explored recovery from AN using qualitative methods in an attempt to understand the patient’s experience. These qualitative studies have identified themes associated with recovery from AN, such as supportive relationships, family, determination, self-confidence, self-discovery, self-acceptance, motivation to change, and being understood (Federici & Kaplan, 2008; Lamoureux & Bottorff, 2005; Nilsson & Hagglof, 2006; Tozzi, Sullivan, Fear, McKenzie, & Bulik, 2003). Outside the fields of psychology and medicine, sociologists and anthropologists have examined the social and cultural meanings ascribed to AN and its recovery, and have suggested that cultural practices, gender, and embodiment are important considerations (e.g., Garrett, 1997; Warin, 2010).
Despite the growth of research into AN from multiple perspectives, our understanding of AN recovery is limited. In general, recovery in mental health is a complex issue. Researchers have looked broadly at recovery across diagnoses resulting in two predominant models. One of these models, the medical model, has become the dominant approach in the field of eating disorders. This model positions recovery as an objective “cure,” a condition defined by the absence of symptoms and a return to normal functioning (Roberts & Wolfson, 2004). The other, the recovery model, is driven by consumers, positioning recovery as part of a personal journey, the product of empowerment and resulting in an improvement in quality of life (Anthony, 1993). There is a relative absence of research explicating the implications of these two models for AN. At the same time there remains uncertainty about the factors that lead to successful recovery. Reliable prediction as to which patients will recover and which will spend a lifetime with AN is still not possible (Strober, 2004). These issues raise serious questions as to how and why some people recover whereas others do not.
Significant methodological issues relating to the definition and measurement of recovery from AN have also clouded our understanding. There is a lack of a consensus definition in the field as to what constitutes recovery from AN. Definitional criteria vary vastly between studies (Couturier & Lock, 2006). In outcome studies and treatment trials, recovery is often defined as failing to meet recognized diagnostic criteria for AN, such as the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV; American Psychiatric Association [APA], 2000). However, this does not necessarily mean a return to full physical and mental health. Although patients might have regained weight, they might still experience psychological problems and be susceptible to eating disorder cognitions (Lowe et al., 2001).
Recently, researchers have identified the importance of a comprehensive, definitional approach, which includes the resolution of psychological symptoms as well as physical and behavioral symptoms. Despite this evidence, such an approach has not been consistently used (Bardone-Cone et al., 2010). The time period required for the patient to be symptom-free has also varied, with some researchers requiring only brief time periods—in some cases as little as 8 weeks—to be considered recovered (Strober, Freeman, & Morrell, 1997). It is questionable whether these researchers are studying full or temporary recovery, because such definitions might not account for later relapse.
In most of the qualitative studies exploring “recovered” patients’ perspectives, the researchers have also adopted vague or questionable recovery criteria, with a significant lack of formal assessment for recovery status (Nilsson & Hagglof, 2006; Patching & Lawler, 2009). Many have required participants to self-define as recovered (D’Abundo & Chally, 2004; Jenkins & Ogden, 2012; Lamoureux & Bottorff, 2005; Weaver, Wuest, & Ciliska, 2005). Other researchers have recruited participants in various “stages of recovery” (Garrett, 1997; Hardin, 2003; Jenkins & Ogden, 2012) or still in the process of recovering from an eating disorder (D’Abundo & Chally, 2004; Darcy et al., 2010). These equivocal findings raise questions of the trustworthiness of the data of the few qualitative recovery studies in the published literature. The inclusion of participants who are not fully recovered for such research is problematic considering that studies indicate that the individual’s view of recovery is influenced by illness status (Keski-Rahkonen & Tozzi, 2005), and those with eating disorders are perceived as lacking insight into underlying psychological features of their disorder (Michel, 2002).
An additional limitation of previous studies is the lack of attention to the process of recovery over time. Outcome studies have provided little insight into the complex process from illness to recovery (Strober et al., 1997) and provide a superficial representation of the actual experience of recovery (Matusek & Knudson, 2009). Qualitative studies have provided some awareness of the themes that facilitate recovery; however, their benefit is limited when there is little understanding of the sequence of themes, whether factors are intertwined, and perhaps most significantly, how individuals might operationalize recovery. We are left with a fragmented understanding of how the various aspects of recovery might connect and little understanding of temporal processes.
The Transtheoretical Model of Change (TMC; Prochaska & DiClemente, 1982) has been used by some researchers to explain the process of recovery. This model posits that change occurs over five key stages (precontemplation, contemplation, preparation, action, and maintenance). Nonetheless, it remains unclear if these stages can explain recovery from AN (Dray & Wade, 2012; Waller, 2012; Wilson & Schlam, 2004). It is most likely that clinicians and patients have little knowledge of what to expect of the AN recovery process.
Many people with AN will go on to develop a protracted course of the illness, some for decades, with the possibility of recovery lessening as the duration of AN increases (Strober, 2004). To our knowledge, there has been no published study exploring recovery from AN when it is long term and chronic. Chronic AN, which is defined here as experiencing AN for a duration of more than 7 years (George, Thornton, Touyz, Waller, & Beumont, 2004), is gravely concerning because it is resistant to traditional treatments and is associated with very high levels of impairment in most areas of life (Lowe et al., 2001). Those with chronic AN tend to have the poorest outcomes, exhibit an extreme ambivalence about change, and are ego-syntonically attached to their disorder. A small but growing body of research has been conducted on chronic AN; however, we know little about chronic patients and appropriate treatments for this group (Wonderlich et al., 2012). To our knowledge, full recovery from chronic AN, including the maintained resolution of physical, behavioral, and cognitive symptoms, has not been documented. We might learn the most from any who are found to have recovered from chronic AN, because their recovery is arguably the most remarkable of those suffering the illness.
The aim of the current research was to address some of the critical gaps in the literature. Our focus was the process of recovery from chronic AN from the perspective of participants who had fully recovered according to a comprehensive, stringent, and objective definition of recovery. Our position on recovery is drawn from both the medical and recovery models. The objective method for determining recovery was chosen to ensure a consistent sample of participants, increasing the trustworthiness of results. Personal processes and subjective experience were prioritized in the data collection and analysis. In this way, we adopted an interpretivist paradigm by placing importance on participants’ own interpretations of their experience.
Method
Inclusion Criteria / Definition of Recovery
The comprehensive recovery criteria, informed by Bardone-Cone and colleagues (2010), included weight, behavioral, and psychological indices. The combination of both weight and psychological criteria has been found to yield the most accurate representation of recovery (Bardone-Cone et al.). We defined recovery as (a) a body mass index (BMI) between 20 and 25 kg/m2 (placing participants well out of the underweight range); (b) absence of behavioral features of an eating disorder (e.g., restrictive eating, bingeing, purging); and (c) scoring within 1 standard deviation of community norms on all subscales of the Eating Disorder Examination (EDE; Fairburn & Cooper, 1993): restraint, eating concern, weight concern, and shape concern (placing participants in the normal ranges for body-image concerns). The EDE is a standardized, investigator-based interview that measures the severity of the characteristic psychopathology of eating disorders and is considered the “gold standard” when assessing for eating disorder psychopathology.
Participants were required to have been recovered for 5 or more years (self-reported) and to have had AN for more than 7 years. The first author assessed for past AN based on DSM-IV (APA, 2000) criteria. Height and weight measurements were taken by the first author. Research has indicated that self-reported height and weight tend to be inaccurate; therefore, direct measurement of height and weight is the optimal method for assessing BMI (Engstrom, Paterson, Doherty, Trabulsi, & Speer, 2003).
Participants
Purposive sampling, specifically extreme sampling, was used. This method is appropriate when exploring atypical manifestations of phenomena, such as outstanding recovery stories (Sandelowski, 1995). Following approval from The University of Sydney Ethics Committee, participants were recruited through use of the media, with details of the study published in Australian national newspapers and broadcast on radio and television. Eighty-six interested people contacted us and were sent information about the study (see Figure 1); 56 were excluded because of either (a) residing more than 100 kilometers away (precluding researchers from taking height and weight measurements in person); (b) not meeting inclusion criteria; (c) declining to participate; or (d) failing to contact the researchers after receiving additional information about the study.
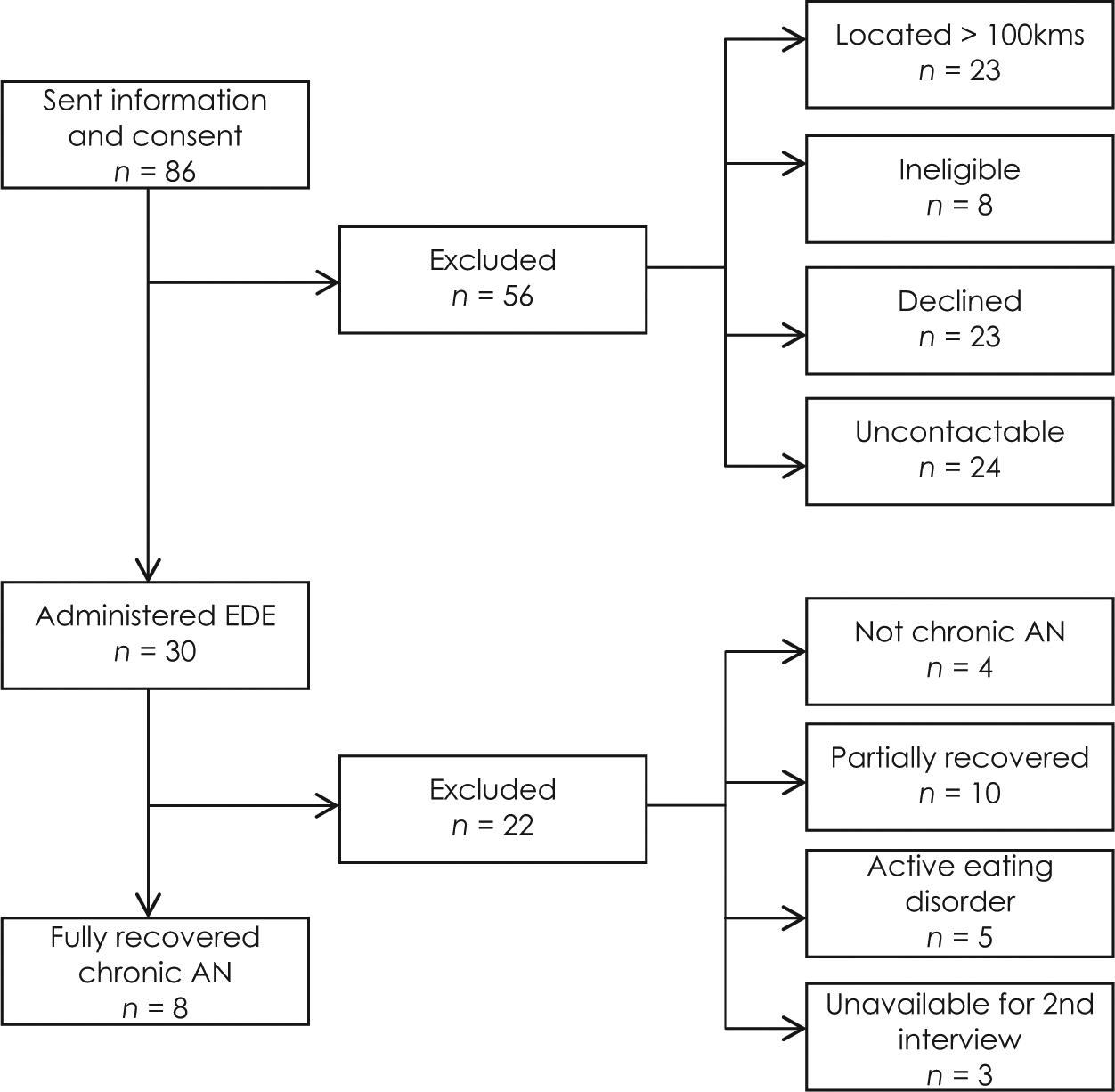
Recruitment procedure.
Following this, 30 participants, who identified as recovered and appeared to meet criteria regarding the duration of illness, were administered the EDE (Fairburn & Cooper, 1993) over the phone to assess for recovery status. Additional details of the duration of illness were taken at this point. Written consent was obtained and all participants were informed that participation in the study was strictly confidential. Of the 30 people screened, 1 participant was a man. Of those screened, 19 were excluded because they did not meet recovery criteria and 3 were unable to attend the face-to-face interview. Finally, 8 people (all women) were assessed as being fully recovered and participated in the study. When using extreme sampling, smaller sample sizes are sufficient given the rarity of the subject of interest (Sandelowski, 1995), and such a sample size is consistent with other studies using the same method employed in this study to explore recovery from mental illness (e.g., Kirkpatrick & Byrne, 2009).
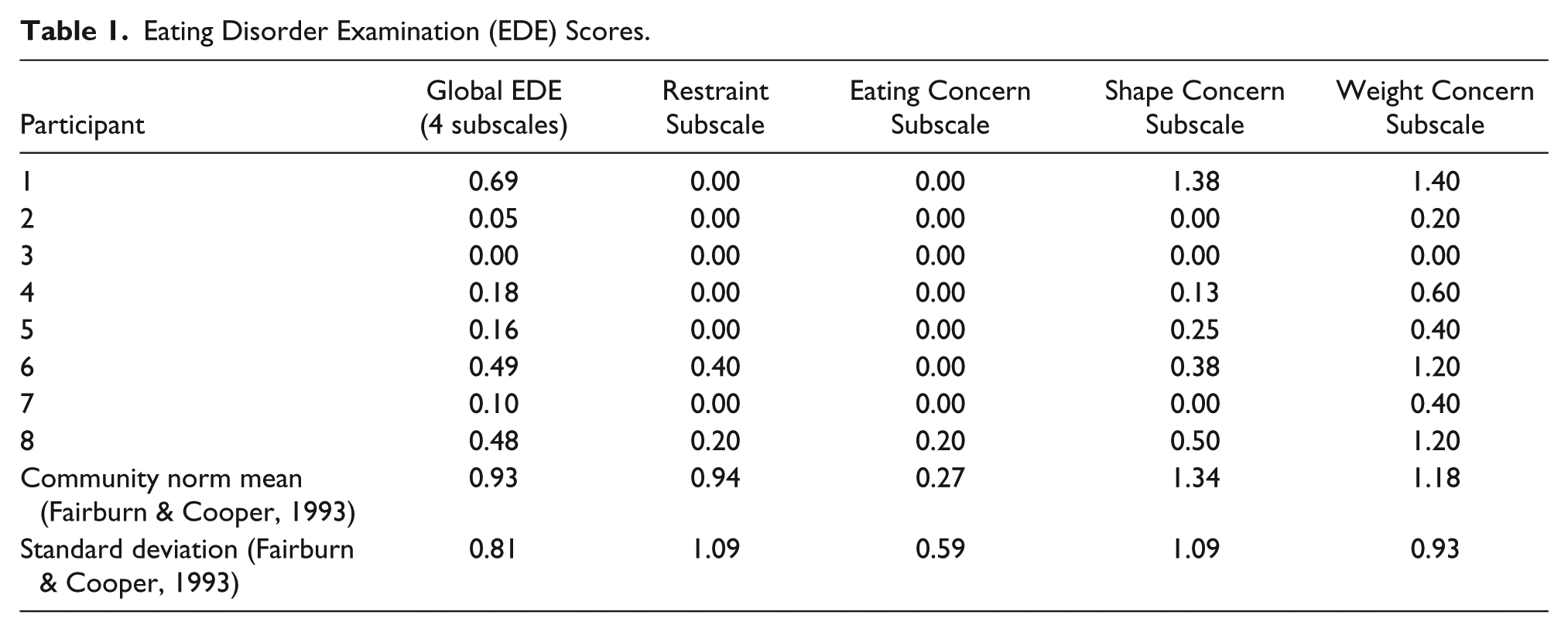
The 8 participants ranged in age from 31 to 64 years. All scored within 1 standard deviation of community norms on all subscales of the EDE (Fairburn & Cooper, 1993; see Table 1) and had an absence of behavioral features of an eating disorder. Participants estimated the number of years they had an eating disorder, which ranged from 9 to 44 years (average duration 15.5 years). Participants reported the number of years they had been fully recovered, which ranged from 5 to 30 years (average duration 13 years). Despite differences in length of illness and length of time since recovery, no differences were noted in participants’ capacity to recall the details of their recovery process or their ability to reflect on this. Four of the participants reported having experienced some form of childhood sexual abuse.
Eating Disorder Examination (EDE) Scores.
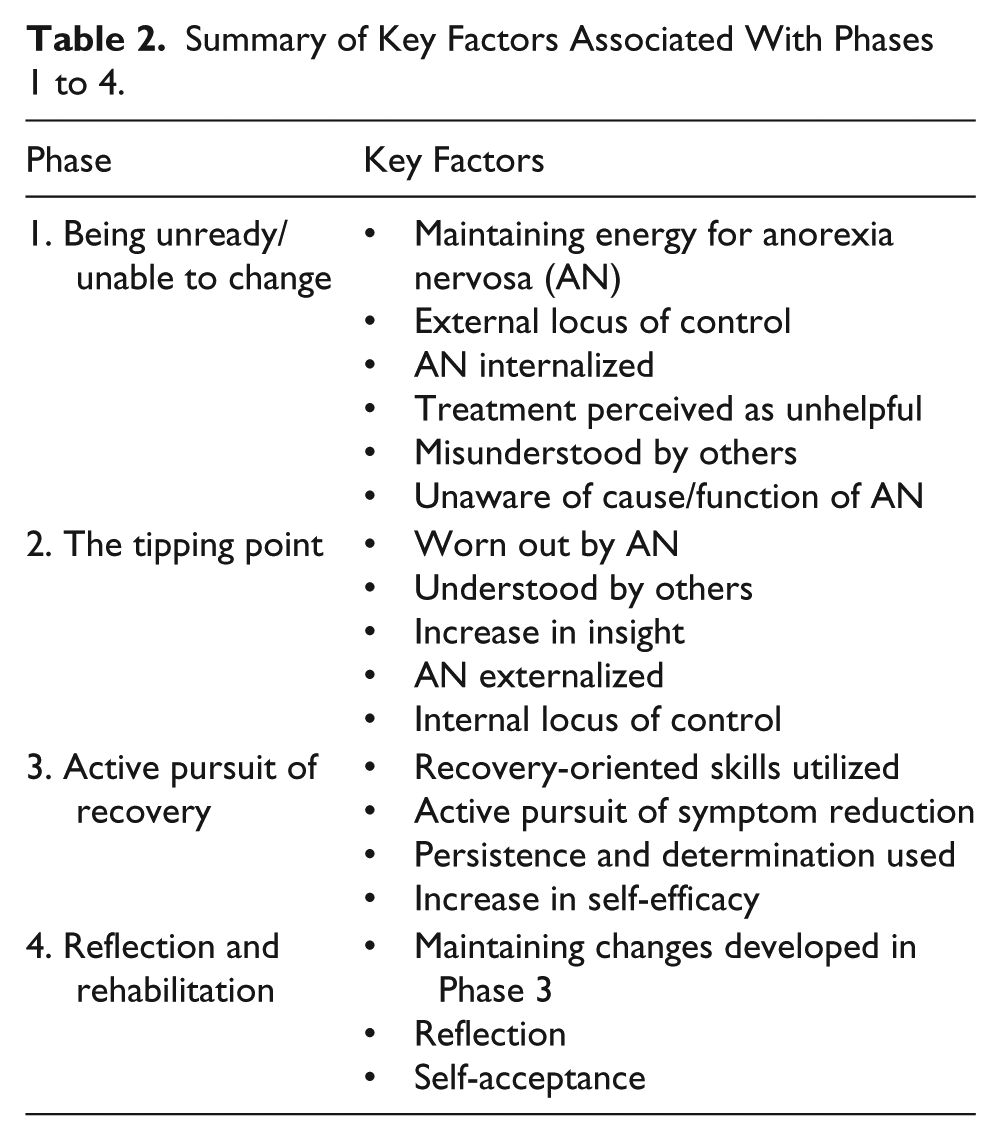
Summary of Key Factors Associated With Phases 1 to 4.
Design
Narrative inquiry (Clandinin & Connelly, 2000) was used for this research. This method involves the collection and analysis of personal narratives of experience as a means to understand human action (Riessman, 2005). We chose this method because it is particularly useful for investigating a process over time, such as recovery (Murray, 2003). Unlike other qualitative methods, such as grounded theory, narrative inquiry has the ability to portray a holistic depiction of phenomena, as opposed to a fragmented account of a larger picture (Howie, 2010). This is important when trying to understand the temporal process of recovery, as opposed to the identification of contributing factors in isolation.
This method also allows the research participant to maintain more control of the topic under investigation because the narrator determines how events are described and how various elements are connected. Narrative inquiry takes a co-research position between participant and researcher (Kirkman, 2008). In using narrative inquiry, we adopted a constructionist approach (Holstein & Gubrium, 2008) in that we viewed meaning as cocreated between the researcher and participants. In our analysis, we prioritized the participants’ interpretations of their individual experience.
Procedure
Following initial screening for recovery status, the first author conducted individual, in-depth, face-to-face interviews. During interviews, participants were invited to tell their story of the experience of developing, living with, and eventually recovering from AN. Following interviews, we took each participant’s height and weight measurements. Interviews were approximately 1.5 hours in duration and were audiorecorded and transcribed verbatim.
Transcripts were then used to create a narrative summary of the process of recovery for each participant. Creating a narrative summary involved placing data from the transcript into temporal order (starting from the development of AN and ending with present day). Data from the transcript were organized so that narratives had a clear beginning, middle, and end, or what Polkinghorne (1995) described as a chronological organization method. Narratives were created with an emphasis on maintaining plot, scene, and narrative flow, as well as preserving the “voice” of each individual participant. This was done by using participants’ own words as much as possible. We removed extraneous material from the interview that was unrelated to the research question, as well as any identifying data, to increase confidentiality. In an effort to capture the detail of participants’ experiences as well as pay respect to their stories, the narratives were in-depth, averaging around 5,000 words.
To enhance the rigor of the data (Clandinin & Connelly, 2000; Kirkman, 2008; Kirkpatrick & Byrne, 2009), the narrative summary was member-checked with each participant to ensure it reflected her story and understanding. Participants were emailed copies of the narratives and were invited to give feedback, either by email or over the phone. They were able to add to or alter the summaries because the narratives were cocreations between researcher and participant. Alterations to the narratives by participants were minimal; some were clarifications about details or extra insight or comments. Once participants endorsed each narrative as an accurate account of her experience, we analyzed the narratives individually and across participants.
Data Analysis
The narratives were exported to the computer software program, NVivo (Qualitative Solutions Research, 2010), for initial coding. Each narrative was first analyzed in depth, line by line, on its own. Main themes and subthemes were identified. Narratives were then analyzed across participants, which Polkinghorne (1995) called paradigmatic analysis. To analyze the process of recovery over time, we synthesized each narrative to a timeline outlining the process from illness development to present day. We positioned the identified themes from the initial coding along the timelines to place them in temporal context. It was then possible to examine commonalities across narratives (Kirkpatrick & Byrne, 2009) and to analyze the chronological and unfolding dimension of the women’s experiences. From this, similarities in the individual processes of recovery emerged.
In line with our interpretivist approach, inductive analysis was used in which concepts were developed from the data. When higher-order conceptualizations began to emerge from the analysis, evidence was found in the data until a “best fit” was reached (Polkinghorne, 1995). Throughout the analysis, memo writing was used as an analytical strategy to develop higher-order concepts while remaining true to the data. To ensure rigor throughout the process of data analysis, narratives were not only verified and member-checked by participants but also cross-coded by two of the authors. We kept an audit trail to ensure analytic transparency, which allowed data analysis to be traced from initial coding through to final higher-order conceptualizations of the data.
Results
The participants’ descriptions of the course of recovery from chronic AN suggested a very long, multidimensional process that appeared to be marked by four phases: (a) unready and/or unable to change, (b) the tipping point of change, (c) active pursuit of recovery, and (d) reflection and rehabilitation. All of the participants progressed through the phases in the same direction from Phases 1 to 4, although the duration spent in phases differed between participants and individual courses varied. It appeared that for some participants the demarcation of phases was clearly defined, whereas for others there was an overlap between consecutive phases (e.g., Phases 2 and 3 experienced simultaneously). The demarcation of phases (that is, exit out and entry into the next phase) was easier to identify for participants who moved through the recovery process faster compared to participants whose recovery spanned decades; for them, phases tended to be blurred.
Phase 1: Unready and/or Unable to Change
During Phase 1, life for participants was dominated by the AN and marked by heightened distress. This stage was characterized by participants as a time in which they (a) had an external locus of control, (b) internalized the AN, (c) perceived treatment as unhelpful, (d) felt misunderstood by others, and (e) had little understanding of the cause or function of the illness. Participants spent from 4 to 22 years in Phase 1, with the majority of them being in this stage for 4 to 5 years.
External locus of control and internalization of the AN
There was a sense that participants had felt controlled by AN: “At some point the anorexia took over. I didn’t understand why I was doing it but I couldn’t stop.” The AN was perceived as impossible to escape, all-consuming, and chronic. Participants had internalized AN and were unable to externalize the illness. Accordingly, they had a significant lack of agency and low self-efficacy about their ability to make changes.
Unhelpful treatment
Treatment was largely perceived as having been unhelpful, partly because participants lacked faith in their capacity for change, but also because of multiple hospital admissions and repeated failed treatment attempts over many years: “From the ages of nineteen to twenty-seven I had dozens of hospital admissions with no success. . . . Treatment felt like banging my head against a brick wall.” Participants also felt highly disconnected from clinicians and sometimes hostile toward them. They described how clinicians “couldn’t get through to them,” using “scare tactics” to attempt to increase motivation, misdiagnosing them, or targeting treatment in ways patients felt were inappropriate. Some participants described feeling pressured and punished, which led to defiant resistance: “If the clinicians told me what to do I’d think, ‘Well screw you. I’m not doing that.’ . . . It became more about the ‘us’ and ‘them.’” Treatment was sought as a result of external pressures from family and/or health professionals, adding to feelings of alienation: “It felt like the staff at the hospital was telling me there was no hope for me. They thought I was stupid and ignorant.”
Misunderstood by others
Participants felt alienated and misunderstood not only by health professionals but also by family and friends. There was a sense that those around them had difficulty comprehending how AN affected the women, which, in some cases, led to the women perceiving a lack of empathy from others:
Everyone blamed me for making my parents’ life hell. No one was concerned for me. It wasn’t like, “You’re sick, you poor thing.” It was more like, “Why are you doing this? You’re ruining everyone else’s life.” People didn’t understand.
Unawareness of the cause and function of AN
If those around them had difficulty understanding the AN, participants themselves had little insight into AN during Phase 1. This was particularly noticeable for those whose AN appeared to develop in the context of childhood sexual abuse. These participants had little understanding of any potential connection between these traumas and the AN, nor did they recall a history of trauma at this phase.
Low motivation
The combination of external locus of control, internalization of the AN, perception of unhelpful treatment, the feeling of being misunderstood, and a lack of insight into the AN was associated with low motivation to change. In some cases, hopelessness and helplessness were pervasive, shared by patient, clinicians, and family alike. Life outside the eating disorder was not highly valued, which led to maintenance of the illness: “Because I’d been in hospital before, it felt like there was no hope for me. I’d already failed and I was told by the psychiatrist and nurses that there was no hope. Recovery seemed impossible.”
Phase 2: The Tipping Point of Change
After living with the illness for many years and being largely unmotivated to change, the aligning of some key factors in time led to a “tipping point” of change at which the balance finally tipped in favor of pursuing recovery as opposed to continuing with the illness (see Figure 2). For some, this was one discreet moment in time; for others, it was a series of moments. At this stage, the trajectory of the AN was disrupted; motivation increased and meaningful change was triggered.
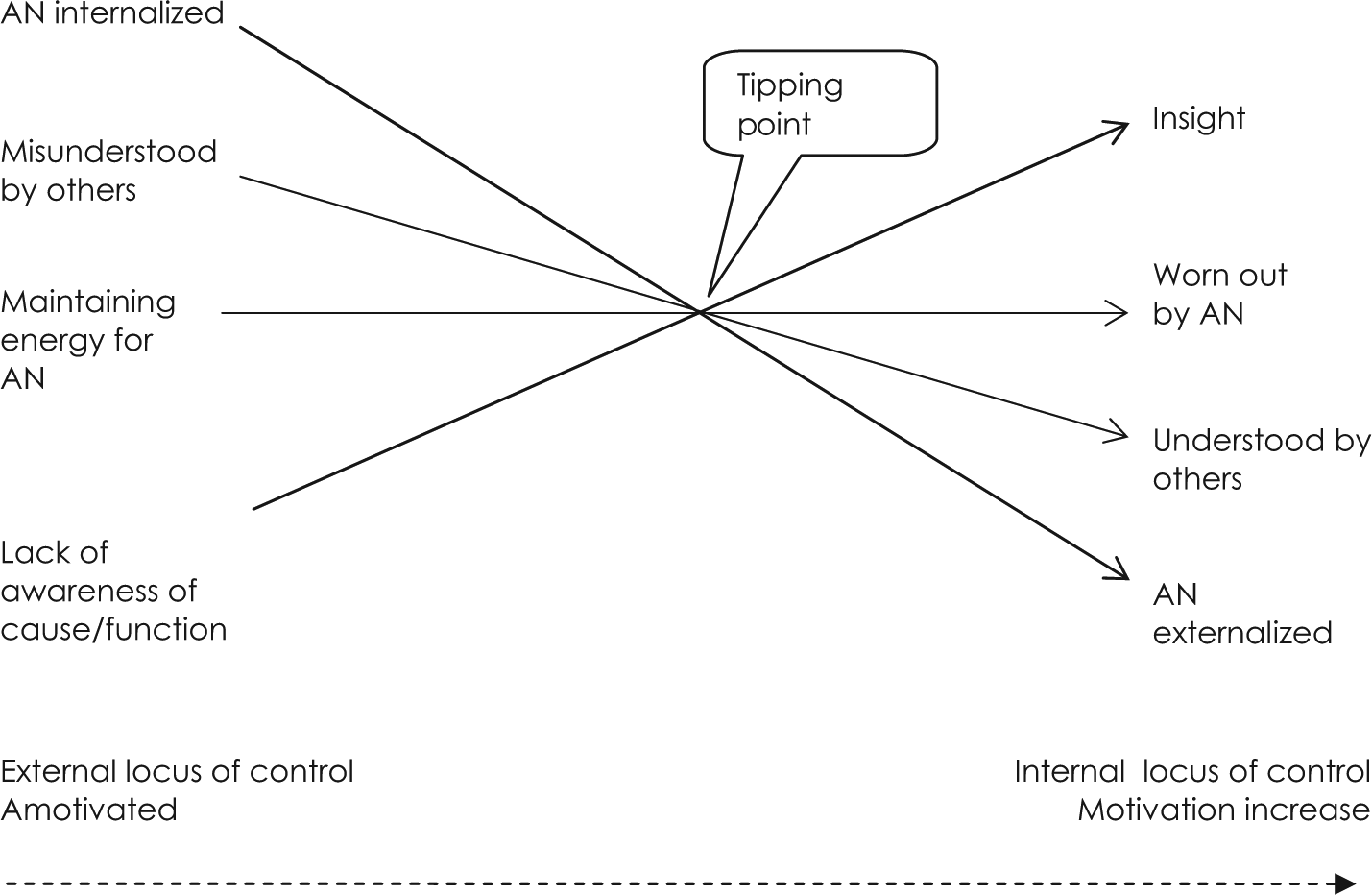
Factors that led to the tipping point of change.
From maintaining energy to being worn out by AN
As the AN progressed (somewhere between 5 and 22 years), participants became exhausted, defeated, and depleted from years spent living with the illness. Negative feelings associated with AN had accumulated and amassed over time, leading to an eventual climax when participants could no longer maintain energy for the disorder. Some described a sense of “hitting rock bottom.” The combination of the severity of the AN and the long-term endurance of the illness led to changes in the perception of AN from something of potential value to something that was damaging and unproductive:
It was a very hard time for me. I got scars on the back of my hands from where they hit my teeth when I made myself sick. I got very bad acne around my face, my eyes were sore and bloodshot, and my teeth lost enamel from the bile because it corroded my teeth. The eating disorder was very exhausting and it took up a lot of my time. After years of this, I realized the eating disorder wasn’t getting me anywhere. It wasn’t achieving anything. It wasn’t helping me in any way. The eating disorder began to spiral out of control. I found myself bingeing, dieting, bingeing, dieting. It was awful. It felt like I was just always spiraling toward the next disaster. I couldn’t handle it anymore.
From lack of awareness to insight
The women started to gain more insight into the nature of AN. For half the participants, whose AN had developed in the context of childhood trauma, an increasing awareness about the possible cause or function of the AN began to emerge. One participant remembered being abused by her brother as a child, and her need for control made more sense. Another participant realized that she was using AN to feel good about herself because of feeling shamed as a child. Two women also partly recalled childhood traumas:
I started to become aware that the anorexia wasn’t a choice—it was a reaction. As a teenage girl, the only thing I could control was my body because I had no power. Exploring the issues behind the eating disorder was helpful for me—knowing where my need to be perfect came from and realizing that I achieved perfection through eating. A memory that I had completely blocked as a child was uncovered. During the course of therapy, I suddenly remembered that I had been sexually abused by my brother. This revelation was very distressing and intense for me. My need for control made a lot more sense. It seemed clearer to me why I wanted to torture myself and why I felt so controlled and angry as a child.
From internalization to externalization of AN
As the women’s insight increased, many began to externalize the illness, which assisted them in moving to the next stage:
I started to wonder that maybe a disease was controlling me and that, perhaps, I wasn’t to blame for it. . . . If it was a disease, then I didn’t have to have it. Having the strength to realize that I could get out enabled me to break out. This was a big revelation.
From being misunderstood to being understood by others
Crucially, around the same time as the women’s awareness and perception of AN were changing, most described either improvements in their current relationships or establishing new, more helpful relationships. For some, their parents came to an eventual understanding of the AN. Others found trusting relationships with psychologists, nurses, or other people with an eating disorder. Through these relationships, participants experienced support and empathy. This was in marked contrast to Phase 1:
I started to feel more understood by my dad. After that point I knew I had the support of my parents and that was really all I needed—as long as I knew they were prepared to go on the journey with me. I eventually found two amazing therapists who I stayed with until the end of treatment. One of them had had an eating disorder herself, and she was by far the most important therapist I had ever seen. It felt like she was reading my mind. She understood it and she instilled hope that I could get over it.
When locus of control becomes internal and motivates change
The aligning of the key factors in time, particularly weariness with AN in the context of support and understanding from others, tipped the balance in favor of the pursuit of recovery. Not all factors were necessary for this to occur. Many participants could recall particular moments or turning points. There was a sense of, “Enough!”: “After eight years of going in and out of hospital, I decided I was sick of it. I was sick of yo-yoing in and out of hospital. ‘That’s it!’ I thought.” These moments were often intensely emotional: “The fact that I was seriously considering suicide scared the shit out of me and I knew I needed to get well. Thinking about suicide was a turning point for me. I knew I wanted to live.”
At the tipping point, two key factors emerged: an increase in motivation and the establishment of an internal locus of control. Participants now wanted to recover and felt more able to do so. Most participants recalled making a conscious decision to recover at this stage:
Being in hospital on Christmas day was awful. I felt so alone and, like, the staff were not trying to help me. That day a man died from anorexia in the hospital. It became very clear to me then that you could die from anorexia. I had seen him die. It became very real then. It hit me that I wasn’t normal, and I was so sick of battling my brain. I had to make a decision: Am I going to let myself die, or am I going to beat this and make a go of my life? I made a conscious decision to get better. That day was a turning point.
All participants began to demonstrate some form of agency over their AN, with decisions to change self-determined and self-initiated rather than instigated or mediated by others: “In order to get out of it, I had to decide to do it and also decide on the path to take. . . . Nobody else was going to do it for me.” “It was something I had to make a choice to do, and I made that choice because I didn’t want to be a prisoner anymore.”
Phase 3: Active Pursuit of Recovery
The tipping point did not lead to the resolution of symptoms; rather, it triggered a process of action. During this phase, participants focused on the active pursuit of symptom reduction. Although many of the women had previously attempted to take action against the AN, the quality of their motivation was different now. Challenging the AN was still difficult but they were now motivated and determined to change their behavior:
When I reached a crossroad, I could either listen to the eating disorder or challenge it. I would say to myself, “Right, that’s the eating disorder. I know I’m going to feel bad. I know it’s uncomfortable but I need to challenge this now. I choose to challenge this now.” It was really up to me.
A wide variety of skills were used at this stage, including goal setting, externalization of the AN, cognitive challenging, behavioral challenging, helpful self-talk, self-awareness/mindfulness, learning to be flexible, and the learning of alternative healthy coping skills: “I would work on changing something in my food and getting a sense of a normal portion size. Gradually I started to step out of the eating disorder and create new rules—rules with more of a life involved.” Some developed these ideas through treatment, which was now perceived as more helpful. Some sought out or re-engaged with treatment at this stage and noted improved relationships with clinicians. For some, treatment during this stage was very important; others pursued recovery by themselves.
Skill development and habit formation were extremely difficult and challenging, requiring a great deal of persistence and self-discipline over many years. Healthy behaviors had to be repeatedly practiced until a new way of life was created:
I changed my mindset and changed my thinking. I shifted to believing that eating equaled health, well-being, freedom, lifestyle, and choice. It almost felt like reprogramming myself, like reprogramming a computer. . . . It was difficult, though, for me to change my thinking, because I felt like I’d brainwashed myself. . . . It was hard to turn it all around. It took me a long time.
Recovery during this phase was certainly not straightforward. Participants described having good and bad days, and sometimes stated that motivation would wane. The determination to “do what it takes” and not be beaten by the AN enabled them to win through:
After I had made the conscious decision to get better, I started to do what the staff told me to do. It was absolute hell. I kept telling myself, though, that the devil was a sickness that was trying to take a hold of me and I wasn’t going to let it, otherwise I would die.
At this point, more value was placed on life outside the AN than the disorder itself: “I’m stronger than this; I’ve got so much to live for.” Participants accepted that their plans for life could not be achieved while living with AN, and they used this knowledge to maintain motivation over time: “I would challenge the eating disorder because I wanted to get more out of life.” They were more in control during this phase, driving change from within rather than being controlled by AN. Each success was seen as a victory over the disorder, leading to greater self-efficacy and change: “Once I started to break the eating disorder patterns, I realized I could do it, and it felt like these experiences were adding to my life.” The active fight against the eating disorder took a long time, somewhere between 2 and 10 years.
Phase 4: Reflection and Rehabilitation
The final phase was characterized by the maintenance of achievements from Phase 3 but also by personal reflection, self-discovery, and self-acceptance. “Learning to love myself” was important for many participants. They described the importance of developing a capacity to be kind to themselves and to see themselves as valuable beings who deserved to be treated with respect. The women worked toward broadening their interests and engaging more with life outside the eating disorder. This was a process of self-discovery that, for some, involved rebuilding a lost identity: “It was like having a valuable smashed plate and putting all the pieces back together to rebuild your identity and reclaim it.”
Over time and as symptoms declined, participants continued to gain insight into the function or cause of the AN. “Having a reason for the eating disorder” allowed those who had experienced childhood sexual abuse to make sense of their illness:
In my forties, at a time in my life when I was relaxed and happy, I started to have flashbacks and I realized that I had been raped as a young child. I finally realized what had happened and I had a reason for the anorexia. With this understanding came some closure and I could get on with my life now.
This phase was a gradual process that took between 3 and 10 years. Although there was no clear end point, the process eventually resulted in a capacity to self-identify as recovered. For some, this was an end state; others perceived recovery as an ongoing process that required a continual awareness to identify potential future signs and triggers of an eating disorder. In both cases, however, this state was associated with feeling free of AN and feeling understood and accepted.
The experience of living with and recovering from AN was extremely hard. Some participants continued to reflect on the effect it had on them personally. Many believed it had led to an increase in strength: “If you can recover from an eating disorder, there’s not much you can’t do.” Participants reflected on what they deemed to be most important in their recovery. The belief that recovery was possible and support from others were highlighted as essential.
Discussion
The results of this study provide a framework for understanding the slow and complex process of recovery from chronic AN. Recovery for these participants spanned four phases, from inability or unreadiness to change (Phase 1), to a tipping point at which motivation increased and changed in quality (Phase 2), to action against the AN (Phase 3), and finally reflection and rehabilitation (Phase 4). These phases have some parallels with those identified in the Transtheoretical Model of Change (TMC; Prochaska & DiClemente, 1982). First developed for addictions, this model has been applied to eating disorders to describe and assess stage of change (e.g., Rieger et al., 2000). The TMC is cyclical, whereby patients might move various times through the change cycle before achieving sustained change; however, individuals in the current study did not revert to earlier phases once having progressed to the next. In accordance with other research (Wilson & Schlam, 2004), this suggests that the TMC might not adequately describe recovery from chronic AN and that a model that is more specific to AN is needed.
In line with the TMC (Prochaska & DiClemente, 1982), motivation-based interventions used in the treatment of AN often involve a decisional balance model (weighing up the pros and cons of change), with less emphasis on addressing patients’ hopelessness and helplessness about the prospect of recovery (Waller, 2012). Hopelessness was a major obstacle to change for those in the current study. This finding is consistent with other research that has found that low self-esteem and ineffectiveness predict poorer outcomes in AN (Wade, Treasure, & Schmidt, 2011). For patients who have spent years with the illness and often endured multiple failed treatments, therapeutic interventions emphasizing hope that recovery is possible might have some effect. Hope and self-efficacy might be promoted by circulating stories of recovery between those who have recovered and those who have not yet commenced recovery.
The importance of motivation in recovery from AN is well established (Federici & Kaplan, 2008; Geller, Zaitsoff, & Srikameswaran, 2005; Nordbo et al., 2012), particularly the importance of self-determined motivation (Keski-Rahkonen & Tozzi, 2005; Tozzi et al., 2003). Findings from our study underscore the importance of an internal locus of control; these findings are consistent with Self-Determination Theory (SDT; Deci & Ryan, 2000), which posits that the quality as well as quantity of motivation leads to change (Vandereycken & Vansteenkiste, 2009). According to SDT, change requires the individual to value the personal importance of the activity. When people internalize the value of change, it becomes more autonomous, and, thus more self-determined.
In this study, specific factors were identified that assisted individuals to internalize the value of change leading to self-determined action toward recovery. Such factors included the devaluation of the AN, an increase in insight, externalization of the AN, and the feeling of being understood by and connected to others. Treatments that emphasize these factors might, therefore, be helpful. Given that the data point to the positive impact of adaptive interpersonal relationships with both professionals and family, treatments that include interpersonal and family work would also be helpful. Such a treatment might be the newly developed Maudsley Anorexia Nervosa Treatment for Adults (Schmidt et al., 2012), which focuses on intrapersonal work, work with significant others, development of an identity beyond AN, the questioning of the value of AN, and externalization of the AN.
Although motivation is important, it cannot wholly explain recovery. The current research supports the view of change as a complex, multidimensional process; the women needed to progress along the continuum on key factors, and these key factors needed to align in time. This seems like an extraordinary occurrence and might explain the rarity of recovery from chronic AN. These findings also suggest that both internal (e.g., insight) and external (e.g., support from others) factors are implicated in the recovery process and that both are important considerations for treatment.
Although these research findings have contributed to knowledge about chronic AN, there are limitations. Participants self-reported the time spent with the illness because this could not, in practice, be assessed objectively. This research involved Australian women’s interpretations of their recovery; thus, our conceptualization of this process is related to the culture and gender of the participants. Future research would benefit from exploring the recovery process for men and people from other cultural backgrounds. The women in this study did not greatly examine the sociocultural context from which their AN developed and recovery took place. Future research should explore the sociocultural conditions that lead to such interpretations of recovery from AN to deepen our understanding. It is hoped that the current article has contributed to knowledge about the process of recovery and, in particular, some of the factors that might lead to a tipping point of change; however, there remains an ongoing need to extrapolate further how these mechanisms function.
Previous research has found that full recovery from AN, defined as reaching a normal body weight and developing normal attitudes toward food and the body, is possible (Bardone-Cone et al., 2010). We have documented that full recovery is also possible from chronic AN. This suggests that residual eating disorder symptoms do not necessarily persist in those recovered from chronic AN. Given this possibility, questions are raised as to the appropriateness of labeling AN as chronic. There might be a risk that the term “chronic anorexia” can serve as a self-fulfilling prophecy (Theander, 1985), contributing toward the sense of helplessness and hopelessness experienced by patients, carers, or clinicians (Waller, 2012).
Questions are also raised about the applicability of the recovery model stance in eating disorders, as has been employed in other mental illnesses such as psychosis and addictions. The recovery movement developed from the assumption that many people with severe mental illness do not recover (Roberts & Wolfson, 2004); however, as the current research demonstrates, this is not necessarily the case for AN. This model emphasizes a rehabilitative process and adaption to symptoms as opposed to striving for complete recovery; that is, absence of symptoms (Anthony, 1993). Our findings suggest that clinicians should be hesitant to abandon hope that all people with enduring AN cannot fully recover. Nonetheless, the recovery movement embraces and promotes many factors that were found to be important for participants, such as hope, autonomy, and empowerment. It is our position that the medical model and recovery model are not necessarily mutually exclusive. How these models might apply to AN is an area that requires further exploration.
In the absence of effective treatment for those with chronic AN, a new paradigm is needed. It is hoped that this article might alleviate some of the pessimism about outcomes in chronic AN while maintaining an appreciation for the great difficulty and complexity in achieving full recovery. Hope is continuously recognized as a key component in recovery from mental illness, deemed to be both a trigger of the recovery process and a maintaining factor (Schrank, Stanghellini, & Slade, 2008). As the results of this study suggest, patient and clinician beliefs and attitudes about prognosis will have important implications for outcomes. People with AN and clinicians alike are encouraged to maintain the belief that, although rare, recovery from chronic AN is possible.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.